Embed Size (px)
Citation preview

Diagnostik und Therapie -
Infektionen 2015
Univ. Prof. DDr. Wolfgang Graninger

Die „Infektionslatte“ bei Pneumonie
Masern
HSV, CMV, VZV
RSV
Influenza A/B
Parainfluenza
Adenovirus
Mycoplasma pneumoniae

Die „Infektionslatte“ bei Status febrilis
EBV, CMV
Influenza A/B
Parainfluenza
Adenovirus
Enteroviren
Mumps, Röteln, Masern
Toxoplasmose

Schwindlige Infektionsparameter
Astal
Ateich A
A-Streptolysin
A-StrepDNAase B
Candida Ag/Ak
Ak gg Mykobakterien (A60)
LBP
PCT
Fibrinogen
Ak gg. Chlamydia pneumoniae

Standardentzündungsparameter
CRP
SAA
PCT
HPT
Fe
Ferritin
Calprotectin
IL-6
IL-10
IFN-g Release Assay (IGRA)

Drugmonitoring
bei infektiösen Erkrankungen
• Aminoglykoside: Gentamicin
• Glykopeptide: Vancomycin, Teicoplanin
• Azole
• Oxazolidinone: Linezolid
• Makrolide, Rifampicin, Cyclosporin,…
• NAT2-Polymorphismus: Isomiazid, Langsamacetylierer
• IL28B – Polymorphismus
• CYP2C9 Cytochrom P450 – 2C9

Infektionsparameter
bei viralen Erkrankungen
• Transaminasen
• LDH
• Lymphopenie
• Thrombopenie
• Anämie
• Neopterin
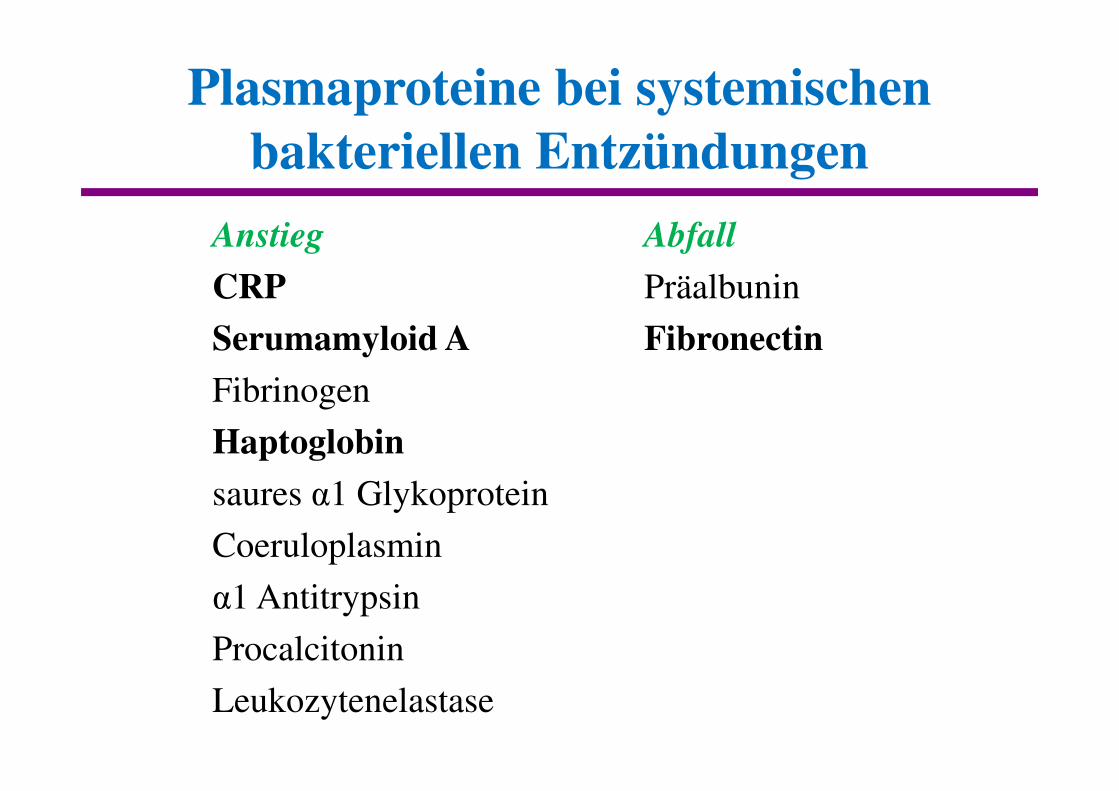
Plasmaproteine bei systemischen
bakteriellen Entzündungen
Anstieg
CRP
Serumamyloid A
Fibrinogen
Haptoglobin
saures α1 Glykoprotein
Coeruloplasmin
α1 Antitrypsin
Procalcitonin
Leukozytenelastase
Abfall
Präalbunin
Fibronectin

Direktnachweis mikrobieller Antigene
Pneumokokken Ag
Legionellen Ag
P. falciparum
Candida Ag
im Harn

Spiegelbestimmungen
• Aminoglykoside: Miniumumspiegel (vor Gabe)Kurzinfusion über 30 minMaximumspiegel (30 min nach Ende)
Einhaltung der Zeiten extrem wichtig!!!Generell angegebene therapeutische Bereiche:
Min < 2 mg/LMax 5 – 10 mg/l
• Vancomycin: Miniumumspiegel (vor Gabe)Kurzinfusion über 1 hMaximumspiegel (1 h nach Ende)
Therapeutische Bereiche:Min 5 – 10 mg/LMax 20 – 40 mg/l

Rey, 2007

Rey, 2007

Rey, 2007

Entdeckung der Antibiotika
1897 Duchesne: Penicillin
1910 Ehrlich: Arsphenamin
1935 Domagk: Sulfonamid
1942 Fleming: Penicillin
1945 Waksman: Streptomycin
Tetrazykline
Makrolide
1958 Vancomycin
1984 Chinolone

Selection of bacteria
by antimicrobial treatment
Penicillin � Klebsiella sp.
Cephalosporins � Enterococci, ESBL-E. coliCl. difficile, MRSA
Penems � P. aeruginosa, S. maltophiliaCl. difficile, C. albicans
Quinolones � S. aureus, StreptococciQR – E. coli
Vancomycin � E. coli, Klebsiella sp., VRE
COLONIZATION � INFECTION

Clostridium difficile: Massnahmen
1. Verhinderung
- restriktiver Antibiotikagebrauch!
- Händehygiene
2. Erkennung
3. Eindämmung
- Isolation / Cohorting
- spezielle Umgebungsdesinfektion

Evidence of safety and treatment effects
of faecal transplantation (n=124)
• 83% resolution of diarrhea immediatelyafter FT procedure
• 95% freedom from diarrhea for 27 months
Guo, 2012


ESCAPE
• Enterococcus faecium (VRE)
• Staphylococcus aureus (MRSA)
• Clostridium difficile (NAP1, O27, O78)
• Acinetobacter baumannii (4MRGN)
• Pseudomonas aeruginose (3MRGN, 4MRGN)
• Enterobacteriaceae(E. coli, Klebsiella sp. ESBL, 3MRGN, 4MRGN, CRE, KPC)

Percentage of P. aeruginosa isolates in HAIs
non-susceptible to carbapenems, by country
(n=756 isolates, ECDC PPS 2011-2012

Use carbapenems as initial pluripotent
antibiotics and you will end up in colonization
with:
- Candida
- Stenotrophomonas
- Acinetobacter
- Pseudomonas

Glycopeptides
Daily doses
Vancomycin 3 – 6 g
Teicoplanin 0.8 – 1.2 g
Dalbavancin
Oritavancin
Ramoplanin
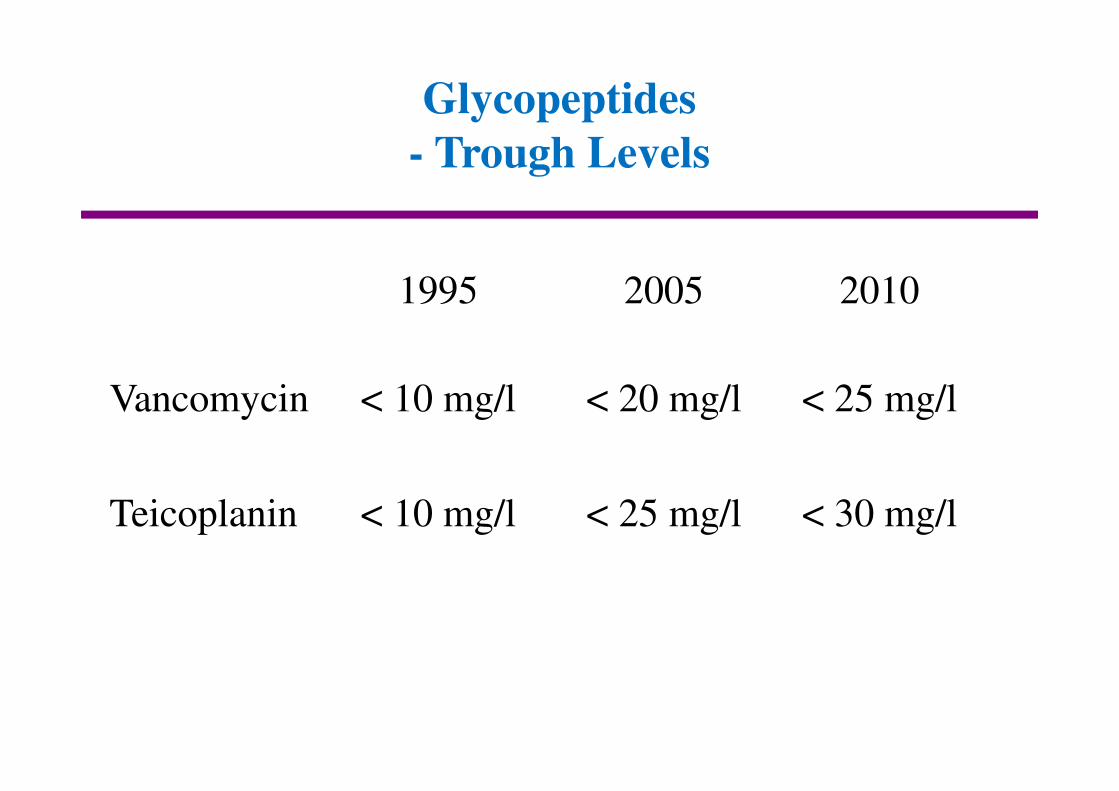
Glycopeptides
- Trough Levels
1995 2005 2010
Vancomycin < 10 mg/l < 20 mg/l < 25 mg/l
Teicoplanin < 10 mg/l < 25 mg/l < 30 mg/l

Drugs of choice against MRSA 2013
Vancomycin, Teicoplanin
Daptomycin
Linezolid
Tri/Sulf
Doxycyclin
Fusidic acid
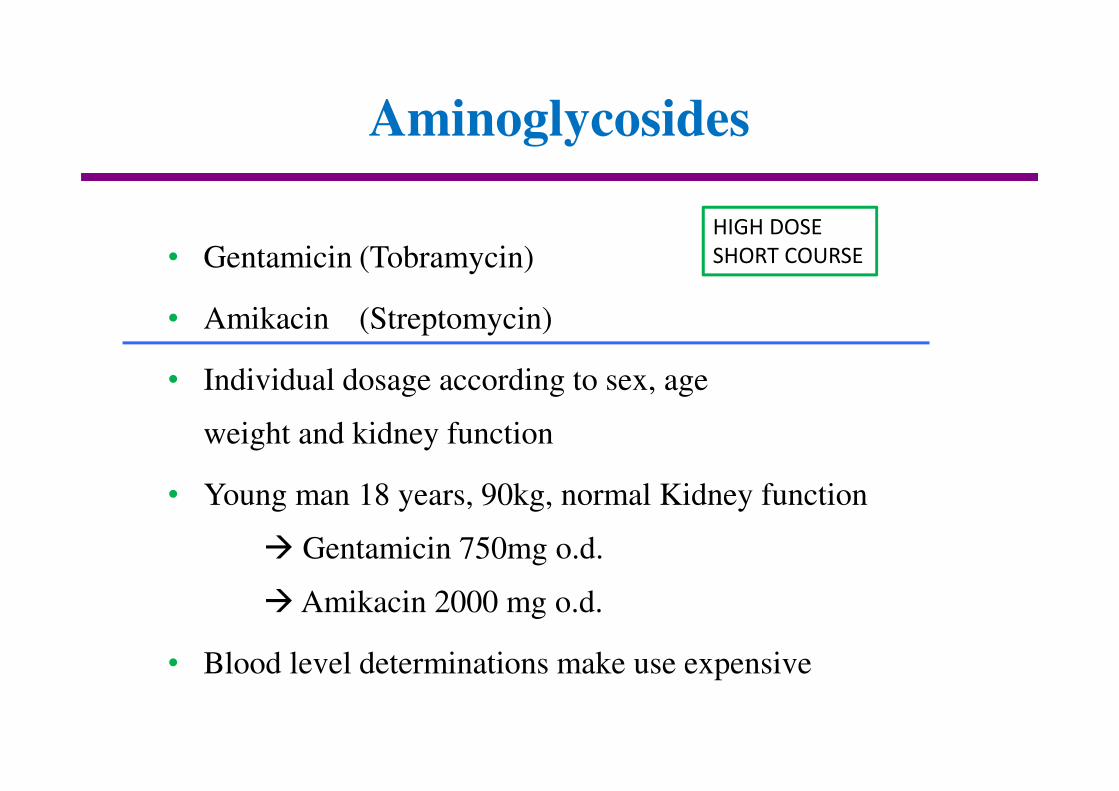
Aminoglycosides
• Gentamicin (Tobramycin)
• Amikacin (Streptomycin)
• Individual dosage according to sex, age
weight and kidney function
• Young man 18 years, 90kg, normal Kidney function
� Gentamicin 750mg o.d.
� Amikacin 2000 mg o.d.
• Blood level determinations make use expensive
HIGH DOSE
SHORT COURSE

Initialtherapie des septischen Patienten
Deeskalationstrategie
TARRAGONA
Meropenem, Vancomycin,
Fluconazol
?
Pen G
Anästhesist
Chirurg
Eskalationsstrategie
COPENHAGEN
Fluconazol
Penem
Pip/Taz, Cefepim
Amoxi/Clav, Cefuroxim
Infektosoph

Warum treten immer
mehr resistente Erreger auf?
• Geänderte Demographie?
• Geographische Unterschiede
Kenntnisse der Ärzte unterschiedlich
Einfluss der Hersteller
• Schnellere Verbreitung von Resistenzmechanismen
Kriege
Patiententourismus
� ANTIMICROBIAL STEWARDSHIP
“Rufer in der Wüste?“
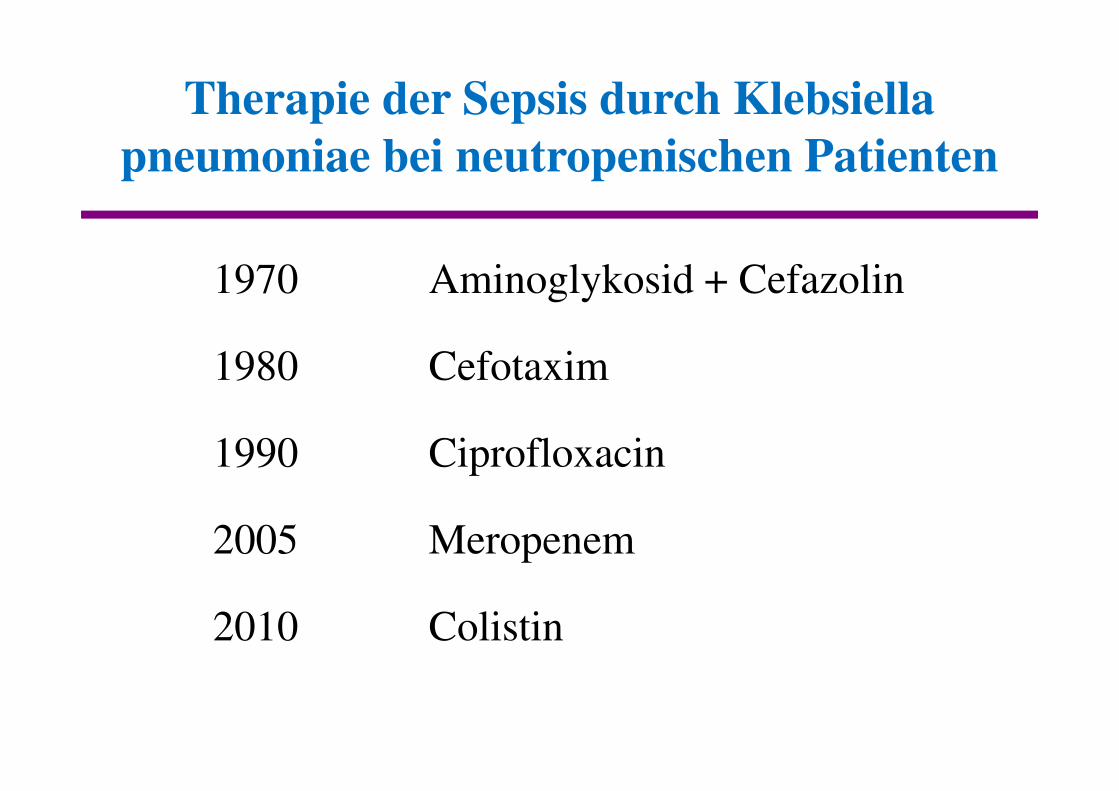
Therapie der Sepsis durch Klebsiella
pneumoniae bei neutropenischen Patienten
1970 Aminoglykosid + Cefazolin
1980 Cefotaxim
1990 Ciprofloxacin
2005 Meropenem
2010 Colistin

Therapie der Sepsis durch Pseudomonas
aeruginosa beim neutropenischen Patienten
1970 Carbenicillin 2 x 10 g
1985 Piperacillin 3 x 4 g
1995 Ceftazidim 3 x 2 g
2005 Meropenem 3 x 2 g
2015 Colistin ?

Optimierte Verwendung von Antibiotika
• Schmalspektrum-AB
z. B. Pen G bei Streptokokken
Oxacillin bei Staphylokokken
Fidaxomicin bei Clostridium difficile
• Verwendung von Breitspektrum-AB beim Patienten mit Sepsis, Erreger unbekannt
z. B. Piperacillin/Tazobactam
Amoxicillin/Clavulansäure
• Vermeidung der Peneme als Initialtherapie, die “Deeskalation“ findet nie statt
• Bronchialsekrete (auch BAL) nicht überbewerten, meist nur Kolonisation (Pseudomonas, Candida, Sterotrophomonas, Acinetobacter)
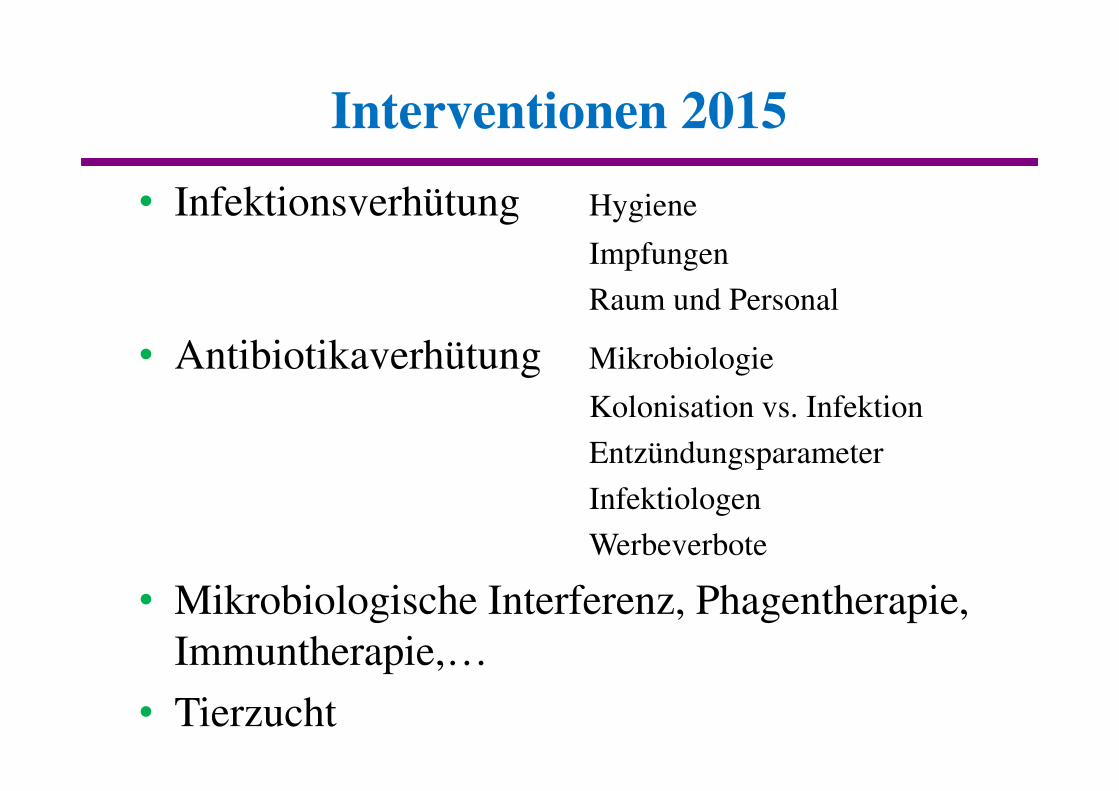
Interventionen 2015
• Infektionsverhütung Hygiene
Impfungen
Raum und Personal
• Antibiotikaverhütung Mikrobiologie
Kolonisation vs. Infektion
Entzündungsparameter
Infektiologen
Werbeverbote
• Mikrobiologische Interferenz, Phagentherapie, Immuntherapie,…
• Tierzucht

Was gibt es Neues 2015?
Ceftarolin
Ceftobiprol
Ceftazidim + Avibactam
Dalbavancin
Oritavancin
Torezolid
Nemonoxacin
Finafloxin
Surotomycin
Fidaxomycin

Sepsis – was kann ich außer
AB geben noch tun ?
• Immunglobuline
• AT 3
• Anti-TNF
• Akt. Protein C
• Hydrocortison
• Clucosekontrolle
• Physostigmin
• Fokussanierung
?

Perspektiven 2013/15
• Es gibt (momentan) keine neuen marktreifen Antibiotika
• Die Verwendung der derzeit existierenden Antibiotika muss optimiert werden.
“Antibiotic stewardship“
• Mikrobiologische Methoden müssen beschleunigt werden – mit 24 Stundenservice
• Der Einfluss von Herstellern auf den Verschreiber muss objektiviert werden
• Isolation, Hygienemaßnahmen

Acute Phase Proteins
Positive acute phase proteins
Serum amyloid A
C-reactive protein
Haptoglobin
Fibrinogen
Coeruloplasmin
α-1-acid glycoprotein

PCT, SAA und CRP Serumkonzentration
nach TNF-Infusion
Nijsten 2000

PCT, SAA und CRP Serumkonzentration nach 7
Tagen IL-6 -Infusion

Lebersynthese nach TNF bzw. IL-6
Exposition in vitro
Nijsten 2000

PCT und IL-6 bei neonataler Sepsis (n=17/9)
Tag 0 Tag 3 Tag 7
PCT Überlebt 2-89 (10) 0.2-92 (1) 0.2-69 (0.7)
Tot 0.4-68 (3) 0.4-94 (9) 4.8-96 (92)
IL-6 Überlebt 4,8-78 (20) 2.1-43 (9) 1-24 (3.7)
Tot 3.1-18 (10) 9.8-39 (22) 11-55 (40)
Kocabas, 2007
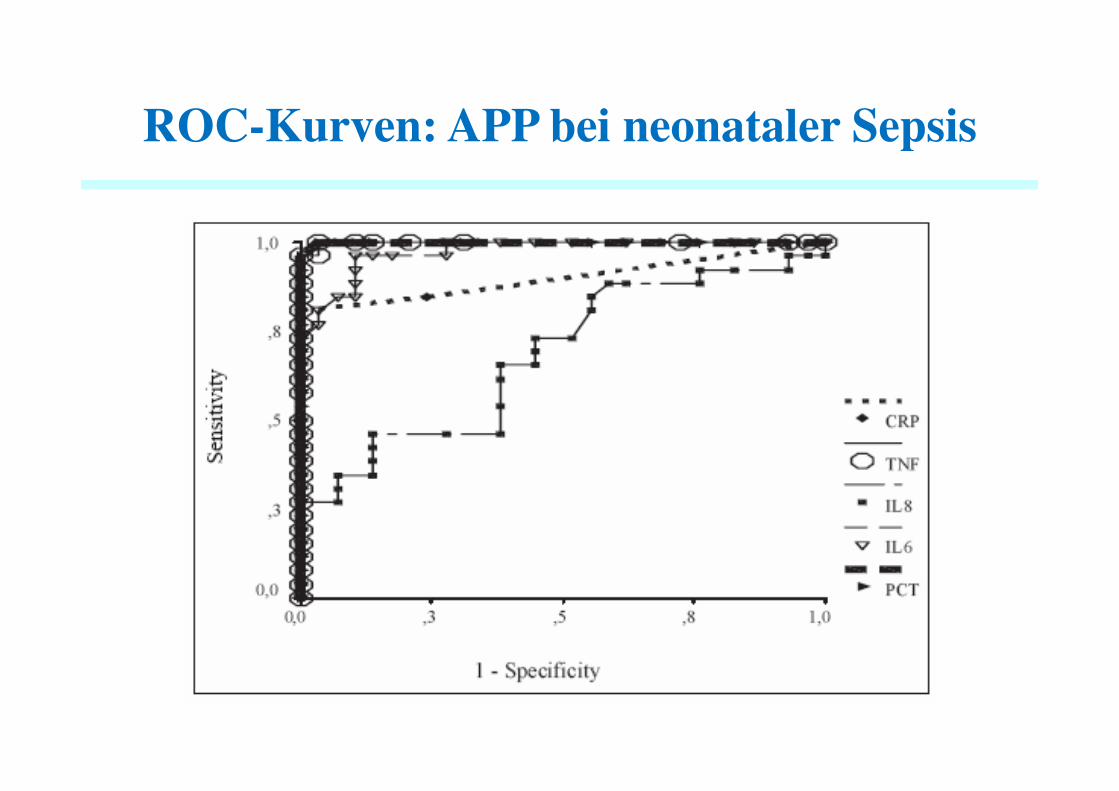
ROC-Kurven: APP bei neonataler Sepsis
Kocabas 2007

Accuracy of PCT for sepsis diagnosis
• 18 studies: sensitivity and specificity of 0.78
procalcitonin cannot reliably
differentiate sepsis from other
causes for SIRS
• Evidence does not lend support to the
widespread use of procalcitonin test
Tang, Infection.the lancet 2007

Acute Phase Proteins
Negative acute phase proteins
Transferrin
Transthyretin
Rehinolbindung protein
Fibronectin
Albumin

Fibronektin
• In der Leber synthesiert
• Permanent nieder = Zi, …
• Vorübergehender Abfall nach
Zytokinsturm z.B. Sepsis
• Fibronektin < 8 mg/dl = tot
> 40 mg/dl = hält alles aus
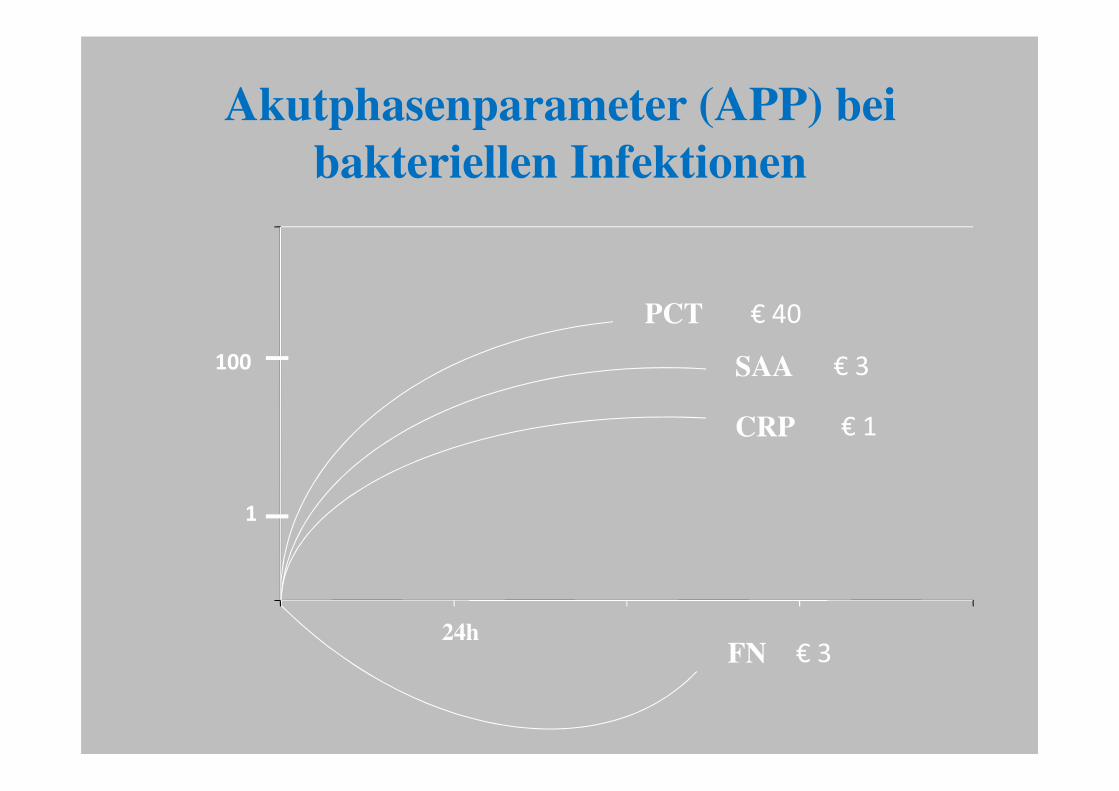
Akutphasenparameter (APP) bei
bakteriellen Infektionen
PCT
SAA
CRP
FN24h
1
100
€ 40
€ 3
€ 1
€ 3

Reaktionsschnelligkeit der Sepsisparameter
TNF
IL-6
PCT
SAA
CRP
FN
PA
HPT

Fehlerquellen
• Anstieg der APP zu träge
PCT > CRP > HPT
• Nur einmalige Bestimmung
• Insensitive Methoden zur Bestimmung
• Andere ‚Entzündungsquellen‘
Malaria, Trauma, Verbrennungen
FMF, Pankreatitis

Gesunder Patient stirbt zufällig
• 52 jähriger Polizeibeamter mit nutritiv toxischer Hepatopathie
• wird 500m von Wirtshaus entfernt im Straßengraben benommen aufgefunden
• Ausnüchterungszelle – wird nicht nüchtern
• Krankenhaus: benommenkein PCT, kein CRPTemp. 37,5°C
�
abwarten
• Tot � Obduktion: Pneumokokkenmeningitis





























