Embed Size (px)
DESCRIPTION
Discussion of Case. 疑难病例讨论. 神经内科 魏微 2006.12.20. Case Characteristic. This patient is a female with age 79 Acute onset Initail symptom was headache and fever The situation aggravated rapidly, dead after two weeks - PowerPoint PPT Presentation
Citation preview

Discussion of Case

疑难病例讨论
神经内科 魏微2006.12.20

Case Characteristic
This patient is a female with age 79 Acute onset Initail symptom was headache and fever The situation aggravated rapidly, dead after two
weeks She had congenital heart disease, cardiac
inadequacy occurred gradually

病历特点
患者 79 岁,高龄女性 ; 急性起病 ; 首发症状为头痛、发热; 病情进展迅速,发病到死亡 2 周; 既往有先心病病史,逐渐出现心功能不全;

Medical examination
Breathing sound of lungs was coarse, moist rale could be found.
Heart bouncary expanded, heart rate was irregular, double phase noise was found in cardiac apex
Liver was under costa 3CM Two sides Babinski was positive by nervous
system check

体格检查
双肺呼吸音粗,可闻及湿性罗音 ; 心界扩大,心律不齐,心尖部可闻及双期杂音 ; 肝脏肋下 3CM; 神经系统检查双侧 Babinski 征阳性。

Auxiliary examination
Lab examinaion: BUN10.5mmmol/l, WBC was normal, neutrality classificatin was a little high.
Imageology examinaion: Lung CT :There was double-lung lump shadow,
the shadow of heart expanded Brain MRI was normal

辅助检查
实验室检查: BUN10.5mmol/l ,白细胞正常,中性分类高。
影像学检查: 1 )胸部 CT 双肺团块影、心影增大;符合心
力衰竭。 2 )头颅 MRI 平扫未见异常;

Auxiliary examination
Heart ultrasonic inspection: atrial septal defect(ASD), tricuspid incompetence, arteria pulmonalis expandation, pulmonary valve backstreaming, mitral regurgitation(MR), composite congenital heart disease.
ECG: atrial fibrillation with conduction block (CB) on right bundle branch(RBB)

辅助检查
心脏超声检查:房间隔缺损、三尖瓣关闭不全、肺动脉扩张、肺动脉瓣返流、二尖瓣返流;符合先心病。
心电图提示:房颤伴右束支传导阻滞

Diagnosis Analysis

诊断分析

Location Analysis
Double-side pyramidal tract damage based on double-side pathology were positive.

定位分析
根据双侧病理征阳性定位于双侧锥体束损害。

Qualitative Analysis:

定性分析及诊断:

Diagnosis 1: menigeal canceration
support: The sufferer is senile. Acute/subac onste Heavy headache No physical sign for cerebrum parenchyma damage Brain MRI is normal Suspectable focus of infection on lungs Possibility of menigeal canceration cannot be excluded

诊断 1. 脑膜癌病 支持点: 患者高龄 急性 / 亚急性起病 头痛剧烈 无脑实质损害的定位体征 头颅 MRI 检查未见异常 可疑的肺部占位病灶 不能除外脑膜癌病的可能

nonsupport: No cancer cell found by cerebrospinal fluid
cytological examination. No abnormal found by enhanced MRI

不支持点: 1. 无脑脊液细胞学检查发现癌细胞的证据
2. 无增强 MRI 检查结果

Menigeal Canceration
Menigeal Canceration is meninges diffuse infiltrating by cancer cell.
It can be classified as primarily and metastatic, the later is more popular and of which lung cancer metastasis is more common.
Symptom of brain is headache,emesis, obvious meningeal irritation sign. Its main characteristic is severe headache, gradual aggravation. Sometimes behaved as epileptic attack, awareness and mental aberration

脑膜癌病是脑脊膜弥漫性癌细胞浸润。 分原发性、转移性,以后者多见,其中肺癌脑
转移最常见。 脑部症状以头痛、呕吐、脑膜刺激征突出,剧
烈头痛、渐进性发展、不缓解为特点。部分可表现癫痫发作、意识及精神障碍。

This disease can also has fever, but usually low-grade fever, which is caused by metabolic product of tumor diffused into blood and this is different from fever caused by infection.
Examination of cerebrospinal fluid is important to diagnose this disease. Its criteria is high pression of skull, high WBC in cerebrospinal fluid, high proteinum and low carbohydrates.

本病也可出现发热,但一般低热,系肿瘤代谢产物进入血液引起,与感染性发热不同。
脑脊液检查对本病诊断有重要意义。颅压高、脑脊液白细胞高、蛋白高、糖低。

It cannot exclude possibility of this disease if no malignant cell found in cerebrospinal fluid. Multiple examination of cerebrospinal fluid can improve the detection rate of malignant cell.
Using CEA/EMA immunocytology examination can also improve the detection rate.

脑脊液细胞学检查未找到癌细胞不能排除本病,反复多次查脑脊液可提高癌细胞的检出率。
用 CEA/EMA 免疫细胞学检查可提高检出率。

This disease behaved as complication and diversification. And it is difficult to to make a definite diagnosis. Especially primary lesion is usually masked. Damage of nervous system simply reflects as headache, which make diagnosis more difficult.

该病临床表现复杂化、多样化,生前诊断很困难,常易漏诊、误诊。特别是原发病灶隐蔽、神经系统损害单纯表现为头痛诊断更加困难。

Summary1: This sufferer should have done further lumbar
puncture cerebrospinal fluid cytology examination if condition allowed.
If cortical sulci nodus focus of infection or irregular thickening of meninges can be found by Enhanced Skull MRI examination, this assumption can be furthersupported.
Meningeal carcinomatosis has two types: diffuse and focal. And can occur diffuse linetype intensification or nodus intensification

回顾总结 1
该患者如有条件应进一步腰穿脑脊液细胞学检查。
头颅增强 MRI 检查如发现脑沟池内结节病灶或脑膜不规则的增厚强化进一步支持诊断。
脑膜癌病肿瘤生长以弥漫性和局灶性两种,可出现弥漫性线型强化、结节型强化。

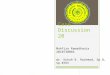
脑脊液细胞学检查

头颅MRI平扫未见明显异常 增强扫描可见脑膜明显强化

头颅MRI平扫未见异常 增强扫描可见脑膜明显强化

图 1. 矢状位TWI扫描脑膜未见异常图 2. 水平增强TWI扫描 , 见硬脑膜 蛛网膜沿颅骨内侧面呈线型、弯曲状增强 , 该增强不伸入脑沟

图 3. 冠状位增强T 1 WI扫描 , 见小脑幕、大脑镰增强 ( 箭头 ) 图 4. 横轴位增强扫描显示主要为软脑膜 蛛网膜下腔弥漫性增强 , 该增强伸入脑沟

图 5 横轴位T 1 WI扫描脑膜未见异常 图 6 增强T 1 WI扫描 , 见硬脑膜 蛛网膜增强 ( 箭头 ) 同时伴有软脑膜、 蛛网膜下腔弥漫性增强

Currently, mixed intensification found by enhanced skull MRI is an important symbol for meningeal carcinomatosis diagnosis.
If primary lesion in lung could be confirmed, it might be meninges carcinomatosis complicated by lung cancer.
But the patient's family refuse further examination, so we couldn't find related evidence.

目前认为头颅 MRI 增强扫描混合型强化是脑膜癌病与其他鉴别的重要标志。
如能确定肺部原发病灶可考虑肺癌并发脑膜转移。
但患者家属拒绝进一步检查,无法寻找诊断证据。

Diagnosis 2: Brain metastases tumor
support: old age heavy headache had doubtful primary lesion in lung
nonsupport: No abnormal found by brain MRI

诊断 2. 脑转移瘤
支持点: 患者高龄 头痛剧烈 有可疑的肺部原发占位病灶 应考虑肺癌脑转移瘤不支持点: 头颅 MRI 平扫未见异常

Brain has rich blood suply,and its blood flow accouns for 20% in the body. The possibility of lung cancer embolus transferred to brain is high.
Moreover, lung cancer has the characteristic of addict to nerve tissue, expecially for central nerve. So it is easy for lung cancer embolus transfer.
Intracranial metastasis focus has four types: 1.brain essence transfer,2 skull metastasis focus 3. scleromeninx metastasis focus 4. meninges metastasis focus.

脑具有丰富的血液供应,血流量占全身血流量20% ,肺癌栓子转移到脑组织的机会高,另外肺癌具有嗜神经组织的特性,对中枢神经组织具有特别的亲和力,肺癌脑转移发生机率大。
颅内转移灶有四种形式: 1 )脑实质转移 2 )颅骨转移灶 3 )硬膜下转移灶 4 )脑膜转移灶。

As for this patient, no abnormal found by skull MRI, while most brain metastases tumor can be confirmed by MRI
But a very few cases in early phase, MRI cannot find abnormal symbol.
Enhanced MRI should be used if highly suspect brain metastases tumor. Sometimes even dosis of constrast medium can be added.

患者头颅 MRI 检查未见异常,绝大多数脑转移瘤 MRI即可诊断。
但极少数病例在转移的早期,或者病灶位于皮层, MRI 平扫不能发现异常信号。
当临床高度怀疑脑转移瘤时应增强扫描,甚至造影剂可加大剂量。

肺癌脑转移 , MRI增强可显示平扫未显示的转移灶

左图为左颞叶单发转移右图为MRI增强显示为多发转移

when brain metastases tumor happens, part of blood brain barrier (B.B.B.) will be damaged. Newly born micrangium of tumor develops badly.So permeability is high. Enhanced CM Gd-DTPA easilly permeates into interstitial fluid.Enhanced scan can discover focus of infection, which cannot be found by plain scan.

脑转移瘤时局部血脑屏障破坏,肿瘤新生毛细血管发育差,通透性增加,增强对比剂 Gd-DTPA极易渗透到局部组织间液中,出现显著强化,平扫时不能显示的病灶增强时可显示。

Summary 2:
Enhanced scan can find more ealier focus of infection, and improve detection rate. Especially for little focus without peripheral edema, it has more importance.
This patient didn't do enhanced skull MRI, so brain metastases tumor cannot be excluded.

回顾总结 2
增强扫描可以发现更多更早的病灶,从而提高病灶的检出率,特别是对于没有周围水肿的小病灶诊断意义更大。
本患者未能进行增强头颅 MRI 检查因此不能完全除外脑转移瘤。

Diagnosis 3: Cerbral Tuberculosis
Support: Headache Low-level fever in afternoon no symptom of brain essence damage nodus shadow discovered by lung CT scan

诊断 3. 结核性脑膜炎:
支持点: 头痛 午后低热 无脑实质损害定位体征 肺部 CT 提示多发结节影

Nonsupport:
acute onste no abnormal in blood sedimentation no result of PPD no result of sputum culture no abnormal in skull MRI no support from lumbar puncturecerebrospinal
fluid examination fever could also be caused by lung infection

不支持点: 急性起病 无血沉结果 无 PPD 实验结果 无痰涂片、痰培养结果 头颅 MRI 未见异常 无腰穿脑脊液化验结果支持 发热也可用肺感染解释

Summary 3: Cerebral tuberculosis usually behaved as high pression in
head, and meningeal irritation sign is positive. Sometimes it will aggravate into hydrocephaly, hydrocephalus or cerebral hernia dead.
Recently the number of old phymatiosis sufferer increases. Old people immune function decrease, so the rate of phymatiosis increases. usually they have no typical clinical symptom, light toxic symptom, meningeal irritation sign might not be clear. Besides many old sufferer have complication for heart and lung,symptoms are easily masked.

回顾总结 3
结核性脑膜炎一般有高颅压症状,脑膜刺激征阳性,有颅神经受累,进行性加重可出现脑积水、脑水肿加重,脑疝死亡。
近年来老年结核患者增多,老年人免疫功能低下,结核发病率上升,临床症状不典型,结核中毒症状轻,脑膜刺激征可以不明显,老年患者多有心肺合并症,症状易掩盖。

Cerebrospinal fluid may be not typical, positive phymatiosis antibody in cerebrospinal fluid can support the diagnosis; but due to Bacillus Tuberculosis has cross-immunity, so positive phymatiosis antibody can not completely confirm the conclustion.
We can try to find some images evidence, such as meninges linetype intensification by enhanced MRI scan. Sometimes Bacillus tuberculosis establisth tuberculoma, which result in segment intensification. But they only appear in the base of skull instead of above meninges or below ependyma.

脑脊液化验可以不典型,血 / 脑脊液结核抗体检查阳性支持诊断,结核分支杆菌有交叉免疫性因此阳性也不能完全确诊。
可寻找影象学证据,如头颅 MRI 增强扫描可见脑膜线型强化,有时结核杆菌在颅底形成结核球而出现结节型强化,但一般只出现在颅底而不会出现在脑膜表面或室管膜下。

Diagnosis 4: congenital cardiopathy (atrial septal defect, patent ductus arteriosus)Support: has related disease history cardiac murmur by AUSC cardiac dilatation, liver expand supported by heart hypersound examination

诊断 4先心病(房间隔缺损、动脉导管未闭 )
支持点 有先心病史 听诊心脏杂音 查体心脏扩大、肝脏肿大 心脏超声证据支持诊断

Diagnosis 5: Infective endocarditis
Support: patent ductus arteriosus easily results in
concurrent infection for endocarditis property of cardiac murmur changed bloody urinenonsopport: no direct evidence for endocardium infection ---
find ecphyma in heart inner membrane positive result no found by bl.cult

诊断 5 感染性心内膜炎支持点 有动脉导管未闭易合并感染性心内膜炎 心脏杂音性质改变 镜下血尿不支持点 无心内膜受累的直接证据——超声心动图发现
心脏内膜赘生物 无血培养阳性结果

summary 5:
Although Ecphyma not found in heart inner membrane by the first echocardiogram examinaion, examination of Infective endocarditis should be followed regularly. Based on these tracing, we can track cause and pathologic diagnosis, clinic process,curative effetive for Infective endocarditis.
Esophagus echocardiogram examinaion can be used for better discernibility.

回顾总结 5
首次超声心动图检查未能够发现赘生物 , 不能够排除感染性心内膜炎的诊断 ,应该定期追踪。
据此可以对感染性心内膜炎作出病因、病理诊断 , 评判临床进程、预后及治疗的效果。
经食道超声心动图检查 , 可以获得更佳的超声分辨能力

Diagnosis 6: Lung cancer
Support: the aged Multiple nodus shadow discovered by chest CT
Nonsupport: CT change is not typical, need further enhanced CT If focus of infection is near to the centra,
bronchofiberscopy can be used. Tumor markers and expectoration exfoliative cytology

诊断 5. 肺癌
支持点: 高龄 胸部 CT 提示多发结节影

不支持点: CT改变不典型,需进一步增强 CT 扫描明确
肺部病灶性质 如病灶位置接近中央位置,可进一步纤维支气管镜检查
肿瘤标志物、痰脱落细胞学检查结果

Antidiastole
This patient had ache in left occiput, should be distinguished from occipital neuralgia.
But the sufferer is old, had no other ache history. Nervus occipitalis is from 2-3 cervical nerve root.
So if pathological changing of meninges is limited, part of high cervical segments nerve root will be irriated, and result in severe ache of nervus occipitalis.

鉴别诊断:
1. 神经性头痛: 患者有左枕部痛,应与枕神经痛鉴别, 但患者高龄,既往无疼痛发作。 枕神经发自颈 2-3 神经根,当脑膜病变较局限时,局部高颈段神经根受刺激可出现可出现枕神经分布区的剧烈疼痛。

2. Other brain disease which can cause headache no trauma in head no loss of function for focal nerver no abnormal in brain MRI brain hemorrhage, cerebral infarction, SAH and
haematoma of dura can be excluded

2. 其他可引起的头痛的脑部疾病: 无头部外伤史 无局灶性神经功能缺失 头颅 MRI 平扫未见异常 可除外脑出血、脑梗死、 SAH 、硬膜下 / 外
血肿等

Reason of turnover
Great age Servere concomitant disease, cardiopathia Congestive heart failure caused by congenital
cardiopathy, and complicated wih lung infection or doubtful lung cancer.
Bad cardiorespiratory function is the main reason of accelerated dead.

转归原因
患者高龄; 严重的并存疾病,先心病心衰同时合并肺感染、
可疑肺癌,心肺功能差是加速死亡的重要原因;

Sufferer concurrent infection Morbus cardiacus complicated with atrial
fibrillation, pulmonary embolism is easily caused by congestive heart failure(since esophagu sonography not done, embolus of heart internal paries cannot be excluded.)
Infective endocarditis cannot be excluded because of cardiac murmur changing and RBC in UR.

患者卧床合并感染;
慢性心脏病并发房颤病史 ,心衰患者易引起肺血栓栓塞(未行经食道超声检查,不能完全除外心脏内附壁栓子的可能);
杂音性质改变及尿中红细胞也不能完全除外感染性心内膜炎;

Abnormal clotting mechanism caused by lung cancer
Possibility of lung embolism cannot be excluded since anhelation aggravation
But further examination could not be continued.

肺癌引起凝血机制异常
呼吸困难突然加重不能除外肺栓塞的可能;
但进一步检查无法完成。

Before lung embolism, the patient's pulmonary arterial pressure was increased, so minor embolism also leads to great harm of haemodynamics.
When pulmonary arterial pressure and right ventricular pressure are increased,the right ventricle cann't afford overloaded afterloading, so the right ventricle end diastolic pressure is also increased.

肺栓塞前患者有肺动脉压升高 , 较小的栓塞就可以引起严重的血流动力学损害。
当肺动脉压升高、右心室压增加、右心室不能承受过重的后负荷时 ,则右心室舒张末压增高。

In the situation, Myocardium of right ventricle needs more coronary blood flow to provide oxygen, otherwise complic blood pressure will be down, thus to aggravate Myocardium of right ventricle ischemia and decrease cardiac output. It's possible to spur suddenly stop of breathing and heartbeating, even lead to death.

在这种情况下右心室心肌需要更多的冠状动脉血流供氧 ,如合并血压下降 ,加重右心室心肌缺血 , 进一步降低心输出量 , 有可能促使呼吸、心脏骤停 ,危及生命。

Becasue lumbar puncture was denied, enhanced MRI cann't be done, so the diagnosis isn't verified further. the possiblity of severe brain edema and centra respiratory failure cann't be excluded.
At the same time, cerebrocardiac syndrome will aggravate nonfunction all over body.

因拒绝腰穿、无法完成头颅 MRI 增强扫描,无法进一步确定诊断,不除外有严重的脑水肿,中枢性呼吸衰竭可能;
同时脑心综合征可加重全身脏器功能衰竭。

谢谢