Embed Size (px)
Citation preview
GASTROENTEROLOGY 00954543 /96 $0.00 + .20
DYSPHAGIA Evaluation, Diagnosis, and Treatment
Douglas M. Trate, MD, Henry P. Parkman, MD, and Robert S. Fisher, MD
The simple act of swallowing is actually a complex process that can be divided into three stages: oral, pharyngeal, and esophageal. During the voluntary oral stage of swallowing, a food or liquid bolus is propelled from the oral cavity into the pharynx by the coordinated contraction of several groups of striated muscles. The involuntary pharyngeal stage is characterized by bolus movement from the pharynx across the upper esophageal sphincter (UES) and into the proximal esophagus, again caused by the integrated actions of striated muscles. In the involuntary esophageal phase of swallowing, the bolus progresses aborally from the proximal striated-muscle esophagus through the smooth-muscle mid and distal esophagus, across the smooth-muscle lower esophageal sphincter (LES), and into the stomach.
Dysphagia is defined as the subjective sensation of difficulty swal- lowing and is derived from the Greek roots dys (with difficulty) and phugiu (to eat). The patient perceives that food or liquid is impeded in its aboral passage from the mouth and pharynx through the esophagus into the stomach. Dysphagia is characterized by a spectrum of sensations ranging from difficulty initiating a swallow to the perception of a hang-up or complete obstruction to the propagation of food down the esophagus. The presence of dysphagia implies that there is a problem with the anatomy (mechanical obstruction) or the motor function (functional obstruction) of the oral cavity, the pharynx, the esophagus, or the cardia of the stomach. In a recent survey of US households, 7% of people experienced dysphagia at some time during their lives, with increasing prevalence during ad- vancing years. It also has been reported that 30% to 40% of patients in
From the Division of Gastroenterology, Department of Medicine, Temple University Hos- pital, Philadelphia, Pennsylvania
PRIMARY CARE
VOLUME 23 * NUMBER 3 * SEPTEMBER 1996 417
418 TRATEetal
nursing homes have swallowing disorders. This article reviews the pre- sentation, diagnosis, and treatment of the varied pathologic conditions that result in dysphagia.
EVALUATION OF PATIENTS WITH DYSPHAGIA
History and Physical Examination
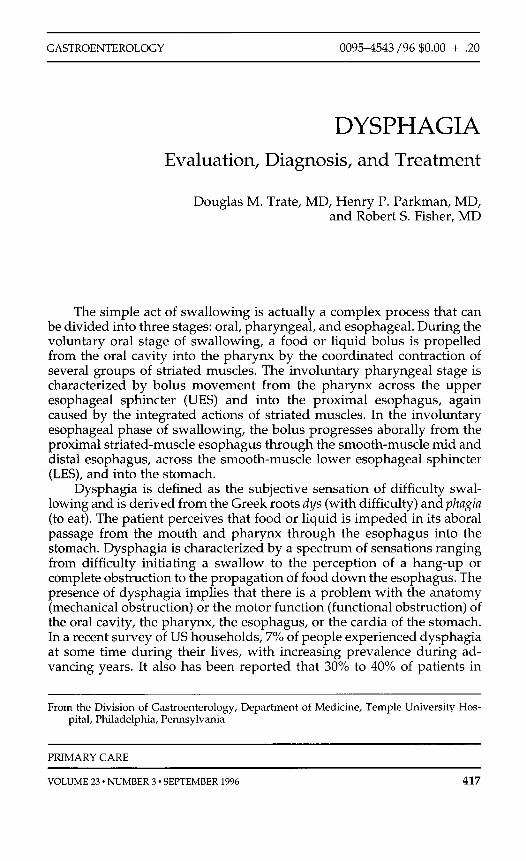
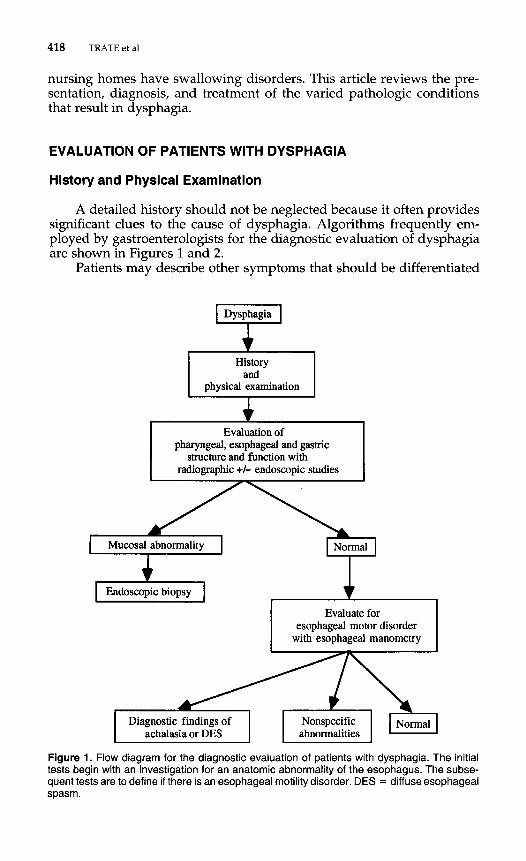
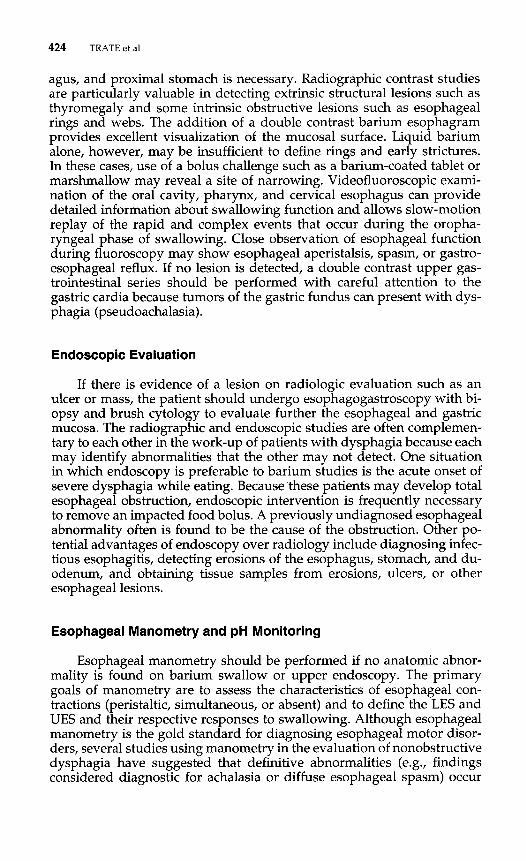
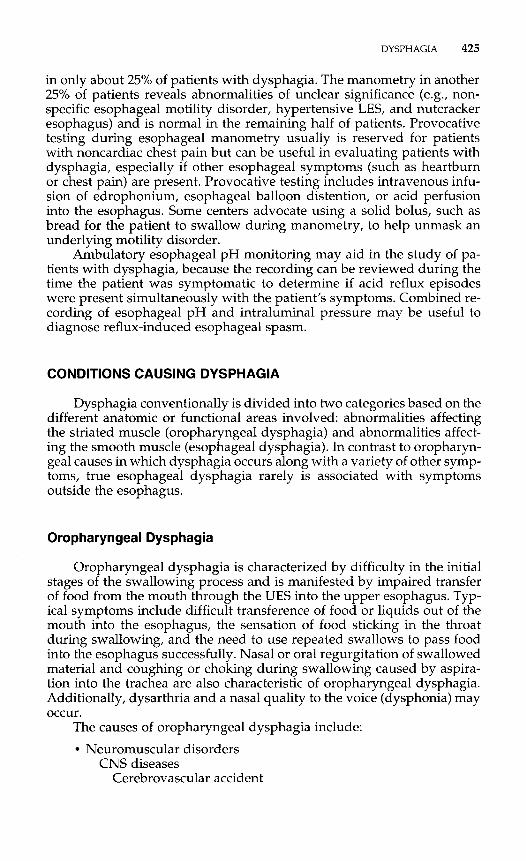
A detailed history should not be neglected because it often provides significant clues to the cause of dysphagia. Algorithms frequently em- ployed by gastroenterologists for the diagnostic evaluation of dysphagia are shown in Figures 1 and 2.
Patients may describe other symptoms that should be differentiated
D y sphagia 'i History
and physical examination
Evaluation of pharyngeal, esophageal and gastric
structure and function with radiographic +/- endoscopic studies
Mucosal abnormality Normal
Endoscopic biopsy
Evaluate for esophageal motor disorder
with esophageal manometry
Diagnostic findings of Nonspecific Normal achalasia or DES abnormalities
Figure 1. Flow diagram for the diagnostic evaluation of patients with dysphagia. The initial tests begin with an investigation for an anatomic abnormality of the esophagus. The subse- quent tests are to define if there is an esophageal motility disorder. DES = diffuseesophageal spasm.
DYSPHAGIA 419
Difficulty in initiating swallowing
Dysphagia I-r' Sensation of food stopping
or sticking after swallowing
Solids and liquids 'r' Anatomic obstruction
Figure 2. Flow diagram for history taking in patients with dysphagia to help arrive at a working diagnosis. The logic pattern depends on (1 ) the differentiation of oropharyngeal dysphagia Vom esophageal dysphagia, (2) whether the dysphagia is for solid food alone or solids and
.#rids, (3) the presence of intermittent or progressive symptoms, and (4) associated symp- IS of heartburn, regurgitation, or weight loss.
420 TRATEetal
from dysphagia. Odynophagia, or pain on swallowing, implies an inflam- matory process of the esophageal mucosa and should be distinguished from the usually painless dysphagia. Globus is the constant sensation of a lump in the throat associated with dry swallows or the need to swallow, with no readily identifiable cause. In contrast with true dysphagia, there is no difficulty when swallowing is actually performed. The symptom often is regarded as psychogenic and, in the past, often was termed globus hys tericus. With appropriate testing, however, the majority of patients with globus sensation are found to have a variety of responsible organic factors. The diagnosis of globus therefore should never be made without investigation for an anatomic lesion or motor abnormality of the oro- pharynx, larynx, or esophagus.
Useful questions to ask the patient with dysphagia include:
1. Is the difficulty with swallowing a problem in initiating the swal- low or is it that the food sticks going down after it is swallowed?
2. What kinds of food are difficult to swallow: solids, liquids, or both?
3. Is the dysphagia intermittent, or is it getting progressively worse?
4. Where does the food get stuck? 5. Did the problem occur suddenly or has it been present for some
time? 6. Are there associated symptoms such as chest pain, heartburn,
pain with swallowing, regurgitation, or a constant feeling of a lump in the throat? Are there related complaints such as hoarse- ness or coughing and choking while eating?
7. Are there associated neuromuscular symptoms such as double vision, facial droop, change in voice, muscle weakness, and dif- ficulty walking or using one’s hands to hold things?
8. Has there been weight loss in the past several months? 9. Are there any pre-existing medical conditions such as diabetes,
stroke, cancer, heart problems, or AIDS? 10. What medications are being used (including over-the-counter
medications)? Have aspirin, ibuprofen (Motrin, Advil), or in- creased amounts of antacids been taken recently?
The patient should be asked if the difficulty with swallowing is a problem initiating a swallow or if the food stops or sticks after being swallowed. A patient’s localization of the site of dysphagia may not be reliable in determining the true anatomic site of obstruction. For example, the sen- sation of dysphagia in the region of the suprasternal notch may occur as a result of an obstructing lesion anywhere along the course of the esoph- agus. In contrast, when the bolus sticks at the level of the xiphoid process, an underlying stricture, malignancy, or ring frequently is found in the lower esophagus.
Determining the type of bolus that is arrested and the temporal pro- gression of dysphagia may help differentiate between an obstructive le- sion and a motor disorder. In neuromuscular disorders, the patient typi- cally notes dysphagia for solids and liquids from the onset, whereas in patients with mechanical obstruction, dysphagia initially involves solid
DYSPHAGIA 421
foods alone and only later progresses to involve liquids. In motor disor- ders of the esophagus, the onset of dysphagia is usually gradual, with progression during many months to years. An esophageal carcinoma should be suspected if the time course of the dysphagia is characterized by rapid progression of dysphagia for solids, especially in an older patient with anorexia and weight loss. Peptic strictures typically produce low- grade dysphagia for solid food in a patient with long-standing heartburn or chronic antacid use. Episodic dysphagia for solids may be produced by an esophageal ring without other esophageal symptoms or weight loss. In the typical “beef house syndrome” caused by a Schatzki’s ring, a bolus of poorly chewed beef sticks in the lower esophagus, producing the sen- sation of dysphagia. The food bolus eventually clears, and the patient is able to finish the meal without difficulty because the ring has been auto- dilated by the beef bolus.
The patient should be asked directly about medications that may cause pill-induced esophagitis. The most commonly implicated agents in- clude tetracycline and its derivatives (doxycycline, minocycline), potas- sium chloride, iron preparations, vitamin C, quinidine and its derivatives, aspirin, and other nonsteroidal anti-inflammatory agents. Characteristi- cally, medication-induced esophagitis presents with acute retrosternal pain exacerbated by swallowing (odynophagia) and followed by dyspha- gia. Chronic esophageal injury may lead to the formation of esophageal strictures usually located in the proximal esophagus or midesophagus. Pill esophagitis is caused by local mucosal injury produced by chemical burn. The pill often becomes lodged in the esophagus at the level of the aortic arch or left atrium. Treatment includes withdrawal of the offending medication, acid suppressive therapy, viscous lidocaine for local anesthe- sia, and sucralfate slurry to coat the mucosa. To prophylax against a re- currence patients should be instructed to ingest their medications after drinking 4 oz of water, accompanied by an 8-oz glass of water followed by a 4-oz chaser of water. Medications should be taken when the patient is sitting or standing and should not be ingested within 2 hours of going to bed.
The history and physical examination of the patient may be useful in uncovering extraesophageal evidence suggesting a cause for the patient’s dysphagia.
1. Residual neurologic deficits from a previous cerebrovascular ac-
2. Typical tremor, gait, or posture of Parkinson’s disease 3. Ptosis in patients with myasthenia gravis or oculopharyngeal dys-
4. Typical hand shake, facies, or muscular wasting of myotonic dys-
5. Hyporeflexia, eyebrow changes, or skin and hair changes of hy-
6. Cervical or supraclavicular lymphadenopathy in cancer of the
7. Tylosis (hyperkeratosis of palms of hand and soles of feet) in pa-
cident
trophy
trophy
pothyroidism
esophagus
tients with cancer of the esophagus
422 TRATEetal
8. Cachexia in primary cancer of the esophagus, metastatic cancer to the esophagus (breast, lung, and melanoma), or a paraneoplastic syndrome
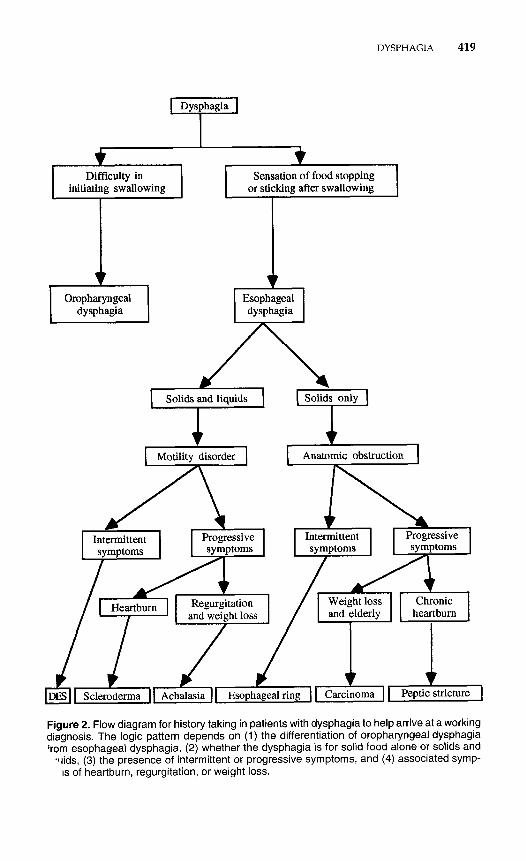
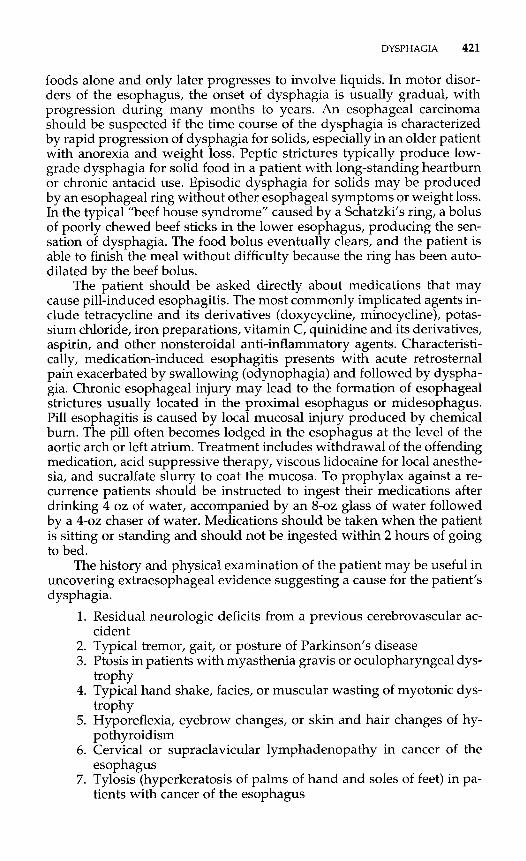
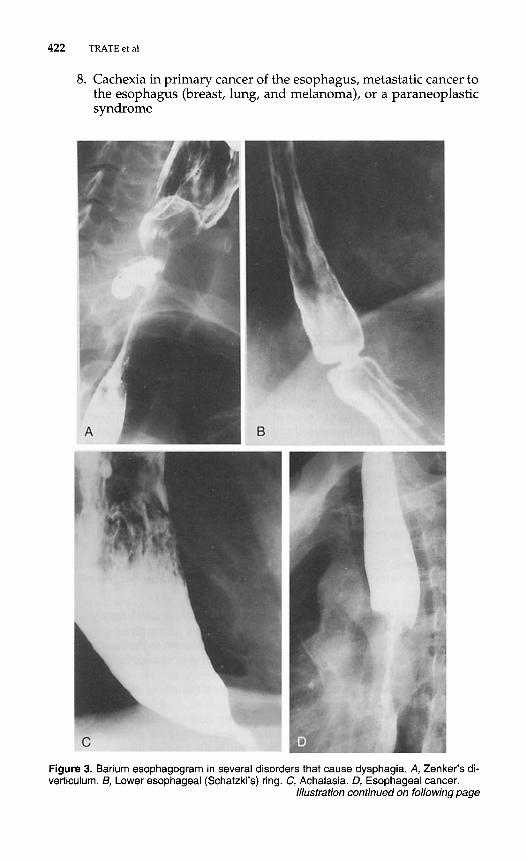
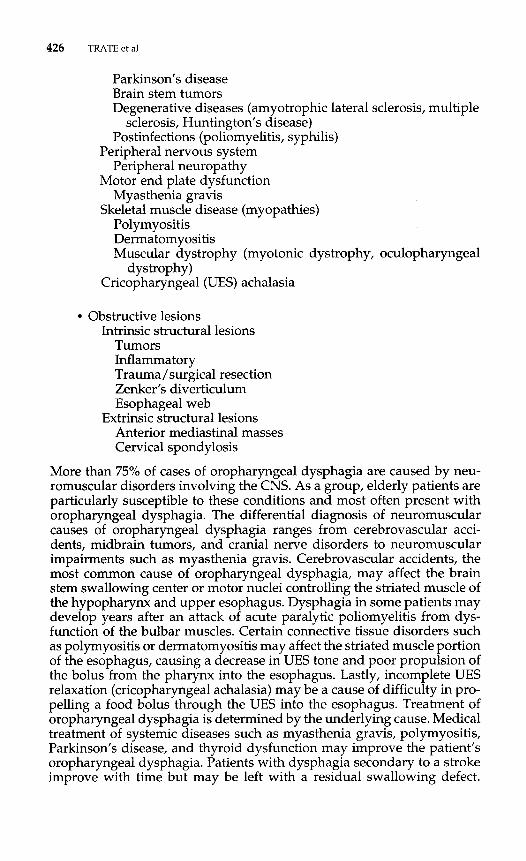
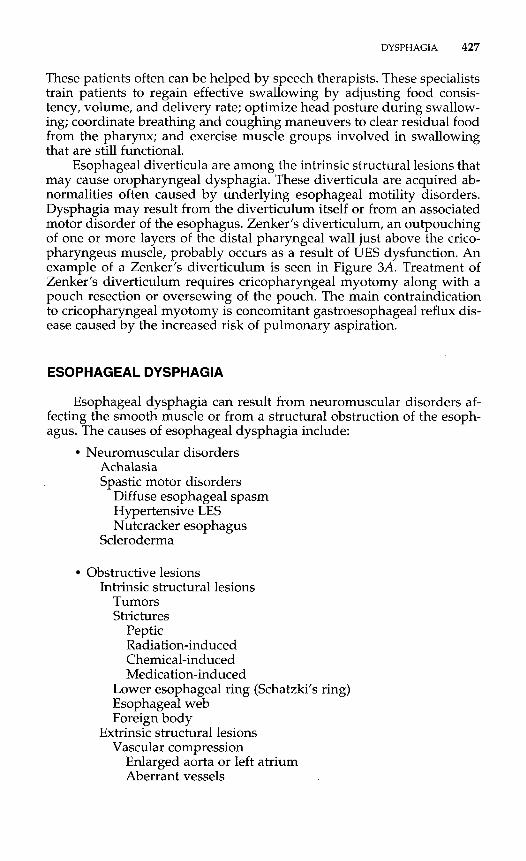
Figure 3. Barium esophagogram in several disorders that cause dysphagia. A, Zenker’s di- verticulum. B, Lower esophageal (Schatzki’s) ring. C, Achalasia. D, Esophageal cancer.
Illustration continued on following page
DYSPHAGIA 423
9. Typical sclerodactyly, facies, calcinosis, and telangiectasia of
In particular, symptoms of a cerebrovascular accident and its temporal relationship to the development of dysphagia should be a subject of in- quiry. A neurologic examination can be valuable in identifying abnor- malities of the central or peripheral nervous system that may not have been recognized by patients. In patients with rheumatologic diseases, spe- cial attention is directed to manifestations of scleroderma or the CREST syndrome (calcinosis cutis, Raynaud's phenomenon, esophageal dysmo- tility, sclerodactyly, and telangiectasia).
In general, physical examination in patients with esophageal dys- phagia is normal, except if the problem is chronic or if the patient has scleroderma. In these cases, the presence of lymphadenopathy and mal- nutrition usually reflect serious underlying disease. One also should pay attention to the mouth and pharynx during the physical examination be- cause factors contributing to dysphagia frequently are found.
scleroderma
DIAGNOSTIC STUDIES
Radiographic Evaluation
To determine if an anatomic lesion is present, a barium esophagram with views of the pharynx, esophagus, and stomach should be performed initially (Fig. 3). Because the patient's subjective localization of dysphagia may be inaccurate, radiologic evaluation of the entire oropharynx, esoph-
Figure 3 (Continued). €, DES.
424 TRATEetal
agus, and proximal stomach is necessary. Radiographic contrast studies are particularly valuable in detecting extrinsic structural lesions such as thyromegaly and some intrinsic obstructive lesions such as esophageal rings and webs. The addition of a double contrast barium esophagram provides excellent visualization of the mucosal surface. Liquid barium alone, however, may be insufficient to define rings and early strictures. In these cases, use of a bolus challenge such as a barium-coated tablet or marshmallow may reveal a site of narrowing. Videofluoroscopic exami- nation of the oral cavity, pharynx, and cervical esophagus can provide detailed information about swallowing function and allows slow-motion replay of the rapid and complex events that occur during the oropha- ryngeal phase of swallowing. Close observation of esophageal function during fluoroscopy may show esophageal aperistalsis, spasm, or gastro- esophageal reflux. If no lesion is detected, a double contrast upper gas- trointestinal series should be performed with careful attention to the gastric cardia because tumors of the gastric fundus can present with dys- phagia (pseudoachalasia).
Endoscopic Evaluation
If there is evidence of a lesion on radiologic evaluation such as an ulcer or mass, the patient should undergo esophagogastroscopy with bi- opsy and brush cytology to evaluate further the esophageal and gastric mucosa. The radiographic and endoscopic studies are often complemen- tary to each other in the work-up of patients with dysphagia because each may identify abnormalities that the other may not detect. One situation in which endoscopy is preferable to barium studies is the acute onset of severe dysphagia while eating. Because these patients may develop total esophageal obstruction, endoscopic intervention is frequently necessary to remove an impacted food bolus. A previously undiagnosed esophageal abnormality often is found to be the cause of the obstruction. Other po- tential advantages of endoscopy over radiology include diagnosing infec- tious esophagitis, detecting erosions of the esophagus, stomach, and du- odenum, and obtaining tissue samples from erosions, ulcers, or other esophageal lesions.
Esophageal Manometry and pH Monitoring
Esophageal manometry should be performed if no anatomic abnor- mality is found on barium swallow or upper endoscopy. The primary goals of manometry are to assess the characteristics of esophageal con- tractions (peristaltic, simultaneous, or absent) and to define the LES and UES and their respective responses to swallowing. Although esophageal manometry is the gold standard for diagnosing esophageal motor disor- ders, several studies using manometry in the evaluation of nonobstructive dysphagia have suggested that definitive abnormalities (e.g., findings considered diagnostic for achalasia or diffuse esophageal spasm) occur
DYSPHAGIA 425
in only about 25% of patients with dysphagia. The manometry in another 25% of patients reveals abnormalities of unclear significance (e.g., non- specific esophageal motility disorder, hypertensive LES, and nutcracker esophagus) and is normal in the remaining half of patients. Provocative testing during esophageal manometry usually is reserved for patients with noncardiac chest pain but can be useful in evaluating patients with dysphagia, especially if other esophageal symptoms (such as heartburn or chest pain) are present. Provocative testing includes intravenous infu- sion of edrophonium, esophageal balloon distention, or acid perfusion into the esophagus. Some centers advocate using a solid bolus, such as bread for the patient to swallow during manometry, to help unmask an underlying motility disorder.
Ambulatory esophageal pH monitoring may aid in the study of pa- tients with dysphagia, because the recording can be reviewed during the time the patient was symptomatic to determine if acid reflux episodes were present simultaneously with the patient’s symptoms. Combined re- cording of esophageal pH and intraluminal pressure may be useful to diagnose reflux-induced esophageal spasm.
CONDITIONS CAUSING DYSPHAGIA
Dysphagia conventionally is divided into two categories based on the different anatomic or functional areas involved: abnormalities affecting the striated muscle (oropharyngeal dysphagia) and abnormalities affect- ing the smooth muscle (esophageal dysphagia). In contrast to oropharyn- geal causes in which dysphagia occurs along with a variety of other symp- toms, true esophageal dysphagia rarely is associated with symptoms outside the esophagus.
Oropharyngeal Dysphagia
Oropharyngeal dysphagia is characterized by difficulty in the initial stages of the swallowing process and is manifested by impaired transfer of food from the mouth through the UES into the upper esophagus. Typ- ical symptoms include difficult transference of food or liquids out of the mouth into the esophagus, the sensation of food sticking in the throat during swallowing, and the need to use repeated swallows to pass food into the esophagus successfully. Nasal or oral regurgitation of swallowed material and coughing or choking during swallowing caused by aspira- tion into the trachea are also characteristic of oropharyngeal dysphagia. Additionally, dysarthria and a nasal quality to the voice (dysphonia) may occur.
The causes of oropharyngeal dysphagia include:
Neuromuscular disorders CNS diseases
Cerebrovascular accident
426 TRATEetal
Parkinson’s disease Brain stem tumors Degenerative diseases (amyotrophic lateral sclerosis, multiple
Postinfections (poliomyelitis, syphilis) Peripheral nervous system
Peripheral neuropathy Motor end plate dysfunction
Myasthenia gravis Skeletal muscle disease (myopathies)
Pol ymyositis Dermatomyositis Muscular dystrophy (myotonic dystrophy, oculopharyngeal
dystrophy)
sclerosis, Huntington’s disease)
Cricopharyngeal (UES) achalasia
Obstructive lesions
Tumors Inflammatory Trauma/surgical resection Zenker’s diverticulum Esophageal web
Extrinsic structural lesions Anterior mediastinal masses Cervical spondylosis
Intrinsic structural lesions
More than 75% of cases of oropharyngeal dysphagia are caused by neu- romuscular disorders involving the CNS. As a group, elderly patients are particularly susceptible to these conditions and most often present with oropharyngeal dysphagia. The differential diagnosis of neuromuscular causes of oropharyngeal dysphagia ranges from cerebrovascular acci- dents, midbrain tumors, and cranial nerve disorders to neuromuscular impairments such as myasthenia gravis. Cerebrovascular accidents, the most common cause of oropharyngeal dysphagia, may affect the brain stem swallowing center or motor nuclei controlling the striated muscle of the hypopharynx and upper esophagus. Dysphagia in some patients may develop years after an attack of acute paralytic poliomyelitis from dys- function of the bulbar muscles. Certain connective tissue disorders such as polymyositis or dermatomyositis may affect the striated muscle portion of the esophagus, causing a decrease in UES tone and poor propulsion of the bolus from the pharynx into the esophagus. Lastly, incomplete UES relaxation (cricopharyngeal achalasia) may be a cause of difficulty in pro- pelling a food bolus through the UES into the esophagus. Treatment of oropharyngeal dysphagia is determined by the underlying cause. Medical treatment of systemic diseases such as myasthenia gravis, polymyositis, Parkinson’s disease, and thyroid dysfunction may improve the patient’s oropharyngeal dysphagia. Patients with dysphagia secondary to a stroke improve with time but may be left with a residual swallowing defect.
DYSPHAGIA 427
These patients often can be helped by speech therapists. These specialists train patients to regain effective swallowing by adjusting food consis- tency, volume, and delivery rate; optimize head posture during swallow- ing; coordinate breathing and coughing maneuvers to clear residual food from the pharynx; and exercise muscle groups involved in swallowing that are still functional.
Esophageal diverticula are among the intrinsic structural lesions that may cause oropharyngeal dysphagia. These diverticula are acquired ab- normalities often caused by underlying esophageal motility disorders. Dysphagia may result from the diverticulum itself or from an associated motor disorder of the esophagus. Zenker’s diverticulum, an outpouching of one or more layers of the distal pharyngeal wall just above the crico- pharyngeus muscle, probably occurs as a result of UES dysfunction. An example of a Zenker’s diverticulum is seen in Figure 3A. Treatment of Zenker’s diverticulum requires cricopharyngeal myotomy along with a pouch resection or oversewing of the pouch. The main contraindication to cricopharyngeal myotomy is concomitant gastroesophageal reflux dis- ease caused by the increased risk of pulmonary aspiration.
ESOPHAGEAL DYSPHAGIA
Esophageal dysphagia can result from neuromuscular disorders af- fecting the smooth muscle or from a structural obstruction of the esoph- agus. The causes of esophageal dysphagia include:
Neuromuscular disorders Achalasia Spastic motor disorders
Diffuse esophageal spasm Hypertensive LES Nutcracker esophagus
Scleroderma
Obstructive lesions
Tumors Strictures
Peptic Radiation-induced Chemical-induced Medication-induced
Intrinsic structural lesions
Lower esophageal ring (Schatzki’s ring) Esophageal web Foreign body
Extrinsic structural lesions Vascular compression
Enlarged aorta or left atrium Aberrant vessels

428 TRATEetal
Mediastinal masses Lymphadenopathy Substernal thyroid
The majority of cases of esophageal dysphagia are associated with struc- tural abnormalities, the most common of which are peptic strictures, Schatzki’s ring, and carcinoma. The most frequently defined esophageal motility disorders that lead to dysphagia are achalasia, diffuse esophageal spasm, and scleroderma.
Esophageal Rings, Webs, and Strictures
Patients who have only intermittent dysphagia for solids most fre- quently are found to have esophageal rings or webs. Whereas esophageal webs are located most often in the cervical region (Plummer-Vinson syn- drome), esophageal rings are narrowings found in the distal esophagus and gastroesophageal junction. The internal diameter of a mucosal ring is the most important factor in determining the occurrence of dysphagia. Rings more than 20 mm in caliber are rarely symptomatic, whereas rings less then 13 mm in diameter almost always cause dysphagia. Dysphagia is typically episodic and not progressive but may be severe when it occurs acutely because of temporary obstruction. Treatment consists of one-time dilation with a large-caliber bougie dilator.
Peptic esophagitis from gastroesophageal reflux disease can produce a marked inflammatory reaction leading to fibrosis and stricture forma- tion, often extending for several centimeters in the distal esophagus. Most peptic strictures are circumferential with a smooth or tapered appearance. Patients complain of episodic dysphagia that is slowly progressive and usually report a long antecedent history of heartburn or antacid use. In contrast, patients with esophageal carcinoma have a history of rapidly progressive dysphagia with anorexia and significant weight loss. Because malignant strictures cannot be reliably distinguished radiographically from benign ones, all patients with esophageal strictures should undergo endoscopy with biopsy and brush cytology to exclude carcinoma or Bar- rett’s esophagus. Treatment of peptic strictures includes periodic bou- gienage along with aggressive acid suppression using a proton pump inhibitor. Patients with documented Barrett’s esophagus also should un- dergo periodic surveillance endoscopy with random biopsies to assess the degree of dysplasia.
Carcinoma
Neoplasms of the esophagus tend to present with anorexia and rap- idly progressive dysphagia for solids, generally associated with weight loss. The two major esophageal neoplasms are squamous cell carcinoma and adenocarcinoma. Squamous cell carcinoma, the more prevalent of the two, is associated with the long-term use of alcohol or tobacco, especially
DYSPHAGIA 429
in African Americans, whereas adenocarcinoma tends to occur in white men with a long history of gastroesophageal reflux disease and is super- imposed on an underlying Barrett’s esophagus. It recently has been re- ported that adenocarcinoma may develop within an area of “short seg- ment Barrett’s,” and therefore a high index of suspicion is required when evaluating patients with a consistent clinical scenario. The diagnosis may be suggested strongly on barium swallow radiography by the classic find- ings of nodularity, rigidity, abrupt luminal angulation or “shelving,” ulceration, and stenosis of the lumen, which typically has asymmetric margins. The best method for confirming the diagnosis of carcinoma is endoscopy with biopsy and cytology. Endoscopic ultrasonography may be employed to detect disease confined to the mucosa, early invasion of the lamina propria, depth of invasion, and local nodal status. This infor- mation as well as that obtained from abdominal/thoracic CT scan can be used to determine potential resectability.
Treatment of esophageal carcinoma for the most part is palliative, consisting of surgery, chemotherapy, and radiation therapy; however, surgery occasionally can be curative in patients with early esophageal cancer. In patients with dysphagia who are not surgical candidates, pal- liative treatment options for dysphagia include esophageal dilatation, esophageal prosthesis, and tumor ablation using electrocoagulation or la- ser therapy.
Achalasia
The best understood primary esophageal motility disorder is acha- lasia. Dysphagia for solid and liquid food typically is present from the beginning and slowly worsens with time. Although the onset of primary achalasia is usually insidious with an average symptom duration of 5 years at the time of initial treatment, 16% of patients with primary acha- lasia present within the first year of symptom development. The site of obstruction usually is recognized correctly by the patient as occurring at the xiphoid area. Patients often develop maneuvers that enable them to finish meals, such as repeated swallowing, eating only small quantities of food, or drinking large volumes of water in an attempt to facilitate emp- tying of the esophagus. The characteristic appearance of a barium esoph- agram in a patient with achalasia is a dilated, fluid-filled esophagus and a smooth tapered distal portion (bird beak). Manometry often is used to confirm esophageal aperistalsis, elevated LES pressure, and incomplete relaxation of the LES on swallowing. Traditionally, early achalasia has been treated with calcium channel blockers, anticholinergic agents, ni- trates, or intermittent bougie dilation. Medical therapy unfortunately is at best adjunctive. Achalasia more typically has been treated with pneumatic dilation or surgical myotomy (Heller myotomy). The overall success rate of pneumatic dilation is about 80%; however, esophageal perforation com- plicates pneumatic dilation in 4% to 5% of cases. The second, less trou- blesome complication of pneumatic dilation is gastroesophageal reflux disease. Two new treatment options for achalasia include botulinum toxin
430 TRATEetal
injection into the LES and laparoscopic myotomy. The advantage of per- forming the myotomy laparoscopically is that the length of hospital stay and time to return to work may be greatly reduced. Botulinum toxin in- jection into the LES is an easy and relatively safe procedure that has been shown to produce almost immediate relief of the patient’s symptoms. Un- fortunately, recent studies indicate that the effect tends to diminish during a 6-month to 12-month period, requiring repeat treatment.
Secondary achalasia, or pseudoachalasia, refers to the development of achalasia as a result of an underlying disorder, usually gastric or esoph- ageal carcinoma. Malignancies distant from the esophagogastric junction such as lung cancer, pancreatic cancer, lymphoma, hepatoma, and pros- tate carcinoma also have been associated with secondary achalasia in the United States. Distinguishing malignancy-induced achalasia from pri- mary achalasia on clinical grounds can be difficult. Three clinical features that suggest the possibility of malignancy as a cause of achalasia include (1) age older than 55 years, (2) short duration of dysphagia (< 1 year), and (3) significant weight loss (> 15 lb). These criteria are only guidelines because exceptions to each have been reported. Indeed, 15% of patients with primary achalasia present older than the age of 60, and some cases of malignancy-induced achalasia have occurred in patients as young as 15 years of age. Therefore, all patients with achalasia should undergo upper endoscopy to exclude malignancy. In South America the most com- mon cause of secondary achalasia is Chagas’ disease caused by infection with Typanosoma cruzi.
Scleroderma (Progressive Systemic Sclerosis)
Dysphagia to liquids and solids characteristically is present in pa- tients with esophageal involvement by scleroderma. Patients typically are middle-aged women who complain of chronic heartburn associated with progressive dysphagia. The classic manometric findings of diminished or ineffective peristalsis in the distal 2/3 to 3/4 of the esophagus, accom- panied by a hypotensive LES, account for severe gastroesophageal reflux disease and stricture formation observed in patients with scleroderma. Treatment of these severe peptic strictures consists of periodic bougienage and long-term aggressive acid suppression with a proton pump inhibitor. There has been a hesitance to send patients with scleroderma for antireflux surgery because of the risk of worsening their dysphagia; however, this risk may be overstated.
Spastic Motor Disorders of the Esophagus
Dysphagia may be a prominent symptom in patients with spastic motor disorders of the esophagus such as diffuse esophageal spasm. Al- though the mechanism of dysphagia is unknown, it may result from in- effective peristalsis (caused by simultaneous contractions) or impaired re- laxation of the LES. Diagnosis of diffuse esophageal spasm rests on the presence of simultaneous, high amplitude esophageal contractions (in at least 10% to 30% of wet swallows) interspersed with normal peristaltic
DYSPHAGIA 431
contractions, occurring in symptomatic patients with chest pain or dys- phagia. Diffuse esophageal spasm and achalasia often are considered dif- ferent manifestations of a similar underlying disorder. In some patients, diffuse esophageal spasm has been reported to progress to achalasia. Pa- tients with spastic motility disorders can be tried on smooth muscle re- laxants such as calcium channel blockers, nitrates, or anticholinergics; however, responses to medical therapy are inconsistent. Some patients may respond to periodic bougie dilation or even botulinum toxin injection into the LES.
Gastroesophageal Reflux Disease
Dysphagia occurs in up to 40% of patients with gastroesophageal reflux disease and may arise from a host of obstructive causes, including peptic strictures caused by long-standing reflux esophagitis, esophageal carcinoma arising within a Barrett’s esophagus, or esophageal peristaltic dysfunction. Ambulatory 24-hour esophageal pH monitoring may show an association of reflux episodes with dysphagia and when performed in conjugation with motility monitoring, may help determine a more specific mechanism for the dysphagia. Aggressive acid suppression with a proton pump inhibitor or antireflux surgery (Nissen fundoplication) would be the treatments of choice in patients with severe dysphagia.
CONCLUSIONS AND FUTURE PROSPECTS
The description of difficulty swallowing by a patient should direct the physician to an orderly series of diagnostic tests of esophageal func- tion to help determine the cause of the dysphagia (see Figs. 1 and 2). Initial testing should begin with a dynamic videofluoroscopic barium exami- nation of the swallowing process (oropharyngeal and esophageal), using liquid and then solid bolus challenges if no anatomic abnormalities are seen. Although esophagogastroscopy is performed most often in patients with esophageal dysphagia who have abnormal radiographic studies, en- doscopy sometimes can provide additional information in patients in whom barium examinations have been unrevealing. If no underlying cause of dysphagia is identified by these tests, esophageal manometry should be employed to determine whether an esophageal motility disor- der is present. More sophisticated evaluation of esophageal motor func- tion with prolonged ambulatory esophageal pH recording and occasion- ally pH and motility recording may provide additional information in complex patients. The clinical utility of these tests awaits further defini- tion, however.
References
1. Bott S, Prakash C, McCallum RW: Medication-induced esophageal injury: Survey of the
2. Castell D O Approach to the patient with dysphagia. In Yamada T (ed): Textbook of literature. Am J Gastroenterology 82:758,1987
Gastroenterology. Philadelphia, JB Lippincott, 1995, pp 638448
432 TRATEetal
3. Castell DO, Donner MW: Evaluation of dysphagia: A careful history is crucial. Dyspha-
4. Castell DO, h u f f TE, Brown FC, et al: Dysphagia. Gastroenterology 76:1015, 1979 5. Decktor DL, Allen ML, Robinson M: Esophageal motility, heartburn, and gastroesopha-
geal reflux: Variations in clinical presentation of esophageal dysphagia. Dysphagia 5:211, 1990
6. Edwards DAW: Discriminary value of symptoms in the differential diagnosis of dys- phagia. Clinics in Gastroenterology 5:49, 1976
7. Groher ME (ed): Dysphagia-Diagnosis and Management, ed 2. Boston, Butterworth-
gia 2:65-71, 1987
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21. 22.
23.
24.
25.
26.
_ _ - - - Heinemann, 1992 Hendrix TR Art and science of history taking in the patient with difficulty swallowing. Dysphagia 8:69-73,1993 Hogan WJ: Swallowing problems: Dysphagia and odynophagia. In Berk JE, Haubrich WS (eds): Gastrointestinal Symptoms-Clinical Interpretation. Philadelphia, BC Decker, 1991, pp 71-90 Jones 8, Donner MW: Examination of the patient with dysphagia. Radiology 167319, 1988 Jones B, Ravich WJ, Donner MW, et al: Pharyngoesophageal interrelationships: Obser- vations and working concepts. Gastrointestinal Radiology 10:225, 1985 Kahrilas PJ, Kishk SM, Helm JF, et al: Comparison of pseudoachalasia and achalasia. Am J Med 82:439,1987 Katz PO, Dalton CB, Richter JE, et al: Esophageal testing in patients with noncardiac chest pain or dvsphagia. Ann Intern Med 106:593,1987 Levin; MS, Ribkin- SE: Radiologic investigation of dysphagia. Am J Roentgen01 1541157.1990 Maxfield DL: Non-GERG disorders. Confronting the range of non-GERD esophageal disorders. J Am Osteopath Assoc 95:S11,1995 McCord GS, Clouse RE: Pill-induced esophageal stricture: Clinical features and risk fac- tors for development. Am J Medicine 88:512, 1990 Moser G, Vacariu-Granser GV, Schneider C, et a1 High incidence of esophageal motor disorders in consecutive patients with globus sensation. Gastroenterology 101:1512,1991 Nelson JB, Richter JE: Upper esophageal motility disorders. Gastroenterology Clinics of North America 18:195, 1989 Ott DJ: Radiographic techniques and efficacy in evaluating esophageal dysphagia. Dys- phagia 5:192, 1990 Ott DJ, Gelfand DW, Wu WC, Castell DO: Esophagogastric region and its rings. Am J Roent 142281,1984 Reynolds JC, Parkman HI? Achalasia. Gastroenterol Clin North Am 18:223, 1989 Richter JE: Diagnosis and management of common swallowing disorders. Mediguide to GI Diseases 6:l-7,1995 Rozman RW Jr, Achkar E: Features distinguishing secondary achalasia from primary achalasia. Am J Gastroenterology 85:1327, 1990 Singh S, Stein HJ, DeMeester TR, et al: Nonobstructive dysphagia in gastroesophageal reflux disease: A study with combined pH and motility monitoring. Am J Gastroenterol 87562,1992 Vantrappen G, Janssens J: Recent studies of the pathophysiology and diagnosis of esoph- ageal symptoms. Scand J Gastroenterol25 (suppl175):34,1990 Vantrappen G, Janssens J, Hellemans J, et al: Achalasia, DES, and related motility dis- orders. Gastroenterology 76:450, 1979
Address reprint requests to Robert S. Fisher, MD
Department of Medicine Temple University Hospital
Parkinson Pavilion, 8th Floor 3401 North Broad Street Philadelphia, PA 19140