Embed Size (px)
Citation preview
ECG
& E
P C
ASES
54 Journal of Cardiac Arrhythmia
발작성심실상성빈맥의진단에도움이되는심전도소견
연세대학교 의과대학 내과학교실 정 보Bo-Young Joung, MD, PhDDivision of Cardiology, Yonsei University College of Medicine, Seoul, Korea
ECG findings to diagnose supraventricular tachycardia
ABSTRACTOften, the P waves of AV nodal reentry are seen just prior to or just after the end of the QRS and cause asubtle alteration in the QRS complex that results in a pseudo-S or pseudo-r’. The AV nodal reentry beginsabruptly, usually following a premature atrial complex that conducts with a prolonged PR interval. Theretrograde P wave of AV reciprocating tachycardia occurs after completion of the QRS complex, in the STsegment, or early in the T wave. The presence of an ipsilateral bundle branch block can facilitate reentry andcause the prolonging of the tachycardia cycle length. Finally, vagal maneuvers or an adenosine injection couldhelp in case of differential diagnosis of regular narrow QRS tachycardias.
Key words: ■ AV nodal reentry ■ AV reciprocating tachycardia ■ ECG
서론
발작성 심실상성 빈맥(paroxysmal supraventricular
tachycardia, PSVT)은전극도자절제술의시술성공률과
안전성이높아서일차치료로권유되고있다. 비교적시술이
용이하여서자세한심전도관찰의중요성이점점경시되고
있다. 하지만심전도를통하여전기생리학검사전에심실상
성빈맥(Supraventricular tachycardia, SVT)의기전에
대한예측이가능하며, 시술난이도를미리결정할수있는
장점이있다. 이 에서는몇가지증례를통하여심전도를
통하여SVT의진단및기전을파악하는데도움이되는소견
에대하여기술하고자한다.
증례1
방실결절회귀성빈맥(atrioventricular nodal reentrant
tachycardia, AVNRT)은심실상성기원의좁은QRS 파형
을가지고, 시작및종료가갑작스러운특성을가지고있으며,
맥박수는성인의경우일반적으로분당 180~200회정도이
다. 편위전도(aberrant conduction) 혹은전도장애가있지
않으면, QRS의모양및기간은정상이다. P파는주로QRS
파형내혹은바로뒤에따라오게되며, QRS에미세한변화
를주어서, 가성(pseudo) s파혹은가성r’파를보이게된다.
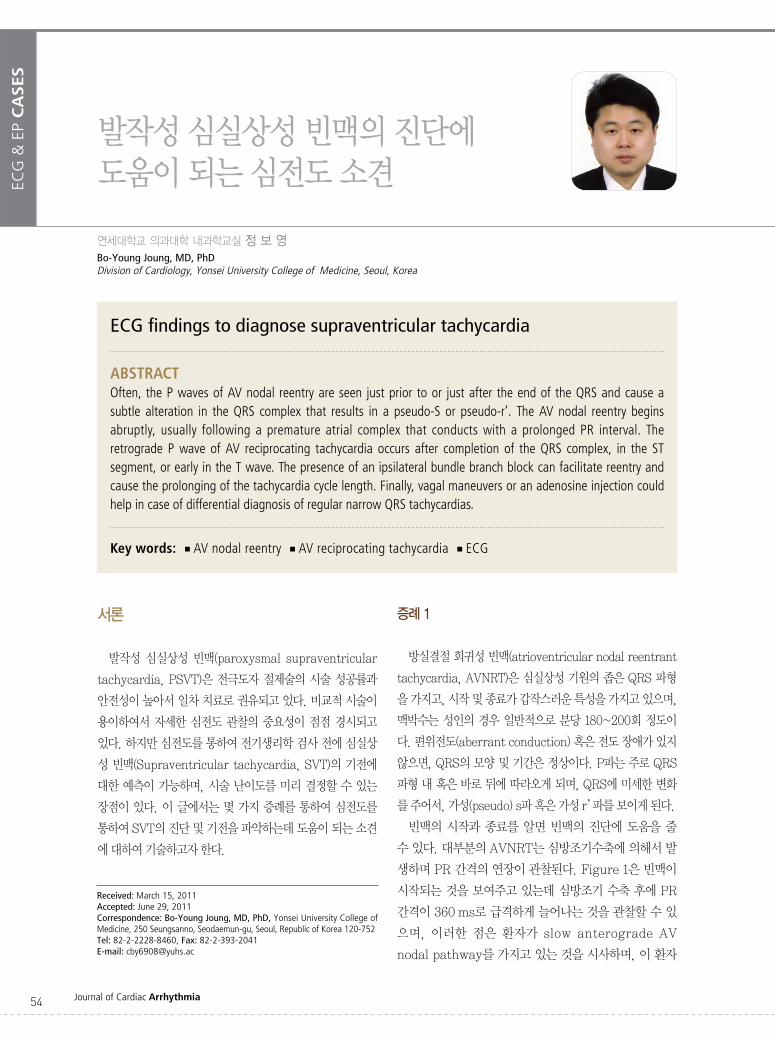
빈맥의 시작과 종료를 알면 빈맥의 진단에 도움을 줄
수있다. 대부분의AVNRT는심방조기수축에의해서발
생하며PR 간격의연장이관찰된다. Figure 1은빈맥이
시작되는것을보여주고있는데심방조기수축후에PR
간격이360ms로급격하게늘어나는것을관찰할수있
으며, 이러한 점은 환자가 slow anterograde AV
nodal pathway를가지고있는것을시사하며, 이환자
Received: March 15, 2011Accepted: June 29, 2011Correspondence: Bo-Young Joung, MD, PhD, Yonsei University College ofMedicine, 250 Seungsanno, Seodaemun-gu, Seoul, Republic of Korea 120-752Tel: 82-2-2228-8460, Fax: 82-2-393-2041E-mail: [email protected]
55
ECG
& E
P C
ASES
VOL.12 NO.2
의빈맥이AVNRT임을시사한다.
증례2
우회로를 이용한 방실 재귀성 빈맥(AV reciprocating
tachycardia)의경우전향적전도는방실결절His bundle
전도로(AV node-His bundle pathway)를 이용하며, 역
방향전도는우회로를이용한다. 이경우역방향P파의위치
는주로QRS가끝난후, ST분절혹은T파앞에위치하게되
어감별에도움이된다.
넓은QRS 빈맥을보이면심실빈맥및SVT의편위전도를
고려해야한다. 동일한환자가좁은QRS 빈맥과넓은QRS
빈맥을모두보인다면심실빈맥보다는SVT가편위전도되는
경우가더욱흔하다. Figure 2의환자는내원당시좌각차단
(left bundle branch block, LBBB)을동반한넓은QRS
빈맥을보 다(Figure 2A). 환자의혈압이 75/50 mmHg
정도로 낮아서 심율동전환(cardioversion)을 하 는데 넓
은QRS 빈맥이좁은QRS 빈맥으로변경되었다. LBBB를
동반한넓은QRS 빈맥과좁은QRS 빈맥의주기를살펴보
면각각320 ms, 280 ms로약40 ms 정도LBBB 빈맥의
주기가길었다. 이와같이각차단을보이면서빈맥주기가늘
어나면 동측에 우회로가 있음을 시사하며, 이러한 법칙을
Coumel’s law라고한다.
증례3
규칙적인좁은QRS 빈맥은심방빈맥의경우에도관찰된
다. Figure 3은 30세여성환자가두근거림을주소로응급
실에 내원하 을 때 심전도 소견인데 좁은 QRS 빈맥
(Figure 3A)과 우각차단(right bundle branch block,
RBBB) 유형의넓은QRS 빈맥(Figure 3B)이관찰되고있
다. Vagal maneuver나adenosine의투여후변화되는심
전도는부정맥의기전을파악하는데많은도움을줄수있
다. Adenosine 투여후심전도를보면빈맥은종료되지않
Figure 1. Paroxysmal AV nodal reentrant tachycardia initiated by an atrial premature beat (A). After 4 sinus beats, anatrial premature beat (❶) is conducted with a longer PR and initiates reentry in the AV junction; retrograde P waves (❷)are seen right at the end of the subsequent QRS complexes (slow-fast tachycardia) (B). After the 5th beat, the retrogradeP wave disappears (❸) (B).
❶
❷
❸
A
B
III
V5
III
V5
ECG
& E
P C
ASES
56 Journal of Cardiac Arrhythmia
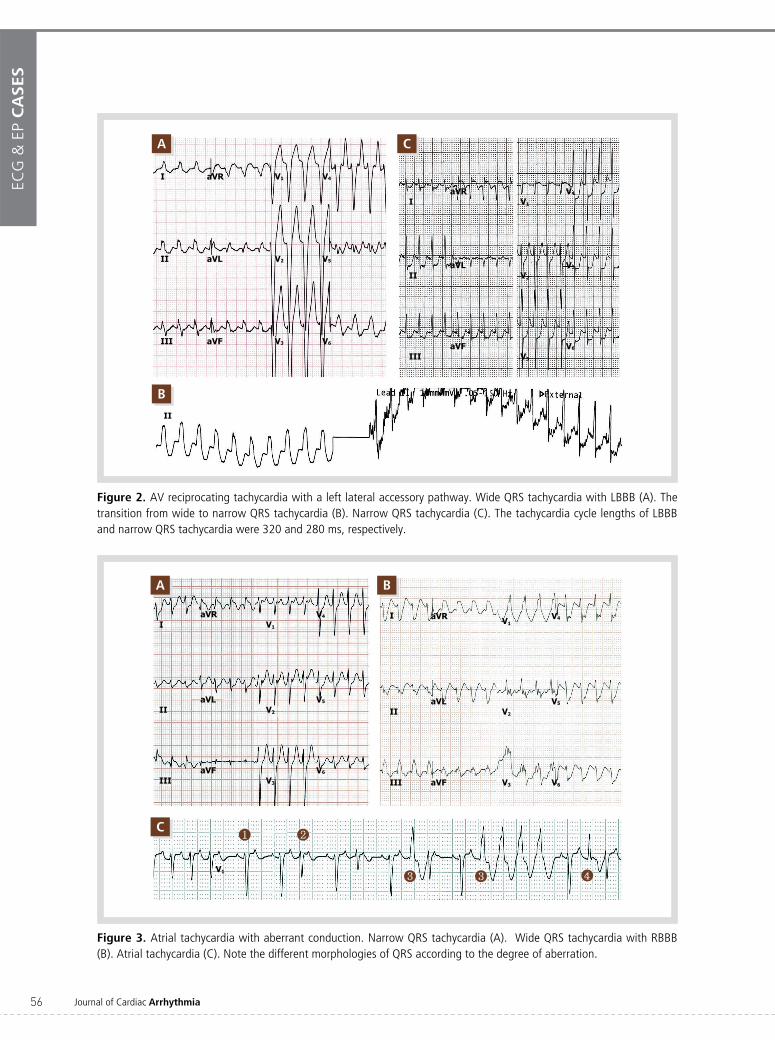
Figure 3. Atrial tachycardia with aberrant conduction. Narrow QRS tachycardia (A). Wide QRS tachycardia with RBBB(B). Atrial tachycardia (C). Note the different morphologies of QRS according to the degree of aberration.
A
C
B
❶ ❷
❸ ❸ ❹
IaVR
V1
V4
IIaVL
V2
V5
IIIaVF
V3
V6
I aVR V1V4
IIaVL
V2
V5
III aVF V3 V6
V1
Figure 2. AV reciprocating tachycardia with a left lateral accessory pathway. Wide QRS tachycardia with LBBB (A). Thetransition from wide to narrow QRS tachycardia (B). Narrow QRS tachycardia (C). The tachycardia cycle lengths of LBBBand narrow QRS tachycardia were 320 and 280 ms, respectively.
A
B
C
I aVR V1 V4
II aVL V2 V5
III aVF V3 V6
II
IaVR
V1
V4
IIaVL
V2
V5
IIIaVF
V3
V6

57
ECG
& E
P C
ASES
VOL.12 NO.2
고, 방실결절전도의정도에따라서다양한편위전도를보
다(Figure 3C). ❷로표시된박동은정상적vector의QRS
를보여주고있으나, ❸과❹로표시된박동은RBBB 유형
이며편위(aberration)의정도에차이가있음을알수있다.
흥미로운점은❸과❹로표시된박동의차이가이전의RR
간격이길면이상이잘나타나는Ashman 현상을보여주고
있다는점이다.
고찰
심전도에서 PSVT의 진단에도움이되는소견을종합해
보면다음과같다. ①빈맥의심전도V1 유도에가성s파혹
은가성r’파소견이관찰되면방실결절성회귀빈맥을시사
하는소견이며, ②빈맥의시작시PR 간격의연장소견이
관찰되는경우전향적완속방실결절로가있음을예측할수
있다. ③넓은QRS 및좁은QRS를가진빈맥이동시에관
찰되면빈맥의주기에대한자세한관찰이필요하며, 각차단
시빈맥의주기가연장되면동측에우회로가있음을시사한
다. ④Vagal maneuver나adenosine 등의약제는빈맥의
종료뿐아니라, 감별진단에도도움이된다.
References
1. Olgin JE, Zipes D. Specific arrhythmias: Diagnosis and treatment.In Libby P, Bonow R, Mann D, Zipes D, eds: Braunwald’s HeartDisease. eighth edition. Philadelphia: Saunders Elsevier, 2010, pp873-893.

![Journal of Arrhythmia - COnnecting REpositories · of arrhythmia diagnosis [1], and implantable loop recorders are especially suitable for identifying undetected sources of a suspected](https://img.pdfslide.tips/doc/110x75/607210056cc22557db7f5efd/journal-of-arrhythmia-connecting-repositories-of-arrhythmia-diagnosis-1-and.jpg)