Embed Size (px)
Citation preview

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 1/43
ECG Interpretation for
Primary Care PhysicianAamir A. Cheema M.D.

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 2/43
Welcome
Pakistan
Society of FamilyPhysicians

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 3/43
ECG Grid

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 4/43
6 Steps
1. Rate
2. Rhythm
3. Axis
4. Intervals
5. Hypertrophy
6. Infarction/Ischemia

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 5/43
Rate
300-150-100-75-60-50
300-150-100-75-60-50

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 6/43
What if rate is <50/min or rhythm is
irregular ?
Count the number of R waves in a 6 second stripand multiply by 10.
For example, if there are 7 R waves in a 6 secondstrip, the heart rate is 70 (7x10=70).

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 7/43
Rhythm
1. Locate the P wave
If absent and rhythm is irregular, think of atrial
fibrillation.
If present- check rate: If <60, bradycardia. If >100,
tachycardia. In general, if narrow-complex tachycardia is present and
heart rate is
100-150, think of sinus tachycardia
150-250, think of SVT (supraventricular tachycardia)
250-350, think of atrial flutter
>350, think of atrial fibrillation

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 8/43
Rhythm
2. Establish the relationship between Pwave and QRS complex
If 1:1, it is normal
If more P waves than QRScomplexes, think of AV block
If more QRS complexes than Pwaves, think of accelerated junctional or ventricular rhythm

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 9/43
Rhythm
3. Analyze the QRS morphology
If normal duration (<120 msec),
think of supraventricular origin e.g.normal sinus rhythm or
supraventricular tachycardia
If wide (>120 msec), think of ventricular origin e.g. ventricular
tachycardia

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 10/43
Axis

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 11/43
Intervals
PR interval: <200 msec(one big box)
QRS complex:<100 msec(2½ small boxes)
ST segment: evaluatefor elevation or depression
below baselineQT segment: roughly lessthan half of R-R interval
At high or low heart rates, calculate corrected QT intervalQTc = QT interval ÷ square root of the RR interval (in sec)
The normal value for the QTc is <440 msec (2½ big boxes)

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 12/43
Hypertrophy
Left ventricular hypertrophy criteria
Sum of S wave in V1 and R wave inV5 or V6 3.5 mV (35 mm)
and/or
R wave in aVL 1.1 mV (11 mm)

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 13/43
Normal ECG

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 14/43
Infarction
Clinically significant ST segmentelevation is considered to be presentif it is greater than 1 mm (0.1 mV) in
at least two contiguous precordialleads or in at least two adjacent limbleads.

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 15/43
Diagnosis?

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 16/43
One or more of the precordial leads (V1-V6) and leads I
and aVL suggest anterior wall ischemia or infarction
Leads V4 to V6 suggest apical or lateral ischemia or
infarction

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 17/43
Diagnosis?

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 18/43
Leads V1 to V3 suggest
anteroseptal ischemia or infarction.

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 19/43

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 20/43

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 21/43
Diagnosis?

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 22/43
Leads II, III, and aVF suggest inferior
wall ischemia or infarction

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 23/43

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 24/43
Diagnosis?

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 25/43
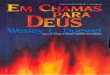
Acute infero-postero-lateral myocardialinfarction
1. ST depression in V2 and V3 (posteriorwall MI)
2. ST elevation in II, III and aVF (inferiorwall MI)
3. T wave inversion in V4-6 (lateral wall MI)

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 26/43
Posterior wall MI
The ST elevations of acute posterior MIare usually associated with reciprocal STdepressions in leads V1 to V3.
Posterior inferior wall MI can bedifferentiated from anterior wall ischemiaby the presence of ST segment elevationsin the inferior (II, III, aVF). Relatively tallR waves may also appear in leads V1-V3,corresponding to the appearance of pathologic Q waves (loss of depolarizationforces) in the posterior leads.

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 27/43

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 28/43
Diagnosis?

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 29/43
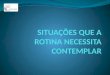
Ischemia
ST depression is defined by an STsegment which is depressed >1 mmbelow the baseline
Typically there are ST segmentchanges associated with T waveflattening or inversion; isolated T
wave changes are not usually seenwith ischemia.

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 30/43
Diagnosis?

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 31/43
New LBBB: Treat as ST Elevation
MI i.e. rush to cath lab for PCI
LBBB Diagnosis:Slurring of S wave in V5 and V6 and
QRS duration > 100 msec (i.e more than 2½ small squares)

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 32/43
Abnormal Q wave
According to the new criteria, anabnormal Q wave is any Q wave inleads V1 to V3 or a Q wave 30 msec
in leads I, II, aVL, aVF, or V4 to V6;the Q wave must be present in anytwo contiguous leads and 1 mm in
depth.(European Society of Cardiology (ESC) and
American College of Cardiology (ACC) 2000)

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 33/43
Diagnosis?

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 34/43
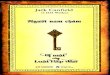
Ventricular Tachycardia
Tachycardia
Wide complex
Regular

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 35/43

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 36/43
Atrial Fibrillation:•Absent P waves
•Irregulary irregular rhythm

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 37/43

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 38/43

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 39/43

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 40/43
Sinus rhythm with complete (third-degree) heart block. There is independentatrial (as shown by the P waves) andventricular activity, with respective ratesof 83 and 43 beats/min.

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 41/43

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 42/43
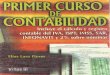
Mobitz type I (Wenckebach) seconddegree AV block
A progressively increasing PRinterval until a P wave is notconducted (arrow)

7/28/2019 ecginterpretation-100530002445-phpapp01
http://slidepdf.com/reader/full/ecginterpretation-100530002445-phpapp01 43/43
?