-
8/3/2019 Edema Cerebral Infarto Pulm
1/24
CEREBRAL EDEMA
Edema of the brain is dangerous because the
rigidity of the cranium allows little room for
expansion. Increased intracranial pressure
from edema compromises cerebral blood
supply, distorts the gross structure of the brain
and interferes with central nervous system
function. Cerebral edema is divided intovasogenic, cytotoxic,
and interstitial forms.
-
8/3/2019 Edema Cerebral Infarto Pulm
2/24
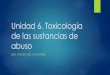
VASOGENIC EDEMA
The most common variety of edema, is excessfluid in the
extracellular space of the brain. Itresults from increased vascular
permeability,
mainly in white matter. The tight endothelialjunctions of the
blood brain barrier are disruptedand fluid filters into the
interstitial space.Disorders associated with cerebral vasogenic
edema include trauma, neoplasms, encephalitis,abscesses,
infarcts, hemorrhage, and toxic braininjury (e.g., lead
poisoning).
-
8/3/2019 Edema Cerebral Infarto Pulm
3/24
-
8/3/2019 Edema Cerebral Infarto Pulm
4/24
-
8/3/2019 Edema Cerebral Infarto Pulm
5/24
CYTOTOXIC EDEMA
Is equivalent to hydropic cell swelling (i.e.,accumulation of
intracellular water). It is
usually a response to cell injury, such as that
produced by ischemia. Cytotoxic cerebral
edema preferentially affects the gray matter.
-
8/3/2019 Edema Cerebral Infarto Pulm
6/24
INTERSTICIAL EDEMA
Is a consequence of hydrocephalus, in whichfluid accumulates in
the cerebral ventricles
and periventricular white matter.
-
8/3/2019 Edema Cerebral Infarto Pulm
7/24
-
8/3/2019 Edema Cerebral Infarto Pulm
8/24
-
8/3/2019 Edema Cerebral Infarto Pulm
9/24
-
8/3/2019 Edema Cerebral Infarto Pulm
10/24
-
8/3/2019 Edema Cerebral Infarto Pulm
11/24
-
8/3/2019 Edema Cerebral Infarto Pulm
12/24
-
8/3/2019 Edema Cerebral Infarto Pulm
13/24
-
8/3/2019 Edema Cerebral Infarto Pulm
14/24
-
8/3/2019 Edema Cerebral Infarto Pulm
15/24
-
8/3/2019 Edema Cerebral Infarto Pulm
16/24
CEREBRAL EDEMA
At autopsy, an edematous brain is soft and
heavy. Gyri are flattened and sulci narrowed.Because of
alterations in brain function,
patients with cerebral edema suffer vomiting,
disorientation, and convulsions. Severe
cerebral edema leads to herniation of the
cerebral tonsils, ordinarily a lethal event.
-
8/3/2019 Edema Cerebral Infarto Pulm
17/24
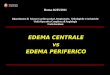
PULMONARY EMBOLISM
Pulmonary thromboemboli are reported in more than half of all
autopsies. Furthermore, thiscomplication occurs in 1% to 2% of
postoperative patients over the age of 40. The risk after
surgeryincreases with advancing age, obesity, length of operative
procedure, postoperative infection,cancer, and preexisting venous
disease.
Most pulmonary emboli (90%) arise from deep veins of the lower
extremities; most fatal ones form
in iliofemoral veins (Fig. 7-11). Only half of patients with
pulmonary thromboembolism have signsof deep vein thrombosis. Some
thromboemboli arise from the pelvic venous plexus and othersfrom
the right side of the heart.
The clinical features of pulmonary embolism are determined by
the size of the embolus, the healthof the patient, and whether
embolization occurs acutely or chronically. Acute pulmonary
embolismis divided into the following syndromes:
Asymptomatic small pulmonary emboli
Transient dyspnea and tachypneawithout other symptoms
Pulmonary infarction, with pleuritic chest pain, hemoptysis, and
pleural effusion Cardiovascular collapse with sudden death
Chronic pulmonary embolism, with numerous (usually asymptomatic)
emboli lodged in smallarteries of the lung, can lead to pulmonary
hypertension.
-
8/3/2019 Edema Cerebral Infarto Pulm
18/24
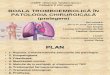
PULMONARY INFARTATION
Small pulmonary emboli are not ordinarily lethal. They tend
tolodge in peripheral pulmonary arteries. Sometimes (15% - 20%
ofall pulmonary emboli) they produce lung infarcts.
Clinically, pulmonary infarction is usually seen in the context
of CHFor chronic lung disease, because the normal dual circulation
of the
lung ordinarily protects against ischemic necrosis; since
thebronchial artery pumps blood into the necrotic area,
pulmonaryinfarcts are typically hemorrhagic. Patients experience
cough,stabbing pleuritic pain, shortness of breath, and
occasionalhemoptysis. Pleural effusion is common and often bloody.
Withtime, the blood in the infarct is resorbed, and the center of
the
infarct becomes pale. Granulation tissue forms on the edge of
theinfarct, after which it is organized to form a fibrous scar.
-
8/3/2019 Edema Cerebral Infarto Pulm
19/24
-
8/3/2019 Edema Cerebral Infarto Pulm
20/24
-
8/3/2019 Edema Cerebral Infarto Pulm
21/24
-
8/3/2019 Edema Cerebral Infarto Pulm
22/24
-
8/3/2019 Edema Cerebral Infarto Pulm
23/24
-
8/3/2019 Edema Cerebral Infarto Pulm
24/24