Embed Size (px)
Citation preview

Available online at www.sciencedirect.com
Journal of Nutritional Biochemistry 24 (2013) 1634–1644
Effects of excess dietary iron and fat on glucose and lipid metabolism☆
Joo Sun Choi, In-Uk Koh, Hyo Jung Lee, Won Ho Kim, Jihyun Song⁎
Division of Metabolic Diseases, Center for Biomedical Sciences, Korea National Institute of Health, Chungbuk –do 363–951, South Korea
Received 19 August 2012; received in revised form 9 January 2013; accepted 6 February 2013
Abstract
Purpose: Diets rich in fat and energy are associated with metabolic syndrome (MS). Increased body iron stores have been recognized as a feature of MS. High-fatdiets (HFs), excess iron loading and MS are closely associated, but the mechanism linking them has not been clearly defined. We investigated the interactionbetween dietary fat and dietary Fe in the context of glucose and lipid metabolism in the body.Methods: C57BL6/J mice were divided into four groups and fed the modified AIN-93G low-fat diet (LF) and HF with adequate or excess Fe for 7 weeks. The Fecontents were increased by adding carbonyl iron (2% of diet weight) (LF+Fe and HF+Fe).Results: High iron levels increased blood glucose levels but decreased high-density lipoprotein cholesterol levels. The HF group showed increases in plasma levelsof glucose and insulin and insulin resistance. HF+Fe mice showed greater changes. Representative indices of iron status, such hepatic and plasma Fe levels, werenot altered further by the HF. However, both the HF and excess iron loading changed the hepatic expression of hepcidin and ferroportin. The LF+Fe, HF andHF+Fe groups showed greater hepatic fat accumulation compared with the LF group. These changes were paralleled by alterations in the levels of enzymesrelated to hepatic gluconeogenesis and lipid synthesis, which could be due to increases in mitochondrial dysfunction and oxidative stress.Conclusions: High-fat diets and iron overload are associated with insulin resistance, modified hepatic lipid and iron metabolism and increased mitochondrialdysfunction and oxidative stress.© 2013 Elsevier Inc. All rights reserved.
Keywords: High-fat diet; Iron overload; Insulin resistance; Hepcidin; Hepatic steatosis
1. Introduction
Iron is an essential element for cell growth, erythropoieticfunction, oxidative metabolism and cellular immune responses.However, it is a strong prooxidant, and cells and organisms havedeveloped sophisticated mechanisms for maintaining iron levelswithin the physiologically optimal range [1].
Recently, increased body iron stores have been shown to becharacteristic of the metabolic syndrome and Type 2 diabetes [1,2].Adult humans with iron overload due to hereditary hemochromatosis(HH) have a high prevalence of diabetes and impaired glucosetolerance [2]. There are also close associations between hyperferri-tinemia and both metabolic syndrome and Type 2 diabetes in thegeneral non-HH population [3–6]. Increased ferritin levels and bodyiron stores have been shown to be associated with insulin resistance(IR) and metabolic syndrome in Korean, American and Chinese
☆ Grants: This work was supported in part by a Korea National Instituteof Health intramural research grant (4845-302-210-13). No conflicts ofinterest are declared by the authors.
⁎ Corresponding author. Division of Metabolic Disease, Center forBiomedical Science, Korea National Institutes of Health, 187 Osongsaeng-myeong 2-ro, Cheongwon-gun, Chungcheongbuk-do 363–951, South Korea.Tel.: +82 43 719 8690; fax: +82 43 719 8602.
E-mail address: [email protected] (J. Song).
0955-2863/$ - see front matter © 2013 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.jnutbio.2013.02.004
populations [3–6]. In addition, hepatic iron deposition has beendetected in up to one third of patients with nonalcoholic fatty liverdisease (NAFLD), characterized by a form of hepatic IR called insulinresistance-associated hepatic iron overload [7].
The mechanisms underlying the increased body iron stores duringthe development of IR, metabolic syndrome and diabetes are not clearyet. Chronically excessive iron absorption in HH patients could lead toiron overload. Iron overload can cause free radical formation andsubsequent β-cell dysfunction, resulting in decreased insulin secre-tory capacity [8,9]. High body iron stores along with IR and metabolicsyndrome occur in the general non-HH population [10,11]. Increasedbody iron levels under conditions such as excess iron, excess fatconsumption, obesity and the metabolic syndrome seem to cause IRand diabetes in a manner different than HH alone, but the mechanismhas yet to be clearly defined. The association of iron deposition and IRmay be bidirectional because compensatory hyperinsulinemia in IRmay also facilitate iron accumulation within the body. Insulinstimulates ferritin synthesis and facilitates iron uptake [12]. Con-versely, iron reduces hepatic extraction and metabolism of insulin,leading to peripheral hyperinsulinemia, and may increase oxidativestress, which inhibits the internalization and action of insulin [13].The generation of reactive oxygen species (ROS) by metal oxidantssuch as iron may also be involved in the cell damage that occurs inliver disease [14]. Hepatic injury triggered by an excessively lipid-richdiet may increase the serum levels of metabolites, which are

1635J.S. Choi et al. / Journal of Nutritional Biochemistry 24 (2013) 1634–1644
considered risk factors for metabolic diseases [15]. As a high lipidintake also causes oxidative stress and hepatic steatosis, thecombination of iron and a high-fat diet may aggravate these aberrantsituations synergistically.
Theironregulatoryhormonehepcidinisacirculatorypeptidethatactsas the key regulator of iron stores by inhibiting the absorption of ironthrough the duodenum and the release of iron from macrophages,therebybringingabouttheinternalizationanddegradationofferroportin.The altered iron trafficking underlies the accumulation of iron as ferritinandhemosiderin [16].Hepcidinsynthesis is inducedby ironoverloadandinflammatory signals such as interleukin (IL)-6 and lipopolysaccharide(LPS), as well as by leptin [17,18]. While hepcidin is known to play akey role in iron metabolism, evidence regarding the expression ofhepcidin and its role in IR is relatively sparse and indirect [19,20].
The relationships between iron, lipid and glucose metabolism arecomplex, and the progression of diabetes must be clarified to identifythe specific factors leading to IR and diabetes.
The objective of the present study was to investigate the effects ofhigh-fat diet-induced obesity and iron overload on iron metabolismand the mechanisms leading to hepatic steatosis, IR, inflammationand oxidative stress in an animal model.
2. Materials and methods
2.1. Animals and experimental diets
All animal protocols were approved by the Animal Care and Use Committee of theKorea National Institute of Health. Male C57BL/6J mice (aged 7 weeks) were obtainedfrom the Animal Center of SLC, Inc. (Hamamatsu, Shizuoka, Japan) and housed inindividual cages at 22°±2°C with a 12-h light–dark cycle. Animals were acclimatized tothis environment for 1 week with ad libitum access to water and control chow diet(Purina #5001 Chow; Dyets Inc., Bethlehem, PA, USA). After acclimatization, mice wererandomly divided into four groups after their body weights had been checked. Micefrom each group received a low-fat diet (10% of energy from fat) or a high-fat diet (45%of energy from fat) with or without 2% carbonyl iron (#C3518; Sigma, Stockholm,Sweden) for 7 weeks as follows: low-fat and high-iron diet (LF+Fe group, n=16) orhigh-fat and high-iron diet (HF+Fe group, n=16). Equivalent groups of mice were fedthe low-fat diet (LF group, n=15) or the high-fat diet (HF group, n=16) without ironsupplementation (0.02% iron). Experimental diets were formulated, and dietaryingredients were supplied by Dyets, Inc. The experimental diet was modified bychanging the fat and carbohydrate contents, based on the AIN-93G diet (ICN, Irvine, CA,USA). The low-fat diet provided 3.85 kcal/g (dry weight) and contained thefollowing metabolic energy contents (kcal%): 20% from protein, 10% from fat and70% from carbohydrates. The high-fat diet provided 4.75 kcal/g (dry weight) and hadthe following metabolic energy contents (kcal%): 20% from protein, 45% from fat and35% from carbohydrates. The vitamin and mineral contents of the diets wereidentical and in accordance with the requirements for standard rodent diets (exceptiron content). Water was freely available throughout the experiment, and bodyweight was recorded every week. Food intake was measured every 2–3 days for theduration of the experiment.
2.2. Blood and tissue collection
At the end of Week 7, mice were fasted overnight and anesthetized using CO2.Blood was collected into heparinized tubes by heart puncture. Plasmawas separated bycentrifugation at 3000 rpm and 4°C for 20 min and stored at −80°C until furtheranalysis. The liver, pancreas and spleen were removed, weighed and immediatelystored in either liquid nitrogen or 4% paraformaldehyde solution for biochemical andhistological analysis.
2.3. Plasma analysis
The plasma concentrations of glucose (AM-201K), triglycerides (TGs; AM-157SK),cholesterol (Chol; AM-202K), high-density lipoprotein (HDL, AM203-3)-Chol andaspartate aminotransferase (AST; AM-101K) were determined by an enzyme assaymethod (Asan Pharmaceutical, Yongin, Gyeonggido, Korea). The low-density lipopro-tein (LDL)-Chol level was calculated using the formula of Friedewald et al. [21]. Freefatty acids (FFAs) were measured using a Wako NEFA kit (Wako, Osaka, Japan). Plasmainsulin [Mouse High Range Insulin enzyme-linked immunosorbent assay (ELISA), 80-INSMSH-E01], leptin (mouse/rat leptin ELISA kit 022-LEP-E06) and IL-6 (IL-6 mouseEIA kit 45-IL6MS-E01) levels were determined using ELISA kits (ALPCO Diagnostics,Salem, NH, USA). The Homeostatic model assessment (HOMA) index, an IR index, wascalculated as follows: (fasting serum insulin concentration, nmol/L)×(fasting serumglucose concentration, mmol/L)/22.5 [22]. A high HOMA index indicates low insulin
sensitivity and decreased β-cell function. The plasma concentrations of non-heme iron(#K390-100 Iron Assay Kit; BioVision, Milpitas, CA, USA) and hemoglobin (Hb; AM-503K; Asan Pharmaceutical) were determined by enzyme assay methods. Plasmaferritin (41-FERMS-E01) and transferrin (41-TRANS-E01) levels were determinedusing ELISA kits (ALPCO Diagnostics). Total iron binding capacity (TIBC; AM-507K;Asan Pharmaceutical) was determined by an enzyme assay method, and the degree oftransferrin saturation (TS) and unsaturated iron binding capacity (UIBC) were thencalculated. The hematocrit level was measured using heparinized capillary tubes(MCH-41B2501; Chase, Rockwood, TN, USA).
2.4. Hepatic and pancreatic lipid contents
Liver and pancreas tissues were homogenized, and tissue lipids were extracted inchloroform–methanol solution by the Bligh & Dyer method [23]. The solution wascentrifuged after addition of 0.9% NaCl, and the lower phase was collected forevaporation. Then, phosphate-buffered saline (pH 7.4) containing 1% Triton-100 wasadded to dissolve the pellet [24]. Hepatic and pancreatic TG and Chol concentrationswere measured using the same commercially available kits as used to analyze plasma.
2.5. Liver iron content and lipid peroxidation products
The liver concentration of non-heme iron was analyzed after homogenizationusing the same commercially available kits as used to analyze plasma. Commerciallyavailable kits (Oxis Research, Portland, OR, USA) were used to measure lysateconcentrations of malondialdehyde (MDA; Bioxytech MDA-586).
2.6. Liver and pancreas histology
Liver and pancreas tissue fragments were fixed in 4% paraformaldehyde solution,embedded in paraffin, cut into 5-μm sections and mounted on glass slides. Afterdehydration, they were stained with hematoxylin and eosin (H&E) for visualization ofhistological changes and subjected to Perls' Prussian blue staining to evaluate tissueiron deposits. Digital morphometric analysis, conducted to determine the average sizeand area of pancreatic islets and to quantify tissue iron pools, was performed using aLeica DM5000 optical microscope with Leica Qwin Plus analysis software (Houston,TX, USA).
2.7. Immunohistochemistry for pancreatic insulin
After embedding the specimens in epoxy resin (Araldite), serial semithin sections(0.5 μm) were cut and processed for immunohistochemical staining. The antibody fordetection of insulin was obtained from Santa Cruz Biotechnology (Santa Cruz, CA, USA).Immunostaining was performed according to the avidin–biotin–peroxidase complextechnique using a Vectastain Universal Elite ABC Kit (Vector Laboratories, Burlingame,CA, USA).
2.8. RNA extraction and analysis of mRNA expression
Total RNA was extracted from tissues using TRI reagent (Molecular Research,Cincinnati, OH, USA) according to the manufacturer's instructions. RNA expression wasquantified by real-time quantitative polymerase chain reaction (PCR) using SYBR greenPCR reagents (Applied Biosystems, Foster City, CA, USA) and the ABI PRISM 7900 HTsequence-detection system (Applied Biosystems). Relative quantification values werecalculated by analyzing changes in SYBR green fluorescence during PCR according tothe manufacturer's instructions.
2.9. Immunoblotting analysis
Equal amounts of liver whole-cell lysate proteins were separated by sodiumdodecyl sulfate polyacrylamide gel electrophoresis (SDS-PAGE), transferred ontopolyvinylidene difluoride (PVDF) membranes, and immunoblotted with primaryantibodies. Rabbit polyclonal antibodies against ferritin heavy chain, ceruloplasmin,signal transducer and activator of transcription 3 (STAT3), phospho-STAT3 (p-STAT3),glucokinase (GK), phosphoenolpyruvate carboxylase (PEPCK), glucose 6-phosphatase(G6Pase), fatty acid synthase (FAS), peroxisomal acyl CoA oxidase (AOX), leptin,superoxide dismutase (SOD), glutathione peroxidase (GPx), succinate dehydrogenase(SDH), cytochrome c oxidase (COXIII), catalase, insulin, peroxisome proliferator-activated proteinα (PPARα), sterol regulatory element-binding protein 1 (SREBP1),α-tubulin and β-actin were obtained from Santa Cruz Biotechnology. A rabbit polyclonalantibody against ferroportin was purchased from Novus Biologicals (Littleton, CO,USA). A rabbit polyclonal antibody against hepcidin was purchased from Abcam Inc.(Cambridge, MA, USA). Appropriate secondary antibodies were applied, and the bandswere visualized using enhanced chemiluminescence western blotting detectionreagents (RPN2106; Amersham Biosciences, Uppsala, Sweden) and X-ray film (Agfa,Mortsel, Belgium). Tina 2.0 (Silk Scientific Inc., Orem, UT, USA) was used fordensitometric analysis of immunoreactive bands. Each blot was probed with antibodiesagainst α-tubulin or β-actin to verify equal loading of samples.

1636 J.S. Choi et al. / Journal of Nutritional Biochemistry 24 (2013) 1634–1644
2.10. Statistical analysis
All data are expressed as the means±standard error (S.E.). Data were analyzed byone-way analysis of variance using the SAS statistical analysis program (SAS Institute,Cary, NC, USA). Duncan's multiple-range tests were used to determine the significanceof differences in group means. Differences between means were consideredstatistically significant at Pb.05.
3. Results
3.1. General characteristics
The energy intake of the HF group was greater than that of the LFgroup (LF, 10.27±0.08 kcal/day; HF, 13.11±0.66 kcal/day, HF vs. LF,Pb.05). Loading of the LF diet with iron did not decrease the energyintake significantly, but loading of the HF diet with iron reduced theenergy intake (LF+Fe, 9.27±0.19 kcal/day; HF+Fe, 11.24±0.57 kcal/day; HF vs. HF+Fe, Pb.05). These changes in food intake partiallyexplained the changes in bodyweight. The HF group showed a greaterincrease in body weight than the LF group; iron overload significantlydecreased body weight gain (LF, 5.23±0.35 g; HF, 10.51±0.58 g,LF+Fe, 1.77±0.35 g; HF+Fe, 3.29±0.32g; Pb.05). The high-fat dietsignificantly increased fat weight gain. Iron overload significantlydecreased total epididymal, perirenal and retroperitoneal fat weightsby reducing energy intake and body weight gain (LF, 0.273±0.019g; HF, 0.670±0.040 g; LF+Fe, 0.128±0.016 g; HF+Fe, 0.169±0.011g; Pb.05). The high-fat diet did not significantly increase liverweight. Overloading the low-fat and high-fat diets with ironsignificantly increased liver weights (LF, 1.00±0.02 g; HF, 0.92±0.08 g; LF+Fe, 1.22±0.08 g; HF+Fe, 1.17±0.06 g; Pb.05). There
200
300
400
500
aba
b400
600
800a ab
A D
C B
G H
0
100
Fe(ug/dl)0
200
TIBC(
2
3
4
5
bc
a
d 200
300
400
500 a
0
1
Transferrin(mg/ml)0
100
200
Ferritin
c
40
60
80
10
15
20
25
0
20
Hemato0
5
10
Hemoglobin(mg/dl)
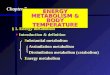
Fig. 1. Effects of the high-fat diet and iron overload on plasma iron parameters. All data are exletters are significantly different (Pb.05).
were no significant differences in pancreas weight between thegroups (LF, 0.124±0.010 g; HF, 0.140±0.006 g; LF+Fe, 0.125±0.011 g; HF+Fe, 0.139±0.011 g).
3.2. Plasma biochemical parameters for iron andglucose/lipid metabolism
LF+Fe mice had higher plasma levels of iron, ferritin, TIBC, UIBCand TS than those in the LF group. Similar trends were observed in HF+Fe versus HF groups (Fig. 1). Plasma transferrin concentration wasdecreased by iron consumption but increased by the HF diet (Fig. 1).The plasma Hb concentration and hematocrit did not differ signifi-cantly between groups (Fig. 1).
Compared with the LF group, the LF+Fe and HF groupsshowed higher plasma glucose levels; the HF+Fe group had thehighest glucose levels (Fig. 2). Levels of insulin and IR werehigher in the HF group than in the LF and LF+Fe groups andwere higher in HF+Fe mice than in HF mice. Plasma T-Chol levelswere higher in the HF group, but lower in the LF+Fe group,compared with the LF group. T-Chol levels were significantlydecreased by iron supplementation. Adding iron to the dietsdecreased T-Chol levels without altering LDL-Chol levels. Conse-quently, HDL-Chol levels were significantly decreased by the high-iron diet. The HF+Fe group had the lowest HDL-Chol levels; theLF+Fe group and HF groups had intermediate Chol levels; and theLF group had the highest HDL-Chol level. Plasma TG and FFAconcentrations were not significantly different among the groups(Supplementary Table 1).
ba
40
60
80
100
b
a
b
a
F
ug/dl)0
20
TS(%)
b
(ng/ml)
c
LF LF+FeHFHF+Fe
crit(%)
pressed as the means±S.E. of 12–15 mice per group. Groups with different superscript

A B
200
250
a 4
5
a
0
50
100
150
c
bb
mg
/dl
0
1
2
3
ng
/ml
cbc
b
C1205
Glucose
DInsulin
20
40
60
80
100 a
c
ab
bc
mg
/dl
1
2
3
4
c
a
bbc
0
20
HDL-Chol0
IR index
LF LF+Fe HF HF+Fe
Fig. 2. Effects of the high-fat diet and iron overload on plasma biochemical parametersfor glucose/lipid metabolism All data are expressed as the means±S.E. of 12–15 miceper group. Groups with different superscript letters are significantly different (Pb.05).
1637J.S. Choi et al. / Journal of Nutritional Biochemistry 24 (2013) 1634–1644
3.3. Hepatic changes in iron and lipid metabolism
The activity of AST, a marker of hepatic injury, did not differsignificantly among the groups (Supplementary Table 1). Onhistological examination, the HF group showed marked hepaticsteatosis compared with the LF group (Fig. 3A and B). Ironsupplementation increased the accumulation of hepatic fat withinflammatory foci (Fig. 3A and B). Dietary iron supplementationresulted in a significant increase in hepatic iron content, asdetermined by Perls' Prussian blue staining (Fig. 3C) and biochemicalanalysis (Fig. 3D). The LF group showed normal liver histologywithout any apparent iron deposits (Fig. 3C). The high-fat diet did notaffect hepatic iron content as compared to the low-fat diet (Fig. 3Cand D). In contrast, groups with iron overload exhibited hepatic irondeposition, predominantly in Kupffer cells, and intense hydropicdegeneration in a few areas.
Iron supplementation led to a significant increase in hepaticferritin protein expression, as determined by immunoblottinganalysis (Fig. 4A and B). No such significant elevation was observedin mice fed with the high-fat diet in comparison to those fed with thelow-fat diet. In contrast, mice fed with the high-fat diet hadsignificantly higher hepcidin protein expression levels compared tothose fed with the low-fat diet. When iron was supplemented, thelevel of hepcidin protein expression was significantly increased andwas significantly higher in mice fed with the high-fat diet (Fig. 4A andB). Accordingly, the HF group showed significantly lower hepaticferroportin and ceruloplasmin protein expression levels compared tothe LF group (Fig. 4A and B). The LF+Fe and HF+Fe groups showedlower ferroportin expression than the LF and HF groups (Fig. 4A andB). Ceruloplasmin protein expression was similarly altered by thehigh-fat diet and iron treatment (Fig. 4A and B).
3.4. Hepatic iron and inflammatory responses
As inflammatory processes play a role in the pathogenesis of IR,we investigated plasma IL-6 levels and hepatic expression profiles
of proinflammatory cytokines in high-fat diet-fed and iron-treatedmice. While the high-fat diet tended to increase plasma IL-6 levels,it significantly increased hepatic IL-6 mRNA expression (Fig. 5A andB). Iron supplementation significantly increased plasma IL-6 levelsand hepatic IL-6 and IL-1β mRNA expression. The HF+Fe groupshowed higher tumor necrosis factor (TNF-α) and C-reactiveprotein (CRP) mRNA expression than the HF group (Fig. 5B). Asproinflammatory cytokines are considered molecular mediators ofIR, we assessed the effects of the high-fat diet and iron overload onSTAT3 signaling in the liver. The high-fat diet significantly increasedphosphorylation of STAT3 in the liver, and iron overload furtherincreased STAT3 phosphorylation (Fig. 5C and D).
3.5. Hepatic gluconeogenesis and lipid metabolism
Next, we examined how iron affected the expression of proteinsinvolved in gluconeogenesis. Levels of GK protein were significantlylower in the HF group than in the LF group and were lowest in theHF+Fe group (Fig. 6A and B). The levels of G6Pase and PEPCKexpression were significantly higher in the LF+Fe group and HFgroup than in the LF group (Fig. 6A and B). To further investigate theinvolvement of excess iron accumulation in hepatic lipid homeostasis,wemeasured the expression of proteins involved in fatty acid synthesisand oxidation. The high-fat diet significantly increased the expressionlevels of the lipogenesis-related proteins FAS and SREBP1 (Fig. 6C andD). The protein expression levels of PPARα andAOX (the product of oneof its target genes and a protein involved in fatty acid oxidation) weresignificantly decreased in the HF group (Fig. 6C and D). Ironsupplementation increased these changes in the LF+Fe group but notin the HF+Fe group (Fig. 6C and D).
3.6. Mitochondrial function and the antioxidant defense system
We determined the protein expression of members of theantioxidant defense system (SOD, GPx and catalase) and therespiratory chain complexes SDH (Complex II) and COXIII (ComplexIV) in liver lysates. The high-fat diet significantly reduced SOD andGPx expression compared with the low-fat diet (Fig. 7A and B). The LF+Fe and HF+Fe groups showed significantly reduced expression ofthese proteins compared to the LF and HF groups (Fig. 7A and B). Thelevels of SDH and COXIII expression were significantly lower in the HFgroup than the LF group (Fig. 7A and B). COXIII levels were lower inthe LF+Fe group than in the LF group (Fig. 7A and B). MDA, an indexof lipid peroxidation, was measured in liver homogenates (Fig. 7C).The HF group showed significantly higher levels of MDA comparedwith the LF group (Fig. 7C). Iron supplementation in the LF groupincreased lipid peroxidation, as did the high-fat diet (Fig. 7C).Excessive iron accumulation is associated with an increase in freeradical-induced oxidative stress and may lead to antioxidantdepletion and mitochondrial dysfunction.
3.7. Insulin and iron metabolism in the pancreas
The high-fat diet induced significant increases in fat dropletaccumulation (Fig. 8A) and TG content in the pancreas (Fig. 8E)compared to the LF group (Fig. 8A and E). Pancreatic iron contentwas increased by iron overload (Fig. 8B). Similarly, iron overloadled to a significant increase in pancreatic ferritin protein levels(Fig. 8G and H), while ferritin levels were not significantly affectedby the high-fat diet. However, the HF group showed a significantincrease in pancreatic hepcidin protein expression compared to theLF group (Fig. 8G and H). The HF and HF+Fe groups showed lowerislet expression of insulin than the LF group. The LF+Fe group alsoshowed lower insulin levels than the LF group (Fig. 8D). Similarchanges in insulin levels were detected by immunoblotting

A H&E stain
LF LF+Fe HF HF+Fe
B Lipid levels
400
800
1200
1600
baa a
b
aaa
mg
/g li
ver LF
LF+FeHF HF+Fe
C Prussian blue stain
0
400
TG T-chol
LF LF+Fe HF HF+Fe
D Iron levels
20
30
40
a a LF LF+FeHF
0
10
20
Fe
ug
/g li
ver
bb HF+Fe
Fig. 3. Effects of the high-fat diet and iron overload on hepatic lipid and iron contents. Histological analysis of liver sections frommice fed with experimental diets (n=4). Sections weresubjected to H&E staining (A) and Perls' Prussian blue staining (C) and are shown at ×40 and ×100magnification; (B) Hepatic lipid levels weremeasured by an enzymatic method afterlipid extraction (n=12–15); (D) Iron levels in liver homogenates were measured by chemical analysis. All data are expressed as the means±S.E. of 12–15mice per group. Groups withdifferent superscript letters are significantly different (Pb.05).
1638 J.S. Choi et al. / Journal of Nutritional Biochemistry 24 (2013) 1634–1644
(Fig. 8G and H). However, islet circumference was significantlyincreased by the high-fat diet and was further increased by ironoverload (Fig. 8C and F).
4. Discussion
Recent studies have demonstrated a relationship between ironmetabolism and IR by showing the strong correlation between ironstores and IR in clinical situations [2,13,25]. Patients with metabolicsyndrome or Type 2 diabetes exhibit a form of IR associated withhepatic iron overload [8,12]. However, the mechanisms underlyingthe effect of iron overload on the development of diabetes are not wellknown, despite data from animal studies of genetic obesity. Thepresent study was performed to explore the biochemical mechanisms
by which excessive iron accumulation leads to obesity and IR andvice versa.
In this study, we investigated the effects of iron overload and high-fat diet on glucose metabolism in an animal model of obesity. Ourresults indicated that mice fed with a high-fat diet showedhyperglycemia, hyperinsulinemia and IR, abnormalities characteristicof metabolic syndrome and Type 2 diabetes. Iron loading also led tohyperglycemia, hyperinsulinemia and IR. Concomitant consumptionof a high-fat diet and iron synergistically increased IR. These resultssuggest that excess iron intake could cause pathology similar to thoseseen in Type 2 diabetes, metabolic syndrome and associated vasculardisorders. It is interesting to note that iron supplementation increasedLDL-Chol levels and decreased HDL-Chol levels.
Next, the molecular mechanisms of iron-induced IR wereinvestigated. A number of epidemiological studies have suggested

Ferritin
A Protein expression B Densitometry
2468
10
b
aa
b 1.01.52.02.5
cbab
aLF LF+Fe HF HF+Fe
Hepcidin
Ferroportin
Ceruloplasmin1.0
1.5 a
cbcb
a
cbb
02
Ferritin
Arb
itra
ry u
nit
s
Arb
itra
ry u
nit
s
0.00.5
Hepcidin
Actin 0.0
0.5
Ceruloplasmin
c
Arb
itra
ry u
nit
s
1.0
1.5
0.0
0.5
Arb
itra
ry u
nit
s
Ferroportin
LF LF+Fe HF HF+Fe
Fig. 4. Effects of the high-fat diet and iron overload on iron metabolism in the liver. (A, B) Immunoblotting analysis of iron metabolism-related proteins. All data are expressed as themeans±S.E. of 12–15 mice per group. Groups with different superscript letters are significantly different (Pb.05).
B Gene expression
6 7 8 9
10
aa
aa
0 1 2 3 4 5
IL-6 IL-1β TNFα CRP
(gen
e/18
S r
RN
A)
cabb
a
bb
ab
b
a
ba
b b
LF LF+Fe HF HF+Fe
mR
NA
exp
ress
ion
C Protein expression D Densitometry
p-STAT3
123456
cb
a
bc
LF LF+Fe HF HF+Fe
STAT3
Tubulin
0
LF
LF
+Fe
HF
HF
+Fe
Arb
itra
ry u
nit
sA Plasma IL6 levels
50
010203040
pg
/ml a
bcc
b
LF+FeHF HF+Fe
IL-6
LF
Fig. 5. Effects of the high-fat diet and iron overload on inflammatory processes in the plasma and liver. (A) Plasma IL-6 levels (B) real-time PCR analysis of inflammation-relatedproteins; (C) Immunoblotting analysis of inflammation-related proteins. All data are expressed as the means±S.E. of 12–15 mice per group. Groups with different superscript lettersare significantly different (Pb.05). IL-6, IL-6; IL-1β, IL-1β; TNFα, tumor necrosis factor α.
1639J.S. Choi et al. / Journal of Nutritional Biochemistry 24 (2013) 1634–1644

A Glucose metabolism B Densitometry
GK
0.2 0.4 0.6 0.8 1.0 1.2
a
bc
c
b
Arb
itra
ry u
nit
sLF LF+Fe HF HF+Fe
G6Pase
Actin1.5
2.0
2.5
c
aa
b
1.5 2.0 2.5 3.0
cb
aba
0.0
0.0
0.5
1.0
G6Pase0.0 0.5 1.0
PEPCK
2.0
3.0
4.0
5.0
c
aa
b 0.8 1.0 1.2 1.4 1.6
a
bcb
LF LF+Fe HF HF+Fe
FAS
PPARα
2.5 aaa 1.2
1.4 a
0.0
1.0
SREBP10.0 0.2 0.4
PPARα
Actin
AOX
0.0
0.5
1.0
1.5
FAS
b
0.0 0.2 0.4 0.6 0.8 1.0
AOX
b
b b
LF LF+Fe HF HF+Fe
C Lipid metabolism D Densitometry
PEPCK
SREBP1
2.0
c
Arb
itra
ry u
nit
s
Arb
itra
ry u
nit
s
0.6
Arb
itra
ry u
nit
sA
rbit
rary
un
its
Arb
itra
ry u
nit
sA
rbit
rary
un
its
1.4
GK
Fig. 6. Effects of the high-fat diet and iron overload on glucose and lipid metabolism in the liver. Immunoblotting analysis of glucose and lipid metabolism-related proteins. All data areexpressed as the means±S.E. of 12–15 mice per group. Groups with different superscript letters are significantly different (Pb.05).
1640 J.S. Choi et al. / Journal of Nutritional Biochemistry 24 (2013) 1634–1644
that obesity is associated with iron deficiency, reflecting consump-tion of energy-dense, nutrient-poor food [26,27]. In the presentstudy, severe iron deficiency was not induced by fat consumption.Mice fed with high-fat diet had similar plasma levels of iron andferritin, as well as values for other iron metabolism-relatedparameters, to those fed with low-fat diet. Similarly, mice in theHF+Fe and LF+Fe groups had similar values for these factors. As thelow- and high-fat diets in our study contained adequate levels of ironfor mice, iron metabolism-related parameters in plasma and tissueswere similar in high-fat diet- and low-fat diet-fed mice. Therefore,we concluded that iron deficiency in obesity cannot be entirelyexplained by the lower iron content of fat-dense diets. Physiologicalconditions and fluctuations in iron absorption, transport andmetabolism should be taken into consideration in mice receiving ahigh-fat diet. Iron supplementation would have affected ironmetabolism in plasma and tissues. Iron supplementation markedlyincreased the levels of iron and ferritin in plasma, liver and pancreas,and also promoted iron storage as ferritin due to the scavenging ofexcess iron in tissues. In fact, hepatic and pancreatic ferritin levelstended to be higher in mice fed with iron-enriched high-fat dietcompared to the HF group. Ferritin and increased body iron stores
were shown to be associated with IR and metabolic abnormalitiesdefining metabolic syndromes in population studies [1,2,12–14]. Ironstores are associated with metabolic syndrome and Type 2 diabetesin ethnically diverse populations. However, iron overload-associatedIR remains a matter of debate as inflammation and oxidative stressmay also complicate the storage of iron.
The iron regulatory hormone hepcidin is primarily produced byhepatocytes and controls iron metabolism following binding toferroportin by inducing its internalization and degradation[16,28,29]. Ferroportin is an iron export protein expression of whichis negatively regulated by hepcidin [16]. Marked down-regulation ofthe cellular iron exporter ferroportin has been observed in NAFLD,whereas hepcidin levels were increased in dysregulated iron overloadsyndrome [30,31]. Although the high-fat diet had no effect on overalliron homeostasis in the present study, the levels of hepcidinexpression in the liver and pancreas were increased in high-fatdiet-fed mice compared to those fed the low-fat diet. Generally,hepcidin is linked with inflammation. In the present study, ironoverload increased the levels of IL-6, a marker of inflammation. Micefed with an iron-supplemented diet showed higher hepcidinexpression in the liver and pancreas, consistent with increased tissue

A Protein expression B Densitometry
SOD 0.5
1.0
1.5
c
ab
c
Arb
itra
ry u
nits
0.5
1.0
1.5
bca
c
b
Arb
itra
ry u
nitsLF LF+Fe HF HF+Fe
0.5
1.0
1.5 a
b b
a
bit
rary
un
its
GPx
Catalase
0.0
GPx
A0.0
SOD
A
SDH
0.0
Catalase
Arb
Actin
COXIII
0.5
1.0
1.5 a
c
abbc
trar
y u
nits
0.5
1.0
1.5 a
bcbc
trar
y u
nits
0.0
0.5
SDH
Arb
it
0.0
0.5
COXIII
Arb
it
LF LF+Fe HF HF+Fe
C Malondialdehyde
60
80
cab a
b
rote
insu
e
0
20
40
LF LF+Fe HF HF+Fe
uM
/mg
p/g
tis
s
Fig. 7. Effects of the high-fat diet and iron overload on antioxidative activity andmitochondrial function in the liver. (A, B) Immunoblotting analysis of insulin and iron-related proteins;(C) MDA levels in liver homogenates, as measured by an enzymatic method. All data are expressed as the means±S.E. of 12–15 mice per group. Groups with different superscriptletters are significantly different (Pb.05).
1641J.S. Choi et al. / Journal of Nutritional Biochemistry 24 (2013) 1634–1644
levels of iron and ferritin. The increase in hepcidin expressionfollowed decreases in the expression of ferroportin and ceruloplas-min, which are believed to be induced by inflammation andmicronutrient imbalance. Interestingly, these effects were lesspronounced in mice fed with high-fat diet compared to those fedwith low-fat diet. The frequent observation of inflammatory re-sponses in obese individuals led to the suggestion that disturbances ofiron homeostasis in obesity may be partly due to inflammation. Takentogether, the results of our studies suggest that iron accumulation inmice fed with an iron-enriched diet results from increased hepcidinlevels, leading to reduced iron release based on increased ferroportindegradation. We also concluded that consumption of a high-fat dietmay contribute to increased hepcidin levels in obesity, resulting fromthe increased production of proinflammatory cytokines.
A close connection between IR and inflammatory signalingpathways has been identified. The proinflammatory cytokine IL-6induces hepcidin gene transcription by stimulating the phosphoryla-tion and nuclear translocation of STAT3, where it binds to a proximalpromoter element [32]. IL-1β also activates hepcidin via the CCAAT/enhancer binding protein (C/EBPα) and bone morphogenetic protein(BMP)/SMAD pathways [32]. Although we did not find thatexcessive iron-mediated inflammatory cytokine production directlyattenuates insulin signaling, excessive fat and iron intake inducedhyperglycemia and IR in our study. Our results indicated that the
plasma IL-6 level was increased in mice fed with high-fat diet. Ironsupplementation also markedly increased liver expression of IR-mediating adipocytokines, such as the inflammatory genes encod-ing TNF-α, IL-6, IL-1β and CRP, and plasma IL-6 levels, suggestingthat excessive iron accumulation may activate inflammatorypathways. These results indicated that excessive fat or iron intakecan exacerbate IR through activation of inflammatory genes. Highlevels of fat and iron intake play important roles in increasing thelevels of these cytokines, and they may contribute to induction ofhepcidin expression.
Feeding mice with a high-fat or iron-supplemented diet worsenedhyperglycemia, hyperinsulinemia and IR and had harmful effects onfatty acid and glucose metabolism. Moreover, the high-fat diet and ironsupplementation acted synergistically. This synergistic action of ironsupplementation was stronger for the low-fat diet than the high-fatdiet. The protein expression levels of rate-limiting gluconeogenicenzymes were significantly affected. The high-fat diet and ironsupplementation significantly increased G6Pase and PEPCK expressionbut decreased GK expression. The levels of expression of these glucose-metabolizing related enzymes were affected more strongly by ironsupplementation of the low-fat diet than the high-fat diet.We observedan increase in glucose levels in high-fat diet-fed and iron-overloadedmice in the presence of elevated insulin levels, suggesting increased IRduring iron deposition. Both the high-fat diet and iron supplementation

A Lipid
80 a
E TG levels B Iron C Islet D Insulin
LF
LF+Fe 0
20
40
60
b
aab
TG
HF
HF
+Fe
ab
F Islet Circumference
HF+Fe
G Western blot0
500100015002000 c
Isle
t ci
rcu
mfe
ren
ce(µ
)
LF LF+Fe HF HF+Fe
H Relative expression
0.5
1.0
1.5
2.0
2.5
aab
bc
c
Hep
cid
in
3
6
9
12
15
b
a
b
a
Fer
riti
n
0.3
0.6
0.9
1.2
a
bb b
Insu
lin
0.0
LF
LF
+Fe
HF
HF
+Fe
0
LF
LF
+Fe
HF
HF
+Fe
0.0
LF
LF
+Fe
HF
HF
+Fe
(mg
/g p
ancr
eas)
HF
LF
LF
+Fe
HF
+Fe
HF
LF
LF
+Fe
b30002500
Insulin
Ferritin
Hepcidin
Tubulin
1.5 3.0
Fig. 8. Effects of the high-fat diet and iron overload on insulin levels and iron metabolism in the pancreas. Histological analysis of pancreas sections from mice fed experimental diets(n=4). Sections were subjected to H&E staining for lipid droplet analysis (A) and Perls' Prussian blue staining for iron analysis (B) and are shown at ×40 and ×100magnification; (C, F)Images of islets were acquired using an Axioskop microscope with an Axio Cam camera (Carl Zeiss, Jena, Germany) after H&E staining, and islet circumferences were determined usingImage-Pro Plus 4.0 software (Media Cybernetics Inc, Silver Spring, MD, USA); (D) Representative images of histochemical analysis of insulin expression using an antiinsulin antibody.Brown areas indicate positive staining for insulin; (E) Pancreatic lipid levels, as measured by an enzymatic method after lipid extraction; (G, H) Immunoblotting analysis of insulin andiron-related proteins. All data are expressed as the means±S.E. of 12–15 mice per group. Groups with different superscript letters are significantly different (Pb.05).
1642 J.S. Choi et al. / Journal of Nutritional Biochemistry 24 (2013) 1634–1644
were also found to affect fatty acid synthesis and oxidation in the liver;they resulted in significantly increased expression of SREBP1 and FASand reduced expression of PPARα and AOX. The levels of expression ofthese proteins were more markedly altered by iron supplementation ofthe low-fat diet than the high-fat diet, which may result in inductionof lipid synthesis, and thereby increase hepatic TG and Chol levels,resulting in hepatic steatosis. Based on the excessive iron accumulationin hepatic tissues, we concluded that activation of SREBP1, FAS, G6Pase
and PEPCK and deactivation of PPARα, AOX and GK enhance IR throughactivation of gluconeogenesis and lipid synthesis in the liver. It has beenreported that iron depletion caused by deferoxamine amelioratedglucose metabolism, inducing glucose clearance and utilization andincreasing insulin receptor binding activity and signaling, in a model offatty liver characterized by increased basal glucose levels [33,34]. Theseobservations suggest that iron status may affect the progression tohyperglycemia in patients with hepatic IR.

Fat overload Iron overload
Hyperinsulinemia Inflammatory index Oxidative stress, mitochondrial dysfunction
Iron depositHepcidin, Ferritin
PancreasLiver Pancreas Insulin secretion Lipid accumulation
Liver Gluconeogenesis Lipid accumulation Insulin extraction
Metabolic syndromes Di b tDiabetes
Fig. 9. Potential mechanism on how iron overload and fat overload may contribute to IR.
1643J.S. Choi et al. / Journal of Nutritional Biochemistry 24 (2013) 1634–1644
Endoplasmic reticulum (ER) stress has attracted a great deal ofattention as it has been linked to the pathogenesis of Type 2 diabetesand inhibition of insulin signaling [35,36]. The acute inflammatoryresponse has been linked to ER stress, and both LPS and IL-6 are alsopotent inducers of hepcidin in the liver [37]. The CREBH-hepcidin axismay cooperate with other signaling pathways, such as the IL-6/STAT3pathway, to stimulate hepcidin expression during inflammation [32].There is evidence that free radical formation may play a role in themechanism by disrupting the action of insulin and total body glucosedisposal. Iron is a powerful prooxidant, and oxidative stress increasesunder conditions of glucose intolerance [12–14]. ROS have beenimplicated in the pathogenesis of IR based on the associations ofoxidative stress markers with obesity and Type 2 diabetes [38,39].Unbalanced oxidative stress is considered to act as a trigger of NAFLD[40]. In the present study, iron supplementation induced steatosisthrough deposition of iron in the liver and pancreas. Theseobservations suggest that iron accumulation increases oxidativestress throughout the whole body. Increased plasma and hepaticiron contents and ferritin levels were observed in iron-supplementedmice in the present study. Hepatic lipid peroxidation was alsoincreased in iron-supplemented mice. The high-fat diet caused theformation of ROS, such as MDA and hydrogen peroxide, and reducedSOD and GPx expression, resulting in subsequent hepatic damage.Iron overload induced similar effects on oxidative stress by promotingboth ROS production and reduced expression of antioxidant enzymes.As hepatic fat and iron overload lead to oxidative stress, there is anassociated down-regulation of antioxidant defenses that may becritical for limiting the accumulation of oxidative damage. The co-occurrence of steatosis and these oxidative responses may compro-mise the ability to mediate iron-dependent oxidative damage andmetabolic dysfunction. With the above-mentioned inflammatoryresponse, ER stress and hepatic steatosis, this oxidative stress causesmitochondrial dysfunction. Notably, the levels of SDH and COXIIIexpression were reduced in our study. There is little doubt that irondeposition in diabetes mellitus exacerbates oxidative stress. Thus,iron deposition may ameliorate diabetic abnormalities by promotingROS generation with the decreased labile iron pool.
Next, we examined whether iron overload affected insulinproduction, which is important for β-cell function. We found that
pancreatic iron and TG deposition significantly decreased insulinexpression in the pancreas. Iron overload induced iron deposition andthe expression of ferritin protein, which triggered the down-regulation of insulin protein expression. These findings wereconfirmed by immunocytochemical analysis of insulin. Weak insulinstaining was detected in the islets in high-fat diet-fed and iron-overloaded mice. Iron overloaded β-cells showed weak staining,suggesting β-cell dysfunction. Kulaksiz et al. [41] reported that thesubcellular level of hepcidin was confined to the typical secretorygranules of β-cells, where insulin is localized. We found that hepcidinwas also expressed in the pancreas, where the peptide wasspecifically localized to the β-cells. Interestingly, insulin expressionwas also regulated in a hepcidin-dependent manner. The relationshipbetween iron overload and pancreatic β-cell impairment may resultin hyperglycemia. Iron accumulation in the liver may interfere withhepatic insulin extraction, thereby causing IR.
The results of the present study indicated that iron accumulationin the plasma, liver and pancreas affected unfavorably lipid andglucose metabolism. The IR induced by the high-fat diet and ironoverload is thought to be due to disturbance of not only ironmetabolism but also of metabolic events/processes, such as IR,glucose and lipid metabolism, inflammatory responses, oxidativestress and mitochondrial dysfunction (Fig. 9).
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.jnutbio.2013.02.004.
References
[1] Munŏz M, García-Erce JA, Remacha AF. Disorders of iron metabolism. Part 1:molecular basis of iron homoeostasis. J Clin Pathol 2011;64:281–6.
[2] McClain DA, Abraham D, Rogers J, Brady R, Gault P, Ajioka R, et al. Highprevalence of abnormal glucose homeostasis secondary to decreased insulinsecretion in individuals with hereditary haemochromatosis. Diabetelogia2006;49:1661–9.
[3] Kim CH, Kim HK, Bae SJ, Park JY, Lee KU. Association of elevated serum ferritinconcentration with insulin resistance and impaired glucose metabolism in Koreanmen and women. Metabolism 2010;60:414–20.
[4] Ford ES, Cogswell ME. Diabetes and serum ferritin concentration among US adults.Diabetes Care 1999;22:1978–83.
[5] Luan de C, Li H, Li SJ, Zhao Z, Li X, Liu ZM. Body iron stores and dietary iron intakein relation to diabetes in adults in North China. Diabetes Care 2008;31:285–6.

1644 J.S. Choi et al. / Journal of Nutritional Biochemistry 24 (2013) 1634–1644
[6] Sun L, Franco OH, Hu FB, Cai L, Yu Z, Li H, et al. Ferritin concentrations, metabolicsyndrome, and type 2 diabetes in middle aged and elderly Chinese. J ClinEndocrinol Metab 2008;93:4690–6.
[7] Hramiak IM, Finegood DT, Adams PC. Factors affecting glucose tolerance inhereditary hemochromatosis. Clin Invest Med 1997;20:110–8.
[8] HaapM, Fritsche A, Mensing HJ, Haring HU, Stumvoll M. Association of high serumferritin concentration with glucose intolerance and insulin resistance in healthypeople. Ann Intern Med 2003;139:869–71.
[9] Cooksey RC, Jones D, Gabrielsen S, Huang J, Simcox JA, Luo B, et al. Dietary ironrestriction or iron chelation protects from diabetes and loss of β-cell function inthe obese (ob/ob lep −/−) mouse. Am J Physiol Endocrinol Metab 2010;298:1236–43.
[10] George DK, Goldwurm S, MacDonald GA, Cowley LL, Walker NI, Ward PJ, et al.Increased hepatic iron concentration in nonalcoholic steatohepatitis is associatedwith increased fibrosis. Gastroenterology 1998;114:311–8.
[11] Valenti L, Fracanzani AL, Bugianesi E, Dongiovanni P, Galmozzi E, Vanni E, et al.HFE genotype, parenchymal iron accumulation, and liver fibrosis in patients withnonalcoholic fatty liver disease. Gastroenterology 2010;138:905–12.
[12] Jehn M, Clark JM, Guallar E. Serum ferritin and risk of the metabolic syndrome inU.S. adults. Diabetes Care 2004;27:2422–8.
[13] Tuomainen TP, Nyyssonen K, Salonen R, Tervahauta A, Korpela H, Lakka T, et al.Body iron stores are associated with serum insulin and blood glucoseconcentrations. Population study in 1,013 eastern Finnish men. Diabetes Care1997;20:426–8.
[14] Mendler MH, Turlin B, Moirand R, Jouanolle AM, Sapey T, Guyader D, et al. Insulinresistance-associated hepatic iron overload. Gastroenterology 1999;117:1155–63.
[15] Silvaa M, Silvaa ME, de Paulaa H, Carneiroc CM, Pedrosaa ML. Iron overload altersglucose homeostasis, causes liver steatosis, and increases serum triacylglycerolsin rats. Nutr Res 2008;28:391–8.
[16] Nemeth E, Tuttle MS, Powelson J, Vaughn MB, Donovan A, Ward DM, et al.Hepcidin regulates cellular iron efflux by binding to Ferroportin and inducing itsinternalization. Science 2004;306:2090–3.
[17] Nicolas G, Chauvet C, Viatte L, Danan JL, Bigard X, Devaux I, et al. The geneencoding the iron regulatory peptide hepcidin is regulated by anemia, hypoxia,and inflammation. J Clin Invest 2002;110:1037–44.
[18] Chung B, Matak P, McKie AT, Sharp P. Leptin increases the expression of the ironregulatory hormone hepcidin in HuH7 human hepatoma cells. J Nutr 2007;137:2366–70.
[19] Bekri S, Gual P, Anty R, Luciani N, Dahman M, Ramesh B, et al. Increased adiposetissue expression of hepcidin in severe obesity is independent from diabetes andNASH. Gastroenterology 2006;131:788–96.
[20] Fernandex-Real JM, Equitani F, Moreno JM, Manco M, Ortega F, Ricart W. Study ofcirculating prohepcidin in association with insulin sensitivity and changing ironstores. J Clin Endocrinol Metab 2009;94(3):982–8.
[21] Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparativeultracentrifuge. Clin Chem 1972;18(6):499–502.
[22] Matthews DR, Hosker JP, Rudenski AS. Homeostasis model assessment: insulinresistance and β-cell function from fasting plasma glucose and insulinconcentrations in man. Diabetologia 1985;28:412–9.
[23] Bligh EG, Dyer WJ. A rapid method of total lipid extraction and purification. Can JMed Sci 1959;37:911–7.
[24] Burant CF, Sreenan S, Hirano K, Tai TA, Lohmiller J, Lukens J, et al. Troglitazoneaction is independent of adipose tissue. J Clin Invest 1997;100:2900–8.
[25] Kishimoto M, Endo H, Hagiwara S, Miwa A, Noda M. Immunohistochemicalfindinds in the pancreatic islets of a patient with transfusional iron overload anddiabetes: case report. J Med Invest 2010;57:345–9.
[26] McClung JP, Karl JP. Iron deficiency and obesity: the contribution of inflammationand diminished iron absorption. Nutr Rev 2009;67:100–4.
[27] Pinhas-Hamiel O, Newfield RS, Koren I, Agmon A, Lilos P, Phillip M. Greaterprevalence of iron deficiency in overweight and obese children and adolescents.Int J Obes Relat Metab Disord 2006;27:416–8.
[28] Weiss G. Iron metabolism in the anemia of chronic disease. Biochim Biophys Acta2009;1790:682–93.
[29] Hentze MW, Muckenthaler MU, Andrews NC. Balancing acts: molecular control ofmammalian iron metabolism. Cell 2004;117:285–97.
[30] Aigner E, Theurl I, Theurl M, Lederer D, Haufe H, Dietze O, et al. Pathwaysunderlying iron accumulation in human nonalcoholic fatty liver disease. Am J ClinNutr 2008;87:1374–83.
[31] Pigeon C, Ilyin G, Courselaud B, Leroyer P, Turlin B, Brissot P, et al. A new mouseliver-specific gene, encoding a protein homologous to human antimicrobialpeptide hepcidin, is overexpressed during iron overload. J Biol Chem 2001;276:7811–9.
[32] Wang J, Pantopoulos K. Regulation of cellular iron metabolism. Biochem J2011;434:365–81.
[33] Dongiovanni P, Valenti L, Fracanzani AL, Gatti S, Cairo G, Fargion S. Iron depletionby deferoxamine up-regulates glucose uptake and insulin signaling in hepatomacells and in rat liver. Am J Pathol 2008;172:738–47.
[34] Vaithilingama V, Oberholzerb J, Guilleminc GJ, Tuchd BE. Beneficial effects ofdesferrioxamine on encapsulated human islets—in vitro and in vivo study. Am JTransplant 2010;10:1961–9.
[35] Muoio DM, Newgard CB. Biomedicine, Insulin resistance takes a trip through theER. Science 2004;306:452–6.
[36] Ozcan U, Cao Q, Yilmaz E, Lee AH, Iwakoshi NN, Ozdelen E, et al. Endoplasmicreticulum stress links obesity, insulin action, and type 2 diabetes. Science2004;306:457–61.
[37] Vecchi C, Montosi G, Zhang K, Lamberti L, Duncan SA, Kaufman RJ, et al. ER stresscontrols iron metabolism through induction of hepcidin. Science 2009;325:877–80.
[38] Furukawa S, Fujita T, Shimabukuro M, Iwaki M, Yamada Y, Nakajima Y, et al.Increased oxidative stress in obesity and its impact on metabolic syndrome. J ClinInvest 2004;114:1752–61.
[39] Urakawa H, Katsuki A, Sumida Y, Gabazza EC, Murashima S, Morioka K, et al.Oxidative stress is associated with adiposity and insulin resistance in men. J ClinEndocrinol Metab 2003;88:4673–6.
[40] Jouihan HA, Cobine PA, Cooksey RC, Hoagland EA, Boudina S, Abel ED, et al. Iron-mediated inhibition of mitochondrial manganese uptake mediates mitochondrialdysfunction in a mouse model of hemochromatosis. Mol Med 2008;14:98–108.
[41] Kulaksiz H, Fein E, Redecker P, Stremmel W, Adler G, Cetin Y. Pancreatic b-cellsexpress hepcidin, an iron-uptake regulatory peptide. J Endocrinol 2008;197:241–9.




![HYDRO BASIC - · PDF fileHYDRO BASIC 3ULUXþQLN]DXSRUDEX ... ergonomic design, the performance of advanced ... metabolism, aids in the draining of excess fluids](https://img.pdfslide.tips/doc/110x75/5a7ba67e7f8b9a2e358c0d49/hydro-basic-basic-3uluxqlndxsrudex-ergonomic-design-the-performance-of-advanced.jpg)


















![[Kelompok 2] Excess-3](https://img.pdfslide.tips/doc/110x75/55c3a6bcbb61ebeb7b8b4572/kelompok-2-excess-3.jpg)


