Embed Size (px)
Citation preview

專題報告主題:
Diabetes Mellitus (DM)糖尿病
日期:3/18(五) 1600-1730
報告人:莊承翰、詹雅衣、許瑞育實習生
指導藥師:鄭淑妃總藥師、許家禎藥師、王敏如藥師

Introduction
Diagnosis
Treatment
Case report
Discussion
2
Outline

國人洗腎原發原因以糖尿病居第一位(43.2%)。台灣腎臟醫學會
高血糖個案未來5年內發生心臟病、中風及腎臟疾病的危險性是一般人的1.5倍、2.9倍及2.4倍。國民健康局
3
前言

Age populations
Obesity
Physical inactivity
High sugar & Fat diet
Others
4
Epidemics
http://www.deo.ucsf.edu/types-of-diabetes/type-2.html

項目
盛行率
全體 男 女
高血糖 8.0% 8.7% 7.5%
表 96年20歲以上民眾高血糖盛行率高血糖定義:空腹8小時以上血糖值≧126mg/dL或服用降血糖藥物。
5

Pathogenitise

7
The Effect of Insulin
http://www.deo.ucsf.edu/type1/understanding-diabetes/how-the-body-processes-sugar/cotrolling-blood-sugar.html

8
Insulin Secretion
Panel 2. Insulin secretion-www.betacell.org

Metabolic disorders Fat metabolism
Carbohydrate metabolism
Protein metabolism
A relative or an absolute lack of insulin
Glucose intolerance Hyperglycemia
9
Causes of DM

Type 1 diabetes mellitus (T1DM)
Type 2 diabetes mellitus (T2DM)
Gestational diabetes mellitus (GDM)
Other specific type (uncommon)
10
Classification

11
T1DM & T2DM
The cells ignore the insulin or the body
does not produce enough insulin.
Normal insulin function, but not enough.
Hyperglycemia when 80% to 90% of
β-cells are destroyed.

12
Peripheral
insulin
resistance
Impaired
glucose
tolerance
Early diabetes
Late diabetes
Hyperinsulinemia
Defective glucorecognition
Deterioration of b-cell function
b-cell failure
Saltiel AR, Olefsky JM. Diabetes. 1996;45:1661-1669.
From Insulin resistance to T2DM
Environment

Characteristics Type 1 Type 2
Other names IDDM(Insulin-Dependent
Diabetes Mellitus)
NIDDM(Non-insulin-
Dependent Diabetes Mellitus)
Age at onset Can occur in any age, but
usually diagnosed in children
and young adults
Usually >40 y/o, but increasing
prevalence among obese
children
% of diabetic 5%-10% 90%
Pancreatic
function
Usually none Insulin present in low, normal
or high amounts
Pathogenesis Islet cell Ab (autoimmune
destruction of the beta cells
of the pancreas)
Defect in insulin secretion;
tissue resistance to insulin;
↑hepatic glucose output
(gluconeogenesis)
Family history Not strongly relative Strongly relative
Obesity Uncommon Common (60-90%) 13
Type 1 and type 2 Diabetes

Characteristics Type 1 Type 2
Clinical
presentation
Moderate to severe
symptom
Mild polyuria, fatigue;
often diagnosed on routine
physical examination
Symptom 3Ps (polyuria, polydipsia, polyphagia) , weight loss, fatigue
Same as T1DM , blurred vision, frequent infections, trauma slow healing, numbness in the hands/feet
Ketoacidosis Often present Rare, except in
circumstances of unusual
stress (eg. Infection)
Microvascular/
Macrovascular
complication
No
Rare
Common
Common

Affects about 7% of all pregnancies (In the U.S.)
Defined as glucose intolerance that is first recognized
during pregnancy
Some will develop to T2DM or glucose intolerance
later in life
Might cause fetus’s brain progress
Diet, exercise, and/or insulin administration
15
Gestational Diabetes Mellitus (GDM)

Maternal age > 35 y/o
Family history of diabetes
Obesity : >20% IBW or BMI >27 kg/m2
History of GDM or polyhydramnios
Prior infant weight > 9 lb. at birth (macrosomia) or with congenital anomalies
16
Risk Factors for GDM

Genetic defect of b-cell
Maturity-Onset Diabetes of the Young (MODY)
Impaired insulin secretion
Minimal or no insulin resistance
Usually develop < 25 y/o
Genetic defect in insulin action
Disease of exocrine pancreas
Endocrinopathies
Drug or chemical-induce
Infections17
Other specific type

18
Plasma Glucose Status Meaning

19
Diagnosis of DM

20
Diagnose of GDM

Can DM be treated?
21

Type 1 DM Insulin
Diet
Physical activity
Amylin mimetic (ex. pramlintide)
Pancreas transplantation
Type 2 DM Diet
Physical activity
Antidiabetic agents
Insulin
Amylin mimetic22
Treatment

Physiology Reaction and Blood Sugar

Liver
Acts as the body’s glucose (or fuel) reservoir
Helps to keep circulating blood sugar levels
Both stores and manufactures glucose depending upon the body’s need
Blood sugar
Primarily dependent on the hormones insulin and glucagon
24
Liver & Blood Sugar

Glycogenolysis
Turns glycogen into glucose
Gluconeogenesis
Manufactures necessary sugar or glucose by harvesting amino acids, waste products and fat byproducts
25
Liver in Fasting State -1
http://www.deo.ucsf.edu/type2/understanding-diabetes/how-the-body-processes-sugar/the-liver-and-blood-sugar.html
25

Ketogenesis Begin is a low level of insulin
When sugar is in short supply, the liver also makes ketones, another fuel from fats
Burned as fuel by muscle and other body organs, while sugar is saved for the organs that need it
For the organs that always require sugar, including the brain, red blood cells and parts of the kidney
26
Liver in Fasting State -2
http://www.deo.ucsf.edu/type2/understanding-diabetes/how-the-body-processes-sugar/the-liver-and-blood-sugar.html
26

Accelerates transport of glucose from blood into cells Accelerates conversion of glucose into glycogen
(glycogenesis).
Accelerates transport of amino acids from blood into cells and increases rate of protein synthesis in the cells
Increases lipogenesis
Decreases glycogenolysis and gluconeogenesis
27
The role of insulin

Amylin
GLP-1 (glucagon-like peptide-1), GIP (glucose-dependent insulinotropic polypeptide)
Epinephrine, cortisol, and growth hormone
28
Other Hormones & Blood Sugar

Released along with insulin from beta cells
Reduce the production of sugar by the liver during a meal
Has much the same effect as GLP-1 Decreases glucagon levels
Slows the rate at which food empties from stomach
Make brain feel satisfying meal
29
Amylin
http://www.deo.ucsf.edu/type1/understanding-diabetes/how-the-body-processes-sugar/blood-sugar-and-other-hormones.html
29

Incretin hormones released from gut
Signal the beta cells to increase insulin secretion and decrease the alpha cells’ release of glucagon
GLP-1 also slows down the rate at which food empties from stomach, and makes the brain feel full and satisfied
For type 1 DM patients, having absent or malfunctioning beta cells, the releasing of GLP-1 during a meal cannot enhance insulin secretion
30
GLP-1 and GIP
http://www.deo.ucsf.edu/type1/understanding-diabetes/how-the-body-processes-sugar/blood-sugar-and-other-hormones.html
30

Along with glucagon
Called “stress” or “gluco-counter-regulatory” hormones, which make the blood sugar rise.
Enhance the production of glucose by the liver.
Counterbalance the effect of insulin .
31
Epinephrine, Cortisol, and Growth Hormone
http://www.deo.ucsf.edu/type1/understanding-diabetes/how-the-body-processes-sugar/blood-sugar-and-other-hormones.html
31

Treatment

DM Patient treatment goal
To ameliorate symptoms
Reduce the risk for microvascular and macrovascular disease complications
Improve life quality
Reduce mortality
33

34
ADA Goals for Adults with DM
Glycemic goals
A1c <6.5% (normal 4 %-6 %)
Preprandial plasma glucose 70-130 mg/dL (3.9-7.2 mmol/L)
Postprandial plasma glucose <180 mg/dL (<10 mmol/L)
Blood pressure <130/80 mmHg
Lipid
LDL <100 mg/dL (<2.6 mol/L)
TG <150 mg/dL (<1.7 mmol/L)
HDL-Men
-Women
>40 mg/dL (>1.1 mmol/L)
>50 mg/dL (>1.3 mmol/L)

Insulin Therapy

36
Proinsulin
Applied Therapeutics: The clinical use of drug, 2009, 9th Figure 50-3 Proinsulin.
Proinsulin=A chain+ B chain+ C chain(35 a.a)=86 a.a.Insulin=A chain(21 a.a.) + B chain(30 a.a.)

37
Properties of InsulinInsulin Brand Name Onset (hr) Peak (hr) Duration Appearance
Rapid acting
Lispro
Aspart
Glulisine
Inhaled
human insulin
Humalog
Novorapid
Apidra
5–25 min
15–30
min
30–90 min
1–2
<5hr
6hr
Clear
Powder
Short Acting
Regular Humulin R 0.5–1 2–3 5–8hr Clear
Intermediate Acting
NPH Humulin N 2–4 4–12 12–18hr Cloudy
Long Acting
Glargine
Detemir
Lantus
Levemir
1.5
3–8
No pronounced
peak
Relatively flat
20–24 hr
5.7–
23.2hr
Clear
Clear

38
Onset and Duration of Insulin
R.A. Harvey et al. Lippincott’s illustrated Reviews: Pharmacology 3rd ed., 2006 p 285

39
Combination Insulins
Type/Duration of Action Brand Name Manufacturer
NPH/regular mixture (70%/30%) Humulin 70/30
Novolin 70/30
Lilly
Novo Nordisk
NPH/regular mixture (50%/50%) Humulin 50/50 Lilly
Insulin aspart protamine/insulin aspart
mixture (70%/30%)NovoMix 30 Novo Nordisk
Insulin lispro protamine/insulin
lispro(75%/25%)Humalog Mix25 Lilly
Insulin lispro protamine /insulin
lispro mixture(50%/50%)
Humalog Mix
50/50Lilly

40
Insulin Injection
40

Hypoglycemia (tachycardia, sweating, blurred vision, hunger, tremulousness, confusion, vertigo and coma) <60 mg/dL-may or may not be symptomatic
<40 mg/dL-symptomatic <20 mg/dL-associated with seizure and coma Treatment of hypoglycemia
Oral administration of glucose or sugar 50% glucose solution (i.v.) Glucagon (i.m. or s.c)
Lipodystrophy Allergic reactions
41
Adverse Effect

Insulin pump
Continuous S.C. infusion by pump
Can program an extra dose of insulin at meals
Inhaled insulin
Taken before meals as an rapid-acting insulin, in conjunction with an injected basal insulin
Reduce number of daily injections required
The lower bioavailability
42
Other Preparations of Insulin

Restore near-normal glucose patterns throughout the day while minimizing the risk of hypoglycemia
Current regimens generally use intermediate- or long-acting insulin to provide basal coverage
Rapid- or short-acting insulin to meet the mealtime requirements
43
Aims of Insulin Therapy

44
Empiric Insulin Doses
Type 1 diabetes
Initial dose 0.3-0.5 Unit/kg
honey moon phase 0.2-0.5 Unit/kg
With ketosis, during illness,
during growth
1-1.5 Unit/kg
Type 2 diabetes
With insulin resistance 0.7-1.5 Unit/kg

Normal Early peak
Immediate release of stored insulin
Late phase Release of newly formed
insulin to normalize glycemia
Type 1 DM Almost no release
Type 2 DM Release slowly
45
Insulin Release
R.A. Harvey et al. Lippincott’s illustrated Reviews: Pharmacology 3rd ed., 2006 p 282.
45

Insulin Levels throughout the Day
http://www.deo.ucsf.edu/type1/understanding-diabetes/how-the-body-processes-sugar/controlling-blood-sugar.html
46
Low steady secretion of insulin
Overnight, fasting and between meals
Spikes of insulin
At mealtimes

Typical split-mixed regimen
Variation of A Regimen that
incorporates ultralenteor glargine insulin
Variation of C Continuous
subcutaneous insulin infusion
Multiple Daily Injection
47

Goals of Physiological (Basal-Bolus) Insulin Therapy
Monitoring
parameter
(mg/dL)
Adults School Age
(6–12 years)
Adolescent
s and young
adults(13-
29 years)
Pregnancy
Fasting 70-130 90-180 90-130 60-90
2 hr
postprandial
180 ≦120
2-4 AM >70 100-180 90-150 60
A1C 6.5% 8% 7.5% 5-6%
Urine
ketones
Absent to
rare
Absent to
rare
Absent to
rare
rare
48

49
Glysolated Hemoglobin ( A1c)
A1c Estimated Average
Glucose (mg/dL)
5% 97
6% 126
7% 154
8% 183
9% 212
10% 240
11% 269
12% 298
49

Oral Anti-diabetic Drugs Therapy(OHA)

Type 2 DM treatment of Oral Drugs classification
Insulin secretagogues Sulfonylureas
Non-sulfonylureas
(Meglitinides)
Insulin sensitizers Biguanides
Thiazolidinediones
(Glitazones)
Delaying carbohydrate absorption α – glycosidase antagonists
Gut hormones DPP- IV Inhibitiors
GIP , GLP-1 , Amylin analogs
51

Sulfonylureas
Pharmacology Enhance insulin secretion
Bind to sulfonylurea receptor(SUR) on pancreatic beta cells
Pharmacokinetics All sulfonylureas are metabolized by liver
CYP2C9 is involved with the hepatic metabolism of the majority of sulfonylureas
52

Sulfonylureas
Side effects Hypoglycemia alert(most common)
Hyponatremia (serum sodium<129mEq/L)
Weight gain
DDI(related to CYP2C9)
53

DrugDuration of biologic
effect, hUsual daily dose, mg Dosing per day
First-generation sulfonylureas
Acetohexamide 12 to 18 500 to 750 Once or divided
Chlorpropamide (Diabinese) 24 to 72 250 to 500 Once
Tolbutamide (Orinase) 14 to 16 1000 to 2000 Once or divided
Second-generation sulfonylureas
Glipizide 14 to 16 2.5 to 10 Once or divided
(Glucotrol)
(Glucotrol XL) 5 to 10 Once
Gliclazide 24 40 to 240 Once
(Diamicron R)
(Diamicron MR)
Glyburide (Glibenclamide) 20 to 24+ 2.5 to 10 Once
(Diabeta)
(Micronase)
(Glynase)
Glimepiride (Amaryl) 24+ 2 to 4 Once
Sulfonylureas
54

Meglitinides
Pharmacology Similar to sulfonylureas, it also enhance insulin secretion
Primarily used to target postpradial glycemia (because it is a short-acting insulin secretagogues)
Pharmacokinetics Rapidly absorbed(0.5 ~ 1 hr)and t1/2=1~1.5 hrs Nateglinide and Repaglinide can be metabolized by liver
or other pathways like renal or biliary
Side effects Hypoglycemia(lower) Similar risk for weight gain
55

Meglitinides
56

Biguanides
Pharmacology
Enhancement of insulin sensitivity
Metformin only
Pharmacokinetics
B.A.=50~60%
NOT METABOLIZED BY LIVER
Renal inffciency is contraindicated for metformin use
In men : serum creatinine ≥1.5mg/dL
In women : serum creatinine ≥ 1.4mg/dL
57

While comparison with sulfonylurea or insulin Reduce all-cause mortality
Reduce the risk of stroke
Reduce CV death
Side effects GI side effects(Diarrhea ,nausea/vomiting or flatulence )
Lactic acidosis(<1%)
Biguanides
58

Biguanides
Q: Only metformin ? What about Buformin(Bigunal) or Phenformin?
59

Thiazolidinedione(TZD or -glitazones)
Pharmacology
Bind to the peroxisome proliferator activator receptor-γ(PPAR-γ)
Enhance insulin sensitivity
Pharmacokinetics
Mainly metabolized by liver
Side effect
Weight gain
Water remain - induce CV risk60

Progress slowly
Liver toxicity of Troglitazone
Patient
Should not start if ALT> 2.5times ULN
DC if ALT> 3 times ULN
Thiazolidinedione(TZD or -glitazones)
61

Not suggest for understatement Ischemic heart diease
CHF(Contraindication for Class III & IV)
#目前此類藥物不可做為第一線用藥, 而使用Avandia前須簽同意書。
Thiazolidinedione(TZD or -glitazones)
62

α-Glucosidase inhibitor
Pharmacology Competitive inhibit starch and di-saccharides metabolism,
cause glucose intake decrease
Acarbose & Miglitol
Pharmacokinetics Work on intestine
Commonly use for after-meal plasma glucose control (take with meals)
Side effects GI discomfort (bloating, diarrhea…)
63

α-Glucosidase inhibitor
64

DPP-IV inhibitor
Pharmacology 能阻止內生性的GLP-1遭分解
GLP-1具有降低血糖、刺激胰島素分泌、抑制升糖素分泌的作用
Pharmacokinetics Sitagliptin 做成水溶性磷酸鹽,Oral B.A.可達87%,
Protein binding達38%,t1/2約12hrs
另外還有Saxagliptin (新藥,是Januvia 2-3倍強度) 為DPP-IV 抑制劑,也可以使GLP-1濃度上升
65

DPP-IV inhibitor
66

Pharmacology Exendin-4可與GLP-1 receptor結合,產生擬似血糖素樣胜肽作用
(GLP-1 mimetic effect)
合成的Exendin-4稱為Exenatide (Byetta)
Pharmacokinetics 體內被DPP-IV 水解,S.C.後t1/2約2-4hrs
Side effects
Nausea and vomiting, diarrhea,headache, dizziness
GLP-1 agonists
#通常用在飯後皮下注射給藥,控制Type 2 DM67

Pharmacology 是Amylin 的合成類似物,減少升糖素(glucagon)的釋出反應,可皮下注射調節飯後血糖的濃度
可活化中樞系統之Amylin受體,因此能使糖化血色素減少及降低飯後葡萄糖的濃度
Pharmacokinetics 體內約20 min達 Peak concentration, t1/2約0.5hrs ,主要由腎排除
Side effects Nausea and vomiting, hypoglycemia
Amylin agonists
#通常用在飯前皮下注射給藥,治療Type 1與2 DM 68

Total Data
69

糖尿病二型 guildline
70 70 XD

Case Report

Mr. Li 61y/o 169.3 cm 58.2 kg BMI:20.305
DOA:2011-02-08 DOD:2011-02-24
Section:META
Chief complaint: Syncope last afternoon, denied fever, alcohol, head injury ;
conscious clear at ER
History of present illness : Type 2 Diabetes Mellitus 40+, under OADs and Levemir control,
but poor compliance
72
Case report-1

Past medical history:
status post debridement and full thickness skin graft
Perforated peptic ulcer s/p subtotal gastrectomy + gastrojejunostomy 30+ yrs ago
Hypertension
Vitreous Hemorrhage OD
73
Case report-2

Personal history
Alcohol : nil
Smoking : nil
Drugs allergy : nil
Family history:
DM
HTN
74
Case report-3

Vital signs:T/P/R:35/103/20,BP:131/ 77 mmHg Lab data :
EKG showed sinus rhythm Ccr=(140-age)*Wt(kg)/Serum creatinine creatinine *72
=43.73858….中度慢性腎病75
Emergency Department Course
Hgb12-15
NA 135-147
K 3.4-4.7
free Ca2+ 0.9-1.5
BUN7-20
9.9 g/dL
134 mmol/L
4.1 mmol/L 1.03 mmol/L
24 mg/dl
Cr0.5-1.5
GLU65-115
CK/MB/TnI24-168/-/0-0.05(AMI>1.5)
CRP0-0.05
1.46mg/dl
492 mg/dl
75/-/0.04 0.13mg/dl

Drug Profile

77
2007-2011年用藥紀錄
2007.4.21
• Amaryl tab 2 mg BID
• Glucophage tab 500 mg BIDCC
2007.11.10
•Amaryl tab 2 mg BID•Glucophage tab 500 mg BIDCC•Insulatard HM 100 iu/Ml HS
2008.1.28
•Amaryl tab 2 mg BID
•Glucophage tab 500 mg BIDCC
•Lantus inj 100 iu/Ml QD
2008.5.19
• Glucophage tab 850 mg BIDCC
• Lantus inj 100 iu/Ml QD
2009.1..13
• Humulin-R 100 iu/mL
• Glucophage tab 850 mg
• Lantus pen 100 iu/mL

78
2007-2011年用藥紀錄(續)
2009.12.16
• Glucophage tab 850 mg BIDCC
• Lantus pen 100 iu/Ml QD
2010.5.14
• Mixtard 30 inj 100 iu/mL
2011.1.21
• Starlix FC tab 120 mg
• Levemir flexpen 100 io/mL
• glucophage tab 500 mg
2011.2.24
• Humulin-N 100 iu/mL
• Novorapid penfil 100 u/3L
點我>0<

商品名/學名/含量/劑型日期+頻次/
途徑2/8 2/9 2/10 2/11 2/12 2/13 2/14 2/15 2/16 2/20 2/22 2/24
2011/3/9(出院)
Co-Diovan(Valsartan +
Hydrochlorothiazide) FC tab 80/12.5 mg
QD/PO
Norvasc(Amlodipine) tab 5 mg
QD /PO
Starlix(Nateglinide) FC tab 120 mg
QD-BL*#1QD-BD*#1
QD-BBF*#0.5/P
OGlucophage tab 500
mgBIDCC /PO
Humulin-R inj 100iu/ml 1iu (UD
QD-BBFQD-BL
QD-BD /SC
Humulin-N inj 100iu/ml 1iu (UD
HS /SC ST ST
Novorapid penfill 100 u/ml 3ml
TIDAC /SC ST ST ST
Levemir flexpen 100 iu/ml 3ml
QD-INSL /SC
HS
Ferrum hausmann chewa.tab 100 mg
QD /PO
Chloramphenicol oph sol0.25% 10ml
QID /OU
STST
ST ST
STSTST
HS

Discussion-1

81
近兩年空腹血糖v.s.糖化血色素值

82
2/8-2/24住院期間血糖值
橫軸:日期 縱軸:血糖值
0
100
200
300
400
500
600
日期
2011
/2/9 2
1:36
2011
/2/11
06:3
7
2011
/2/12
15:1
8
2011
/2/13
22:0
2
2011
/2/15
06:1
5
2011
/2/16
06:4
8
2011
/2/17
10:2
0
2011
/2/18
15:2
5
2011
/2/19
22:2
6
2011
/2/20
22:5
5
2011
/2/21
21:5
3
2011
/2/22
21:5
8
2011
/2/24
06:5
4
血糖值
線性 (血糖值)

What causes bad PG controll ?
1.Irregular meals(dessertsor something else)
2.Medication Compliance (which influences glucose)
3.Hypersensitivity for medication(Caused hypoglycemia)
4.Individual tolerance(feeling of SMBG)
5.Worsing of DM

Discussion-2

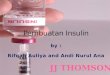
FIGURE 24-32 Long-term complications of diabetes85
Complication

Patient’s Complication
Macrovascular Skin necrosis over the lower leg ulcer over the big toe
Microvascular Had been a sudden blurred vision (HYPERTENSIVE
RETINOPATHY , CRVO, NIDDM RETINOPATHY)
86

From HA1C Control to Retinopathy
87

Complication Treatment
Macrovascular Skin necrosis over the lower leg
STSG Neomycin Ointment 0.5% Augmentin tab 375 mg Betadine sol 10% 100 ml
ulcer over the big toe FTSG
Microvascular Had been a sudden blurred vision
Trental tab 100 mg Transamin cap 250 mg Fluorometholone Oasis oph sol
88

From DM to Nephropathy
89

I GOT PROTEINURIA !!
90 90

DM comes, Dyslipidemia follows
91

Screening Test
Glucose monitor : Once half year (HbA1c)
Cardiac vascular health:
Check blood pressure daily
Check plasma lipid
Eye : Check once in two years
Kidney : Check micro proteinuria annually
Peripheral perfusion : Foot exam at least once a year
92

Prevention complication
Diet
Exercise
Not smoking
Taking a low-dose aspirin every day if indicated (for adults only)
Proper and exact medications
Monitoring goals
Avoid getting trauma
93

Discussion-3

Control diet amount Avoid high caloric foods such as organs, crab egg, fish egg
Egg yolk control under three per week
Quit sugar
Cut oil Use vegetable oil while cooking.
Choose steam, water boil mostly to cook your food
Decrease salt intake
DM patient diet formula-casual time
95

Calorie 30-35 cal/Kg/day, equals to 2 slice of toast, or a bottle of coke
45% to 65% of daily caloric intake carbohydrates
Protein Insignificant Proteinuria, daily protein 0.8-1.0 g/Kg/day
Significant Proteinuria, daily protein 0.8/Kg/day
Study show protein can improve DM p’t PG control
Glycemic control Does not recommend restricting diets to <130 grams of
carbohydrate a day
96
DM patient diet formula - while ill

Aerobic exercise Improves insulin resistance and glycemic control
Reduces cardiovascular risk factors
Weight maintenance
Improves well-being
Physical activity goals At least 150 minutes/week of moderate intensity exercise
Exercise
97

Light exercise Patient had surgery on his leg, suggest exercise which need not
too much walking, such as swimming
Wear elastic socks
Warm feet bath
Increase protein in take Patient has miner kidney problem
Patient doesn’t take enough protein at home
Patient show terrible PG control
Keep candies at hand98
Suggesting health care for patient

Applied Therapeutics: The clinical use of drug
Pharmacotherapy: a pathophysiologic approach
http://www.deo.ucsf.edu/index.html
Up to date
國民健康局
行政院衛生署全民健康保險醫療品質資訊公開網(DM)
行政院衛生署
全民糖尿病觀測站
99
Reference

100
Thanks for your attention