Embed Size (px)
Citation preview

Bhutan 2017
FACT SHEET
Expanded Programme on Immunization (EPI)

Acronyms
AD Auto disable
AEFI Adverse events following immunization
AFP Acute flaccid paralysis
BCG Bacillus Calmette-Guérin vaccine
CES Coverage evaluation survey
cMYP Comprehensive multi-year plan
CRS Congenital rubella syndrome
DHS Demographic health survey
DT Diphtheria tetanus toxoid, pediatric
DTP Diphtheria – tetanus – pertussis vaccine
DTP-Hib-HepB Pentavalent vaccine
DTP-Hib-HepB3 3rd dose pentavalent vaccine
EPI Expanded programme on immunization
GDP Gross domestic product
HCW Health care worker
HepB Hepatitis B vaccine
Hib Haemophilus influenzae type b
HPV Human papilloma virus
IgM Immunoglobulin M
IPV Inactivated poliovirus vaccine
JE Japanese encephalitis
JE_Live-Atd JE live attenuated vaccine
JRF WHO UNICEF joint reporting form
LB Live birth
M Measles
MCV1 First dose measles containing vaccine
MCV2 Second dose measles containing vaccine
MICS Multiple indicator cluster survey
MMR Measles mumps rubella vaccine
MNT Maternal and neonatal tetanus
MR Measles rubella vaccine
NCIP National committee on immunization practices
NID National immunization day
NTAGI National technical advisory group on immunization
NPEV Non-polio enterovirus
NT Neonatal tetanus
OPV Oral poliovirus vaccine
bOPV Bivalent OPV
tOPV Trivalent OPV
PCV Pneumococcal conjugate vaccine
SEAR WHO South-East Asia Region
SIA Supplementary immunization activities
SNID Subnational immunization day
Td Tetanus diphtheria toxoid; older children, adults
TT Tetanus toxoid
TT2+ 2 or more doses TT
VDPV Vaccine derived poliovirus
VPD Vaccine preventable diseases
WCBA Women of child bearing age
WPV Wild poliovirus
Contents
Impact of routine immunization Page No.
EPI history 5
Basic information 2016 Table 1 5
Immunization schedule 2016 Table 2 5
National immunization coverage 1980 - 2016 Figure 1 6
Immunization system highlights Table 3 6
DTP3 coverage, diphtheria and pertussis cases 1980 - 2016 Figure 2 7
Reported cases of vaccine preventable diseases 2011 - 2016 Table 4 7
DTP-Hib-HepB3 coverage by district 2015 Figure 3 7
DTP-Hib-HepB3 coverage by district 2016 Figure 4 7
Towards measles elimination and rubella/congenital rubella syndrome control
Page No.
MCV1 and MCV2 coverage, measles and rubella cases, 1980-2016 Figure 10 11
MCV supplementary immunization activities Table 7 11
MCV1 coverage by district 2015 Figure 11 12
MCV1 coverage by district 2016 Figure 12 12
MCV2 coverage by district 2015 Figure 13 12
MCV1 coverage by district 2016 Figure 14 12
Immunity against measles – immunity profile by age in 2016 Figure 15 12
Subnational risk assessment for measles and rubella Figure 16 12
Sporadic and outbreak associated measles cases by month 2011 - 2016 Figure 17 13
Immunization status of confirmed (laboratory and Epi linked) measles outbreak associated cases by age 2011 – 2016 Figure 18 13
Quality of field and laboratory surveillance for measles and rubella 2012 - 2016 Table 8 14
Performance of laboratory surveillance 2012 - 2016 Table 9 14
WHO supported laboratory network for VPD surveillance Figure 19 15
Maternal and neonatal tetanus elimination is sustained Page No.
TT2+ coverage and NT cases 1980 - 2016 Figure 5 8
Polio-free status is maintained Page No.
AFP surveillance indicators 2011 - 2016 Table 5 9
Non-polio AFP rate by district 2015 Figure 6 9
Non-polio AFP rate by district 2016 Figure 7 9
Adequate stool specimen collection percentage by district 2015 Figure 8 10
Adequate stool specimen collection percentage by district 2016 Figure 9 10
OPV supplementary immunization activities Table 6 10

WHO South-East Asia Region
Disclaimer: The boundaries and names shown and the designations used on all the maps do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area of its authorities, or concerning the delimitation of its frontiers or boundaries.
Bhutan: district level map
4

EPI history
• EPI launched on 15 November 1979
• TT for pregnant women introduced in 1983
• HepB vaccine introduced in 1997
• DTP-HepB vaccine introduced in 2003
• AD syringes introduced in 2003
• MR vaccine introduced in 2006
• DTP-Hib-HepB vaccine introduced in 2009
• HPV vaccine introduced in 2010
• HepB birth dose introduced in 2012
• TT vaccine replaced by Td vaccine in 2012
• IPV vaccine introduced in 2015
• tOPV to bOPV switched on 25 April 2016
• MMR vaccine introduced in October 2016.
Source: cMYP 2014-2018 and VPDP/MOH
Table 1: Basic information1 2016
Total population 757,042
Live births 12,869
Children <1 year 11,227
Children <5 years 82,561
Children <15 years 229,796
Pregnant women 11,680
WCBA (15-49 years) 186,509
Neonatal mortality rate 18.3 (per 1,000 LB)
Infant mortality rate2 27.2 (per 1,000 LB)
Under-five mortality rate 32.9 (per 1,000 LB)
Maternal mortality ratio2 148 (per 100,000 LB)
1SEAR annual EPI reporting form, 2016 and WHO, World Health Statistics 20162VPDP/MOH
Division/Province/State/Region -
Dzongkhag/District 20
Gewog/Block 205
Sub-block/Ward 1,050
Village (approx.) 3,717
Population density (per sq. km) 18
Population living in urban areas 37%
Population using improved drinking-water sources2
97.7%
Population using improved sanitation2 66.3%
Total expenditure on health as % of GDP 3.6%
Births attended by skilled health personnel2
74.6%
Neonates protected at birth against NT 83%
Table 2: Immunization schedule, 2016
Vaccine Age of administration
BCG Birth
HepB Birth
OPV Birth, 6 weeks, 10 weeks and 14 weeks
DTP-Hib-HepB 6 weeks, 10 weeks and 14 weeks
IPV 14 weeks
MMR 9 months and 24 months
DTP 24 months
HPV Females 12 years and grade VI girls
Td 6 and 12 years
Vitamin A 6 to 30 months (6 months interval)Source: WHO/UNICEF JRF,, 2016
Impact of routine immunization
5

Table 3: Immunization system highlights
cMYP for immunization 2014-2018
NTAGI fully functional
Spending on vaccines financed by the government 41%
Spending on routine immunization programme financed by the government 24%
Updated micro-plans that include activities to improve immunization coverage 20 districts (100%)
National policy for health care waste management including waste from immunization activities in place
National system to monitor AEFI in place
Most recent EPI CES National Health Survey 2012
>80% coverage for DTP-Hib-HepB3 20 districts (100%)
>90% coverage for MCV1 16 districts (80%)
>10% drop-out rate for DTP-Hib-HepB1 to DTP-Hib-HepB3 1 district (5%)
Source: WHO/UNICEF JRF, 2016
Figure 1: National immunization coverage, 1980-2016
% C
over
age
0
20
40
60
80
100
Source: WHO/UNICEF estimates of national immunization coverage, July 2017 revision
1980 1985 1990 1995 2000 2005 2010 2014 2015 2016BCG 43 54 99 98 97 92 96 99 99 99DTP3 6 41 96 87 92 95 91 99 99 98OPV 4 41 96 86 98 95 92 98 98 97MCV1 21 44 93 85 78 93 95 97 97 97
6

Figure 3: 2015
Figure 4: 2016
Source: SEAR annual EPI reporting form, 2016 (administrative data)
Source: SEAR annual EPI reporting form, 2015 (administrative data)
Figure 2: DTP3 coverage1, diphtheria and pertussis cases2, 1980-2016
Year
Diphtheria Cases Pertussis Cases DTP3 Coverage
% C
over
age
No.
of c
ases
201620152014201320122011201020052000199519901980 1985
464
0
20
40
60
80
100
0
50
100
150
200
250
300
1WHO/UNICEF estimates of national immunization coverage, July 2017 revision 2WHO vaccine-preventable diseases: monitoring system 2016
Table 4: Reported cases of vaccine preventable diseases, 2011-2016
Year Polio Diphtheria Pertussis NT(% of all tetanus) Measles Rubella Mumps JE CRS
2011 0 0 0 0 10 3 262 3 ND
2012 0 0 0 0 1 2 198 0 0
2013 0 0 0 0 0 6 20 0 0
2014 0 0 0 0 0 0 206 2 0
2015 0 0 12 0 11 1 620 5 0
2016 0 0 4 0 45 3 795 5 0
Source: WHO/UNICEF JRF, (multiple years) ND=No data
DTP-Hib-HepB3 coverage by district
<70% 70% - 79% 80% - 89% > 90%
7
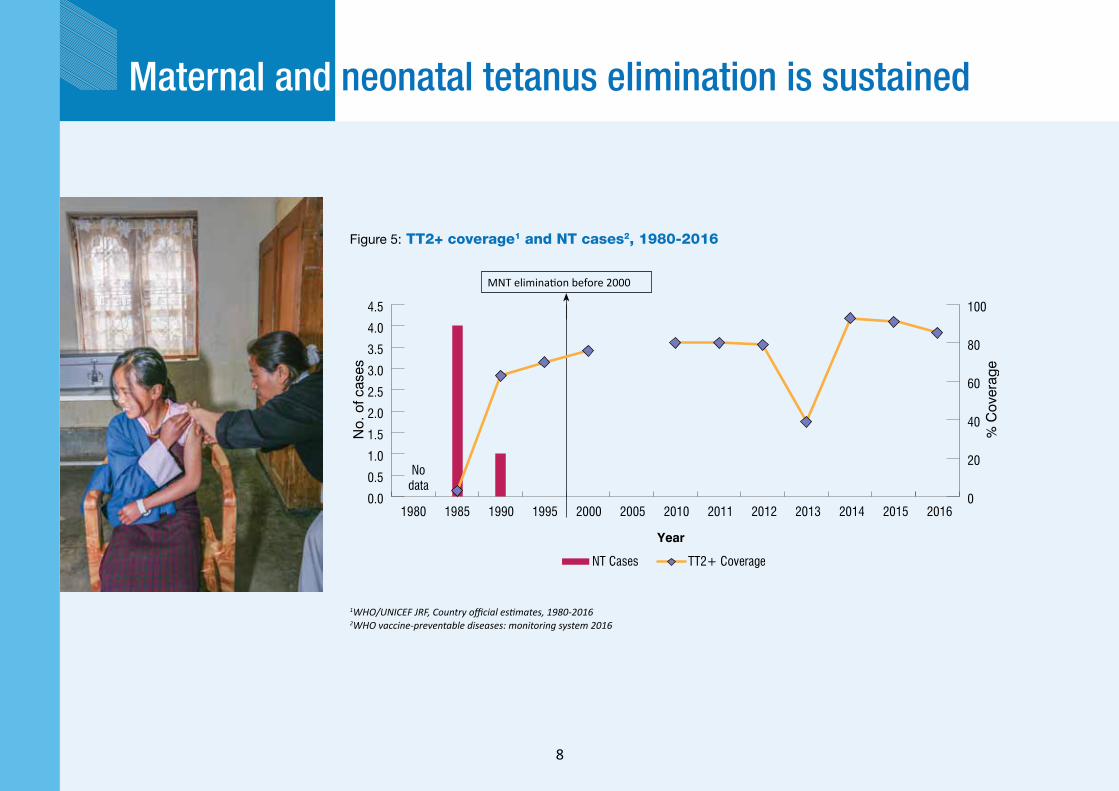
Figure 5: TT2+ coverage1 and NT cases2, 1980-2016
1WHO/UNICEF JRF, Country official estimates, 1980-20162WHO vaccine-preventable diseases: monitoring system 2016
Maternal and neonatal tetanus elimination is sustained
1980 1985 1990 1995 2000 2005 2010 2011 2012 2013 2014 2015 2016
% C
over
age
No.
of c
ases
Year
NT Cases TT2+ Coverage
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
0
20
40
60
80
100
No data
MNT elimination before 2000
8

Table 5: AFP surveillance performance indicators, 2011-2016
Indicator 2011 2012 2013 2014 2015 2016
AFP cases 6 10 10 11 9 11
Wild poliovirus confirmed cases 0 0 0 0 0 0
Compatible cases 0 0 0 0 0 0
Non-polio AFP rate1 2.74 5.14 4.52 4.84 4.18 5.11
Adequate stool specimen collection percentage2 83% 70% 80% 73% 67% 73%
Total stool samples collected 7 21 11 22 16 20
% NPEV isolation 0 0 0 9 0 0
% Timeliness of primary result reported3 71 100 100 100 100 1001Number of discarded AFP cases per 100,000 children under 15 years of age.2Percent with 2 specimens, at least 24 hours apart and within 14 days of paralysis onset.3Results reported within 14 days of sample received at laboratory.
Figure 6: 2015 Figure 7: 2016
Polio-free status is maintained
Last clinically-confirmed polio case was reported in 1986.
Non-polio AFP rate by district
<1 1 – 1.99
>2 No non-polio AFP case
© WHO/Bhutan/S Bahadur
9

Table 6: OPV SIAs
Year Vaccine Geographic coverage Target age
Target population Coverage (%)
Round 1 Round 2 Round 1 Round 2
1995 OPV NID <5 years 80,336 99 100
1996-1997 OPV SNID <5 years 37,107 100 100
1997-1998 OPV SNID <5 years 37,465 100 100
1998-1999 OPV SNID <5 years 36,006 100 100
1999-2000 OPV SNID <5 years 36,541 100 100
2000-2001 OPV SNID <5 years 38,604 100 100
2001 OPV SNID <5 years 36,753 100 100
2002 OPV SNID <5 years 37,665 96 100
Source: WHO/UNICEF JRF, (multiple years)
Figure 9: 2016Figure 8: 2015
Adequate stool specimen collection % by district
<60% 60% - 79%
>80% No AFP
10
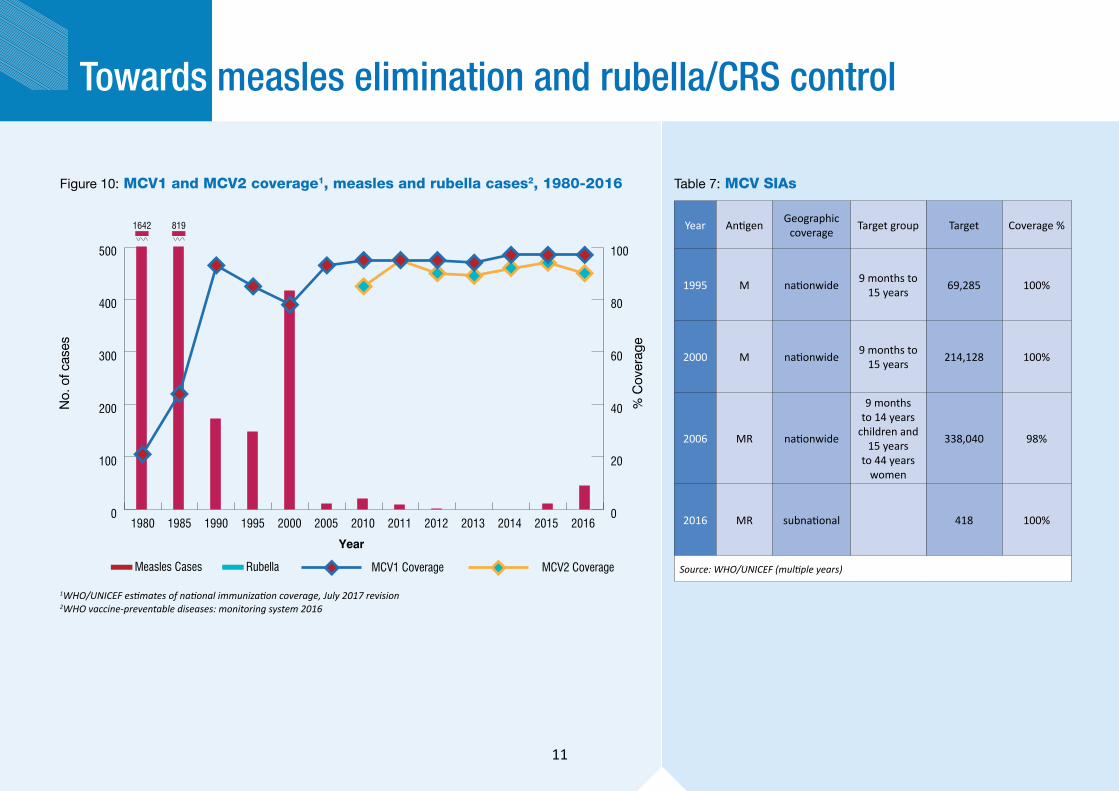
Towards measles elimination and rubella/CRS control
Figure 10: MCV1 and MCV2 coverage1, measles and rubella cases2, 1980-2016
Measles Cases Rubella MCV1 Coverage MCV2 Coverage
2016201520142013201220112010200520001995199019851980
1642 819
% C
over
age
No.
of c
ases
Year
0
100
200
300
400
500
0
20
40
60
80
100
1WHO/UNICEF estimates of national immunization coverage, July 2017 revision 2WHO vaccine-preventable diseases: monitoring system 2016
Table 7: MCV SIAs
Year Antigen Geographic coverage Target group Target Coverage %
1995 M nationwide 9 months to 15 years 69,285 100%
2000 M nationwide 9 months to 15 years 214,128 100%
2006 MR nationwide
9 months to 14 years
children and 15 years
to 44 years women
338,040 98%
2016 MR subnational 418 100%
Source: WHO/UNICEF (multiple years)
11

0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
Per
cent
of p
opul
atio
n
Age (in years)Protected by maternal antibodies Protected by routine vaccination with 1st doseProtected by routine vaccination with 2nd dose Protected by SIAsImmune due to past infection Susceptible
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Figure 15: Immunity against measles - immunity profile by age in 2016
* Modeled using MSP tool ver 2 assuming the schedule and MCV coverage remain unchanged and no SIAs between 2009 & 2016.
<80% 80% - 89% 90% - 94% >95%
Figure 12: 2016 Figure 13: 2015 Figure 14: 2016
Source: SEAR annual EPI reporting form, 2016 (administrative data)
Source: SEAR annual EPI reporting form, 2016 (administrative data)
Figure 11: 2015
Source: SEAR annual EPI reporting form, 2015 (administrative data)
Source: SEAR annual EPI reporting form, 2015 (administrative data)
Figure 16: Sub-national risk assessment - measles and rubella
MCV1 coverage by district MCV2 coverage by district
Source: developed using WHO risk assessment tool based on JRF & ARF data base
Very high riskHigh riskMedium riskLow riskNot available
12
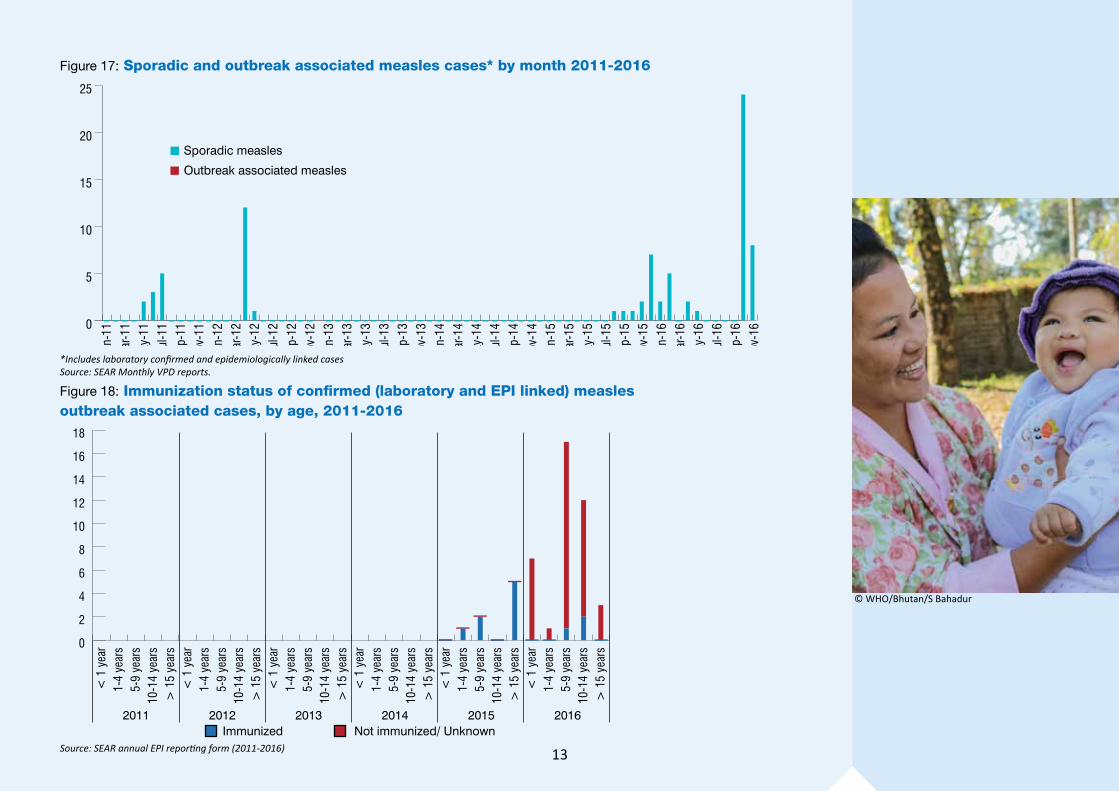
Figure 17: Sporadic and outbreak associated measles cases* by month 2011-2016
Nov-
16Se
p-16
Jul-1
6M
ay-1
6M
ar-1
6Ja
n-16
Nov-
15Se
p-15
Jul-1
5M
ay-1
5M
ar-1
5Ja
n-15
Nov-
14Se
p-14
Jul-1
4M
ay-1
4M
ar-1
4Ja
n-14
Nov-
13Se
p-13
Jul-1
3M
ay-1
3M
ar-1
3Ja
n-13
Nov-
12Se
p-12
Jul-1
2M
ay-1
2M
ar-1
2Ja
n-12
Nov-
11Se
p-11
Jul-1
1M
ay-1
1M
ar-1
1Ja
n-11
Sporadic measles
Outbreak associated measles
0
5
10
15
20
25
*Includes laboratory confirmed and epidemiologically linked casesSource: SEAR Monthly VPD reports.
Figure 18: Immunization status of confirmed (laboratory and EPI linked) measles outbreak associated cases, by age, 2011-2016
> 1
5 ye
ars
10-1
4 ye
ars
5-9
year
s1-
4 ye
ars
< 1
yea
r>
15
year
s10
-14
year
s5-
9 ye
ars
1-4
year
s<
1 y
ear
> 1
5 ye
ars
10-1
4 ye
ars
5-9
year
s1-
4 ye
ars
< 1
yea
r>
15
year
s10
-14
year
s5-
9 ye
ars
1-4
year
s<
1 y
ear
> 1
5 ye
ars
10-1
4 ye
ars
5-9
year
s1-
4 ye
ars
< 1
yea
r>
15
year
s10
-14
year
s5-
9 ye
ars
1-4
year
s<
1 y
ear
2011 2012 2013 2014 2015 2016Immunized Not immunized/ Unknown
0
2
4
6
8
10
12
14
16
18
Source: SEAR annual EPI reporting form (2011-2016)
© WHO/Bhutan/S Bahadur
13

Table 8: Surveillance performance indicators for measles and rubella, 2012-2016
Year
No.
of s
uspe
cted
mea
sles
Case classification (number) Indicators
Measles Rubella
Disc
arde
d no
n-m
easle
s no
n-ru
bella
cas
es
Annu
al in
cide
nce
of
confi
rmed
mea
sles c
ases
per
m
illio
n to
tal p
opul
ation
Annu
al in
cide
nce
of
confi
rmed
rube
lla c
ases
per
m
illio
n to
tal p
opul
ation
Prop
ortio
n of
all
susp
ecte
d m
easle
s and
rube
lla c
ases
th
at h
ave
had
an a
dequ
ate
inve
stiga
tion
initi
ated
with
in
48 h
ours
of n
otific
ation
Disc
arde
d no
n-m
easle
s no
n-ru
bella
inci
denc
e pe
r 10
0,00
0 to
tal p
opul
ation
Prop
ortio
n of
dist
ricts
re
porti
ng a
t lea
st tw
o di
scar
ded
non-
mea
sles
non-
rube
lla c
ases
per
10
0,00
0 to
tal p
opul
ation
Prop
ortio
n of
sub-
natio
nal
surv
eilla
nce
units
repo
rting
to
the
natio
nal l
evel
on
time
Lab-
confi
rmed
EPI-l
inke
d
Clin
ical
ly-c
onfir
med
Lab-
confi
rmed
EPI-l
inke
d
Target ➔ - - 80% 2 80% 80%
2012 82 1 0 0 2 0 80 0.7 1.4 0 11.4 ND ND
2013 99 0 0 0 6 0 93 0 4.2 0 13.3 ND ND
2014 69 0 0 0 4 0 65 0 2.8 0 9.3 ND ND
2015 120 11 0 0 1 0 108 16 0.13 0 0 0 0
2016 146 45 ND ND 3 ND 106 53 4 ND 14 ND NDSource: SEAR annual EPI reporting form, 2011-2016 ND=No data
Year
Seru
m sp
ecim
en
colle
cted
from
su
spec
ted
mea
sles c
ases
Seru
m sp
ecim
en
rece
ived
in
labo
rato
ry
with
in 5
day
s of
colle
ction
Spec
imen
po
sitive
for
mea
sles I
gM
Spec
imen
po
sitive
for
rube
lla Ig
M
% R
esul
ts w
ithin
4
days
of r
ecei
pt
% P
ositi
ve c
ases
te
sted
for v
iral
dete
ction
Geno
type
s de
tect
ed
No (%) No (%) No. % No. % Measles Rubella
2012 82 (100) 50 (81) 1 1% 2 2% 37 0 - -
2013 99 (100) 57 (69) 0 0% 6 6% 52 0 - -
2014 69 (100) 30 (43) 0 0% 4 6% 100 0 - -
2015 120 (100) 120 (100) 11 9% 1 1% 100 0 - -
2016 146 (100) 146 (100) 40 27% 3 2% ND ND ND NDSource: SEAR annual EPI reporting form, 2012-2016 ND=No data
Table 9: Performance of laboratory surveillance, 2012-2016
14
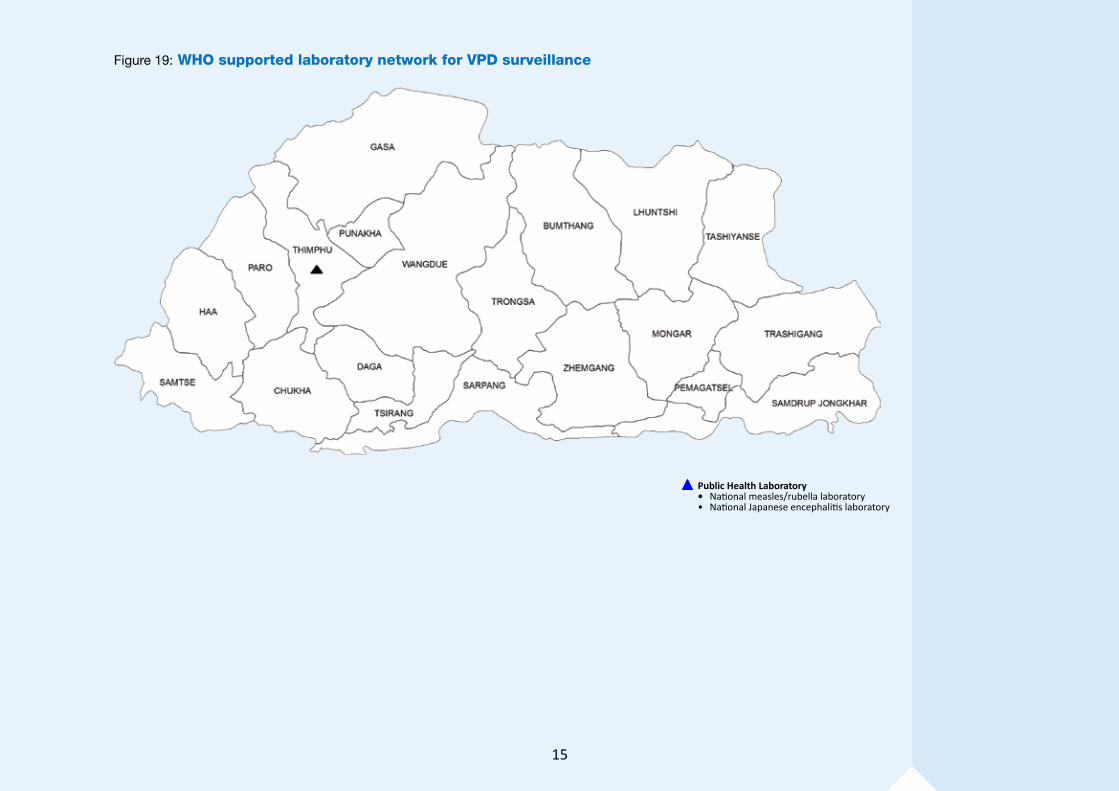
Figure 19: WHO supported laboratory network for VPD surveillance
Public Health Laboratory• National measles/rubella laboratory• National Japanese encephalitis laboratory
15

For contact or feedback:Expanded Programme on ImmunizationMinistry of Health, Thimphu, BhutanTel: +975-2-332296, Fax: +975-2-332296Email: [email protected]
Immunization and Vaccine Development (IVD)WHO-SEARO, IP Estate, MG Marg, New Delhi 110002, IndiaTel: +91 11 23370804, Fax: +91 11 23370251Email: [email protected]/entity/immunization