Embed Size (px)
Citation preview


Cervical teratomaMediastinal teratomaLymphangiomaGoiterThyroid cystsThyroglosal duct cystBranchial cleft cystNeuroblastomaHamartomaHemangiomaLipomaParotid tumorCervical MMCEpignathus
Fetal Neck and Chest LesionsExtrinsic Compression

Fetal Neck MassesCervical Teratomas•All 3 germ layers represented•Totipotential germ cells vs conjoined twin•40% contain thyroid tissue•Large bulky tumors•Airway compromise•Polyhydramnios in 40%•Benign lymph node metastases•Thyroid destruction•Parathyroid engulfment•Mandibular hypoplasia•Marginal mandibular nerve palsy•Laryngotracheomalacia

Fetal Neck Masses
•No matter the etiology•Very large masses can cause:
•Neck hyperextension•Pulmonary hypoplasia•Secondary to carina pulled into neck•Lungs pulled into apex of hemithorax

The EXIT ProcedureThe EXIT ProcedureAirway Algorithm
•Direct laryngoscopy•Flexible bronchoscopy•Rigid bronchoscopy•Tracheotomy with retrograde intubation•Tracheostomy•Mass resection + tracheostomy•TRI-EXIT

Establishing an airway
Laryngoscopy Bronchoscopy

Tracheostomy

Resection

Congenital High Airway Obstruction Syndrome
USMRI
Prenatal DiagnosisOften misdiagnosedBilateral CCAMsBilateral extremely large echogenic lungsCompressed heart and mediastinumNon‐immune hydropsComplete airway obstruction

CHAOS
Intrinsic Airway Obstruction•Laryngeal atresia/stenosis•Tracheal atresia/stenosis•Laryngeal cyst
Prenatal Natural History• 2/3 Hydrops and IUFD• 1/3 Resolution of hydrops
•Laryngeal fistula•Tracheoesophageal fistula

CHAOS
• Diagnosed with bilateral CCAMs• Dilated tracheobronchial tree• Massively enlarged lungs• Inverted and stretched
diaphragms• Non-immune hydrops• Massive Ascites• Complete airway obstruction
CHAOS

CHAOS
CHAOS

Fetal Lamb Model of CHAOS
•Fetal tracheal occlusion at mid‐gestation•Non‐immune hydrops•Massive ascites•Massively enlarged lungs•Inverted stretched diaphragms
•Dilated tracheobronchial tree
•Release of tracheal occlusion•Resolution of hydrops•Normal at delivery

CHAOS

CHAOS
Profound capillary leak syndromeSevere RDSHepatic synthetic defectDiaphragmatic paralysis
Stretch injuryHyper‐compliant lungsAscites‐behave like cirrhoticGut disfunctionPrune bellyIntact larynxSubglottic trecheal atresia

Tracheal Reconstruction for CHAOS

Laryngo-Tracheoplasty

- Definition of natural history
- Shunts
- Open fetal surgery
- SteroidsCCAM
Fetal MRI

• CPAM Volume Ratio (CVR)
- 3 dimensions volume of lesion /Head circumference
- CVR= .52 x L x W x HHC
- >1.6 high risk hydrops
Saggital
Transverse

• Fastest rate of growth 20- 25 weeks• Plateau at 26 weeks
Range 24-28 weeks• No growth once plateau reached• CAM volume lagged behind CVR

• Low risk CPAM - Excellent survival (98%)• High risk CPAM n=42− Lower survival(71.4%)
• Excellent survival in non-hydropic high risk CPAM treated with steroid (100%)
• Hydropic CPAM treated with steroids- Survival 45% compared to 0% in
historical controls- 88.9% survival with resolution of
hydrops- Persistent of hydrops predicts
mortality
8 weeks
post steroid


Fetal Pericardial Teratoma
• Rare benign congenital tumor• 40 prenatally diagnosed cases• 2:1 female to male ratio• Often associated pericardial effusion
• Rapid growth between 20-30 wks• 50% develop hydrops• Polyhydramnios common• Fatal in setting of hydrops/poly• Fetal Therapy
• Pericardiocentesis• Fetal surgery

Fetal Pericardial Teratoma
Open Pericardium to expose Teratoma

Fetal Pericardial TeratomaResection/repair complete

CFCC
Improved Survival and Decreased Need for ECMO in CDH
Pre‐CDH Team CDH Team CDH Team & FCC
Liver 33 56%Patch 33 67%
CHCOCDH Team

LHRRight Lung Area/Head
Circumference
UCSF AP Method
Longest Methods
Tracing Methods

Observed to Expected LHRSurvival with Conventional Postnatal Therapy
DePrest et al, Seminars Fetal and Neonatal Medicine 2008

Congenital Diaphragmatic Hernia
Percent Predicted Lung Volume (PPLV)
Total Lung VolumeTotal Thoracic Vol‐Mediastinal Vol
= PPLV
Mahieu‐Caputo et al BJOG 108: 863‐868, 2001Paek et al Radiology 220: 63‐67, 2001Gorincour et al Ultrasound Obstet Gynecol 26: 738‐744Barnewolt et al J Pediatr Surg 42: 193‐197, 2007

Total Lung VolumeTotal Lung Volume• By 34 wk fetal lung growth
should be complete.
• Fetal MRI to estimate total lung volume
• Goal to identify, counsel, and develop a treatment plan for high risk CDH patient
Mahieu‐Caputo et al. BJOG 2001; 108:863Neff et al. AJR 2007;189:1307
Rypens et al. Radiology 2001; 236


Assessment of Postnatal Assessment of Postnatal Pulmonary Hypertension in CDHPulmonary Hypertension in CDH
• All prognostic indicators focus on lung
- Indirect indicators
- LHR, PPLV, TLV, Liver position
- All measure lung size or volume
• Indicators of pulmonary hypoplasia
• No prenatal measurement has tried to predict severity of postnatal pulmonary hypertension

Prenatal Pulmonary Hypertension Index= PPHI= PPHI
LPA
RPA
Vermis
PPHI = (LPA d / Vermis l) x 10

Modified Modified McGoonMcGoon Index = MGIIndex = MGI
LPA
RPA
Ao
MGI = (RPA d + LPA d) / Ao d

CDH Prognostic Profile
• Congenital heart disease• Karyotype• Liver position• O/E LHR
- <25th% 20% survival• LHR
- >1.0 100% survival- < 1.0 50% survival
• PPLV early and late- < 15% high risk- > 22% low risk- Late more reliable
• TLV late- > 25cc favorable- < 18cc unfavorable
• Modified Magoon Index?- <0.8 severe pulm htn- >1.0 mild pulm htn
Criteria for EXIT-to-ECMO(and tracheal occlusion)Liver upLHR< 1.0PPLV <15TLV <18Normal karyotype

CDH-Composite Prognostic Index(CDH-CDI)

CDHCDH--Composite Prognostic IndexComposite Prognostic Index(CDH(CDH--CDI)CDI)

CDHCDH
TRACHEAL TRACHEAL OCCLUSIONOCCLUSION

• FETO Task Group• Leuven, Barcelona, London • FETO at 26-28 wks• Prenatal reversal of tracheal
occlusion• Outcomes in 210 cases
- Survival 49%• Conventional therapy
- Survival 20%• NA Consortium: TOTAL
• CHOP, Cincinnati, Denver
• Maryland and Texas• Toronto
Deprest et al J Pediatr Surg 2011Jani et al Ultrasound Obstet Gynecol 2009

EXITEXIT--toto--ECMO for High Risk CDHECMO for High Risk CDH• Rationale:
- Minimize hemodynamic instability- Minimize barotrauma- Eliminates resuscitation- Time for pulm vascular remodeling - Smooth transition to postnatal life- Early repair to allow remodeling
• Maternal risks- Deep general anesthesia- Cesarean section for subsequent
pregnancy- Risk of uterine atony
Bouchard S, Johnson MP, Flake AW, Howell LJ, Myers LB, Adzick NS, Crombleholme TM:The EXIT Procedure: Experience and Outcome in 31 Cases. J Pediatr Surg 37: 428‐426, 2002

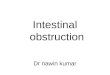
EXIT‐to‐ECMO N=8
EXIT‐to‐ECMOSurvival50% (4/8)
Cesarean with ECMO Standby
N=2
Cesarean Delivery Alone
N=5
ECMO*60% (3/5)
Survival 20% (1/5)
Non‐ EXIT Delivery Survival25% (2/8)
ECMO50% (1/2)
Survival50% (1/2)
Cesarean DeliveryN=7
ECMO100% (1/1)
Survival 0%
ECMO00% (8/8)
* 2 died at birth
Excluded forAbnormal Posture
N=2
Vaginal DeliveryN=1
Excluded forComfort Care
N=1Non‐EXIT
N=8
Met EXIT‐to‐ECMO CriteriaN=19

Conclusions
• Essential role of prenatal imaging in neck and chest lesions• Combination of ultrasound, MRI and echocardiography• Serial assessment• Prognostic assessment • Treatment options
•Open fetal surgery•Fetoscopic treatment?•Interstitial laser treatment •EXIT strategy
•EXIT‐to‐Airway•EXIT‐to‐Resection

Fetal Care Center of Cincinnati•Maternal-Fetal Medicine
− Mounira Habli MD−William Polzin, MD−Kim Brady, MD−Jim VanHook, MD−Ronald Jaekle,MD−David Lewis, MD
•Fetal Echocardiography−Erik Michelfelder, MD−James |Cnota,MD−William Gottliebson, MD−Allison Divanovic,MD−Haleh Hadarian, MD
•Urology/Nephrology−Pramod Reddy,MD−Robert Defore,MD−Elizabeth Jackson,MD
•ENT−Ravi Ellarhu,MD−Paul Willging,MD
•Neurosurgery−Karin Bierbrauer,MD−Francesco Mangano,MD
•Cardiac Surgery−Pirooz Eghtesady,MD−Peter Manning,MD
•Neonatology− James Greenberg, MD− Tanya Cahill, MD− Kurt Schibler, MD− Beth Haberman, MD− Paul Kingma, MD− Amy Nathan, MD
•Nursing Director− Kelli Young
•Coordinators− Gina Sharp, RN− Deb Voet, RN− Jenni Mason− Steve Imhoff− Judy Hostiuck
•Genetics− Rob Hopkin,MD− Howard Saul,MD− Christine Spaeth, CGC− Diana Smith, CGC
•Social Services− Erin Hartman, MSW
•Administrative− Rachel Jones− Emmie Beyer− Cheryl Snell
•Level III L&D Nurses• Good Samaritan Hospita
•Nurse Midwife– Karen McGirr
•Pediatric Surgery•Timothy Crombleholme,MD•Foong-Yen Lim,MD•Sundeep Keswani MD
•Anesthesiology–Ann Boat,MD–Mohammad Mahmoud,MD–Bonnie Hugus
•Radiology•Connie Bitters•Linda Martin–Beth Kline-Fath, MD–Maria Calvo, MD–Eva Rubio, MD–Leann Linam, MD–Kyuran Choe, MD
•Operating Room Nurses•Missy Ritter•Stacy Ruth•Tracy Heidrich•Latressa Ratner•Curtis Johnson

•Maternal-Fetal Medicine- Henry Galan, MD- Shane Reeves, MD- John Hobbins MD- Joyce Sung, MD
•Fetal Echocardiography- Adel Younozsai, MD- Lisa Howley, MD- Pei Ni Jone MD- Karrie Villavicencio,MD
•Urology/Nephrology- Duncan Wilcox, MD- Jeffrey Campbell, MD- Vijay Velmulakonda, MD
•ENT- Peggy Kelley MD- Jeremy Prager, MD
•Neurosurgery- Michael Handler, MD- Corbett Wilkinson, MD
•Cardiac Surgery- James Jaggers, MD- David Campbell, MD- Max Mitchell, MD
•Neonatology- Regina Reynolds, MD- Peter Hulac, MD- Jason Gien, MD- John Kinsella, MD- Therese Grover MD
•Coordinators- Kelli Young, RN- Jann Hodge, RN- Carrie Rafferty, RN
•Genetics- David Manchester, MD- Naomi Meks, MD
•Administrative
- Kelli Young, RN, CNP- Mary Beth Martin, RN, MBA- Gina Dooley
• Fetal and Pediatric Surgery•Timothy M Crombleholme MD•Stigg Somme, MD
•Anesthesiology–Geoffrey Galinkin, MD–Debnath Chaterjee, MD –Joy Hawkins, MD– Carrie Dean, MD–Christine Wood, MD
•Radiology• Lisa Waters, RDMS– Mariana Meyers, MD– Kim Dannull, MD– Laura Brown, MD– David Mersky, MD
• Obstetric Nursing•Jennifer Livingston, MD•Jena•Tiffany
•Operating Room• Erin Hughey,RN• Nicole Stuart, RN• Heidi
Colorado Fetal Care Center