Embed Size (px)
Citation preview

Four-year Surgical Results for
Traumatic Aortic Injury in
China Medical University Hospital, Mid-Taiwan
Yi-Chun Lin 林怡均 (5th grade medical student),
MingLi Li 李明禮, Chih-Hsiang Hsu, Ching-Feng Wu, Hui-Han Lin
Cardiovascular Division, Surgery Department, China Medical University Hospital, Taichung City, Taiwan
LINC Asian-pacific 2019
Hong Kong
March 12(Tue)-13(Wed) 2019

Speaker name: Yi-Chun Lin
.................................................................................
I have the following potential conflicts of interest to report:
Consulting
Employment in industry
Stockholder of a healthcare company
Owner of a healthcare company
Other(s)
I do not have any potential conflict of interest
Disclosure
Background
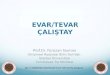
✓ Blunt traumatic aortic injury (BTAI) carries a high mortality rate up to 10-30% [1]
✓ Urgent TEVAR is mandatory for Grade II to IV blunt traumatic aortic injuries. [2]
[1] Aorta, July 2013, Vol.1, Issue 2: 117–122[2] Journal of Vascular Surgery 2009, Vol.49, 1403-08
• Grade I : intimal tear/flap
• Grade II : intramural hematoma
• Grade II’: AORTIC DISSECTION
• Grade III : pseudoaneurysm
• Grade IV: rupture
• Grade X : PERIAORTIC HEMATOMAEndovascular Today 2014, 38-42.

1. Accuracy of BTAI diagnosis and grading
2. Surgical strategy and results in our center
3. Analysis of mortality causes,
complications and reinterventions
4. Aortic remodeling after TEVAR
Aim

Jan. 2015 – Jan. 2019
all patients performed TEVAR for BTAI.
Retrospective review of
Initial data Operative Data Post-operation Diagnostic data
Mechanism of injury Operation time Length of ICU stay Grade of aortic injury
Associated injury Number of stents Length of ward stay Pre-operative CXR
Injury severity score Tapered stent usage Early complication Pre-operative CT
Glasgow coma scale Diameter of stents Late complication CT after operation
Initial / lowest BP Proximal landing Early reintervention False lumen thrombosis
Initial heart rate Proximal landing Late reintervention Change of aortic diameter
Comorbidity LSCA coverage Mortality cause
Door to operation time Associated operation Operation to mortality time
BP: blood pressure LSCA: left subclavian artery ICU: intensive care unit CXR: chest X-ray CT: computed tomography
Method
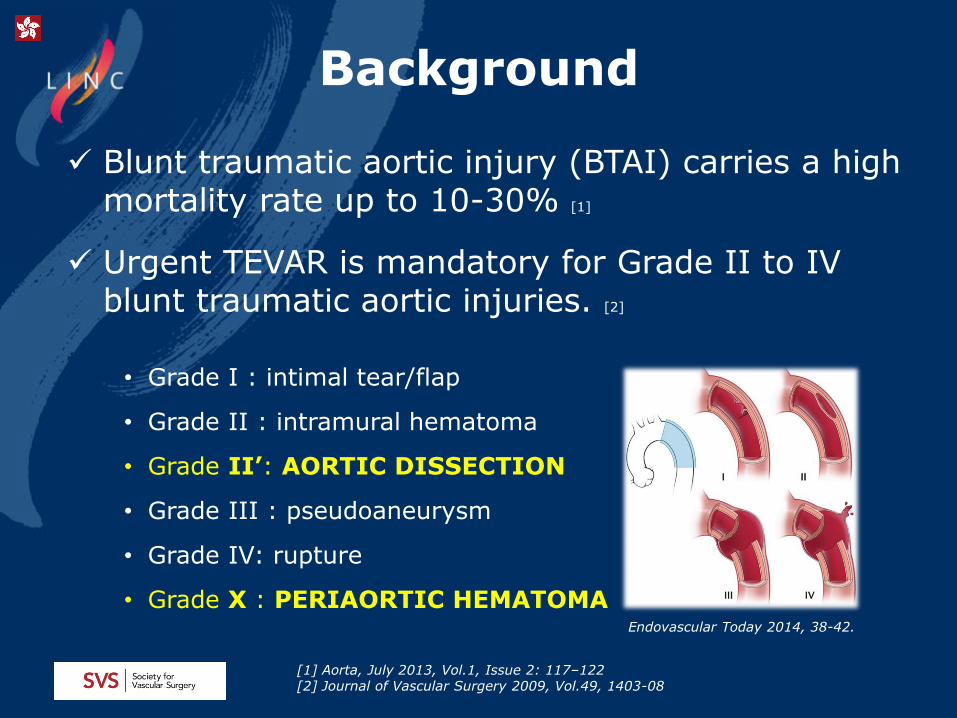
False Lumen Thrombosis

43 BTAI
Gr 2
1Type A
IMH
4Type B
IMH
Gr 2’
4Type A
dissection
7Type B
dissection
Gr 3
15Pseudo-
aneurysm
Gr 4
8 Contained
rupture
Gr X
4 Periaortic hematoma
IMH: intramural hematoma
BTAI Grading

17 y/o Malescooter vs car
17 y/o Male scooter vs car
22 y/o Male scooter vs car
72 y/o Male car vs electric pole
Periaortic hematoma

Fall
23%Motorcycle
Crash
54%
Bike
Crash
2% Car
Crash
12%
Pedestrian
7%Other: hit
by electric
cable
2%
0 10 20 30
Lung
Sternal and Ribs
Abdomen
Brain
Extremity
Spine
Pelvis
Facial bone
28
19
18
17
17
14
11
3
PERSON
Pre-operative Results
Mechanism of Injury Associated Injury
Injury Severity Score (ISS): 31±9

Age 52.8 ± 17.6
Male 34 (79.07%)
Comorbidities
Hypertension 15 (34.88%)
Cigarette 13 (30.23%)
CVA 1 (2.33%)
DM 7 (16.28%)
Medication
Antiplatelet 2 (4.65%)
Pre-operative Results
Pre-operation CXR
0 10 20 30 40
Widened mediastinum
Indistinct aortic knob
Deviation of trachea
Ribs/Clavical/Scapula fracture
cardiomegaly
Pleural effusion
Hemothorax
Deviation of NG
Traumatic pulmonary edema
Tracheal compression
Lung contusion
Compression of bronchus
Apical cap
37
37
11
9
6
5
4
2
2
1
1
1
1

Door to Operation Time
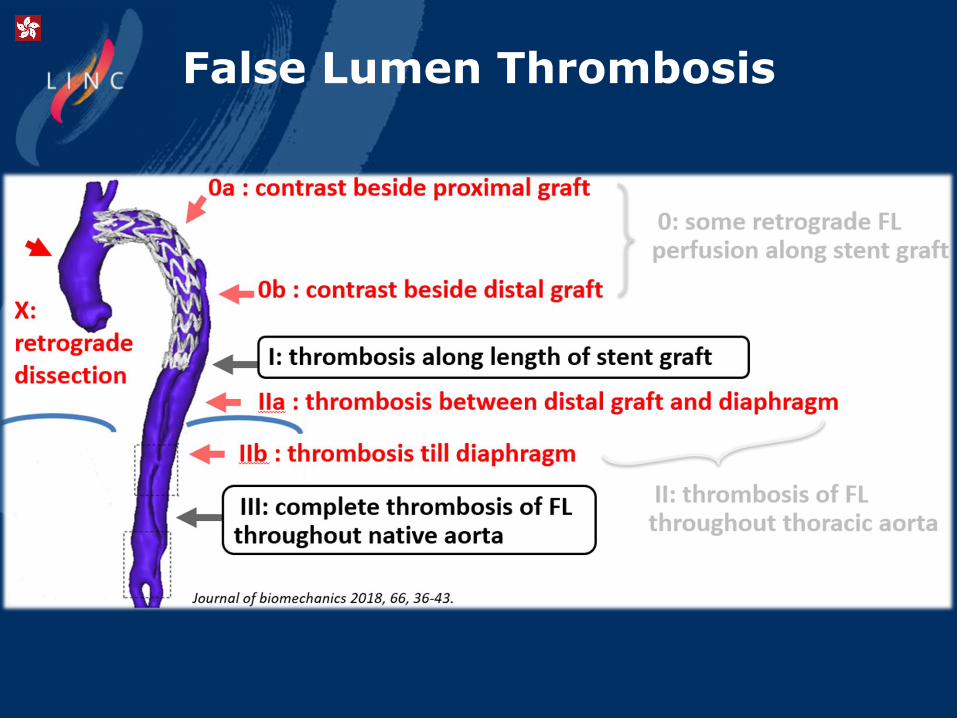
BTAI (43) BAAD (46)
Age 52.8 ± 17.6 55.3 ± 13.3
Operation time 100.9 min 124.5 min
Number of graft 2 (64.3%) 2 (71.7%)
Tapered graft 37.5% 26.1%
Proximal diameter
28 mm (34.5%) 34 mm (26.1%)
Distal diameter 24 mm (30%) 28 mm (39.1%)
Proximal landing ≥ Zone3 (52.4%) Zone2 (52.2%)
Distal landing T8 (26.8%) / T9 (22.0%) T8 (56.5%)
Management of LSA coverage
23.8% TAE 2 / rChim 6 / aChim 1/ fenestration 1/ covered 2
54.3% TAE 2/ rChim 18/ aChim3/ fenestration 1/ ligate 1
Operation
BAAD: acute Type B aortic dissection TAE: trans-arterial embolization rChim: reversed chimney aChim: antegrade chimney
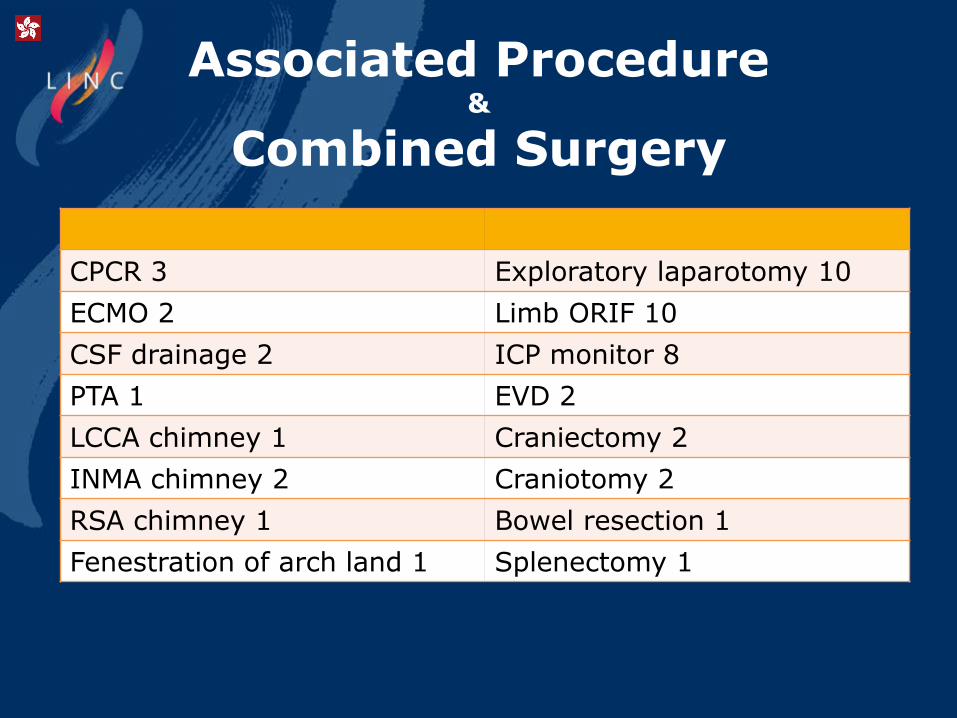
CPCR 3 Exploratory laparotomy 10
ECMO 2 Limb ORIF 10
CSF drainage 2 ICP monitor 8
PTA 1 EVD 2
LCCA chimney 1 Craniectomy 2
INMA chimney 2 Craniotomy 2
RSA chimney 1 Bowel resection 1
Fenestration of arch land 1 Splenectomy 1
Associated Procedure &
Combined Surgery

BTAI BAAD
30-day Mortality 13/43 (30.2%) 4/46 (8.7%)
Procedure-related 5/43 (11.6%) (free rupture 3) 2/46 (4.3%)
Brain injury 5/43 (11.6%) 2/46 (4.3%)
Lung 1/43 (2.3%) Tension pneumothorax 1 0
Abdomen2/43 (4.7%)Visceral ischemia 1/Intraabdominal bleeding 1
0
Early complication7.1% Type A AD with aortic valve entrapment 1Type A AD AKI 2
15.2%
Reintervention3.3 %RSA to LSA due to LSA steal syndrome 1
23.9 %
Surgical Results

Analysis of Mortality
Grade
Gr II Gr II' Gr III Gr IV Gr X
A
IMH
B
IMH
Type A
AD
Type B
AD
Pseudo-
aneurysm
Contained
rupture
Periaortic
hematoma
Mortality no. 1 / 1 1 / 4 3 / 4 2 / 7 2 /15 4 /8 0
Type Management Outcome / mortality cause
A IMH Z4 TEVAR mortalityPre-operative spinal shock,
medulla infarction
A AD Asc. Ao grafting + Z3 TEVARMBD in 26 day,
persistent patent false lumen at arch
A AD Z0 TEVAR mortalitySevere AR, related to
aortic valve entrapment
A ADTotal arch replacement + Z2
TEVAR + LSCA aChimneymortality
Pre-operative cerebellum
infarction
A AD Z0 TEVAR +INMA rChimney mortality True lumen collapse

A 79 y/o female falling from stairsGr II Type B IMH

A 59 y/o male falling from 2nd floorGr II’ Type A Aortic Dissection
Gr4 AR
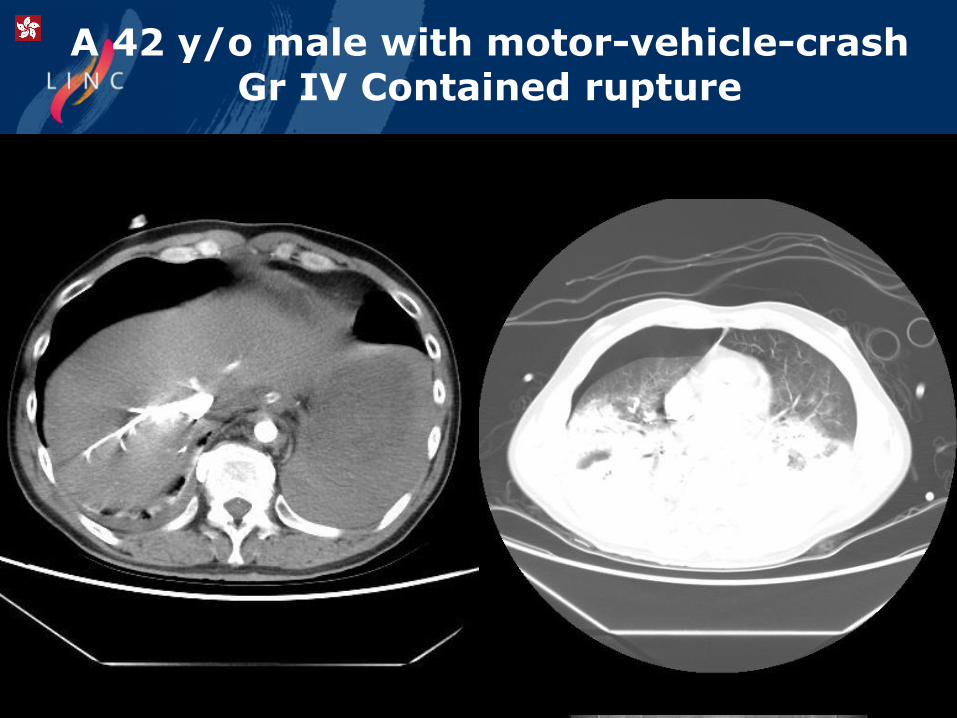
A 42 y/o male with motor-vehicle-crashGr IV Contained rupture
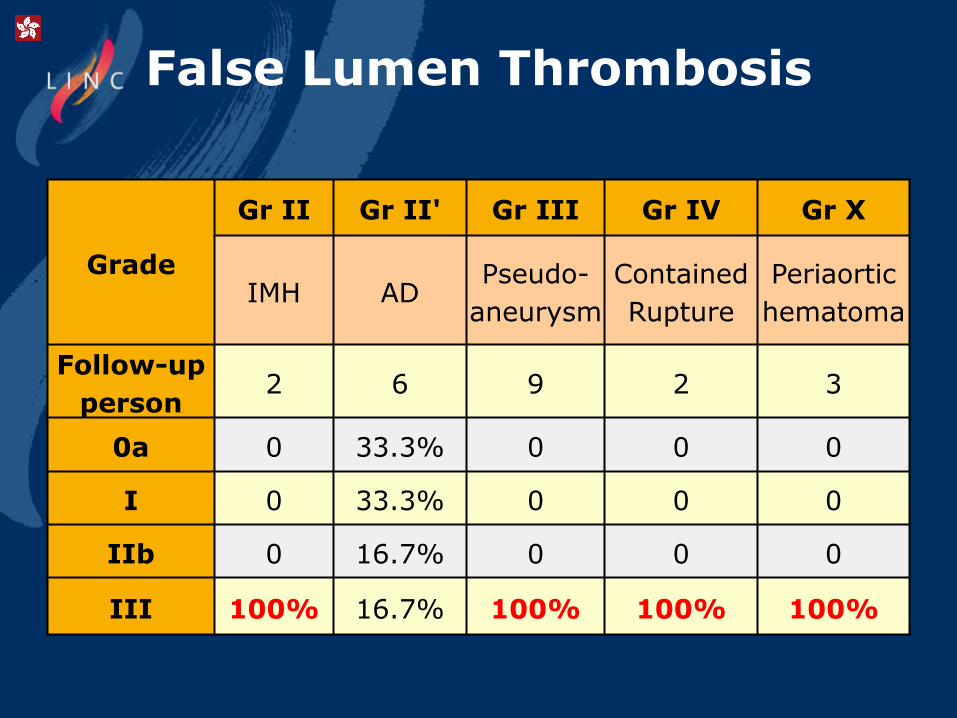
False Lumen Thrombosis
Grade
Gr II Gr II' Gr III Gr IV Gr X
IMH ADPseudo-
aneurysm
Contained
Rupture
Periaortic
hematoma
Follow-up
person2 6 9 2 3
0a 0 33.3% 0 0 0
I 0 33.3% 0 0 0
IIb 0 16.7% 0 0 0
III 100% 16.7% 100% 100% 100%
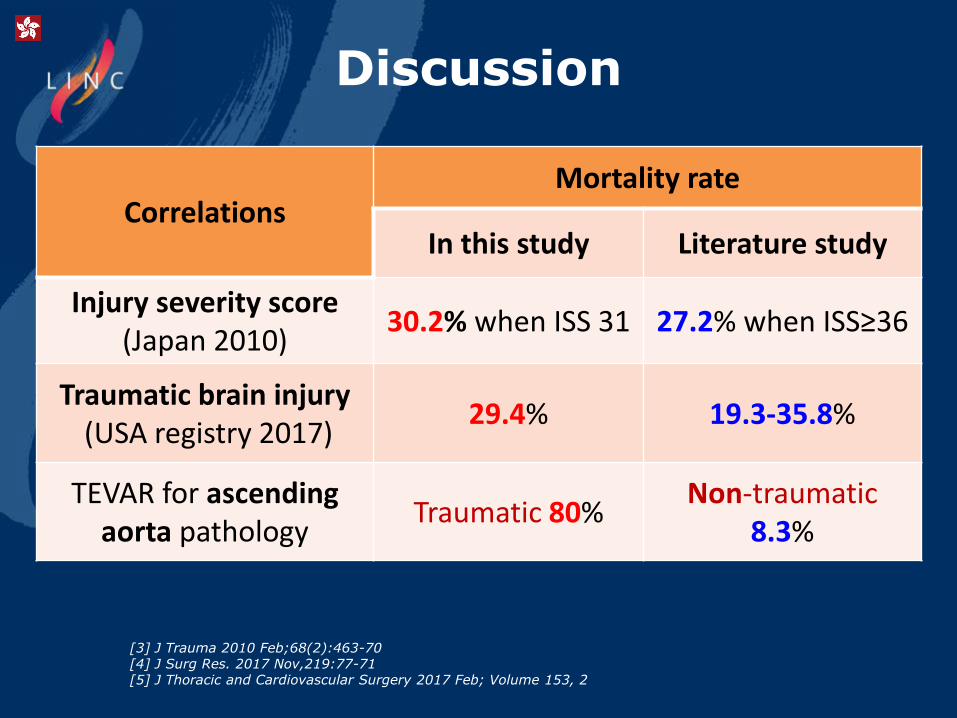
Discussion
[3] J Trauma 2010 Feb;68(2):463-70[4] J Surg Res. 2017 Nov,219:77-71[5] J Thoracic and Cardiovascular Surgery 2017 Feb; Volume 153, 2
CorrelationsMortality rate
In this study Literature study
Injury severity score(Japan 2010)
30.2% when ISS 31 27.2% when ISS≥36
Traumatic brain injury (USA registry 2017)
29.4% 19.3-35.8%
TEVAR for ascending aorta pathology
Traumatic 80%Non-traumatic
8.3%
1. Disrupted intercostal arteries, azygos vein and IVC may mimic BTAI
2. TEVAR for BTAI is always a dilemma in multiple traumatic patients
3. Strategy for BTAI with ascending aortic pathology needs further evaluation
4. Promising aortic remodeling for Gr III-IV BTAI after TEVAR procedure
Conclusion

Yi-Chun Lin 林怡均, MingLi Li 李明禮,
Cardiovascular Division, Surgery Department, China Medical University Hospital, Taichung City, Taiwan
LINC Asian-pacific 2019
Hong Kong
March 12(Tue)-13(Wed) 2019
Thank you for your attention












![Fran Milčinski U BTAI CL - domžalec.si · 2019. 1. 10. · 821.163.6-93-32(0.034.2) MILČINSKI, Fran, 1867-1932 Butalci [Elektronski vir] / Fran Milčinski. ... Leta 1890 je postal](https://img.pdfslide.tips/doc/110x75/60f97bfd4c669727cc3b5b70/fran-milinski-u-btai-cl-domalecsi-2019-1-10-8211636-93-3200342.jpg)