Embed Size (px)
Citation preview
T k i H lthTeamwork in HealthcareWhat’s the Big Deal?
MARK EARNEST MD , PHDD IRECTOR OF I N T ERPROFESS IONAL EDUCAT ION AMCD IRECTOR OF I N T ERPROFESS IONAL EDUCAT ION ‐ AMC
An Exercise
THE STORYA businessman has just turned off the lights in a store j gwhen a man appeared and demanded money. The owner opened the cash register. The contents of the
h d d h dcash register were scooped up, and the man sped away. A member of the police force was notified.

STATEMENTS ABOUT THE STORYCi l h i (‘?’ h i f i )Circle the appropriate answer. (‘?’ means not enough information)
1. A man appeared after the owner had turned off the lights.2. The robber was a man.
True False ?True False ?
3. The man who appeared did not demand money.4. The man who opened the cash register was the owner.5. The storeowner scooped up the contents of the cash register
d
True False ?True False ?
T F l ?and ran away.6. Someone opened a cash register.7. After the man who demanded the money scooped up the
contents of the cash register he ran away
True False ?True False ?
True False ?contents of the cash register, he ran away.8. While the cash register contained money, the story does not
state how much.9 The man demanded money of the owner
True False ?
True False ?True False ?9. The man demanded money of the owner. True False ?
STATEMENTS ABOUT THE STORYCircle the appropriate answer T/ F/ ‘?’ (not enough information)
10 The robber opened the cash register
Circle the appropriate answer T/ F/ ? (not enough information)
True False ?10. The robber opened the cash register.11. After the store closed, a man appeared.12. The robber did not take the money with him.13 The man who appeared did not threaten the owner
True False ?
True False ?True False ?
True False ?
13. The man who appeared did not threaten the owner.14. The owner opened the cash register.15. The age of the store’s owner was not revealed.16 Taking the contents of the cash register with them someone left
True False ?True False ?True False ?True False ?16. Taking the contents of the cash register with them, someone left
the store.17. The story concerns a series of events in which only three persons
are referred to: the owner of the store, a man who demanded
True False ?
,money, and a policeman.
18. The following events were included in the story: someone demanded money, a cash register was opened, its contents were
True False ?
scooped up, and a person dashed out of the store. True False ?
How did you do?
How did you do?
1) T 10) ?1) T2) ?3) F
10) ?11) ?12) ?3) F
4) ?5) ?
12) ?13) ?14) T5)
6) T7) ?
4)15) T16) ?
8) ?9) ?
17) ?19) F
Patterns?
h l ( l l ) Teams are smarter than individuals (almost always) Team performance is almost never lower than the highest indi id al score on the teamhighest individual score on the team
If Team score < Best individual score, then Someone withheld information Someone withheld information
OR Someone rejected valuable information
(Thanks to Carl Larson PhD, Professor Emeritus, DU)
What is a Team?
b Two or more members Each with specific roles, perform specific tasks, interact or coordinate to achie e a common goalor coordinate to achieve a common goal
Teams make decisionsT i li d k l dg d kill ft Teams possess specialized knowledge and skills, often function under high workload
Teams demonstrate task interdependency (members Teams demonstrate task interdependency (members must adjust their actions relative to each other to accomplish team goals)p g )
AHRQ – Medical Teamwork and Patient Safety – The Evidence‐Based Relation
Back to our Exercise
Sources of poor performance: Inadequate Assertiveness ‐ Someone withheld qimportant information
Ineffective Leadership Model ‐ Someone rejected important information
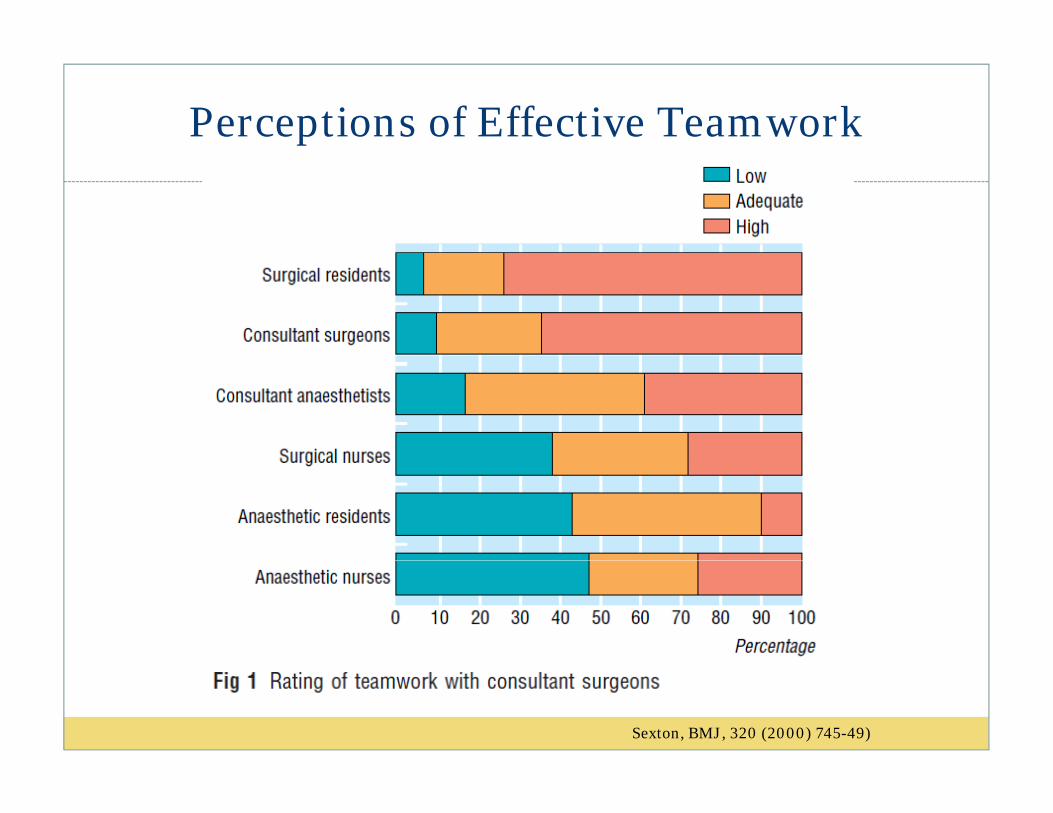
Perceptions of Effective Teamwork
Sexton, BMJ, 320 (2000) 745-49)
Conclusions
In hierarchical organizations, those at the top of the hierarchy perceive a higher degree of collaboration than those lower downthan those lower down
True of managers as well as providers Singer SJ, Falwell A, Gaba DM, Baker LC. Med Care. 2008;46:1149‐1156Singer SJ, Falwell A, Gaba DM, Baker LC. Med Care. 2008;46:1149 1156
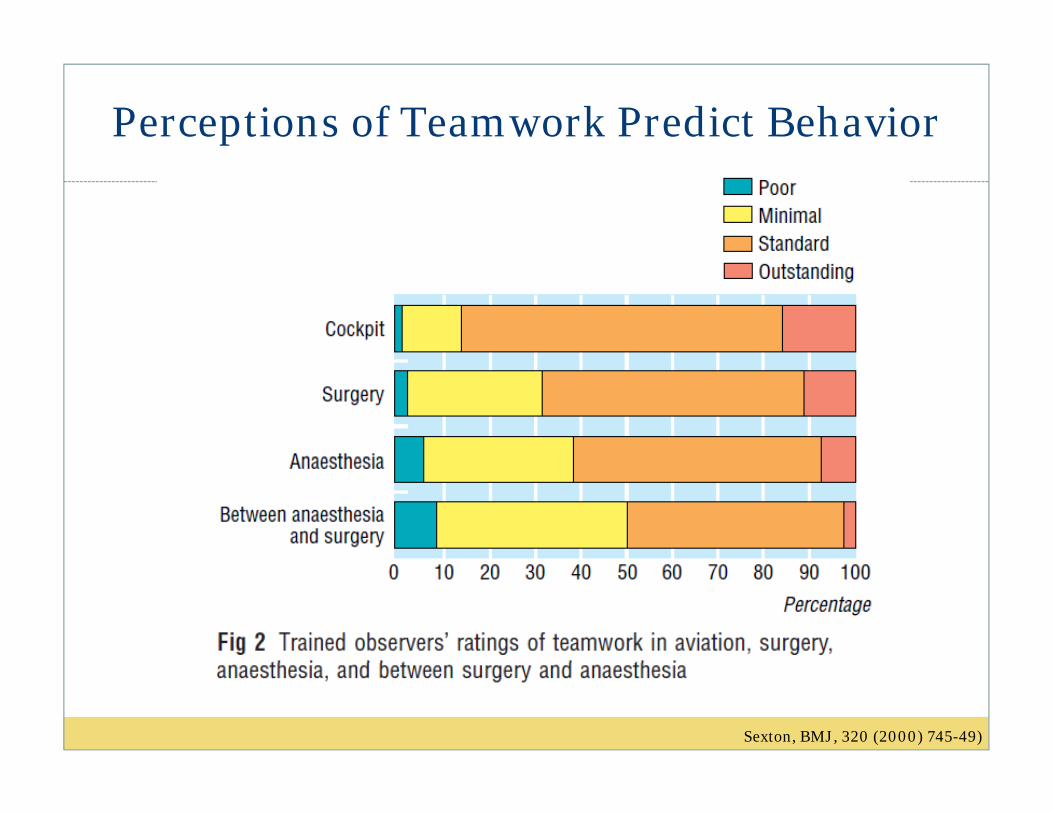
Perceptions of Teamwork Predict Behavior
Sexton, BMJ, 320 (2000) 745-49)
Teamwork
Does It Matter?
The Epidemiology of Error
IOM 1999 – To Err is Human Estimate of deaths from medical error Figures extrapolated from two large studies
Harvard Medical Practice Study, Utah‐Colorado Medical Practice Study
Estimate: 44 98 000 deaths per year from medical Estimate: 44‐98,000 deaths per year from medical error

Top Causes of Death in US: 2007 Top Causes of Death in US: 2007
H di 6 61. Heart disease: 615,6512. Malignant neoplasm: 560,1873 Cerebrovascular disease: 133 9903. Cerebrovascular disease: 133,9904. Chronic, lower respiratory disease: 129,331 5. All accidents: 117,0755 7, 756. Alzheimer’s: 74,9447. Diabetes: 70,9058. Influenza and pneumonia: 52,8479. Nephritis/nephrosis: 46,09510 Septicemia: 34 85110. Septicemia: 34,851
National Vital Statistics Reports, Vol. 58, No. 1, August 19,2009; www.cdc.gov/nchs
Lessons from Aviation
Enormous resources devoted to understanding mishaps Of 35,000 mishaps, 50% were due to flight crew errors and 35% to air traffic errors
Dysfunctional communication within hierarchy is common in many of the worst outcomesmany of the worst outcomes
Crew errors occur most often when they fail to manage the resources that are available to them
Led to development of Crew Resource Management training and emphasis on culture of safety
From other Fields…
Teams working together in high risk, high stakes endeavors make fewer mistakes than individuals Firefighting Manufacturing
Th ilit The military Rapid response police activities
Mt Sinai J Med. 2009 Aug;76(4):318‐29
Evidence in Medicine is growing
Poor team function in surgery increases mortality and post‐op complications
Mazzocco K, Petitti DB, Fong KT, et al. Am J Surg. 2009;197:678‐685
Pronovost’s Keystone ICU intervention, decreased line related infections from 2 7/1000 pt days to zero in 3 related infections from 2.7/1000 pt days to zero in 3 months. Didn’t work until nurses empowered to stop the procedure p
Pronovost P, Needham D, Berenholtz S, et al. N Engl J Med. 2006;355:2725‐2732
Crew Resource Management training reduces frequency and severity of adverse obstetrical events and improves providers attitudes toward safety.
Pratt SD, Mann S, Salisbury M, et al. Jt Comm J Qual Patient Saf. 2007;33:720‐725
Crew Resource Management training reduced clinical errors in the ED and improved staff attitudes clinical errors in the ED and improved staff attitudes toward teamwork
Morey JC, Simon R, Jay GD, et al. Health Serv Res. 2002;37:1553‐1581Morey JC, Simon R, Jay GD, et al. Health Serv Res. 2002;37:1553 1581
Caveats
Not all trials of CRM have had positive results, though none have demonstrated harm
f Reasons cited for negative Inadequate time for the intervention Short f/u time Short f/u time Baseline variability in adverse events between institutions in the
studies
Nielsen PE, Goldman MB, Mann S, et al. Obstet Gynecol. 2007;109:48‐55
Institutional Comparison Study
Developed a quality index for Academic Medical Centers. Using patient level data, identified cohort of high
f ( ) d ( ) fperformers (3) and average (3) performers Six trained observers, blinded to the quality index measures of each institution made site visits: reviewed measures of each institution made site visits: reviewed documents (org structure, strategic plans, job descriptions, etc.) and interviewed leaders observed their behaviorbehavior
Qualitative methodology (Grounded Theory inductive analysis)y )
Institutional Comparison Study
Identified five characteristics of top performers1. Shared sense of purpose (“patients first”, service focused,
di ti f ti ith t f )dissatisfaction with current performance)2. Leadership style (hands on, visible, embody the patients
first ethos, merger of campus and practice accountability)3. Accountability systems for service, quality, and safety
(consistent measurement, central goals, chairs accept accountability for quality w/in departments)accountability for quality w/in departments)
4. A focus on results (results outweigh approach, focus on human behavior as key…)
Institutional Comparison Study
ll b ( l f k)5. Collaboration (Culture of Teamwork)‐ Collaboration characterizes the relationship between administration, physicians, nurses, and other staffRecognition of employee contributions at every level is ‐ Recognition of employee contributions at every level is frequent
‐ Employees value each other’s critical knowledge when problem solving
Comparison sites – Staff were more likely to feel that senior leaders did not work with
them or understand their perspectives. f At worst: rivalry and credit grabbing among disciplines, tendency of
nurses to work around reluctant physicians rather than involving them.
Kerouk, Academic Medicine: December 2007 ‐ Volume 82 ‐ Issue 12 ‐ pp 1178‐1186
Teamwork: Beneficial Side Effects
Error reduction Increase in morale Increase in morale Improved efficiency Higher job satisfaction Higher job satisfaction Lower staff turnover
Gawande, The Checklist Manifesto

What’s New at the AMC?
REACH – Realizing Educational Advancement forCollaborative Health $1.8 million, 3 year collaborative grant (Colorado Health
Foundation and Josiah Macy Jr. Foundation)
l i ll h l h f i ’ d Goal: Train all health professions’ student on campus in basic interprofessional care competencies

Interprofessional Care Competencies
Role Clarification Interprofessional Conflict Resolutionp Team Functioning Patient/family/community‐centered care/ y/ y Collaborative Leadership Interprofessional Communicationte p o ess o a Co u cat o Conflict resolution
Canadian Interprofessional Health Collaborative
REACH Programs
Health Mentors Program Students grouped at orientation into IP teams of 5‐6 Groups maintained for 2 years (REACH and Ethics coursework) Each group paired with a community member with a disability or
chronic illness (“health mentor”)( )
Health Mentors Program
Teams meet with mentors each semester to complete a task Life/health history Access to care/patient experience Wellness plan Wellness plan Drug and OTC safety

Health Mentors Program
One month after meeting with mentors, teams meet for facilitated Team Based Learning exercise
F i Foci: Interprofessional knowledge Team process/Leadership Specific learning objectives from the modules
Team Based Learning One facilitator to 6‐8 teams Facilitator directs process within the groups and common
discussion between the groupsg p

Health Mentors Program Needs
Health Mentors – Patients with chronic illness Can get to campus
W ld b li bl i ki ith t d t Would be reliable in working with students Have needs that students would benefit from understanding
Facilitators/Program Advisors Facilitators/Program Advisors Participate in developing curricula Facilitate TBL sessions and advise re: refinement
TeamSTEPPS
Team Strategies and Tools to Enhance Performance & Patient Safety
Evidence‐based clinical communication curriculum designed by DOD and AHRQ
Team-Based CompetenciesAddressed by TeamSTEPPSAddressed by TeamSTEPPS
Team leadership Mutual performance monitoring (situation
)monitoring) Back‐up behavior (mutual support) Adaptability Shared mental models Communication
TeamSTEPPS
All health professions student on campus will receive: TeamSTEPPS training IP simulation exercises where TeamSTEPPS skills will be practiced
and reviewed
IP Clinical Rotations
Goal: All health professions students will have a meaningful educational experience in a clinical setting h h l d h l lwhere they explore in‐depth clinical care or practice
improvement from an interprofessional perspective
We need you…
Health mentors TBL facilitators Wisdom for rotations implementation IP practice sites for student rotations