Embed Size (px)
Citation preview

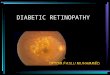
HYPERTENSIVE RETINOPATHYChikita Artia Sari / I 11109014

Definition Hypertensive retinopathy represents the
ophthalmic findings of end-organ damage secondary to systemic arterial hypertension.
The appearance of the fundus in hypertensive retinopathy is determined by the degree of elevation of the blood pressure and the state of the retinal arterioles.
In mild to moderate systemic hypertension, the retinal signs may be subtle. Focal attenuation of a major retinal arteriole is one of the earliest signs. Diffuse arteriolar attenuation, broadening of the arteriolar light reflex, and arteriovenous crossing changes also occur.

Definition In young patients with accelerated malignant
hypertension, an extensive retinopathy is seen, with hemorrhages, retinal infarcts (cotton-wool spots), choroidal infarcts (Elschnig's spots), and occasionally serous detachment of the retina.
Severe disk edema is a prominent feature and may be accompanied by a macular star of hard exudate. Vision may be impaired and may deteriorate further if blood pressure is reduced too quickly.

Incidence In the Beaver Dam Eye Study, which
evaluated hypertensive patients without coexisting, confounding vascular diseases, the overall incidence of hypertensive retinopathy was about 15%; specifically, 8% showed retinopathy, 13% showed arteriolar narrowing, and 2% showed arteriovenous nicking.

The Stage of Hypertensive Retinopathy
Hemorrhage
Exudate Disc Edema
Grade 1
- - -
Grade 2
- - -
Grade 3
+ + -
Grade 4
+ + +

Normal Retina and Hypertensive Retinopathy
Normal Retina
Hypertensive Retinopathy
A: HemorrhagesB: Exudates (Fatty Deposits)C: Cotton Wool Spots (Micro Strokes)
A B
C

GRADE I Generalized
arteriolar attenuation
Broadening of arteriolar light reflex
Concealment of vein at a-v crossings
Arteriolar Narrowing

GRADE II Severe
generalized and focal arteriolar constriction
A-v crossing changes (salus sign)

Grade II (AV Nicking) Arteriovenous nicking is a highly specific finding
and the hallmark of chronic hypertensive retinopathy. At the arteriovenous crossings in the retina, the vessels share a common adventitial sheath.
Arteriovenous nicking is diagnosed when the crossing retinal vein becomes less apparent or even disappears on either side of the artery.
The course of the vein may change to a more perpendicular direction as well. If there is impedance to flow, the segment of the vein distal to the constriction appears larger, darker, and more tortuous.

GRADE III Copper wiring of arterioles Venous banking distal to A-V
crossing (bonnet’s sign) Venous tapering on either
side of crossing (gunn’s sign)
Right angle deflection of veins.
Flame shaped hemorrhages cotton wool spots, hard exudates.

GRADE IV All changes of grade 3 Silver wiring of
arterioles Disc edema Papilledema from
malignant hypertension. There is blurring of the borders of the optic disk with hemorrhages (yellow arrows) and exudates (white arrow)

Clinical Signs Patients with hypertensive retinopathy are usually
asymptomatic. Common clinical findings include focal constriction and dilatation of the retinal arterioles, tortuosity of the retinal arterioles, an increase in the arteriolar light reflex, and loss of transparency of the intra-arterial blood column.
Additional signs of impedance to flow are retinal hemorrhages, macular edema, and cotton-wool spots. In areas of frank obstruction, the presence of venous-venous collaterals may be long standing.

Clinical Signs Secondary ocular complications of chronic
systemic arterial hypertension include retinal vascular occlusive disease, macroaneurysm formation, and nonarteritic anterior ischemic optic neuropathy.
The appearance of the ocular fundus in hypertension is related directly to the status of the retinal arteries and the rate of rise and degree of systemic blood pressure.
Visual disturbances are common in malignant hypertension. Symptoms include headache, scotoma, diplopia, dimness in vision and photopsia

Clinical Signs Ocular findings in malignant arterial
hypertension are divided into three distinct categories: hypertensive retinopathy, hypertensive choroidopathy, and hypertensive optic neuropathy.
The causes of these clinical findings includes constriction of vascular beds from circulating catecholamines, obstruction of arterioles, and breakdown in the blood-retina barrier.

Clinical Signs In acute malignant hypertensive retinopathy
include focal arteriolar narrowing, cotton-wool spots, intraretinal transudates, macular edema, and retinal hemorrhages.
Retinal hemorrhages are linear, occurring in the nerve fiber layer in the peripapillary region. Cystoid macular edema, lipid deposits, and arteriolar changes are signs of more chronic malignant hypertensive retinopathy.

Clinical Signs Arteriolar narrowing observed on ophthalmoscopy has
been challenged by Hayreh, who refers to this clinical finding as “pseudonarrowing” secondary to retinal edema creating a visual effect of narrowing of the retinal arteriole.
Cotton-wool spots are fluffy, elevated, tan–white areas of retinal opacity occurring within a few disc diameters of the optic nerve, caused by occlusion of terminal retinal arterioles. Capillary nonperfusion is present on angiography. Cotton-wool spots typically resolve in 3–6weeks and are associated with permanent nerve fiber layer loss in the vicinity of the lesion.

Clinical Signs Periarteriolar intraretinal transudates are tan–white
retinal lesions occurring in the vicinity of an arteriole. The lesions measure about one quarter of the disc area but are clinically larger, as they coalesce with adjacent lesions.
Intraretinal transudates occur secondary to focal areas of arteriolar leakage identified on angiography and resolve without residual retinal damage in 2–3weeks.
Macular edema and subretinal fluid are retinal findings related to hypertensive choroidal changes affecting the retinal pigment epithelium (RPE), with alterations in the blood-retina barrier.

Clinical Signs Several classification schemes have been
used to stage hypertensive retinal changes. The two most widely accepted are the Keith-Wagener-Barker classification and the Scheie classification.
The Keith-Wagener-Barker scheme combines the clinical findings of hypertension and atherosclerosis.
The Scheie classification keeps the two disease processes separate.

KEITH-WAGENER-BARKER CLASSIFICATION
Group I
Mild-to-moderate narrowing or sclerosis of the arterioles
Group II
Moderate to marked narrowing of the arteriolesLocal and/or generalized narrowing of arteriolesExaggeration of the light reflex Arteriovenous crossing changes
Group III
Retinal arteriolar narrowing and focal constrictionRetinal edema Cotton-wool patchesHemorrhage

SCHEIE CLASSIFICATION
HYPERTENSIONGrade 0
No change
Grade I
Barely detectable arteriolar narrowing
Grade 2
Obvious arteriolar narrowing with focal irregularities
Grade 3
Grade 2 plus retinal hemorrhages and/or exudates
Grade 4
Grade 3 plus papilledema

SCHEIE CLASSIFICATION
ARTERIOLAR SCLEROSISGrade 0
Normal
Grade 1
Barely detectable light reflex changes
Grade 2
Obvious increased light reflex changes
Grade 3
Copper-wire arterioles
Grade 4
Silver-wire arterioles

Pathology Microscopically, early changes from
hypertension demonstrate sclerosis and thickening of the arteriolar walls with luminal narrowing. These findings become more prominent with long-standing systemic hypertension.
Arteriole thickening in the choroidal vessels is typically more severe than in the retinal arterioles and more closely resembles systemic arterial changes.

Pathology In malignant hypertension, the arterioles are
similarly thickened, but necrosis and fibrinoid deposition in the vessel wall occur.
Electron micrographs of retinal arterioles in malignant hypertension eventually demonstrate dilatation of the lumen, with focal breaks in the endothelium surrounded by lipid and fibrin, as the autoregulatory mechanisms of the arterioles are exceeded.
Other pathological findings include optic nerve edema, cotton-wool spots, microaneurysms, and focal infarcts

Treatment Treatment of the underlying systemic condition
can halt the progress of the retinal changes, but arteriolar narrowing and arteriovenous nicking usually are permanent.
Treatment of malignant hypertensive retinopathy, choroidopathy, and optic neuropathy consists of lowering blood pressure in a controlled fashion to a level that minimizes end-organ damage. The actual level of blood pressure is less important in gauging the urgency of the situation than is the ongoing end-organ damage.

Treatment In hypertensive patients, the autoregulatory
mechanism that maintains constant blood flow to tissues is elevated to a higher level. This allows for the tolerance of higher blood pressures, and lowering blood pressure below the regulatory range can prevent adequate blood flow from reaching vital organs.
Therefore, blood pressure should be lowered in a slow, deliberate, controlled fashion to prevent end-organ damage. Too rapid a decline can lead to ischemia of the optic nerve head, brain, and other vital organs, resulting in permanent damage.

Treatment Medications used to treat hypertensive
emergencies include sodium nitroprusside, nitroglycerin, calcium channel blockers, beta blockers, and angiotensin-converting enzyme inhibitors.
Treatment should be initiated in a controlled, monitored setting under the auspices of a physician skilled in the use of antihypertensive medications.

THANK YOU