Embed Size (px)
Citation preview

Clinical–patient studies
Increased concentrations of transforming growth factor b1 and b2 in the plasma of patients
with glioblastoma
Thomas Schneider1, Michael Sailer3, Siegfried Ansorge4, Raimund Firsching1 and Dirk Reinhold21Department of Neurosurgery Otto-von-Guericke University, Leipziger Strasse 44, D-39120 Magdeburg, Germany;2Institute of Immunology Otto-von-Guericke University, Leipziger Strasse 44, D-39120 Magdeburg, Germany;3Department of Neurology II Otto-von-Guericke University, Leipziger Strasse 44, D-39120 Magdeburg, Germany;4Institute of Medical Technology Magdeburg, IMTM, Leipziger Strasse 44, D-39120 Magdeburg, Germany
Key words: glioblastoma, plasma concentrations, TGF-b1, TGF-b2
Summary
Recently, several in vitro studies have demonstrated production of the potent immunosuppressive cytokine trans-forming growth factor b (TGF-b)2 in glioblastoma cell lines. Systematic studies of the concentration of TGF-bisoforms in the plasma of patients harboring intracerebral tumors do not exist. In the present study, the concen-trations of TGF-b1 and TGF-b2 in platelet-poor plasma of 21 patients with glioblastoma before and after extensiveresection were measured by specific ELISA systems and related to survival. The plasma concentrations of latentTGF-b1 of patients with glioblastoma prior to surgery were significantly higher in comparison to healthy controlprobands, but not to patients with multiple sclerosis (MS). Furthermore, latent TGF-b2 was found to be signifi-cantly increased in the plasma of patients with glioblastoma in comparison to healthy control probands and patientswith MS. After extensive resection of the tumor, the value of latent TGF-b2 evidently decreased. Interestingly, theconcentration of latent TGF-b2 prior to surgery was correlated with survival and a strong relationship was foundbetween the survival and the difference of latent TGF-b2 levels prior to surgery minus the TGF-b2 concentrations7 days after surgery. A higher difference in these plasma concentrations >6 ng/ml vs. <6 ng/ml clearly correlateswith a longer survival time. In conclusion, this study suggests that glioblastoma does secret TGF-b2 in vivo and thatTGF-b2 may play an important role in glioblastoma patients.
Abbreviations: IL – interleukin; MS – multiple sclerosis; TGF-b – transforming growth factor-b
Introduction
Glioblastoma patients are characterized by an impairedimmune system, especially by depressed T lymphocytefunctions [1]. An immunosuppressive ‘glioblastoma-derived T cell suppressor factor’ has been detected inglioblastoma cell lines. This factor was found to beidentical with the multifunctional cytokine transform-ing growth factor-b2 (TGF-b2) [2].
TGF-b isoforms (in humans TGF-b1, TGF-b2 andTGF-b3) are known to be the most potent immunosup-pressive cytokines, controlling the growth and differen-tiation of several cell types. TGF-b is capable of inhibitingT cell and B cell activation and proliferation, depressingthe activity of natural killer (NK) cells, reducing theproduction of cytokines like IL-2, IL-6, IL-10, IFN-c, andsuppressing the expression of human leukocyte antigen(HLA)-DR on glioma cells [2–7]. TGF-bs are mostlysecreted not as an active form, but as a latent compound,inwhich the active TGF-b and theTGF-bbinding protein(latency-associated peptide, LAP) are bound together [8].
Besides the original function of TGF-b2 as a growthregulating cytokine, it is held responsible for thedepressed immune system in patients with glioblastoma
and contributes to loss of tumor immune surveillance inthese patients [9,10].
In the last 10 years a lot of data have been collectedby in vitro studies investigating TGF-b2 secretion indifferent tumor cell lines [2,7,9,11]. Little is known aboutin vivo plasma concentrations of TGF-b1 and TGF-b2in patients suffering from glioblastoma.
TGF-b2 has been detected in tumor cysts and incerebrospinal fluid of patients with glioma [12,13]. Asyet, there are no systematic studies on the concentrationof active and latent forms of TGF-b in the plasma ofpatients harboring intracerebral tumors.
In the present study, the concentrations of TGF-b1and TGF-b2 isoforms in plasma of patients with glio-blastoma before and after extensive resection wereanalyzed and related to survival.
Materials and methods
Subjects
Plasma samples from 21 patients with glioblastoma (8female and 13 male; mean age 58.4 years, range from 27
Journal of Neuro-Oncology (2006) 79: 61–65 � Springer 2006DOI 10.1007/s11060-005-9116-7

to 83 years) were analyzed. The histological investigationof the tumors identified a glioblastoma multiforme.Seventeen patients were operated by an extendedmicrosurgical tumor resection. In four cases the neuro-surgical intervention was a biopsy, which was performedin three cases using stereotaxy. A medication of dexa-methasone (12 mg/day) was preoperatively applied to 14patients. The blood samples were collected 1 day beforeand 7 days after the intracranial operation.
Moreover, plasma samples were taken from 19 pa-tients with clinically defined multiple sclerosis (MS) andfrom 26 healthy subjects (normal control group).
Blood sample collection
About 10 ml citrate blood samples were collected frompatients with glioblastoma, MS and from healthy con-trol probands. The blood was centrifuged not later than20 min after sampling, platelet-poor citrate plasma wasprepared using a standardized two-step-separationmethod and the samples were stored at )70 �C [14].
TGF-b1 and TGF-b2 ELISA
In the plasma samples active and latent forms of TGF-b1and TGF-b2 were determined by specific ELISA systems,as described by Danielpour [15] and Szymkowiak et al.[16]. For differentiation between active and latent TGF-b,samples were tested before and after transient acidificat-ion (reduction of the pH to 1.5 by addition of 5 NHCl for30 min at 37 �C with 1.4 N NaOH in 0.7 M Hepes)[14,17].
Statistical analysis
The T-test for independent samples and for pairedsamples as well as the Cox regression test were per-formed using the computer program SPSS 10.07 (SPSSInc., Chicago, USA). Plasma levels were correlated withsurvival after surgery.
Results
To study the role of the immunosuppressive cytokineTGF-b in patients harboring intracerebral tumors, theconcentrations of TGF-b1 and TGF-b2 were measuredin the plasma of patients with glioblastoma before andafter extensive resection. As shown in Table 1, the levelof latent TGF-b1 in the plasma of patients with glio-blastoma prior to surgery (5.7±4.2 ng/ml ) was signifi-
cant higher in comparison to healthy control probands(3.0±2.0 ng/ml, P = 0.01) but in the range of theconcentrations in the plasma of patients with MS(6.58±1.66 ng/ml). The mean value of active TGF-b1 inplasma of patients with glioblastoma was 0.6±2.3ng/ml, in the contrast to the plasma of the controlgroup, in which the active form could not be found.Moreover, the concentrations of latent TGF-b2 in theplasma of patients with glioblastoma were significantlyhigher than in the plasma of normal control probandsand of patients with MS (P<0.001). As shown inTable 1, the mean value of all 21 glioblastoma patientswas 38.9±11.4 ng/ml in comparison to 16.9±4.4 ng/mlfor healthy controls and 14.40±1.69 ng/ml for patientswith MS.
Interestingly, the plasma concentrations of latentTGF-b2 were significantly higher prior to surgery in95% of the patients with glioblastoma (20 of 21patients) as compared to the control group. The meanvalue in the group of patients preoperatively applieddexamethasone was 37.9 ng/ml in comparison to47.7 ng/ml in the group of patients without steroids.This difference was not significant.
Active TGF-b2 was detectable in the plasma of 16 ofthe 21 glioblastoma patients. The mean concentrationwas 0.17±0.16 ng/ml. In the plasma of the normalcontrols no active TGF-b2 could be detected at all. Thisdifference was highly significant as well (P<0.001).
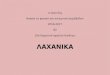
In 17 patients with glioblastoma, which were treatedby an extended tumor resection, concentrations of TGF-b could be determined 1 day prior to and 7 days aftersurgery. In 14 out of 17 patients (82.4%) the concen-tration of latent TGF-b2 significantly dropped within7 days after surgery without reaching the ‘normal’ range(concentration of the control group). The mean value ofthese 17 patients fell from 40.6±10.2 ng/ml prior tosurgery to 34.6±8.7 ng/ml after surgery (Figure 1). Thisreduction of the mean level of latent TGF-b2 was highlysignificant (P = 0.001).
This difference of plasma levels obtained prior to andafter surgery was not significant for active TGF-b2 (priorto = 0.16±0.17 ng/ml vs. after = 0.12±0.13 ng/ml),latent TGF-b1 (prior to = 6.0±4.6 ng/ml vs. after =6.1±6.7 ng/ml) and active TGF-b1 (prior to =0.7±2.6 ng/ml vs. after = 0.2±0.18 ng/ml).
Because of difficulties in obtaining survival data, thecorrelation between survival and TGF-b concentrationswas only evaluated in 17 cases of patients with glio-blastoma. The correlation between increasing survivaland plasma levels of latent forms of TGF-b2 obtainedprior to surgery was significant. In the Cox regression
Table 1. Plasma concentrations of TGF-b1 and TGF-b2 (mean value±SD) of patients with glioblastoma, with multiple sclerosis and of healthy
control probands as well as the comparison of the TGF-b concentrations in glioblastoma patients to each other (T-test for independent sample)
Active TGF-b1 (ng/ml) Latent TGF-b1 (ng/ml) Active TGF-b2 (ng/ml) Latent TGF-b2 (ng/ml)
Glioblastoma, n = 21 0.60±2.3 5.7±4.2 0.17±0.16 38.9±11.4
Multiple sclerosis, n = 19 n.d. 6.58±1.66 n.d. 14.40±1.69
Healthy control, n = 26 0 3.0±2.0 0 16.9±4.4
Glioblastoma vs. multiple sclerosis n.d. Not elevated n.d. Elevated P<0.001
Glioblastoma vs. healthy control Elevated P<0.001 Elevated P=0.01 Elevated P<0.001 Elevated P<0.001
n.d.=not determined.
62
the level of significance was determined at P = 0.006. Aweak relation was determined between long survival andlow concentration of the latent form of TGF-b1 prior tosurgery (P = 0.06). The latent form of TGF-b2 aftersurgery, the active form of TGF-b1 or TGF-b2 prior toand after surgery, and the latent form of TGF-b1 aftersurgery were all not significantly correlated with survival(data not shown).
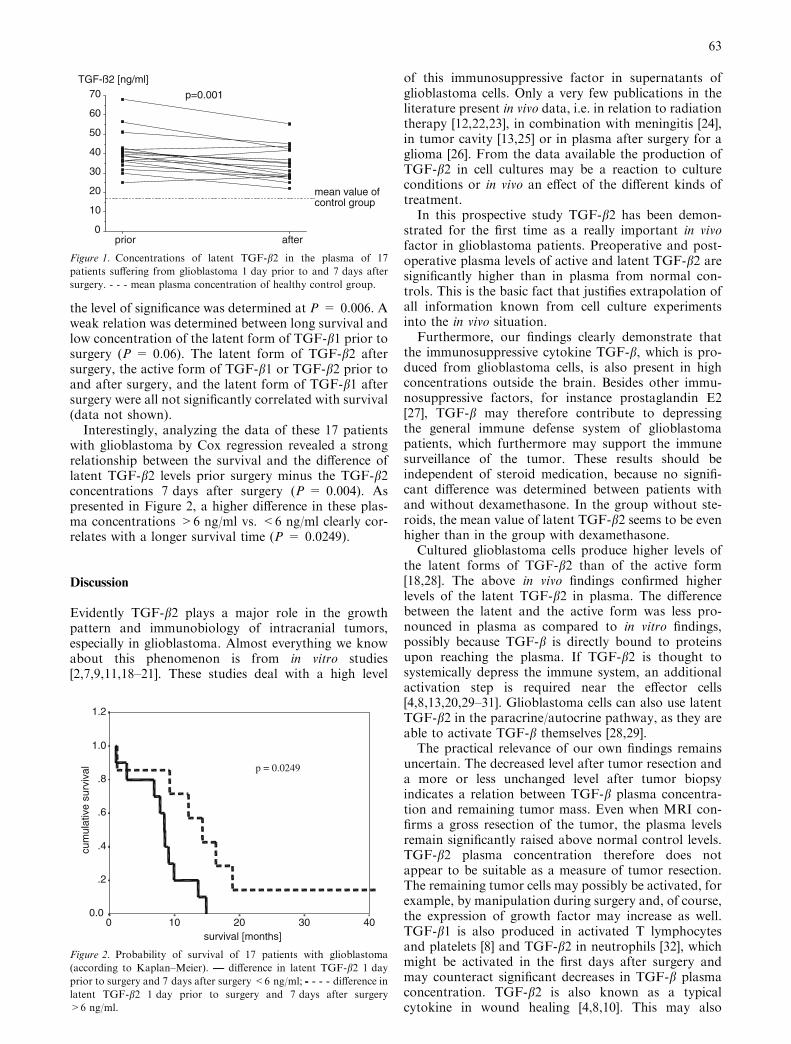
Interestingly, analyzing the data of these 17 patientswith glioblastoma by Cox regression revealed a strongrelationship between the survival and the difference oflatent TGF-b2 levels prior surgery minus the TGF-b2concentrations 7 days after surgery (P = 0.004). Aspresented in Figure 2, a higher difference in these plas-ma concentrations >6 ng/ml vs. <6 ng/ml clearly cor-relates with a longer survival time (P = 0.0249).
Discussion
Evidently TGF-b2 plays a major role in the growthpattern and immunobiology of intracranial tumors,especially in glioblastoma. Almost everything we knowabout this phenomenon is from in vitro studies[2,7,9,11,18–21]. These studies deal with a high level
of this immunosuppressive factor in supernatants ofglioblastoma cells. Only a very few publications in theliterature present in vivo data, i.e. in relation to radiationtherapy [12,22,23], in combination with meningitis [24],in tumor cavity [13,25] or in plasma after surgery for aglioma [26]. From the data available the production ofTGF-b2 in cell cultures may be a reaction to cultureconditions or in vivo an effect of the different kinds oftreatment.
In this prospective study TGF-b2 has been demon-strated for the first time as a really important in vivofactor in glioblastoma patients. Preoperative and post-operative plasma levels of active and latent TGF-b2 aresignificantly higher than in plasma from normal con-trols. This is the basic fact that justifies extrapolation ofall information known from cell culture experimentsinto the in vivo situation.
Furthermore, our findings clearly demonstrate thatthe immunosuppressive cytokine TGF-b, which is pro-duced from glioblastoma cells, is also present in highconcentrations outside the brain. Besides other immu-nosuppressive factors, for instance prostaglandin E2[27], TGF-b may therefore contribute to depressingthe general immune defense system of glioblastomapatients, which furthermore may support the immunesurveillance of the tumor. These results should beindependent of steroid medication, because no signifi-cant difference was determined between patients withand without dexamethasone. In the group without ste-roids, the mean value of latent TGF-b2 seems to be evenhigher than in the group with dexamethasone.
Cultured glioblastoma cells produce higher levels ofthe latent forms of TGF-b2 than of the active form[18,28]. The above in vivo findings confirmed higherlevels of the latent TGF-b2 in plasma. The differencebetween the latent and the active form was less pro-nounced in plasma as compared to in vitro findings,possibly because TGF-b is directly bound to proteinsupon reaching the plasma. If TGF-b2 is thought tosystemically depress the immune system, an additionalactivation step is required near the effector cells[4,8,13,20,29–31]. Glioblastoma cells can also use latentTGF-b2 in the paracrine/autocrine pathway, as they areable to activate TGF-b themselves [28,29].
The practical relevance of our own findings remainsuncertain. The decreased level after tumor resection anda more or less unchanged level after tumor biopsyindicates a relation between TGF-b plasma concentra-tion and remaining tumor mass. Even when MRI con-firms a gross resection of the tumor, the plasma levelsremain significantly raised above normal control levels.TGF-b2 plasma concentration therefore does notappear to be suitable as a measure of tumor resection.The remaining tumor cells may possibly be activated, forexample, by manipulation during surgery and, of course,the expression of growth factor may increase as well.TGF-b1 is also produced in activated T lymphocytesand platelets [8] and TGF-b2 in neutrophils [32], whichmight be activated in the first days after surgery andmay counteract significant decreases in TGF-b plasmaconcentration. TGF-b2 is also known as a typicalcytokine in wound healing [4,8,10]. This may also
0
10
20
30
40
50
60
70 p=0.001
afterprior
mean value ofcontrol group
TGF-ß2 [ng/ml]
Figure 1. Concentrations of latent TGF-b2 in the plasma of 17
patients suffering from glioblastoma 1 day prior to and 7 days after
surgery. - - - mean plasma concentration of healthy control group.
survival [months]403020100
cum
ulat
ive
surv
ival
1.2
1.0
.8
.6
.4
.2
0.0
p = 0.0249
Figure 2. Probability of survival of 17 patients with glioblastoma
(according to Kaplan–Meier). —— difference in latent TGF-b2 1 day
prior to surgery and 7 days after surgery <6 ng/ml; -- - - - difference in
latent TGF-b2 1 day prior to surgery and 7 days after surgery
>6 ng/ml.
63

enhance the plasma level of TGF-b in the first days afterany surgical manipulation as well. Further studiesshould focus on a longer follow up of plasma levels.Future research should also clarify the diagnostic use-fulness of TGF-b2 levels to differentiate glioblastomafrom other intracranial lesions for example abscesses oranaplastic astrocytoma.
The correlation of TGF-b2 with survival has severalaspects. The longer survival with increasing plasma levelsof latent TGF-b2 is evidence that TGF-b2 itself has noserious harmful effect on life expectancy. Furthermore, itmay be concluded that a more dedifferentiated tumorloses its ability to control its growth pattern by increasedexpression of TGF-b. Only less aggressive tumors areable to increase the TGF-b production, demonstrated byhigher plasma levels of TGF-b in patients with longersurvival. In addition, the bigger the difference betweenTGF-b concentration prior to and after surgery, thelonger the survival period. There may be several expla-nations for this phenomenon: (a) Reduction of TGF-bcorrelates directly with reduction of tumor mass, whichseems to be a prognostic factor for survival [33]; (b) Ahigh reduction of TGF-b concentration in a very shorttime may impair further tumor growth and may supportthe immune system of the patients at least for a shorttime; (c) Only a small reduction of TGF-b in spite ofsignificant tumor reduction may indicate a lot ofunknown tumor cell clones outside the circumscribedtumor removed, not visible on MRI-scans, and respon-sible for the less favorable outcome.
In conclusion, this study suggests that glioblastomadoes secret TGF-b2 in vivo. TGF-b may play animportant role in glioblastoma patients. Further studiesshould focus on TGF-b as a target of immunological ormolecular biological therapy.
References
1. Brooks W, Netsky MG, Normansell DE, Horwitz DA: Depressed
cell mediated immunity in patients with primary intracranial
tumors. J Exp Med 136: 1631–1647, 1972
2. Kuppner MC, Hamou MF, Sawamura Y, Bodmer S, de Tribolet
N: Inhibition of lymphocyte function by glioblastoma-derived
transforming growth factor beta 2. J Neurosurg 71: 211–217, 1989
3. Darley R, Morris A, Passas J, Bateman W: Interactions between
interferon c and retinoic acid with transforming growth factor b in
the induction of immune recognition molecules. Cancer Immunol
Immunother 37: 112–118, 1993
4. Fontana A, Constam DB, Frei K, Malipiero U, Pfister HW:
Modulation of the immune response by transforming growth
factor beta. Int Arch Allergy Immunol 99: 1–7, 1992
5. Kehrl JH, Wakefield LM, Roberts AB, Jakowlew SB, Alvarez-
Mon M, Derynck R, Sporn MB, Fauci AS: Production of
transforming growth factor b by human T lymphocytes and its
potential role in the regulation of T cell growth. J Exp Med 163:
1037–1050, 1986
6. Kehrl JH, Roberts AB, Wakefield LM, Jakowlew SB, Sporn MB,
Fauci AS: Transforming growth factor beta is an important
immunomodulatory protein for human B-lymphocytes. J Immu-
nol 137: 3855–3860, 1986
7. Maxwell M, Galanopoulos T, Neville-Golden J, Antoniades HN:
Effect of the expression of transforming growth factor-b2 in pri-
mary human glioblastomas on immunosuppression and loss of
immune surveillance. J Neurosurg 76: 799–804, 1992
8. Roberts AB, Sporn MB: The transforming growth factor-bs. In:Sporn MB, Roberts AB (eds) Peptide Growth Factors and Their
Receptors (Handbook of Experimental Pharmacology). Springer
Verlag, Heidelberg, 1990, Vol 95, pp 419–472
9. Fontana A, Bodmer S, Frei K, Malipiero U, Siepl C: Expression
of TGF-beta 2 in human glioblastoma: a role in resistance to
immune rejection? Ciba Found Symp 157: 232–238, 1991
10. Bodmer S, Strommer K, Frei K, Siepl C, de Tribolet N, Heid I,
Fontana A: Immunosuppression and transforming growth factor-
b in glioblastoma. Preferential production of transforming growth
factor-b 2. J Immunol 143: 3222–3229, 1989
11. Jachimczak P, Hessdorder B, Fabel-Schulte K, Wismeth C, Brysch
W, Schlingensiepen K-H, Bauer A, Blesch A, Bogdahn U:
Transforming growth factor-b-mediated autocrine growth regu-
lation of gliomas as detected with phosphorothioate antisense
oligonucleotides. Int J Cancer 65: 332–337, 1996
12. Tada T, Yabu K, Kobayashi S: Detection of active form of
transforming growth factor-ß in cerebrospinal fluid of patients
with glioma. Jpn J Cancer Res 84: 544–548, 1993
13. Bodmer S, Huber D, Heid I, Fontana A: Human glioblastoma cell
derived transforming growth factor-beta 2: evidence for secretion
of both high and low molecular weight biologically active forms.
J Neuroimmunol 34: 33–42, 1991
14. Reinhold D, Bank U, Buhling F, Junker U, Kekow J, Schleicher E,
Ansorge S: A detailed protocol for the measurement of TGF-b1 in
human blood samples. J Immunol Methods 209: 203–206, 1997
15. Danielpour D: Improved sandwich enzyme-linked immunosorbent
assays for transforming growth factor b1. J Immunol Methods
158: 17–25, 1993
16. Szymkowiak CH, Mons I, Gross WL, Kekow J: Determination of
transforming growth factor b2 in human blood samples by ELISA.
J Immunol Methods 184: 263–271, 1995
17. Kekow J, Wachsman W, Mc Cutchan JA, Gross WL, Zachariah
M, Carson DA, Lotz M: Tranforming growth factor b and sup-
pression of humoral immune response in HIV infection. J Clin
Invest 87: 1010–1016, 1991
18. Constam DB, Philipp J, Malipiero UV, ten Dijke P, Schachner M,
Fontana A: Differential expression of transforming growth factor-
b 1, -b 2, and -b 3 by glioblastoma cells, astrocytes, and microglia.
J Immunol 148: 1404–1410, 1992
19. Helseth E, Unsgaard G, Dalen A, Vik R: The effect of type beta
transforming growth factor on proliferation of clonogenic cells from
human gliomas. Acta Neurochir Suppl Wien 43: 118–120, 1988
20. Olofsson A, Miyazono K, Kanzaki T, Colosetti P, Engstrom U,
Heldin CH: Transforming growth factor-beta 1, -beta 2, and -beta
3 secreted by a human glioblastoma cell line. Identification of
small and different forms of large latent complexes. J Biol Chem
267: 19482–19488, 1992
21. Sasaki A, Naganuma H, Satoh E, Nagasaka M, Isoe S, Nakano S,
NukuiH: Secretionof transforming growth factor-beta 1 and -beta 2
by malignant glioma cells. Neurol Med Chir Tokyo 35: 423–430,
1995
22. Gridley DS, Loredo LN, Slater JD, Archambeau JO, Bedros AA,
Andres ML, Slater JM: Pilot evaluation of cytokine levels in
patients undergoing radiotherapy for brain tumor. Cancer Detect
Prev 22: 20–29, 1998
23. Hulshof MC, Sminia P, Barten-Van Rijbroek AD, Gonzalez GD:
Prognostic value of plasma transforming growth factor-beta in
patients with glioblastoma multiforme. Oncol Rep 8: 1107–1110,
2001
24. Peterson PK, Chao CC, Hu S, Thielen K, Shaskan EG: Glio-
blastoma, transforming growth factor-beta, and Candida menin-
gitis: a potential link. Am J Med 92: 262–264, 1992
25. Ruffini PA, Rivoltini L, Silvani A, Boiardi A, Parmiani G: Fac-
tors, including transforming growth factor b, released in the
glioblastoma residual cavity, impair activity of adherent lympho-
kine-activated killer cells. Cancer Immunol Immunother 36: 409–
416, 1993
26. SablotzkiA,EbelH,Muhling J,DehneMG,NopensH,Giesselmann
H, Hempelmann G: Dysregulation of immune response following
neurosurgical operations. Acta Anaesthesiol Scand 44: 82–87, 2000
64

27. Couldwell WT, Dore-Duffy P, Apuzzo MLJ, Antel JP: Malignant
glioma modulation of immune function: relative contribution of
different soluble factors. J Immunol 33: 89–96, 1991
28. Naganuma H, Sasaki A, Satoh E, Sakihama T, Tasaka K, Nukui
H: Improved bioassay for the detection of transforming growth
factor-b 1 and b 2 in malignant gliomas. Neurol Med Chir (Tokyo)
34: 143–149, 1994
29. Huber D, Philipp J, Fontana A: Protease inhibitors interfere with
the transforming growth factor-ß-dependent but not the trans-
forming growth factor-ß-independent pathway of tumor cell-
mediated immunosuppression. J Immunol 148: 277–284, 1992
30. Lyons RM, Keski-Oja J, Moses HL: Proteolytic activation of
latent transforming growth factor-b from fibroblast-conditioned
medium. J Cell Biol 106: 1659–1665, 1988
31. Miyazono K, Heldin CH: Role for carbohydrate structures in
TGF-b1 latency. Nature 338: 158–160, 1989
32. Szymkowiak CH, Csernok E, Reinhold D, Bank U, Gross WL,
Kekow J: Neutrophils synthesize and activate TGFbeta2. Cyto-
kine 12: 397–400, 2000
33. Nazzarro JM, Neuwelt EA: The role of surgery in the managa-
ment of supratentorial intermediate and high grade astrocytoma in
adults. J Neurosurg 72: 408–417, 1990
Address for offprints: Thomas Schneider, Department of Neurosurgery
Otto-von-Guericke University, Leipziger Strasse 44, 39120 Magde-
burg, Germany; Tel.: +49-391-6715534; Fax: +49-391-6715544;
E-mail: [email protected]
65












![Mosul - Journals · 2020-06-06 · _____ 2010(18) 4%אמאא א [5] xt = β1 xt-1 + β2 xt-2 + … + βp xt-p + ut …(2) لﺜﻤﺘ ﻱﺃ)Autoregressive Parameters ﻲﺘﺍﺫﻟﺍ](https://img.pdfslide.tips/doc/110x75/5f2545d376880b0ef4609d43/mosul-journals-2020-06-06-201018-4-5-xt-1-xt-1-2.jpg)