Embed Size (px)
Citation preview

Interesting case conference
นำ��เสนำอ โดย พ. อรนำ�ช ศร�สวั�สด�� พ. กมลทิ�พย� ประสพส�ขควับค�มโดย อ. วัรวั�ธ ล�ภพ�เศษพ�นำธ�� วั�นำทิ�! 5 ม�ย. 2546 เวัล�7.30 นำ

Interesting case conference
ID : ผู้#$ป%วัยหญิ�งไทิยค#* อ�ย� 79 ป+ อ�ช�พ คนำชร� ภ#ม�ล��เนำ� อ. ป%�ซ�ง จ. ล��พ#นำ เช./อช�ติ� ไทิย ส�ญิช�ติ�
ไทิยCC : ปวัดทิ$อง3 วั�นำก*อนำม�โรงพย�บ�ลPI : -2 เด.อนำก*อนำม�โรงพย�บ�ล เร�!มม�อ�ก�รปวัดทิ$อง คล��ก$อนำได$ทิ�!ทิ$อง ปวัดบร�เวัณก$อนำติลอดเวัล� ไปพบแพทิย�ทิ�!โรงพย�บ�ลล��พ#นำ ,u/s พบม� large
abdominal aortic aneurysm just below renal arteries
to biforcation but no evidence of dissection

Interesing case coference
Dx. Abdominal aortic aneurysm โรงพย�บ�ลล��พ#นำ conservative treatment ม�ติลอด
- 3 วั�นำก*อนำม�โรงพย�บ�ลผู้#$ป%วัยม�อ�ก�ร ปวัดบร�เวัณก$อนำ ติ��แหนำ*งเด�ม แติ*ม�อ�ก�ร ปวัดม�กกวั*�เด�ม ไปพบแพทิย�รพ.ล��พ#นำ
ให$ก�รร�กษ�โดยให$ย�แก$ปวัด อ�ก�รไม*ด�ข5/นำ จ5งส*งติ�วัม�ร�กษ�ติ*อทิ�!รพ. มห�ร�ชนำคร
เช�ยงใหม*

Interesing case conference
PH : ปฏิ�เสธ underlying disease
ม�ประวั�ติ� chronic smoking ปฏิ�เสธ ประวั�ติ� alcoholic
drinking ปฏิ�เสธประวั�ติ�แพ$ย� เคยผู้*�ติ�ด ใส$ติ�!งอ�กเสบ 30 ป+
ก*อนำ

Interesing case conference
Physical examination V/S : BP=170/100 in all extermities PR=74/min ,
Temp=36.5C ,RR=15/min General appearance : an old woman with normal
conciousness body weight =30 kgs ,height=145
cm HEENT : no pale conjunctiva ,no
juandice

Interesting case conference
Heart : normal heart sounds,regular rhythm , no murmur
Lung : normal contour, no tachypnea normal breathing sounds Abdomen : pulsatile mass ขนำ�ดประม�ณ 4cm*4cm just below umbilicus , no abdominal
distension BS active Extremities : no deformity,normal pulse in all
extremities

Interesting case conference
Airway assessment Interinciser gap > 3 cm thyromental distance >5
cm mal l ampati
cl assi fi cati on : I I neck movement : no
limitation

Interesting case conference
Impression : Abdominal aortic
aneurysm with impendingrupture

Interesting case conference
Work up CBC : Hb = 13.5 g% Hct=42.3 Wbc=7300 Plt =212000 Electrolyte : Na =126 K=3.4 Cl =93 CO2=24 BUN=5 Cr =0.6 FBS =132

Interesting case conference
Work up ( Cont. ) PT=10.3(11.8) ,
PTT=31.4(31.0) Ca =9.5 , Mg=1.28 , P=2.8
UA: Sp.gr. 1.010 , Wbc = 8-10/HPF
Rbc = 1-3/HPF

Interesting case conference
Work up( Cont. ) CXR: widening mediastinum
R/O Thoracic aortic aneurysm
EKG : inverted T in V1 -V3
Trop T : negative CT abdomen :

Interesting case conference
Set OR emergency for aneurysmorhappy ร�บ set case เวัล� 1630. นำ . วั�นำทิ�! 25/05/03
NPO time เวัล� 900. นำ. วั�นำทิ�! 25/05/03

Interesting case conference
Problem list 1. Infrerenal AAA 2. Old age 3. Hyponatremia 4. R/O HT 5. Widening mediastinum R/O
Thoracic aneurysm 6. Abnormality of EKG 7. Moderate renal insufficiency

Interesting case conference
Anesthetic consideration 1. P reoperative evaluation 2 . Preoperative preparation
& 3 . Mornitoring 4 . Anesthetic technique 5 . Intraoperative complication 6 . Postoperative care

Interesting case conference
1. Preoperative evaluation LLLLLLLLLL LLLL LLL LLLL LLL LLLLL LLLLLLLLLLL L L LLL:
LLLLLLLL BUN ,Cr : CCr =33.9 Coagulation profile

Interesting case conference
Urine analysis CXR : Widening
mediastinum EKG : Inverted T 2. Preoperative preparation
& Premedication Cross maching No premedication

Interesting case conference
3. Mornitoring LLLLLLLLLL2
LLLL EKG
LLL L- LLLL

Interesting case conference
3. Mornitoring (cont.) Temp I/O 4. Anesthetic technique LLLLLLL LLLLLLLLLL
LLLLLLLLL LLLL L LLLLLL LLLLLLLL LLL LL,
l anti l e agent

Interesting case conference
4. Anesthetic technique ( Cont.) LLLLLLLLL L LLLLLLLLLLL LLLLLL 5. Intraoperative complication 6. Post operative care Pain control

Abdominal aortic aneurysm
L LLLLLLLLLLLL LLLLLLLLL L LL;,, ,LLLLLLLL LLL LLLLLLLLLLL
LLLLL LLLLLLLLLL LLLLL LL LLLLLLLLLLLLLLL
LLLLL LL LLL LLLLLLL LLLLLLL LLLLLLL , infection, syphilis, Marfan syndro
LL

The diameter and rate of expansion of AAA
AAA 4 to 5 cm. In diameter is not w ell defined , and significant controve rsy exists regarding surgical repair
Surgical repair is recommened if s uch aneurysms become symptomati
-c , expand more than 0.5 cm. In a 6 month period , diameter 5 cm. or gre
ater

Aortic cross- clamping Most abdominal aortic
reconstruction require clamping at the infrarenal level
Ischemic complication may result i n renal failure , hepatic ischemic an d coagulopathy
Thoracic and supraceliac cros- s clamping may increase left ventri
cular wall stress ( resultant acute l eft ventricular dysfunction and/or
myocardial ischemia )

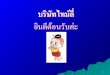
ภาพ systemic hemodynamic response to aortic cross-clamping

Physiologic changes (cross-clamping ) Hemodynamic changes ;
increase arterial blood pressure
increase left ventricular wall tension and seg mental wall motion abnormalities
increase pulmonary artery occlusion pressure
increase central venous pressure
increase coronary blood flow
decrease cardiac output and ejection fraction
decrease renal blood flow

Metabolic changes decrease total body oxygen consumpti
on decrease total body carbon dioxide pro
duction decrease total body oxygen extraction increase mixed venous oxygen saturat
ion increase epinephrine and norepinephri
ne respiratory alkalosis metabolic acidosis

Therapeutic interventions (cross-clamping)
Afterload reduction ; sodium nitroprusside , inhalation anestheti
cs , amrinone Preload reduction ; nitroglycerine ,
shunts and left heart bypass Renal protection ; Mannitol , low do
se dopamine , fluid administration Other ; decrease minute
ventilation , sodium bicarbonate

Aortic unclamping
The hemodynamic responses to unclamping depend on the level of aorti
c occlusion, the total occlusion time, th e use of diverting support and the intra
vascular volume Humoral factors and mediators which m
ay also play a role in organ dysfunction after aortic occlusion include lactic acid
- -, renin angiotensin, oxygen free radical s, neutrophil, prostaglandins, activated
-complement, cytokines and myocardial depressant factors

ภาพ aortic unclamping

Physiologic changes ( aortic unclamping )
Hemodynamicschanges ; decrease myocardial
contractility decrease arterial blood press
ure decrease central venous pres
sure decrease venous return decrease cardiac output

LLLLLLL L; i ncr ease t ot al body oxygen co
LLLLLLLLL LLLLLLLLLLLLLLL , ,
activated complement , myocardia- l depressant factors
LLLLLLLL LLLLL LLLLLL LLLLLL LLLLLLLLLL
LLLLLLLLL LLLLLLLL

Therapeutic interventions (aortic unclamping )
LLLLLLLL LLLLLLLLLL LLLLLLLLLLL
LLLLLLLL LLLLLLLLLLL increase fluid administration LLLLLLLL LLLLLLLLLLLLLLL
LLLLL - reapply cross clamp for severe hy
LLLLLLLLL

Anesthetic management
Preoperative considerations High incidence of coexistent cardiac, re
nal, pulmonary disease, hypertension, diabetes
Severe hypertension, myocardial ische mia, aortic valve regurgitation, left ventr
icular failure may be precipitated The location of the lesion The procedure of complicated by the po
tential for large intraoperative blood los ses

Intraoperative monitoring central venous or pulmonary artery c
atheter direct arterial blood pressure and NIB
P - two lead ECG or modified V5 ECG temperature I/O pulse oximetry - two dimensional TEE

Anesthetic drugs and techniques
Combined techniques most commonly employ a lumbar or lo
w thoracic epidural catheter Induction of general anesthesia
should controll such that stable hemodynamics are maintained d
uring loss of conciousness, laryn goscopy and intubation , the im mediate postinduction period

Induction, intravenous hypnotic agents ( t hiopentone , etomidate, propofol ) or a sho
- rt acting potentopioid ( such as fentanyl- 3 8 microgram/kg) and halogenated age
nts may be admi ni steredi n l owconcentr ati onbefore i ntubati on
- - - - Esmolol(1025mg),sodiumnitroprusside(525microgram),nitroglycerine(50100microgram),andphenylephrine(50100microgram)shoul dbL LLLLLLLLL LLL LLLLL LLLLLLLLLLLLLL L
uri ngi nducti on Anestheti c mai ntenance may be
accompl i shedwi tha combi nati onof a p otent opi oi dandani nhal edanestheti c

Epidural local anesthetics are used the same balanced technique and reduce t
he opioid dose ( but avoiding significa nt hypotension at the time of aortic un
clamping) Extubation of the trachea is generally
not attempted in patients with suprac - eliac aortic cross clamp times greater than 30 minutes, patients with poor ba
seline pulmonary function , or patients requiring large volumes of blood or cry
stalloid during surgery

Routine use nasal airway afte r induction but before systemic
heparinization in all patients fo r whom extubation is planned
Hypertension and tachycardia are aggressively controlled dur -ing emergence by use of short
acting agents , such as esmolol , nitroglycerine, and sodium nit
roprusside