Embed Size (px)
Citation preview

Interhospital Conference15/05/2012
Division of Hematology Oncology, Department of Pediatrics,
Faculty of Medicine, Khon Kaen University
• เดกชายไทย อาย 9 ป 3 เดอน• ภมล าเนา อ. กมลาไสย จ. กาฬสนธ•Admit 15/02/12-23/03/12•Chief complaint : ไข 20 วน

Present illness
20วน กอนมารพ. ผปวยมไขสง ตวรอน เหงอออกมาก มารดาไดใหรบประทานยาลดไข ยงมไขทกวน
16วน กอนมารพ. ยงมไขสง ไปรพ.และนอนรกษาตวทรพ.ไดยา ceftriaxone 4วน และ doxycycline 2วน ไขลดลง จงออกจากรพ.
12วน กอนมารพ. หลงจากกลบบานไป2วน มไขสงขนมาอก ลกษณะเปนเชนเดม มารดาจงพาไปรพ. ไดยาceftazidime 5 วน และ doxycycline 3 วน ตรวจไมพบสาเหต อาการไมดขน จงสงตวมาท รพ.ศรนครนทร

Past history• โรคประจ าตว asthma ตดตามการรกษาทรพ.ศรนครนทรเปนประจ า• ไมแพยา ไมเคยผาตด• แตกอนตอนเดกๆเปนหวดบอยๆ แตพอเรยนชนประถมสขภาพแขงแรงด ไมมอาการหอบ เปนหวดนานๆครง
• เคยเปน TB lymph nodes ตอนอาย 9 เดอน• เปนบตรคนท2 มพสาว1คน คลอดปกต ไมมภาวะแทรกซอนระหวางคลอด

Past history• พฒนาการปกต ก าลงศกษาอยชน ป.3 ผลการเรยนด• ไดรบวคซนครบ• ไมมประวตเขาปา/ลยน า• อยทบานไมมสตวเลยง• ไมเคยไดรบเลอดมากอน

Family history• ปฏเสธโรคประจ าตว โรคมะเรงในครอบครว• บดามารดารบราชการ• คนในครอบครวไมมประวตไอเรอรง ปาทอยขางบานมประวตไอเรอรงแตไมเคยตรวจ
• ทกคนในครอบครวไดท าเอกซเรยปอดแลว ผลปกต

ขอมลเพมเตม
• ไขเฉพาะตอนกลางคน ตอนกลางวนมกจะไมมไข ไมมน ามก ไมไอ ไมปวดศรษะ ตาไมแดง ไมมแผลหรอผนตามรางกาย ไมปวดขอ ปสสาวะและ อจจาระปกต ตอนกลางวนเลนได ไมเบออาหาร ไมน าหนกลด
• ปจจบน on seretide(125/25) 2 puff bid, singulair(5) 1tab oral pc เชา เคยได oral prednisolone (5) ป 2548 2tabs oral bid 5 วน
• TB lymph nodeรกษาหายแลว (ตอนนนมตอมน าเหลองโตทรกแรดานซาย ไดกนยา INH 9 เดอน)

ขอมลเพมเตม
• ยายเคยเปนวณโรค รกษาหายแลว และเสยชวตกอนทผปวยจะเกด• เคยไปเทยวถ าทมคางคาวเมอ2ปกอน• แถวบานมนกพราบ มมากตามระเบยงบานและซอกหลงคา ผปวยไมไดเลนใกลชดนก

Physical examinationA thai boy, fully consciousnessVital signs: BT 38.4oC, PR 112/min,
RR 22/min, BP 110/69 mmHgBW 30 kg.(P50-75) , Ht 134 cm.(P50-75)
HEENT: pink conjunctivae , anicteric sclerae, no oral ulcer,not tender at sinus area, pharynx & tonsils were not injected, cervical and supraclavicular lymph nodesimpalpable, no thyroid gland enlargement , no discharge per nose/ears/eyes
Physical examinationHeart: regular HR, no active precordium,
no heaving, no thrill , normal S1S2, no murmur
Lungs : trachea in midline, equal lungs expansion ,normal breath sound, no adventitious sound
Abdomen : soft, not tender, impalpable liver, spleen just palpable, no mass, active bowel sound

Physical examination
Ext.: no edem , no rash, no lymphadenopathyno joint swelling/tender, no clubbing finger
Neurological examination: E4V5M6, pupil 2 mm. react to light both eyes, no stiffneckCN: all intactMotor power: grade 5 allsensation: intact , DTR: 2+all

Problem lists

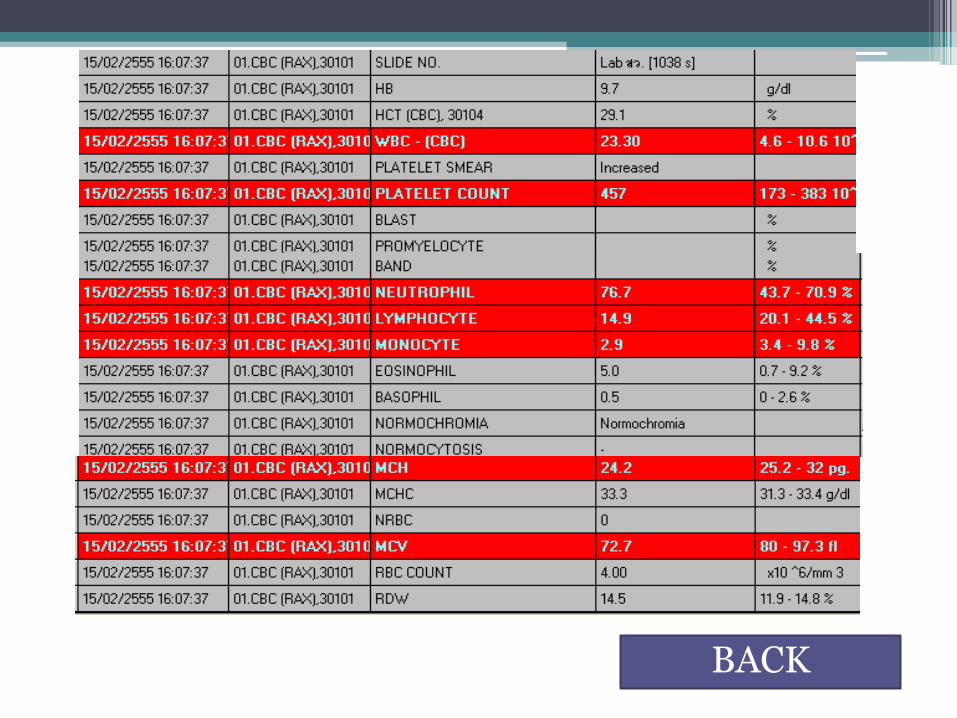
Investigation

BACK
BACK

UA
• UA: yellow, clear, sp.gr. 1.023,pH 6.0
Glu, Ket, Blood, Alb : neg, WBC 1-2/HF
BACK

stool
• Stool exam: brown, soft, mucous& gross blood neg, parasite not seen
• Stool AFB 3 days: no acid fast bacilli found• Stool conc. 3 days: not found parasite
BACK

CRP and ESR
• CRP – QL positive
• CRP – QT 84.3• ESR 86 mm/hr.
BACK

• ANF/ANA by IFA(15/02/12): negative/but positive for cytoplasmic pattern(filament) 1:80
• Anti DSDNA: negative• Rheumatoid factor: negative
BACK

• Murine typhus IgM: positive
• Scrub typhus IgM: negative
• Murine typhus(IFA): positive• Scrub typhus(IFA): negative
BACK

• Direct antiglobulin test: positive 2+
• Antibody screening test: negative
• Melioid titer: 1:320
BACK

BACK

•H/C (15/02/12): NG•Anti-HIV: non reactive
BACK

Bone marrow
•BMA (23/02/12): no evidence of leukemia•Bone marrow culture: NG

Flow cytometry
• Blast gate:3.49% of total event, Granulocyte gate:71.1%
• Myeloid associated markerMPO positive 98.6%, CD 33 positive 52.4%CD11b positive 88.2%, CD64 positive 93.1%CD 15 positive 98.6%, CD13,117,61,GPA neg
• Lymphoid associated markers B cell type: CD19 neg
• Lymphoid associated markers T cell type: CytoCD3 neg , CD7 neg

Flow cytometry
• Others: CD34 neg, HLA-DR neg
• Cytochemistry staining: not done
• Interpretation/comments: blast gate 3.49%, immunophenotypic displays above markers expression on granulocyte gate, no evidence of acute leukemia
Flow cytometry
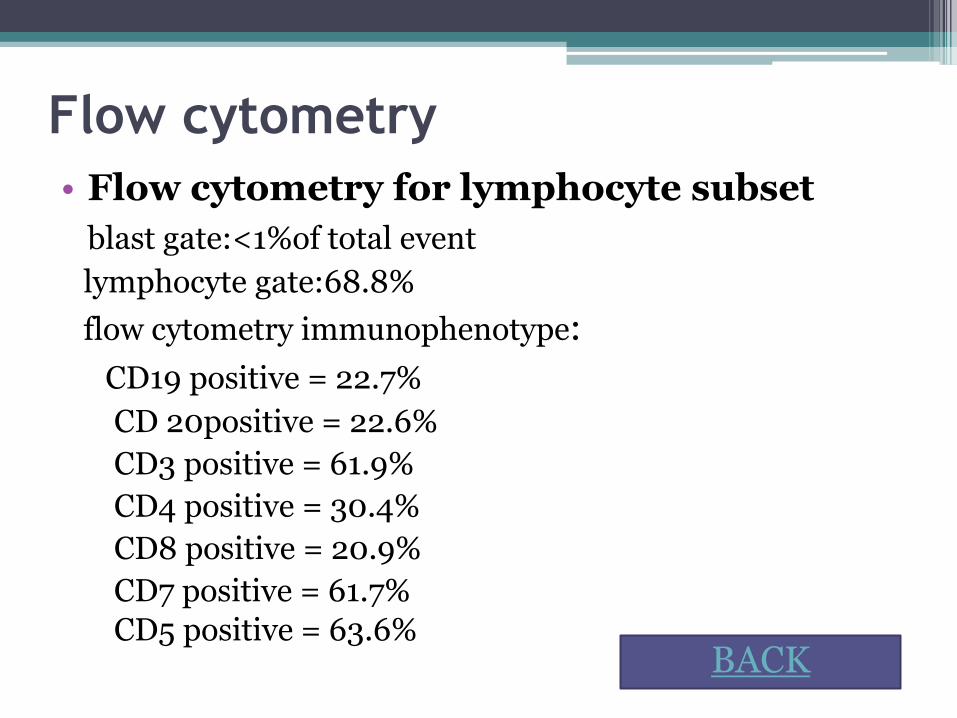
• Flow cytometry for lymphocyte subset
blast gate:<1%of total event
lymphocyte gate:68.8%
flow cytometry immunophenotype:
CD19 positive = 22.7%
CD 20positive = 22.6%
CD3 positive = 61.9%
CD4 positive = 30.4%
CD8 positive = 20.9%
CD7 positive = 61.7%
CD5 positive = 63.6%BACK


CHEST FILM; PA UPRIGHT AND LATERAL VIEW
FINDINGS;Rotational and poor inspiration film is obtained.Soft tissue density lesions at both hilar regions are found, hilarlymphadenopathy is likely.Interstitial infiltration at both perihilar regions is noted.Normal heart size is detected.Costophrenic angles are clear bilaterally.Bony thorax and soft tissue are unremarkable.IMPRESSION; Primary tuberculosis is likely. BACK



Paranasal sinus
BACK


ULTRASONOGRAPHY OF UPPER ABDOMEN
IMPRESSION: - Multiple lymph nodes at celiac trunk, periportal, paraaortic and mesenteric region; lymphoma is DDx. - Mild dilatation of intrahepatic bile duct in both lobe of liver due to partially obstruction from periportal lymph node is possible.- Mild diffuse thickened of gallbladder wall .- Mild splenomegaly.- Hydronephrosis of left kidney without demonstrated cause of obstruction.- Tiny amount of ascites.
BACK


CT SCAN OF WHOLE ABDOMEN TECHNIQUE :Pre and post contrast MDCT of whole abdomen.FINDINGS :-Hypodense along bilateral periportal region are observed, periportalcongestion.-No liver mass is detected.-Severe splenomegaly with multiple ill-defined hypodense lesion scattered in the spleen are found.-Multiple intraabdominallymphadenopathy are shown. Some necrotic lymph nodes at celiac region are noted.-Pancreas, kidneys, adrenal glands and urinary bladder appears normal.-Minimal ascites is found.-Both basal lungs are clear.IMPRESSION :-Multiple intraabdominal lymphadenopathy with splenic involvement ; Lymphoma is suspected.
BACK

•EL and intraabdominal LN biopsy (28/02/12)•Finding : malted enlarge mesenteric lymph nodes ,
liver congested , enlarge spleen , clear ascites fluid

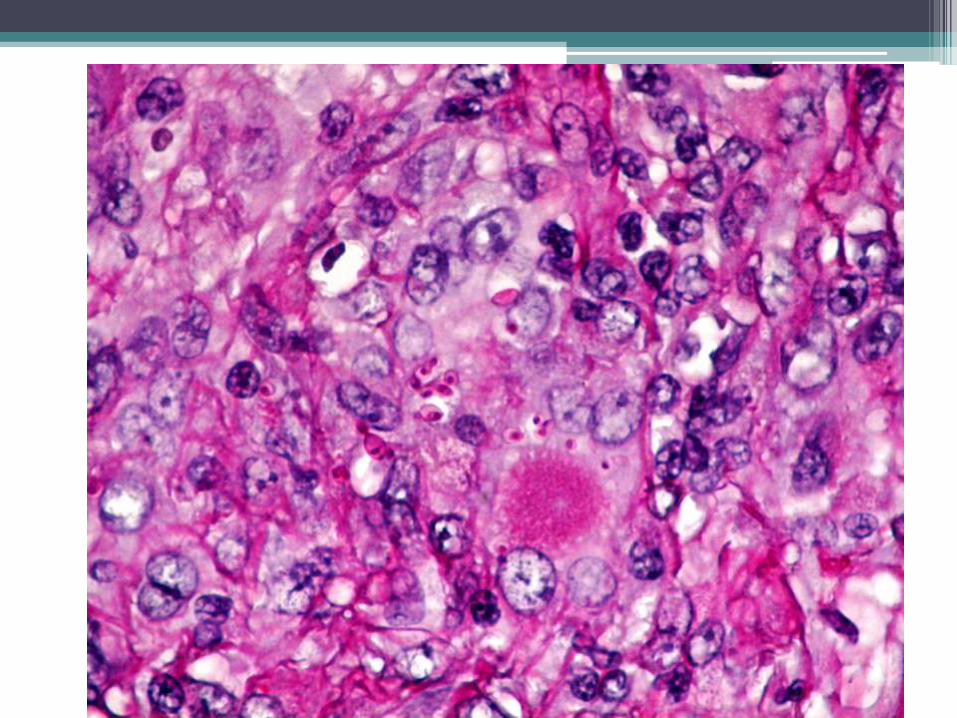
Pathology; lymph node
•Lymph node,mesenteric,biopsy : suggestive of histoplasmosis
Note : AFB stain reveals no acid fast bacilli
BACK










Treatment
• Amphotericin B 30 mg + 5%DW 100ml
IV drip in 4 hr OD (09/03/12-22/03/12) ไขลงด และ D/C 23/03/12

Histoplasmosis
• Histoplasma capsulatum is a dimorphic fungus that remains in a mycelial form at ambient temperatures and grows as yeast at body temperature in mammals.
• The soil in areas endemic for histoplasmosis.
• Highly infectious soil is found near areas inhabited by bats and birds.
• Birds cannot be infected by the fungus and do not transmit the disease.

• Most individuals with histoplasmosis are asymptomatic.
• Those who develop clinical manifestations are usually immunocompromised or are exposed to a high quantity of inoculum.
• Histoplasma species may remain latent in healed granulomas and recur, resulting in cell-mediated immunity impairment.

• Conversion from the mycelial to the pathogenic yeast form occurs intracellularly.
• Proposed theories suggest that the yeasts may produce proteins that inhibit the activity of lysosomal proteases.

Presentations
• Acute pulmonary histoplasmosis
• Chronic pulmonary histoplasmosis
• Progressive disseminated histoplasmosis

Treatment
• therapy with itraconazole for 6-12 weeks.
• In patients with prolonged symptoms (>4 wk) or those with overwhelming pulmonary involvement
• Response to therapy should be monitored via chest imaging
• Patients should be monitored for several years after treatment for possible relapse
Treatment
• Patients with severe infection should be treated with amphotericin B for 1-2 weeks;
• the patient is stable, amphotericin B may be changed to itraconazole and should be continued for 1 year.
• Patients with acute respiratory distress symptoms may require methylprednisone for 1-2 weeks.