Embed Size (px)
DESCRIPTION
nota
Citation preview

Definition
An Intracranial Aneurysm is a dilation of the walls of a cerebral artery that develops as a result
of weakness in the arterial wall.
Contents
Causes
Clinical Manifestations
Assessment and Diagnostic Methods
Medical Management
Nursing Assessment
Nursing Diagnoses
Potential Complications
Planning and Goals
Nursing Care Plans
Nursing Interventions
o Improving Cerebral Tissue Perfusion
o Relieving Sensory Deprivation
o Monitoring and Managing Potential Complications
o Teaching Patients Self Care
o Continuing Care
Evaluation
o Expected Patient Outcomes
See Also
Causes
Its cause is unknown, but it may be due to atherosclerosis, a congenital defect of the vessel walls,
hypertensive vascular disease, head trauma, or advancing age. Most commonly affected are the
internal carotid, anterior or posterior cerebral, anterior or posterior communicating, and
middle cerebral arteries.
Symptoms are produced when the aneurysm presses on nearby cranial nerves or brain tissue or
ruptures, causing subarachnoid hemorrhage.
Prognosis depends on the age and neurologic condition of the patient, associated diseases, and
the extent and location of the aneurysm.
Clinical Manifestations
Neurologic deficits (similar to those of ischemic stroke)
Rupture of the aneurysm causes sudden, unusually severe headache; often, loss of
consciousness for a variable period; pain and rigidity of the back of the neck and spine;
and visual disturbances (visual loss, diplopia, ptosis). Tinnitus, dizziness, and
hemiparesis may also occur.

If the aneurysm leaks blood and forms a clot, patient may show little neurologic deficit or
may have severe bleeding, resulting in cerebral damage followed rapidly by coma and
death.
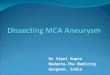
The four types of aneurysms (A) saccular, (B) dissecting, (C) mycotic, and (D) pseudoaneurysm.
Assessment and Diagnostic Methods
CT scan or MRI, cerebral angiography, and lumbar puncture are diagnostic procedures
used to confirm an aneurysm.
Medical Management
Allow the brain to recover from the initial insult (bleeding).
Prevent or minimize the risk of rebleeding.
Prevent or treat other complications: rebleeding, cerebral vasospasm, acute
hydrocephalus, and seizures.
Provide bed rest with sedation to prevent agitation and stress.
Manage vasospasm with calcium channel blockers, such as nimodipine (Nimotop).
Endovascular techniques may also be used.
Administer supplemental oxygen and maintain the hemoglobin and hematocrit at
acceptable levels to assist in maintaining tissue oxygenation.
Institute surgical treatment (arterial bypass) or medical treatment to prevent rebleeding.
Manage increased intracranial pressure (ICP) by draining the CSF via ventricular catheter
drainage.
Administer mannitol to reduce ICP, and monitor for signs of dehydration and rebound
elevation of ICP.
Administer antifibrinolytic agents to delay or prevent dissolution of the clot if surgery is
delayed or contraindicated.
Manage systemic hypertension with antihypertensive therapy, arterial hemodynamic
monitoring, and stool softeners to prevent straining and elevation of blood pressure.
Nursing Assessment
Perform a complete neurologic assessment: level of consciousness, pupillary reaction
(sluggishness), motor and sensory function, cranial nerve deficits (extraocular

eye movements, facial droop, ptosis), speech difficulties, visual disturbance or headache,
and nuchal rigidity or other neurologic deficits.
Document and report neurologic assessment findings, and reassess and report any
changes in patient’s condition.
Detect subtle changes, especially altered levels of consciousness (earliest signs of
deterioration include mild drowsiness and slight slurring of speech).
Diagnosis
Nursing Diagnoses
Ineffective tissue perfusion (cerebral) related to bleeding or vasospasm
Disturbed sensory perception due to the restrictions of aneurysm precautions
Anxiety due to illness or restrictions of aneurysm precautions
Potential Complications
Vasospasm
Seizures
Hydrocephalus
Aneurysm rebleeding
Hyponatremia
Planning and Goals
Patient goals include improved cerebral tissue perfusion, relief of sensory and perceptual
deprivation, relief of anxiety, and absence of complications.
Nursing Care Plans
Main Article: 8 Cerebrovascular Accident (Stroke) Nursing Care Plans
Nursing Interventions
Improving Cerebral Tissue Perfusion
Monitor closely for neurologic deterioration, and maintain a neurologic flow record.
Check blood pressure, pulse, level of consciousness, pupillary responses, and motor
function hourly; monitor respiratory status and report changes immediately.
Implement aneurysm precautions (immediate and absolute bed rest in a quiet,
nonstressful setting; restrict visitors, except for family).
Elevate the head of bed 15 to 30 degrees or as ordered.
Avoid any activity that suddenly increases blood pressure or obstructs venous return (eg,
Valsalva maneuver, straining), instruct patient to exhale during voiding or defecation to
decrease strain, eliminate caffeine, administer all personal care, and minimize
external stimuli.

Apply antiembolism stockings or sequential compression devices. Observe legs for signs
and symptoms of deep vein thrombosis tenderness, redness, swelling, warmth,
and edema.
Relieving Sensory Deprivation
Keep sensory stimulation to a minimum.
Explain restrictions to help reduce patient’s sense of isolation.
Relieving Anxiety
Inform patient of plan of care.
Provide support and appropriate reassurance to patient and family.
Monitoring and Managing Potential Complications
Assess for and immediately report signs of possible vasospasm, which may occur several
days after surgery or on the initiation of treatment (intensified headaches, decreased level
of responsiveness, or evidence of aphasia or partial paralysis). Also administer calcium
channel blockers or fluid volume expanders as prescribed.
Maintain seizure precautions. Also maintain airway and prevent injury if a seizure occurs.
Administer antiseizure medications as prescribed (phenytoin [Dilantin] is medication of
choice).
Monitor for onset of symptoms of hydrocephalus, which may be acute (first 24 hours
after hemorrhage), subacute (days later), or delayed (several weeks later).
Report symptoms immediately: acute hydrocephalus is characterized by sudden stupor or
coma; subacute or delayed is characterized by gradual onset of drowsiness,
behavioral changes, and ataxic gait.
Monitor for and report symptoms of aneurysm rebleeding. Rebleeding occurs most often
in the first 2 weeks.
Symptoms include sudden severe headache, nausea, vomiting, decreased level of
consciousness, and neurologic deficit.
Administer medications as ordered.
Hyponatremia: monitor laboratory data often because hyponatremia (serum sodium
level under 135 mEq/L) affects up to 30% of patients. Report low levels persisting for 24
hours, as syndrome of inappropriate antidiuretic hormone (SIADH) or cerebral
salt wasting syndrome (kidneys cannot conserve sodium) may develop.
Teaching Patients Self Care
Provide patient and family with information to promote cooperation with the care and
required activity restrictions and prepare them for patient’s return home.
Identify the causes of intracranial hemorrhage, its possible consequences, and the medical
or surgical treatments that are implemented. Discuss the importance of
interventions taken to prevent and detect complications (eg, aneurysm precautions, close
monitoring of patient). As indicated, facilitate transfer to a rehabilitation unit or center.
Continuing Care

Urge patient and family to follow recommendations to prevent further complications and
to schedule and keep followup appointments. Refer for home care if warranted,
and encourage health promotion and screening practices.