Embed Size (px)
Citation preview

IVM IVF/ICSI nin
IVM IVF/ICSI nin
YERİNİ ALACAK MI ?
YERİNİ ALACAK MI ?
Prof Dr Bülent GÜLEKLİDokuz Eylül Üniversitesi Tıp FakültesiKadın Hastalıkları ve Doğum ABD BaşkanıReprodüktif Endokrinoloji ve IVF Bilim Dalı Öğretim Üyesi

0
10
20
30
40
50
60
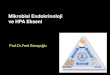
0 1 3 6
25 - 29 30 - 34 35 - 38 > 39 normal
Number of cycles / monthCu
mula
tive c
on
cepti
on
rate
(%
)n: 4777 IVF cycles
Tan et.al Lancet 1990

1. Ovarian stimulation with protocols involving GnRH agonist or antagonist in combination with gonadotrophins
2. More oocytes available for insemination3. Success rates related to the number of
embryos available for transfer4. Initially designed for tubal factor
infertility, but currently used for other indications
5. Good pregnancy rates
IVF treatment with ovarian stimulation

• Rock and Menkin (1944): Science, 100:105-107.• Edwards (1965): Nature, 208:349-351.
- matured human oocytes from antral follicles• Kennedy and Donahue (1969): Science,
164:1292-1293.
‘An alternative to the hyperstimulatory techniques is oocyte-maturation in-vitro’ – John Eppig (1989, Nat. Acad. Sci.)
Early studies on IVM of Early studies on IVM of humanhuman oocytesoocytes

Immature oocytes from unstimulated Immature oocytes from unstimulated ovaries (Egg donation)ovaries (Egg donation)
• Cha Cha et al.et al. (1991): (1991): Fertil. Steril., Fertil. Steril., 55:109-113. – birth of healthy twins55:109-113. – birth of healthy twins
• Cha Cha et al.et al. (1992): (1992): Reprod. Fertil. Reprod. Fertil. Dev.,Dev., 4:695-701. 4:695-701.
• Hwang Hwang et al.et al. (1997): (1997): Fertil. Steril.,Fertil. Steril., 68:1139-114068:1139-1140

Immature oocytes from unstimulated Immature oocytes from unstimulated ovaries ovaries
(Oocytes from natural cycles)(Oocytes from natural cycles)
Paulson et al. (1992): Fertil. Steril., Paulson et al. (1992): Fertil. Steril., 57:290-293.57:290-293.
Paulson et al. (1994): Hum. Reprod., Paulson et al. (1994): Hum. Reprod., 9:1571-1575.9:1571-1575.
Thornton et al. (1998): Fertil. Steril., Thornton et al. (1998): Fertil. Steril., 70:647-650.70:647-650.

Development of the follicle
Follicular growth
Stage Follicular size (mm)
Primordial 0.03 – 0.04Primary 0.05 – 0.06Secondary 0.07 – 0.11Preantral 0.12 – 0.20Early antral 0.21 – 0.40Antral 0.41 – 16.00Preovulatory 16.10 – 20.00
Gougeon, A. (1986): Hum. Reprod., 1:81-87.

Why IVM is an alternative treatment option?
1.Recovery of immature oocytes followed by IVM is a potentially useful treatment for patients with infertility
2.Women with polycystic ovaries (PCO) or polycystic ovarian syndrome (PCOS) have a slightly higher risk of developing ovarian hyperstimulation syndrome (OHSS)

Advantages of IVM for Advantages of IVM for infertile patientsinfertile patients
1.1. Avoidance of side effects resulting Avoidance of side effects resulting from gonadotrophin stimulation, from gonadotrophin stimulation, including OHSSincluding OHSS
2.2. To simplify treatment, especially for To simplify treatment, especially for the womenthe women
3.3. Reduced costReduced cost
4.4. Rescue early folliclesRescue early follicles

Selection criteria for IVM Selection criteria for IVM patientspatients
1.1. Patients with PCO or PCOS, irregular or Patients with PCO or PCOS, irregular or regular-cyclingregular-cycling
2.2. Antral follicle count (AFC) >20Antral follicle count (AFC) >20
3.3. Age <35 yearsAge <35 years
4. ‘IVM is suitable for patients with normal 4. ‘IVM is suitable for patients with normal ovaries; suitable for MF and Unexp ovaries; suitable for MF and Unexp patients’ - acceptable preg. rates patients’ - acceptable preg. rates (Suikkari, Finland)(Suikkari, Finland)
5. Other 5. Other (previous poor response to IVF, (previous poor response to IVF, oocyte donation and fertility preservation oocyte donation and fertility preservation for cancer patients)for cancer patients)

Clinical preparation of patients for IVM
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
U/SrFSH 150IU/day
ORICSI
ET
Protocol 2 (stimulation)
Protocol 1(no stimulation)
ET (day 3)U/S U/S OR
ICSIhCG

IVM oocyte retrieval Oocyte retrieval 36 hrs after hCG injectionOocyte retrieval 36 hrs after hCG injection Performed under general anesthesia Performed under general anesthesia Oocyte aspiration as per standard IVF,Oocyte aspiration as per standard IVF, aspiration aspiration
pressure 7.5 – 8.0 KPa (85 – 100 mm Hg)pressure 7.5 – 8.0 KPa (85 – 100 mm Hg) using Cook using Cook aspiraton needle. aspiraton needle.
3 – 4 follicles aspirated, one after another3 – 4 follicles aspirated, one after another Follicular fluid collected in tubes containing 2 ml of Follicular fluid collected in tubes containing 2 ml of
warm heparinised saline soln. (heparin 2 IU/ml). The warm heparinised saline soln. (heparin 2 IU/ml). The needle is then flushed with warm heparinised salineneedle is then flushed with warm heparinised saline
Tube containing aspirate is handed to the Tube containing aspirate is handed to the embryologistembryologist

Priming with hCG before retrieval of immature oocytes in women with infertility due to polycystic ovary syndrome
Chian RC, Gülekli B, Buckett WM, Tan SL
N Engl J Med 1999; 341: 1624-1626
McGill Reproductive Center, Royal Victoria Hospital
Montreal, Canada

Table 1.Results of IVM and Fertilization of Oocytes Followed by ET in 20 Women with the PCOS
VARIABLE VALUE
Cycles of IVF 25Age - yr 35.4 4.7Oocytes retrieved - no
Total 249Mean 10.3 5.4
Oocytes matured - no (%) 209 (84)Oocytes fertilized - no (%) 182 (87)Embryos cleaved - no (%) 173 (95)Embryos transferred - no
Total 73Mean 2.9 0.6
Clinical pregnancies - no (%) 10 (40)Implantation - no (%) 8 (32)
N Engl J Med 1999; 341: 1624-1626

Chian RC et al., Hum Reprod 15: 165-170, 2000

Randomized, controlled trial of priming with 10,000 IU versus 20,000 IU of human
chorionic gonadotropin in women with polycystic ovary syndrome who are
undergoing in vitro maturation
Gulekli B, Buckett WM, Chian RC, Child TJ, Abdul-Jalil AK, Tan SL
McGill Reproductive Center, Royal Victoria Hospital, Montreal, Canada
Fertil Steril. 2004 Nov;82:1458-1459


IVM of oocytes – laboratory procedure
Oocytes cultured in maturation medium
Mature oocyte (M-2)
Insemination (ICSI)
Embryos for Embryo Transfer
Oocytes washed
24 – 48 hrs culture
Insemination
Cleavage
Fertilized oocytes (2PN)
16-18 hours

Essential componentsEssential components
Optimal maturation media
Synchronized endometrium

Media used for IVM
Type of medium Composition Usage
SAGE - IVM media kit (ART-1600)IVM Washing Hepes-buffered O.R., ICSI
mediumIVM Oocyte Maturation Med Maturation
cultureIVM Development Cleavage Embryo
culture cleavage
OR
Medicult IVM system (Medicult no. 82214010)
LAG medium Handling medium O.R.
IVM medium Maturation med. Maturation culture

Essential componentsEssential components
Optimal maturation media
Synchronized endometrium

Endometrial PreparationEndometrial thickness on day of OPU
< 6 mm 10 - 12 mg oestradiol
6 - 8 mm 8 - 10 mg oestradiol
8 mm 6mg oestradiol
Progesterone support (200mg, bid, p.v) started following ICSI



A comparison of in vitro maturation and in vitro fertilization for women with polycystic ovariesChild TJ, Philips SJ, Abdul-Jalil AK, Gulekli B, Tan
SL
McGill Reproductive Center, Royal Victoria Hospital
Montreal, Canada
Obstet Gynecol 2002; 100:665-70


IN-VITRO MATURATION AND FERTILIZATION OF OOCYTES FROM UNSTIMULATED OVARIES: PREDICTING THE NUMBER OF IMMATURE OOCYTES RETRIEVED BY EARLY FOLLICULAR PHASE ULTRASOUND SCAN
Tan SL, Child TJ, Gülekli B
McGill Reproductive Center, Royal Victoria Hospital
Montreal, Canada
Am J Obstet & Gynecol, 2002 ,186:684-9

Results
No. of cycles 189Total # of immature oocytes 1695 Viable # “ “ “ 1616# M-II oocytes 1292Maturation rate (%) 80.0 % # 2PN embryos 965Fertilization rate (%) 74.7 % Mean # immature oocytes(SD) 9.0 7.0
Am J Obstet & Gynecol, 2002 ,186:684-9



Embryology data from an IVM programme
McGill DEU
Average number of oocytes retrieved 14.2 13.4Percentage of oocytes matured 76.8% 65.8%Percentage of oocytes fertilized 63.1% 64.2%Percentage of embryos cleaved 89.0% 87.5%Average number of embryos transferred 3.9 3.4

Outcomes from IVM programs
Center No of cases Clinical Preg/ETMaria Hospital 419 32.7% (Korea, ’00-’02)a
Memorial Hosp. 68 33.8%(Taiwan)a
Hopital Antoine-B 17 23.5%(France, ’02-’03)a
McGill Rep. Ctr. 66 32.3%(Canada, ’03)b
DEU 34 28.5%
a Chian RC (2003), RBMonline 8(2): 148-66
b McGill Rep. Ctr. (2003), personal data

Sonuç PCO tespit edilen kadınlardaki daha yüksek gebelik oranları bu hastalara IVF yerine rutin tedavide IVM önerilmesini düşündürmelidir
Daha önceki geleneksel IVF sikluslarına kötü cevap verenler (poor responders) ve kötü kaliteli embryolar elde edilmiş hastalarda IVM yararlı olabilir
IVM özellikle polikistik overi olan ve oosit donörü olmaya hazırlanan kadınlar için avantajları nedeni ile daha caziptir, böylelikle donör sayısını artırabilir