-
7/23/2019 Kyle Takayama dissertation.pdf
1/65
1
DIETARY QUALITY, REPORTING ACCURACY, AND TEMPORAL
EATING PATTERNS AMONG LOW-INCOME, HISPANIC MOTHERS
by
Kyle Takayama
A thesis submitted to the Faculty of the University of Delaware
in partialfulfillment of the requirements for the degree of Master
of Science in Human Nutrition
Spring 2014
2014 Kyle M. Takayama
All Rights Reserved
-
7/23/2019 Kyle Takayama dissertation.pdf
2/65
All rights reserved
INFORMATION TO ALL USERSThe quality of this reproduction is
dependent upon the quality of the copy submitted.
In the unlikely event that the author did not send a complete
manuscriptand there are missing pages, these will be noted. Also,
if material had to be removed,
a note will indicate the deletion.
Microform Edition ProQuest LLC.All rights reserved. This work is
protected against
unauthorized copying under Title 17, United States Code
ProQuest LLC.789 East Eisenhower Parkway
P.O. Box 1346
Ann Arbor, MI 48106 - 1346
UMI 1562432
Published by ProQuest LLC (2014). Copyright in the Dissertation
held by the Author.
UMI Number: 1562432
-
7/23/2019 Kyle Takayama dissertation.pdf
3/65
2
DIETARY QUALITY, REPORTING ACCURACY, AND TEMPORAL
EATING PATTERNS AMONG LOW-INCOME, HISPANIC WOMEN
by
Kyle Takayama
Approved:
__________________________________________________________Jillian
C. Trabulsi, Ph.D., R.D.Professor in charge of thesis on behalf of
the Advisory Committee
Approved:
__________________________________________________________
P. Michael Peterson, Ed.D.Chair of the Department of Behavioral
Health and Nutrition
Approved:
__________________________________________________________Kathleen
S. Matt, Ph.D.Dean of the College of Health Sciences
Approved:
__________________________________________________________James G.
Richards, Ph.D.Vice Provost for Graduate and Professional
Education
-
7/23/2019 Kyle Takayama dissertation.pdf
4/65
iii
ACKNOWLEDGMENTS
I would like to acknowledge my advisor, Dr. Jillian Trabulsi,
for introducing
me to the world of research, and whose wisdom and patience I
have only begun to
appreciate. I must also acknowledge Dr. Nancy Cotugna, who has
been there for me
every step of the way as an undergraduate student, young
professional, and graduate
student. I would also like to thank Dr. Mia Papas for serving on
my thesis committee
and for affording me the opportunity to work on Project Vida
Sana, as well as Dr.
Gregory Dominick and the rest of the research team at La
Comunidad Hispana.
Finally, I would like to thank my parents, Kim and Anne, for
being the gold standard
of hard work and integrity, and my sister, Kelly, for showing me
that theres more
than one way to peel a banana.
-
7/23/2019 Kyle Takayama dissertation.pdf
5/65
iv
TABLE OF CONTENTS
LIST OF TABLES
........................................................................................................
viABSTRACT
.................................................................................................................
vii
Chapter
1 INTRODUCTION
..............................................................................................
1
2 REVIEW OF THE LITERATURE
....................................................................
3
2.1
Diet and Nutrient Intake
............................................................................
3
2.2
Temporal Eating Patterns
..........................................................................
6
2.3 Reporting Accuracy
.................................................................................
11
3 SPECIFIC AIMS
..............................................................................................
17
3.1 Statement of the Problem
........................................................................
173.2 Specific Aims
..........................................................................................
17
4 METHODS
.......................................................................................................
19
4.1 Study Design
...........................................................................................
19
4.2
Measurement Tools
.................................................................................
20
4.3 Anthropometrics
......................................................................................
204.4 Diet Analysis
...........................................................................................
204.5 Statistical Methods
..................................................................................
21
4.5.1 Diet and Nutrient Intake
.................................................................
214.5.2 Reporting Accuracy
.....................................................................
224.5.3
Temporal eating patterns
.............................................................
23
5 RESULTS
.........................................................................................................
24
5.1 Subjects
....................................................................................................
24
5.1.1 Demographics
..............................................................................
245.1.2 Anthropometrics
..........................................................................
25
5.2 Nutrient Intake and Diet Quality
............................................................ 25
-
7/23/2019 Kyle Takayama dissertation.pdf
6/65
v
5.2.1 Energy/macronutrient intake
....................................................... 255.2.2
Micronutrient intake
....................................................................
265.2.3 Healthy Eating Index
...................................................................
26
5.3 Temporal distribution of energy and macronutrient intake
..................... 27
6 DISCUSSION
...................................................................................................
29
TABLES
.......................................................................................................................
35REFERENCES
.............................................................................................................
50Appendix
......................................................................................................................
54
IRB LETTERS
.................................................................................................
55
-
7/23/2019 Kyle Takayama dissertation.pdf
7/65
vi
LIST OF TABLES
Table 1: List ofmeasures included in Project Vida
Sana.....36
Table 2: Scoring standards for the 2010 Healthy Eating
Index....38
Table 3: Demographic and anthropometric characteristics of (all
subjects).........39
Table 4: Comparison of subject characteristics by reporting
accuracy.....40
Table 5: Total daily macronutrient intake of (all
subjects).......41
Table 6: Total daily macronutrient intake by reporting
accuracy.42
Table 7: Total daily micronutrient intake of (all
subjects)............43
Table 8: Healthy Eating Index scores (all
subjects)..........45
Table 9: Temporal distribution of energy and macronutrient
intake (all subjects)...46
Table 10. Comparison of temporal distribution of energy intake
by BMI category(all subjects)........47
Table 11: Comparison of energy and intake and macronutrient
distribution fromProject Vida Sana and nationally representative
data.48
Table 12: Comparison of daily micronutrient intake among
Mexican-Americanwomen ........49
-
7/23/2019 Kyle Takayama dissertation.pdf
8/65
vii
ABSTRACT
Background:According to the 2010 United States (US) Census, the
Hispanic
population now accounts for one of every six people living in
the US, and this
proportion is expected to reach one in four by the year 2050. As
the Hispanic
population continues to increase, so does its impact on the
overall health status of the
US as a whole. Epidemiologic studies have revealed inter-ethnic
disparities in health
outcomes experienced by the Hispanic population such as
increased prevalence of
obesity and diabetes. A detailed analysis of health and
nutrition behaviors such as
dietary quality, temporal eating patterns, and reporting
accuracy may lead to a greater
understanding of these disparities, and provide a foundation for
the development of
strategies for the prevention and management of health outcomes
associated with these
disparities.
Aims:The primary aim of this study is to describe the nutrient
intake and diet quality
among Hispanic women of child bearing age. The secondary aim is
to assess the
temporal distribution of food intake. These aims will be
conducted with consideration
for the accuracy of reported energy intake within the
population.
Methods:As part of an ongoing, longitudinal study of Hispanic
mothers and their
children, anthropometric data, demographic, health behavior,
physical activity and
-
7/23/2019 Kyle Takayama dissertation.pdf
9/65
viii
dietary data (one 24-hour dietary recall) has been collected.
Participant data collection
has been facilitated by bilingual research assistants.
Descriptive statistics will be used
to summarize nutrient intake and Healthy Eating Index scores
will be used to assess
diet quality. Temporal eating patterns will be summarized using
descriptive and
inferential statistics. The Goldberg method will be used to
determine the accuracy of
reported energy intake.
Results:Comparison of micronutrient intake to the Dietary
Reference Intakes (DRI)
for women between the ages of 18-50 suggests the Hispanic women
in this population
may have suboptimal intake of vitamin D and E. Further, the mean
Healthy Eating
Index-2010 (HEI-2010) score in this population (47.1 12.2)
indicates poor adherence
to federal dietary guidelines. A one-way ANOVA to assess percent
daily energy and
percent daily macronutrient intake showed a significant
difference in kcal (p < 0.01),
carbohydrate (p < 0.01), protein (p = 0.02), and fat (p <
0.01) across three time
intervals. No significant difference in percent energy intake in
the morning (p = 0.92),
afternoon (p = 0.88), and evening (p = 0.65) was observed across
body mass index
(BMI) categories. Similarly, no significant difference in
percent energy intake at T1 (p
= 0.47), T2 (p = 0.78), and T3 (p = 0.80) with respect to
reporting accuracy was
observed.
Conclusion:Nutrition education should focus on improving overall
adherence to
federal dietary guidelines, with an emphasis on increasing the
intake of whole grains,
oils, and foods low in sodium. More evidence is needed to
determine the influence of
meal size during the various time intervals on overall energy
and macronutrient intake.
-
7/23/2019 Kyle Takayama dissertation.pdf
10/65
1
Chapter 1
INTRODUCTION
According to the 2010 US Census, the Hispanic population now
accounts for
one of every six people living in the US and this proportion is
expected to exceed one
in four by the year 2050.1As one of the fastest growing ethnic
subgroups in the
country, the impact on the overall health status of the country
as a whole has become a
topic of interest in public health. Consequently, an
understanding of health outcomes
experienced by Hispanics has become an important objective of
public health
research, practice, and advocacy.
Researchers have identified disparities in health outcomes
across
socioeconomic and ethnic subpopulations of the US.2To date,
epidemiologic studies
have shown that Hispanics display higher rates of poverty, food
insecurity, and low
socioeconomic status, but also lower participation rates in
preventive health care.3
Particularly alarming is the disproportionate prevalence of
obesity and diabetes
observed over the last 25 years among the Hispanic population.
Data from the 2009-
2010 National Health and Nutrition Examination Survey (NHANES)
showed a 40.7%
and 44.3% prevalence in obesity among Hispanic and
Mexican-American women
respectively, whereas the prevalence among Caucasian,
non-Hispanic women was
33.4%.4However, the cross-sectional nature of these studies has
prevented researchers
from suggesting causal links for these health disparities. A
detailed analysis of health
and nutrition behaviors such as dietary quality, temporal eating
patterns, and reporting
accuracy may lead to a greater understanding of these
disparities and provide a
-
7/23/2019 Kyle Takayama dissertation.pdf
11/65
2
foundation for the development of strategies for the prevention
and management of
health outcomes associated with these discrepancies.
Dietary quality, often described as an individuals compliance to
federal
dietary guidelines, is an important factor which may lead to
changes in health
outcomes among individuals of differing race and
ethnicity.2Large, population-based
investigations have shown that nutrient intake and diet quality
are associated with a
variety of risk factors and health outcomes including total
serum cholesterol, obesity,
blood pressure, dental caries, diabetes, and cardiovascular
disease.5Consequently,
differences in food selection and nutrient intake may lead to
alterations in diet quality
and temporal eating patterns. These factors, with consideration
for the accuracy of diet
assessment, may have important implications for morbidity and
mortality among
ethnic sub-populations.
-
7/23/2019 Kyle Takayama dissertation.pdf
12/65
3
Chapter 2
REVIEW OF THE LITERATURE
2.1 Diet and Nutrient Intake
Population based, cross-sectional studies have revealed both
inter- and intra-
ethnic variations in food selection and nutrient intake.
Differences in nutrient intake
within the Hispanic population, related to age, acculturation,
nativity, length of US
residency, and ethnic subgroup have been observed in several
studies.3,6-11
With respect to overall diet, analysis of NHANES data collected
from 1999-
2002 have suggested a lower mean scores for the Healthy Eating
Index among
Mexican Americans compared with non-Hispanic whites older than
60 years of age,
indicating a poorer quality of diet among these older population
groups.12Data from
the 1982-1984 HHANES, 1988-1994 NHANES, and 1999-2006 NHANES
surveys (n
= 3,935, n = 4,641, n = 4,048 respectively) have been used to
investigate trends in
both nutrient intake and chronic health conditions among
Mexican-American adults. A
significant increase in carbohydrates and total energy intake,
and a significant
decrease in the intake saturated fat, protein, and percent
energy from fat were observed
over a 25-year period.5There was also a significant increase in
the prevalence of
obesity and diabetes in this population over the same time
period.
Changes in health outcomes related to nativity have also been
observed.
Mexican-Americans born in the US displayed an increased risk of
high blood pressure
and obesity compared to those born outside of the US.5Nativity
does indeed account
-
7/23/2019 Kyle Takayama dissertation.pdf
13/65
4
for some of the differences in nutrient intake among the
Hispanic population.
Investigation of the 2003-2006 NHANES data compared food
selection between
Mexican-American and non-Hispanic whites.6The sample included
foreign-born
Mexican Americans (n = 539), US-born Mexican Americans (n =
536), and US-born
non-Hispanic whites (n = 2,530). Dietary patterns were assessed
via principle
component analysis (PCA) using the subjects food frequency
questionnaire. The
results showed an inverse relationship between dietary quality
and duration of US
residence among Mexican-Americans. US-born subjects reported
greater tendency
towards a western diet favoring red meat, processed meats,
desserts, pasta, and fried
potatoes, compared to foreign-born subjects who displayed
greater tendency for a
tomato/tortilla diet consisting of more tomatoes, tortillas, and
beans. Foreign-born
Mexican-Americans reported higher consumption of fiber, fruits,
and vegetables, and
less fiber, whole grains, and total fat compared to US-born
Mexican Americans,
although this comparison did not reach statistical
significance.6
Acculturation, defined as the adoption of characteristics
displayed by the
dominant culture, also appears to play a role in dietary intake.
For instance, less
acculturated Hispanics display healthier eating patterns
characterized by greater
consumption of fruits, rice, and beans and lower consumption of
sugar and sugar-
sweetened beverages.10Also, compared to their US-born
counterparts, foreign-born
Hispanics report higher consumption of fruits, vegetables,
fruit/vegetable juice, high
fiber/low fat breads, but also a lower intake of snacks,
desserts, soda, fruit drinks, and
fast food.11It stands to reason that differences in food
preference can lead to changes
-
7/23/2019 Kyle Takayama dissertation.pdf
14/65
5
in both macro and micronutrient intake. A large, cross-sectional
study using data from
the 1982-1984 Hispanic Health and Nutrition Examination Survey
(HHANES)
quantitatively assessed 24-hour recalls collected from first and
second-generation
Mexican Americans (n = 475 and 898 respectively) compared to
non-Hispanic whites
(n = 2,326) participating in the 1976-1980 NHANES survey. A
significantly higher
intake of cholesterol was observed among first and second
generation of Mexican-
American women compared to non-Hispanic women. Unexpectedly,
first generation
Mexican-American women with lower socioeconomic status consumed
significantly
more protein, carbohydrates, cholesterol, vitamins A and C,
folic acid, and calcium
compared to second generation Mexican-American or white
non-Hispanic women.7
This same data set was analyzed to determine if nationality
affects dietary intake
(Mexican-American, Cuban-American, Puerto Rican, and
non-Hispanic). Puerto
Ricans were found to consume a higher percentage energy from
carbohydrates, and
Cuban-Americans consumed a higher percentage of protein compared
to the other
ethnic subgroups (p < .01).8A similar study of Hispanic (n =
711) and non-Hispanic
(n = 226) women over the age of 60. Subjects were stratified
women by country of
origin: Puerto Rican, Dominican, and other Hispanic.Nutrient
intake was assessed
via 24-hour dietary recall. After adjusting for age, Puerto
Rican and Dominican
women were found to consume significantly less total energy and
simple sugars but
reported significantly higher intake of polyunsaturated fats
compared to non-Hispanic
white women (p < .001). All Hispanic groups consumed more
complex carbohydrates,
but less monounsaturated and saturated fats than non-Hispanic
white women (p
-
7/23/2019 Kyle Takayama dissertation.pdf
15/65
6
.001). Changes in diet related to length of US residency were
also observed. As length
of US residency increased, dietary macronutrient composition
among Hispanic
subjects trended towards a composition reflective of
non-Hispanic participants.9
Healthy eating patterns may also be related to income.
Kirkpatrick and
colleagues2analyzed NHANES data collected between 2001 and 2004
to determine
the rate of compliance to the 2005 Dietary Guidelines for
Americansamong adults
from varying income levels and ethnic subgroups. As income level
increased, so did
the proportion of adults meeting the minimum recommendations for
fruit, whole fruits,
total vegetables, dark green vegetables, other vegetables, whole
grains, meat and
beans, milk, and oils. Compared to non-Hispanic white and
non-Hispanic black adults,
Mexican-American adults were more likely to meet the
recommendations for dry
beans and peas and total grains, but less likely to meet the
recommendations for dark
green vegetables, starchy vegetables, and oils.
Altogether these data show that differences in food selection
and nutrient
intake have been observed among subjects of varying age, gender,
and ethnicity. The
current investigation provides a unique opportunity to describe
nutrient consumption
of a more specific subset of an ethnic population; low-income
Hispanic females of
child-bearing age.
2.2 Temporal Eating Patterns
Body weight is a function of energy balance. In adults, positive
energy
balance, an energy intake that exceeds energy expenditure, can
result in weight gain
-
7/23/2019 Kyle Takayama dissertation.pdf
16/65
7
over time. The temporal distribution of eating events may also
play a role in body
weight. Analysis of eating patterns in free-living humans
indicates that energy and
macronutrient intake varies at different times of the
day.13Temporal eating patterns
have been assessed using dietary data from 24-hour recall or
food record assessment
methods; these diet assessment methods are used by researchers
to describe the time of
day and nutrient composition of eating events. This component of
eating behavior and
its role in body mass index has been explored in several studies
to date.
In one of the earliest studies of temporal eating patterns, de
Castro and
colleagues14evaluated the 7-day dietary records of 867 adults
(375 males, 492
females) to capture dietary intake. The absolute and mean energy
throughout the day
was categorized into five different 4-hour intervals (6:00AM to
9:59AM, 10:00AM to
1:59PM, 2:00PM to 5:59PM, 6:00PM to 9:59PM, 10:00PM to 1:59AM).
Each interval
includes a period of peak consumption bound by periods of low
energy and nutrient
intake as observed in a prior study.13A significant difference
in energy intake among
each of the five time intervals was observed (p < .001). The
proportion of energy
intake in the morning was negatively correlated with total daily
energy intake (r =
-.13, p < .01); in other words, an increased consumption of
energy in the morning was
associated with lower total daily energy intake. The proportion
of energy intake in the
evening was positively correlated with total energy intake (r =
.14, p < .01); a larger
evening meal was associated with greater total daily energy
intake. The results also
revealed an increase in meal size and meal frequency during
afternoon and evening
intervals. This finding was consistent among both male and
female subjects, and in
-
7/23/2019 Kyle Takayama dissertation.pdf
17/65
8
food records collected from both week and weekend days. After
further investigation
of the same data set, temporal correlations in energy intake
were consistent among
macronutrients as well. Total daily intake of carbohydrates,
fats and proteins was
negatively correlated with the intake of these nutrients within
the morning time
interval.15
Forslund and colleagues16examined circadian eating among one
group of
obese women (BMI > 33.5) and one group of randomly selected
women living the
southwest region of Sweden (2002). This study utilized a meal
pattern questionnaire to
classify eating events as traditionalif eating occurred in any
of the following time
intervals: 6:00AM to 9:59AM (breakfast), 12:00PM to 1:59PM
(lunch), and 4:00PM
to 7:59PM (dinner). Eating events outside of these time
intervals were considered
non-traditional.Compared to the randomly selected reference
group, the obese
group consumed more meals during non-traditional meal times (p
< .001) in the
afternoon (p < .01) and in the evening (p < .01), but a
smaller proportion of total meals
in the morning (p < .01).
Temporal eating patterns of children have also been explored. A
large, cross-
sectional study by Eng and colleagues17investigated changes in
body mass index
(BMI) related to proportional energy intake during various time
intervals in US
children. Subjects were children, ages 2-18 (n = 11,072), who
were enrolled in the
NHANES survey between 1999 and 2002. Dietary data were collected
from a 24-hour
recall using a multiple-pass approach. Overweight children (BMI
= 25.0 - 29.9),
consumed 47% of their total energy intake between the hours of
4:00PM and
-
7/23/2019 Kyle Takayama dissertation.pdf
18/65
9
12:00AM, and significantly more calories (23.0 kcal) than normal
weight children
(BMI < 25.0) between the hours of 4:00PM and 8:00PM (p <
.0001). Obese children
(BMI > 29.9) consumed 49% of their total energy intake
between 4:00PM and
12:00AM, and significantly more calories (27.4 kcals) between
the hours 4:00PM and
8:00PM compared to their normal weight counterparts (p <
.0003).17
Temporal eating patterns may play a role in weight loss as well.
Keim and
colleagues conducted a longitudinal investigation of weight loss
among female
subjects consuming a isocaloric diet, with one group consuming a
large meal in the
morning and the other group consuming a large meal in the
evening.18Participants (n
= 10) werebetween 20 and 40 years old, healthy, premenopausal
with normal
menstrual cycles, andbody fat 30%. Subjects lived exclusively in
a metabolic suite
during the study period. Using a randomized, cross-over study
design, subjects were
assigned to the two treatment groups for six weeks each. Total
energy requirements
were calculated for each participant using the Harris-Benedict
equation and the daily
energy intake was adjusted to lead to gradual weight loss. Group
A consumed a meal
containing 35% of their total calories at breakfast (8:00 to
8:30AM), and Group B
consumed a meal containing 35% of their total calories at dinner
(10:00 to 10:30PM).
The results showed a significant decrease in overall weight (p
< .01) and fat-free mass
(p < .001) among subjects in Group A, whereas subjects in
Group B experienced a
greater reduction in body fat percentage (p < .05).
The prevalence of obesity related to various other aspects of
eating patterns has
also been explored. In addition to the temporal distribution of
meals, meal frequency,
-
7/23/2019 Kyle Takayama dissertation.pdf
19/65
10
breakfast participation, and frequency of meals eaten away from
home have also been
examined. In one study, subjects (n = 499) between 20 and 70
years old completed
three, 24-hour recalls over the course of a 1-year study
period.19Subjects height and
weight were measured on-site, and BMI was calculated each visit.
The authors
observed no significant correlation between obesity and the
distribution of meals
throughout the day (measured by calculating the average interval
between time out of
bed and first eating, average interval between time of last
episode of eating and time in
bed, and average time of the largest episode of eating from
waking up). However,
eating fewer than three meals per day and regular breakfast
skipping were both
associated with an increased risk of obesity. Also, subjects
reported significantly
higher daily caloric intake on days when breakfast was
skipped.
The studies by de Castro and colleagues13-15attribute
differences in the
temporal distribution of energy intake to a decrease in both the
satiation and the satiety
value of food relative to time of day, with foods eaten towards
the end of the day
being less satiating. The authors hypothesize that a decrease in
the satiation value of
food leads to both increased meal size and increased meal
frequency as the day
progresses. Epidemiologic investigations of breakfast
consumption among children
and adolescents, reviewed extensively by Alexy and
colleagues20reinforce this theory;
individuals who regularly skip breakfast display an increased
risk of overweight and
obesity. Although the the relationship between body weight and
breakfast
consumption has been well studied, the strength and direction of
this association is
still unclear.21
-
7/23/2019 Kyle Takayama dissertation.pdf
20/65
11
While it is recognized that the cross-sectional nature of
studies regarding
temporal eating prevents researchers from establishing a causal
pathway for this
relationship, these investigations have consistently revealed a
negative correlation
between energy intake in the morning and total energy intake.
Since energy intake in
the morning is related to total energy intake, it may also be
associated with an
individuals risk of overweight and obesity. Although significant
associations between
meal patterns, total energy intake, and body mass index have
been observed, little is
known about the strength of this relationship across ethnic
groups. The increased
prevalence of overweight and obesity observed among Hispanics is
justification for
the current study to learn more about temporal eating patterns
displayed by this
population.
2.3 Reporting Accuracy
An important component in diet and health outcome research is an
accurate
description of habitual dietary intake. For most studies,
assessing the validity of
reported energy intake is an essential component of dietary
assessment. Misreported
energy intake can lead to under- or over-estimation of nutrient
intake and incorrect
conclusions regarding diet and disease
relationships.22Disparities in reported energy
intake versus actual energy consumption may be attributed to
inadequate or
incomplete record keeping, conscious misreporting, reporting
bias, or lack of
skill/training.23Individuals who report a dietary intake level
below what is considered
biologically plausible, given their physiologic status and
physical activity level, are
-
7/23/2019 Kyle Takayama dissertation.pdf
21/65
12
known as under-reporters.24An extensive review by Poslusna and
colleagues
concluded that under-reporting of energy intake is prevalent in
the majority of dietary
studies. However, the prevalence varies based on the methods
employed to assess
diet.25The prevalence of under-reporting ranged from 21.5-67%,
11.9-44%, and 14.3-
38.5% in studies using 24 hour recall, FFQ, and weighed food
records respectively.
Statistically significant predictors of under-reporting were
also identified by these
studies. Age, BMI, total energy intake, percent energy from fat,
and variability in
number of meals per day were positively correlated with
under-reporting whereas
socioeconomic status and level of education were negatively
correlated with under-
reporting. Under-reporting also appears to be more prevalent
among smokers and
subjects with a history of dieting.25These reviews also found
that underreporting is
more common that over-reporting.
One of the largest studies to examine reporting accuracy was
conducted by
Tooze and colleagues26using data collected by the National
Cancer Institute from
1999-2000. This investigation, called the Observing Protein and
Energy Nutrition
(OPEN) study, classified participants (n = 484) as
under-reporters, accurate reporters,
or over-reporters based on reported energy intake from both a
food frequency
questionnaire (FFQ) and 24 hour recall (24HR) methods. Analysis
of reporting
accuracy using the doubly labeled water method, a biomarker of
total energy
expenditure (TEE), revealed the magnitude and prevalence of
under-reporting among
subjects. When subjects reported energy intake was compared to
the median TEE,
men underreported by 11% on 24HRs and by 30% on FFQ. The
magnitude of under-
-
7/23/2019 Kyle Takayama dissertation.pdf
22/65
13
reporting among women was 17% and 24% of the 24HR and FFQ
respectively.
Classification of individual subjects showed that the prevalence
of under-reporting
was 22% for women and 21% for men when comparing subjects 24HRs
to TEE.
Analysis of subjects FFQ revealed a prevalence of 49% and 50%
among women and
men respectively. Furthermore, 13% of female subjects and 14% of
males subjects
under-reported on both 24HR and FFQ.
The study by Tooze and colleagues26also identified
characteristics associated
with underreporting. Analysis of subjectsFFQs showed that fear
of negative
evaluation, weight-loss history, and percent energy from fat
were predictive of
underreporting among women (R = .09), and in men the best
predictors of
underreporting were BMI, relative activity level, and eating
frequency (R = .10).
Analysis of subjects 24HR revealed that social desirability,
fear of negative
evaluation, BMI, percent energy from fat, usual activity, and
variability in number of
meals per day were the best predictors of under-reporting in
women (R = .22),
whereas social desirability, dietary restrain, body mass index,
eating frequency,
dieting history, and education were the best predictors among
men (R = .25).
However, the prevalence of underreporting with respect to
ethnicity was not addressed
in this study.
The gold-standard for validation of reported energy intake is
the doubly-
labeled water technique. However, this method is expensive and
requires the skill of a
trained technician. A more cost-effective approach is to
validate reported energy
intake using the Goldberg method, which uses an empirically
derived equation to
-
7/23/2019 Kyle Takayama dissertation.pdf
23/65
14
assess reporting accuracy. In this equation, subjects total
energy expenditure (TEE) is
calculated by multiplying basal metabolic rate (BMR) by physical
activity level
(PAL). To calculate BMR, an individuals weightand age are
entered into the
Schofield equation. PAL is set to a constant value of 1.55,
which represents the
activity level of a sedentary individual as defined by the
FAO/WHO/UNU.27To
validate subjects reported energy intake (rEI), a 95% confidence
interval about the
log of the ratio rEI:TEE is calculated. Subjects whose rEI falls
within the confidence
interval are classified as acceptable reporters and those that
report above or below the
confidence interval are classified as over- and under-reporters,
respectively.28
Research conducted by Tooze and colleagues28evaluated the
accuracy of the Goldberg
method to classify subjects (n = 484) as either acceptable or
unacceptable reporters
using data from the OPEN study; this study identified acceptable
reporters using the
Goldberg equation, and compared the results to the gold
standard, energy expenditure
as measured by doubly labeled water. The results showed that the
sensitivity of
Goldberg method for determining reporting accuracy on an FFQ was
92.6% for men
and 92.1% for women, with a specificity of 87.6% for both. The
positive predictive
value was 88% and the negative predictive value was 92% for both
men and women.
In comparing the Goldberg method to subjects 24HR, the
sensitivity was 45.1% for
men and 54.3% for women, with a specificity of 98.9% and 95.5%
respectively. The
positive predictive value for men and women was 92% with a
negative predictive
value of 86% for men and 88% for women.28The results of this
analysis suggest that
the Goldberg cut-off is highly accurate in identifying subjects
who under-report
-
7/23/2019 Kyle Takayama dissertation.pdf
24/65
15
energy intake, and can be used in studies to determine reporting
accuracy if utilizing
the doubly labeled water method is not possible.
To date, few studies have investigated reporting accuracy among
Hispanic
populations. Olendzki and colleagues29described the prevalence
of under-reporting
among low-income, low-literacy, Caribbean Hispanics (n = 215)
enrolled in a
prevention program for type 2 diabetes. The sample was
predominantly female (76%)
with a mean age of 51.5 years old (SD = 11.11). Dietary data
were collected from
three unannounced 24-hour recalls performed by bilingual
dietitians using a multiple-
pass technique, and energy expenditure was measured by basal
metabolic rate. The
prevalence of under-reporting among subjects was not reported,
however, the analysis
revealed that subjects under-reported energy intake by an
average of 254 kcals per
day. Participants with higher BMI reported lower energy intake
compared to their
basal metabolic rate (p < .001). Subjects who were
unemployed, physically inactive,
or had siblings diagnosed with diabetes were more likely to
under-report, although
these differences did not reach statistical significance.29
A similar study was conducted by Bothwell and colleagues24using
random
sample of both Mexican and Mexican-American women (n = 357)
between the ages of
21 and 67. This study analyzed the prevalence of under-reporting
using four variations
of the Goldberg method. Method 1 used a PAL cutoff value of
1.51, the value
representing sedentary behavior and was adjusted to the full
sample size. Method 2
was adjusted for the full sample size and PAL cutoff values of
1.51, 1.58, and 1.76 to
account for physical activity levels of low, moderate, and high
physical activity levels
-
7/23/2019 Kyle Takayama dissertation.pdf
25/65
16
respectively. Methods 3 and 4 used a conservative sample size
(n=1), with Method 3
employing a constant PAL cutoff of 0.81 for sedentary behavior,
and Method 4
adjusting for participant physical activity level using 0.81,
0.85, and 0.95 as cutoff
values for low, moderate, and high physical activity levels
respectively. The
percentage of participants classified as under-reporting was
72.2% (Method 1), 81.3%
(Method 2), 11.9% (Method3), and 20.5% (Method 4).Clearly the
PAL selected
greatly affects the results of the Goldberg method, and likely
Methods 3 and 4 selected
PAL levels that were too low. Nonetheless, the results of this
study also showed a
significant association between underreporting and both
overweight and obesity (p elementary school 37 (57)
Marital Status
Married 46 (71)Not married 19 (29)
Employment
Unemployed, not looking 23 (35)
Unemployed, looking 16 (25)
Working part time 11 (17)
Working full time 15 (23)
-
7/23/2019 Kyle Takayama dissertation.pdf
49/65
40
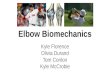
Table 4. Comparison of subject characteristics by reporting
accuracy (all subjects)
Under-reporters
(n = 29)
Accuratereporters
(n = 36)
Teststatistic* p-value
Mean (sd) Mean (sd)
Age (years) 31.5 (4.7) 33.6 (5.4) 1.6242 0.1094
Height (cm) 155.9 (5.9) 155.9 (5.3) 0.0112 0.9911
Weight (kg) 70.5 (11.0) 67.4 (10.7) -1.1505 0.2545
Body mass index(kg/m2) 29.0 (4.0) 27.7 (4.2) -1.2488 0.2129
Number of children 2.6 (0.8) 2.8 (1.5) 0.9338 0.3545
Energy (kcals) 965 (151) 1788 (407) 11.2225 < .0001
BMI Category N (%) N (%) 1.1260 0.5695
Normal weight (18.5 - 24.9) 5 (17) 10 (28)Overweight (25.0 -
29.9) 15 (52) 15 (42)
Obese (30.0) 9 (31) 11 (31)
Marital Status 0.0680 0.7936
Married 21 (72) 25 (69)
Not married 25 (28) 11 (31)
Employment 0.5850 0.8998
Unemployed, not looking 10 (34) 13 (36)
Unemployed, looking 7 (24) 9 (25)
Working part time 6 (21) 5 (14)
Working full time 6 (21) 9 (25)
Own a car? 0.7580 0.3839
Yes 25 (86) 28 (78)
No 4 (14) 8 (22)
Education 0.5770 0.4474
Some/Completed elementary 14 (48) 14 (39)
> elementary 15 (52) 22 (61)
Monthly income 0.4800 0.4883
< $2,000 17 (59) 18 (50)
$2,000 18 (41) 18 (50)* Pearson chi-square for categorical and
t-test for continuous variables
-
7/23/2019 Kyle Takayama dissertation.pdf
50/65
41
Table 5: Total daily macronutrient intake (all subjects)
Nutrient Mean (SD) Median Q1 Q3 AMDR
Energy (kcals) 1421 (519) 1306 1008 1743 --
Discretionary kcals 387 (226) 364 208 501 --
Carbohydrates (g) 262 (140) 229 157 330 --% kcal from CHO 52.1
(11.6) 51.5 45.3 58.8 45-65%
Dietary fiber (g) 13.9 (7.5) 12.9 7.7 18.4 --
Sugar (g) 77.6 (36.2) 70.3 51.6 94.2 --
Protein (g)* 97.0 (60.7) 79.9 48.8 135.5 --
% kcal from PTN 18.8 (9.0) 17.9 14.4 21.8 10-35%
Total fat (g) 72.6 (51.8) 59.1 35.3 95.3 --
% kcal from FAT 30.2 (9.0) 31.1 23.4 37.3 20-35%
Saturated (g) 17.2 (10.4) 15.2 9.3 21.2 --
% kcal from SFAT 8.1 (3.7) 7.2 4.9 11 --
Cholesterol (mg) 233 (177) 187 100 338 --AMDR: Acceptable
Macronutrient Distribution Range-- no data available
-
7/23/2019 Kyle Takayama dissertation.pdf
51/65
42
42
Table 6: Total daily macronutrient intake by reporting
accuracy
Under-reporters (n = 29) Accurate reporters (n = 36)
Nutrient Mean (SD) Median Q1 Q3 Mean (SD) Median Q1
Q3TestStatistic
p-value
Energy (kcals/d)a 965 (151) 1000 842 1069 1788 (407) 1718 1490
2061 12.90 < 0.01
Discretionary kcalsa 247 (113) 241 161 337 499 (232) 447 365 700
4.72 < 0.01
% kcal from discretionary 25.1 (10.2) 24.3 19.0 32.3 27.5 (11.2)
29.3 20.7 33.0 0.92 0.36
Carbohydrates (g/d)a 133 (37) 128 106 163 221 (63) 212 177 270
4.46 < 0.01
% kcal from CHO 55.0 (11.5) 54.6 47.7 63.3 49.8 (11.3) 50.9 44.0
55.5 -1.81 0.08
Dietary fiber (g/d)a 9.8 (4.8) 8.7 6.6 13.8 17.2 (7.7) 16.5 12.6
21.1 4.53 < 0.01
Dietary fiber (g/1000kcal)a 10.3 (5.0) 9.8 6.3 12.9 9.6 (3.8)
8.9 7.0 11.6 -0.39 0.70
Sugar (g/d)a 64.0 (23.8) 64.6 43.4 76.6 88.7 (40.8) 82.2 64.0
111.3 2.64 0.01
Sugar (g/1000kcal)a 65.6 (19.2) 57.0 51.6 78.3 50.2 (24.4) 44.8
35.2 62.8 -3.57 < 0.01
Protein (g)a 45.5 (13.4) 43.4 35.3 53.8 83.2 (38.0) 79.7 58.7
97.8 3.28 < 0.01
% kcal from PTN 19.2 (6.2) 18.1 14.1 22.1 18.4 (6.0) 17.9 14.6
21.3 -0.49 0.63
Total fat (g/d)a 29.3 (11.9) 29.6 17.6 36.6 65.6 (23.2) 63.6
47.4 81.1 5.95 < 0.01
% kcal from FAT 27.1 (9.6) 26.3 19.4 36.0 32.8 (7.8) 32.2 28.7
39.3 2.55 0.01
Saturated (g/d)a 10.3 (4.4) 10.4 7.2 13.6 22.7 (10.5) 20.6 15.0
28.4 6.35 < 0.01
% kcal from SFAT 7.7 (4.0) 7.0 4.4 11.2 8.4 (3.4) 7.9 5.3 10.9
6.35 < 0.01
Cholesterol (mg/d)a 161 (109) 151 77 206 291 (200) 260 132 385
3.01 < 0.01
Cholesterol (mg/1000kcal)a 171 (125) 146 82 219 162 (109) 147 78
202 -0.33 0.74
a Values were log transformed prior to t-test
-
7/23/2019 Kyle Takayama dissertation.pdf
52/65
43
43
Table 7: Total daily micronutrient intake (all subjects)
Nutrient Mean (SD) Median Q1 Q3 %EAR % RDA/AI < EAR (%) >
UL (%)
Vitamins
Thiamin (mg/d) 1.4 (0.7) 1.3 0.9 1.9 156 127 23 --
Thiamin (mg/1000kcal) 1.0 (0.5) 0.9 0.7 1.2 -- -- -- --
Riboflavin (mg/d) 1.7 (0.7) 1.6 1.1 2.2 189 155 12 --
Riboflavin (mg/1000kcal) 1.3 (0.6) 1.1 1.0 1.6 -- -- -- --
Niacin (mg/d) 19 (8) 18 13.0 25 173 136 12 3Niacin (mg/1000kcal)
14.4 (4.8) 13.6 9.2 16.5 -- -- -- --
Vitamin B6 (mg/d) 1.9 (0.9) 1.8 1.20 2.5 173 146 23 0
Vitamin B6 (mg/1000kcal) 1.5 (0.8) 1.2 0.9 1.7 -- -- -- --
Folate (mcg/d) 388 (215) 354 241 512 121 97 59 3
Folate (mcg/1000kcal) 293 (180) 254 159 362 -- -- -- --
Vitamin A (RAE/d) 550 (321) 511 335 697 110 79 49 0
Vitamin A (RAE/1000kcal) 410 (246) 360 254 517 -- -- -- --
Vitamin B12 (mcg/d) 5.3 (3.6) 4.9 2.5 7.5 265 221 17 --
Vitamin B12 (mcg/1000kcal) 4.0 (2.8) 2.9 1.9 5.6 -- -- -- --
Vitamin C (mg/d) 88 (60) 76 41 122 147 117 40 0
Vitamin C (mg/1000kcal) 68 (56) 52 35 84 -- -- -- --
Vitamin D (mcg/d) 4.2 (2.9) 3.9 1.6 6.6 42 28 99 0Vitamin D
(mcg/1000kcal) 3.1 (2.1) 2.8 1.2 4.6 -- -- -- --
Vitamin E (mg/d) 5.5 (4.1) 4.8 2.9 6.1 46 37 95 0
Vitamin E (mg/1000kcal) 4.0 (3.2) 3.3 2.6 4.2 -- -- -- --
-
7/23/2019 Kyle Takayama dissertation.pdf
53/65
44
44
: continuedTable 7: Total daily micronutrient intake (all
subjects)
Nutrient Mean (SD) Median Q1 Q3 %EAR % RDA/AI < EAR (%) >
UL (%)
Minerals
Calcium (mg/d) 744 (362) 723 481 938 93 74 62 0
Calcium (mg/1000kcal) 546 (263) 497 332 689 -- -- -- --
Copper (mg/dl) 933 (415) 901 632 1151 133 104 31 0
Copper (mg/1000kcal) 667 (193) 662 504 794 -- -- -- --
Iron (mg/d) 14.5 (7.4) 13.3 8.2 18.8 179 81 23 0Iron
(mg/1000kcal) 10.7 (5.5) 8.8 7.1 12.1 -- -- -- --
Phosphorus (mg/d) 1036 (441) 946 733 1293 179 148 11 0
Phosphorus (mg/1000kcal) 735 (173) 728 624 814 -- -- -- --
Sodium (mg/d) 2483 (1243) 2177 1525 3077 -- 165 -- 46
Sodium (mg/1000kcal) 1754 (609) 1626 1354 2048 -- -- -- --
Zinc (mg/d) 10.8 (6.6) 9.8 5.8 14.3 159 135 35 0
Zinc (mg/1000kcal) 7.7 (4.2) 6.6 4.8 9.3 -- -- -- --
-- no data available
-
7/23/2019 Kyle Takayama dissertation.pdf
54/65
45
45
Table 8. Healthy Eating Index scores (all subjects)
Category (maximum points) Mean (SD) Median Q1 Q3
n (%) meeting
standard
Adequacy
Total Fruit (5) 3.5 (2.0) 5.0 1.7 5.0 37 (57)
Whole Fruit (5) 3.2 (2.3) 5.0 0.0 5.0 32 (49)
Total Vegetables (5) 3.5 (1.7) 3.7 2.4 5.0 25 (38)
Greens and Beans (5) 2.0 (2.3) 0.3 0.0 5.0 18 (28)
Whole Grains (10) 2.4 (3.2) 3.7 2.4 5.0 4 (6)
Dairy (10) 6.0 (3.5) 6.8 3.0 10.0 18 (28)
Total Protein Foods (5) 3.7 (1.8) 5.0 2.2 5.0 33 (51)
Seafood and Plant Proteins (5) 1.2 (1.9) 0.1 0.0 1.9 9 (14)
Fatty Acids (10) 3.8 (3.3) 3.4 0.7 6.0 6 (9)
Moderation
Refined Grains (10) 4.1 (3.6) 3.7 0.6 6.8 10 (15)
Sodium (10) 4.1 (3.6) 3.3 0.0 6.9 6 (9)
Empty Calories (10) 9.6 (6.8) 8.4 4.4 17.3 15 (23)
Total Score (100) 47.1 (12.2) 46.1 39.4 52.4 13.6 - 79.5*
*Range
-
7/23/2019 Kyle Takayama dissertation.pdf
55/65
46
46
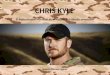
Table 9: Temporal distribution of energy and macronutrient
intake (all subjects)
a Values were log transformed prior to ANOVA; data presented as
absolute valuesbcd Dissimilar superscripts indicate significant
difference between time frames
Nutrient T1 (4:00AM - 10:29AM) T2 (10:30AM - 4:59PM) T3 (5:00PM
- 3:59AM)
Mean (SD) Median Q1 Q3 Mean (SD) Median Q1 Q3 Mean (SD) Median
Q1 Q3
Absolute daily intakea
Energy (kcals)
543
(423)
bc
443 231 708 832 (573)
c
652 370 1137 690 (588)
c
565.0 259 922.0Carbohydrate(g) 79.2 (59.6) 65.8 36.9 109
100.4(72.9) 85.4 44.8 151.7 81.8 (60.1) 69.9 41.9 125.6
Protein (g)
22.7(26.1)b 16.7 5.9 24.7 39.5 (29.9)c 31.9 15.2 58.7 34.9
(37.0)c 19.7 8.6 52.2
Fat (g)
16.1(17.6)b 10.4 4.7 18.5 30.9 (27.1)c 20.7 12.7 44.5 25.6
(29.1)c 16.8 5.1 32.7
Percent daily intake
Energy
26.0(14.5)b 20.9 14.9 39.9 41.8 (21.2)c 37.4 29.6 54.3
32.1(18.3)b 32.0 29.1 48.6
Carbohydrate
30.3(16.7)b 28.8 17.7 40.5 38.0 (21.4)c 35.6 24.1 47.4
31.7(17.1)bc 32.1 21.6 45.7
Protein
22.0(16.5)b 18.1 11.1 28.6 43.4 (26.1)c 39.4 19.4 63.0
34.5(25.5)d 36.5 12.1 55.3
Fat22.2(18.2)b 17.4 8.9 33.0 45.3 (25.3)c 42.9 28.6 59.7
32.5(22.1)d 30.2 13.4 50.3
-
7/23/2019 Kyle Takayama dissertation.pdf
56/65
47
47
Table 10. Comparison of temporal distribution of energy intake
by BMI category (all subjects)
T1 (4:00AM - 10:29AM) T2 (10:30AM - 4:59PM) T3 (5:00PM -
3:59AM)
Absolute daily intakea
Normal weight 535 (387) 804 (560) 786 (713)
Overweight 493 (351) 834 (592) 654 (545)
Obese 624 (541) 851 (581) 672 (573)
F-Test statistic (p-value) 0.5757 (p = 0.5653) 0.0292 (p =
0.9713) 0.2579 (p = 0.7735)
Percent daily intake
Normal weight 25.2 (13.8) 40.3 (23.9) 34.5 (20.4)
Overweight 25.8 (13.4) 41.3 (18.6) 33.0 (17.7)
Obese 27.1 (17.1) 43.8 (23.6) 29.1 (18.1)
F-Test statistic (p-value) 0.0863 (p = 0.9174) 0.1296 (p =
0.8787) 0.4268 (p = 0.6545)a Values were log transformed prior to
ANOVA
-
7/23/2019 Kyle Takayama dissertation.pdf
57/65
48
48
Table 11. Comparison of energy intake and macronutrient
distribution from Project
Vida Sana and nationally representative data
HHANES
(1982-1984)
NHANES
(1988-1994)
NHANES
(1999-2006)
Project Vida
Sana (2012-
2013)
Energy (kcals) 1552 (14.69) 1744 (22.44) 1827 (23.61) 2065
(140.80)
Carbohydrates (%) 47.5 (0.42) 51.7 (0.31) 52 (0.38) 52.1
(11.60)
Total fat (%) 35.7 (0.34) 32.6 (0.26) 32.7 (0.27) 30.2
(1.12)Saturated fat (%) 12.7 (0.14) 10.8 (0.12) 10.7 (0.13) 8.1
(0.46)
Protein (%) 17.2 (0.10) 16.1 (0.09) 15.8 (0.14) 18.8 (0.75)
Table adapted from Fryar and colleagues (2012)
Values reported as mean (SE)
-
7/23/2019 Kyle Takayama dissertation.pdf
58/65
49
49
Table adopted from Gregory-Mercado and colleagues (2007)Values
reported as mean (SE)--no data available
Table 12: Comparison of daily micronutrient intake among
Mexican-American women
WISEWOMEN (1998-2000) Project Vida Sana (2012-2013)
Vitamins
Vitamin A (RAE) 1191.4 (0.02) 550 (39.77)
Thiamin (mg) 1.25 (0.01) 1.4 (0.08)
Riboflavin (mg) 1.44 (0.01) 1.7 (0.09)
Niacin (mg) 16.8 (0.01) 19 (1.05)
Vitamin B6 (mg) 1.66 (0.01) 1.9 (0.11)Folate (mcg) 269 (0.01)
388 (26.64)
Vitamin B12 (mcg) 2.06 (0.00) 5.3 (0.44)
Vitamin C (mg) 130.2 (0.01) 88 (7.46)
Vitamin D (mcg) -- 4.2 (0.36)
Vitamin E (mg) 6.64 (0.02) 5.5 (0.50)
Minerals
Calcium (mg) 649.4 (0.01) 744 (44.90)
Copper (mg) 1.14 (0.01) 0.93 (0.42)
Iron (mg) 12.6 (0.01) 14.5 (0.91)
Magnesium (mg)* 239.8 (0.01) 223 (11.32)
Phosphorus (mg) 930.7 (0.01) 1036 (54.69)
Sodium (mg) 2572.2 (16.5) 2483 (154.1)
Zinc (mg) 9.26 (0.01) 10.8 (0.82)
-
7/23/2019 Kyle Takayama dissertation.pdf
59/65
50
REFERENCES
1. McArthur L, Anguiano R, Gross K. Are household factors
putting immigrantHispanic children at risk of becoming overweight:
a community-based study ineastern North Carolina.J Community
Health.2004;29:387-404
2. Kirkpatrick S, Dodd K, Reedy J, Krebs-Smith S. Income and
race/ethnicity areassociated with adherence to food-based dietary
guidance among US adults andchildren.J Acad Nutr
Diet.2012;112:624-635.
3. Fitzgerald N, Himmelgreen D, Damio G, Segura-Perez S, Peng Y,
Perez-Escamilla R. Acculturation, socioeconomic status, obesity and
lifestyle factors
among low-income Puerto Rican women in Connecticut, U.S.,
1998-1999.RevPanam Salud Publica. 2006;19:306-313.
4. Flegal K, Carroll M, Kit B, Ogden C. Prevalence of obesity
and trends in thedistribution of body mass index among US adults,
1999-2010.JAMA.2012;307:491-497.
5. Fryar C, Wright J, Eberhardt M, Dye B. Trends in nutrient
intakes and chronichealth conditions among Mexican-American adults,
a 25-year profile: UnitedStates, 1982-2006.Natl Health Stat Report.
2012:1-20.
6. Sofianou A, Fung T, Tucker K. Differences in diet pattern
adherence by nativity
and duration of US residence in the Mexican-American population.
J Am DietAssoc. 2011;111:1563-1569.
7. Guendelman S, Abrams B. Dietary intake among Mexican-American
women:generational differences and a comparison with white
non-Hispanic women.Am JPublic Health. 1995;85:20-25.
8. Loria C, Bush T, Carroll M, et al. Macronutrient intakes
among adult Hispanics: acomparison of Mexican Americans, Cuban
Americans, and mainland PuertoRicans.Am J Public Health.
1995;85:684-689.
9. Bermudez O, Falcon L, Tucker K. Intake and food sources of
macronutrientsamong older Hispanic adults: association with
ethnicity, acculturation, and lengthof residence in the United
States.J Am Diet Assoc. 2000;100:665-673.
10. Ayala G, Baquero B, Klinger S. A systematic review of the
relationship betweenacculturation and diet among Latinos in the
United States: implications for futureresearch.J Am Diet Assoc.
2008;108:1330-1344.
-
7/23/2019 Kyle Takayama dissertation.pdf
60/65
51
11. Duffey K, Gordon-Larsen P, Ayala G, Popkin B. Birthplace is
associated withmore adverse dietary profiles for US-born than for
foreign-born Latino adults.JNutr. 2008;138:2428-2435.
12. Ervin R. Healthy Eating Index scores among adults, 60 years
of age and over, bysociodemographic and health characteristics:
United States, 1999-2002.Adv Data.2008:1-16.
13. de Castro JM. Circadian rhythms of the spontaneous meal
pattern, macronutrientintake, and mood of humans.Physiol Behav.
1987;40:437-446.
14. de Castro JM. The time of day of food intake influences
overall intake in humans.J Nutr. 2004;134:104-111.
15. de Castro JM. The time of day and the proportions of
macronutrients eaten arerelated to total daily food intake.Br J
Nutr. 2007;98:1077-1083.
16. Berteus Forslund H, Lindroos A, Sjostrom L, Lissner L. Meal
patterns and obesityin Swedish women-a simple instrument describing
usual meal types, frequencyand temporal distribution.Eur J Clin
Nutr. 2002;56:740-747.
17. Eng S, Wagstaff D, Kranz S. Eating late in the evening is
associated withchildhood obesity in some age groups but not in all
children: the relationshipbetween time of consumption and body
weight status in U.S. children.Int J BehavNutr Phys Act.
2009;6:27.
18. Keim N, Van Loan M, Horn W, Barbieri T, Mayclin P. Weight
loss is greaterwith consumption of large morning meals and fat-free
mass is preserved with
large evening meals in women on a controlled weight reduction
regimen. J Nutr.1997;127:75-82.
19. Ma Y, Bertone E, Stanek E, et al. Association between eating
patterns and obesityin a free-living US adult population.Am J
Epidemiol. 2003;158:85-92.
20. Alexy U, Wicher M, Kersting M. Breakfast trends in children
and adolescents:frequency and quality.Public Health Nutr.
2010;13:1795-1802.
21. Timlin MT, Pereira MA. Breakfast frequency and quality in
the etiology of adultobesity and chronic diseases.Nutr Rev.
2007;65:268-281.
22. Livingstone M, Black A. Markers of the validity of reported
energy intake.JNutr. 2003;133:895S-920S.
23. Maurer J, Taren D, Teixeira P, et al. The psychosocial and
behavioralcharacteristics related to energy misreporting.Nutr Rev.
2006;64:53-66.
-
7/23/2019 Kyle Takayama dissertation.pdf
61/65
52
24. Bothwell E, Ayala G, Conway T, Rock C, Gallo L, Elder J.
Underreporting offood intake among Mexican/Mexican-American Women:
rates and correlates.JAm Diet Assoc. 2009;109:624-632.
25. Poslusna K, Ruprich J, de Vries J, Jakubikova M, van't Veer
P. Misreporting ofenergy and micronutrient intake estimated by food
records and 24 hour recalls,control and adjustment methods in
practice.Br J Nutr. 2009;101:S73-85.
26. Tooze J, Subar A, Thompson F, Troiano R, Schatzkin A, Kipnis
V. Psychosocialpredictors of energy underreporting in a large
doubly labeled water study.Am JClin Nutr. 2004;79:795-804.
27. Energy and protein requirements. Report of a joint
FAO/WHO/UNU ExpertConsultation. World Health Organ Tech Rep Ser.
1985;724:1-206.
28. Tooze J, Krebs-Smith S, Troiano R, Subar A. The accuracy of
the Goldbergmethod for classifying misreporters of energy intake on
a food frequency
questionnaire and 24-h recalls: comparison with doubly labeled
water.Eur J ClinNutr. 2012;66:569-576.
29. Olendzki B, Ma Y, Hebert J, et al. Underreporting of energy
intake and associatedfactors in a Latino population at risk of
developing type 2 diabetes.J Am DietAssoc. 2008;108:1003-1008.
30. Guenther P, Casavale K, Reedy J, et al. Update of the
Healthy Eating Index: HEI-2010.J Acad Nutr Diet.
2013;113:569-580.
31. Schofield W. Predicting basal metabolic rate, new standards
and review of
previous work.Hum Nutr Clin Nutr. 1985;39:5-41.
32. Black A. Critical evaluation of energy intake using the
Goldberg cut-off forenergy intake:basal metabolic rate. A practical
guide to its calculation, use andlimitations.Int J Obes Relat Metab
Disord. 2000;24:1119-1130.
33. Goldberg G, Black A, Jebb S, et al. Critical evaluation of
energy intake data usingfundamental principles of energy
physiology: 1. Derivation of cut-off limits toidentify
under-recording.Eur J Clin Nutr. 1991;45:569-581.
34. Gregory-Mercado K, Staten L, Gillespie C, et al. Ethnicity
and nutrient intakeamong Arizona WISEWOMAN participants.J Womens
Health. 2007;16:379-389.
35. Guenther P, Reedy J, Krebs-Smith S. Development of the
Healthy Eating Index-2005.J Am Diet Assoc. 2008;108:1896-1901.
36. Leung C, Ding E, Catalano P, Villamor E, Rimm E, Willett W.
Dietary intake anddietary quality of low-income adults in the
Supplemental Nutrition AssistanceProgram.Am J Clin Nutr.
2012;96:977-988.
-
7/23/2019 Kyle Takayama dissertation.pdf
62/65
53
37. Kharmats A, Jones-Smith J, Cheah Y, et al. Relation between
the SupplementalNutritional Assistance Program cycle and dietary
quality in low-income AfricanAmericans in Baltimore, Maryland.Am J
Clin Nutr. 2014.
-
7/23/2019 Kyle Takayama dissertation.pdf
63/65
54
Appendix
-
7/23/2019 Kyle Takayama dissertation.pdf
64/65
55
IRB LETTERS
-
7/23/2019 Kyle Takayama dissertation.pdf
65/65