Embed Size (px)
Citation preview

Le infezioni respiratorie ricorrenti Epidemiologia e diagnosi
Giovanni A. Rossi
U.O. di Pneumologia e Allergologia
I.R.C.C.S. G. Gaslini, Genova
Fondazione
Gerolamo
Gaslini
Istituto
Giannina
Gaslini

Outline
• Cosa intendiamo per Infezioni Respiratorie Ricorrenti?
• Perché i bambini in età prescolare sono più esposti alle Infezioni
Respiratorie Ricorrenti ?
• Cosa dobbiamo fare di fronte ad un bambino con Infezioni
Respiratorie Ricorrenti ?
La Diagnosi
La Profilassi

Le Infezioni Respiratorie Ricorrenti?
• Questa situazione si manifesta, solitamente, in età prescolare, in coincidenza della prima socializzazione del bambino con l’ingresso alla scuola materna
• Benché si tratti di una patologia benigna destinata ad evolvere favorevolmente verso i 5-9 anni, essa interferisce notevolmente sul benessere del bambino e della famiglia e determina importanti costi medico sociali
• Con “infezioni respiratorie ricorrenti (IRR)” ci si riferisce a una serie di episodi acuti a carico di uno o più settori definiti: il naso, l’orecchio, il faringe, le tonsille, il laringe, la trachea e i bronchi

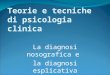
Livelli di Ig seriche nel lattante %
ris
pet
to a
i liv
elli
ne
gli a
du
lti
100 80 60 40 20 0
- - - - - - -3 0 3 6 9 12 18
Mesi
IgG materne
IgM Bambino N
asci
ta IgG Bambino
IgA Bambino

Il bambino con IRR
La dimensione del problema
• In Italia il 6% dei bambini in età prescolare, presenta IRR nei primi 2-3 anni di vita
Lancet 2003; 361: 51–59

Gli agenti eziologici
• Gli agenti eziologici responsabili delle IRR siano identificabili solo occasionalmente, tuttavia quelli più frequentemente implicati sono i virus respiratori
• La primitiva infezione virale può essere complicata da infezioni secondarie, causate sia da batteri che da virus con la comparsa di otiti medie, sinusiti ed infezioni broncopolmonari

Viral involved in the pathogenesis of upper respiratory tract infections
Rhinoviruses 30 - 40%
Coronaviruses 10 – 15%
Influenza viruses 5 -15%
Respiratory syncytial virus 5%
Parainfluenza viruses 5%
Adenoviruses < 5%
Enteroviruses < 5%
Metapneumovirus ? Unknown ?
Unknown 20 – 30%
0 20 40 60 80 100 Estimated annual proportion of cases
Heikkinen T. Lancet 2003; 361: 51–59
?

Rhinovirus a … “soft” virus”
• Epithelial cell cytotoxicity does not appear to play a major role in the pathogenesis of Rhinovirus (RV) infection that is characterized by RV-induced
secretion of mediators of inflammation by airway structural/inflammatory cells

Gern JE. JACI 2006;117:72-8.
Seasonality and etiology of wheezing episodes in 285 children in the 1st year of life
RV
RV
RV
RV

Rhinoviruses replicate effectively at lower airway temperatures
Papadopoulos NG. Journal of Medical Virology 58:100–104 (1999)
Rhinovirus serotypes 1b, 2, 7, 9, 14, 16, 41, and 70 titrated in Ohio-HeLa cell cultures at either 33°C or 37°C.

Viral infections in relation to age among children hospitalized for wheezing
Heymann PW. JACI 2004: 114: 239-47.
Influenza Rhinovirus RSV Other viruses
Rhino
Rhino Rhino
Rhino
Rhino
RSV
RSV RSV

RV disrupts epithelial tight junctions and promotes transmigration of NTHi by paracellular route
Sajjan U. AJRCCM 2008; 178: 1271–1281
Control Rhinovirus (RV) 39
NTHi
NTHi
T.J. Zona occludins (ZO)-1

Outline
• Cosa intendiamo per Infezioni Respiratorie Ricorrenti?
• Perché i bambini in età prescolare sono più esposti alle Infezioni
Respiratorie Ricorrenti ?
• Cosa dobbiamo fare di fronte ad un bambino con Infezioni
Respiratorie Ricorrenti ?
La Diagnosi
La Profilassi
La Terapia

Host-related
• Low birth weight
• Chronological age
• Genetic factors
• Atopy
• Immunodeficiencies
Environment-related
• Day-care attendance
• Having a siblings <5 years of age at home
• Household crowding
• 2 or more smokers in the home
Major risk factors for RRI in childhood
• Atopy
• Immunodeficiencies
Immunity

Allergic children have more numerous and severe respiratory infections than
non-allergic children
Ciprandi G. Pediatr Allergy Immunol 2006: 17: 389–391
Rhinovirus
Nu
mb
er
of
RI/
3 m
on
ths
2.50 2.0 1.5 1.0 0.5 0.0
- - - - - -
Atopics Control
1.26
0.94
A. Total RI Number
***
10 8 6 4 2 0
- - - - - -
Atopics Control
8.92
4.85
B. Total RI Duration
Day
s
***

Vicious circle involving viral infection and allergic sensitization
Viral infection
Allergic sensitization
I.G.G.

Airway Epithelial
Cell
HDM
Oddera S. J of Asthma 1998; 35: 401-408.
Rhinovirus
Interaction between atopy and viral infection at respiratory level
Increased epithelial
permeability

Atopy and immunological disorders in 218 preschool Italian children with RRI
Dellepiane RM. Pediatr Med Chir 2009; 31: 161-4.
- - - - - -
IRR Control
50.5
35.3
A. RRI & Atopy A
top
ic c
hild
ren
(%
)
100 80 60 40 20 0
Rhinovirus
- - - - - -
39
B. RRI & Immunological disorders*
Ch
ildre
n w
ith
ID (
n°)
50 40 30 20 10 0
IRR
*IgA and IgG2 deficiency and transient
hypogammaglobulinemia

Coexistence of (partial) immune defects in children (4-14 yrs old) with recurrent respiratory infections
Bossuyt X. Clinical Chemistry 2007; 53: 124–130
A. IgA and/or IgG subclass deficiency
% o
f ch
ildre
n
50 40 30 20 10 0
- - - - - -
IRR Control
49%
14%
There was no increase in the prevalence of partial C4 or C2 deficiency, lymphocyte subset deficiency, or FcRII polymorphism in the IRR patients compared to controls
Belgium B. Deficient Ab response to Pneumococcal Polysaccharides
% o
f ch
ildre
n
50 40 30 20 10 0
- - - - - -
IRR Control
19%
0

IgA and/or IgG subclass deficiency in 225 children aged 6 months to 6 years with RRI
Ozkan H. J Invest Allergol Clin Immunol 2005; 15: 69-74.
IgG subclasses deficiency
% o
f ch
ildre
n
25 20 15 10 5 0
- - - - - -
IgG3 IgG2 IgG2+IgG3
9% 8%
19%
2%
Turkey

Outline
• Cosa intendiamo per Infezioni Respiratorie Ricorrenti?
• Perché i bambini in età prescolare sono più esposti alle Infezioni
Respiratorie Ricorrenti ?
• Cosa dobbiamo fare di fronte ad un bambino con Infezioni
Respiratorie Ricorrenti ?
La Diagnosi
La Profilassi
La Terapia

Diagnosis
• Careful Medical History and Clinical Examination are usually sufficient to make a diagnosis of RRI and no further examinations are generally needed in the majority of the cases
• A complete Blood Count with differential is sufficient to exclude neutropenia, while the evaluation of Antibodies against Recall Antigens rules out T-lymphocyte defects
• Total Immunoglobulin Levels are also important to evaluate the presence of a selective IgG or IgA deficiency but more severe cases may need further evaluation

Low proportion of children with recurrent RRI have detectable amounts of antigen-specific salivary sIgA
• Staphylococcus aureus
• Streptococcus pyogenes
• Klebsiella pneumoniae
• Haemophilus influenzae
• Moraxella catarrhalis
• Streptococcus pneumoniae
0 5 10 15 20 25 30 40 % of children
Rossi GA. Immunol Letters 2003; 86: 85-91.
sIgA

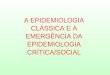
A 13 years old girl with 2nd episode of pneumonia of the right lower lobe

Angio-TAC con ricostruzione 3D
Pulmonary sequestration

A. B.
C.
Sacco O. Ped Pulmonol 2009; 44:244–248
Recurrent LRTI in a 5-yr-old girl

Reassure parents and give simple advises
• An accurate environmental prophylaxis
• Reducing environmental tobacco smoke at home
• The postponed enrolment of children at day-care centers reduces the risk of RI
• Optimal day-care center selection, when possible:
De Martino M. PAI 2007: 18 (Suppl. 18): 13–18.
Only a limited number of children
Large rooms with a good ventilation
Located in modern buildings in areas with less air pollution
With professionally trained staff

Prophylaxis-treatment
• Prophylactic treatment with antibiotics is neither indicated nor useful
De Martino M. PAI 2007: 18: 13–18.
• Adenoidectomy and tonsillectomy should be planned only in conditions included in validated guidelines
• The role of biological response modifiers (BRM) claimed to improve immunity in RRI children is still uncertain ……. As we will discuss later…..

Adenoidectomia o vigile attesa?
Adenoidi Adenoidectomia