Embed Size (px)
Citation preview

Left �trial Remodeling in Patients Youngerthan 70 Years with Diastolic and Systolic
Heart FailureFilippos Triposkiadis, MD, FESC, FACC, Christos Harbas, MD, Glafkos Kelepeshis, MD,
George Sitafidis, MD, John Skoularigis, MD, FESC, FACC, Vasilios Demopoulos, MD, and
Nikolaos Tsilimingas, MD, Larissa, GreeceObjective: We sought to determine left atrial (LA)volume and systolic function (LA remodeling) inyounger (<70 years) patients with systolic and dia-stolic heart failure (HF).Methods: In all, 32 patients with diastolic HF (leftventricular [LV] ejection fraction > 0.50), 26 patientswith systolic HF (LV ejection fraction < 0.50), and 48control subjects were studied. L� volume (cm3/m2)was echocardiographically determined at mitralvalve opening (maximal), mitral valve closure (min-imal), and atrial systole (electrocardiographic �wave) using the biplane area-length method. The LAactive emptying fraction (%) and ejection force(kdyne/m2) served as indices of LA systolic function.Results: LA maximal volume was greater in systolicHF than diastolic HF and in the latter greater thancontrol (68.6 � 13.8 vs 52 � 11.6 vs 42.9 � 14.4,
doi:10.1016/j.echo.2006.08.013
was similar between diastolic HF and control, andgreater than systolic HF (31.5 � 8.1 vs 36.3 � 7 vs26.6 � 6.2, respectively, P < .0001), whereas LAejection force was similar in diastolic and systolicHF and greater than control (5.05 � 1.3 vs 4.98 �2.17 vs 3.63 � 2.05, respectively, P � .001). Vmaxwas related to body surface area, brain natriureticpeptide, and LV mass in diastolic HF (multiple R2 �0.74) and to diastolic blood pressure, LV mass, andearly to late transmitral flow velocity ratio in sys-tolic HF (multiple R2 � 0.96).Conclusions: LA remodeling is more severe in sys-tolic HF than diastolic HF and governed by differentmechanisms. This may be of significant clinicalrelevance regarding the morbidity and mortality ofthese two conditions. (J Am Soc Echocardiogr 2007;20:177-185.)
respectively, P < .0001). Active emptying fraction
Traditionally, chronic heart failure (HF) has beenattributed to left ventricular (LV) systolic dysfunc-tion with decreased LV ejection fraction (LVEF)leading to an increase in LV filling pressures andvolumes (systolic HF).1 However, recent studiessuggest that in approximately 40% of incident and50% to 60% of prevalent cases with HF, LVEF ispreserved.2 Although abnormalities of LV systolicfunction are often present in this setting,3 the pre-dominant underlying pathophysiology seems to bean abnormality of LV active relaxation and passivestiffness (diastolic HF).4 Patients with systolic HFdiffer substantially from those with diastolic HF indemographic characteristics, ventricular remodel-ing, ventricular function, mortality, and underlyingpathophysiology.5 There is limited information re-
From the Departments of Cardiology and Cardiovascular andThoracic Surgery (N.T.), Larissa University Hospital.Reprint requests: Filippos Triposkiadis, MD, FESC, FACC, De-partment of Cardiology, Larissa University Hospital, PO Box1425, 411 10 Larissa, Greece (E-mail: [email protected]).0894-7317/$32.00Copyright 2007 by the American Society of Echocardiography.
garding the extent of left atrial (LA) remodeling inyounger (�70 years) patients with HF.
We used a simple and feasible echocardiographicmethod to assess LA volumes in 58 consecutivepatients with HF (32 with diastolic and 26 withsystolic) and compared the findings with those of 48healthy control subjects. Our objective was to ex-amine the changes in LA volume and systolic func-tion (LA remodeling) and the underlying mecha-nisms in this patient population.
METHODS
Patients
From May 2003 to January 2005, 86 consecutive patientswith HF defined according to the Framingham criteria6
were prospectively studied in our department. After ex-clusion of those with atrial fibrillation (n � 14), moderateor severe mitral regurgitation (n � 8), and atrioventricularconduction abnormalities (n � 4), 58 patients entered thestudy. In all, 32 had diastolic HF (15 arterial hypertension,11 coronary artery disease, 5 aortic stenosis, and 1 hyper-
trophic cardiomyopathy), whereas 26 had systolic HF (11177

Journal of the American Society of Echocardiography178 Triposkiadis et al February 2007
ischemic and 9 idiopathic dilated cardiomyopathy, 5arterial hypertension, and 1 aortic regurgitation).
Diastolic HF was defined by the presence of: (1) LVEFof 0.50 or greater within 72 hours of the HF event; and(2) one or more of the following: LV concentric hypertro-phy; systolic blood pressure (SBP) greater than 160 mmHg; diastolic blood pressure (DBP) greater than 100 mmHg; precipitation of the event by a fluid load (eg, �500 mLsodium chloride (NaCl) 0.9% within 15 minutes intrave-nously); and clinical improvement in response to ther-apy.7,8 Systolic HF was defined by the presence of: (1)LVEF less than 0.50; and (2) LV eccentric hypertrophy.
In all, 48 consecutive normotensive patients evaluatedfor dyspnea or chest pain with normal findings in exerciseelectrocardiography and echocardiography served ashealthy control subjects. The study complied with theDeclaration of Helsinki and was conducted according tothe guidelines of the hospital ethics committee.
Echocardiography
Echocardiography was performed with an imaging systemequipped with a 3.0-MHz transducer (Sonos 1000, Hewlett-Packard Co, Loveland, Colo). Simultaneously with the ultra-sound examination, an electrocardiogram was recorded forlater review with a videorecorder. M-mode measurementswere made according to the guidelines of the AmericanSociety of Echocardiography.9 LV mass (LVM) was deter-mined according to the method of Devereux and Reichek.10
The LV morphologic pattern was considered normal if LVMindex (LVMI) was 50 g/height(m)2.7 or less and relative wallthickness (RWT) [(interventricular septum diameter � pos-terior wall diastolic thickness)/LV end-diastolic diameter]was 0.44 or less. Concentric hypertrophy was defined as aLVMI greater than 50 g/m2.7 and RWT greater than 0.44,whereas eccentric hypertrophy was defined as LVMI greaterthan 50 g/m2.7 and RWT of 0.44 or less.11
LV end-diastolic and end-systolic volumes were calcu-lated with 2-dimensional echocardiography using the for-mula of Teichholz et al.12 Cardiac output was calculated asthe product of stroke volume and heart rate. LV systolicfunction was quantified with the shortening and EF.Moreover, the LV end-systolic wall stress (SBP � R/h)(expressed in mm Hg)13 and the LV end-systolic meridi-onal wall stress [(SBP � D � 1.35)/4 � h � (1 � h/D)]14
(expressed in g/cm2) were also calculated. In these for-mulas, D is the LV systolic diameter, h is the LV systolicwall thickness, 1.35 is the converting factor from mm Hgto g/cm2, and R is the LV systolic radius (D/2).
LA volumes were determined with the biplane area-lengthmethod as follows: volume � 8 (area in 4-chamber) � (areain 2-chamber)/3 � (LA common length).15,16 Commonlength was defined as the longest line that could be drawnbetween the posterior LA wall and the midportion of themitral valve (MV). LA maximal volume was measured atthe point of MV opening and minimal volume was mea-sured at the point of MV closure; LA volume at onset of LAsystole was considered the volume corresponding to theonset of the � wave in the simultaneously recorded
electrocardiogram.The transmitral flow velocity profile was assessed byplacing the sample volume between the tips of the MVleaflets, where the maximal diastolic flow velocity wasrecorded. Parameters measured were the E wave, A wave,the ratio of E wave to A wave (E/A), and deceleration time.Triphasic mitral inflow with middiastolic filling, a markerof advanced LV diastolic dysfunction, was also searched.17
Right upper pulmonary vein flow velocities were re-corded from the apical view with the use of pulsedDoppler in 74 (69.8%) of the study participants. Dopplermeasurements were analyzed for peak systolic, peak dia-stolic, and flow reversal velocities. The difference be-tween the duration of pulmonary vein flow reversal andmitral A-wave duration was also calculated as an index ofLV filling pressure.18
The LA active emptying (systolic) function was assessedwith the following parameters16: (1) LA active emptyingvolume (ACTEV), LA volume at onset of LA systole minusLA minimal volume; (2) LA active emptying fraction(ACTEF), ratio of LA ACTEV to LA volume at onset of LAsystole; and (3) LA ejection force (LAEF) according to themethod of Manning et al19: LAEF � 0.5 � � � MV� � A2,where � is blood density � 1.06 gm/cm3, MVA is MV area(cm2), and � is peak late diastolic transmitral flow velocity(cm/s). By substituting the ratio of LA ACTEV (cm3/m2)/late diastolic transmitral flow velocity integral (VTIA) (cm)for MVA, the equation becomes: LAEF � 0.5 � � � (ACTEV/VTIA) � A2. Taking into consideration that ACTEV � Vp� ACTEF, where Vp � LA volume at onset of atrial systoleand ACTEF � LA ACTEF, LAEF (kdyne/m2) � 0.5 � � � Vp� ACTEF � A2/VTIA.16
The values of all echocardiographic Doppler parametersin this study represent the mean value of measurementstaken in 3 consecutive cardiac cycles. The reproducibility ofechocardiographic measurements was determined by com-paring 35 echocardiograms read by two skilled sonographers(G. K. and G. S.). The interobserver mean percent error(absolute difference between two observations divided bythe mean and expressed in percentage) was 8.1% for LVMand 4.1% for LA volume measurements. The intraobservermean percent error for G. S. was 8.7% for LVM and 3.9% forLA volume measurements. The corresponding values forG. K. were 8.8% and 3.7%, respectively.
Brain Natriuretic Peptide Plasma Levels
Brain natriuretic peptide (BNP) plasma levels were deter-mined with a single-use fluorescence immunoassay devicedesigned to determine the concentration of BNP in EDTAanticoagulated whole blood or plasma specimens (TriageBN� test, Biosite, San Diego, Calif).
Statistical Analysis
Continuous variables are expressed as mean 1 SD andcompared with 1-way analysis of variance, whereas cate-gorical variables are expressed as percentages and com-pared using the 2-sided Fisher exact test or the 2 test asappropriate. Multiple comparisons of both continuous
and categorical variables were adjusted using Bonferroni’s
Journal of the American Society of EchocardiographyVolume 20 Number 2 Triposkiadis et al 179
correction. The association between LA maximal volumeand continuous variables (age, body surface area [BSA],SBP, DBP, heart rate, BNP, E/A, deceleration time, pulmo-nary vein reverse flow velocity, LVEF, LVM, LV stress, LVmeridional end-systolic stress) was assessed separately indiastolic and systolic HF using univariable linear regres-sion analysis. Then, the variables exhibiting a P value lessthan .1 were incorporated in backward multivariableregression analysis, to further assess their associationwith LA maximal volume. The adequacy of the modelsfor diastolic and systolic HF was checked using thecoefficient of determination (R2), the normal probabil-ity plot,and the plot of residuals against predictedvalues. An effect was considered statistically significantwhen P was less than .05. A statistical package (GBSTAT v10.0, Dynamic Microsystems Inc, Silver Spring,Md) was used for data analysis.
RESULTS
Demographic and Clinical Characteristics
As shown in Table 1, patients were older in diastolicHF group than in the control group. Sex distribution,weight, height, and BSA were not significantly differ-ent in the 3 groups, whereas heart rate was higher inpatients with systolic HF than healthy control subjects.SBP and DBP were greater in diastolic HF than in
Table 1 Baseline demographic and clinical features of the
Parameter
Control
(n � 48)
Age, y 48.2 11Male/female 36/12Weight, kg 74.3 12.4Height, cm 173.2 8Body surface area, m2 1.89 0.19Heart rate, beats/min 65 8.6Systolic BP, mm Hg 119.6 10.2Diastolic BP, mm Hg 76.1 6.5History of hypertension —Diabetes mellitus —History of COPD —NYHA functional class
II —III —IV —
MedicationsDiuretics —Beta-blockers —ACEi/ARB —Dihydropyridines —
ACEi, Angiotensin-converting enzyme inhibitor; ARB, angiotensin receptoheart failure; NYHA, New York Heart Association.*P � .05 vs control.†P � .01 vs control.‡P � .01 vs diastolic HF.
systolic HF or control groups. Hypertension was more
common in diastolic than in systolic HF. There wereno differences in the prevalence of diabetes orchronic obstructive pulmonary disease/asthma,New York Heart Association functional class, ordrug treatment in the two HF groups.
LV Morphology and Function
As shown in Table 2, the interventricular septal thick-ness was greater in diastolic than in systolic HF and inthe latter greater than control, whereas posterior wallthickness was greater in diastolic than in systolic HF orcontrol. The LV end-diastolic and end-systolic diame-ters were greater in systolic HF than control and in thelatter greater than diastolic HF. The RWT was greaterin diastolic than systolic HF or control, whereas theLVMI was greater in systolic than diastolic HF and inthe latter greater than control. Concentric hypertro-phy was present in 25 patients with diastolic HF(78.1%), whereas eccentric hypertrophy was by defi-nition present in all patients with systolic HF. The LVend-diastolic and end-systolic volume indices weregreater in systolic HF than control and in the lattergreater than diastolic HF, whereas the stroke volumeindex was similar in the 3 groups. The LV shorteningand EFs were similar in diastolic HF and control andgreater than systolic HF, whereas the cardiac indexwas similar in the 3 study groups. The LV end-systolicwall stress and end-systolic meridional wall stress were
opulation
stolic HF
n � 32)
Systolic HF
(n � 26)
P value
(overall)
9 10.2† 53.5 12.2 �.000116/16 18/8 .3713 13 79.1 20.3 .3949 4.9 169.5 9.3 .4029 0.18 1.92 0.27 .8163 12.1 71.5 9.1* .0201 13.7† 115.5 18‡ �.00015 9.3† 69.5 12.5‡ �.0001(78.1%) 9 (34.6%)‡ �.0001(31.3%) 8 (30.1%) 1.000(15.6%) 3 (11.5%) .719
(68.8%) 15 (57.7%) .422(15.6%) 6 (23.1%) .517(15.6%) 5 (19.2%) .740
(56.3%) 18 (69.2%) .416(43.8%) 14 (53.8%) .598(50%) 18 (69.2%) .183(56.3%) 12 (46.2%) .598
r; BP, blood pressure; COPD, chronic obstructive pulmonary disease; HF,
study p
Dia
(
5
77.167.1.869.
150.84.2510
5
2255
18141618
r blocke
greater in systolic than in diastolic HF or control.

Journal of the American Society of Echocardiography180 Triposkiadis et al February 2007
The BNP plasma levels were greater in systolicthan in diastolic HF and in the latter greater thancontrol (Figure 1).
Pulmonary and Transmitral Flow
As shown in Table 3, the pulmonary vein systolicand diastolic flow velocities were similar in the 3study groups, whereas the pulmonary vein reverseflow velocity was greater in systolic than indiastolic HF or control. Mild mitral regurgitationwas more common in systolic than in diastolic HFor control. The E wave was similar in the 3 studygroups, whereas the A wave was greater in dia-stolic than in systolic HF or control. The differ-ence between pulmonary vein flow reversal dura-tion and mitral A-wave duration was greater inpatients with diastolic and systolic HF than inhealthy control subjects. Finally, the decelerationtime was greater in diastolic than in systolic HF orcontrol. Two of the study patients (6.25%) withdiastolic HF exhibited triphasic mitral inflow withmiddiastolic filling.
LA Function
As shown in Table 4, LA volumes (maximal, atonset of atrial systole, and minimal) were greaterin systolic than in diastolic HF and in the lattergreater than control. The LA ACTEV and the LAcontribution to LV stroke volume were similar insystolic and diastolic HF and greater than control,whereas the LA ACTEF was lower in systolic thanin diastolic HF or control. The LAEF was similar indiastolic and systolic HF and greater than control.
In univariable regression analyses (Table 5) the LA
Table 2 Left ventricular morphology and function
Parameter
Control
(n � 48)
Interventricular septal thickness, mm 0.82 0.14Posterior wall thickness, mm 0.88 0.13End-diastolic diameter, mm/m2 2.84 0.46End-systolic diameter, mm/m2 1.91 0.65Relative wall thickness 0.33 0.06Mass index, g/m2 87.5 20.6Mass index, g/height2.7 37.5 9.2End-diastolic volume, mL/m2 74.2 22.1End-systolic volume, mL/m2 34.6 22.1Stroke volume index, mL/m2 39.6 8.1Shortening fraction, % 33 15Ejection fraction, % 56.5 13.5Cardiac index, L/m2 2.55 0.54End-systolic wall stress, mm Hg 197 67End-systolic meridional wall stress, g/cm2 103 43
HF, Heart failure.*P � .05 vs control.†P � .01 vs control.‡P � .01 vs diastolic HF.
maximal volume was related to BSA, BNP plasma
levels, and LVM in diastolic HF and to age, BSA, DBP,BNP plasma levels, E/A ratio, deceleration time,pulmonary vein reverse flow velocity, LVEF, andLVM in systolic HF.
In multivariable regression analysis (Table 6) themost important determinants of LA maximal volume indiastolic HF were BSA, BNP plasma levels, and LVM,whereas in systolic HF they were DBP, LVM, and E/Aratio. In checking the adequacy of the models, thecoefficients of determination (R2) were 0.74 and 0.96in diastolic and systolic HF, respectively, whereas inboth patient groups the normal probability plotshowed no deviation from normality, and the plot of
Figure 1 Brain natriuretic peptide (BNP) plasma levels instudy population.
Diastolic HF
(n � 32)
Systolic HF
(n � 26)
P value
(overall)
1.33 0.14† 1.1 0.3†‡ �.00011.33 0.10† 0.92 0.17‡ �.0001
2.5 0.28† 3.7 0.43†‡ �.00011.63 0.20* 3.18 0.45†‡ �.00010.57 0.07† 0.29 0.06‡ �.0001
134.5 24† 162.4 21.6†‡ �.000162.4 9.5† 75.5 15.1†‡ �.000156.3 13.8† 137.7 26.5†‡ �.000120.9 4.3† 98.4 24.4†‡ �.000135.3 11 39.4 3.4 .200
35 4.4 14 3.2†‡ �.000161.9 6.2 29.6 6.2†‡ �.00012.49 0.71 2.8 0.3 .086173 19 398 116†‡ �.0001
81 10 235 75†‡ �.0001
residual versus predicted volume showed no pattern.
itral flow
Journal of the American Society of EchocardiographyVolume 20 Number 2 Triposkiadis et al 181
DISCUSSION
This study demonstrated that: (1) LA remodeling ismore severe in systolic than in diastolic HF asindicated by the greater increase in LA volume andthe depressed LA systolic function in the former;
Table 3 Pulmonary and transmitral flow velocities
Parameter
Control
(n � 48)
Pulmonary vein systolic flow, cm/s 56.8 11.6Pulmonary vein diastolic flow, cm/s 51.5 10.9Pulmonary vein reverse flow, cm/s 28.6 5.9Mild mitral regurgitation 9 (18.8%)E wave, cm/s 66.6 11.4A wave, cm/s 60.1 20.1E/A 1.24 0.47PVa-MVa �21 12Deceleration time, ms 202.3 35.7
E/A, Ratio of peak early to peak late transmitral flow velocity; HF, heart failuand mitral A-wave duration.*P � .05 vs control.†P � .01 vs control.‡P � .01 vs diastolic HF.
Table 4 Left atrial volumes and systolic function
Parameter
Control
(n � 48)
Maximal volume, cm3/m2 42.9 14.4Volume at onset of atrial systole, cm3/m2 31.2 12.4Minimal volume, cm3/m2 20.4 10.1Active emptying volume, cm3/m2 10.9 3.3Active emptying fraction, % 36.3 7Atrial contribution to LV filling, % 26 9.5Ejection force, kdyne/m2 3.63 2.05
HF, Heart failure; LV, left ventricular.*P � .05 vs control.†P � .01 vs control.‡P � .05 vs diastolic HF.§P � .01 vs diastolic HF.
Table 5 Pearson’s correlation coefficient of left atrial maxi
Parameter
Diastoli
r
Age �0.001Body surface area 0.360Systolic blood pressure �0.064Diastolic blood pressure 0.239Heart rate �0.309BNP 0.655E/A �0.118Deceleration time �0.026Pulmonary vein reverse flow �0.301LV ejection fraction 0.213LV mass 0.440LV stress 0.077LV meridional end-systolic stress 0.103
BNP, Brain natriuretic peptide; E/A, ratio of peak early to peak late transm
and (2) the mechanisms that govern LA remodeling
differ in diastolic and systolic HF. However, LVM isa major determinant of LA volume in both.
Comparison with Previous Studies
Our findings are in accordance with those of previ-ous studies, which showed that LA size is greater in
Diastolic HF
(n � 32)
Systolic HF
(n � 26)
P value
(overall)
63.2 31.4 61.6 17.1 .36053.9 29.9 65 31.4 .06328.3 4.4 38.8 5.6*‡ �.000110 (31.3%) 19 (73.1%)†‡ .0005
62.3 11.9 67.2 12.7 .19289 22.9* 63.6 19.3‡ �.0001
0.72 0.13* 1.20 0.53‡ �.00017 18* 15 23* �.0001
271.5 40.8* 202.3 39.1‡ �.0001
MVa, difference between duration of pulmonary vein flow reversal duration
Diastolic HF
(n � 32)
Systolic HF
(n � 26)
P value
(overall)
52 11.6† 68.6 13.8†§ �.000138.6 8.9* 55.4 13.3†§ �.000126.6 7.7* 41.3 12.6†§ �.0001
13 3.5* 14.2 2.7* �.000131.5 8.1 26.6 6.2†‡ �.0001
37 14† 37 8.4† .0065.05 1.3† 4.98 2.17* .001
lume with clinical and echocardiographic parameters
� 32) Systolic HF (n � 26)
P r P
.994 �0.495 .010
.043 0.410 .037
.726 �0.344 .085
.188 �0.483 .012�.086 �0.352 .078�.0001 0.458 .019
.557 0.694 �.0001
.889 �0.710 �.0001
.094 0.728 �.0001
.259 �0.392 .043
.012 0.503 .009
.674 0.144 .482
.576 0.168 .413
velocity; HF, heart failure; LV, left ventricular.
re; PVa-
mal vo
c HF (n
eccentric than concentric hypertrophy20 and di-

itral flow
Journal of the American Society of Echocardiography182 Triposkiadis et al February 2007
rectly related to LVM.21,22 Moreover, they are in fullagreement with the findings of Rossi et al,23 whodemonstrated that the LA is frequently dilated inpatients with HF and preserved LVEF compared
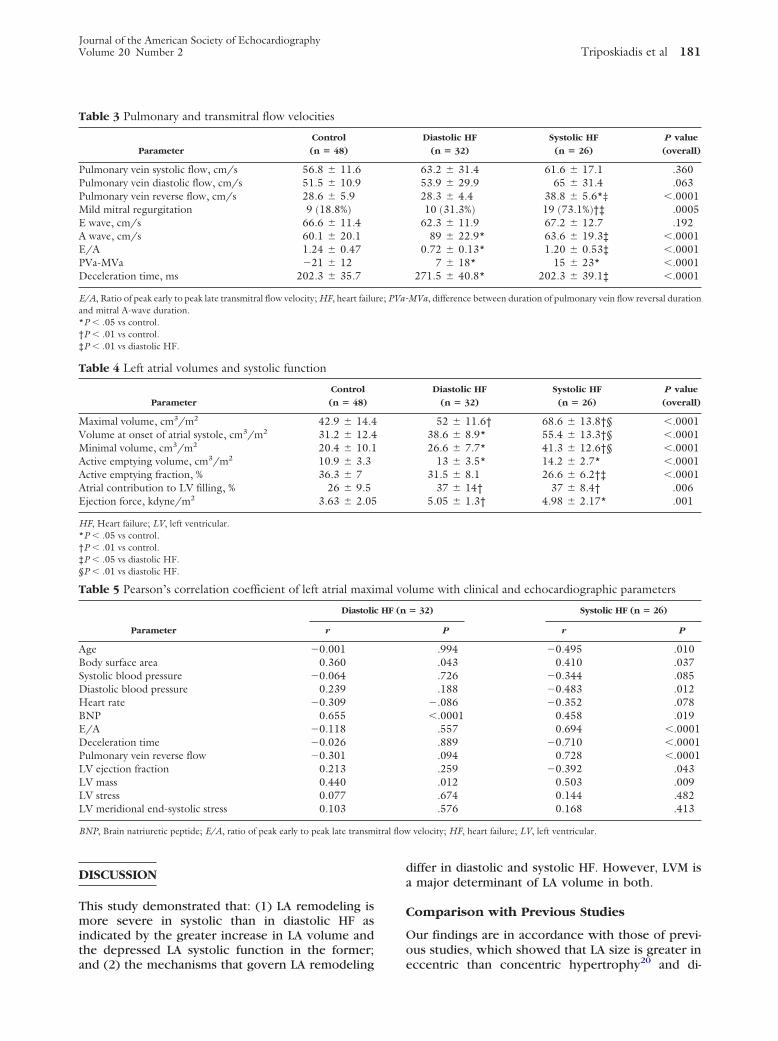
Figure 2 Mechanisms of left atrial (LA) remodeling andLA dynamics at rest in diastolic heart failure. Insult leadsto left ventricular (LV ) diastolic dysfunction, which isassociated with LV hypertrophy in majority of cases. LVejection fraction is preserved. Resulting chronic increasein LA afterload leads to increase in LA volume at onset ofatrial systole, which increases LA ejection force. Increasein LA ejection force results in increase in LA activeemptying volume and in active LA contribution to LVfilling, maintaining resting LV stroke volume and cardiacoutput.
Table 6 Multivariate stepwise regression analyses for left a
Independent variable
Beta
coefficient
Diastolic HF (multiple R � 0.86, multiple R2 � 0.74, SE � 12.0Body surface area 41.2BNP 0.10LV mass 0.13
Systolic HF (multiple R � 0.98, multiple R2 � 0.96, SE � 5.57,Diastolic blood pressure �0.50LV mass 0.24E/A 42.9
BNP, Brain natriuretic peptide; E/A, ratio of peak early to peak late transm
with healthy control subjects. In contrast to our
findings, Gottdiener et al24 recently reported that LAvolume does not differ between elderly (�65 years)patients with systolic versus diastolic HF. However,these findings cannot be extrapolated to youngerpatients with HF, because aging per se is associatedwith progressive LV diastolic dysfunction, character-ized by a decrease in the transmitral early wave/atrial wave (E/A) velocity ratio, LA hypertrophy, andLA enlargement.25 Indeed, grades II and III diastolicdysfunction are associated with 24% and 62% in-creases in LA volume, respectively, and the capacityof the LA to dilate is not unlimited.26 The presenceof triphasic mitral inflow in only two of the patients(6.25%) with diastolic HF in the current study doesnot exclude severe diastolic dysfunction, becausebradycardia is prerequisite for its appearance.17
LA Function
The LA modulates pulmonary vein flow and LVfilling. In pulmonary vein Doppler recordings, ante-grade systolic and diastolic components and flowreversal during atrial contraction may be found.27
However, the pronounced heterogeneity of pulmo-nary vein flow patterns in healthy individuals in-creases the difficulty of discerning abnormal fromnormal flow patterns.28 In the current study systolicand diastolic pulmonary flow velocities were similarin the control and patient groups, whereas thepulmonary vein reverse flow velocity was greater insystolic than in diastolic HF or control.
LV filling is modulated through a phase of reser-voir during systole, a conduit phase during diastole,and an active contractile (active emptying) compo-nent during late diastole.15,16 Loss of atrial contrac-tion, as a result of atrial fibrillation or ventricularpacing, reduces cardiac output by approximately15% to 20%.29
LA dilation associated with augmented LA activeemptying (systolic) function and active LA contribu-tion to LV stroke volume (booster pump function)are common in LV diastolic dysfunction.29 However,attenuation of LA active emptying function has beenreported in idiopathic dilated cardiomyopathy, de-
aximal volume
SE (B)
T
value P value
25.96)14.5 2.85 .0082
0.014 7.4 �.00010.05 2.7 .011
3.8)0.098 �5.14 �.00010.019 13.1 �.00012.17 19.8 �.0001
velocity; HF, heart failure; LV, left ventricular.
trial m
1, F �
F � 20
spite the severe LV diastolic and systolic dysfunction
Journal of the American Society of EchocardiographyVolume 20 Number 2 Triposkiadis et al 183
in this disease state and has been attributed to LAmyopathy.30-32
In this study the LAEF, ACTEV, and active LAcontribution to LV stroke volume were increasedboth in diastolic and in systolic HF, despite theincreased LV filling pressure in both disease entities.However, the underlying mechanisms were signifi-cantly different. Indeed, in diastolic HF a moderateincrease in LA volume at onset of atrial systoleassociated with no significant changes in LA ACTEFwas observed, whereas in systolic HF a markedincrease in LA volume at onset of atrial systole wasobserved that compensated for the depressed LAACTEF (Figures 2 and 3). Functional mitral regurgi-tation, which was significantly more common in
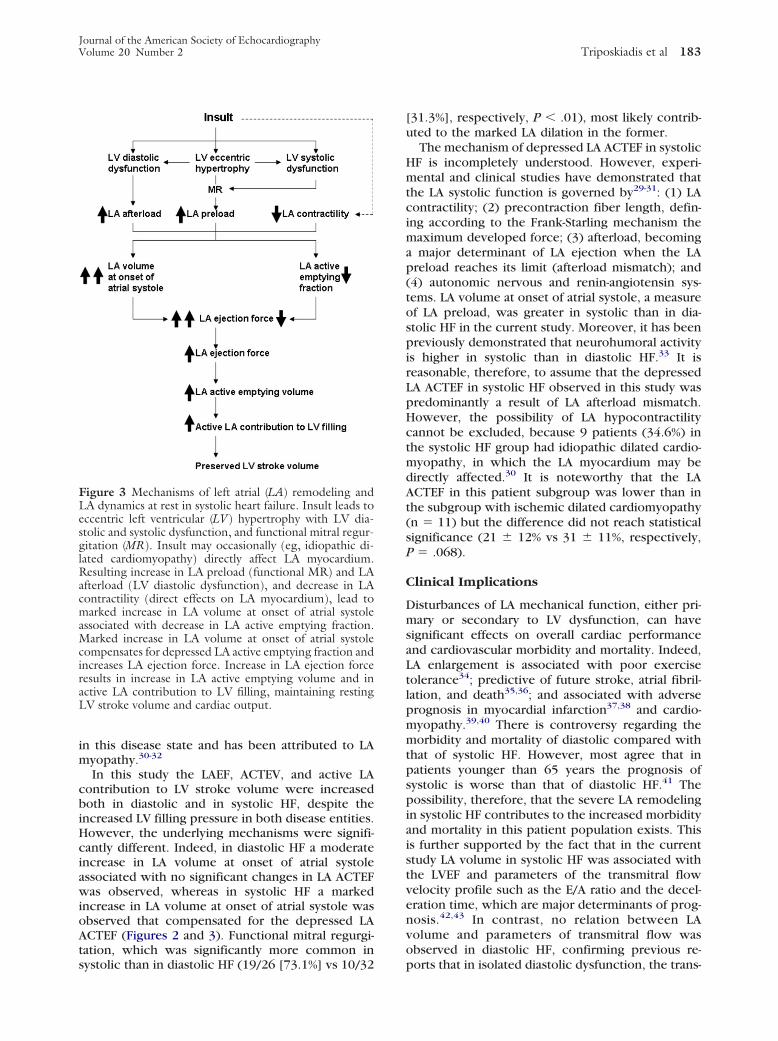
Figure 3 Mechanisms of left atrial (LA) remodeling andLA dynamics at rest in systolic heart failure. Insult leads toeccentric left ventricular (LV) hypertrophy with LV dia-stolic and systolic dysfunction, and functional mitral regur-gitation (MR). Insult may occasionally (eg, idiopathic di-lated cardiomyopathy) directly affect LA myocardium.Resulting increase in LA preload (functional MR) and LAafterload (LV diastolic dysfunction), and decrease in LAcontractility (direct effects on LA myocardium), lead tomarked increase in LA volume at onset of atrial systoleassociated with decrease in LA active emptying fraction.Marked increase in LA volume at onset of atrial systolecompensates for depressed LA active emptying fraction andincreases LA ejection force. Increase in LA ejection forceresults in increase in LA active emptying volume and inactive LA contribution to LV filling, maintaining restingLV stroke volume and cardiac output.
systolic than in diastolic HF (19/26 [73.1%] vs 10/32
[31.3%], respectively, P � .01), most likely contrib-uted to the marked LA dilation in the former.
The mechanism of depressed LA ACTEF in systolicHF is incompletely understood. However, experi-mental and clinical studies have demonstrated thatthe LA systolic function is governed by29-31: (1) LAcontractility; (2) precontraction fiber length, defin-ing according to the Frank-Starling mechanism themaximum developed force; (3) afterload, becominga major determinant of LA ejection when the LApreload reaches its limit (afterload mismatch); and(4) autonomic nervous and renin-angiotensin sys-tems. LA volume at onset of atrial systole, a measureof LA preload, was greater in systolic than in dia-stolic HF in the current study. Moreover, it has beenpreviously demonstrated that neurohumoral activityis higher in systolic than in diastolic HF.33 It isreasonable, therefore, to assume that the depressedLA ACTEF in systolic HF observed in this study waspredominantly a result of LA afterload mismatch.However, the possibility of LA hypocontractilitycannot be excluded, because 9 patients (34.6%) inthe systolic HF group had idiopathic dilated cardio-myopathy, in which the LA myocardium may bedirectly affected.30 It is noteworthy that the LAACTEF in this patient subgroup was lower than inthe subgroup with ischemic dilated cardiomyopathy(n � 11) but the difference did not reach statisticalsignificance (21 12% vs 31 11%, respectively,P � .068).
Clinical Implications
Disturbances of LA mechanical function, either pri-mary or secondary to LV dysfunction, can havesignificant effects on overall cardiac performanceand cardiovascular morbidity and mortality. Indeed,LA enlargement is associated with poor exercisetolerance34; predictive of future stroke, atrial fibril-lation, and death35,36; and associated with adverseprognosis in myocardial infarction37,38 and cardio-myopathy.39,40 There is controversy regarding themorbidity and mortality of diastolic compared withthat of systolic HF. However, most agree that inpatients younger than 65 years the prognosis ofsystolic is worse than that of diastolic HF.41 Thepossibility, therefore, that the severe LA remodelingin systolic HF contributes to the increased morbidityand mortality in this patient population exists. Thisis further supported by the fact that in the currentstudy LA volume in systolic HF was associated withthe LVEF and parameters of the transmitral flowvelocity profile such as the E/A ratio and the decel-eration time, which are major determinants of prog-nosis.42,43 In contrast, no relation between LAvolume and parameters of transmitral flow wasobserved in diastolic HF, confirming previous re-
ports that in isolated diastolic dysfunction, the trans-
Journal of the American Society of Echocardiography184 Triposkiadis et al February 2007
mitral flow pattern is poorly related to filling pres-sures.44
Study Limitations
This study has several limitations.First, accurate diagnosis of diastolic HF requires
demonstration of an upward shift of diastolic pres-sure-volume relation compared with normal.4 How-ever, it has been recently demonstrated that in HFwith normal EF there are significant abnormalities inactive relaxation and passive stiffness and that theprinciple cause of elevated diastolic pressures is theabnormal diastolic function.4
Second, LV filling pressures were not measured.Alternatively the ratio of mitral E velocity to earlydiastolic velocity of the mitral annulus might havebeen used. However, there is wide variability in LVdiastolic pressure for the ratio mitral E velocity toearly diastolic velocity of the mitral annulus valuesbetween 8 and 15, which may be found in up to 36%of patients.45 Moreover, it has been recently demon-strated that the difference between the duration ofthe pulmonary vein flow reversal and mitral A-waveduration, which was used in this study, is a reliableindicator of LV end-diastolic pressure.17
Third, LA volume measurements are based ongeometric assumptions, which have not been thor-oughly validated. Moreover, although several meth-ods have been described for the measurement of LAvolume, no standardized method has been adopted.46
However, the biplane area-length method used inthe current study compares favorably with the 3-di-mensional echocardiographic methods of LA vol-ume determination47,48 and has been recently vali-dated in a population study.49
Conclusions
LA remodeling is more severe in systolic than indiastolic HF as indicated by the greater increase inthe LA volume and the depressed LA emptyingfraction in the former. LA dilation and depressed LAsystolic function have been linked with poor exer-cise tolerance, increased morbidity, and increasedmortality in a variety of clinical settings and may,therefore, contribute to the adverse prognosis ofsystolic HF. Routine echocardiographic Dopplerevaluation of LA volume and systolic function mayprove useful in the risk stratification and evaluationof the response to treatment of patients with HF.
REFERENCES
1. Goldsmith SR, Dick C. Differentiating systolic from diastolicheart failure: pathophysiologic and therapeutic considerations.Am J Med 1993;95:645-5.
2. Senni M, Redfield MM. Heart failure with preserved systolicfunction. A different natural history? J Am Coll Cardiol 2001;
38:1277-82.3. Yip G, Wang M, Zhang Y, Fung JW, Ho PY, Sanderson JE.Left ventricular long axis function in diastolic heart failure isreduced in both diastole and systole: time for a redefinition?Heart 2002;87:121-5.
4. Zile MR, Baicu CF, Gaasch WH. Diastolic heart failure–abnormalities in active relaxation and passive stiffness of theleft ventricle. N Engl J Med 2004;350:1953-9.
5. Aurigemma GP, Gaasch WH. Clinical practice: diastolic heartfailure. N Engl J Med 2004;351:1097-105.
6. McKee PA, Castelli WP, McNamara PM, Kannel WB. Thenatural history of congestive heart failure; the Framinghamstudy. N Engl J Med 1971;285:1441-6.
7. Vasan RS, Levy D. Defining diastolic heart failure: a call forstandardized diagnostic criteria. Circulation 2000;101:2118-21.
8. Triposkiadis F, Moyssakis I, Makris T, Hatzizaharias A, Had-jinikolaou L, Kyriakidis M. Assessment of left ventriculardiastolic reserve in essential hypertension: the acute saline loadtest. Eur J Clin Invest 2001;31:690-7.
9. Gardin JM, Henry WL, Savage DD, Ware JH, Burn C, BorerJS. Echocardiographic measurements in normal subjects: eval-uation of an adult population without clinically apparent heartdisease. J Clin Ultrasound 1979;7:439-45.
10. Devereux RB, Reichek N. Echocardiographic determinationof left ventricular mass in man: anatomic validation of themethod. Circulation 1977;55:613-8.
11. Ganau A, Devereux RB, Roman MJ, de Simone G, PickeringTG, Saba PS, et al. Patterns of left ventricular hypertrophy andgeometric remodeling in essential hypertension. J Am CollCardiol 1992;19:1550-8.
12. Teichholz LE, Kreulen T, Herman MV, Gorlin R. Problemsin echocardiographic volume determinations: echocardio-graphic angiographic correlations in the presence or absenceof asynergy. Am J Cardiol 1976;37:7-11.
13. Quinones MA, Mokotoff DM, Nouri S, Winters WL Jr, MillerRR. Noninvasive quantification of left ventricular wall stress:validation of method and application to assessment of chronicpressure overload. Am J Cardiol 1980;45:782-90.
14. Grossman W, Jones D, McLaurin LP. Wall stress and patternsof hypertrophy in the human left ventricle. J Clin Invest1975;56:56-64.
15. Ren JF, Kotler MN, DePace NL, Mintz GS, Kimbiris D,Kalman P, et al. Two-dimensional echocardiographic deter-mination of left atrial emptying volume: a non-invasive indexin quantifying the degree of non-rheumatic mitral regurgita-tion. J Am Coll Cardiol 1983;2:729-36.
16. Triposkiadis F, Tentolouris K, Androulakis A, Trikas A, Tout-ouzas K, Kyriakidis M, et al. Left atrial mechanical function inthe healthy elderly: new insights from a combined assessmentof changes in atrial volume and transmitral flow velocity. J AmSoc Echocardiogr 1995;8:801-9.
17. Ha JW, Oh JK, Redfield MM, Ujino K, Seward JB, Tajik AJ.Triphasic mitral inflow velocity with middiastolic filling: clin-ical implications and associated echocardiographic findings.J Am Soc Echocardiogr 2004;17:428-31.
18. Hadano Y, Murata K, Liu J, Oyama R, Harada N, Okuda S,et al. Can transthoracic Doppler echocardiography predict thediscrepancy between left ventricular end-diastolic pressure andmean pulmonary capillary wedge pressure in patients withheart failure? Circ J 2005;69:432-8.
19. Manning MJ, Silverman DI, Katz SE, Douglas PS. Atrialejection force: noninvasive assessment of left atrial systolicfunction. J Am Coll Cardiol 1993;22:221-5.
20. Gerdts E, Oikarinen L, Palmieri V, Otterstad JE, Wachtell K,
Boman K, et al. Correlates of left atrial size in hypertensive
Journal of the American Society of EchocardiographyVolume 20 Number 2 Triposkiadis et al 185
patients with left ventricular hypertrophy: the losartanintervention for endpoint reduction in hypertension (LIFE)study. Hypertension 2002;39:739-43.
21. Gioffi G, Mureddu GF, Stefenelli C, de Simone G. Relation-ship between left ventricular geometry and left atrial size andfunction in patients with systemic hypertension. J Hypertens2004;22:1589-96.
22. Cuspidi C, Meani S, Fusi V, Valerio C, Catini E, Sala C, et al.Prevalence and correlates of left atrial enlargement in essentialhypertension: role of ventricular geometry and the metabolicsyndrome; the evaluation of target organ damage in hyperten-sion study. J Hypertens 2005;23:875-82.
23. Rossi A, Cicoira M, Florea VG, Golia G, Florea ND, Khan AA,et al. Chronic heart failure with preserved left ventricularejection fraction: diagnostic and prognostic value of left atrialsize. Int J Cardiol 2006;110:386-92.
24. Gottdiener JS, Kitzman DW, Aurigemma GP, Arnold AM,Manolio TA. Left atrial volume, geometry, and function insystolic and diastolic heart failure of persons � or �65 years ofage (the cardiovascular health study). Am J Cardiol 2006;97:83-9.
25. Lakatta EG, Levy D. Arterial and cardiac aging; major share-holders in cardiovascular disease enterprises, part II: the agingheart in health–links to heart disease. Circulation 2003;107:346-54.
26. Pritchett AM, Mahoney DW, Jacobsen SJ, Rodeheffer RJ,Karon BL, Redfield MM. Diastolic dysfunction and left atrialvolume: a population-based study. J Am Coll Cardiol 2005;45:87-92.
27. Jensen JL, Williams FE, Beilby BJ, Johnson BL, Miller LK,Ginter TL, et al. Feasibility of obtaining pulmonary venousflow velocity in cardiac patients using transthoracic pulsedwave Doppler technique. J Am Soc Echocardiogr 1997;10:60-6.
28. de Marchi SF, Bodenmuller M, Lai DL, Seiler C. Pulmonaryvenous flow velocity patterns in 404 individuals without car-diovascular disease. Heart 2001;85:23-9.
29. Stefanadis C, Dernellis J, Toutouzas P. A clinical appraisal ofleft atrial function. Eur Heart J 2001;22:22-36.
30. Triposkiadis F, Moyssakis I, Hadjinikolaou L, Makris T, ZiorisH, Hatzizaharias A, et al. Left atrial systolic function is de-pressed in idiopathic and preserved in ischemic dilated cardio-myopathy. Eur J Clin Invest 1999;29:905-12.
31. Moyssakis I, Papadopoulos DP, Kelepeshis G, Gialafos E,Votteas V, Triposkiadis F. Left atrial systolic reserve in idio-pathic vs ischemic-dilated cardiomyopathy. Eur J Clin Invest2005;35:355-61.
32. Ohtani K, Yutani C, Nagata S, Koretsune Y, Hori M, KamadaT. High prevalence of atrial fibrosis in patients with dilatedcardiomyopathy. J Am Coll Cardiol 1995;25:1162-9.
33. Benedict CR, Weiner DH, Johnstone DE, Bourassa MG,Ghali JK, Nicklas J, et al. Comparative neurohormonal re-sponses in patients with preserved and impaired left ventricularejection fraction: results of the studies of left ventricular dys-function (SOLVD) registry; the SOLVD investigators. J AmColl Cardiol 1993;22:146-53A.
34. Triposkiadis F, Trikas A, Pitsavos C, Papadopoulos P, ToutouzasP. Relation of exercise capacity in dilated cardiomyopathy to left
atrial size and systolic function. Am J Cardiol 1992;70:825-7.35. Benjamin EJ, D’Agostino RB, Belanger AJ, Wolf PA, Levy D.Left atrial size and the risk of stroke and death: the Framing-ham heart study. Circulation 1995;92:835-41.
36. Tsang TS, Barnes ME, Bailey KR, Leibson CL, MontgomerySC, Takemoto Y, et al. Left atrial volume: important riskmarker of incident atrial fibrillation in 1655 men and women.Mayo Clinic Proc 2001;76:467-75.
37. Møller JE, Hillis GS, Oh JK, Seward JB, Reeder GS, WrightRS, et al. Left atrial volume: a powerful predictor of survivalafter acute myocardial infarction. Circulation 2003;107:2207-12.
38. Beinart R, Boyko V, Schwammenthal E, Kuperstein R, Sagie A,Hod H, et al. Long-term prognostic significance of left atrialvolume in acute myocardial infarction. J Am Coll Cardiol 2004;44:327-34.
39. Sabharwal N, Cemin R, Rajan K, Hickman M, Lahiri A, SeniorR. Usefulness of left atrial volume as a predictor of mortality inpatients with ischemic cardiomyopathy. Am J Cardiol 2004;94:760-3.
40. Rossi A, Cicoira M, Zanolla L, Sandrini R, Golia G, Zardini P,et al. Determinants and prognostic value of left atrial volumein patients with dilated cardiomyopathy. J Am Coll Cardiol2002;40:14-25.
41. Hogg K, Swedberg K, McMurray J. Heart failure with pre-served left ventricular systolic function; epidemiology, clinicalcharacteristics, and prognosis. J Am Coll Cardiol 2004;43:317-27.
42. Juilliere Y, Barbier G, Feldmann L, Grentzinger A, Danchin N,Cherrier F. Additional predictive value of both left and rightventricular ejection fractions on long-term survival in idiopathicdilated cardiomyopathy. Eur Heart J 1997;18:276-80.
43. Werner GS, Schaefer C, Dirks R, Figulla HR, Kreuzer H.Prognostic value of Doppler echocardiographic assessment ofleft ventricular filling in idiopathic dilated cardiomyopathy.Am J Cardiol 1994;73:792-8.
44. Ommen RS, Nishimura RA. A clinical approach to the assess-ment of left ventricular diastolic function by Doppler echocar-diography: update 2003. Heart 2003;89:III18-23.
45. Ommen SR, Nishimura RA, Appleton CP, Miller FA, Oh JK,Redfield MM, et al. Clinical utility of Doppler echocardiogra-phy and tissue Doppler imaging in the estimation of leftventricular filling pressures: a comparative simultaneous Dop-pler-catheterization study. Circulation 2000;102:1788-94.
46. Tirrito SJ, Augustine DR, Kerut EK. How to measure leftatrial volume. Echocardiography 2004;21:569-71.
47. Khankirawatana B, Khankirawatana S, Porter T. How shouldleft atrial size be reported? Comparative assessment with use ofmultiple echocardiographic methods. Am Heart J 2004;147:369-74.
48. Jenkins C, Bricknell K, Marwick TH. Use of real-time three-dimensional echocardiography to measure left atrial volume:comparison with other echocardiographic techniques. J AmSoc Echocardiogr 2005;18:991-7.
49. Tsang TS, Gersh BJ, Appleton CP, Tajik AJ, Barnes ME,Bailey KR, et al. Left ventricular diastolic dysfunction as apredictor of the first diagnosed nonvalvular atrial fibrillation in840 elderly men and women. J Am Coll Cardiol 2002;40:
1636-44.




























