-
8/13/2019 Lengkap Banget Atopic Transient Wheezing
1/8
2002;109;362Pediatrics
Fernando D. MartinezDevelopment of Wheezing Disorders and Asthma
in Preschool Children
http://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.htmllocated
on the World Wide Web at:
The online version of this article, along with updated
information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005.
Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois,
60007. Copyright 2002 by the American Academypublished, and
trademarked by the American Academy of Pediatrics, 141 Northwest
Point
publication, it has been published continuously since 1948.
PEDIATRICS is owned,PEDIATRICS is the official journal of the
American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on February 19,
2014pediatrics.aappublications.orgDownloaded from at Indonesia:AAP
Sponsored on February 19,
2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.htmlhttp://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.htmlhttp://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.html
-
8/13/2019 Lengkap Banget Atopic Transient Wheezing
2/8
Development of Wheezing Disorders and Asthma in Preschool
Children
Fernando D. Martinez, MD
ABSTRACT. Recent longitudinal studies have shedlight on the
pathogenesis and progression of asthma. Thepatterns of expression
of childhood asthma that persistinto adult life have been explored.
Distinct asthma phe-notypes (transient wheezing, nonatopic
wheezing, andatopy-associated asthma) have been identified.
Definingwhich children are at risk for persistent asthma couldallow
for better management and, potentially, for re-duced morbidity and
mortality. Pediatrics 2002;109:362367;asthma expression,
phenotypes, wheezing, atopy.
ABBREVIATIONS. IgE, immunoglobulin E; FEV1, forced expira-tory
volume in 1 second; RSV, respiratory syncytial virus;
IFN-,interferon-; IL, interleukin.
Much about the natural history of asthmaremains unknown;
longitudinal studies,however, have shed some light on the
pathogenesis and progression of the disease. Asthmais a
heterogeneous condition with variable signs andsymptoms in patient
groups, as well as variabilitywithin each individual patient over
time.1 Certainpatterns of asthma expression observed
duringchildhood persist into adulthood.2,3 Although mildasthma
during childhood may resolve, it seems thatasthma is a progressive
condition in many children,especially those who have severe
disease.4 Early al-lergic sensitization is an important risk factor
forpersistent asthma,5 and the role of allergen exposureduring the
early years of life in the course of thedisease, as well as the
role of other factors, hasemerged as an important focus.
Longitudinal studiesof wheezing disorders from childhood to
adulthoodare necessary for understanding the true progressionand
the risk factors of what is understood to beasthma.
PATTERNS OF ASTHMA EXPRESSION DURINGCHILDHOOD INTO ADULTHOOD
In some young children with mild asthma, wheez-
ing resolves spontaneously; in others, especiallythose with
severe asthma, wheezing continues intoadulthood.6 Defining which
children are at risk forpersistent asthma could allow for better
manage-ment and, potentially, for reduced morbidity andmortality.
In 1964, a longitudinal study was initiated
in Melbourne, Australia, to follow childhood asthmainto
adulthood.2,3,7 Starting from a cohort of 30 000children, 401 were
enrolled at age 7, based on theirparents responses to a
questionnaire concerningtheir childs history of asthma, wheezing
episodes,and bronchitis. The children were classified into
4categories: those who never wheezed (controls,n 106); those with
fewer than 5 episodes associatedwith apparent respiratory infection
(mild wheezy
bronchitis, n 75); those with 5 or more episodesassociated with
apparent respiratory infection(wheezy bronchitis,n 107); and those
with wheez-ing not associated with respiratory infection
(asthma,
n 113). A fifth group of children with severeasthma (n 79) was
selected from the same cohort atage 10.2 Evaluationsincluding
physical examina-tions, patient questionnaires on symptoms and
ther-apy, laboratory measurements such as eosinophiland
immunoglobulin E (IgE) levels, pulmonary func-tion (with
spirometry, lung volumes, and histaminechallenge), and skin
reactivity testing have beenconducted every 7 years.2 At the
evaluation con-ducted when patients were 35 years old, the
partic-ipants were categorized as follows2: no recentasthma (not
having wheezed for 3 or more yearsprevious to the evaluation);
infrequent wheeze (hav-
ing wheezed in the previous 3 years but not in the 3months
before evaluation); frequent asthma (havingwheezed less than once
per week in the 3 previousmonths); or persistent asthma (having
wheezed atleast once weekly in the previous 3 months).
Symptom assessment at age 35 was comparedwith the categorization
established when partici-pants were 7 to 10 years of age (Table 1).
Resultsshowed that of the 65 patients who had mild wheezy
bronchitis at 7 years of age, 77% (n 50) had nosymptoms at age
35, whereas only 23% (n 15) hadfrequent or persistent asthma.7 Of
the 98 participantswith asthma at 7 years of age, 50% (n 49) had
no
recent asthma or infrequent asthma as adults,whereas 50% (n 49)
had frequent or persistentasthma. Importantly, 75% (n 50) of those
who hadsevere asthma (n 67) at age 10 had frequent orpersistent
asthma at age 35. According to these re-sults, many children do not
remit from their asthma,and the more severe their asthma, the less
likely theyare to remit. These data support the tracking conceptof
the disease: children with mild disease had remis-sion or continued
with mild disease in their adult-hood, whereas children with severe
asthma sufferedpersistent severe asthma when they reached
adult-hood.
Assessmentof the participants every 7 years over
From the University of Arizona, Tucson, Arizona.
Received for publication May 4, 2001; accepted Oct 22, 2001.
Reprint requests to (F.D.M.) Arizona Respiratory Center, Box
245030, 1501
N Campbell Ave, Room 2349, Tucson, AZ 85724. E-mail:
fernando@resp-
sci.arizona.edu
PEDIATRICS (ISSN 0031 4005). Copyright 2002 by the American
Acad-
emy of Pediatrics.
362 PEDIATRICS Vol. 109 No. 2 February 2002at Indonesia:AAP
Sponsored on February 19,
2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
8/13/2019 Lengkap Banget Atopic Transient Wheezing
3/8
age 28 showed that those with asthma and severeasthma at age 7
experienced abnormal pulmonaryfunction as adults,2 although in the
participants withasthma, the abnormalities were relatively minor
(Fig1). Participants who were classified at age 7 as hav-ing mild
wheezy bronchitis and wheezy bronchitishad no evidence of airway
obstruction at age 35.2 Thepatterns of wheezing and asthma
expressed early inlife generally persisted into adulthood.
Conversely,persistent airway obstruction in adulthood was
as-sociated with more troublesome asthma during
childhood.2,7These patterns presented in Fig 1 suggest that
no
significant additional loss of pulmonary function oc-curs after
the age of 7 to 10 years and up to the ageof 35, even in
individuals with severe disease. Thiswould imply that children are
either born with thedeficit of pulmonary function or that there is
a loss ofpulmonary function after birth, after which no addi-tional
loss occurs. The studies from the Tucson Chil-drens Respiratory
Study would argue that the latteris the case.
Children were categorized at age 6 based on thehistory of their
wheezing from before age 3. The
categories included the following: nonwheezers(children who had
never wheezed); transient wheezers(at least 1 lower respiratory
tract illness with wheez-
ing during the first 3 years of life but who had nowheezing at 6
years); late-onset wheezers (no lowerrespiratory tract illness with
wheezing during thefirst 3 years of life but who had wheezing at 6
years);and persistent wheezers (at least 1 lower respiratorytract
illness with wheezing during the first 3 years oflife and wheezing
at 6 years). Based on pulmonaryfunction measurements made before
age 1, non-wheezers and persistent wheezers had no
significantdifference in pulmonary function. At age 6,
however,persistent wheezers and nonwheezers had a signifi-
cant difference in pulmonary function (Table 2),which was still
measurable, using forced expiratoryvolume in 1 second (FEV1), at
age 11.
8 Therefore,significant loss of pulmonary function seems to
haveoccurred after age 1 but before age 6, and, conse-quently, the
deficits in pulmonary function in wheez-ing are not significantly
present early after birth, butseem to be acquired during the first
years of life.
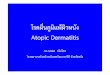
ASTHMA PHENOTYPES
Most epidemiologic studies have suggested thatthere are several
different asthma phenotypes, re-flecting a heterogeneous group of
conditions that
follow a common final pathway characterized byrecurrent airway
obstruction. Three of these pheno-types are transient early
wheezing (wheezing up toage 3 but not after), nonatopic wheezing of
the tod-dler and early school years, and
IgE-mediatedwheezing/asthma (Fig 2).1
Transient Early Wheezing
In most children, transient early wheezing charac-teristically
resolves by age 3. Generally, transientwheezing in infants is not
associated with a familyhistory of asthma or allergic
sensitization.9 The pri-mary risk factor for this phenotype seems
to be re-
duced pulmonary function.1,9
The lower level of pul-monary function seems to track along
individualgrowth curves, and it remains low at age 6.10 Ofinterest,
however, is that children younger than 3years of age with transient
early wheezing had noincreased prevalence of methacholine
hyperrespon-siveness or positive peak flow variability at age
11.1
These results suggest that mechanical pulmonarycharacteristics,
such as reduced airway resistanceor increased dynamic compliance,11
play a role intransient wheezing, rather than increased
airwaylability.1
Other risk factors for transient wheezing includeprematurity12
and exposure to siblings and other
Fig 1. FEV1as percentage of predicted values in different
groupsof subjects enrolled in the Melbourne Longitudinal Study
ofasthma. Subjects were classified according to their diagnosis
attime of enrollment: control;fmild wheezy bronchitis; wheezy
bronchitis; asthma; severe asthma. Assessmentof the participants
every 7 years showed that those with asthmaand severe asthma at age
7/10 showed diminished lung functionas adults, those with asthma
having relatively mild abnormalities.These abnormalities tracked
with age. Adapted from Oswald etal.2 Used with permission.
TABLE 1. Distribution of Asthma in 401 Subjects Aged 35
According to Whether They Had Bronchitis or Asthma as Children
At Age 7* No RecentAsthma
Asthma at Age 35* N(%) Total
Infrequent Frequent Persistent
Mild wheezy bronchitis 42 (65) 8 (12) 10 (15) 5 (8) 65Wheezy
bronchitis 54 (63) 10 (12) 9 (10) 13 (15) 86Asthma 29 (30) 20 (20)
18 (18) 31 (32) 98Severe asthma 7 (10) 10 (15) 8 (12) 42 (63)
67Total 132 48 45 91 401
* Values are numbers (percentages) of participants. Eighty-five
controls are excluded.Patients entered study at age 10.
Adapted from Oswald et al.7
SUPPLEMENT 363at Indonesia:AAP Sponsored on February 19,
2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
8/13/2019 Lengkap Banget Atopic Transient Wheezing
4/8
children at day care centers.13 Maternal smokingduring
pregnancy, as well as postnatal exposure totobacco smoke, increases
the risk for transient
wheezing in children younger than 3 years ofage.14,15
Nonatopic Wheezing
Most school-aged asthmatic children have a his-tory of airway
obstruction during the first 2 to 3years of life.16,17 The most
common cause of airwayobstruction in infancy is viral infection,
most fre-quently caused by the respiratory syncytial virus(RSV).18
Several studies have explored the relation-ship between RSV
respiratory tract infection andwheezing. The objective of a
recently reported lon-gitudinal study, the Tucson Childrens
Respiratory
Study, was to determine whether RSV lower respi-ratory tract
illness, by itself, and occurring during thefirst 3 years of life,
was a risk factor for subsequentpersistent wheezing.19
A total of 472 children with lower respiratory tractillness
underwent testing for the infecting organism.Of these, RSV was
documented in 207 (43.9%) chil-dren, parainfluenza in 68 (14.4%),
other agents (ad-enovirus, influenza,Chlamydia, cytomegalovirus,
rhi-novirus, bacteria, mixed infection) in 68 (14.4%), andno
infecting pathogen in 129 (27.3%). Analyses dem-onstrated that RSV
infection significantly increasedthe risk for wheezing during the
first 10 years of life;the risk decreased with age, however, and
was no
longer significant by 13 years of age (Fig 3).19 Fur-thermore,
RSV infection during the first 3 years of
life was not associated with increased risk for skintest
positivity or higher IgE levels later in life com-pared with other
causes of lower respiratory tractinfection (Table 3). No
relationship of RSV lowerrespiratory tract infection to allergic
sensitization,irrespective of family history of asthma, was
identi-fied.
The effect of RSV lower respiratory tract infectionon pulmonary
function was also assessed. Childrenwho had RSV infection before 3
years of age hadsignificantly lower FEV1, adjusted for length
andgender than children who had not had lower respi-ratory tract
illness. This difference remained inde-pendent of current wheezing
at 11 years of age (P .001). The children with a history of RSV
infectionwere also more likely to respond to bronchodilata-tion
than their counterparts with no such history(P .05; Table 4). These
findings may indicate thatthe children with lower levels of
pulmonary functionwere either born with reduced function, or had
aninteraction between the immune system and RSVinfection that
altered lung growth, or both.19
Although additional research is needed to definealterations in
airway function secondary to RSV re-spiratory tract infection,
findings from the TucsonChildrens Respiratory Study provide
important im-plications.19 First, although RSV infection is a risk
for
subsequent wheeze during childhood, RSV-associ-ated wheezing
resolves in most children by 13 yearsof age. Second, the
relationship between persistentwheezing up to 13 years of age after
RSV infectiondoes not seem to be associated with an increased
riskfor allergic sensitization.
Atopic Wheezing/Asthma
More than half of all cases of persistent asthmastart before age
3, and 80% begin before age 6.Among school-aged children with
persistent asthma,the onset of symptoms before age 3 is associated
with
increased severity of the disease and increased bron-chial
hyperresponsiveness. Patients with early-onsetasthma also have
significant deficits in pulmonaryfunction growth. Thus, the
decisive airway changesseem to begin early in life.5
Frequently, asthma that begins early in life is as-sociated with
atopy, the genetic predisposition forsensitization to allergens
(Fig 4).20 Early allergic sen-sitization seems to play an important
role in persis-tent asthma.
The correlation between allergic sensitization andrespiratory
symptoms of asthma was studied in 380Australian (Belmont, New South
Wales) school chil-dren enrolled between 8 to 10 years of age.21
The
Fig 2. Hypothetical yearly peak prevalence of wheezing
accord-ing to phenotype in childhood. Asthma phenotypes reflect a
het-erogenous group of conditions characterized by recurrent
airwayobstruction. Three of these phenotypes are shown. This
classifica-tion of wheezing phenotypes should not imply that the
groups areexclusive. Dashed lines suggest that wheezing can be
represented
by different curve shapes resulting from many different
factors,including overlap of groups. Adapted from Stein et al.1
TABLE 2. Maximal Expiratory Flow at Functional Residual Capacity
(VmaxFRC in mL/sec)During the First Year of Life and at 6 Years of
Age According to History of Wheezing
Nonwheezer Persistent Wheezer P
VmaxFRC* at 1 y 123.3 (110.0, 138.0) 104.6 (73.6, 144.5)
NSVmaxFRC* at 6 y 1262.1 (1217.4, 1308.1) 1069.7 (906.9, 1146.5)
.01
* mL/sec; mean (95% confidence interval).
364 SUPPLEMENTat Indonesia:AAP Sponsored on February 19,
2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
8/13/2019 Lengkap Banget Atopic Transient Wheezing
5/8
participants underwent skin prick testing to 13 aller-
gens at enrollment and 2 and 4 years later. Threegroups of
children emerged: those who were sensi-tized at the time they
entered the study, those who
became sensitized during the study, and those whonever became
sensitized during the study. The prev-alence of persistent
respiratory symptoms (wheeze,exercise wheeze, or night cough) was
the same inchildren who became sensitized during the studyand
children who did not become sensitized (11% to12%). The children
who were sensitized at the begin-ning of the study, however, had a
prevalence ofrespiratory symptoms that was significantly
greater(approximately 40%) than the other groups, and theywere at
significantly greater risk for the development
of asthma than the other groups.21These findings underscore the
importance of early
allergic sensitization in the development of persis-tent asthma.
Interestingly, specific factors have beenidentified that decrease
the risk for persistent disease(Table 5). In these cases, increased
exposure to otherchildren, pets, or farm animals in early life
mayprotect against the development of asthma in chil-dren.
In 412 Swedish children, exposure to pets duringthe first year
of life resulted in a lower incidence ofallergic rhinitis at 7 to 9
years of age and a decreasedfrequency of asthma at 12 to 13 years
of age.22 An
increased number of siblings also showed an inverserelationship
to subsequent development of allergic
rhinitis and asthma. Similarly, in a controlled study
of secondary school children in rural areas surround-ing Quebec
City, Canada, children who had beenraised on a farm exhibited
significantly less wheeze,airway hyperresponsiveness, and allergic
skin testpositivity during adolescence than did children with-out
exposure to a farming environment.23 The oddsratio among children
raised on a farm for havingcurrent wheeze was 0.70; for having
asthma, 0.59;and for atopy, 0.58. The number of siblings among
both groups did not affect the results. These findingshave been
confirmed in other studies; some investi-gators, however, question
whether heightened earlyexposure offers protection against airway
inflamma-tion or whether increased urban pollutants cause
symptoms in children not raised on a farm.24The possible
protective effects of increased early
exposure to other children were supported by astudy involving
1035 children followed since birth aspart of the Tucson Childrens
Respiratory Study.13
The risk for asthma (children given a diagnosis ofasthma by a
physician and who had an exacerbationof their asthma during the
previous year) was com-pared between children with and without
older sib-lings and between children who attended and didnot attend
day care before 6 months of age.
In children with older siblings in the home andchildren who
attended day care during the first 6
months of life, 12% developed asthma. In childrenwithout older
siblings in the home and in children
Fig 3. Adjusted odds ratios (95% confidence in-tervals) for
infrequent and frequent wheeze as-sociated with RSV lower
respiratory tract infec-tions before 3 years of age. RSV
infectionsignificantly increased the risk for wheezingduring the
first 10 years of life. The risk de-creased with age and was no
longer significantat 13 years of age. Results were adjusted
forconfounding variables including family historyof asthma,
positive skin test at 6 or 11 years ofage, gender, maternal
education, birth weight,and current maternal smoking. Adapted
fromStein et al.19 Used with permission.
TABLE 3. Skin Test Positivity and Serum IgE Concentrations at
Different Ages in Children With Lower Respiratory Tract
IllnessBefore 3 Years of Age
CausativeAgent
Positive Skin Test (%) Serum IgE Concentration (IU/L)
Age 6 Years Age 11 Years Age 9 Months Age 6 Years Age 11
Years
RSV 37.4 59.3 4.31 33.1 58.6Parainfluenza 40.7 52.9 3.25 26.0
78.5Other agents 39.2 56.5 4.29 30.3 69.4Negative tests 39.8 55.8
4.24 35.1 51.7None 39.7 58.9 4.25 39.5 64.8
Adapted from Stein et al.19
SUPPLEMENT 365at Indonesia:AAP Sponsored on February 19,
2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
8/13/2019 Lengkap Banget Atopic Transient Wheezing
6/8
who did not attend day care during the first 6months of life,
however, 21% developed asthma.Similarly, children with older
siblings and childrenwho attended day care during the first 6
months oflife were less likely to develop frequent wheezing(3
wheezing episodes during the previous year)when they were older.13
The adjusted relative risk
for frequent wheezing at 2 years of age among chil-dren with
greater exposure was 1.4, but by 6 yearsold, the adjusted relative
risk declined to 0.8, and atage 13 it declined even further to 0.3.
Therefore, earlyexposure to older siblings in the home and day
careattendance offers protective effects against frequentwheezing
and asthma later in childhood.13
A preliminary investigation suggested that the ef-fects of early
exposure to endotoxin in house-dust inearly life may protect
against the later developmentof allergic sensitization.25 A total
of 61 infants, aged9 to 24 months with at least 3 episodes of
physician-documented wheezing, were included in this study
from Denver. The investigators measured the con-centrations of
house-dust endotoxin and allergens inthe childrens homes. Allergic
skin tests were per-formed in all children, and flow cytometry was
usedto measure proportions of T-lymphocytes
producinginterferon-(IFN-), and interleukin (IL)-4, IL-5, andIL-13.
Children living in homes with significantlylower concentrations of
house-dust endotoxin testedpositive on allergic skin testing more
often than chil-dren living in homes with higher concentrations
ofhouse-dust endotoxin. The children living in homeswith a greater
concentration of house-dust endotoxinalso had increased proportions
of T-lymphocytesthat produced IFN-but not IL-4, IL-5, andIL-13.
It
was suggested that early exposure to house-dustendotoxin may
protect against allergic sensitizationvia augmentation of TH1-type
immunity.
ASTHMA AS A PROGRESSIVE DISEASE
As reviewed above, many longitudinal studies ofasthma have given
us important insights into itsnatural history.18,1215,2125 There
seem to be differ-ent forms of asthma, and one of these is a
progressivedisease that begins mainly during the first years
oflife. If interventions take place after the age of 6 to 7years,
it seems to be too late to alter the natural
course of this form of the disease, and from then on,only
symptoms can be controlled. Identifying thosechildren who are or
will be affected by this form ofasthma before 6 years of age may
allow us to treatthem by the critical time. The children with this
formof the disease seem to be a minority of the childrenwho have
asthma, and although they show symp-toms early in life and are
sensitized early in life, thereis no clear way to identify them at
present.
The Childhood Asthma Management Program ex-amined the
relationships between disease severityand duration in 1041 children
aged 5 to 12 years withmild-to-moderate chronic asthma, atopy, and
well-
preserved pulmonary function.4
Pulmonary func-tion, as determined by PC20FEV1, pre- and
postbron-chodilator percent predicted FEV1 and pre-
andpostbronchodilator FEV1/forced vital capacity, de-clined
significantly (P .001) with each years dura-tion of asthma; the
strongest association was demon-strated in comparing function
before bronchodilatoruse with that after bronchodilator use.4
Childrenwith a longer duration of asthma also had higherlevels of
symptoms (P .001) and greater use ofalbuterol (P .064) during a
prospective 28-dayscreening period. These findings are consistent
withother ongoing studies showing that persistentasthma is
associated with chronic airway inflamma-tion, reduced pulmonary
function, and increasedasthma symptomatology.
The recently published results of The ChildhoodAsthma Management
Program have shown that in-haled corticosteroids were effective in
significantlyreducing the subjective measures of asthma, such
assymptoms, in children during the 4 years of study,
but the course of asthma, as reflected in postbron-chodilator
FEV1, the primary outcome of the study,was not altered.26
Therefore, if the adverse effects ofpersistent asthma are to be
prevented, diagnosis andintervention would seem to be necessary
before theage of 5 to 6years.
Fig 4. Pathogenesis of persistent childhood asthma: a
hypothesis.In genetically predisposed children, exposure during
early life toallergens induces an immune-mediated response that
results inairway inflammation. In turn, chronic airway inflammation
pro-duces bronchial hyperresponsiveness and persistent wheeze.
TABLE 4. Mean Baseline FEV1 at 11 Years of Age (95% Con-fidence
Interval)
Causative Agent Baseline FEV1 AfterBronchodilator
RSV (n 110) 2.11 (2.052.15)* 2.26 (1.702.90)Parainfluenza (n 38)
2.16 (2.072.25) 2.29 (1.632.67)Other agents (n 32) 2.19 (2.092.24)
2.27 (1.692.60)Negative test (n 72) 2.14 (2.082.20) 2.25
(1.832.76)None (n 189) 2.22 (2.182.25) 2.31 (1.702.99)
*P .001 compared with subgroup having no illness.P .05 compared
with subgroup having no illness.
Adapted from Stein et al.19
TABLE 5. Factors Associated With the Onset of
PersistentAsthma
Increased Risk Decreased Risk
Early allergic sensitization Exposure to other childrenearly in
life
Sensitization to certainaeroallergens (perennial?)
Exposure to pets
Eosinophilia Exposure to farm animals
366 SUPPLEMENTat Indonesia:AAP Sponsored on February 19,
2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
8/13/2019 Lengkap Banget Atopic Transient Wheezing
7/8
-
8/13/2019 Lengkap Banget Atopic Transient Wheezing
8/8
2002;109;362PediatricsFernando D. Martinez
Development of Wheezing Disorders and Asthma in Preschool
Children
ServicesUpdated Information &
E1/362.full.htmlhttp://pediatrics.aappublications.org/content/109/Supplement_including
high resolution figures, can be found at:
References
E1/362.full.html#ref-list-1http://pediatrics.aappublications.org/content/109/Supplement_at:This
article cites 25 articles, 4 of which can be accessed free
Citations
E1/362.full.html#related-urlshttp://pediatrics.aappublications.org/content/109/Supplement_This
article has been cited by 2 HighWire-hosted articles:
Subspecialty Collections
bhttp://pediatrics.aappublications.org/cgi/collection/asthma_suAsthma
following collection(s):This article, along with others on
similar topics, appears in the
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables)
or in its entirety can be found online at:Information about
reproducing this article in parts (figures,
Reprintshttp://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Village,
Illinois, 60007. Copyright 2002 by the American Academy of
Pediatrics. All rightstrademarked by the American Academy of
Pediatrics, 141 Northwest Point Boulevard, Elk Grove
andpublication, it has been published continuously since 1948.
PEDIATRICS is owned, published,PEDIATRICS is the official journal
of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on February 19,
2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.htmlhttp://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.htmlhttp://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.htmlhttp://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.htmlhttp://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.html#ref-list-1http://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.html#ref-list-1http://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.html#ref-list-1http://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.html#ref-list-1http://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.html#related-urlshttp://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.html#related-urlshttp://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.html#related-urlshttp://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.html#related-urlshttp://pediatrics.aappublications.org/cgi/collection/asthma_subhttp://pediatrics.aappublications.org/cgi/collection/asthma_subhttp://pediatrics.aappublications.org/cgi/collection/asthma_subhttp://pediatrics.aappublications.org/cgi/collection/asthma_subhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/reprints.xhtmlhttp://pediatrics.aappublications.org/site/misc/reprints.xhtmlhttp://pediatrics.aappublications.org/site/misc/reprints.xhtmlhttp://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/site/misc/reprints.xhtmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/cgi/collection/asthma_subhttp://pediatrics.aappublications.org/cgi/collection/asthma_subhttp://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.html#related-urlshttp://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.html#related-urlshttp://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.html#ref-list-1http://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.html#ref-list-1http://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.htmlhttp://pediatrics.aappublications.org/content/109/Supplement_E1/362.full.html