Embed Size (px)
Citation preview

8/2/2019 Leuk Oarai Osis
http://slidepdf.com/reader/full/leuk-oarai-osis 1/13
REVIEWPract Neurol 2008; 8: 26–38
LeukoaraiosisMike O’Sullivan
M O’SullivanHumboldt Research Fellow,Neurologische Klinik, KlinikumGroßhadern, Marchioninstraße 15,81377 Munchen, Germany;
Leukoaraiosis describes diffuse white matter abnormalities on CT or MR brainscans, often seen in the normal elderly and in association with vascular riskfactors such as hypertension, or in the context of cognitive impairment. The
term was introduced to avoid confusing an imaging appearance with aspecific pathology. Neurologists often come across this appearance, but itssignificance is sometimes uncertain. The effects on cognitive function and gaitare insidious and can be difficult to detect at the bedside, but are neverthelessimportant. However, gradually it is becoming clearer how leukoaraiosis relatesto cerebrovascular disease, Alzheimer’s and other diseases, and how thisappearance should influence treatment decisions.
The term ‘‘leukoaraiosis’’ was introducedalmost exactly 20 years ago by
Vladimir Hachinski and his colleagues.1
A new term was needed because, withthe rapid rise of CT brain imaging, it wasbecoming clear that diffuse low densitychanges in cerebral white matter were oftenseen in the context of dementia and vascularrisk factors. Initially, this newly revealedimaging appearance was thought of as theradiological correlate of Binswanger’s disease,considered rare in the pre-imaging era (seeboxes opposite). However, it became apparentthat the relation between these imaged whitematter lesions and pathology was morecomplex. Leukoaraiosis was, therefore, pro-posed as a purely descriptive term to avoidmaking assumptions about the underlyingpathology, with the intention, in time, ‘‘tohave labels replaced by understanding’’.1 Theterm was derived from the Greek stem‘‘leuko-’’ meaning white and referring to thewhite matter, and the adjective ‘‘araios’’meaning rarefied.
Leukoaraiosis is defined as diffuse, con-
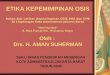
fluent white matter abnormality (low densityon CT, hyperintensity on T2-weighted or FLAIR
MRI; fig 1), often with irregular margins. As apurely radiological concept, the term could
equally be applied to the leukodystrophies, aswell as some metabolic and inflammatorydisorders. However, the need for a neutralterm that avoids assumptions about pathol-ogy is less pressing in patients likely onclinical grounds to have these conditions.Therefore I will focus on the vascular anddegenerative forms of leukoaraiosis (table 1),which are the commonest and generate themost controversy.
WHO GETS LEUKOARAIOSIS?Leukoaraiosis is seen in a range of differentclinical contexts and by different specialists—not just by neurologists, but also by strokephysicians and physicians who care for olderadults. In large unselected stroke series likethe Lausanne Stroke Registry about 7% of allpatients with ischaemic stroke2 had leukoar-aiosis, linked particularly with lacunar strokewhich accounts for 20% of all strokes.Leukoaraiosis is also seen in patients withdementia; in early unselected series, leukoar-
aiosis was found in 30–40% of cases, and inrecent clinical trials in vascular dementia as
Practical Neurology
10.1136/jnnp.2007.139428

8/2/2019 Leuk Oarai Osis
http://slidepdf.com/reader/full/leuk-oarai-osis 2/13
many as two thirds had leukoaraiosis.3
However, the link with dementia is not
confined to cerebrovascular disease and upto 30% of patients with ‘‘pure’’ Alzheimer’sdisease also have leukoaraosis;4 not surpris-ingly, therefore, leukoaraosis is seen inmemory and ‘‘early dementia’’ clinics.
In addition, leukoaraiosis may be seen in thecontext of normal ageing. Non-specific whitematter lesions become increasingly commonwith age, although frank leukoaraiosis, asopposed to scattered focal lesions, is seen lesscommonly. Early confluent, or confluent
lesions, corresponding to leukoaraiosis are seenin just over 10% of asymptomatic people aged
Binswanger’s disease: a potted history
In 1894, in a paper on the differential diagnosis of general paresis of the insane, OttoBinswanger linked marked atrophy of the cerebral white matter and arteriosclerosis to asyndrome of progressive decline of mental functions with depression and personality change,diminished power in the legs and tremor.i Diffuse white matter injury distinct from ischaemicinfarcts had already been described by Durand-Fardel under the heading,atrophie interstitielle du cerveau , but Binswanger was probably the first to draw a causal linkbetween such diffuse abnormalities and a progressive clinical syndrome. However, he did notprovide microscopic descriptions and this lack of detail has led to perennial uncertainty overexactly what pathological entity he was describing. The autopsy description just comments ongranular deposits on the dura mater at the skull base, minimal intracranial atherosclerosis,enlargement of the lateral ventricles and multiple ependymal thickenings. In 1962, whilereviewing the original descriptions and noting that the patient had a history of syphilis,Olszewski suggested that the changes in the dura mater and ependyma made neurosyphilis amore likely diagnosis.ii
For decades, Binswanger’s disease was recognised as an entity but thought to be rare. This
perception changed with the advent of CT and initially leukoaraiosis on CT was assumed toreflect Binswanger’s disease; a critique of this view was one of the pillars of Hachinski’soriginal paper introducing the term leukoaraiosis.
In more recent times, use of the eponymous term has declined while inconsistency hasgrown. One prevalent myth is that Binswanger’s disease can be diagnosed definitively atautopsy. In fact, the entity is not well-defined at pathological, clinical or radiological levels.Even if the pathology had been well defined there is evidence that the pathology may havechanged with time and the full-blown syndrome of dementia, pseudobulbar palsy and gaitdisturbance is now rare, perhaps reflecting advances in the treatment of vascular risk factors.The lack of precise definition seriously undermines the value of the concept of Binswanger’sdisease; one can have sympathy with the view that it is ‘‘neither Binswanger’s, nor adisease’’.iii
N i. Blass JP, Hoyer S, Nitsch R. A translation of Otto Binswanger’s article, ‘The delineationof the generalized progressive paralyses’Arch Neurol 1991;48 :961–72.
N ii. Olszewski J Subcortical arteriosclerotic encephalopathy.World Neurol 1965;3:359–73.N iii. Hachinski V. Binswanger’s disease: neither Binswanger’s nor a disease.J Neurol Sci
1991;103 :1.
Otto Binswanger (1852–1929) was aSwiss psychiatrist and neurologist whocame from a famous family of physicians. After receiving his medicaldegree in 1877, Binswanger spent thenext few years as assistant to TheodorMeynert in Vienna and Karl FriedrichOtto Westphal at the Charite Hospital inBerlin. From 1882 until 1919 he was aprofessor and director of psychology atthe University of Jena. One of his morefamous patients was Germanphilosopher Friedrich Nietzsche.
Figure 1An MR FLAIR (fluid attenuated
inversion recovery) image showingdiffuse leukoaraiosis and coexistentlacunes, which appear as cerebrospinalfluid intensity ‘‘holes’’ (arrows).
2O’Sullivan
www.practical-neurology.com

8/2/2019 Leuk Oarai Osis
http://slidepdf.com/reader/full/leuk-oarai-osis 3/13
50–75 years and the prevalence increases withage.
PATHOLOGY White matterIn regions of leukoaraiosis the major patho-logical findings are myelin pallor, enlarge-ment of perivascular spaces, gliosis andaxonal loss (fig 2).5, 6 Originally it wassuggested that selective demyelination might
occur as a result of ‘‘incomplete’’ ischaemia,but a single electron microscopy studyshowed that pallor was largely due to lossof nerve fibres in their entirety.7 A very similarpathology picture is observed in regions of true leukoaraiosis in asymptomatic olderadults, although the pathology underlyingscattered focal hyperintensities is much more
diverse. Fazekas et al demonstrated thatpathological heterogeneity diminishes as thelesion severity increases from small punctatehyperintensities to early confluent and thenconfluent lesions, which almost always havean ischaemic appearance with myelin loss,gliosis and microinfarction.8 In contrast,periventricular ‘‘caps’’ and a smooth haloaround the lateral ventricles (or ‘‘band’’) havea non-ischaemic appearance with subepen-dymal gliosis and discontinuity of theependymal lining.
Although these are by far the commonestsubstrates of leukoaraiosis, it needs to beremembered that other quite different pro-cesses can mimic this imaging appearance.For example, disseminated white mattermetastases, lymphoma and obstructivehydrocephalus have appeared as unexpectedcauses in postmortem series.9, 10
Blood vessel abnormalities
The white matter of the cerebral hemispheres islargely supplied by long, narrow penetrating
TABLE 1 Vascular causes of leukoaraiosis in older adults
Diagnosticgroup
Common clinicalassociations Diagnosis
Main pathologicalabnormality of smallvessels
Additional radiolo-gical features
Ischaemicleukoaraiosis
Lacunar stroke/transientischaemic attack (TIA)
Combination of previousclinical lacunarstroke/TIA
Arteriosclerosis (‘‘simple’’small vessel disease)Lipohyalinosis (‘‘complex’’small vessel disease)
Lacunar infarcts
Established risk factors:age and hypertensionEmerging risk factors:homocysteine
Sporadiccerebral amyloidangiopathy
Lobar haemorrhage Boston criteria (in brief): Amyloid deposits inproximal portions of penetrating arteries/arterioles (consistingmostly of Ab 1–40 )
Cortical/juxtacorticalmicrohaemorrhage(gradient echo MRI;see fig 5)
Transient neurologicalsymptoms due to petechialhaemorrhage triggeringfocal seizures have beendescribed
. 55 yearsmultiple cortical or juxtacortical bleedsno other cause of haemorrhage
CADASIL Lacunar stroke/TIAMigraine, past or presentdepressive symptoms
Notch3 genetic testingSkin biopsy Granular osmiophilicmaterial (GOM) and lossof smooth muscle cellsin the media of smallarteries
Anterior temporalpole hyperintensityon T2 MRILacunae andmicrohaemorrhageare also establishedfeatures
Clinical and radiological features which can help distinguish between types are listed, but common features—for example,progressive cognitive impairment, gait difficulties—are not included in the table. CADASIL is included because this can presentwith a first stroke or TIA even in the seventh or eighth decades.
In regions of leukoaraiosis the major pathological findings are myelin pallor, enlargement of perivascular spaces, gliosis and axonal loss
Practical Neurology
10.1136/jnnp.2007.139428

8/2/2019 Leuk Oarai Osis
http://slidepdf.com/reader/full/leuk-oarai-osis 4/13
arteries and arterioles that arise from branchesof the major cerebral arteries on the pialsurface of the brain. In regions of leukoaraiosisalterations in the structure of these vessels arean invariable feature. In the classical earlyseries changes in the vessels seemed to span a
hierarchy of severity from: hyaline thickeningand arteriosclerosis (which some refer to assimple small vessel disease) (fig 2) to ‘‘lipohya-linosis’’—a term which refers to a moredisorganised vessel wall with foamy macro-phages (complex small vessel disease), tofibrinoid necrosis.11 There are few more recentpathology data, but these suggest that thevascular pathology may have changed, withfibrinoid necrosis a much rarer finding thanpreviously, possibly reflecting better treatmentof hypertension.12
In asymptomatic older adults, blood vesselchanges are still a constant feature, but rarelyprogress beyond arteriosclerosis with con-centric hyaline thickening. In the mostcomprehensive pathology survey of the brainsof asymptomatic older adults9 parenchymalchanges were invariably linked with a reduc-tion in the ratio of arterial lumen to externaldiameter.
Alzheimer’s disease and cerebralamyloid angiopathyGiven its association with Alzheimer’s diseaseand predilection for small arteries, cerebralamyloid angiopathy might seem the mostobvious cause of leukoaraiosis in Alzheimer’sdisease. However, the early pathology studiesof Brun and Englund showed that leukoaraiosiswas associated with non-amyloid ‘‘fibrohya-line’’ thickening of arterial walls, as it is inageing and cerebrovascular disease.13 Thisinitial study also found no correlation betweenwhite matter pathology and degenerativepathology in the overlying neocortex, suggest-ing that leukoaraiosis is not merely secondaryto the degenerative process and dying back of axons through Wallerian degeneration.Furthermore, the extent of white matterpathology in Alzheimer’s disease correlateswith non-amyloid arteriosclerosis, not withthe severity of amyloid angiopathy, even whenboth forms of microvascular pathology arepresent.14 In summary, in Alzheimer’s disease,
leukoaraiosis co-localises with, and correlateswith the severity of non-amyloid arteriosclero-
sis. However, this does not necessarily rule outa role for b-amyloid in the pathogenesis of these changes, as will be discussed later.
Leukoaraiosis is also increasingly recognisedas a feature of sporadic cerebral amyloidangiopathy, without Alzheimer’s disease.15
Amyloid deposits are found in more proximalportions of the small penetrating arteries thanarteriosclerotic changes and it is not knownwhether these deposits alone, without down-
stream arteriosclerosis, are sufficient to causeleukoaraiosis. Notably, leukoaraiosis is found insome of the genetic amyloid angiopathies (forexample, familial British dementia) suggestingthat amyloid angiopathy alone is sufficient tocause this imaging appearance.
Leukoaraiosis and small vesseldiseaseThe pathological studies suggest that leu-koaraiosis is one manifestation of cerebral
small vessel disease. This is supported by
Figure 2Pathology of leukoaraiosis. Two smallvessels (arrows) are shown withconcentric hyaline thickening, loss of smooth muscle cells and with luminalnarrowing. The perivascular space iswidened, and the surrounding whitematter appears gliotic. (Haematoxylinand eosin. Courtesy of Dr AlistairLammie, Cardiff, UK.)
Figure 3The cognitive profile of ischaemicleukoaraiosis. Memory tests: WechslerMemory Scale logical memory (WMS)paired associate learning (PAL).Executive tests: Digit Symbol (DSym),letter fluency (FAS), Trail Making part (Trail), total errors (TE) and percentageperseverative errors (PE) on theWisconsin Card Sorting Test.(Reproduced with permission from the
BMJ Publishing Group.)
2O’Sullivan
www.practical-neurology.com

8/2/2019 Leuk Oarai Osis
http://slidepdf.com/reader/full/leuk-oarai-osis 5/13
strong pathological and clinical associationswith the other major manifestation of smallvessel disease—lacunar stroke.2 However,although leukoaraiosis and lacunar infarctsare often found together, in individualpatients one type of imaging appearancemay predominate, leading to the notion of subtypes of diffuse small vessel disease;either what has been labelled as ischaemicleukoaraiosis (defined by the combination of leukoaraiosis with a history of a clinicallacunar syndrome), or isolated lacunar infarc-tion (in which a similar clinical presentation isaccompanied by multiple lacunar lesions but noleukoaraiosis on imaging). Essentially this is themodern day imaging analogue of the distinc-
tion between diffuse white matter pathologyand a state of multiple discrete lacunar infarcts,described by Pierre Marie in 1901 andchristened etat lacunaire . These two imagingtypes have recently been shown to differ intheir risk factor profile; age and hypertension
are most strongly associated with ischaemicleukoaraiosis while hypercholesterolaemia, dia-betes mellitus and myocardial infarction aremore associated with isolated lacunar infarc-tion.16 These findings suggest some differencesin pathogenesis, with leukoaraiosis, perhapsreflecting a non-atheromatous pathology of smaller calibre vessels than those implicated inlacunar infarcts. A better appreciation of distinct subtypes may explain conflictingresults about the association of certain novelrisk factors with stroke; for example, althoughhomocysteine is a risk factor for both types of manifestation, it has a much stronger associa-tion with ischaemic leukoaraiosis than withisolated lacunar infarction.17
ASSOCIATED CLINICALFEATURESMany patients with leukoaraiosis have ahistory of, or develop, lacunar stroke. Butare there clinical features that can be linkedspecifically with leukoaraiosis? The evidence ismost convincing for associations with cogni-tive impairment, gait disturbance and falls.
Cognitive functionFor some time leukoaraiosis was consideredby many to be a benign imaging appearanceof no great consequence. Early cognitivestudies gave conflicting results, at least inpart because of inconsistency in the neuro-psychological tests that were applied. Forexample, executive deficits were only patchilyassessed in the early studies. However, it isnow clear that leukoaraiosis is associatedwith deficits of information processing speedand executive function—by which we adapt tocomplex situations where more than onecognitive process is at play18, 19 (fig 3).
The presence of leukoaraiosis also modifiesthe cognitive profile of Alzheimer’s disease. Inmixed samples of patients (including criteria-defined Alzheimer’s disease, vascular demen-tia and mixed cases) leukoaraiosis is linked to
performance on tests of executive functionand processing speed across disease groups.
TABLE 2 Prognosis
Association Study Magnitude of risk, details
Recurrent stroke NASCET 36% of patients with leukoaraiosis andcarotid stenosis had a stroke over a 6-year follow-up period compared with24% with carotid stenosis alone.Recurrent strokes were more oftenlacunar
Streifler et al ,2002
Vascular death Inzitariet al ,1997
8-year follow-up study of patients withand without leukoaraiosis admitted to ageriatric unit. Threefold higher risk of vascular death in leukoaraiosis group
Warfarin-relatedintracranialhaemorrhage
SPIRIT Leukoaraiosis increases the risk of bothdeep and lobar intracerebralhaemorrhages
Smith et al ,2000
Falls resulting in
fracture
Brileyet al ,
2000
Cox hazard ratio of 6.8. The association
is attenuated after adjusting for gait,suggesting that it is mediated by gaitdisturbance
Pneumonia anddeath frompneumonia
Brileyet al ,2000
The cause of this association isunknown, although conceivably effectson bulbar function or central control of breathing could play a role
Haemorrhagefollowingthrombolysis foracute stroke
CASES Leukoaraiosis carries a relative risk of 2.7for symptomatic intracerebralhaemorrhage. In patients withleukoaraiosis and/or multiple lacunarinfarcts the risk climbs to approximately10%
Palumboet al , 2007
Leukoaraiosis is linked to performance on tests of executive function and processing speeds across disease groups
Practical Neurology
10.1136/jnnp.2007.139428

8/2/2019 Leuk Oarai Osis
http://slidepdf.com/reader/full/leuk-oarai-osis 6/13
Walking and fallingAs many as 80% of patients with leukoar-aiosis have some degree of gait disorder.20
This association is independent of age,gender, previous stroke and hypertension.21
Furthermore, deterioration of gait is asso-
ciated with progression of leukoaraiosis.22 Themechanisms underlying this gait disturbanceremain unclear, although a correlation withfrontal lobe atrophy,23 as well as with thewhite matter lesions, could imply an inter-ruption of circuits involving the medial frontallobe that are important for gait control.23, 24
What is clear is that gait disturbance isimportant. A number of studies support thelink between gait disturbance and falls,22, 25
and leukoaraiosis is associated with a majorincrease in the risk of serious falls withfractures and hospitalisation25 (table 2).Therefore recognition of gait disturbance hasimplications for preventing falls and harmthrough falls, in part through initiatingphysiotherapy which has been shown toimprove gait.26 A small pilot study withamantadine showed a trend for an improve-ment in gait steadiness, but there was noclear advantage over placebo,27 so pharmaco-logical options remain limited but relativelyunexplored.
Other featuresOther features include bladder instability28
and mood disturbance; interestingly earlymood disturbance is a cardinal feature of one of the genetic causes of leukoaraiosis,CADASIL. The recent LADIS study has empha-sised the link between leukoaraiosis and bothdepression and disability in the elderly, and‘‘hidden’’ functional impairment in the non-disabled.29 Some of the classical features of
the early descriptions of ‘‘Binswanger’s dis-ease’’, such as pseudobulbar palsy, are rarelyseen now—perhaps because better treatmentof hypertension has modified the severity of the vascular pathology.12
CLINICAL ASSESSMENT ANDINVESTIGATIONAssessment and investigation is guided to alarge extent by the clinical context in whichleukoaraiosis is found:
N Stroke and transient ischaemic attack (TIA) .The approach to clinical evaluation and
investigation of acute stroke/TIA should beno different in patients found to haveleukoaraiosis. The clinical relevance of emerging risk factors, such as serumhomocysteine which is closely linked tothis appearance, remains to be established.Carotid Doppler studies should be per-formed in recently symptomatic patients inthis as in other subtypes of stroke, becausepatients with leukoaraiosis still benefitfrom endarterectomy if they have severecarotid stenosis.30
N Cognitive symptoms . In the initial assess-
ment of patients presenting with cogni-tive symptoms, and in cognitive screeningfollowing stroke, an appreciation of thecognitive profile and the limitations of the screening tools is important. Manystandard screening tools such as theMini-Mental State Examination (MMSE)are insensitive to executive deficits andare of limited value in these patients.Detection of executive deficits can bemarkedly improved by adding a fewadditional brief tests such as DigitSymbol , let te r f luency, and Trai lMaking.31 An extended screening instru-ment like the Addenbrooke’s cognitiveexamination, which includes letter flu-ency, is also likely to perform much betterthan the MMSE alone.32 Clock-drawingtasks can be helpful in some patients(fig 4), although they are less sensitivethan fluency or Trail Making tasks.Neuropsychological assessment can bevery useful and should be carried out inyounger patients, those with prominentcognitive difficulties and those who
present with cognitive symptoms in theabsence of previous stroke, where the
Figure 4An example of bedside cognitive testingin a patient with ischaemicleukoaraiosis. This patient had a Mini-Mental State Examination of 29/30, butthe addition of a clock-drawing taskrevealed a cognitive deficit. Top:Patient’s attempt to draw a clockfollowing the instruction, ‘‘Draw a clockthat shows the time as a quarter totwo. Draw the hands and numbers onthe face so that a child could readthem.’’ The drawing shows poorstrategy, sectoring, perseveration of thedigit 4 and an inability to complete thetask without help. Bottom: The patientwas able to copy a clock face withoutdifficulty, showing that the problemwas not because of constructional,perceptual or motor deficits.
3O’Sullivan
www.practical-neurology.com

8/2/2019 Leuk Oarai Osis
http://slidepdf.com/reader/full/leuk-oarai-osis 7/13
diagnostic possibilities are wider. Inparticular, physicians should be alert topatterns that do not fit well with theusual profile. For example, early loss of memory for day-to-day events (autobio-graphical memory), difficulties with spa-tial navigation and a prominent episodicmemory deficit on neuropsychologicaltesting should prompt consideration of Alzheimer’s disease even if leukoaraiosisis the predominant imaging finding.Rapid progression of cognitive and gaitdifficulties, over weeks to a few months,should also prompt consideration of other causes such as normal pressurehydrocephalus, malignancy or inflamma-tory brain disorders.
N Walking difficulties . In patients withprominent gait difficulties and leukoar-
aiosis the main aim of assessment is todetermine whether these features are
causally linked or merely coincidental.This partly depends on characterisation of the gait disturbance and careful exclusionof features that suggest parkinsonism oranother diagnosis.24 Walking difficultiescan be the main presenting feature,particularly when exacerbated by inter-current illness, and may be a commonmanifestation of leukoaraiosis in patientswho present ‘‘off legs’’ to acute medicalservices. Most leukoaraiosis patients withgait difficulties will have coexistentcognitive problems, which should besought.
N Incidental . The key question in thissetting is the extent to which leukoar-aiosis is disproportionate to age and riskfactor profile. It is difficult to approachthis question objectively, partly because
of the difficulties in grading leukoaraiosisseverity (see below). In older people,investigation of vascular risk will oftenbe adequate, but in younger people amuch wider differential diagnosis needsto be contemplated and investigations formetabolic and inflammatory causes con-sidered.
IMAGINGWhen the term leukoaraiosis was introduced,
only CT imaging was widely available. Similarappearances are conspicuous, and more floridon T2-weighted MRI, particularly on FLAIRimages, and these also distinguish leukoar-aiosis from lacunar infarcts, which appear asCSF intensity ‘‘holes’’ (fig 1).
Leukoaraiosis severity has traditionally beengraded by visual rating scales. Simple scales likethat of vanSwieten divide the appearances intoonly two grades of severity. Progressively morecomplex scales attempt to provide morecomprehensive quantitation and localisationof lesions. For example, the Fazekas scalediscriminates ‘‘punctate’’, ‘‘early confluent’’and ‘‘confluent’’ white matter lesions, whilethe Scheltens scale adopts a 0–6 scale inmultiple anatomical regions. Common pro-blems include comparability of CT and MRIratings (although a ‘‘unified’’ CT/MRI scale hasbeen proposed33 ), observer variability whichincreases with scale complexity, and ceilingeffects compared with quantitative measure-ments. However, even fully quantitative volu-
metric measurements of leukoaraiosis correlateweakly with cognitive and physical function,
Figure 5MR images from a 71-year-old manwith probable cerebral amyloidangiopathy. The FLAIR image showsleukoaraiosis (top). Multiple juxtacortical microhaemorrhages arevisible only with gradient echo MRI(bottom and arrow heads). (Reproducedwith permission from MassachusettsMedical Society from Greenberg SM,N Engl J Med 2006;354 :1452.)
Practical Neurology
10.1136/jnnp.2007.139428

8/2/2019 Leuk Oarai Osis
http://slidepdf.com/reader/full/leuk-oarai-osis 8/13
suggesting that T2-weighted MRI provides onlya rough impression of the severity of theunderlying pathology. In general, rating of leukoaraiosis severity has yet to find a clearplace in the clinical evaluation of thesepatients.
Newer MRI sequences can provide usefuladditional information. Diffusion-weightedimaging, for example, allows the distinction of new lacunar infarcts from background leukoar-aiosis. In patients who present with intracer-ebral haemorrhage, especially lobarhaemorrhage, gradient echo (T2*-weighted)images should be performed to look forevidence of previous haemorrhages or micro-bleeds (fig 5). The presence of multiple corticalor juxtacortical haemorrhages in patients over
55 years accurately predicts amyloid angio-pathy neuropathologically,34 which may be the
main substrate of leukoaraiosis or be foundalongside the small vessel arterioscleroticchanges. Microbleeds may be important inother groups and have prognostic implicationsin predicting haemorrhage risk, although a rolein guiding treatment decisions is yet to be fully
worked out (see below).In terms of quantifying white matter
damage, several techniques currently usedin research are proving superior to T2-weighted imaging and are likely to enter theclinical arena in the near future. Diffusiontensor MRI provides a much better index of white matter damage, and simple whole-brain measurements, such as diffusion histo-grams, can help track disease progression.35
Diffusion tensor MRI also demonstrates
the variability in the extent of whitematter disruption both within lesions and in
Figure 6Diffusion tensor imaging inleukoaraiosis. Right: colour-codedmean diffusivity maps. Hot colours(yellow to red to black) indicateincreasing mean diffusivity (waterdiffusion averaged in all directions,which increases as tissue is damaged,removing the myelin and axonalmembranes that restrict diffusion). Thevariability of diffusion within areas of leukoaraiosis is evident. Whole-brainhistograms of mean diffusivity providea much better index of disease severityand progression than the degree of leukoaraiosis, seen on MR on the left.(Images courtesy of Bioimaging Inc,Lyon, France.)
3O’Sullivan
www.practical-neurology.com

8/2/2019 Leuk Oarai Osis
http://slidepdf.com/reader/full/leuk-oarai-osis 9/13
normal-appearing white matter (fig 6).Measurement of brain atrophy from volu-metric T1-weighted images is also potentiallyvaluable in these patients, as it is in patientswith cortical dementias.
MECHANISMS OFLEUKOARAIOSISThe precise mechanisms linking the pathologyof the vessel walls with tissue injury havebeen the source of considerable controversy.The pathology changes in white matter havebeen most often interpreted as ‘‘incompleteinfarction’’—tissue injury consistent withischaemia not severe enough to producefrank infarction—but this remains controver-sial. Attention has tended to focus on
ischaemic mechanisms, but proving causalityhas been difficult.
Ischaemia?Reduced white matter cerebral blood flow inthe context of leukoaraiosis has been demon-strated in a range of studies and with a widevariety of techniques. The main difficulty isthe distinction between true hypoperfusionand the secondary reduction in cerebral bloodflow (CBF) that results from reduced function(through intact vasoneuronal coupling); inother words, it is difficult to know whetherreduced blood flow is a cause or consequenceof tissue damage. One observation that hintsat a causal role is that CBF, measured by MRperfusion imaging, is also reduced in whitematter that appears normal on T2-weightedscans.36 However, the situation is morecomplex than it appears at first sight fortwo reasons. First, newer structural imagingtechniques have shown that areas thatappear normal to the naked eye on T2-
weighted scans often harbour importantalterations in white matter integrity.37
Second, even if white matter is entirely intactstructurally, this does not necessarily meanthat it is functioning normally, so thepossibility of a secondary reduction in CBF,though smaller, still remains.
Blood-brain barrier dysfunction?The leading non-ischaemic theory is thatblood-brain barrier disruption leads to white
matter damage, presumably through toxiceffects of serum proteins.38 In patients with
leukoaraiosis, extravasation of proteins thatare usually confined to the plasma, such asIgG, complement and fibrinogen has beenidentified in white matter, in parallel with thepattern of leukoaraiosis.39 Also, there is araised CSF:serum albumin ratio in patients
with ‘‘vascular dementia’’ which correlateswith the degree of leukoaraiosis, suggestingthat the damaged white matter may be thesite of blood-brain barrier leakage.40 Morerecently, careful MRI studies of tissue con-trast uptake have demonstrated reducedblood-brain barrier integrity in vivo and thatthis relates to the severity of visible whitematter lesions.41
However, the development of new regionsof leukoaraiosis in areas of abnormal perfu-sion or altered blood-brain permeability hasnot been shown in longitudinal studies. Thecore problem is that both mechanisms mayoccur in parallel, and without the ability toexperimentally manipulate one or other, it willbe difficult to disentangle their effects, ordemonstrate causality.
The endothelium?Ischaemic and blood-brain barrier theories arenot necessarily mutually exclusive. Emergingevidence of endothelial dysfunction in leu-koaraiosis provides a framework to unifythese theories; alterations in blood flow andhaemodynamics, and blood-brain barrierfunction, may both be part of a broaderfailure of endothelial function.42 Studies of circulating endothelial markers are beginningto hint at a specific pattern of endothelialfunction that is associated with leukoaraiosis.A pro-coagulant pattern has been found inischaemic leukoaraiosis, which contrasts withthe pattern linked with lacunar infarction.
Leukoaraiosis and b amyloid?The association with a non-amyloid angio-pathy at the pathological level might be seenas evidence that leukoaraiosis is simplycoincidental in Alzheimer’s disease. However,recent evidence suggests a far more complexinteraction. In Alzheimer’s disease, and inpatients with mild cognitive impairment,some of whom will have prodromalAlzheimer’s, white matter changes correlate
with serum levels of the Ab1-40 peptide,which is the predominant peptide found in
Practical Neurology
10.1136/jnnp.2007.139428

8/2/2019 Leuk Oarai Osis
http://slidepdf.com/reader/full/leuk-oarai-osis 10/13
vessel deposits in cerebral amyloid angio-pathy.43 But intriguingly, plasma Ab alsocorrelates with the severity of white matterlesions in the population-based Rotterdamstudy.44 Given that cerebral amyloid angio-pathy is a rare cause of leukoaraiosis at the
population level, this suggests that Ab has animpact on white matter damage even inpatients with arteriosclerotic small vesseldisease and no pathological evidence of cerebral amyloid angiopathy. The underlyingmechanisms of this association are not yetclear. Conversely, pathological studies inAlzheimer’s disease suggest that arterio-sclerotic small vessel disease can drive moreextensive amyloid deposition and neurofibril-lary tangle formation,45 which is consistentwith epidemiological evidence that vascularrisk factors are important, and suggests thatthe interaction may work in both directions.
PROGNOSIS AND TREATMENTIn several prospective studies, leukoaraiosishas been associated with an increased risk of ischaemic stroke, cerebral haemorrhage,vascular death and all-cause mortality.27
Increased mortality occurs not just throughstroke and vascular death but also via anincreased risk of pneumonia and falls (table 2).
Stroke and TIAIn acute stroke or TIA, there is no evidence tosuggest that a different approach to treat-ment should be taken in the presence of leukoaraiosis. Very recently, the implicationsof finding leukoaraiosis in patients eligible forthrombolysis have been evaluated in theCanadian Alteplase for Stroke EffectivenessStudy (CASES). Although the risk of rt-PArelated haemorrhage was higher the chances
of a good outcome were not reduced.46
Patients with leukoaraiosis also benefit fromcarotid endarterectomy, despite higher perio-perative risks.30 So in general, based oncurrent evidence, the same approach shouldbe taken except, perhaps, if anticoagulantsare to be used (see below).
Leukoaraiosis and anticoagulantsThe association of leukoaraiosis with treat-ment-associated haemorrhage is especially
important as it may be partly preventable bycarefully weighed treatment decisions. In the
SPIRIT trial of oral anticoagulation followingnon-disabling cerebral ischaemia, patients insinus rhythm received either anticoagulationwith a target INR of 3–4.5, or aspirin. The trialwas stopped early because of an unacceptableincrease in cerebral haemorrhage, and leu-koaraiosis was found to be a strong inde-pendent risk factor for this complication, withan odds ratio of 9.2.47 Furthermore, in patientswith a previous ischaemic stroke, leukoar-aiosis is a strong risk factor for subsequent
symptomatic haemorrhage,48 either of lobaror deep subcortical type.
It is not yet clear whether the risk of bleeding can be predicted by the pattern orseverity of leukoaraiosis, or any associatedimaging features. Severity is probably impor-tant. In SPIRIT, patients with ‘‘severe’’leukoaraiosis had a haemorrhage risk 2.5times that of ‘‘moderate’’ leukoaraiosis and adose-response relation was also seen in thecase-control study of intracerebral haemor-
rhage. However, all of the studies of bleedingrisk are based on collapsing leukoaraiosisseverity into only 1 or 2 grades (correspond-ing to the van Swieten scale) on CT assess-ment. The potential role of more detailedseverity rating, based on MRI, or of additionalMRI techniques such as the detection of microbleeds is unclear. There is at least onefurther source of uncertainty; the relationbetween leukoaraiosis and bleeding riskseems to vary in different clinical contexts.For example, there was a striking differencebetween intracranial haemorrhage risk inpatients with ‘‘ischaemia of presumed arterialorigin’’ (SPIRIT), and stroke in the context of atrial fibrillation. This almost certainly reflectspathological heterogeneity.47
Given these major uncertainties, whatrecommendations can be made? Certainly,warfarin should not be used for recurrentstroke/TIA in patients with leukoaraiosis whoare in sinus rhythm and have no other clearindication; high intensity anticoagulation
(INR. 3) is hazardous in these patients withan annual risk of major bleeding of 7% (about
In acute stroke or transient ischaemic attack, there is no evidence to suggest that a different approachto treatment should be taken in the presence of leukoaraiosis
3O’Sullivan
www.practical-neurology.com

8/2/2019 Leuk Oarai Osis
http://slidepdf.com/reader/full/leuk-oarai-osis 11/13
half of which will be intracranial andapproximately a third fatal). Warfarin prob-ably should be given to patients with previousstroke and atrial fibrillation, but with caution.The influence of leukoaraiosis on bleeding riskis less clear in this group47 but, nevertheless,cognitive aspects and the risk of falls shouldbe carefully evaluated. Better methods of riskstratification are certainly needed. Newimaging approaches that provide a deeperinsight into the underlying pathology mayhelp, but other aspects such as betterevaluation of the risk of falls will also beimportant.
Risk factorsCurrently, treatment of vascular risk factors isoften all that physicians have at their disposalin patients who are found to have leukoar-aiosis. But even here, there has long been aconcern that blood pressure lowering couldexacerbate white matter ischaemia because of impaired autoregulation. But so far clinicaltrials of anti-hypertensive therapy have notidentified a subgroup of patients who dodeteriorate in practice. In addition, in thePROGRESS study of blood pressure loweringwith perindopril, the effect of treatment toslow the progression of white matter diseasewas greatest in the subgroup with leukoar-aiosis at baseline.49 However, patients withsevere leukoaraiosis are probably not well-represented in previous trials, and assessmentof severity has been limited, so the existence
of a subgroup vulnerable to hypotensivetreatment remains possible.
There is less evidence about how leukoar-aiosis should influence treatment in othercontexts such as cognitive impairment, or inasymptomatic older people. Many physicianswould treat risk factors in these individuals,and observational studies lend some supportto this strategy, but more data are needed.
CONCLUSIONSThe concept of leukoaraiosis has now beenwith us for two decades and has generatedcontroversy, debate and fruitful investigation.In the last decade, a number of thecontroversies have faded: for example, theassociation with cognitive function has beenconvincingly demonstrated, the deficitsdefined more clearly and the prognosticimportance of leukoaraiosis has becomeclearer. Far from being an incidental andharmless consequence of ageing, leukoaraio-sis is a clear predictor of risk of stroke, fallsand, most importantly, treatment-relatedcerebral haemorrhage. In an ageing society,
and with increasing use of imaging andpotentially hazardous treatments, an under-standing of the meaning and significance of this imaging appearance will be valuable toneurologists and physicians in general.
ACKNOWLEDGEMENTSI am very grateful to Dr Tom Hughes, DrFergus Rugg-Gunn and Dr David Sharp forhelpful comments on the manuscript, to DrAlistair Lammie for helpful discussions of the
pathology and for figure 2, and to Dr Anand Viswanathan and Dr Steven Greenberg for
PRACTICE POINTS
l Do not be content to overlook a radiological report of ‘‘some small vessel disease [of uncertain significance]’’. Ask yourself which small vessel disease, consider vascular riskfactors and think about cognitive aspects.
l Alzheimer’s disease and sporadic amyloid angiopathy are commonly associated withleukoaraiosis.
l Cognitive deficits are difficult to detect with many screening tools (for example, the Mini-Mental State Examination).
l Active treatments such as carotid endarterectomy and thrombolysis should not bewithheld; patients with leukoaraiosis still often benefit from them in the right clinicalcontext. But different counselling should be given, quoting higher treatment risks.
l Leukoaraiosis is associated with an increased risk of intracerebral haemorrhage withwarfarin therapy in some cohorts. Warfarin also needs careful consideration given themorbidity and mortality from falls.
Practical Neurology
10.1136/jnnp.2007.139428

8/2/2019 Leuk Oarai Osis
http://slidepdf.com/reader/full/leuk-oarai-osis 12/13
helpful comments on the link with cerebralamyloid angiopathy and figure 5. I am anAlexander von Humboldt fellow in Germanyand supported by the Peel Medical ResearchTrust. This article was reviewed by HeineMattle, Berne, Switzerland.
REFERENCES1. Hachinski VC, Potter P, Merskey H. Leuko-araiosis.
Arch Neurol 1987;44 :21–3.2. Wiszniewska M, Devuyst G, Bogousslavsky J,et al.
What is the significance of leukoaraiosis in patientswith acute ischemic stroke?Arch Neurol 2000;57 :967–73.
3. Erkinjuntti T, Kurz A, Gauthier S,et al. Efficacy of galantamine in probable vascular dementia andAlzheimer’s disease combined with cerebrovasculardisease: a randomised trial.Lancet 2002;359 :1283–90.
4. Steingart A, Hachinski VC, Lau C,et al. Cognitiveand neurologic findings in demented patients withdiffuse white matter lucencies on computedtomographic scan (leuko-araiosis).Arch Neurol 1987;44 :36–9.
5. Caplan LR, Schoene WC. Clinical features of subcortical arteriosclerotic encephalopathy(Binswanger disease).Neurology 1978;28 :1206–15.
6. Babikian V, Ropper AH. Binswanger’s disease: areview.Stroke 1987;18 :2–12.
7. Yamanouchi H, Sugiura S, Tomonaga M. Decreasein nerve fibres in cerebral white matter inprogressive subcortical vascular encephalopathy of Binswanger type. An electron microscopic study.J Neurol 1989;236 :382–7.
8. Fazekas F, Kleinert R, Offenbacher H,et al.Pathologic correlates of incidental MRI whitematter signal hyperintensities.Neurology 1993;43 :1683–9.
9. van Swieten JC, van den Hout JH, van Ketel BA,et al. Periventricular lesions in the white matter onmagnetic resonance imaging in the elderly. Amorphometric correlation with arteriolosclerosisand dilated perivascular spaces.Brain1991;114 :761–74.
10. Lotz PR, Ballinger WE Jr, Quisling RG. Subcorticalarteriosclerotic encephalopathy: CT spectrum andpathologic correlation.AJR Am J Roentgenol 1986;147 :1209–14.
11. Lammie GA. Pathology of small vessel stroke.Br
Med Bull 2000;56 :296–306.12. Lammie GA, Brannan F, Slattery J,et al.
Nonhypertensive cerebral small-vessel disease. Anautopsy study. Stroke 1997;28 :2222–9.
13. Brun A, Englund E. A white matter disorder indementia of the Alzheimer type: a pathoanatomicalstudy. Ann Neurol 1986;19 :253–62.
14. Tomimoto H, Akiguchi I, Akiyama H,et al. Vascularchanges in white matter lesions of Alzheimer’sdisease. Acta Neuropathol (Berl) 1999;97 :629–34.
15. Greenberg SM, Gurol ME, Rosand J,et al. Amyloidangiopathy-related vascular cognitive impairment.Stroke 2004;35 :2616–19.
16. Khan U, Porteous L, Hassan A,et al. Risk factorprofile of cerebral small vessel disease and itssubtypes. J Neurol Neurosurg Psychiatry 2007;78 :702–6.
17. Hassan A, Hunt BJ, O’Sullivan M,et al.Homocysteine is a risk factor for cerebral smallvessel disease, acting via endothelial dysfunction.Brain 2004;127 :212–19.
18. Prins ND, van Dijk EJ, den HT,et al. Cerebral small-vessel disease and decline in informationprocessing speed, executive function and memory.Brain 2005;128 :2034–41.
19. O’Sullivan M, Morris RG, Huckstep B,et al.Diffusion tensor MRI correlates with executivedysfunction in patients with ischaemicleukoaraiosis.J Neurol Neurosurg Psychiatry 2004;75 :441–7.
20. Briley DP, Wasay M, Sergent S,et al. Cerebral whitematter changes (leukoaraiosis), stroke, and gaitdisturbance. J Am Geriatr Soc 1997;45 :1434–8.
21. Baloh RW, Yue Q, Socotch TM,et al. White matterlesions and disequilibrium in older people. I. Case-control comparison.Arch Neurol 1995;52 :970–4.
22. Whitman GT, Tang Y, Lin A,et al. A prospectivestudy of cerebral white matter abnormalities inolder people with gait dysfunction.Neurology 2001;57 :990–4.
23. Rossor MN, Tyrrell PJ, Warrington EK,et al.Progressive frontal gait disturbance with atypicalAlzheimer’s disease and corticobasal degeneration.J Neurol Neurosurg Psychiatry 1999;67 :345–52.
24. Nutt JG, Marsden CD, Thompson PD. Humanwalking and higher-level gait disorders, particularlyin the elderly.Neurology 1993;43 :268–79.
25. Briley DP, Haroon S, Sergent SM,et al. Doesleukoaraiosis predict morbidity and mortality?Neurology 2000;54 :90–4.
26. Liston R, Mickelborough J, Harris B,et al.Conventional physiotherapy and treadmill re-trainingfor higher-level gait disorders in cerebrovasculardisease.Age Ageing 2000;29 :311–18.
27. Baezner H, Oster M, Henning O,et al. Amantadineincreases gait steadiness in frontal gait disorderdue to subcortical vascular encephalopathy: adouble-blind randomized placebo-controlled trialbased on quantitative gait analysis.Cerebrovasc Dis 2001;11 :235–244.
28. Sakakibara R, Hattori T, Uchiyama T,et al. Urinaryfunction in elderly people with and withoutleukoaraiosis: relation to cognitive and gaitfunction. J Neurol Neurosurg Psychiatry 1999;67 :658–60.
29. Pantoni L, Poggesi A, Basile AM,et al. Leukoaraiosispredicts hidden global functioning impairment innondisabled older people: the LADIS (Leukoaraiosisand Disability in the Elderly) Study.J Am Geriatr
Soc 2006;54 :1095–101.30. Streifler JY, Eliasziw M, Benavente OR,et al.Prognostic importance of leukoaraiosis in patientswith symptomatic internal carotid artery stenosis.Stroke 2002;33 :1651–5.
31. O’Sullivan M, Morris RG, Markus HS. Brief cognitiveassessment for patients with cerebral small vesseldisease. J Neurol Neurosurg Psychiatry 2005;76 :1140–5.
32. Bak TH, Mioshi E. A cognitive bedside assessmentbeyond the MMSE: the Addenbrooke’s CognitiveExamination.Pract Neurol 2007;7:245–9.
33. Wahlund LO, Barkhof F, Fazekas F,et al. A newrating scale for age-related white matter changesapplicable to MRI and CT.Stroke 2001;32 :1318–22.
34. Knudsen KA, Rosand J, Karluk D,et al. Clinicaldiagnosis of cerebral amyloid angiopathy:
3O’Sullivan
www.practical-neurology.com

8/2/2019 Leuk Oarai Osis
http://slidepdf.com/reader/full/leuk-oarai-osis 13/13
validation of the Boston criteria.Neurology 2001;56 :537–9.
35. Chabriat H. Diffusion histograms in CADASIL.Stroke 2005;36 :2526.
36. O’Sullivan M, Lythgoe DJ, Pereira AC,et al. Patternsof cerebral blood flow reduction in patients withischemic leukoaraiosis.Neurology 2002;59 :321–6.
37. O’Sullivan M, Summers PE, Jones DK,et al. Normal-
appearing white matter in ischemic leukoaraiosis: adiffusion tensor MRI study.Neurology 2001;57 :2307–10.
38. Wardlaw JM, Sandercock PA, Dennis MS,et al. Isbreakdown of the blood-brain barrier responsiblefor lacunar stroke, leukoaraiosis, and dementia?Stroke 2003;34 :806–12.
39. Akiguchi I, Tomimoto H, Suenaga T,et al. Blood-brain barrier dysfunction in Binswanger’s disease;an immunohistochemical study.Acta Neuropathol (Berl) 1998;95 :78–84.
40. Wallin A, Sjogren M, Edman A,et al. Symptoms,vascular risk factors and blood-brain barrierfunction in relation to CT white-matter changes indementia. Eur Neurol 2000;44 :229–35.
41. Starr JM, Wardlaw J, Ferguson K,et al. Increasedblood-brain barrier permeability in type II diabetesdemonstrated by gadolinium magnetic resonanceimaging.J Neurol Neurosurg Psychiatry 2003;74 :70–6.
42. Hassan A, Hunt BJ, O’Sullivan M,et al. Markers of endothelial dysfunction in lacunar infarction andischaemic leukoaraiosis.Brain 2003;126 :424–32.
43. Gurol ME, Irizarry MC, Smith EE,et al. Plasma beta-amyloid and white matter lesions in AD, MCI, andcerebral amyloid angiopathy.Neurology 2006;66 :23–9.
44. van Dijk EJ, Prins ND, Vermeer SE,et al. Plasmaamyloid beta, apolipoprotein E, lacunar infarcts,and white matter lesions.Ann Neurol 2004;55 :570–5.
45. Thal DR, Ghebremedhin E, Orantes M,et al. Vascularpathology in Alzheimer disease: correlation of cerebral amyloid angiopathy and arteriosclerosis/lipohyalinosis with cognitive decline.J Neuropathol Exp Neurol 2003;62 :1287–301.
46. Palumbo V, Boulanger JM, Hill MD,et al. Leukoaraiosisand intracerebral hemorrhage after thrombolysis inacute stroke.Neurology 2007;68 :1020–4.
47. Gorter JW. Major bleeding during anticoagulationafter cerebral ischemia: patterns and risk factors.Stroke Prevention In Reversible Ischemia Trial(SPIRIT). European Atrial Fibrillation Trial (EAFT)study groups. Neurology 1999;53 :1319–27.
48. Smith EE, Rosand J, Knudsen KA,et al.Leukoaraiosis is associated with warfarin-related
hemorrhage following ischemic stroke.Neurology 2002;59 :193–7.
49. Dufouil C, Chalmers J, Coskun O,et al. Effects of blood pressure lowering on cerebral white matterhyperintensities in patients with stroke: thePROGRESS (Perindopril Protection AgainstRecurrent Stroke Study) Magnetic ResonanceImaging Substudy.Circulation 2005;112 :1644–50.
Practical Neurology