Embed Size (px)
Citation preview

J Korean Neurosurg Soc/Volume 28/March, 1999 347
KISEP Clinical Research J Korean Neurosurg Soc 28::::347-353, 1999
전방 경유 경추 유합술:단순 추체유합과
Locked 및 Non-Locked 금속판을 사용한
추체유합술들에 대한 비교연구*
가톨릭대학교 의과대학 신경외과학교실
박춘근·최영근·조경석·지 철·박성찬·강준기 = Abstract =
Anterior Cervical Interbody Fusion::::Comparison Study between Simple Fusion, Locked and Non-locked Plating Systems
Chun Kun Park, M.D., Young Geun Choi, M.D., Kyung Suk Cho, M.D., Chul Ji, M.D., Sung Chan Park, M.D., Joon Ki Kang, M.D.
Department of Neurosurgery, College of Medicine, Catholic University, Seoul, Korea
he use of metallic plate and screws in the anterior cervical fusion has become generally acceptable and popular.
Mainly, there are two different plating systems available. However, there has been few attempts to compare their
clinical results with and without a plating system or between two different systems in a single series of clinical
study.
The authors reviewed 117 patients who underwent anterior cervical fusion during the period of January 1992 to
September 1996. Simple fusion without a plating system was applied in 55 cases(group 1), a bicortical non-locked
plate screw system in 25(group 2), and a monocortical locked plate screw system in 37(group 3). The average
follow-up period was 13.2 months. In group 1, twenty-two patients(40%) with fracture-dislocation or corpectomy
required a rigid brace such as halo brace and Minerva cast for 3 months postoperatively and seven patients(13%)
experienced graft complications, mainly graft extrusion. In group 2 and 3, the patients required only soft braces for 4
to 8 weeks and no patients experienced serious graft complications like ones in group 1, but, instead two patients
with screw breakages, two back-outs and one non-union were observed. In comparison of the clinical compli-
cations such as hoarsness, there were no significant differences between the groups.
In conclusion, the plating system in anterior cervical fusion appears to be safe despite the facts that more techni-
cal demands are required during surgery. It also provides better postoperative stability in the spine and permits earlier
ambulation without a rigid brace. A monocortical locked plate screw system appears to have less hardware failures
and better surgical results than a bicortical non-locked plate screw system. KEY WORDS:Anterior cervical interbody fusion·Bicortical non-locked plate and screw system·Monocortical loc-
ked plate and screw system·B.O.P.·Allograft.
서 론
하부 경추에 대한 전방 접근법은 다양한 경추 질환에서 이
용되고 있다13)28)32). 경추 전방 접근법은 주로 퇴행성 질환
을 수술하는데 이용되고 있으나, 실제로는 경추체와 경추간
판을 포함한 경추 신경관 전방의 모든 병소에 대한 수술 시
이용 될 수 있다14)17)36)37). 전방 접근법을 이용한 경추부의
수술 시에는 통상 수술 후 경추체 유합술이 필요하며, 특히
수술 전 경추부의 불안정이 관찰되었던 환자에서는 전방 경
TTTT
*본 논문은 가톨릭 중앙의료원의 연구비 지원에 의하여 시행
되었으며, 1997년도 대한신경외과학회 추계 정기학술대회에
서 발표된 바 있음.

전방 경유 경추 유합술:단순 추체유합과 Locked 및 Non-Locked 금속판을 사용한 추체유합술들에 대한 비교연구
J Korean Neurosurg Soc/Volume 28/March, 1999 348
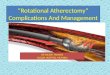
Fig. 1. Immediate postoperative radiograph of 27-year-old manoperated with bicortical non-locked plate screw systemand B.O.P. interbody graft due to traumatic C4-5 sublux-ation. Note the screw piercing the dorsal cortex of thevertebral body(arrow) and radiolucency of B.O.P.
유 수핵제거술을 시행한 경우에도 수술 후 경성 보조구(ri-
gid brace)가 반드시 필요하다. 또한 후방 구조물의 심한 손
상이나 인대의 손상을 동반한 경추 외상에서 전방 접근법으
로 수술을 시행하는 경우 Halo등에 의한 경추부의 외고정
이 수술후 시행되어야 한다1)35)36)37). 그러나 최근 금속판을
이용하여 경추부 전방 내고정술을 수술 시야에서 실시함으로
써 경추부 불안정시 경추체 골유합을 위한 수술 후 경성 보
조구의 착용이나 외고정의 필요성을 감소시켰다.
1970년 Orozoco와 Llovet가 처음으로 stainless steel
금속판을 경추의 전방 유합술에 사용한 이후23) 최근까지 다
양한 전방 경유 경추부 수술용 나사, 금속판 및 기구 등이 이
용되고 있다. 최근에 사용되고 있는 나사 및 금속판들은 bi-
cortical non-locked plate screw system(BNPS)과 mo-
nocortical locked plate screw system(MLPS)의 두 가지
로 크게 대별될 수 있는데10)24)25), 이들은 나사의 고정 방법
에 가장 큰 차이가 있다. 비록 경추부의 여러 질환에서 이들
나사와 금속판을 이용한 내고정의 효용성이 확립되어 있으나,
전방 경유 경추 고정술에 있어서 금속판을 사용한 경우와 사
용하지 않는 경우 각각의 surgical morbidity와 임상 경과의
비교 및 위에서 대별되었던 서로 다른 두 종류의 내고정 기
구 사용에 따른 임상 결과의 비교가 요구될 것으로 사료되었
다. 따라서 저자들은 전방 경추 고정술시 금속판을 사용한 예
와 사용하지 않은 예에 대한 수술 합병증과 수술 후 경과, 입
원기간 및 수술 결과의 비교 분석과 MLPS와 BNPS의 비
교 분석을 동일 연구 계획하에 시행함으로써 향후 전방 경유
경추부 수술시 치료 방침의 결정을 위한 자료를 마련하고자
하였다.
대상 및 방법
1992년 1월부터 1996년 9월까지 4년 6개월간 단일 병
원에서 시행한 전방 경유 경추 고정술 환자 117례에 대하여
후향적 분석을 하였다. 본 연구에서 시행되었던 전방 경추 고
정술의 수술 적응증은 첫째, 골절, 종양 혹은 염증에 의한
하부 경추의 불안정, 둘째, 다발성 추간판 제거술, uncect-
omy 혹은 추체 제거술 등의 다발성 감압술을 시행한 경우,
셋째, 후방 경추의 불안정을 동반한 전방 경추의 병변, 혹은
넷째, 이식한 골편에 의한 합병증 발생시 등이었다. 모든 수
술은 단일 술자(C.K.P.)에 의하여 시행되었다. 수술방법은
시기에 따라 비교적 구분이 뚜렷하였으므로 환자들을 수술
시행 연대와 수술의 방법에 따라 세군으로 나눌 수 있었다.
1992년 1월부터 1993년 12월까지 2년간 금속판을 사용하
지 않고 전방 경추 유합술을 시행한 군은 55례이었고(gro-
up 1), 1994년 1월부터 1994년 6월까지 6개월간 25례에
서 BNPS(Top, Fheling, Germany)를 사용하여 내고정을
시행하였으며(group 2)(Fig. 1), 1994년 7월부터 1996년
9월까지 약 2년간 37례에서 MLPS(Orion, Danek, USA)
를 사용하였다(group 3)(Fig. 2). 수술례중 Cloward 방법
으로 39개 추간판이 제거되었으며, Smith-Robinson방법으
로는 106개의 추간판이 제거되었고, 척추체 제거술은 43례
에서 실시되었다.
골유합에 사용된 이식물은 장골에서 채취한 자가골이식이
23례이었고, fibular allograft(Tutoplast, Biodynamics, Ge-
rmany)를 사용한 례는 46례이었으며, B.O.P.(biocompa-
table osteoconductive polymer;DTI Medical, Belgium)
를 사용한례는 64례이었다. 수술 시행시 추간판과 석회화된
후방 인대 및 추간공의 골극은 광확대된 수술 현미경하에서

박춘근 · 최영근 · 조경석 · 지 철 · 박성찬 · 강준기
J Korean Neurosurg Soc/Volume 28/March, 1999 349
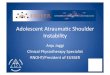
Fig. 2. Postoperative radiograph of 43-year-old woman opera-ted with monocortical locked plate screw system andfibular allograft due to C5-6 and C6-7 HNP. Note the sc-rews not piercing the dorsal cortex of the vertebral body(arrow).
제거되었으며, 2례를 제외한 모든례에서 우측 anterior me-
dial approach가 시행되었고, 나머지 2례의 경우는 cervico
-thoracic junction병변에 대한 우측 상쇄골 접근법(supr-
aclavicular approach)이 시행되었다. 평균 추적 관찰 기간
은 13.2개월(6∼25개월)이었으며, 추적 기간중 환자는 임상
적, 방사선학적으로 관찰되었다. 임상적 관찰은 주로 수술 및
수술 술기와 관련된 임상경과 즉 수술 합병증 혹은 이식 골
편에 의한 합병증등이 관찰되었으며, 신경학적인 결과나 기
능적인 결과는 비교 분석하지 않았는데 이는 본 연구의 대상
이 다양한 종류의 경추 질환으로서 이와 같이 서로 다른 병
변에 대한 임상 결과의 비교는 부적절한 것으로 판단되었기
때문이었다. 방사선학적 추적검사에서는 이식편의 유합율이
나 임상 경과에 대한 수술 후 불안정증 및 기계의 파손이나
기능부전의 영향을 분석하기 위하여 이식된 골편 등의 유합
률과 수술 후 불안정 및 기계 사용 예들에서 기계의 기능부
전 여부를 관찰하였다. 얻어진 수술 자료들은 Chi-square 검
사법으로 통계적 검정을 시행하였으며, 유의 수준은 p<0.05
로 하였다.
결 과
1. 분 포
제1군의 평균 연령은 43.5세(17∼72세)이었고, 제2군은
45.7세(22∼68세), 제3군은 47.2세(21∼70세)이었다(Table
1). 대부분의 환자(80%)들이 남자이었으며(Table 2), 질환
의 분포는 약 1/3의 환자들이 외상성 골절-전이, 약 1/3의 환
자들은 경추 척추증(cervical spondylosis) 및 후종인대 골화
증이었고, 나머지 약 1/3의 환자들은 다발성 경추간판 탈출
증 혹은 경추의 불안정증이었다(Table 3). 수술이 시행되었던
부위의 약 90%가 제4, 5, 제5, 6 및 제6, 7경추부이었다.
Table 2. Sex distribution
Surgical method* Male Female Total
Without P/S 44 11 55 Non-locked P/S 20 5 25 Locked P/S 28 9 37
Total 92 25 117 *p/s:plate and screws
Table 3. Diagnosis in 117 patients who underwent anterior cerv-ical interbody fusion
Surgical method Diagnosis
Without P/S Non-locked Locked P/S
Trauma Fracture and/or dislocation 15 6 16
Cervical spondylosis & OPLL* Corpectomy & discectomy 17 7 8
Cervical HNP** Multiple levels or instability 23 9 12 Graft complication 3
Cervical spine tumor Corpectomy 1
Total 55 25 37 *OPLL:ossified posterior longitudinal ligament **HNP:herniated nucleus pulposus
Table 1. Age distribution
Age Surgical method*
< 20 21-40 41-60 > 60 Total
Without P/S 4 14 31 6 55 Non-locked P/S 8 14 3 25 Locked P/S 15 17 5 37
Total 4 37 62 14 117 *p/s:plate and screws

전방 경유 경추 유합술:단순 추체유합과 Locked 및 Non-Locked 금속판을 사용한 추체유합술들에 대한 비교연구
J Korean Neurosurg Soc/Volume 28/March, 1999 350
2. 수술중 및 수술 직후 임상소견
척추 절제술을 시행하였던 38례중 2례의 경우를 제외한
모든 례에서 수혈은 시행되지 않았다. 수술에 소요된 평균 시
간은 제1군에서는 113분, 제2군에서는 94분, 제3군에서는
79분이었다. 경추 수핵탈출시 수술 후 환자의 재원 일수는 대
부분 3∼4일이었으며 외상성 골절-탈구 환자를 제외하는 경
우 제1군에서는 평균 8.7일이었고, 제2군과 제3군에서는 4.1
일이었다.
3. 수술 후 처치
제1군의 경우 40%의 환자에서 halo vest, Minerva cast,
Somi brace와 같은 경성 경추부 보조구를 사용하였으나, 제
2군 및 3군의 경우 60%와 73%의 환자에서 Philadelphia
collar와 같은 연성 보조구를 8주 이내로 사용하였다. 제1군
의 경우에도 54%의 환자에서 8 내지 12주의 연성 보조구
를 사용하였다(Table 4).
4. 수술 합병증
수술 합병증은 임상 소견, 이식편 합병증, 기계 손상으로
구분하여 비교하였다. 임상 증상에서는 각 군별 유의한 차이
는 보이지 않았으나. 금속판을 사용한 제2군과 3군에서 수술
후 경추부 통증과 음식물을 연하시 식도의 이물감 및 연하곤
란을 호소하는 경우가 단순 척추체 유합술의 경우(제1군)보
다 많은 경향을 보였다. 이식편과 관련된 합병증으로는 제1
군에서 이식골의 돌출이 다른 군들과 비교하여 의의있게 많
이 발생하였으며(p<0.05;Chi-square test), 이에 따른 유
합 부전의 증가도 관찰되었다. 기계 손상에 의한 합병증의 경
우 제3군 즉 MLPS 사용 례들에서는 한 례도 관찰되지 않
았으나 제2군 즉 BNPS 사용 례들에서는 나사못의 파손이
2례에서 발생하였으며, 나사못의 빠져나옴(back-out)이 2례
에서 있었고, 이식골의 불유합도 1례에서 관찰되었으나(Ta-
ble 5), 기계 제거나 재삽입 등을 위한 재수술은 한 례에서
도 시행되지 않았다.
고 찰
본 연구는 후향적으로 시도되었으므로 자료의 분석에 제
한이 있다. 가장 큰 문제점은 각 군별로 일정하지 않은 변수
를 가지고 있다는 것이다. 대표적인 예가 각 군에서 다양한
수술 방법과 다양한 이식편을 사용하였다는 점이다. 그러나
본 연구의 결과를 통하여 저자들은 하부 경추 질환에 대한 전
방 경유 수술법의 전반적 분석을 시도 함으로써, 다양한 변
수에 영향을 적게 받는 범위 내에서 금속판을 이용한 경우
와 이용하지 않은 경우의 수술 전후 임상경과와 수술 합병
증을 비교하였고, 또한 금속판 사용 례들 중 BNPS와 ML-
PS에 대한 결과도 비교 분석하였다.
최근 전방 경유 경추 유합술은 하부 경추의 유합에 널리
사용되고 있다. 비록 여러 가지 경추 질환에서 전방 경유 이
식골 삽입에 의한 단순 경추체 유합술이 광범위하게 사용되
고 있으나, 외상성 경추 질환과 같이 척추 불안정을 보이는
Table 4. Postoperative application of orthoses
Surgical method(Number of patients) Orthoses Without P/S
(55) Non-locked(25)
Locked P/S (37)
Halo vest* 9 Minerva cast* 11 Somi brace* 2 Philadelphia collar
More than 8 weeks 18 10 10 Less than 8 weeks 15 15 27
*Immobilization for about 3 months postoperatively
Table 5. Surgical complication***
Surgical method(number of patients) Complication Without P/S
(55) Non-locked (25)
Locked P/S (37)
Clinical complication Increased neck pain 1 1 Numbness in the hands,
intermittent 3 1 1
Transient hoarsness 2 1 2 CSF leakage 2 Vascular injury 1 Foreign body sensation 3 3
on swallowing Dysphagia 3 3 Infection Hematoma
Graft complication Graft extrusion 5 Graft impact 1 Graft settling* 1 4** 3
Hardware failure Screw breakage 2 Screw back-out 2 Non-union 1 Kyphosis 1
*Without P/S:BOP 1;non-locked:autograft 1, BOP 3;locked:autograft 1, BOP 2 **In two cases, the screws were fractured with the settling of the grafted B.O.P. ***Chi-square test:Graft extrusion, p<0.05;all other variab-les, p>0.05.

박춘근 · 최영근 · 조경석 · 지 철 · 박성찬 · 강준기
J Korean Neurosurg Soc/Volume 28/March, 1999 351
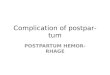
Fig. 3. Hinge effect upon a bicortical screw exerted by settling ofa graft material and axial load.
경우 단순 경추체 유합술만으로는 많은 합병증을 유발할 수
있다33)35). 보고된 합병증에는 이식골의 돌출과 척추의 수술
후 불안정증 등이 있다. 이러한 문제점들을 해결하기 위하여
단순 경추체 유합술 후 경추의 안정을 유지하기 위하여 halo
device나 Minerva cast등을 이용한 외고정을 시행하거나,
전방 수술후 추체 후방 유합을 위한 2차 수술을 시행하는 경
우도 있다. 그러나 이들 방법은 환자를 수술후 빠른 시일내
에 거동시키고 재활치료를 시행하려는 의도에 제약이 된다.
경추간판의 수술이나 경추 척주증의 전방 경유 단순 추체 유
합술시에도 이식골의 돌출이 8%에서 발생하는 것으로 보고
되고 있다30). 본 연구에서도 단순 전방 골유합을 시행한 경
우에 수술후 경성 보조기로 외고정을 시행하였거나, 수술후
수 일간의 안정후 거동을 시행하였는데도 불구하고 약 9%
에서 이식골의 돌출이 관찰되었던 반면, 금속판을 시행하여
유합술을 시행하였던 경우에서는 수술 직후 거동을 시행하였
는데도 한 례에서도 이식골 돌출이 관찰되지 않았다.
금속판을 이용하여 전방 유합술을 시행한 후에 연성 보조구
의 사용이 반드시 필요한 것은 아니나, 많은 척추 외과의들이
수술 후 수 주간의 연성 보조구 착용을 추천하고 있다2)7)8)19)
22)26)27)34). 그러나 이와 같은 수술후 보조구 착용의 필요 여부
는 각각의 경우에 따라서 결정하는 것이 옳을 것으로 사료된
다. 본 저자들은 수술 전 척추 후방 부위의 불안정이 의심되
었던 젊고 건강한 환자의 경우에는 수술 후 4 내지 6주 정도
연성 보조구의 착용을, 심한 불안정이 있었거나 고령 환자의 경
우에는 수술 후 8 내지 12주의 연성 보조구 착용을 권하였다.
전방 경유 경추 유합술은 1950년대부터 고안되어 사용하
기 시작하였으며 이후 다양한 재질의 금속판이 개발되었다.
1970년대에 Orozoco와 Llover는 stainless 금속을 이용한
AO small fragment 금속판을 개발하여 사용하였으며23), 이
후 H-shaped stainless 금속판이 개발되어 사용되었다. 그
러나 이 stainless 금속은 CT와 MRI에서 인공물(artifact)
이 나타나는 단점이 있었다. 최근에는 titanium을 사용한 기
구가 개발되었으며, 이 기구들은 CT와 MRI에도 좋은 영상
을 얻을 수 있는 장점이 있어 널리 사용되고 있다15)29).
이와 같은 기구들의 개발 이후 많은 척추 외과의에 의하여
하부 경추의 외상성 병변, 퇴행성 경추 질환, 종양 및 염증성
질환에 대한 전방 경유 금속판 및 나사못 고정술이 시도되었
다3)4)6)9)16)21)23). 이들의 보고에서는 주로 금속판을 이용한
경추의 고정시 수술에 의한 감압과 동시에 고정을 시행할 수
있다는 점이 강조되었으나 시술중 요구되는 기술적 문제점
이나 기구의 실패율에 대한 분석이 부족하였다. 기술적인 측
면의 경우 저자들의 임상 경험과 본 연구의 결과를 종합할 때
금속판과 나사와 같은 기구의 사용이 수술의 유병율의 증가
나 수술 시간의 뚜렷한 연장을 초래하지 않는 것으로 판단
되었다. 금속판을 사용한 환자들 중 경도의 경부통 호소와 음
식물의 섭취시 식도 이물감과 연하곤란의 증상이 있었으나
이는 모두 일시적인 소견이었다. 4례에서 기계손상이 관찰되
었는데, 2례의 경우 나사 파손이, 나머지 2례에서는 나사의
뒤로 빠짐이 관찰되었다. 이와 같은 기계파손들은 모두 BN-
PS를 사용한 2군에서 발생하였다. 이 결과만을 고려한다면
기구의 강도가 MLPS에서 BNPS보다 더 우수하다고 할 것
이다. 본 저자들이 사용한 기구(Top과 Orion)에 대한 구체
적이고 선택적인 생체역학적 강도의 비교 보고는 없다. 최근
에 Ceddia등이 BNPS인 Caspar와 Lemaire와 MLPS인 Mo-
rscher에 대한 비교 보고를 하였고10), 박 등25)이 Top의 BN-
PS와 MLPS를 비교하여 보고한 바 있는데 이들 역시 기계
손상이 BNPS를 사용한 경우에서 더 많다고 보고하였다. 그
러나 왜 BNPS에서 기계 손상이 더 많이 발생하는지에 대한
이유는 아직 정확히 밝혀지지 않고 있다. 최근의 보고에 의
하면 나사못이 부러진 모든 경우에서 이식골의 주저앉음(se-
ttling)이 동반되었으며, Caspar 금속판과 Cervical Spine
Locked Plate System(CSLPS)에 대한 사체 모델의 비교
연구 결과 BNPS인 Caspar 금속판이 MLPS인 CSLPS에의
한 고정보다 더 안정된 것으로 밝혀졌다11). 이 두 가지의 결
과를 종합할 때, 양측 골피질 관통 나사(bicortical screw)
는 추체의 전방 및 후방의 cortex를 뚫고 있음으로 안정성
은 유지할 수 있으나, 이식골의 주저 앉음이 동반되는 경우
에는 편측 골피질 관통 나사(monocortical screw)보다 상대
적으로 축성 하중(axial loading)을 더 받게 되며 경첩 효과
(hinge effect)에 의하여 나사가 파손될 가능성이 상대적으로
커지는 것으로 가정할 수 있을 것이다(Fig. 3). 저자들의 예

전방 경유 경추 유합술:단순 추체유합과 Locked 및 Non-Locked 금속판을 사용한 추체유합술들에 대한 비교연구
J Korean Neurosurg Soc/Volume 28/March, 1999 352
들에서도 이식골의 주저 앉음이 BNPS의 나사못에 가해지는
축성 하중에 비정상적 영향을 주어 나사의 손상이 발생하였
을 것으로 추측할 수 있었다. 그러나 저자들이 사용한 기구에
서의 손상률 차이의 정확한 기전을 이해하기 위하여는 사용
되었던 기구들에 대한 적절한 생체역학적 비교 연구가 요구
될 것으로 사료된다.
제2군에서 방사선학적 추적 관찰 도중 2례에서 나사의 뒤
로 빠짐이 관찰되었는데, 이는 수술시 나사못이 후방 골피질
을 관통하지 못한 경우이었다. 따라서 BNPS의 경우 척추강
의 침범을 최소화하는 범위 내에서 나사못이 후방 골피질을
관통하여야 안정된 내고정을 유지할 수 있음을 알 수 있었
다. 통상적으로 저자들은 수술 중 나사못의 삽입시 C-arm
방사선 투시기를 이용하여 나사의 후방 골피질 관통 여부를
확인하였으며 따라서 BNPS를 사용한 수술 시간이 방사선
투시기의 사용 없이 나사못 삽입이 가능한 MLPS의 경우보
다 오래 소요되었다. 제3군에서는 나사의 뒤로 빠짐이 관찰
되지 않았으나, 편측 골피질 관통 고정나사를 사용하였더라
도 중증의 골다공증 환자에서 사용하였을 경우나 금속판의
크기를 잘못 선택하여 금속판의 일부가 주변 정상 추간판 전
면에 고정되는 경우 수술 후 거동시 추간부의 운동에 의하여
나사못의 뒤로 빠짐이 발생할 수 있을 것이다.
전방경유 수술에 의한 금속판이 이식편을 고정시키고, 골
유합을 촉진시킨다는 것은 잘 알려진 사실이다. 특히 긴 부
위의 추체 제거술 후 삽입된 이식골을 고정시키기 위하여 이
식골의 중앙 부위에 나사못을 사용함으로써 이식골의 전위를
막을 수 있다18). 본 연구에서는 금속판을 사용한 경우 이식
골의 전위는 일어나지 않았으나, 제2군중 B.O.P.를 이식편으
로 사용하였던 1례에서 불유합이 발생하였으며, 제3군에서
는 불유합이 일어나지 않았다. 따라서 제1군에서의 이식편 돌
출 등 이식편 합병증에 의한 재수술 예를 제외한 경우 전체적
인 유합율은 99%이었다.
본 연구에서는 세 종류의 이식골을 사용하였는데, 장골에
서 채취한 autograft, allograft와 B.O.P.이다. 이중 autog-
raft를 사용한 2례(2/23)와 B.O.P.를 사용한 6례(6/64)에
서 이식골의 주저 앉음이 있었으며 전체적인 이식편 주저 앉
음은 9%이었다. 자가골이식의 함몰은 골다공증을 갖고 있
었던 고령의 환자에서 주로 일어난다고 보고되어 있으며12),
본 저자들이 경험한 2례의 경우도 모두 60세 이상의 환자이
었다. B.O.P.의 장점은 강도가 세기 때문에 그 모양의 변형
이 거의 없으며, 합성된 제품이므로 수술후 조직 제공 부위의
통증이 없고 이로 인해 수술후 조기 거동 및 재원일의 감소
를 가져올 수 있다는 것들이다20). Brotchi등은 100례의 경
추 질환 환자에게서 B.O.P.를 이식골로 사용후, 이에 따른 결
과를 6 내지 30개월 동안 추적 관찰하여 보고하였다5). 이들
의 수술 방법은 저자들과 동일하였으나 저자들의 경우와 달
리 이식편의 주저 앉음과 같은 합병증은 없었다고 보고하였
으나 신 등31)의 최근 보고에 의하면 경추 수술중 B.O.P.를 사
용한 10%에서 유사 소견이 관찰되었다 하였다. 일반적으로
이식골의 주저 앉음이 발생된 대부분의 환자는 증상이 없었
으며 비록 나사못의 골절이 동반된 경우에도 수술적인 치료
가 필요하지는 않았다. 그러나 저자들의 결과를 볼 때 B.O.P.
를 경추부 추체 유합술의 이식 재료로 사용할 경우 이식골의
주저 앉음이나 이로 인한 나사못의 골절 등의 발생 가능성
이 다른 이식 재료보다 더 높으므로 전방 경유 경추체 유합
술시에 이식 재료로 사용하기에는 부적절할 것으로 사료되
었다. 물론 이것을 과학적으로 입증하기 위하여는 좀더 세밀
한 임상 연구가 필요할 것이다. 최근부터 사용되고 있는 fi-
bular allograft의 경우는 최장 약 2년간의 추적검사 결과 이
식편과 관련된 합병증은 없었으나 더 많은 예들에서 오랜 기
간의 관찰 결과가 요구된다 하겠다.
맺 음 말
전방 경유 추체 유합에서의 금속판의 사용은 비록 이를
사용하지 않는 경우보다는 수술 시에 여러 조작이 더 필요하
지만 수술 후 경추의 안정성과 수술후 경성 보조구를 사용하
지 않으며 조기 거동 및 조기 퇴원이 가능하다는 점에서는
유용하다고 하겠다. 이들 금속판과 나사못을 사용하는 경우
추체유합의 수술후 유병율 감소 및 보다 낳은 임상 결과를
얻기 위하여는 기구와 이식 재료의 적절한 선택이 중요할 것
으로 판단된다. 이런 관점에서 bicortical non-locked plate
screw system보다 monocortical locked screw system이
더 우수하였던 것으로 판단되며 이식편 제공부위의 통증 감
소와 조기 거동을 가능케하는 이식 재료로서 fibular allog-
raft가 유용할 것으로 사료된다.
• 논문접수일:1998년 8월 13일 • 심사완료일:1998년 9월 23일 • 교신저자:박 춘 근
137-040 서울 서초구 반포동 505번지 가톨릭대학교 의과대학 신경외과학교실
전화:02) 590-1343, 전송:02) 594-4248
References
1) Bailey RW, Badgley CE:Stabilization of the cervical spine by anterior fusion. J Bone Joint Surg Am 42A:565-624, 1960
2) Boccanera L, Laus M:Osteosynthesis of the cervical spine with an anterior plate. Ital J Ortohp Traumatol 15:287-294, 1989
3) Bohler J, Ganderhak T:Anterior plate stabilization for frac-

박춘근 · 최영근 · 조경석 · 지 철 · 박성찬 · 강준기
J Korean Neurosurg Soc/Volume 28/March, 1999 353
ture dislocations of lower cervical spine. J Trauma 20:3, 1980 4) Bremer AM, Nguyen TQ:Internal metal plate fixation com-
bined with anterior interbody fusion in cases of cervical spine injury. Neurosurgery 12:649-653, 1983
5) Brotchi J, Levivier M, Raftopoulos C, et al:Utilisation D'un greffon synthetique, le biocopolymere BOP, dans les abords anterieurs du rachis cervical. Esperience de 100cas. Rachis 1:367-373, 1989
6) Cabanela ME, Ebersol MJ:Anterior plate stabilization for bursting teardrop fractures of the cervical spine. Spine 13:888-891, 1988
7) Caspar W:Anterior cervical fusion and interbody stabilization with the trapezoidal osteosynthetic plate technique:Aesculap Scientific Information, Tuttlingen, Aesculap- Werke-Ag, 1986
8) Caspar W, Barbier DD, Klara PM:Anterior cervical fusion and Caspar plate stabilization for cervical trauma. Neuros-urgery 25:491-502, 1989
9) Caspar W, Harkey HL:Anterior cervical fusion. Caspar ost-eosynthetic stabilization. In:Young PH(ed):Microsurgery of the Cervical Spine. New York, Raven Press, 1991, pp109-142
10) Ceddia A, Carraturo S, D’Angelo V, et al:Anterior fixation of cervical spine. Bicortical screw-plate vs. monocortical self-locking systems(Abstr):13 th Annual Meeting of Joint Sect-ion on Disorders of the Spine and Peripheral Nerves, 1997, pp151
11) Clausen JD, Ryden TC, Traynelis V, et al:Biomechanical ev-aluation of Caspar and cervical spine locking plate system in a cadaveric model. J Neurosurgery 84:1039-1045, 1996
12) Cloward RB:Complications of anterior cervical disc operat-ion and their treatment. Surgery 69:175-782, 1971
13) Cloward RB:The anterior approach for removal of ruptured cervical disks. J Neurosurg 15:602-617, 1958
14) Cloward RB:Treatment of acute fractures and fracture-dis-locations of the cervical spine by vertebral-body fusion. J Ne-urosurg 18:201-209, 1961
15) Ebraheim NA, Coombs R, Rusin JJ, et al:Reduction of pos-toperative CT artifacts of pelvic fractures by the use of titanium implants. Orthopaedics 13:1357-1358
16) Gasman J, Seligson D:The anterior cervical spine plate. Sp-ine 8:700-707, 1986
17) Hoff JT, Wilson CB:Microsurgical approsch to the anterior cervical spine and spinal cord. Clin Neurosurg 26:513-528, 1979
18) Karasick D:Anterior cervical spine fusion:struts, plugs, and plates. Skeletal Radiol 22:85-94, 1993
19) Levi L, Wolf A, Rigamonti D, et al:Anterior decompression in cervical spine trauma:does the timing of surgery affect the outcome? Neursurgery 29:216-222, 1991
20) Lozes G, Fawaz A, Cama A, et al:Discectomies of the lower cervical spine using interbody biopolymere(BOP) implants. Ac-ta Neurochir 96:88-93, 1989
21) Meyer PR:Surgery of Spine Trauma. Neu York:Churchill Li-
vinstone, 1998 22) Oliveira JC:Anterior plate fixation of traumatic lesions of
the lower cervical spine. Spine 12:324-329, 1987 23) Orozco R, Llovert J:Osteosintesis en las fracturas del ra-
quis cervical. Rev Ortop Traumatol 14:285-288, 1970 24) Park CK, Park CK, Cho KS, et al:Anterior cervical interbody
fusion with or without plate and screws system. J Korean Ne-urosurg 25:2052-2058, 1996
25) Park HC, Youn SH, Park HS, et al:Comparative efficacy st-udy between monocortical and bicortical screws in anterior cervical fusion. J Korean Neurosurg 27:599-605, 1998
26) Randle MJ, Wolf A, Levi L, et al:The use of anterior Ca-spar plate fixation in acute cervical spine injury. Surg Neurol 36:181-189, 1991
27) Ripa DR, Kowall MG, Keyer PR Jr, et al:Series of ninety-two traumatic cervical spine injuries stabilized with anterior ASIF plate fusion technique. Spine 16:S46-S55, 1991
28) Robinson RA, Smith GW:Anterolatral cervical disk removal and interbody fusion for cervical disk syndrome. Bull Johns Hopkins Hosp 96:223-224, 1955
29) Salvolaine ER, Ebraheim NA, Andreshak TG, et al:Anterior and posterior cervical spine fixation using titanium implants to facilitate magnetic resonance imaging evaluation. J Orthop Trauma 3:295-299, 1989
30) Saunders RL, Bernini PM, Shirrefs TG Jr, et al:Central cor-pectomy for cervical spondylotic myelopathy:a consecutive series with long-term follow-up evaluation. J Neurosurg 74:163-170, 1991
31) Shin WH, Park JK, Kim BT, et al:The evaluation of the ili-um and biocompatible osteoconductive polymer(BOP) as graft material in cervical spine surgery. J Korean Neurosurg 27:800-807, 1998
32) Smith GW, Robinson RA:Treatment of certain cervical spine disorders by anterior removal of the intervertebral disk and interbody fusion. J Bone Joint Surg Am 40A:607-624, 1958
33) Stauffer ES, Kelly EG:Fracture-dislocations of the cervical spine:instability and recurrent deformity following treatment by anterior interbody fusion. J Bone Joint Surg 59A:45-48, 1977
34) Tippets RH, Apfelbaum RI:Anterior cervical fusion with the Caspar instrumentation system. Neurosurgery 22:1008-1013, 1988
35) Van Peteghem RK, Schweigel JF:The fractured cervical spine rendered unstable by anterior cervical fusion. J Trauma 19:110-114, 1979
36) Verbiest H:Anterior operative approach in cases of spinal cord compression by old irreducible displacement or fresh fr-acture of cervical spine. J Neurosurg 19:389-400, 1962
37) Verbiest H:Anterolateral operations for fractures and dislo-cations in the midline and lower parts of the cervical spine. Report of a series of forty-seven cases. J Bone Joint Surg Am 51A:1489-1530, 1969
![Successful recovery without any neurological complication ... · PDF fileneurological complication after intraoperative cardiopulmonary ... prone CPR [1], ... Extracorporeal CPR seemed](https://img.pdfslide.tips/doc/110x75/5ab6fdce7f8b9ab7638e558a/successful-recovery-without-any-neurological-complication-complication-after.jpg)