Embed Size (px)
Citation preview

AalaaymmtidvmdromS
*
†
A
0©
S
Malaria and Acute Kidney Injury
Saroj K. Mishra, MD,* and Bhabani Shankar Das, MD†
Summary: Malaria is a major public health problem in tropical countries. About 500 millionpeople suffer from malaria, leading to death in 1 to 3 million cases. Acute kidney injury (AKI)is one of the most dreaded complications of severe malaria. As per World Health Organizationcriteria, acute renal failure (serum creatinine level, �3 mg/dL or �265 �mol/L) occurs as acomplication of Plasmodium falciparum malaria in less than 1% of cases, but the mortalityrate in these cases may be up to 45%. It is more common in adults than children. Renalinvolvement varies from mild proteinuria to severe azotemia associated with metabolicacidosis. It may be oliguric or nonoliguric. AKI may be present as a component of multi-organdysfunction or as a lone complication. The prognosis in the latter is generally better. Severalpathogenic mechanisms interplay for the clinical manifestation. The predominant lesions areacute tubular necrosis and mild proliferative glomerulonephropathy. These patients do notprogress to chronic kidney disease. The management of malaria-induced AKI includes appro-priate antimalarials (parenteral artesunate or quinine), fluid electrolyte management, andrenal replacement therapy at the earliest. The use of diuretics should be avoided.Semin Nephrol 28:395-408 © 2008 Elsevier Inc. All rights reserved.Keywords: Malaria, acute kidney injury, acute renal failure, Plasmodium falciparum
(PTtnr
PfmeatpiularmittEri
pproximately 40% of the world’s popu-lation lives in regions where malariatransmission is endemic, mainly tropical
nd subtropical regions. About 300 to 400 mil-ion clinical cases of malaria are reported annu-lly,1 and mortality estimates range between 0.7nd 2.7 million. Most of these deaths are inoung children. In sub-Saharan Africa, wherealaria mortality is highest, 90% of reportedalaria-related deaths are children younger
han the age of 5. However, the actual figures ofllness, morbidity, and mortality may be veryifferent from those cited because of poor sur-eillance, misdiagnosis, and underreporting ofalarial deaths for various reasons. Malarial
eaths occur mostly at home and rarely areeported.2 Unfortunately, the disease burden isn the rise. By using a combination of epide-iologic, geographic, and demographic data,
now et al3 estimated that there were 515
Internal Medicine, Ispat General Hospital, Orissa, India.
Institute of Life Sciences, Indian Council of Medical Research, Bhua-baneswar, Orissa, India.
ddress reprint requests to Saroj K. Mishra, MD, Joint Director and Head ofInternal Medicine, Ispat General Hospital, Rourkela—769 005, Orissa, India.E-mail: [email protected]
270-9295/08/$ - see front matter
p2008 Elsevier Inc. All rights reserved. doi:10.1016/j.semnephrol.2008.04.007eminars in Nephrology, Vol 28, No 4, July 2008, pp 395-408
range, 300-600) million episodes of clinicallasmodium falciparum malaria in 2002.hese global estimates were up to 50% higher
han those reported by the World Health Orga-ization and 200% higher for areas outside Af-ica.
Malaria is caused by 4 species of the genuslasmodium, namely Plasmodium vivax, Palciparum, Plasmodium malariae, and Plas-
odium ovale. Malaria parasites (sporozoites)nter the circulation and subsequently the liverfter being bitten by an infective mosquito. Inhe liver sporozoites invade hepatocytes, multi-ly, and produce merozoites that are capable of
nvading the red blood cells. The hepatic cyclesually lasts for about a week. Merozoites re-
eased from hepatocytes enter the blood streamnd within a very short period invade the eryth-ocytes. Within the infected erythrocytes,erozoites consume host cell proteins, specif-
cally hemoglobin for their growth and mul-iplication. The parasite grows through ring,rophozoite, schizont, and merozoite stages.ventually the infected erythrocyte ruptures,eleasing an asexual form of merozoites, whichnvades fresh erythrocytes and the cycle is re-
eated. For appearance of clinical manifesta-395

trp(tmeccfiwilia
dohtoilaitstpcw
E
Tp3aaiMpsllpcitf
tpiaappAre
fmmmcefwbdsfewvpEpmtAtmorrNf6vsip1mvch
396 S.K. Mishra and B.S. Das
ions at least 3 to 4 such cycles are necessary toeach a critical level of parasitemia. A smallroportion of parasites grow to sexual formsgametocytes). Circulating gametocytes areaken up by the mosquitoes during their bloodeal. In the mosquito gut, gametocytes differ-
ntiate into male gametocytes (microgameto-ytes) and female gametocytes (macrogameto-ytes). Microgametes and macrogametes fuse toorm a zygote. Developing zygotes transformnto spindle-shaped ookinetes, cross the inner
all of the abdomen, and, finally, transformnto sporozoites. Thousands of sporozoitesodge in the salivary glands, ready to be injectednto human beings through the bite of a femalenopheles mosquito.
Common clinical characteristics of Plasmo-ia infection of all 4 species are periodic par-xysm, chills, rigors, sweating, body aches,eadache, nausea, general weakness, and pros-ration. Chronic anemia and splenomegaly arebserved in a majority of malaria patients resid-
ng in high malaria transmission areas. Severeife-threatening complications such as severenemia, cerebral malaria (CM), acute kidneynjury (AKI), acidosis, jaundice, respiratory dis-ress, acute respiratory distress syndrome, ando forth occur only with P falciparum infec-ion. However, recently a few reports have ap-eared indicating association of severe compli-ations of malaria with P vivax infection asell,4–6 including AKI.7,8
PIDEMIOLOGY
he contribution of malaria to the overall hos-ital admissions for AKI varies from 2% to9%9–11 in different populations. The wide vari-tion is because of its dependence on the agend antimalarial immunity, which in turn arenfluenced by malaria transmission intensity.
alarial AKI (MAKI) is considered a diseaseredominantly of adults and older children,11–13
pecifically in nonimmune adults from areas ofow intensity of malaria transmission. Thus, aarge number of reports on MAKI have ap-eared from southeast Asia and the Indian sub-ontinent where malaria transmission generallys low, with occasional microfoci of intenseransmission. The occurrence of AKI in patients
rom endemic areas with severe malaria is less ohan 1% to 4.8%, whereas in nonimmune Euro-eans it is 25% to 30%. The incidence of AKI
n severe P falciparum malaria is as commons cerebral malaria in nonimmune Europeandults.14 AKI was a frequent accompaniment inatients with severe falciparum malaria re-orted from Austria and The Netherlands.15,16
lmost all patients with fatal cases had AKI andeported a history of recent travel to malaria-ndemic areas.
Only a few reports of MAKI are availablerom Africa, particularly from areas with intensealaria transmission, where malaria affectsostly young children. In contrast to severealaria in adults, none of the 180 Gambian
hildren with severe malaria had AKI.17 How-ver, malaria transmission intensity is not uni-orm in Africa and a higher incidence of AKIith associated morbidity and mortality haseen reported in semi-immune African chil-ren.18 An earlier study from Ghana found mas-ive intravascular hemolysis; and black waterever was the most common cause of AKI. How-ver, only 1 patient had P falciparum malariahereas 26 patients had various bacterial and
iral infections.19 One third of severe malariaatients admitted to a University Hospital inthiopia had AKI, but the majority of theseatients were nonimmune visitors coming toalaria-endemic regions.20 Another study from
he Renal Unit of Tikur Anbessa Hospital inddis Ababa found 29 (21%) of 136 consecu-
ively treated adult AKI patients had falciparumalaria. The contribution of malaria to AKI was
nly second to septic abortion, and mortalityates in MAKI were as high as 37.9%.21 In aecent prospective study from 1994 to 2003 inigerian children, 123 cases of AKI caused by P
alciparum malaria were detected (mean age,.28 � 4.0 y).22 The occurrence of AKI in se-ere falciparum malaria is quite common inoutheast Asia, including India. A significantncrease in the incidence of AKI has been re-orted from several centers across India. In982 a study from Orissa indicated cerebralalaria as the predominant presentation of se-
ere malaria. Associated complications of 173ases of cerebral malaria were AKI (6%) andepatic failure (1%).23 Twenty years later, an-
ther study from the same area and the same
hfscirejtccStAmclhAtmcan
P
Tippirpfmcdatmhi
C
Tlovg
asrtdbnlscadtwAvpisbomtdAcstepg
CS
LtaapaltaipiTpl
Malaria and AKI 397
ospital showed 35% of cases with severe Palciparum malaria had AKI. There was a con-istent increase in incidence of AKI (from 95ases in 1994 to 215 cases in 1998).24 A highncidence of AKI in falciparum malaria has beeneported from eastern,25–27 western,28 north-rn,29 southern,30 and central India.31,32 The ma-ority of the studies had a common inferencehat the incidence of AKI and jaundice is in-reasing, and the development of multipleomplications result in increased mortality.33
tudies from Pakistan also reported MAKI con-ributing significantly to the total AKI burden.34
high incidence of AKI in severe P falciparumalaria was observed from southeast Asian
ountries. Hypercatabolic AKI was noted in Ma-aysia in patients with cerebral malaria witheavy parasitemia and hyperbilirubinemia.35
KI constituted 23.3% of severe malaria pa-ients hospitalized in Kampuchea. Coma andulti-organ failure were the most common
auses of death.36 A high incidence of MAKIlso has been reported from Singapore,37 Viet-am,38 and Thailand.39
ATHOPHYSIOLOGY
he pathogenesis of AKI in falciparum malarias not clearly known. Malarial complicationsossibly are caused by the interaction of thearasite with the host, resulting in mechanical,
mmunologic, and humoral responses. Theseesponses, while attempting to eliminate thearasites, may also injure the host tissues. Dif-
erent hypotheses proposed for MAKI includeechanical obstruction by infected erythro-
ytes, exaggerated host immune response me-iated through cytokines and reactive oxygennd nitrogen species, immune complex deposi-ion, hypovolemia, disturbances in the renalicrocirculation, and so forth. No explanation,owever, is available for the consistent increase
n the incidence of MAKI in some areas.
ytoadherence
he pathogenesis of severe P falciparum ma-aria is attributed in part to the cytoadherencef parasitized red blood cells (PRBCs) to theascular endothelial cells in different host or-
ans.40–42 Parasite proteins referred to as vari- tnt surface antigens expressed on the PRBCurface mediate the adhesion of infected eryth-ocytes to host vascular endothelial recep-ors.43,44 PRBCs preferentially sequester in theeep vascular beds of vital organs, including therain, liver, lung, spleen, intestine, and kid-ey.41,45 Sequestration of PRBCs in glomeru-
ar and tubulointerstitial capillaries has beenhown, although at a lesser degree than theerebral vessels.45 Studies on southeast Asiandults dying from severe falciparum malaria in-icated that the frequency of PRBC sequestra-ion in renal vessels of patients dying from AKIere significantly higher than those withoutKI. Significantly more PRBCs were seen inessels in malarial AKI patients than in non-AKIatients. However, the ultrastructural exam-
nation of renal microvascular sequestrationhowed much less PRBC sequestration than ofrain tissue of the same patients. The majorityf patients showed mononuclear cells in glo-erular and peritubular capillaries, although
he number of leukocytes was not significantlyifferent between the AKI group and the non-KI group.46,47 Margination of mononuclearells to the brain capillary endothelium washown earlier in a significant proportion of pa-ients.48 Thus, contribution of PRBC cytoadher-nce and clogging of the capillaries towardathogenesis of MAKI appears at best only mar-inal.
ytokines, Reactive Oxygenpecies, and Nitrogen Species
iterature on the influence of cytokine concen-rations on renal pathology in malaria is scantylthough cytokines, reactive oxygen intermedi-tes, and nitrogen intermediates (ROI and NO)lay an important role in both protectiongainst malaria and pathogenesis of severe ma-aria. Levels of inflammatory cytokines, such asumor necrosis factor � (TNF-�), interferon-�,nd interleukins 1-�, -6, and -8 are increasedn malaria.49 Higher blood concentrations ofroinflammatory cytokines have been observed
n severe complications of malaria.50–53 Anti–NF-� and anti–interferon-� antibodies are re-orted to abolish the onset of cerebral ma-
aria.54 However, in contrast to observations in
he murine model, monoclonal antibodies to
Tt
bmpshsmNhbsoaf(bctNitsimseoti
S
EscoScMCdatdlvPm
iftcbipop
csGdmstavbsmndadchtspecrcfasccpmmscamA
398 S.K. Mishra and B.S. Das
NF-� ameliorate fever but not the manifesta-ions of human cerebral malaria.55
Increased production of ROI and NO haveeen reported in malaria infection. The involve-ent of ROI and NO in the protection andathogenesis of malaria has been studied exten-ively. An early increase in NO stimulates theelper T-cell-1 (Th1) response to control para-itemia similar to natural immunization duringalaria infection,56 whereas a late increase inO production in the liver and spleen appear toave pathologic consequences.57 During thelood stage of malaria TNF-� up-regulates NOynthesis either alone or in combination withther cytokines.58 Regulatory functions of NOre dependent on the presence of various iso-orms of the enzyme nitric oxide synthaseNOS). Physiologic function of NO is regulatedy low basal concentrations synthesized byonstitutive NOS isoforms. A high concentra-ion of NO usually is produced by inducibleOS isoforms (iNOS), which play a crucial role
n pathologic consequences. Increased iNOS ac-ivity and production of NO have been ob-erved in severe malaria.57 Lipopolysaccharides reported to be a potent stimulator of iNOS
essenger RNA.59 Similarly, ROI also plays aignificant role in the protection and pathogen-sis of malaria.60,61 Higher blood concentrationsf ROI and a depleted antioxidant defense sys-em have been observed in patients with malar-a.62–64
epsis Model for MAKI
xtensive parallels exist between sepsis andevere malaria in the clinical presentation andytokine profile, indicating that the 2 diseasesperate through very similar mechanisms.65
hock and multi-organ failure, a common asso-iation in sepsis, frequently are observed inAKI as well66 (Mishra et al, unpublished data).ontrary to the common belief that respiratoryistress complicating severe malarial anemia isconsequence of biventricular failure, observa-
ions from the clinical picture in African chil-ren indicate characteristic features of hypovo-
emia67 and the administration of albumin forolume expansion reduces mortality rates.68
lasma concentrations of several small- and
iddle-molecular-weight proteins are reduced tn severe malaria because of extravasationsrom the vascular compartment to the intersti-ial space.69,70 Arterial vasodilatation that ac-ompanies sepsis is mediated, at least in part,y cytokines that up-regulate the expression of
NOS in vasculature.71 NO thus released has aotent vasodilatory effect.72 However, severalther studies did not notice severe volume de-letion or hypotension in severe malaria.73,74
Restricted local blood flow in the kidneys isonsidered a major contributor for MAKI. Aimilar pathology is observed in AKI of sepsis.eneralized vasodilatation with an associatedecrease in systemic vascular resistance is theost important hemodynamic abnormality ob-
erved in sepsis. Vasodilatation leads to activa-ion of the sympathetic nervous system, rennin-ngiotensin-aldosterone axis, and release ofasopressin for maintaining the decreasinglood pressure. Unfortunately, these compen-atory mechanisms predispose to AKI.75,76 Si-ultaneously, the vasoconstriction effects of
orepinephrine and angiotensin II are depen-ent on open calcium channels, which are notvailable when associated with increased hy-rogen ion and lactic acid concentrations. In-reased plasma concentrations of lactate andydrogen ions, and a decrease in adenosineriphosphate (ATP) generation in vascularmooth muscle cells, activate the ATP-sensitiveotassium channels,77,78 resulting in potassiumfflux and closure of the voltage gated calciumhannels in the membrane. Therefore, vascularesistance to these pressor hormones occurs inonditions of lactic acidosis. Hypoxia in severealciparum malaria is brought about possibly by
combination of volume depletion, hypoten-ion, pulmonary edema, and clogging of theapillaries by cytoadhered PRBCs and mononu-lear cells, resulting in lactic acidosis. Cyto-athic hypoxia caused by inflammation-induceditochondrial dysfunction is now considered aajor contributor to the pathogenesis of sep-
is.79 Proinflammatory cytokines, higher con-entrations of which are present in both sepsisnd malaria,51,52 are considered responsible foritochondrial shutdown, leading to reducedTP synthesis and increased lactate accumula-
ion. Hyperlactatemia is considered a marker

fm
oAvNoadPtmiem
H
Tvtmaiseht
uuaomg
otadi
enesis
F
Malaria and AKI 399
or poor prognosis in sepsis,80 as well as inalaria.81,82
MAKI can occur as an isolated complicationr as a component of multi-organ involvement.low intake of fluids, loss of fluids because of
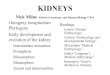
omiting and pyrexial sweating, cytokine- andO-mediated arterial vasodilatation, specificallyrgan-specific release of NO, resistance to vaso-ctive hormones, cytopathic hypoxia leading toecreased ATP synthesis, and cytoadherence ofRBCs all may contribute singly or in combina-ion toward MAKI (Fig. 1). Increased fluid ad-inistration, oxygen toxicity, and as yet un-
dentified factors may contribute to pulmonarydema, acute respiratory distress syndrome,ulti-organ failure, and death.
istology
he histopathology of MAKI is a combination ofarious pathogenetic mechanisms such as acuteubular necrosis, interstitial nephritis, and glo-erulonephritis. However, tubular changes
re the most common and consistent find-ngs.11,12,83 Tubular changes include cell necro-is, tubular swelling, and deposits of hemosid-rin granules. The tubular lumens often containemoglobin casts. Acute interstitial inflamma-
Figure 1. Pathog
ion is associated commonly with acute glomer- d
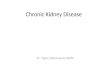
losclerosis. In glomerulonephritis, the glomer-li are swollen with expansion of the mesangialrea and proliferation of mesangial cells. Peri-dic acid-Schiff staining reveals widening of theesangial stalk and irregular thickening of the
lomerular basement membrane (Fig. 2).In a recent report on an ultrastructural study
f renal pathology in fatal falciparum malaria,here was sequestration of PRBCs in glomerularnd tubulointerstitial vessels, and acute tubularamage. However, there was no evidence of
mmunomediated glomerulonephritis. There
of AKI in malaria.
igure 2. Kidney biopsy from an Indian adult male who
ied from cerebral malaria with acute renal failure.
wm
C
Mp4ma0c5roctOlLd1ampp
dhdcmh3iwO
atcub
a(
oirc
chhai
ahwtteippedaPmoa
disgufbdbb
adptwtom
ihyvr
400 S.K. Mishra and B.S. Das
as mild glomerular hypercellularity with hostonocytes in the glomerular capillaries.47
LINICAL PRESENTATION
alaria-related AKI invariably is caused by falci-arum malaria. It is defined as an abrupt (within8 hours) reduction in kidney function thatay be characterized by the following: (1) an
bsolute increase in serum creatinine level of.3 mg/dL or more (�26.4 �mol/L), (2) a per-entage increase in serum creatinine level of0% or more (1.5-fold from baseline), or (3) aeduction in urine output (documented oliguriaf �0.5 mL/kg/h for �6 hours). However, toategorize a patient as having severe malaria onhe basis of renal function as per World Healthrganization criteria,11 the serum creatinine
evel has to be 3 mg/dL or more (�265 �mol/). It is common in adults, and rare in chil-ren.11–13 In a study from Orissa consisting of,857 patients, although both children anddults were vulnerable for severe malaria, al-ost all the MAKI cases were observed in adultatients.26 It is encountered more often in maleatients than in female patients.26,34
The incidence ranges from 0.5% to 15% inifferent series because it depends on the co-ort of patients and the criteria used for theefinition of MAKI. Malaria may be a majorause of renal failure in a hospital, although itay be encountered occasionally in anotherospital. In a study of 500 adults in Vietnam,0% of the patients had MAKI, with a higher
ncidence of jaundice and hypoglycemia,11
hereas the incidence was 4% in a series fromrissa (India).26
A history of recent travel to malaria-endemicreas must always be sought. Although some ofhe complications can be identified easily onlinical examination, recognition of renal fail-re needs a high index of suspicion and earlyiochemical investigations.
MAKI may present in 2 different ways: (1) ascomponent of multi-organ dysfunction, and
2) as AKI alone.When MAKI is a part of multi-organ failure, it
ften is present at the time of presentation andnvariably carries a poor prognosis. It has beeneported that about a third of patients with
erebral malaria have renal impairment (serum sreatinine level, �2 mg/dL).15 These patientsave a higher incidence of anemia, jaundice,ypoglycemia, and prolonged coma. Acidosisppears early and may be associated with cloud-ng of sensorium, convulsions, and coma.
In the other subset, renal impairment occurss a sole complication. This group of patientsas a better prognosis. It invariably occurshen other complications have subsided, and
he patient is fully conscious, oriented, and of-en afebrile. These patients develop oliguria,ncephalopathy, hyperkalemia, and signs of ac-dosis. It has to be noted that this group ofatients is encountered at a time when thearasites are no longer present in the periph-ral blood, making it difficult to establish theiagnosis of malaria. A high index of suspicionnd the use of a dipstick method for detecting
falciparum (eg, rapid diagnostic kits, im-uno-chromatographic test [ICT], and so forth)
r other alternative diagnostic tools are of par-mount importance.
Urine output usually is decreased (�400 mL/).11 Although Prakash et al32 observed oliguria
n 70% of patients in India, Manan et al34 ob-erved it in 76% of patients from Pakistan. Oli-uria usually persists for 3 to 10 days. However,rine output may be normal or increased in aew patients. Hence, oliguria alone should note relied on for a diagnosis of AKI in malaria. Aaily estimation of biochemical tests such aslood urea nitrogen and creatinine levels muste performed.
The complications usually appear 3 to 7 daysfter onset of the fever, and may last for a feways to several weeks. Patients with peripheralarasitemia should be screened regularly forhe presence of renal failure. In a clinical settingith a high index of suspicion of malaria, pa-
ients even without peripheral parasitemia orliguria should be screened for renal impair-ent.Of 402 detected smear-positive malaria cases
n a hospital from Mumbai, Western India, 24ad malarial AKI. Eighteen were age 21 to 40ears. P falciparum was detected in 16, Pivax in 3, and mixed infection in 5. Nonoligu-ic AKI was seen in 14 patients (58%).28
Dehydration, volume depletion, hypoten-
ion, and shock also are encountered. Volume
dptrlsoiaspuas
A
CCbsC�haIccdmo
JJMwmbihsMttd
AAill
cttots
bppHcs
E
Ap6hormtmamrpc
omkmthcpicco
tahi
Malaria and AKI 401
epletion was detected in more than half of theatients and hypotension was detected in ahird of the patients.32 Hypotension occurs as aesult of several factors: low intake of fluids,oss of fluids because of vomiting and pyrexialweating, arterial vasodilatation, and the effectf cytokines. Peripheral blood pooling has been
mplicated in a number of cases. The effectiverterial blood volume is reduced, and hypoten-ion occurs on presentation. Few patients mayresent with shock syndrome (Mishra et al,npublished data). These patients need urgentttention for fluid replenishment including va-opressin (vide supra).
ssociated Complications
erebral malariaerebral malaria often is associated with AKI,ut frank renal failure occurs in about 30%. In aeries from Thailand, 30% of adult patients withM had associated AKI (serum creatinine level,2 mg/dL [2 mg%]). These patients had a
igher incidence of jaundice, hypoglycemia,nd pulmonary edema.84 A large series fromndia reported the incidence as 29% amongerebral malaria patients versus 4% among non-erebral malaria patients.85 An important pre-ictor in the survival of patients with cerebralalaria is the presence of MAKI. The presence
f AKI in CM makes the prognosis worse.86
aundiceaundice is an invariable accompaniment inAKI. It occurs in more than half of patientsith renal failure.11,87 Conversely, renal impair-ent is observed in 10% of patients with hyper-
ilirubinemia. The hyperbilirubinemia predom-nantly is unconjugated in nature owing toemolysis.11,27 However, a few reports de-cribed the presence of malaria hepatitis withAKI. It is important to be aware of the simul-
aneous presence of renal and hepatic dysfunc-ion in certain situations, namely, leptospirosis,engue, hepatorenal syndrome, and so forth.
nemialthough anemia (hemoglobin level �10 g/dL)
s associated in about 60% of patients with ma-arial renal failure, severe anemia (hemoglobin
evel, �5 g/dL) is reported in 10% to 20% of fases. Thrombocytopenia occurs in 70% of pa-ients, half of whom develop an overt bleedingendency. In the majority of patients, this is partf a disseminated intravascular coagulation ini-iated by the gross rheologic abnormality inevere malaria.
Proteinuria usually is insignificant, but it maye as high as 1 g/24 h in about a third ofatients with MAKI. It usually resolves com-letely with recovery from renal impairment.owever, persistent proteinuria may be en-ountered in the presence of significant inter-titial or glomerular involvement.10,12
lectrolyte abnormality
n electrolyte imbalance occurs invariably in allatients. Hyponatremia is reported in 25% to0% of patients.12,32,34 The mechanisms includeemodilution and sodium wasting before thenset of oliguria. However, an increase of se-um antidiuretic hormone is unlikely to play aajor role.10,12 Hyperkalemia is the most impor-
ant electrolytic parameter for renal replace-ent therapy. However, the incidence is as low
s 4%.34 But unless it is identified and promptlyanaged it may be fatal. Hyperkalemia also may
esult from hemolysis and rhabdomyolysis. Hy-okalemia also has been encountered. Electro-ardiographic recordings are often helpful.
The serum calcium level often is reduced outf proportion to phosphate retention, whichay be owing to hypoparathyroidism of un-
nown cause.88 Lactic acidosis has been docu-ented and is a life-threatening condition, of-
en among children. As described before,ypoxia in severe malaria is multifactorial: aombination of volume depletion, hypotension,ulmonary edema, and clogging of the capillar-
es by cytoadhered PRBCs and mononuclearells, resulting in lactic acidosis. High blood orerebrospinal fluid lactate levels are predictorsf poor outcome.81,82
The vulnerable groups to develop M AKI arehe following patients: pregnant, with high par-sitemia, deeply jaundiced, with prolonged de-ydration, and those receiving nonsteroidal anti-
nflammatory drugs.The critical determinants for MAKI are as
ollows: hypovolemia and hypervolemia, hyper-

pb
P
RddIofspaphahrfeaf3
ltsemmat
rfgcmsCetosbp
T
Tm
Et
ttliti
cfcodpaa
A
TnhThlcabiimyrsoTctclebQtHas
402 S.K. Mishra and B.S. Das
arasitemia, hemoconcentration, hyperbiliru-inemia, and hyperpyrexia.
ROGNOSIS
enal failure associated with malaria resolves inays to weeks, and almost always completely. Itoes not progress into chronic kidney disease.t is not associated with hypertension. Theverall mortality rate among those with renalailure ranges from 15% to 50% in differenteries.11,20,34,89–93 Similarly, the simultaneousresence of MAKI in cerebral malaria is associ-ted with a poor prognosis.86 In a study of 110atients with cerebral malaria from India, 38ad evidence of AKI. Associated complicationss well as mortality rates were significantlyigher in the presence of AKI. The mortalityate of patients with cerebral malaria increasedrom 14% to 40% in the presence of AKI. Forach 1 log unit increase of serum creatinine atdmission, the odds of death increased by aactor of 10.8 (95% confidence interval, 3.0-9.4).86
The survival rate with peritoneal dialysis wasower than that of hemodialysis or hemofiltra-ion.94 At Rourkela, the mortality rate decreasedignificantly when hemodialysis was initiatedarly. It is pertinent to mention that AKI inalaria needs urgent recognition and manage-ent. Multiple complications need urgent man-
gement in a tertiary care hospital with a mul-idisciplinary approach.89
Several risk factors had been proposed to beesponsible for the high mortality rate: late re-erral, short acute illness, high parasitemia, oli-uria, hypotension, severe anemia, or signifi-ant jaundice. Patients with severe diarrhea,ultisystem involvement, hepatitis, or acute re-
piratory distress also have a poor prognosis.o-existing viral or bacterial infections may bencountered in patients with MAKI, increasinghe risk of mortality. The presence of multi-rgan failures results in a poor prognosis. Aimple bedside survival scoring system haseen devised that gives relative weighted im-ortance to each complication.95
REATMENT
he management of MAKI needs careful and
eticulous management of several problems. harly and prompt decisions and institutions arehe hallmark of a better prognosis.
The outlines of treatment guidelines includehe following: (1) institution of appropriate an-imalarials, (2) maintenance of fluid and electro-yte levels, (3) renal replacement therapy asndicated, (4) treatment of associated complica-ions, and (5) management of infection includ-ng pneumonia.
Drugs to be avoided in malaria patients be-ause they may impair renal function are asollows: nephrotoxic drugs such as aminogly-osides should be avoided if AKI is suspectedr anticipated, nonsteroidal anti-inflammatoryrugs should not be given because they mayrecipitate prerenal azotemia to ischemic AKI,nd angiotensin-converting enzyme inhibitorsnd cyclooxygenase inhibitors.
ntimalaria Drugs
he preferred antimalarial is artesunate or qui-ine given parenterally. Intravenous quinineas remained as the time-tested first-line drug.he dose is 10 mg/kg/body weight. If quinineas not been given in the previous 7 days, a
oading dose may be given. But it is very diffi-ult to get a definite history, hence it is advis-ble to start a maintenance dose of 10 mg/kg ofody weight every 8 hours. The dose for the
nitial 48 hours should never be modified, evenn the presence of AKI. If quinine needs to be ad-inistered only through a parenteral route be-
ond 48 hours, the dose of quinine must beeduced to two thirds. Oral therapy should betarted as soon as the patient is able to accept itrally. The total duration of therapy is 7 days.he common side effects include dizziness, cin-honism, and hypoglycemia.11,96,97 Careful at-ention needs to be given to the rate of infusion,ardiac monitoring, and prevention of fluid over-oad. Prolonged QT interval, atrial or ventricularctopic beats, heart block and hypotension maye anticipated in patients treated with quinine.uinine is metabolized and 80% is excreted
hrough the liver and 20% through the kidneys.owever, estimation of blood level is not readilyvailable in most centers and careful clinical as-essment at frequent intervals is mandatory.11
The introduction of artemisinin derivatives
as improved the survival rates of patients with
sseidntmt
oaalosl
iqhiviautfll
it
F
MT0fljpfstmb
D
Tan
tmoubhpsutcaifn(10.wurdiihrnds
ptatpocdtrtf6apsps
Malaria and AKI 403
evere malaria.98–100 These drugs clear para-itemia rapidly and are practically devoid of sideffects.98,101 In addition, no dosage modifications needed in the presence of renal or hepaticysfunction. The preferred molecule is artesu-ate because it can be given intravenously. In-ravenous artesunate is given at a dose of 2g/kg/body weight at 0, 12, and 24 hours, and
hen once daily for a total of 7 days.The use of other drugs, namely chloroquine
r sulfadoxine pyrimethamine, should bevoided owing to widespread resistance fromreas where CM and AKI are common. Simi-arly, there are scant data to recommend the usef mefloquine or halofantrine. These oral drugshould not be used in patients with severe ma-aria.
Fluid and electrolyte therapy are of utmostmportance: a meticulous record of fluid re-uirement and urinary output is needed. Itelps to guide the administration of fluid, mon-
toring the improvement, and, most of all, pre-enting fluid overload. This simple but mostmportant factor is overlooked at small, busy,nd overcrowded hospitals. It often is left to theninformed attendants/relatives of the patient,hus getting erroneous information. To preventuid overload a central venous pressure (CVP)
ine can be established.The identification and treatment of co-exist-
ng or acquired infection should be managed athe earliest.
luid Challenge
any patients with oligura are dehydrated.hey should receive fluid, up to 20 mL/kg of.9% saline infused over 60 minutes. To preventuid overload, auscultation of the lungs and
ugular venous pressure measurements (and, ifossible, CVP measurements) should be per-
ormed after every 200 mL of fluid. The CVPhould always be kept between 0 and �5. Ifhere is no urine output after fluid replace-ent, an intravenous diuretic challenge may
e given.11
iuretic Challenge
he loop diuretic (frusemide 40 mg or bumet-nide 1 mg) is given initially. If urination does
ot occur, further diuretic challenge can be sried at every 30-minute intervals with incre-ental doses (frusemide 100, 200, and 400 mg
r bumetanide 2, 4, and 6 mg). If there is still norine flow, dopamine 2.5 to 5 �g/kg/min maye tried. However, the use of diuretics in MAKIas not improved the outcome. Rather, it ap-ears to be ineffective in oliguric patients. In amall number of patients it may increase therine output, but no improvement occurs inhe renal status. Rather, it may give a sense ofomplacency. A systematic review and meta-nalysis was conducted to evaluate loop diuret-cs in the management of AKI in 555 patientsrom 5 randomized controlled trials. There waso statistical difference in the mortality ratesodds ratio, 1.28; 95% confidence interval, 0.89-.84; P � .18) or renal recovery (odds ratio,.88; 95% confidence interval, 0.59-1.31; P �5) with the use of loop diuretics compared
ith controls.102 However, the use of loop di-retics may result in a shorter duration of renaleplacement therapy and a shorter time for theecline in serum creatinine level. It causes an
ncrease in urine output. There was, however,nsufficient data on acid-base status, length ofospital stay, and treatment costs. Four studieseported toxicity, most commonly transient tin-itus and deafness. It was suggested that loopiuretics were not associated with improvedurvival.102
In a prospective, randomized, double-blind,lacebo-controlled, multicenter trial, 338 pa-ients with AKI requiring dialysis therapy weredministered either furosemide (25 mg/kg/d in-ravenously or 35 mg/kg/d orally) or matchedlacebo. The end points were survival, numberf dialysis sessions, and time to achieve a serumreatinine level of less than 200 �mol/L andieresis (urine, �2 L/d). It was observed thathere were no differences in survival and renalecovery rates between the 2 groups. The timeo achieve a 2-L/d diuresis was shorter withurosemide (5.7 � 5.8 d) than placebo (7.8 �.8 d; P � .004). Overall, 148 patients achievedurine output of at least 2 L/d during the studyeriod (94 of 166 patients; 57%) with furo-emide versus 54 of 164 patients (33%) withlacebo (P � .001). However, there were noignificant differences in the number of dialysis
essions and the time on dialysis therapy be-
twtse
D
TtIlipioltodavba3tRccNaTdm
V
AttMlt
A
Tpthja
D
Dtt(hmmdc
(sedak
wsessaaiapcaoMccim
A
Dd5
AStiha
404 S.K. Mishra and B.S. Das
ween the furosemide and placebo groups. So itas reported that high-dose furosemide main-
ains urinary output, but does not influenceurvival or renal recovery rates of patients withstablished renal impairment.103
opamine Challenge
he use of dopamine for the prevention andreatment of AKI has not yet been established.ts use is based on the understanding that se-ective renal vasodilatation will occur when it isnfused at a low dose. A recent article com-ared the effects of dopamine and epinephrine
n various doses on renal hemodynamic andxygen transport in patients with severe ma-
aria and severe sepsis. In a prospective, con-rolled, cross-over trial in an intensive care unitf an infectious diseases hospital in Vietnam,opamine at a renal dose (2.5 �g/kg/min) wasssociated with a mean (95% confidence inter-al) fractional increase in the absolute renallood flow (RBF) index of 37% (13% to 61%)nd in RBF as a fraction of cardiac output of5% (10%-59%; P � .007 and P � .014, respec-ively). At higher doses (10 �g/kg/min), bothBF and RBF/cardiac output were not signifi-antly different from baseline values and de-reased further as the dose was reduced again.either epinephrine nor dopamine significantly
ffected creatinine clearance or urine output.here was no evidence that either drug pro-uced any beneficial effect on renal oxygenetabolism or function.104
asopressin Therapy
s discussed in the pathogenesis, there appearso be a future role for the use of vasopressin inhe management of malarial shock as well asAKI. However, sufficient data need to be col-
ected before this agent is accepted to improvehe survival.
lbumin Infusion
he administration of albumin for volume ex-ansion reduces mortality rates.68 Exchangeransfusion is of use in patients with severeemolysis. However, in the presence of severe
aundice and renal failure, no data are avail-
ble to recommend its use. uialysis
ialysis has improved the survival rates of pa-ients when instituted early in the course ofreatment. It can be intermittent hemodialysisdaily or alternate day), continuous venovenousemofiltration, or continuous arteriovenous he-ofiltration. The latter methods cause less he-odynamic instability than conventional hemo-
ialysis. Peritoneal dialysis is less effective inontrolling biochemical abnormalities.
Indications for dialysis include the following:1) clinical indications: uremic symptoms,ymptomatic volume overload (eg, pulmonarydema, congestive heart failure), and pericar-ial rub; (2) laboratory indications: severe met-bolic acidosis (HCO3 � 15 mEq/L) and hyper-alemia (K� � 6.5 mEq/L).
The clearance of urea and other molecularaste products is much faster with hemodialy-
is as compared with peritoneal dialysis. How-ver, peritoneal dialysis has certain advantagesuch as: peritoneal dialysis does not need apecial set-up, it can be started immediately,nd it may prove to be life-saving. Thus, in thebsence of facilities for hemodialysis wheneverndicated, peritoneal dialysis should be starteds early as possible. Conservative treatment inatients with AKI with severe malaria needsareful monitoring. A patient may develop signss mentioned earlier and at any odd hours with-ut giving a scope for initiation of dialysis.any lives have been lost as dialysis was de-
ided but institution was delayed. Suddenardiac death may ensue in a patient who ismproving owing to the development of pul-
onary edema or hyperkalemia.
dequacy of Dialysis
ialysis is considered adequate when the post-ialysis creatinine and urea levels decrease to0% or less of the predialysis values.
ntimalarial Drugs During Dialysisignificant changes in plasma quinine concen-rations do not occur in patients with AKI dur-ng hemodialysis. Quinine was not detectable inemodialysate fluids. This suggests that dosagedjustment of quinine during hemodialysis is
nnecessary. There are no data as yet available
fi
MTftac
NOpsp
th
ATP(a(
R
Malaria and AKI 405
or the artemisinin drugs for modification dur-ng dialysis.
anagement of the Diuretic Phasehe diuretic phase may return gradually or in a
ew hours. Careful attention needs to be givenoward fluid and electrolyte requirements. Inddition, repeated estimation of Na, K, and bi-arbonate is essential.
utritionne must not overlook the nutrition aspect ofatients with AKI. Attempts should be made touppress endogenous protein catabolism byroviding fat and carbohydrates.In patients without dialysis, protein restric-
ion is advised, whereas those undergoing dailyemodialysis may require additional proteins.
cknowledgmenthe authors express their sincere thanks to Dr. J. K.attnaik of Community Welfare Society HospitalRourkela), for important inputs on histopathology,nd to Dr. S. Mohanty of Ispat General HospitalRourkela) for his valuable interactions.
EFERENCES1. World Health Organization. The world health report
1999; making a difference. World Health Organiza-tion, Geneva, Switzerland, 1999.
2. Greenwood B, Mutabingwa T. Malaria in 2002. Na-ture. 2002;415:670-2.
3. Snow RW, Guerra CA, Noor AM, Myint HY, Hay SI.The global distribution of clinical episodes of Plas-modium falciparum malaria. Nature. 2005;434:214-7.
4. Kochar DK, Saxena V, Singh N, Kochar SK, KumarSV, Das A. Plasmodium vivax malaria. Emerg InfectDis, 2005 Jan [accessed on 22 Feb 2008]. Availablefrom: http://www.cdc.gov/ncidod/EID/vol11no01/04-0519.htm.
5. Kumar S, Melzer M, Dodds P, Watson J, Ord R. P.vivax malaria complicated by shock and ARDS.Scand J Infect Dis. 2007;39:255-6.
6. Ozen M, Gungor S, Atambay M, Daldal N. Cerebralmalaria owing to Plasmodium vivax: case report.Ann Trop Paediatr. 2006;26:141-4.
7. Prakash J, Singh AK, Kumar NS, Saxena RK. Acuterenal failure in Plasmodium vivax malaria. J AssocPhysicians India. 2003;51:265-7.
8. Kaur D, Wasir V, Gulati S, Bagga A. Unusual presen-tation of Plasmodium vivax malaria with severethrombocytopenia and acute renal failure. J Trop
Pediatr. 2007;53:210-2.9. Sitprija V. Nephropathy in falciparum malaria. Kid-ney Int. 1988;34:867-77.
10. Barsoum R, Sitprija V. Tropical nephrology. In:Schrier RW, Gottaschalk CW, editors. Diseases ofthe kidney. 6th ed. Boston: Little Brown & Co; 1996.p. 2221-68.
11. WHO. Severe falciparum malaria. Trans R Soc TropMed Hyg. 2000;94 Suppl 1:s1-90.
12. Barsoum RS. Malaria acute renal failure. J Am SocNephrol. 2000;11:2147-54.
13. Eiam-Ong S. Malaria nephropathy. Semin Nephrol.2003;23:21-33.
14. Weber MW, Böker K, Horstmann RD, Ehrich JH.Renal failure is a common complication in non-immune Europeans with Plasmodium falciparummalaria. Trop Med Parasitol. 1991;42:115-8.
15. Losert H, Schmid K, Wilfing A, Winkler S, StaudingerT, Kletzmayr J, et al. Experiences with severe P.falciparum malaria in the intensive care unit. Inten-sive Care Med. 2000;26:195-201.
16. Gerritsen JG, van der Zwan JC. Acute renal failure insevere chloroquine resistant falciparum malaria. In-tensive Care Med. 1992;18:177-9.
17. Waller D, Krishna S, Crawley J, Miller K, Nosten F,Chapman D, et al. Clinical features and outcome ofsevere malaria in Gambian children. Clin Infect Dis.1995;21:577-87.
18. Ehrich JH, Eke FU. Malaria-induced renal damage:facts and myths. Pediatr Nephrol. 2007;22:626-37.
19. Adu D, Anim-Addo Y, Foli AK, Yeboah ED, QuarteyJKM, Ribeiro BF. Acute renal failure in tropical Af-rica. BMJ. 1976;1:890-2.
20. Habte B. Acute renal failure due to falciparum ma-laria. Ren Fail. 1990;12:15-9.
21. Zewdu W. Acute renal failure in Addis Abeba, Ethi-opia: a prospective study of 136 patients. EthiopMed J. 1994;32:79-87.
22. Wasiu AO, Kayode AA. Pediatric acute renal failurein southwestern Nigeria. Kidney Int. 2004;66:1541-8.
23. Dash RK, Mishra K, Mishra SS, Pandey RS, MohantySC, Sahu H, et al. Cerebral malaria: report of 173patients. J Assoc Physicians India. 1982;30:724A.
24. Panda SK, Das MC, Meher LK, Rathod PK. Riskfactors for acute renal failure in severe falciparummalaria. Indian J Nephrol. 2003;13:55-8.
25. Prakash J, Tripathi K, Malhotra V, Kumar O, Srivas-tava PK. Acute renal failure in eastern India. NephrolDial Transplant. 1995;10:2009-12.
26. Mohanty S, Mishra SK, Pati SS, Pattnaik J, Das BS.Complications and mortality patterns due to Plasmo-dium falciparum malaria in hospitalized adults andchildren, Rourkela, Orissa, India. Trans R Soc TropMed Hyg. 2003;97:69-70.
27. Pati SS, Mishra SK, Mohanty S, Patnaik JK, Das BS.Influence of renal impairment on plasma concentra-tions of conjugated bilirubin in cases of Plasmodiumfalciparum malaria. Ann Trop Med Parasitol. 2003;
97:581-6.
406 S.K. Mishra and B.S. Das
28. Mehta KS, Halankar AR, Makwana PD, Torane PP,Satija PS, Shah VB. Severe acute renal failure inmalaria. J Postgrad Med. 2001;47:24-6.
29. Nitya Nand, Aggarwal H, Sharma M, Singh M. Sys-temic manifestations of malaria. J Indian Acad ClinMed. 2001;2:189-94.
30. Murthy GL, Sahay RK, Srinivasan VR, Upadhaya AC,Shantaram V, Gayatri K. Clinical profile of falcipa-rum malaria in a tertiary care hospital. J Indian MedAssoc. 2000;98:160-2.
31. Dash SC, Bhuyan UN, Gupta A, Sharma LC, Kumar A,Agarwal SK. Falciparum malaria complicating chole-static jaundice and acute renal failure. J Assoc Phy-sicians India. 1994;42:101-2.
32. Prakash J, Gupta A, Kumar O, Rout SB, Malhotra V,Srivastava PK. Acute renal failure in falciparum ma-laria—increasing prevalence in some areas of In-dia—a need for awareness. Nephrol Dial Transplant.1996;11:2414-6.
33. Krishnan A, Karnad DR. Severe falciparum malaria:an important cause of multiple organ failure in In-dian intensive care unit patients. Crit Care Med.2003;31:2278-84.
34. Manan AJ, Ali H, Lal M. Acute renal failure associatedwith malaria. J Ayub Med Coll Abbottabad. 2006;18:47-52.
35. Segasothy M, Swaminathan M, Kong NC. Acute renalfailure in falciparum malaria. Med J Malaysia. 1994;49:412-5.
36. Bouth DM, Giboda M. Malaria in Kampuchea: clini-cal course of falciparum malaria in Chemin de FerHospital, Phnom Penh. Folia Parasitol (Praha). 1987;34:11-8.
37. Zinna S, Vathsala A, Woo KT. A case series of falci-parum malaria-induced acute renal failure. Ann AcadMed Singapore. 1999;28:578-82.
38. Trang TT, Phu NH, Vinh H, Hien TT, Cuong BM,Chau TT, et al. Acute renal failure in patients withsevere falciparum malaria. Clin Infect Dis. 1992;15:874-80.
39. Nacher M, Treeprasertsuk S, Singhasivanon P,Silachamroon U, Vannaphan S, Gay F, et al. Associ-ation of hepatomegaly and jaundice with acute renalfailure but not with cerebral malaria in severe falci-parum malaria in Thailand. Am J Trop Med Hyg.2001;65:828-33.
40. Kyes S, Horrocks P, Newbold C. Antigenic variationat the infected red cell surface in malaria. Ann RevMicrobiol. 2001;55:673-707.
41. Pongponratan E, Riganti M, Punpoowong B, AikawaM. Microvascular sequestration of parasitized eryth-rocytes in human falciparum malaria: a pathologicalstudy. Am J Trop Med Hyg. 1991;44:168-75.
42. Turner GDH, Morrison H, Jones M, Davies TM, Looa-reesuwan S, Buley ID, et al. An immunohistochemi-cal study of the pathology of fatal malaria: evidencefor widespread endothelial activation and a potentialrole for intercellular adhesion molecule-1 in cerebral
sequestration. Am J Pathol. 1994;145:1057-69.43. Baruch DI, Pasloske BL, Singh HB, Xiahui B, Ma XC,Feldman M, et al. Cloning of the P. falciparum geneencoding PfEMP 1, a malarial variant antigen andadherence receptor on the surface of parasitizedhuman erythrocyte. Cell. 1995;82:77-87.
44. Magowan C, Wollish W, Anderson L, Leech J. 1988.Cytoadherence by Plasmodium falciparum in-fected erythrocytes is correlated with the expres-sion of a family of variable proteins on infectederythrocytes. J Exp Med. 1988;168:1307-20.
45. MacPherson GG, Warrell MJ, White NJ, Looareesu-wan S, Warrell DA. Human cerebral malaria: a quan-titative ultrastructural analysis of parasitized erythro-cyte sequestration. Am J Pathol. 1985;119:385-401.
46. Pongponratn E, Turner GD, Day NP, et al. An ultra-structure study of the brain in fatal Plasmodiumfalciparum malaria. Am J Trop Med Hyg. 2003;69:345-59.
47. Nguansangiam S, Day NPJ, Hien TT, Mai NTH,Chaisri U, Riganti M. A quantitative ultrastructuralstudy of renal pathology in fatal Plasmodium fal-ciparum malaria. Trop Med Int Health. 2007;12:1037-50.
48. Patnaik JK, Das BS, Mishra SK, Mohanty S, SatpathySK, Mohanty D. Vascular clogging, mononuclear cellmargination, and enhanced vascular permeability inthe pathogenesis of human cerebral malaria. Am JTrop Med Hyg. 1994;51:642-7.
49. Mshana RN, Boulandi J, Mshana NM, Mayombo J,Mendome G. Cytokines in the pathogenesis of ma-laria: levels of IL-1�, IL-4, IL-6, TNF-�, and IFN-� inplasma of healthy individuals and malaria patients ina holoendemic area. J Clin Lab Immunol. 1991;34:131-9.
50. Day NP, Hien TT, Schollaardt T, Loc PP, Chuong LV,Chau TT, et al. The prognostic and pathophysiologicrole of pro- and anti-inflammatory cytokines in se-vere malaria. J Infect Dis. 1999;180:1288-97.
51. Kern P, Hemmer CJ, Van Damme J, Gruss HJ, Di-etrich M. Elevated tumor necrosis factor alpha andinterleukin-6 serum levels as markers for compli-cated Plasmodium falciparum malaria. Am J Med.1989;87:139-43.
52. Kwiatkowski D, Hill AV, Sambou I, Twumasi P, Cas-tracane J, Manogue KR, et al. TNF concentration infatal cerebral, non-fatal cerebral, and uncomplicatedPlasmodium falciparum malaria. Lancet. 1990;336:1201-4.
53. Wenisch C, Linnau KF, Looareesuwan S, RumpoldH. Plasma levels of the interleukin-6 cytokine familyin persons with severe Plasmodium falciparummalaria. J Infect Dis. 1999;179:747-50.
54. Grau GE, Heremans H, Piguet PF, Pointaire P, Lam-bert PH, Billiau A, et al. Monoclonal antibody againstinterferon gamma can prevent experimental cere-bral malaria and its associated overproduction oftumor necrosis factor. Proc Natl Acad Sci U S A.1989;86:5572-4.
55. Kwiatkowski D, Molyneux ME, Stephens S, Curtis N,

Malaria and AKI 407
Klein N, Pointaire P, et al. Anti-TNF therapy inhibitsfever in cerebral malaria. QJM. 1993;86:91-8.
56. Nahrevanian H, Dascombe MJ. Nitric oxide and re-active nitrogen intermediates in lethal and nonlethalstrains of murine malaria. Parasite Immunol. 2001;23:491-501.
57. Nahrevanian H, Dascombe MJ. Expression of induc-ible nitric oxide synthase (iNOS) mRNA in targetorgans of lethal and non-lethal strains of murinemalaria. Parasite Immunol. 2002;24:471-8.
58. Jacobs P, Radzioch D, Stevenson MM. In vivo regu-lation of nitric oxide production by tumor necrosisfactor alpha and gamma interferon, but not by inter-leukin-4, during blood stage malaria in mice. InfectImmun. 1996;64:44-9.
59. Shultz PJ, Archer SL, Rosenberg ME. Inducible nitricoxide synthase mRNA and activity in glomerularmesangial cells. Kidney Int. 1994;46:683-9.
60. Greve B, Lehman LG, Lell B, Luckner D, Schmidt-OttR, Kremsner PG. High oxygen radical production isassociated with fast parasite clearance in childrenwith Plasmodium falciparum malaria. J Infect Dis.1999;179:1584-6.
61. Griffiths MJ, Ndungu F, Baird KL, Muller DP, MarshK, Newton CR. Oxidative stress and erythrocytedamage in Kenyan children with severe Plasmodiumfalciparum malaria. Br J Haematol. 2001;113:486-91.
62. Nanda NK, Das BS. Presence of pro-oxidants inplasma of patients suffering from Plasmodium fal-ciparum malaria. Trans R Soc Trop Med Hyg. 2000;94:684-8.
63. Das BS, Nanda NK. Evidence for erythrocyte lipidperoxidation in acute falciparum malaria. Trans RSoc Trop Med Hyg. 1999;93:58-62.
64. Das BS, Patnaik JK, Mohanty S, Mishra SK, MohantyD, Satpathy SK, et al. Plasma antioxidants and lipidperoxidation products in falciparum malaria. Am JTrop Med Hyg. 1993;49:720-5.
65. Clark IA, Budd AC, Alleva LM, Cowden WB. Humanmalarial disease: a consequence of inflammatory cy-tokine release. Malaria J. 2006;5:85.
66. Maitland K, Levin M, English M, Mithwani S, PeshuN, Marsh K, et al. Severe P. falciparum malaria inKenyan children: evidence for hypovolaemia. QJM.2003;96:427-34.
67. English M, Waruiru C, Marsh K. Transfusion forrespiratory distress in life-threatening childhood ma-laria. Am J Trop Med Hyg. 1996;55:525-30.
68. Maitland K, Pamba A, English M, Peshu N, Marsh K,Newton C, et al. Randomized trial of volume expan-sion with albumin or saline in children with severemalaria: preliminary evidence of albumin benefit.Clin Infect Dis. 2005;40:538-45.
69. Das BS, Thurnham DI, Das DB. Plasma �-tocopherol,retinol, and carotenoids in children with falciparummalaria. Am J Clin Nutr. 1996;64:94-100.
70. Das BS, Thurnham DI, Das DB. Influence of malaria
on markers of iron status in children: implicationsfor interpreting iron status in malaria-endemiccommunities. Br J Nutr. 1997;78:751-60.
71. Thiemermann C, Szabo C, Mitchell JA, Vane JR.Vascular hyporeactivity to vasoconstrictor agentsand hemodynamic decompensation in hemorrhagicshock is mediated by nitric oxide. Proc Natl Acad SciU S A. 1993;90:267-71.
72. Hollenberg SM, Broussard M, Osman J, Parrillo JE.Increased microvascular reactivity and improvedmortality in septic mice lacking inducible nitric ox-ide synthase. Circ Res. 2000;86:774-8.
73. Planche T, Onanga M, Schwenk A, Dzeing A, Bor-rmann S, Faucher JF. Assessment of volume de-pletion in children with malaria. PLoS Med. 2004;e18:4.
74. Planche T, Dzeing A, Ngou Milama E, Kombila M,Stacpoole PW. Metabolic complications of severemalaria. Curr Top Microbiol Immunol. 2005;295:105-36.
75. Cumming AD, Driedger AA, McDonald JW, LindsayRM, Solez K, Linton AI. Vasoactive hormones in therenal response to systemic sepsis. Am J Kidney Dis.1988;11:23-32.
76. Benedict CR, Rose JA. Arterial norepinephrinechanges in patients with septic shock. Circ Shock.1992;38:165-72.
77. Davies NW. Modulation of ATP-sensitive K� chan-nels in skeletal muscle by intracellular protons. Na-ture. 1990;343:375-7.
78. Keung EC, Li Q. Lactate activates ATP-sensitive po-tassium channels in guinea pig ventricular myocytes.J Clin Invest. 1991;88:1772-7.
79. Fink MP. Cytopathic hypoxia. Mitochondrial dys-function as mechanism contributing to organ dys-function in sepsis. Crit Care Clin. 2001;17:219-37.
80. Azimi G, Vincent JL. Ultimate survival from septicshock. Resuscitation. 1986;14:245-53.
81. Krishna S, Waller DW, Terkuile F, Kwiatkowski D,Crawley J, Craddock CFC, et al. Lactic acidosis andhypoglycaemia in children with severe malaria—pathophysiological and prognostic significance.Trans R Soc Trop Med Hyg. 1994;88:67-73.
82. English M, Muambi B, Mithwani S, Marsh K. Lacticacidosis and oxygen debt in African children withsevere anaemia. QJM. 1997;90:563-9.
83. Eiam-Ong S, Sitprija V. Falciparum malaria and thekidney: a model of inflammation. Am J Kidney Dis.1998;32:361-75.
84. Philips RE, White NJ, Looareesuwan S, et al. Acuterenal failure in P. falciparum malaria in eastern Thai-land: successful use of peritoneal dialysis. Paper pre-sented at: XI International Congress for TropicalMedicine and Malaria; 1984 Sept 6-11; Calgary, Can-ada.
85. Mishra SK, Mohanty S, Satpathy SK, Mohapatra DN.Cerebral malaria in adults—a description of 526cases admitted to Ispat General Hospital in Rourkela,India. Ann Trop Med Parasitol. 2007;101:187-93.
86. Mishra SK, Dietz K, Mohanty S, Pati SS. Influence of

1
1
1
1
1
408 S.K. Mishra and B.S. Das
acute renal failure in patients with cerebral mal-aria—a hospital-based study from India. Trop Doct.2007;37:103-4.
87. Wilairatana P, Looareesuwan S, Charoenlarp P. Liverprofile changes and complications in jaundiced pa-tients with falciparum malaria. Trop Med Parasitol.1994;45:298-302.
88. Davis TM, Li GQ, Guo XB, Spencer JL, St John A.Serum ionized calcium, serum and intracellularphosphate, and serum parathormone concentra-tions in acute malaria. Trans R Soc Trop Med Hyg.1993;87:49-53.
89. Mishra SK, Mohapatra S, Mohanty S, Patel NC, Mo-hapatra DN. Acute renal failure in falciparum ma-laria. J Indian Acad Clin Med. 2002;3:141-7.
90. Prakash J, Singh AK, Gujrati S, Maheswari A. Acuterenal failure in malaria: changing trends. Ind J Neph-rol. 2002;12:113-7.
91. Segasothy M, Swaminathan M, Kong NC. Acute renalfailure in falciparum malaria. Med J Malaysia. 1994;49:412-5.
92. Naqvi R, Ahmad E, Akhtar F, Yazdani I, Abbas K,Naqvi A, et al. Predictors of outcome in malarialrenal failure. Ren Fail. 1996;18:685-8.
93. Sheiban AK. Prognosis of malaria associated severeacute renal failure in children. Ren Fail. 1999;21:63-6.
94. Phu NH, Hien TT, Nguyen THM, et al. Hemofiltra-tion and peritoneal dialysis in infection-associatedacute renal failure in Vietnam. N Engl J Med. 2002;347:895-902.
95. Mishra SK, Panigrahi P, Mishra R, Mohanty S. Predic-tion of outcome in adults with severe falciparummalaria: a new scoring system. Malaria J. 2007;6:24.
96. White NJ, Miller KD, Marsh K, Berry CD, et al.
Hypoglycemia in African children with severemalaria. Lancet. 1987;i:708-11.
97. Das BS, Satpathy SK, Mohanty D, Mohanty S, MishraSK, Satapathy PC, et al. Hypoglycaemia in severefalciparum malaria. Trans R Soc Trop Med Hyg.1988;82:197-201.
98. Mohanty S, Mishra SK, Satpathy SK, Dash S, PatnaikJ. Alpha, beta-Arteether for the treatment of compli-cated falciparum malaria. Trans R Soc Trop MedHyg. 1997;91:328-30.
99. Dondorp A, Nosten F, Stepniewska K, Day N, WhiteN; South East Asian Quinine Artesunate Malaria Trial(SEAQUAMAT) group. Artesunate versus quinine fortreatment of severe falciparum malaria: a random-ised trial. Lancet. 2005;366:717-25.
00. Jones KL, Donegan S, Lalloo DG. Artesunate versusquinine for treating severe malaria. Cochrane Data-base Syst Rev. 2007;4:CD005967.
01. Mishra SK, Mohanty S. Ptyalism as a side effect in thetreatment of falciparum malaria with artemisinin.Ann Trop Med Parasitol. 1999;93:413-4.
02. Cantarovich F, Rangoonwala B, Lorenz H, Verho M,Esnault VL, High-Dose Furosemide in Acute RenalFailure Study Group. High-dose furosemide for es-tablished ARF: a prospective, randomized, double-blind, placebo-controlled, multicenter trial. Am JKidney Dis. 2004;44:402-9.
03. Bagshaw SM, Delaney A, Haase M, Ghali WA, Bel-lomo R. Loop diuretics in the management of acuterenal failure: a systematic review and meta-analysis.Crit Care Resusc. 2007;9:60-8.
04. Day NJ, Phu NH, Bethel DP, et al. The effects ofdopamine and adrenaline infusions on acid-base bal-ance and systemic haemodynamics in severe infec-
tion. Lancet. 2000;348:219-23.