Embed Size (px)
Citation preview
Geriatrik Hastanın Youmlnetimi
Prof Dr Selim NALBANTMaltepe Uumlniversitesi Tıp Fakuumlltesi
Yaşlanma huumlcre doku organ ve sistemlerinde zamanın ilerlemesiyle ortaya ccedilıkan geriye doumlnuumlşuuml olmayan yapısal ve işlevsel değişikliklerin tuumlmuumlduumlr
2
YAŞLANMA-YAŞLI
bull Yaş lanma
ndash Otuzlu yaşlar ile başlayan ve hayat boyu suumlregiden devamlı ve lineer bir suumlreccedil
ndash Organizmanın uyum sağlama yeteneğinin azalması
ndash Yaşa oumlzguumln mortalitenin artması
bull Yaş l ı
ndash Oumlmruumlnuumln son yıllarına ulaşmış
ndash Yaşamsal fonksiyonlarının kapasiteleri azalmış
ndash Ccedilevre ile ilişkisi gerilemiş
3
bull Yaşlı gt 65 yaş
ndashKronolojik yaş
ndashBiyolojik yaş
4
Geriatri yaşlılık doumlnemindeki sağlık sorunları ve bu sorunların tedavileriyle ilgilenen tıp dalıdır
5
Yıllar geccedilince 50 yaşından sonra bir ccedilok insanın bedensel fonksiyonları değişirbull Bazıları ccedilok accedilıktır (Goumlrme kalitesi azalır)
bull Bazıları fark edilmez (Boumlbrek fonksiyonları azalır)
6
bull XXyuumlzyılda tuumlm duumlnyada yaşlı nuumlfus sayısıbelirgin olarak artmıştır
ndash Hastaneye yatanların 43rsquouuml
ndash Yoğun bakıma yatanların 48rsquoi yaşlı
bull İleri yaşlılar
ndash Yaşlı popuumllasyonun 12rsquosi
ndash Acile başvuruların 15rsquoi
ndash Ambulansla başvuruların 36rsquosı
7
Erişkin Tıbbından Farkıhelliphelliphellip
bull Yaşlının temel ihtiyaccedillarını belirlerhellip
bull Ccediluumlnkuuml yaşlı fizyonomisi genccedil bireyinkinden oldukccedila farklıdır
bull Yaşlıdaki semptomları sağlam kalan organların rezervleri belirler
ndash Sigara iccedilenlerin bu rezervi ccedilabuk bitirmesi gibihelliphellip
Fletcher C Peto R The natural history of chronic airflow obstruction Br Med J 1977 1 (6077) 1645ndash8
8
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist hastalıklarla normal yaşlanmanın etkilerini ayırt eder
ndash Boumlbrek fonksiyonlarında azalma yaşlanmanın bir parccedilasıyken boumlbrek yetmezliği ve inkontinans tedavi edilmelidir
9
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist olan hastalığı ve yaşlanmanın vuumlcut uumlzerindeki etkilerini tedavi ya da konsuumllte ederbull Bunun iccedilin hastayı ve sosyo ekonomik
koşullarını bir buumltuumln olarak ele alırhellip
10
Yaşlıya yaklaşım
bull Hor goumlrme
bull Normal yaşlanma
bull Normal-hastalık ayırımı
bull İletişim
ndash Anamnez alma
bull Sağlık uygulama tebliğleri
11
ACİLE BAŞ VURAN YAŞLILAR
Ohio Med 1991 Jul87(7)347-50 A biopsychosocial profile of the geriatric population who frequently visit the emergency department Brokaw M Zaraa AS
NEDEN
Ortalama Yaş 74
50 Psişik
Goumlğuumls Ağrısı 208
Genel somatik ağrı 189
GI 161
Dispne 137
Mental durum değişiklikleri
128
12
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSDoctoral Student Graduate Institute of Nursing College of Nursing Taipei Medical University Taipei Taiwan Department of Nursing Cardinal Tien Junior College of Healthcare and Management Taipei TaiwanAIM The rapid growth of the elderly population has given rise to the need for better geriatric care The present study explored the common conditions of elderly outpatients with multiple physician visits in order to develop feasible clinical indicators that can be rapidly administered for the evaluation of geriatric syndromes in outpatient settingsMETHODS The National Health Insurance Research Database (2008) was analyzed Claims for elderly outpatients with more than two physician visits in the same day were retrieved The primary diagnoses types of prescriptions and comorbidities were cross-examinedRESULTS The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to 3940and which increased steadily with age A maximum of seven physician visits in a single day was observedThe most common multiple physician visit was two visits per day with a prevalence rate of 3097 The twomost common accompanying conditions were hypertension (379) and typethinsp2 diabetes mellitus (368)There was a greater relative increase in the prevalence of senile dementia and chronic obstructivepulmonary disease in older age groups The three overall leading specialties were cardiology internalmedicine and ophthalmology however rehabilitation medicine was the most common female-specificspecialty The most commonly prescribed medications were antihypertension drugs The most prevalentcomorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
13
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSRESULTS
The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to3940 and which increased steadily with age A maximum of seven physician visits in a single
day was observed The most common multiple physician visit was two visits per day with a
prevalence rate of 3097 The two most common accompanying conditions were hypertension (379) andtypethinsp2 diabetes mellitus (368) There was a greater relative increase in the prevalence of senile dementiaand chronic obstructive pulmonary disease in older age groups The three overall leading specialties werecardiology internal medicine and ophthalmology however rehabilitation medicine was the most commonfemale-specific specialty The most commonly prescribed medications were antihypertension drugs Themost prevalent comorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION
We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
14
Yaşlının Değerlendirilmesibull Metabolizmanın yavaşlaması ile ilgili sorunlarbull Strese karşı direncin azalması ile ilgili sorunlarbull Kognitif problemler ve bunların tıbbi ve davranışsal sonuccedillarıbull Polifarmasibull Sosyo-ekonomik sonuccedilların yarattığı sorunlarbull Koruyucu hekimlik
15
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
Yaşlanma huumlcre doku organ ve sistemlerinde zamanın ilerlemesiyle ortaya ccedilıkan geriye doumlnuumlşuuml olmayan yapısal ve işlevsel değişikliklerin tuumlmuumlduumlr
2
YAŞLANMA-YAŞLI
bull Yaş lanma
ndash Otuzlu yaşlar ile başlayan ve hayat boyu suumlregiden devamlı ve lineer bir suumlreccedil
ndash Organizmanın uyum sağlama yeteneğinin azalması
ndash Yaşa oumlzguumln mortalitenin artması
bull Yaş l ı
ndash Oumlmruumlnuumln son yıllarına ulaşmış
ndash Yaşamsal fonksiyonlarının kapasiteleri azalmış
ndash Ccedilevre ile ilişkisi gerilemiş
3
bull Yaşlı gt 65 yaş
ndashKronolojik yaş
ndashBiyolojik yaş
4
Geriatri yaşlılık doumlnemindeki sağlık sorunları ve bu sorunların tedavileriyle ilgilenen tıp dalıdır
5
Yıllar geccedilince 50 yaşından sonra bir ccedilok insanın bedensel fonksiyonları değişirbull Bazıları ccedilok accedilıktır (Goumlrme kalitesi azalır)
bull Bazıları fark edilmez (Boumlbrek fonksiyonları azalır)
6
bull XXyuumlzyılda tuumlm duumlnyada yaşlı nuumlfus sayısıbelirgin olarak artmıştır
ndash Hastaneye yatanların 43rsquouuml
ndash Yoğun bakıma yatanların 48rsquoi yaşlı
bull İleri yaşlılar
ndash Yaşlı popuumllasyonun 12rsquosi
ndash Acile başvuruların 15rsquoi
ndash Ambulansla başvuruların 36rsquosı
7
Erişkin Tıbbından Farkıhelliphelliphellip
bull Yaşlının temel ihtiyaccedillarını belirlerhellip
bull Ccediluumlnkuuml yaşlı fizyonomisi genccedil bireyinkinden oldukccedila farklıdır
bull Yaşlıdaki semptomları sağlam kalan organların rezervleri belirler
ndash Sigara iccedilenlerin bu rezervi ccedilabuk bitirmesi gibihelliphellip
Fletcher C Peto R The natural history of chronic airflow obstruction Br Med J 1977 1 (6077) 1645ndash8
8
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist hastalıklarla normal yaşlanmanın etkilerini ayırt eder
ndash Boumlbrek fonksiyonlarında azalma yaşlanmanın bir parccedilasıyken boumlbrek yetmezliği ve inkontinans tedavi edilmelidir
9
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist olan hastalığı ve yaşlanmanın vuumlcut uumlzerindeki etkilerini tedavi ya da konsuumllte ederbull Bunun iccedilin hastayı ve sosyo ekonomik
koşullarını bir buumltuumln olarak ele alırhellip
10
Yaşlıya yaklaşım
bull Hor goumlrme
bull Normal yaşlanma
bull Normal-hastalık ayırımı
bull İletişim
ndash Anamnez alma
bull Sağlık uygulama tebliğleri
11
ACİLE BAŞ VURAN YAŞLILAR
Ohio Med 1991 Jul87(7)347-50 A biopsychosocial profile of the geriatric population who frequently visit the emergency department Brokaw M Zaraa AS
NEDEN
Ortalama Yaş 74
50 Psişik
Goumlğuumls Ağrısı 208
Genel somatik ağrı 189
GI 161
Dispne 137
Mental durum değişiklikleri
128
12
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSDoctoral Student Graduate Institute of Nursing College of Nursing Taipei Medical University Taipei Taiwan Department of Nursing Cardinal Tien Junior College of Healthcare and Management Taipei TaiwanAIM The rapid growth of the elderly population has given rise to the need for better geriatric care The present study explored the common conditions of elderly outpatients with multiple physician visits in order to develop feasible clinical indicators that can be rapidly administered for the evaluation of geriatric syndromes in outpatient settingsMETHODS The National Health Insurance Research Database (2008) was analyzed Claims for elderly outpatients with more than two physician visits in the same day were retrieved The primary diagnoses types of prescriptions and comorbidities were cross-examinedRESULTS The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to 3940and which increased steadily with age A maximum of seven physician visits in a single day was observedThe most common multiple physician visit was two visits per day with a prevalence rate of 3097 The twomost common accompanying conditions were hypertension (379) and typethinsp2 diabetes mellitus (368)There was a greater relative increase in the prevalence of senile dementia and chronic obstructivepulmonary disease in older age groups The three overall leading specialties were cardiology internalmedicine and ophthalmology however rehabilitation medicine was the most common female-specificspecialty The most commonly prescribed medications were antihypertension drugs The most prevalentcomorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
13
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSRESULTS
The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to3940 and which increased steadily with age A maximum of seven physician visits in a single
day was observed The most common multiple physician visit was two visits per day with a
prevalence rate of 3097 The two most common accompanying conditions were hypertension (379) andtypethinsp2 diabetes mellitus (368) There was a greater relative increase in the prevalence of senile dementiaand chronic obstructive pulmonary disease in older age groups The three overall leading specialties werecardiology internal medicine and ophthalmology however rehabilitation medicine was the most commonfemale-specific specialty The most commonly prescribed medications were antihypertension drugs Themost prevalent comorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION
We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
14
Yaşlının Değerlendirilmesibull Metabolizmanın yavaşlaması ile ilgili sorunlarbull Strese karşı direncin azalması ile ilgili sorunlarbull Kognitif problemler ve bunların tıbbi ve davranışsal sonuccedillarıbull Polifarmasibull Sosyo-ekonomik sonuccedilların yarattığı sorunlarbull Koruyucu hekimlik
15
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
YAŞLANMA-YAŞLI
bull Yaş lanma
ndash Otuzlu yaşlar ile başlayan ve hayat boyu suumlregiden devamlı ve lineer bir suumlreccedil
ndash Organizmanın uyum sağlama yeteneğinin azalması
ndash Yaşa oumlzguumln mortalitenin artması
bull Yaş l ı
ndash Oumlmruumlnuumln son yıllarına ulaşmış
ndash Yaşamsal fonksiyonlarının kapasiteleri azalmış
ndash Ccedilevre ile ilişkisi gerilemiş
3
bull Yaşlı gt 65 yaş
ndashKronolojik yaş
ndashBiyolojik yaş
4
Geriatri yaşlılık doumlnemindeki sağlık sorunları ve bu sorunların tedavileriyle ilgilenen tıp dalıdır
5
Yıllar geccedilince 50 yaşından sonra bir ccedilok insanın bedensel fonksiyonları değişirbull Bazıları ccedilok accedilıktır (Goumlrme kalitesi azalır)
bull Bazıları fark edilmez (Boumlbrek fonksiyonları azalır)
6
bull XXyuumlzyılda tuumlm duumlnyada yaşlı nuumlfus sayısıbelirgin olarak artmıştır
ndash Hastaneye yatanların 43rsquouuml
ndash Yoğun bakıma yatanların 48rsquoi yaşlı
bull İleri yaşlılar
ndash Yaşlı popuumllasyonun 12rsquosi
ndash Acile başvuruların 15rsquoi
ndash Ambulansla başvuruların 36rsquosı
7
Erişkin Tıbbından Farkıhelliphelliphellip
bull Yaşlının temel ihtiyaccedillarını belirlerhellip
bull Ccediluumlnkuuml yaşlı fizyonomisi genccedil bireyinkinden oldukccedila farklıdır
bull Yaşlıdaki semptomları sağlam kalan organların rezervleri belirler
ndash Sigara iccedilenlerin bu rezervi ccedilabuk bitirmesi gibihelliphellip
Fletcher C Peto R The natural history of chronic airflow obstruction Br Med J 1977 1 (6077) 1645ndash8
8
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist hastalıklarla normal yaşlanmanın etkilerini ayırt eder
ndash Boumlbrek fonksiyonlarında azalma yaşlanmanın bir parccedilasıyken boumlbrek yetmezliği ve inkontinans tedavi edilmelidir
9
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist olan hastalığı ve yaşlanmanın vuumlcut uumlzerindeki etkilerini tedavi ya da konsuumllte ederbull Bunun iccedilin hastayı ve sosyo ekonomik
koşullarını bir buumltuumln olarak ele alırhellip
10
Yaşlıya yaklaşım
bull Hor goumlrme
bull Normal yaşlanma
bull Normal-hastalık ayırımı
bull İletişim
ndash Anamnez alma
bull Sağlık uygulama tebliğleri
11
ACİLE BAŞ VURAN YAŞLILAR
Ohio Med 1991 Jul87(7)347-50 A biopsychosocial profile of the geriatric population who frequently visit the emergency department Brokaw M Zaraa AS
NEDEN
Ortalama Yaş 74
50 Psişik
Goumlğuumls Ağrısı 208
Genel somatik ağrı 189
GI 161
Dispne 137
Mental durum değişiklikleri
128
12
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSDoctoral Student Graduate Institute of Nursing College of Nursing Taipei Medical University Taipei Taiwan Department of Nursing Cardinal Tien Junior College of Healthcare and Management Taipei TaiwanAIM The rapid growth of the elderly population has given rise to the need for better geriatric care The present study explored the common conditions of elderly outpatients with multiple physician visits in order to develop feasible clinical indicators that can be rapidly administered for the evaluation of geriatric syndromes in outpatient settingsMETHODS The National Health Insurance Research Database (2008) was analyzed Claims for elderly outpatients with more than two physician visits in the same day were retrieved The primary diagnoses types of prescriptions and comorbidities were cross-examinedRESULTS The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to 3940and which increased steadily with age A maximum of seven physician visits in a single day was observedThe most common multiple physician visit was two visits per day with a prevalence rate of 3097 The twomost common accompanying conditions were hypertension (379) and typethinsp2 diabetes mellitus (368)There was a greater relative increase in the prevalence of senile dementia and chronic obstructivepulmonary disease in older age groups The three overall leading specialties were cardiology internalmedicine and ophthalmology however rehabilitation medicine was the most common female-specificspecialty The most commonly prescribed medications were antihypertension drugs The most prevalentcomorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
13
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSRESULTS
The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to3940 and which increased steadily with age A maximum of seven physician visits in a single
day was observed The most common multiple physician visit was two visits per day with a
prevalence rate of 3097 The two most common accompanying conditions were hypertension (379) andtypethinsp2 diabetes mellitus (368) There was a greater relative increase in the prevalence of senile dementiaand chronic obstructive pulmonary disease in older age groups The three overall leading specialties werecardiology internal medicine and ophthalmology however rehabilitation medicine was the most commonfemale-specific specialty The most commonly prescribed medications were antihypertension drugs Themost prevalent comorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION
We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
14
Yaşlının Değerlendirilmesibull Metabolizmanın yavaşlaması ile ilgili sorunlarbull Strese karşı direncin azalması ile ilgili sorunlarbull Kognitif problemler ve bunların tıbbi ve davranışsal sonuccedillarıbull Polifarmasibull Sosyo-ekonomik sonuccedilların yarattığı sorunlarbull Koruyucu hekimlik
15
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
bull Yaşlı gt 65 yaş
ndashKronolojik yaş
ndashBiyolojik yaş
4
Geriatri yaşlılık doumlnemindeki sağlık sorunları ve bu sorunların tedavileriyle ilgilenen tıp dalıdır
5
Yıllar geccedilince 50 yaşından sonra bir ccedilok insanın bedensel fonksiyonları değişirbull Bazıları ccedilok accedilıktır (Goumlrme kalitesi azalır)
bull Bazıları fark edilmez (Boumlbrek fonksiyonları azalır)
6
bull XXyuumlzyılda tuumlm duumlnyada yaşlı nuumlfus sayısıbelirgin olarak artmıştır
ndash Hastaneye yatanların 43rsquouuml
ndash Yoğun bakıma yatanların 48rsquoi yaşlı
bull İleri yaşlılar
ndash Yaşlı popuumllasyonun 12rsquosi
ndash Acile başvuruların 15rsquoi
ndash Ambulansla başvuruların 36rsquosı
7
Erişkin Tıbbından Farkıhelliphelliphellip
bull Yaşlının temel ihtiyaccedillarını belirlerhellip
bull Ccediluumlnkuuml yaşlı fizyonomisi genccedil bireyinkinden oldukccedila farklıdır
bull Yaşlıdaki semptomları sağlam kalan organların rezervleri belirler
ndash Sigara iccedilenlerin bu rezervi ccedilabuk bitirmesi gibihelliphellip
Fletcher C Peto R The natural history of chronic airflow obstruction Br Med J 1977 1 (6077) 1645ndash8
8
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist hastalıklarla normal yaşlanmanın etkilerini ayırt eder
ndash Boumlbrek fonksiyonlarında azalma yaşlanmanın bir parccedilasıyken boumlbrek yetmezliği ve inkontinans tedavi edilmelidir
9
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist olan hastalığı ve yaşlanmanın vuumlcut uumlzerindeki etkilerini tedavi ya da konsuumllte ederbull Bunun iccedilin hastayı ve sosyo ekonomik
koşullarını bir buumltuumln olarak ele alırhellip
10
Yaşlıya yaklaşım
bull Hor goumlrme
bull Normal yaşlanma
bull Normal-hastalık ayırımı
bull İletişim
ndash Anamnez alma
bull Sağlık uygulama tebliğleri
11
ACİLE BAŞ VURAN YAŞLILAR
Ohio Med 1991 Jul87(7)347-50 A biopsychosocial profile of the geriatric population who frequently visit the emergency department Brokaw M Zaraa AS
NEDEN
Ortalama Yaş 74
50 Psişik
Goumlğuumls Ağrısı 208
Genel somatik ağrı 189
GI 161
Dispne 137
Mental durum değişiklikleri
128
12
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSDoctoral Student Graduate Institute of Nursing College of Nursing Taipei Medical University Taipei Taiwan Department of Nursing Cardinal Tien Junior College of Healthcare and Management Taipei TaiwanAIM The rapid growth of the elderly population has given rise to the need for better geriatric care The present study explored the common conditions of elderly outpatients with multiple physician visits in order to develop feasible clinical indicators that can be rapidly administered for the evaluation of geriatric syndromes in outpatient settingsMETHODS The National Health Insurance Research Database (2008) was analyzed Claims for elderly outpatients with more than two physician visits in the same day were retrieved The primary diagnoses types of prescriptions and comorbidities were cross-examinedRESULTS The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to 3940and which increased steadily with age A maximum of seven physician visits in a single day was observedThe most common multiple physician visit was two visits per day with a prevalence rate of 3097 The twomost common accompanying conditions were hypertension (379) and typethinsp2 diabetes mellitus (368)There was a greater relative increase in the prevalence of senile dementia and chronic obstructivepulmonary disease in older age groups The three overall leading specialties were cardiology internalmedicine and ophthalmology however rehabilitation medicine was the most common female-specificspecialty The most commonly prescribed medications were antihypertension drugs The most prevalentcomorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
13
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSRESULTS
The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to3940 and which increased steadily with age A maximum of seven physician visits in a single
day was observed The most common multiple physician visit was two visits per day with a
prevalence rate of 3097 The two most common accompanying conditions were hypertension (379) andtypethinsp2 diabetes mellitus (368) There was a greater relative increase in the prevalence of senile dementiaand chronic obstructive pulmonary disease in older age groups The three overall leading specialties werecardiology internal medicine and ophthalmology however rehabilitation medicine was the most commonfemale-specific specialty The most commonly prescribed medications were antihypertension drugs Themost prevalent comorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION
We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
14
Yaşlının Değerlendirilmesibull Metabolizmanın yavaşlaması ile ilgili sorunlarbull Strese karşı direncin azalması ile ilgili sorunlarbull Kognitif problemler ve bunların tıbbi ve davranışsal sonuccedillarıbull Polifarmasibull Sosyo-ekonomik sonuccedilların yarattığı sorunlarbull Koruyucu hekimlik
15
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
Geriatri yaşlılık doumlnemindeki sağlık sorunları ve bu sorunların tedavileriyle ilgilenen tıp dalıdır
5
Yıllar geccedilince 50 yaşından sonra bir ccedilok insanın bedensel fonksiyonları değişirbull Bazıları ccedilok accedilıktır (Goumlrme kalitesi azalır)
bull Bazıları fark edilmez (Boumlbrek fonksiyonları azalır)
6
bull XXyuumlzyılda tuumlm duumlnyada yaşlı nuumlfus sayısıbelirgin olarak artmıştır
ndash Hastaneye yatanların 43rsquouuml
ndash Yoğun bakıma yatanların 48rsquoi yaşlı
bull İleri yaşlılar
ndash Yaşlı popuumllasyonun 12rsquosi
ndash Acile başvuruların 15rsquoi
ndash Ambulansla başvuruların 36rsquosı
7
Erişkin Tıbbından Farkıhelliphelliphellip
bull Yaşlının temel ihtiyaccedillarını belirlerhellip
bull Ccediluumlnkuuml yaşlı fizyonomisi genccedil bireyinkinden oldukccedila farklıdır
bull Yaşlıdaki semptomları sağlam kalan organların rezervleri belirler
ndash Sigara iccedilenlerin bu rezervi ccedilabuk bitirmesi gibihelliphellip
Fletcher C Peto R The natural history of chronic airflow obstruction Br Med J 1977 1 (6077) 1645ndash8
8
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist hastalıklarla normal yaşlanmanın etkilerini ayırt eder
ndash Boumlbrek fonksiyonlarında azalma yaşlanmanın bir parccedilasıyken boumlbrek yetmezliği ve inkontinans tedavi edilmelidir
9
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist olan hastalığı ve yaşlanmanın vuumlcut uumlzerindeki etkilerini tedavi ya da konsuumllte ederbull Bunun iccedilin hastayı ve sosyo ekonomik
koşullarını bir buumltuumln olarak ele alırhellip
10
Yaşlıya yaklaşım
bull Hor goumlrme
bull Normal yaşlanma
bull Normal-hastalık ayırımı
bull İletişim
ndash Anamnez alma
bull Sağlık uygulama tebliğleri
11
ACİLE BAŞ VURAN YAŞLILAR
Ohio Med 1991 Jul87(7)347-50 A biopsychosocial profile of the geriatric population who frequently visit the emergency department Brokaw M Zaraa AS
NEDEN
Ortalama Yaş 74
50 Psişik
Goumlğuumls Ağrısı 208
Genel somatik ağrı 189
GI 161
Dispne 137
Mental durum değişiklikleri
128
12
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSDoctoral Student Graduate Institute of Nursing College of Nursing Taipei Medical University Taipei Taiwan Department of Nursing Cardinal Tien Junior College of Healthcare and Management Taipei TaiwanAIM The rapid growth of the elderly population has given rise to the need for better geriatric care The present study explored the common conditions of elderly outpatients with multiple physician visits in order to develop feasible clinical indicators that can be rapidly administered for the evaluation of geriatric syndromes in outpatient settingsMETHODS The National Health Insurance Research Database (2008) was analyzed Claims for elderly outpatients with more than two physician visits in the same day were retrieved The primary diagnoses types of prescriptions and comorbidities were cross-examinedRESULTS The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to 3940and which increased steadily with age A maximum of seven physician visits in a single day was observedThe most common multiple physician visit was two visits per day with a prevalence rate of 3097 The twomost common accompanying conditions were hypertension (379) and typethinsp2 diabetes mellitus (368)There was a greater relative increase in the prevalence of senile dementia and chronic obstructivepulmonary disease in older age groups The three overall leading specialties were cardiology internalmedicine and ophthalmology however rehabilitation medicine was the most common female-specificspecialty The most commonly prescribed medications were antihypertension drugs The most prevalentcomorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
13
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSRESULTS
The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to3940 and which increased steadily with age A maximum of seven physician visits in a single
day was observed The most common multiple physician visit was two visits per day with a
prevalence rate of 3097 The two most common accompanying conditions were hypertension (379) andtypethinsp2 diabetes mellitus (368) There was a greater relative increase in the prevalence of senile dementiaand chronic obstructive pulmonary disease in older age groups The three overall leading specialties werecardiology internal medicine and ophthalmology however rehabilitation medicine was the most commonfemale-specific specialty The most commonly prescribed medications were antihypertension drugs Themost prevalent comorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION
We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
14
Yaşlının Değerlendirilmesibull Metabolizmanın yavaşlaması ile ilgili sorunlarbull Strese karşı direncin azalması ile ilgili sorunlarbull Kognitif problemler ve bunların tıbbi ve davranışsal sonuccedillarıbull Polifarmasibull Sosyo-ekonomik sonuccedilların yarattığı sorunlarbull Koruyucu hekimlik
15
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
Yıllar geccedilince 50 yaşından sonra bir ccedilok insanın bedensel fonksiyonları değişirbull Bazıları ccedilok accedilıktır (Goumlrme kalitesi azalır)
bull Bazıları fark edilmez (Boumlbrek fonksiyonları azalır)
6
bull XXyuumlzyılda tuumlm duumlnyada yaşlı nuumlfus sayısıbelirgin olarak artmıştır
ndash Hastaneye yatanların 43rsquouuml
ndash Yoğun bakıma yatanların 48rsquoi yaşlı
bull İleri yaşlılar
ndash Yaşlı popuumllasyonun 12rsquosi
ndash Acile başvuruların 15rsquoi
ndash Ambulansla başvuruların 36rsquosı
7
Erişkin Tıbbından Farkıhelliphelliphellip
bull Yaşlının temel ihtiyaccedillarını belirlerhellip
bull Ccediluumlnkuuml yaşlı fizyonomisi genccedil bireyinkinden oldukccedila farklıdır
bull Yaşlıdaki semptomları sağlam kalan organların rezervleri belirler
ndash Sigara iccedilenlerin bu rezervi ccedilabuk bitirmesi gibihelliphellip
Fletcher C Peto R The natural history of chronic airflow obstruction Br Med J 1977 1 (6077) 1645ndash8
8
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist hastalıklarla normal yaşlanmanın etkilerini ayırt eder
ndash Boumlbrek fonksiyonlarında azalma yaşlanmanın bir parccedilasıyken boumlbrek yetmezliği ve inkontinans tedavi edilmelidir
9
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist olan hastalığı ve yaşlanmanın vuumlcut uumlzerindeki etkilerini tedavi ya da konsuumllte ederbull Bunun iccedilin hastayı ve sosyo ekonomik
koşullarını bir buumltuumln olarak ele alırhellip
10
Yaşlıya yaklaşım
bull Hor goumlrme
bull Normal yaşlanma
bull Normal-hastalık ayırımı
bull İletişim
ndash Anamnez alma
bull Sağlık uygulama tebliğleri
11
ACİLE BAŞ VURAN YAŞLILAR
Ohio Med 1991 Jul87(7)347-50 A biopsychosocial profile of the geriatric population who frequently visit the emergency department Brokaw M Zaraa AS
NEDEN
Ortalama Yaş 74
50 Psişik
Goumlğuumls Ağrısı 208
Genel somatik ağrı 189
GI 161
Dispne 137
Mental durum değişiklikleri
128
12
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSDoctoral Student Graduate Institute of Nursing College of Nursing Taipei Medical University Taipei Taiwan Department of Nursing Cardinal Tien Junior College of Healthcare and Management Taipei TaiwanAIM The rapid growth of the elderly population has given rise to the need for better geriatric care The present study explored the common conditions of elderly outpatients with multiple physician visits in order to develop feasible clinical indicators that can be rapidly administered for the evaluation of geriatric syndromes in outpatient settingsMETHODS The National Health Insurance Research Database (2008) was analyzed Claims for elderly outpatients with more than two physician visits in the same day were retrieved The primary diagnoses types of prescriptions and comorbidities were cross-examinedRESULTS The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to 3940and which increased steadily with age A maximum of seven physician visits in a single day was observedThe most common multiple physician visit was two visits per day with a prevalence rate of 3097 The twomost common accompanying conditions were hypertension (379) and typethinsp2 diabetes mellitus (368)There was a greater relative increase in the prevalence of senile dementia and chronic obstructivepulmonary disease in older age groups The three overall leading specialties were cardiology internalmedicine and ophthalmology however rehabilitation medicine was the most common female-specificspecialty The most commonly prescribed medications were antihypertension drugs The most prevalentcomorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
13
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSRESULTS
The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to3940 and which increased steadily with age A maximum of seven physician visits in a single
day was observed The most common multiple physician visit was two visits per day with a
prevalence rate of 3097 The two most common accompanying conditions were hypertension (379) andtypethinsp2 diabetes mellitus (368) There was a greater relative increase in the prevalence of senile dementiaand chronic obstructive pulmonary disease in older age groups The three overall leading specialties werecardiology internal medicine and ophthalmology however rehabilitation medicine was the most commonfemale-specific specialty The most commonly prescribed medications were antihypertension drugs Themost prevalent comorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION
We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
14
Yaşlının Değerlendirilmesibull Metabolizmanın yavaşlaması ile ilgili sorunlarbull Strese karşı direncin azalması ile ilgili sorunlarbull Kognitif problemler ve bunların tıbbi ve davranışsal sonuccedillarıbull Polifarmasibull Sosyo-ekonomik sonuccedilların yarattığı sorunlarbull Koruyucu hekimlik
15
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
bull XXyuumlzyılda tuumlm duumlnyada yaşlı nuumlfus sayısıbelirgin olarak artmıştır
ndash Hastaneye yatanların 43rsquouuml
ndash Yoğun bakıma yatanların 48rsquoi yaşlı
bull İleri yaşlılar
ndash Yaşlı popuumllasyonun 12rsquosi
ndash Acile başvuruların 15rsquoi
ndash Ambulansla başvuruların 36rsquosı
7
Erişkin Tıbbından Farkıhelliphelliphellip
bull Yaşlının temel ihtiyaccedillarını belirlerhellip
bull Ccediluumlnkuuml yaşlı fizyonomisi genccedil bireyinkinden oldukccedila farklıdır
bull Yaşlıdaki semptomları sağlam kalan organların rezervleri belirler
ndash Sigara iccedilenlerin bu rezervi ccedilabuk bitirmesi gibihelliphellip
Fletcher C Peto R The natural history of chronic airflow obstruction Br Med J 1977 1 (6077) 1645ndash8
8
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist hastalıklarla normal yaşlanmanın etkilerini ayırt eder
ndash Boumlbrek fonksiyonlarında azalma yaşlanmanın bir parccedilasıyken boumlbrek yetmezliği ve inkontinans tedavi edilmelidir
9
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist olan hastalığı ve yaşlanmanın vuumlcut uumlzerindeki etkilerini tedavi ya da konsuumllte ederbull Bunun iccedilin hastayı ve sosyo ekonomik
koşullarını bir buumltuumln olarak ele alırhellip
10
Yaşlıya yaklaşım
bull Hor goumlrme
bull Normal yaşlanma
bull Normal-hastalık ayırımı
bull İletişim
ndash Anamnez alma
bull Sağlık uygulama tebliğleri
11
ACİLE BAŞ VURAN YAŞLILAR
Ohio Med 1991 Jul87(7)347-50 A biopsychosocial profile of the geriatric population who frequently visit the emergency department Brokaw M Zaraa AS
NEDEN
Ortalama Yaş 74
50 Psişik
Goumlğuumls Ağrısı 208
Genel somatik ağrı 189
GI 161
Dispne 137
Mental durum değişiklikleri
128
12
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSDoctoral Student Graduate Institute of Nursing College of Nursing Taipei Medical University Taipei Taiwan Department of Nursing Cardinal Tien Junior College of Healthcare and Management Taipei TaiwanAIM The rapid growth of the elderly population has given rise to the need for better geriatric care The present study explored the common conditions of elderly outpatients with multiple physician visits in order to develop feasible clinical indicators that can be rapidly administered for the evaluation of geriatric syndromes in outpatient settingsMETHODS The National Health Insurance Research Database (2008) was analyzed Claims for elderly outpatients with more than two physician visits in the same day were retrieved The primary diagnoses types of prescriptions and comorbidities were cross-examinedRESULTS The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to 3940and which increased steadily with age A maximum of seven physician visits in a single day was observedThe most common multiple physician visit was two visits per day with a prevalence rate of 3097 The twomost common accompanying conditions were hypertension (379) and typethinsp2 diabetes mellitus (368)There was a greater relative increase in the prevalence of senile dementia and chronic obstructivepulmonary disease in older age groups The three overall leading specialties were cardiology internalmedicine and ophthalmology however rehabilitation medicine was the most common female-specificspecialty The most commonly prescribed medications were antihypertension drugs The most prevalentcomorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
13
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSRESULTS
The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to3940 and which increased steadily with age A maximum of seven physician visits in a single
day was observed The most common multiple physician visit was two visits per day with a
prevalence rate of 3097 The two most common accompanying conditions were hypertension (379) andtypethinsp2 diabetes mellitus (368) There was a greater relative increase in the prevalence of senile dementiaand chronic obstructive pulmonary disease in older age groups The three overall leading specialties werecardiology internal medicine and ophthalmology however rehabilitation medicine was the most commonfemale-specific specialty The most commonly prescribed medications were antihypertension drugs Themost prevalent comorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION
We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
14
Yaşlının Değerlendirilmesibull Metabolizmanın yavaşlaması ile ilgili sorunlarbull Strese karşı direncin azalması ile ilgili sorunlarbull Kognitif problemler ve bunların tıbbi ve davranışsal sonuccedillarıbull Polifarmasibull Sosyo-ekonomik sonuccedilların yarattığı sorunlarbull Koruyucu hekimlik
15
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26

Erişkin Tıbbından Farkıhelliphelliphellip
bull Yaşlının temel ihtiyaccedillarını belirlerhellip
bull Ccediluumlnkuuml yaşlı fizyonomisi genccedil bireyinkinden oldukccedila farklıdır
bull Yaşlıdaki semptomları sağlam kalan organların rezervleri belirler
ndash Sigara iccedilenlerin bu rezervi ccedilabuk bitirmesi gibihelliphellip
Fletcher C Peto R The natural history of chronic airflow obstruction Br Med J 1977 1 (6077) 1645ndash8
8
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist hastalıklarla normal yaşlanmanın etkilerini ayırt eder
ndash Boumlbrek fonksiyonlarında azalma yaşlanmanın bir parccedilasıyken boumlbrek yetmezliği ve inkontinans tedavi edilmelidir
9
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist olan hastalığı ve yaşlanmanın vuumlcut uumlzerindeki etkilerini tedavi ya da konsuumllte ederbull Bunun iccedilin hastayı ve sosyo ekonomik
koşullarını bir buumltuumln olarak ele alırhellip
10
Yaşlıya yaklaşım
bull Hor goumlrme
bull Normal yaşlanma
bull Normal-hastalık ayırımı
bull İletişim
ndash Anamnez alma
bull Sağlık uygulama tebliğleri
11
ACİLE BAŞ VURAN YAŞLILAR
Ohio Med 1991 Jul87(7)347-50 A biopsychosocial profile of the geriatric population who frequently visit the emergency department Brokaw M Zaraa AS
NEDEN
Ortalama Yaş 74
50 Psişik
Goumlğuumls Ağrısı 208
Genel somatik ağrı 189
GI 161
Dispne 137
Mental durum değişiklikleri
128
12
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSDoctoral Student Graduate Institute of Nursing College of Nursing Taipei Medical University Taipei Taiwan Department of Nursing Cardinal Tien Junior College of Healthcare and Management Taipei TaiwanAIM The rapid growth of the elderly population has given rise to the need for better geriatric care The present study explored the common conditions of elderly outpatients with multiple physician visits in order to develop feasible clinical indicators that can be rapidly administered for the evaluation of geriatric syndromes in outpatient settingsMETHODS The National Health Insurance Research Database (2008) was analyzed Claims for elderly outpatients with more than two physician visits in the same day were retrieved The primary diagnoses types of prescriptions and comorbidities were cross-examinedRESULTS The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to 3940and which increased steadily with age A maximum of seven physician visits in a single day was observedThe most common multiple physician visit was two visits per day with a prevalence rate of 3097 The twomost common accompanying conditions were hypertension (379) and typethinsp2 diabetes mellitus (368)There was a greater relative increase in the prevalence of senile dementia and chronic obstructivepulmonary disease in older age groups The three overall leading specialties were cardiology internalmedicine and ophthalmology however rehabilitation medicine was the most common female-specificspecialty The most commonly prescribed medications were antihypertension drugs The most prevalentcomorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
13
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSRESULTS
The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to3940 and which increased steadily with age A maximum of seven physician visits in a single
day was observed The most common multiple physician visit was two visits per day with a
prevalence rate of 3097 The two most common accompanying conditions were hypertension (379) andtypethinsp2 diabetes mellitus (368) There was a greater relative increase in the prevalence of senile dementiaand chronic obstructive pulmonary disease in older age groups The three overall leading specialties werecardiology internal medicine and ophthalmology however rehabilitation medicine was the most commonfemale-specific specialty The most commonly prescribed medications were antihypertension drugs Themost prevalent comorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION
We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
14
Yaşlının Değerlendirilmesibull Metabolizmanın yavaşlaması ile ilgili sorunlarbull Strese karşı direncin azalması ile ilgili sorunlarbull Kognitif problemler ve bunların tıbbi ve davranışsal sonuccedillarıbull Polifarmasibull Sosyo-ekonomik sonuccedilların yarattığı sorunlarbull Koruyucu hekimlik
15
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist hastalıklarla normal yaşlanmanın etkilerini ayırt eder
ndash Boumlbrek fonksiyonlarında azalma yaşlanmanın bir parccedilasıyken boumlbrek yetmezliği ve inkontinans tedavi edilmelidir
9
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist olan hastalığı ve yaşlanmanın vuumlcut uumlzerindeki etkilerini tedavi ya da konsuumllte ederbull Bunun iccedilin hastayı ve sosyo ekonomik
koşullarını bir buumltuumln olarak ele alırhellip
10
Yaşlıya yaklaşım
bull Hor goumlrme
bull Normal yaşlanma
bull Normal-hastalık ayırımı
bull İletişim
ndash Anamnez alma
bull Sağlık uygulama tebliğleri
11
ACİLE BAŞ VURAN YAŞLILAR
Ohio Med 1991 Jul87(7)347-50 A biopsychosocial profile of the geriatric population who frequently visit the emergency department Brokaw M Zaraa AS
NEDEN
Ortalama Yaş 74
50 Psişik
Goumlğuumls Ağrısı 208
Genel somatik ağrı 189
GI 161
Dispne 137
Mental durum değişiklikleri
128
12
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSDoctoral Student Graduate Institute of Nursing College of Nursing Taipei Medical University Taipei Taiwan Department of Nursing Cardinal Tien Junior College of Healthcare and Management Taipei TaiwanAIM The rapid growth of the elderly population has given rise to the need for better geriatric care The present study explored the common conditions of elderly outpatients with multiple physician visits in order to develop feasible clinical indicators that can be rapidly administered for the evaluation of geriatric syndromes in outpatient settingsMETHODS The National Health Insurance Research Database (2008) was analyzed Claims for elderly outpatients with more than two physician visits in the same day were retrieved The primary diagnoses types of prescriptions and comorbidities were cross-examinedRESULTS The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to 3940and which increased steadily with age A maximum of seven physician visits in a single day was observedThe most common multiple physician visit was two visits per day with a prevalence rate of 3097 The twomost common accompanying conditions were hypertension (379) and typethinsp2 diabetes mellitus (368)There was a greater relative increase in the prevalence of senile dementia and chronic obstructivepulmonary disease in older age groups The three overall leading specialties were cardiology internalmedicine and ophthalmology however rehabilitation medicine was the most common female-specificspecialty The most commonly prescribed medications were antihypertension drugs The most prevalentcomorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
13
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSRESULTS
The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to3940 and which increased steadily with age A maximum of seven physician visits in a single
day was observed The most common multiple physician visit was two visits per day with a
prevalence rate of 3097 The two most common accompanying conditions were hypertension (379) andtypethinsp2 diabetes mellitus (368) There was a greater relative increase in the prevalence of senile dementiaand chronic obstructive pulmonary disease in older age groups The three overall leading specialties werecardiology internal medicine and ophthalmology however rehabilitation medicine was the most commonfemale-specific specialty The most commonly prescribed medications were antihypertension drugs Themost prevalent comorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION
We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
14
Yaşlının Değerlendirilmesibull Metabolizmanın yavaşlaması ile ilgili sorunlarbull Strese karşı direncin azalması ile ilgili sorunlarbull Kognitif problemler ve bunların tıbbi ve davranışsal sonuccedillarıbull Polifarmasibull Sosyo-ekonomik sonuccedilların yarattığı sorunlarbull Koruyucu hekimlik
15
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
Erişkin Tıbbından Farkıhelliphelliphellip
bull Geriatrist olan hastalığı ve yaşlanmanın vuumlcut uumlzerindeki etkilerini tedavi ya da konsuumllte ederbull Bunun iccedilin hastayı ve sosyo ekonomik
koşullarını bir buumltuumln olarak ele alırhellip
10
Yaşlıya yaklaşım
bull Hor goumlrme
bull Normal yaşlanma
bull Normal-hastalık ayırımı
bull İletişim
ndash Anamnez alma
bull Sağlık uygulama tebliğleri
11
ACİLE BAŞ VURAN YAŞLILAR
Ohio Med 1991 Jul87(7)347-50 A biopsychosocial profile of the geriatric population who frequently visit the emergency department Brokaw M Zaraa AS
NEDEN
Ortalama Yaş 74
50 Psişik
Goumlğuumls Ağrısı 208
Genel somatik ağrı 189
GI 161
Dispne 137
Mental durum değişiklikleri
128
12
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSDoctoral Student Graduate Institute of Nursing College of Nursing Taipei Medical University Taipei Taiwan Department of Nursing Cardinal Tien Junior College of Healthcare and Management Taipei TaiwanAIM The rapid growth of the elderly population has given rise to the need for better geriatric care The present study explored the common conditions of elderly outpatients with multiple physician visits in order to develop feasible clinical indicators that can be rapidly administered for the evaluation of geriatric syndromes in outpatient settingsMETHODS The National Health Insurance Research Database (2008) was analyzed Claims for elderly outpatients with more than two physician visits in the same day were retrieved The primary diagnoses types of prescriptions and comorbidities were cross-examinedRESULTS The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to 3940and which increased steadily with age A maximum of seven physician visits in a single day was observedThe most common multiple physician visit was two visits per day with a prevalence rate of 3097 The twomost common accompanying conditions were hypertension (379) and typethinsp2 diabetes mellitus (368)There was a greater relative increase in the prevalence of senile dementia and chronic obstructivepulmonary disease in older age groups The three overall leading specialties were cardiology internalmedicine and ophthalmology however rehabilitation medicine was the most common female-specificspecialty The most commonly prescribed medications were antihypertension drugs The most prevalentcomorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
13
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSRESULTS
The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to3940 and which increased steadily with age A maximum of seven physician visits in a single
day was observed The most common multiple physician visit was two visits per day with a
prevalence rate of 3097 The two most common accompanying conditions were hypertension (379) andtypethinsp2 diabetes mellitus (368) There was a greater relative increase in the prevalence of senile dementiaand chronic obstructive pulmonary disease in older age groups The three overall leading specialties werecardiology internal medicine and ophthalmology however rehabilitation medicine was the most commonfemale-specific specialty The most commonly prescribed medications were antihypertension drugs Themost prevalent comorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION
We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
14
Yaşlının Değerlendirilmesibull Metabolizmanın yavaşlaması ile ilgili sorunlarbull Strese karşı direncin azalması ile ilgili sorunlarbull Kognitif problemler ve bunların tıbbi ve davranışsal sonuccedillarıbull Polifarmasibull Sosyo-ekonomik sonuccedilların yarattığı sorunlarbull Koruyucu hekimlik
15
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
Yaşlıya yaklaşım
bull Hor goumlrme
bull Normal yaşlanma
bull Normal-hastalık ayırımı
bull İletişim
ndash Anamnez alma
bull Sağlık uygulama tebliğleri
11
ACİLE BAŞ VURAN YAŞLILAR
Ohio Med 1991 Jul87(7)347-50 A biopsychosocial profile of the geriatric population who frequently visit the emergency department Brokaw M Zaraa AS
NEDEN
Ortalama Yaş 74
50 Psişik
Goumlğuumls Ağrısı 208
Genel somatik ağrı 189
GI 161
Dispne 137
Mental durum değişiklikleri
128
12
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSDoctoral Student Graduate Institute of Nursing College of Nursing Taipei Medical University Taipei Taiwan Department of Nursing Cardinal Tien Junior College of Healthcare and Management Taipei TaiwanAIM The rapid growth of the elderly population has given rise to the need for better geriatric care The present study explored the common conditions of elderly outpatients with multiple physician visits in order to develop feasible clinical indicators that can be rapidly administered for the evaluation of geriatric syndromes in outpatient settingsMETHODS The National Health Insurance Research Database (2008) was analyzed Claims for elderly outpatients with more than two physician visits in the same day were retrieved The primary diagnoses types of prescriptions and comorbidities were cross-examinedRESULTS The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to 3940and which increased steadily with age A maximum of seven physician visits in a single day was observedThe most common multiple physician visit was two visits per day with a prevalence rate of 3097 The twomost common accompanying conditions were hypertension (379) and typethinsp2 diabetes mellitus (368)There was a greater relative increase in the prevalence of senile dementia and chronic obstructivepulmonary disease in older age groups The three overall leading specialties were cardiology internalmedicine and ophthalmology however rehabilitation medicine was the most common female-specificspecialty The most commonly prescribed medications were antihypertension drugs The most prevalentcomorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
13
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSRESULTS
The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to3940 and which increased steadily with age A maximum of seven physician visits in a single
day was observed The most common multiple physician visit was two visits per day with a
prevalence rate of 3097 The two most common accompanying conditions were hypertension (379) andtypethinsp2 diabetes mellitus (368) There was a greater relative increase in the prevalence of senile dementiaand chronic obstructive pulmonary disease in older age groups The three overall leading specialties werecardiology internal medicine and ophthalmology however rehabilitation medicine was the most commonfemale-specific specialty The most commonly prescribed medications were antihypertension drugs Themost prevalent comorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION
We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
14
Yaşlının Değerlendirilmesibull Metabolizmanın yavaşlaması ile ilgili sorunlarbull Strese karşı direncin azalması ile ilgili sorunlarbull Kognitif problemler ve bunların tıbbi ve davranışsal sonuccedillarıbull Polifarmasibull Sosyo-ekonomik sonuccedilların yarattığı sorunlarbull Koruyucu hekimlik
15
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
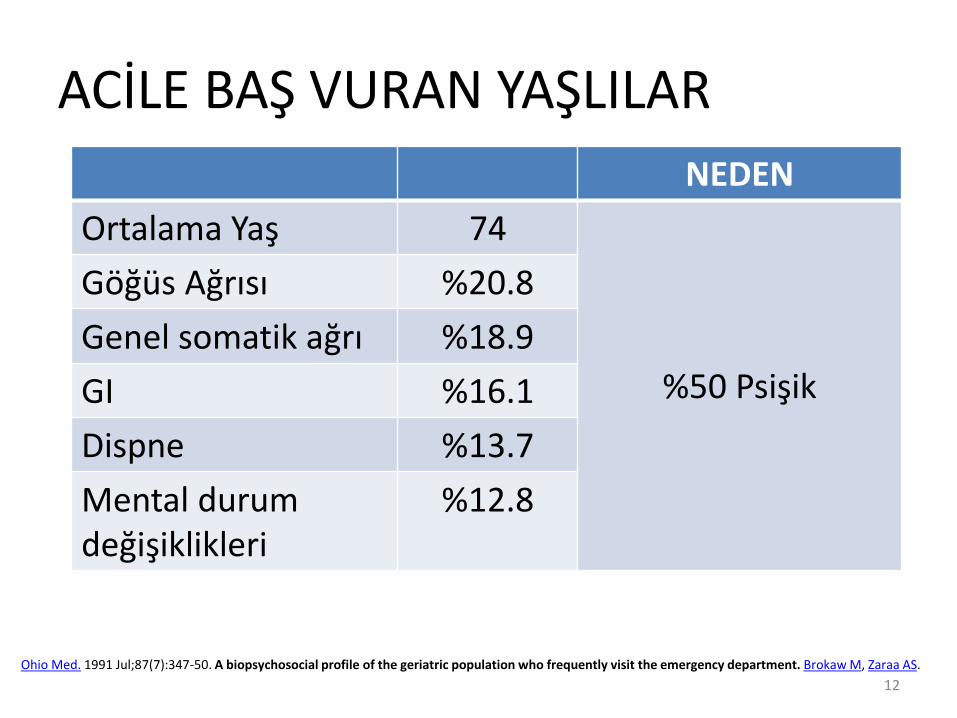
ACİLE BAŞ VURAN YAŞLILAR
Ohio Med 1991 Jul87(7)347-50 A biopsychosocial profile of the geriatric population who frequently visit the emergency department Brokaw M Zaraa AS
NEDEN
Ortalama Yaş 74
50 Psişik
Goumlğuumls Ağrısı 208
Genel somatik ağrı 189
GI 161
Dispne 137
Mental durum değişiklikleri
128
12
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSDoctoral Student Graduate Institute of Nursing College of Nursing Taipei Medical University Taipei Taiwan Department of Nursing Cardinal Tien Junior College of Healthcare and Management Taipei TaiwanAIM The rapid growth of the elderly population has given rise to the need for better geriatric care The present study explored the common conditions of elderly outpatients with multiple physician visits in order to develop feasible clinical indicators that can be rapidly administered for the evaluation of geriatric syndromes in outpatient settingsMETHODS The National Health Insurance Research Database (2008) was analyzed Claims for elderly outpatients with more than two physician visits in the same day were retrieved The primary diagnoses types of prescriptions and comorbidities were cross-examinedRESULTS The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to 3940and which increased steadily with age A maximum of seven physician visits in a single day was observedThe most common multiple physician visit was two visits per day with a prevalence rate of 3097 The twomost common accompanying conditions were hypertension (379) and typethinsp2 diabetes mellitus (368)There was a greater relative increase in the prevalence of senile dementia and chronic obstructivepulmonary disease in older age groups The three overall leading specialties were cardiology internalmedicine and ophthalmology however rehabilitation medicine was the most common female-specificspecialty The most commonly prescribed medications were antihypertension drugs The most prevalentcomorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
13
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSRESULTS
The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to3940 and which increased steadily with age A maximum of seven physician visits in a single
day was observed The most common multiple physician visit was two visits per day with a
prevalence rate of 3097 The two most common accompanying conditions were hypertension (379) andtypethinsp2 diabetes mellitus (368) There was a greater relative increase in the prevalence of senile dementiaand chronic obstructive pulmonary disease in older age groups The three overall leading specialties werecardiology internal medicine and ophthalmology however rehabilitation medicine was the most commonfemale-specific specialty The most commonly prescribed medications were antihypertension drugs Themost prevalent comorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION
We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
14
Yaşlının Değerlendirilmesibull Metabolizmanın yavaşlaması ile ilgili sorunlarbull Strese karşı direncin azalması ile ilgili sorunlarbull Kognitif problemler ve bunların tıbbi ve davranışsal sonuccedillarıbull Polifarmasibull Sosyo-ekonomik sonuccedilların yarattığı sorunlarbull Koruyucu hekimlik
15
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSDoctoral Student Graduate Institute of Nursing College of Nursing Taipei Medical University Taipei Taiwan Department of Nursing Cardinal Tien Junior College of Healthcare and Management Taipei TaiwanAIM The rapid growth of the elderly population has given rise to the need for better geriatric care The present study explored the common conditions of elderly outpatients with multiple physician visits in order to develop feasible clinical indicators that can be rapidly administered for the evaluation of geriatric syndromes in outpatient settingsMETHODS The National Health Insurance Research Database (2008) was analyzed Claims for elderly outpatients with more than two physician visits in the same day were retrieved The primary diagnoses types of prescriptions and comorbidities were cross-examinedRESULTS The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to 3940and which increased steadily with age A maximum of seven physician visits in a single day was observedThe most common multiple physician visit was two visits per day with a prevalence rate of 3097 The twomost common accompanying conditions were hypertension (379) and typethinsp2 diabetes mellitus (368)There was a greater relative increase in the prevalence of senile dementia and chronic obstructivepulmonary disease in older age groups The three overall leading specialties were cardiology internalmedicine and ophthalmology however rehabilitation medicine was the most common female-specificspecialty The most commonly prescribed medications were antihypertension drugs The most prevalentcomorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
13
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSRESULTS
The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to3940 and which increased steadily with age A maximum of seven physician visits in a single
day was observed The most common multiple physician visit was two visits per day with a
prevalence rate of 3097 The two most common accompanying conditions were hypertension (379) andtypethinsp2 diabetes mellitus (368) There was a greater relative increase in the prevalence of senile dementiaand chronic obstructive pulmonary disease in older age groups The three overall leading specialties werecardiology internal medicine and ophthalmology however rehabilitation medicine was the most commonfemale-specific specialty The most commonly prescribed medications were antihypertension drugs Themost prevalent comorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION
We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
14
Yaşlının Değerlendirilmesibull Metabolizmanın yavaşlaması ile ilgili sorunlarbull Strese karşı direncin azalması ile ilgili sorunlarbull Kognitif problemler ve bunların tıbbi ve davranışsal sonuccedillarıbull Polifarmasibull Sosyo-ekonomik sonuccedilların yarattığı sorunlarbull Koruyucu hekimlik
15
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
Geriatr Gerontol Int 2013 Jul 1 doi 101111ggi12111 [Epub ahead of print]Profile of elderly with multiple physician visits Advocacy for tailored comprehensive geriatric assessment use in clinics Kuo MC Jeng C Chen CM Jian WSRESULTS
The overall prevalence rate for elderly patients with multiple physician visits ranged from 2841 to3940 and which increased steadily with age A maximum of seven physician visits in a single
day was observed The most common multiple physician visit was two visits per day with a
prevalence rate of 3097 The two most common accompanying conditions were hypertension (379) andtypethinsp2 diabetes mellitus (368) There was a greater relative increase in the prevalence of senile dementiaand chronic obstructive pulmonary disease in older age groups The three overall leading specialties werecardiology internal medicine and ophthalmology however rehabilitation medicine was the most commonfemale-specific specialty The most commonly prescribed medications were antihypertension drugs Themost prevalent comorbidity was typethinsp2 diabetes mellitus and hypertensionCONCLUSION
We conclude that our data represent crucial information for the design of concise assessment metrics for application to the most chronic conditions in an effort to implement better geriatric healthcare Geriatr Gerontol Int 2013
14
Yaşlının Değerlendirilmesibull Metabolizmanın yavaşlaması ile ilgili sorunlarbull Strese karşı direncin azalması ile ilgili sorunlarbull Kognitif problemler ve bunların tıbbi ve davranışsal sonuccedillarıbull Polifarmasibull Sosyo-ekonomik sonuccedilların yarattığı sorunlarbull Koruyucu hekimlik
15
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
Yaşlının Değerlendirilmesibull Metabolizmanın yavaşlaması ile ilgili sorunlarbull Strese karşı direncin azalması ile ilgili sorunlarbull Kognitif problemler ve bunların tıbbi ve davranışsal sonuccedillarıbull Polifarmasibull Sosyo-ekonomik sonuccedilların yarattığı sorunlarbull Koruyucu hekimlik
15
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
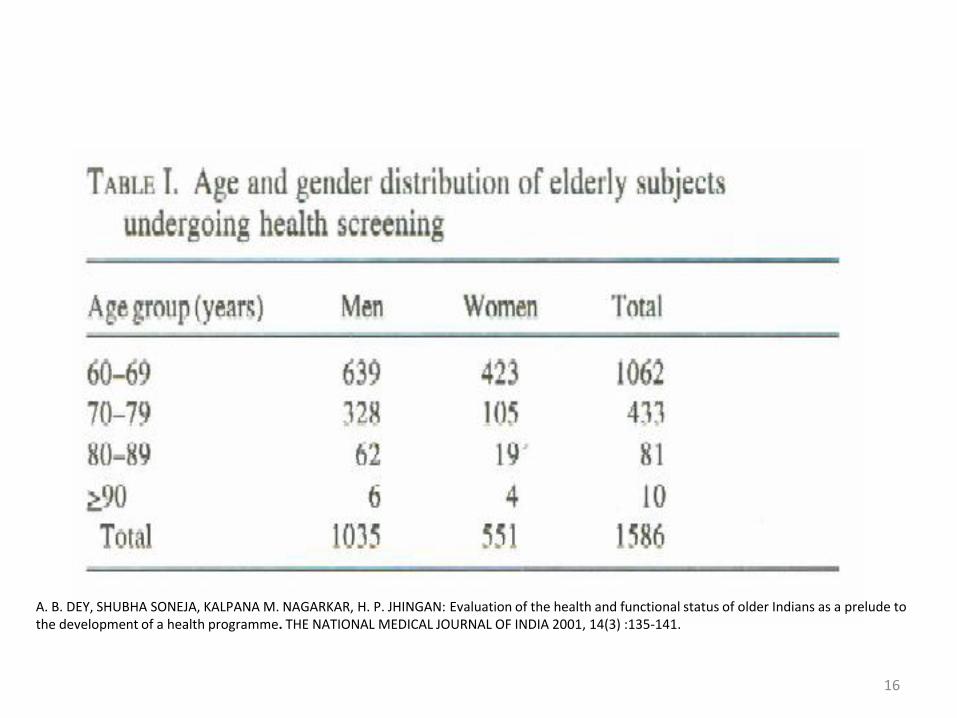
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
16
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
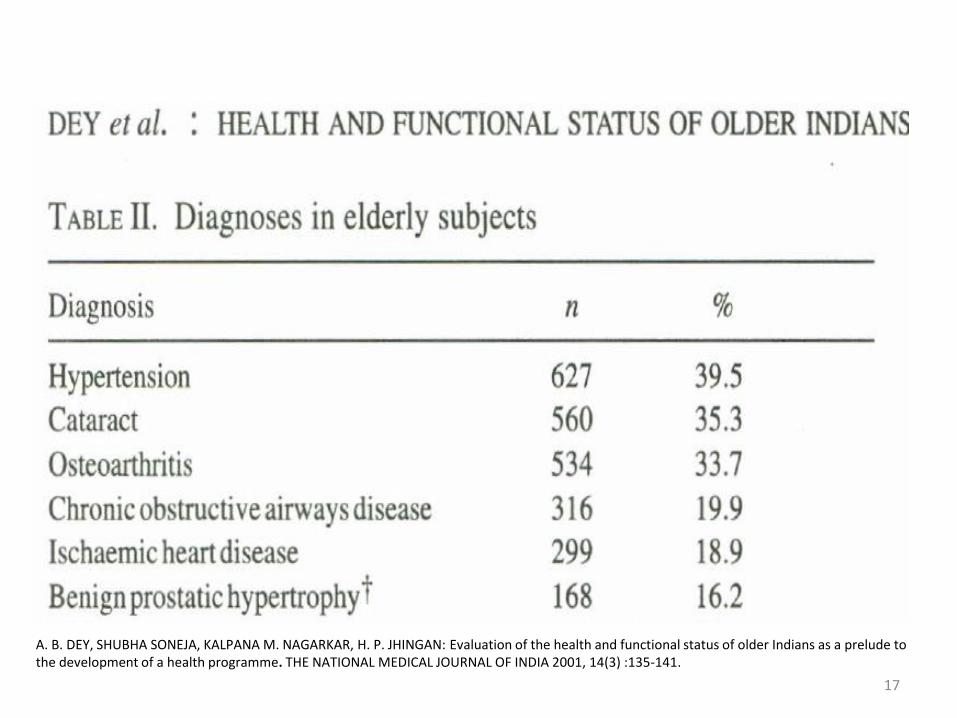
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
17
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
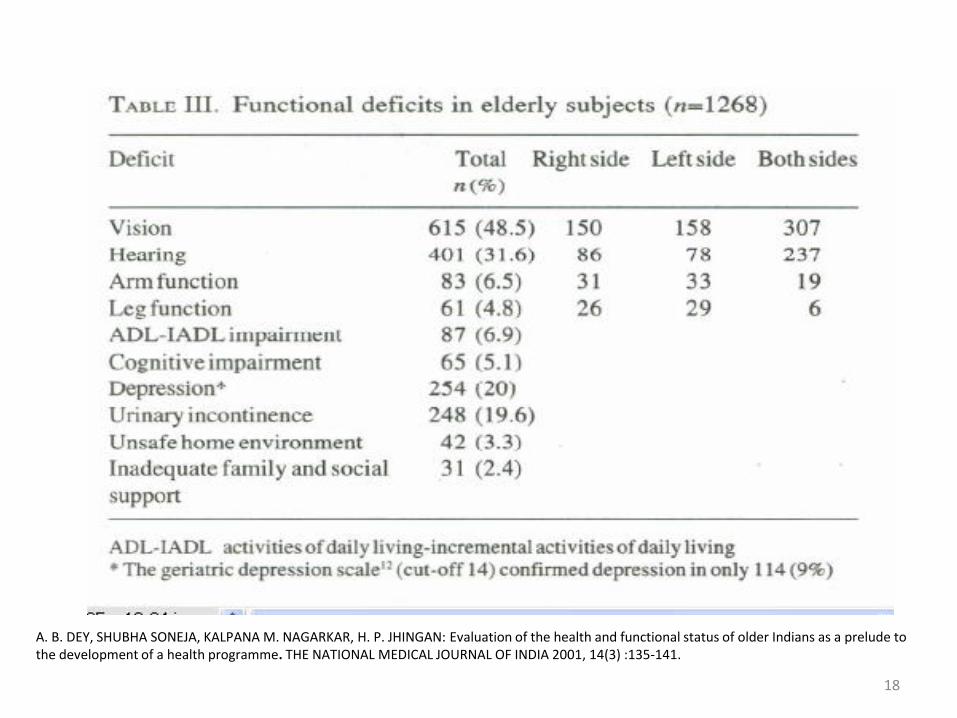
A B DEY SHUBHA SONEJA KALPANA M NAGARKAR H P JHINGAN Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme THE NATIONAL MEDICAL JOURNAL OF INDIA 2001 14(3) 135-141
18
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
Geriatrik tıbbın farklı oumlzellikleri
ndash Karmaşık
ndash Geriatride sık rastlanan semptomlar
ndash Homeostenozis
ndash Multidisipliner ekip ccedilalışması
ndash Ailenin katkısı
ndash Kuumlltuumlruumln uygulamadaki roluuml
ndash Tıbbi etik
19
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
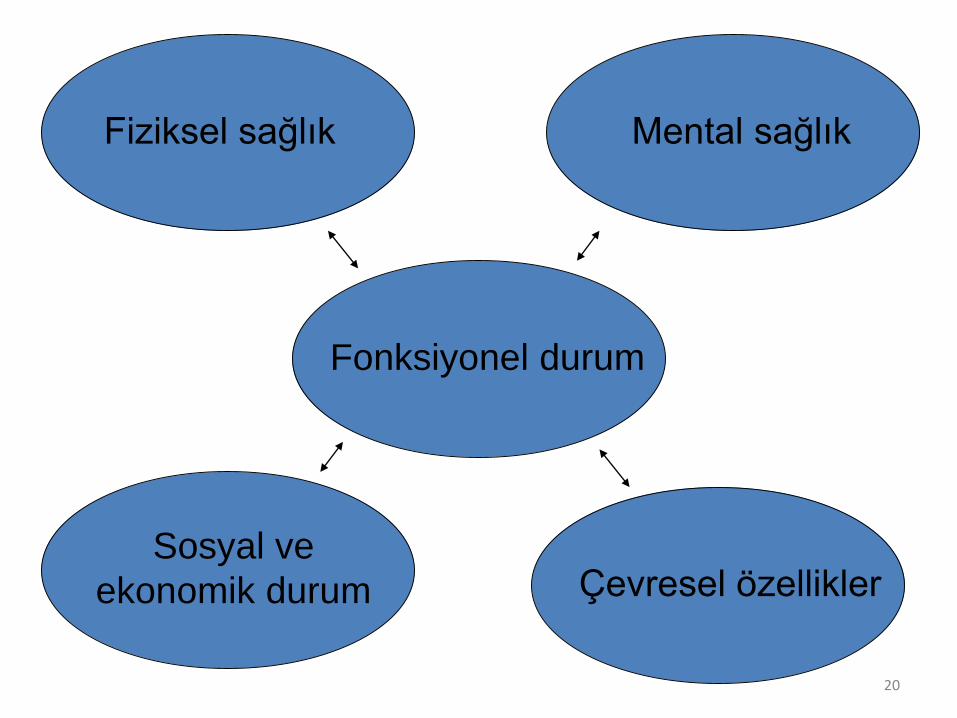
Fiziksel sağlık Mental sağlık
Fonksiyonel durum
Sosyal ve
ekonomik durum Ccedilevresel oumlzellikler
20
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
Değerlendirme suumlreci
bull Riskli popuumllasyonun belirlenmesi
bull Tıbbi ekip uumlyeleri ve konsuumlltanların belirlenmesi
bull Verilerin toplanması ve gerekli planlamalar
bull Planların uygulanması ve gelişmelerin takibi
21
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
Hedef Kitle
bull Kırılgan Yaşlılar
ndash Yedek kapasiteleri ccedilok sınırlı olup hızla
azalarak disfonksiyonlar ortaya ccedilıkabilir ve
yaşlı bağımsızlığını kaybedebilir
ndash Hastaneye yatırılma riskleri yuumlksek hastane
ve bakım evlerinde kalış suumlreleri uzun
22
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
Hedef Kitle
bull Hastaneye yatma ihtimali fazla olan
hastalar
ndash Birlikte bulunan problemlerin sayısı
ndash Kullandığı ilaccedilların sayısı
ndash Fonksiyonel kısıtlılıkların sayısı
bull 75 yaş ve uumlzerindeki yaşlılar
23
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
Fiziksel sağlık
bull Oumlncelikle hastanın başvurusuna neden olan şikayetler
bull Diğer sık rastlanan hastalıklarbull Goumlrme
bull İşitme
bull Yuumlruumlme ve denge
bull Beslenme
bull Kontinans
bull Geriatrik sendromlar24
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
bull Koruyucu hekimlik
bull Sağlıklı yaşlanma oumlzuumlrluumlluumlğuuml oumlnleme-geciktirme
bull Kronik hastalıklarla muumlcadele
bull Sık rastlanan hastalıkların tedavisi
bull Rehabilitasyon
25
YAŞLININ BAĞIMSIZLIĞININ DEVAMININ SAĞLANMASI İCcedilİN
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26
The American Geriatrics Society (AGS) is a not-for-profit organization of over 6000 health professionals devoted to improving the health independence and quality of life of all older people The Society provides leadership to healthcare professionals policy makers and the public by implementing and advocating for programs in patient care research professional and public education and public policy
Our MissionTo improve the health independence and quality of life of all older people
Our Vision for the FutureEvery older American will receive high quality patient-centered care
The American Geriatrics Society (AGS)
26