Embed Size (px)
Citation preview

MANAGEMENT OF POST-ERCP
DUODENAL PERFORATION Magda Recsky
Sept 18, 2012

PATIENT JB
July 13, 2012
43 yr F – JW – history of vague RUQ pain;
investigations including U/S and CT scan
Dilated duct demonstrated: 14.8mm on U/S but
only ~7-8mm on CT
July 13, 2012: ERCP
Diverticulum noted at ampulla
No filling defect; no stone with balloon sweep
GB and cystic duct not visualized
Sphincterotomy conducted

INITIAL CONSULT
July13 – increasing pain
post ERCP
AXR and CXR and CT -
pneumomediastinum
small amount of free air
medially involving the
right inferior hemithorax
free air along the right
perihepatic space
retroperitoneal air
Patient hemodynamically stable; normal T; HR
50-60; improved pain on assessment

JULY 14
Worsening pain
Tachycardia
Increasing WBC
Decision made to take to OR
INTRA-OP FINDINGS
Bile-stained RUQ
Kocherize duodenum with exploration – unable
to identify site of perforation

WHAT WE DID
Pyloric exclusion with gastrotomy, oversew
pylorus
Roux-en-Y gastrojejunostomy using gastrotomy
Cholecystectomy
Drained widely

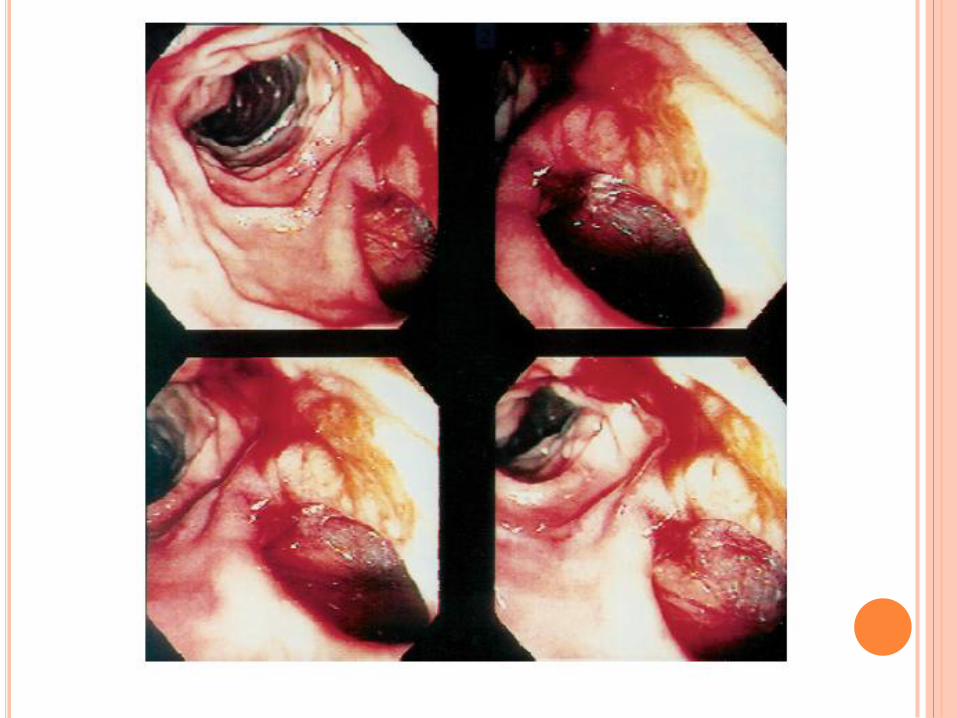
CLASSIFICATION OF DUODENAL INJURIES:
POST-ERCP
Type I – lateral
Type II – peri-
ampullary
Type III – CBD
injury
Type IV – only
retroperitoneal air
Stapfer M et al. Management of duodenal perforation after endoscopic retrograde cholangiopancreaticography and sphincterotomy. Am Surg 2000.

WHAT DOES THE LITERATURE TELL US?
No consensus on management guidelines and
selection criteria for surgery or conservative
management
Recommendations based on anecdotes and small
case series
MACHADO 2012
Literature review 2000 onwards (not a formal
systematic review) of reports that contained 9 or
more cases of post-ERCP perforations
251 cases in 10 reports
Mean age: 58.5
Locations of perforations:
Duodenal wall: 34.5%
Periamullary: 31.3%
CBD: 23%
Unknown: 7.9%


MACHADO 2012
Conservative management: 62.2% (156)
93% successful (145)
Surgical management: (not exclusive)
Primary closure: 49% (+/- other procedures)
Retroperitoneal drainage: 39%
Duodenal exclusion: 24%
CBD exploration and T-tube insertion: 13%
Overall mortality: 8% (20 patients)
6 (30%) – salvage surgery
5 (25%) – delay in diagnosis/intervention >3 days
3 (15%) – multiple surgeries
sepsis

TYPES OF PROCEDURES
Closure of perforation
T-tube insertion
Choledocholithotomy
Tube duodenostomy
Gastrojejunostomy
Retroperitoneal drainage
Duodenal exclusion
Choledochojejunostomy
Duodenogastrectomy

MACHADO 2012 - CONCLUSIONS
Conclusions:
“The most important factors for recent better
outcome were early detection and prompt
treatment. Delay in diagnosis and intervention,
salvage surgery after failed conservative
management, multiple operations, and older age
group contributed significantly to the poor
outcome.”

Delay in treatment well documented in literature
to result in increased morbidity and mortality
Howard TJ et al. Surgery 1999
Krishna RP et al. Surg Today 2011
Lai CH et al. Surgeon 2008
Avgerinos et al. Surg Endosc 2009
Mao Z et al. J LaproendoscAdvSurg Tech 2008
Morgan KA et al. Am Surg 2009
Etc…

DECISION TREE
Conservative vs Operative
Patient’s condition
Mechanism of injury
Site of injury
Site and mechanism (scope vs due to
sphincterotomy etc) may not always be possible
All require NG drainage/decompression
If decide on operative management – then need
to decide what to do

CLINICAL SIGNS AND SYMPTOMS
Epigastric pain and back pain (more intense than
usual)
Tenderness with or without peritoneal signs
(generally rebound tenderness)
Emphysema,
Later:
Tachycardia – constant finding by very sensitive and
not specific
Fever
Leukocytosis – often seen 12 hours or more after
completion of ERCP

SITE OF INJURY
Type I (lateral wall)
Require surgical intervention
Debridement of devitalized tissue
Primary closure in 1 or 2 layers (transversely)
If slightly larger and can’t close – consider a jejunal
serosal patch
If large, treat just like a traumatic
injury with pyloric exclusion and
diversion

DUODENAL DIVERSION TECHNIQUES
Tube decompression
Controversial – may not adequately decompress; may
cause new perforations
Duodenal diverticulization
Billroth II gastrectomy + closure of duodenal wound
+ duodenal catheter to decompress + multiple drains
+/- biliary drainage
Extensive procedure especially in hemodynamically
unstable patient
Pyloric exclusion
Repair of duodenal wound + closure of pylorus
(through gastrotomy or with stapler) + side-to-side
gastrojejunostomy

SITE OF INJURY
Type II (peri-amullary) and Type III (CBD)
Often contained and can be managed non-operatively NG; NPO; broad spectrum antibiotics
Often when type II perforations treated operatively – site of perforation could not be identified
Some advocate diversion of biliary flow in all Type II and Type III Percutaneous transhepatic biliary drainage
Internal biliary stent
Indications for operative management: Failure of non-op
Ongoing leakage
Peritoneal signs
? Large free or retroperitoneal collection Fatima J et al. Arch Surg 2007
Knudson K et al. Am J Surg 2008

MACHADO ET AL – FINAL CONCLUSIONS
“The optimal operation for ERCP induced duodenal perforation appears to be primary repair and duodenal diversion with gastrojejunostomy and pyloric exclusion.
However, if the perforation is noted and managed early, primary repair without diversion has similar results, provided the peritoneal contamination is minimal.
While patients with type I perforation would invariably require immediate surgical intervention, those with type II or III may often be managed conservatively. However, they would require constant observation supported by radiological investigation to confirm satisfactory progress failing which they may require surgical intervention.”

STAPFER ET AL 2000
Recommend that all patients with type I injuries
undergo surgery immediately
Nonsurgical management for type II and III injuries
is acceptable if early contrast study shows:
minimal extravasation OR
a sealed perforation without associated fluid collections
Type IV: probably need no additional treatment or
workup if the findings of the abdominal examination
are normal and there is no evidence or suspicion of
contrast extravasation
Type II, III, or IV injuries with retained stones and
unrelieved bile obstruction or foreign bodies should be
explored in the absence of other indications


WU ET AL.
1996-2002 – 6620 ERCPs performed
30 perforations (0.45%)
Type I: 3
Type II: 11
Type III: 7
Type IV: 0
Unknown: 7
Esophageal: 1
Afferent limb in previous Billroth II: 1
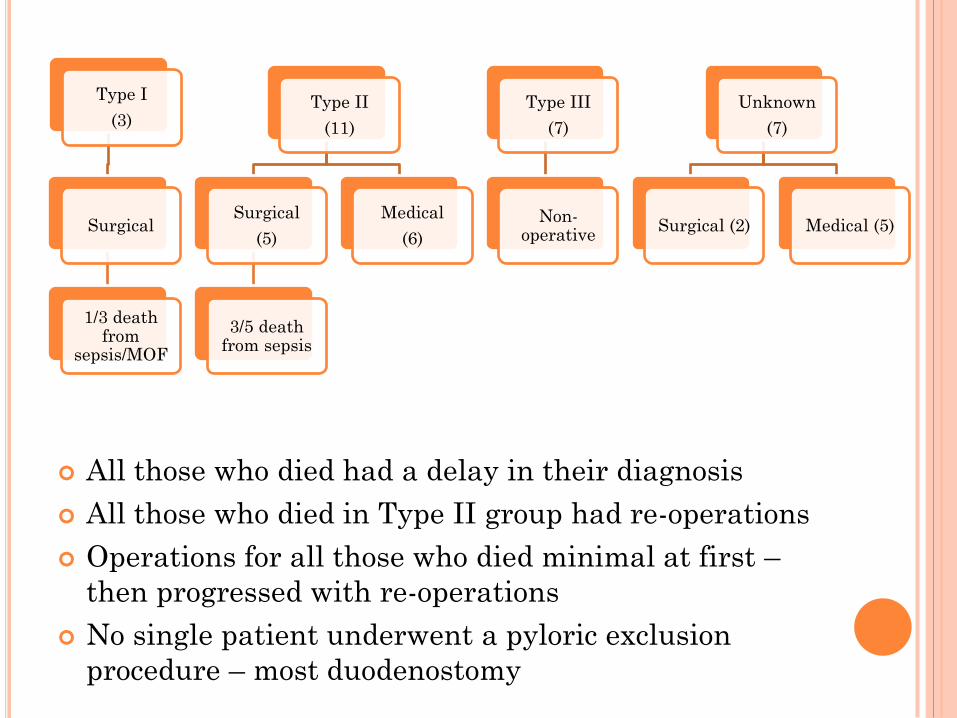
All those who died had a delay in their diagnosis
All those who died in Type II group had re-operations
Operations for all those who died minimal at first –
then progressed with re-operations
No single patient underwent a pyloric exclusion
procedure – most duodenostomy
Type I
(3)
Surgical
1/3 death from
sepsis/MOF
Type II
(11)
Surgical
(5)
3/5 death from sepsis
Medical
(6)
Type III
(7)
Non-operative
Unknown
(7)
Surgical (2) Medical (5)


FATIMA ET AL 2007
1994-2004
12,427
75 perforations identified (0.6%)
0.1% for diagnostic
0.8% for therapeutic
Overall mortality for those with peri-ampullary
perforations (Type II): 7%
Operative group (n=22) mortality: 13%
Non-operative group (n=53) mortality: 4%
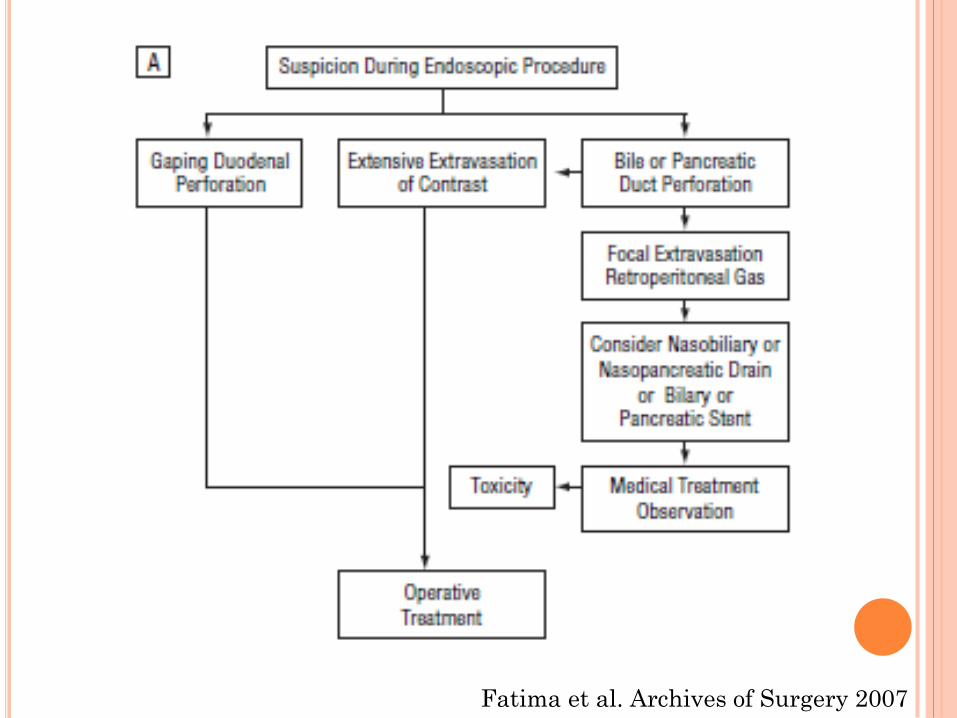
Fatima et al. Archives of Surgery 2007

Fatima et al. Archives of Surgery 2007




PATIENTJB
POD #3: UGI study – gastrojej intact; distal
anastomosis intact; no contrast extravasation
POD #6: OR for sepsis – sudden deterioration in
SCCU
Washout; more drains
Feeding J-tube
Packs left in RUQ
POD #8: OR: packs removed; no evidence of
further contamination

POD #16: OR for sepsis; ongoing bile from drains
Large hole identified in duodenum
Melecot drain used for duodenostomy
More drains
Ongoing bile from drains
Ongoing sepsis
Died on POD #25 (26 days post ERCP)

ADDITIONAL THOUGHTS
No delay in treatment
Definitive operation first time
?Role for percutaneous decompression of biliary
tree

TYPE IV PERFORATION
Retroperitoneal air only
“Common benign finding after endoscopic sphincterotomy and had no predictive value in identifying patients who requires intervention”
13 to 29% incidence of inconsequential retroperitoneal air in several prospective studies
Stapfer M et al. Am Surgery 2000
Machado. J Pancreas 2012
Genzlinger JL et al. Gastroenterol 1999
de Vries JH et al. Endoscopy 1997