Embed Size (px)
Citation preview

6Z J O U R N A L O F T H E F A C U L T Y O F R A D I O L O G I S T S
MECONIUM PERITONITIS
BY T. L. C. PRATT, M.R.C.S., L.R.C.P., D.M.R.D. HALIFAX AND HUDDERSFIELD HOSPITAL GROUPS
MECONIUM peritonitis is an uncommon condition which may be encountered in the newborn infant. I t can be defined as a sterile reaction of the peritoneum to the presence of meconium. A perforation in the wall of the intestine is, of course, essential.
Perforation of the gut can occur before, during, or after birth from the more obvious types of obstruction, viz., congenital atresia, intussusception, peritoneal bands, and volvulus.
Meconium ileus as a cause of obstruction was described by Landsteiner (I9o5). I t seems that the condition is only found when there is fibrosis of the pancreas and a consequent lack of pancreatic
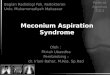
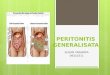
Fig. 73.--A, Free gas in the peritoneum delineates the under-surface of the r ight dome of the diaphragm and three fluid levels are present in peritoneal loculi. B, A single large fluid level is seen and is distinct from visible intestinal shadows.
secretion in the meconium. The meconium is A rendered sticky and ' pu t ty - l i ke ' and, adhering to
the walls of the gut, produces obstruction. A similar chain of events can take place in the presence of a congenital stenosis of the pancreatic du& (Kornblith and Otani, i929).
Other cases occur where no obstruction is present and yet the gut has perforated. In many of these the cause of the perforation is obscure. Boikan (i93o) described a case of perforation of the terminal ileum and suggested persistence of foetal antimesenteric diverticula with excessive surrounding lymphatic tissue hypertrophy as the cause.
Zillner (i884) considered that trauma was of the utmost importance in his case of rupture of the sigmoid flexure.
Intestinal peristalsis commences at the fourth or fifth month of foetal life. Perforation of the gut may occur after this time or later, during birth, or immediately after birth.
Meconium floods the peritoneum and a sterile peritonitis ensues. Loops of gut become matted together and bound down by dense adhesions. The perforation may persist and remain patent or it may become sealed off and often impossible to detect at operation or autopsy.

M E C O N I U M P E R I T O N I T I S 63
Radiologically the case may present in one of four ways : - - I. Intestinal obstruction, occurring shortly after birth, where the perforation has become
sealed. Meconium peritonitis may be suspected but there are no diagnostic radiological criteria. 2. Calcium deposits in the peritoneal cavity with or without obstruction of the intestinal tract
or evidence of perforation of the gut. These calcium deposits are an important diagnostic feature. Neuhauser (1944) reported 3 cases where the calcifications made diagnosis possible prior to opera- tion. Calcifications m a y form within twenty-four hours of perforation (Litten). Brunkow and
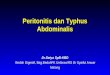
A B Fig. 74 . - -A, T h e dissected colon. T h e arrow indicates the perforation in the antimesenteric border of the mid-transverse colon.
B, T h e perforation in the mid- t ransverse colon with ' pout ing ' mucosa.
others (I949) describe a similar case, which was successfully operated upon, in which the calcifica- tions had disappeared twenty months later.
3. A single large fluid level in the peritoneal cavity.--This occurs where the perforation is so recent that adhesions have not yet had time to form.
4. Multiple fluid levels within the peritoneal cavity.--In these cases a plastic peritonitis is present with a patent perforation of the gut. A cursory glance at the film may suggest multiple fluid levels in dilated loops of gut. Further inspection, however, should clearly show that fluid levels lie in peritoneal loculi for the following reasons : - -
a. Gut mucosal pattern is absent within the loculi. b. Gas may delineate the superior surface of the liver and the inferior aspect of the diaphragm
or some other abdominal organ (e.g., spleen). c. The general disposition of the fluid levels may be at variance with the configuration expected
with intestinal obstruction. Many children with meconium peritonitis are born dead, others survive a few days with
intestinal obstruction or perforation. The general condition of the majority is too poor for surgery. However, Low, Cooper, and Cosby (1949) reported a case which was diagnosed radiologically and at operation an intestinal obstruction and perforation were circumvented by anastomosis, with apparent cure thirty-seven weeks later. Another case reported by Brunkow and others (I949) , in which radiography revealed diagnostic abdominal calcifications, was successfully treated by surgery. Franklin and Hosford (I952) describe 2 cases which they treated successfully and stress the importance of early diagnosis and treatment within forty-eight hours. Normal intestinal bacteria appear after three or four days of life, thus converting the sterile condition into an infective peritonitis which diminishes the chances of survival.

64 J O U R N A L O F T H E F A C U L T Y O F R A D I O L O G I S T S
CASE R E P O R T S Case I.--_An example of Category 4 of the above classification. Baby H. , male, we igh ing 5 lb. 6 oz., del ivered normal ly on Sept. 22, 195o. His a b d o m e n was d i s tended
owing to ascites. O n Sept. 23 the abdomina l c i rcumference measu red 14 in. A diagnosis of ' rhesus baby ' was d isproved
and the aetiology of the d is tended a b d o m e n was reconsidered. O n Sept. 24 X- r ay examina t ions revealed large fluid levels in the per i toneal cavity, indicat ing peri toneal
adhesions and a perfora t ion in the a l imentary tract (Fig. 73). A paracentes is abdominis conf i rmed the presence of gas and mecon i um.
T h e chi ld 's condi t ion was too poor for laparotomy. He f requent ly vomi t ed dark b rown flaky fluid and, on two occasions, a small stool was passed. He was fed via a gastr ic tube.
O n Sept. 26 the abdomina l g i r th was 17 in. He became increasingly cyanosed and died on Sept. 27, weighing 7 lb. 8 oz.
At autopsy, gas and ye l lowish-brown f~ecal mater ia l escaped f rom the peri toneal cavity. Extens ive peri- toneal adhesions were p resen t and the gut was mat ted together and b o u n d down in the uppe r abdomen . O n dissection a perforat ion wi th pou t ing mucosa was revealed in the mid - t r ansve r se colon (Fig. 74). T h e r e was no evidence of intest inal obstruct ion. Unfor tuna te ly , the pancreas was not examined microscopically.
Case 2 . - - T h i s case has been fully repor ted by N a s h and Smi th (1952). T h e radiographic appearances were similar to those seen in Case i . Nec ropsy revealed a perforat ion
proximal to the splenic flexure of the colon. T h e residual m e c o n i u m in the in tes t ine appeared abnormal to the naked eye and the pancreas exhibi ted a severe degree of fibrocystic disease histologically.
S U M M A R Y
~. A brief survey of meconium peritonitis. 2. Radiological signs presenting in this condition are evaluated. 3. One case is fully described.
I wish to thank Dr. W. Niven for his help in preparing this paper and Dr. R. I. Lewis for his interest and permission to publish the films.
R E F E R E N C E S
BOIKAN, W. S. (I93O), Arch. Path., 9, I I64. BaUNKOW, C. W., and others ( i949) , West J. Surg., 57, 424. FRANKLIN, A. W. , and HOSFORIS, J. P. (I952), Brit. med. J., 2, 257. KORNBLITH, B. A., and OTANI, S. (I929), Amer. J. Path., 5, 249. LANDSTEINER, K. (19o5) , Zbl. allg. Path. path. Anat., x6, 9o3. LITTEN, cited by RUDNEW. L o w , J. R., COOPER, G., and COSBY, L., jun . (I949), Surgery, 26, 223. NASH, F. W. , and SMITH, J. F. (1952), Arch. Dis. Childh., I 3 I , 73. NEUHAUSER, E. B. D. (I94-4) , Amer. J. Roentgenol., 5I, 42I . RUDNEW, W. (I915) , Ueber die spontanen Darmrupturen die Foeten und Neugeborenen. ZILLNER, E. (I884), Virchows Arch., 96, 307.
Basel.
E R R A T U M
VOL. 4, No. 4, April, I953, A. S. Whitehead : " The Determination of the Placental Site by Soft- tissue Radiography ", page 250 , line 5, for thick read thin.