-
8/22/2019 Melanoma 0003
1/53
Melanoma
Edward Buckingham, M.D.
Combined Plastics ConferenceSeptember 6, 2000
-
8/22/2019 Melanoma 0003
2/53
Melanoma - Outline
General statistics and development Risk factors and patient
assessement
Pathology and prognosis Work-up and staging
Surgical treatment
Lymph node controversy/sentinel node
Adjuvant therapy
-
8/22/2019 Melanoma 0003
3/53
Melanoma - Data
Incidence increase fastest Mortality increase 2nd only to
lung
5th most prevalent, incidence 7%/yearincrease
5% skin cancer, 75% skin cancer death
1/75 in 2000, 1/1500 in 1935
20% H&N, 51% facial, 26% scalp, 16%
neck, 9% ear
-
8/22/2019 Melanoma 0003
4/53
Development of Nevi
Melanocytes dendritic, neural crest, basal cell layer
synthesis of melanin
1/10 to keratinocytes
hyperplasia- tanning/lentigines, increased ratio
Nevus transformation poorly understood
dendritic- rounded
no longer lentigionous pattern- nests
-
8/22/2019 Melanoma 0003
5/53
Development of Nevi
Junctional nevi nests along dermal-epidermal junction
Compound nevi
invade dermis, first as nests then cords and
single cells
Dermal nevi junctional component lost
-
8/22/2019 Melanoma 0003
6/53
Evolution of Nevi
-
8/22/2019 Melanoma 0003
7/53
Melanocyte Hyperplasia
-
8/22/2019 Melanoma 0003
8/53
Junctional Nevi
-
8/22/2019 Melanoma 0003
9/53
Compound Nevi
-
8/22/2019 Melanoma 0003
10/53
Dermal Nevi
-
8/22/2019 Melanoma 0003
11/53
Developement of Melanoma
Questionable benign melanocytes
progressive hyperplasia/dysplasia
Radial growth
in epidermis, lines of radii, no expansive nests
or nodules slow unrestricted , no metastatic potential
-
8/22/2019 Melanoma 0003
12/53
Development of Melanoma
Vertical growth vertically into dermis
expansive and coalescent nests and nodules
metastatic potential dermal lymphatic and
vascular invasion
Growth patterns biphasic- slow radial months to years- rapid
vertical growth
monophasic- rapid vertical growth only
-
8/22/2019 Melanoma 0003
13/53
Evolution of Melanoma
-
8/22/2019 Melanoma 0003
14/53
Dysplastic Nevi
border melanocytic nevi and malignantmelanoma
clinical resembles malignant melanoma
lentiginous compound nevus, prominent
bridging across rete ridges
aberrant in inter-rete spaces lamellar fibrosis of papillary
dermis,
variable lymphoid response
-
8/22/2019 Melanoma 0003
15/53
Dysplastic Nevi
-
8/22/2019 Melanoma 0003
16/53
Dysplastic Nevi
-
8/22/2019 Melanoma 0003
17/53
Types of Melanoma
Acral lentiginous Mucosal melanoma
Superfical spreading melanoma
Lentigo maligna melanoma
Nodular melanoma
-
8/22/2019 Melanoma 0003
18/53
Superficial spreading
most common head and neck, 50% 4th to 5th decade
clinical mixture of brown/tan, pink/white
irregular borders, biphasic growth
irregular nests in epidermis
underlying lymphoid infiltrate
enlarged nests and single cells in all
epidermal layers
-
8/22/2019 Melanoma 0003
19/53
Superficial spreading
-
8/22/2019 Melanoma 0003
20/53
Lentigo maligna
20% of head and neck longest radial growth phase >15 yrs
elderly sun exposed areas
clinical dark, irregular ink spot
contiguous lintiginous proliferation,
dyshesive, variable shape, atrophicepidermis, infundibular basal
cell layer of
hair follicles
-
8/22/2019 Melanoma 0003
21/53
Lentigo maligna
-
8/22/2019 Melanoma 0003
22/53
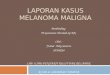
Nodular melanoma
30% of head and neck 5th decade
aggressive monophasic growth
sun-exposed and nonexposed areas
well circumscribed blue/black or nodular
with involution in irregular plaque
downward tumorigenic growth, expand
papillary dermis into reticular dermis
-
8/22/2019 Melanoma 0003
23/53
Nodular melanoma
-
8/22/2019 Melanoma 0003
24/53
Mucosal melanoma
8% head and neck histologic staging little use
local control predicts survival
neck dissection for clinical N+
XRT for histo N+
adjuvant interferon alpha 2-b
-
8/22/2019 Melanoma 0003
25/53
Risk factors
Type I or II skin atypical and congenital nevi
actinic skin changes
history of melanoma
family history of melanoma, atypical nevi
history of significant sun exposure
(blistering)
-
8/22/2019 Melanoma 0003
26/53
Clinical
early, increase in size, change in shape orcolor of pigmented
lesion
most common symptom pruritis
late, tenderness, bleeding, ulceration
ABCDEs (asymmetry, border, color,
diameter, elevation, surrounding tissue) Epiluminescence
microscopy (ELM)
-
8/22/2019 Melanoma 0003
27/53
Biopsy
excisional biopsy or saucerization if small incisional if
large
Depth of biopsy must be to sub-Q fat
if melanoma a second excision must be
performed
-
8/22/2019 Melanoma 0003
28/53
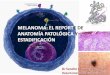
Pathology
diagnosis, tumor thickness in millimeters,margins
histologic subtype, anatomic site, Clark
level, mitotic rate, growth phase, ulceration,regression,
lymphocytes, angiolymphatic
spread, neurotropism, microsatellitosis,
precursor lesion
-
8/22/2019 Melanoma 0003
29/53
Prognosis Breslow (thickness in millimeters) strongest
predictor
-
8/22/2019 Melanoma 0003
30/53
Prognosis
Clark level less predictive, thin skin useful
-
8/22/2019 Melanoma 0003
31/53
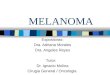
Prognosis
anatomic site, ulceration, gender, histologictype, nodal
disease
head and neck- scalp worse
extremity better trunk
women better men
lymph node + Breslow thickness, ulceration, # pos. nodes
Cohen 10 yr survival # nodes positive
-
8/22/2019 Melanoma 0003
32/53
Work-up
H&P
entire skin, inguinal, axillary, supraclavicular,
H&N nodes,especially primary drainage
brain, bone, GI, constitutional symptoms
palpable nodes FNA
Labs and imaging
vary, CXR to routine CT chest and LFT
H&N CT neck routine
If stage III(regional) or IV (distant) - CT head,
chest, abdomen, pelvis
-
8/22/2019 Melanoma 0003
33/53
Work-up
FDG-PET some use in distant disease
sensitivity 17% in study with SLN biopsy
-
8/22/2019 Melanoma 0003
34/53
Staging-Clark
Level I - in situ at basement membrane Level II - through
basement membrane
into papillary dermis
Level III - spread to papillary/reticular
interface
Level IV - spread to reticular dermis Level V - sub-Q
invasion
-
8/22/2019 Melanoma 0003
35/53
Staging-Breslow
4.00 mm - thick
-
8/22/2019 Melanoma 0003
36/53
Staging
CS/PS (I, II, III) AJCC- Stage I and II - local, III -
regional
IV - distant
-
8/22/2019 Melanoma 0003
37/53
AJCC Staging
-
8/22/2019 Melanoma 0003
38/53
Surgical Treatment
Recommended margins vary Rule of thumb
4mm then 3 cm
All depths to underlying muscle fascia
-
8/22/2019 Melanoma 0003
39/53
Nodal Disease
CS-II remove regional lymphaticsdepending on location of primary
and
presence of distant metastasis
-
8/22/2019 Melanoma 0003
40/53
CSI- The Debate
Balch study- nonrandomized 5 and 10 yr survival intermediate
thickness
(0.76-3.99) doubled with ELND
5 and 10 yr survival for thin (4.0) no change with ELND
-
8/22/2019 Melanoma 0003
41/53
Balch Study
-
8/22/2019 Melanoma 0003
42/53
CSI - The Debate
Four prospective randomized trials Mayo clinic 3 groups stage I
(ELND, delayed,
none) no survival difference, increased
complications if none, criticized not looking atsubgroups to
benefit
WHO no survival benefit, criticized no
subgroups, largely extremity lesions in females
-
8/22/2019 Melanoma 0003
43/53
CSI - The Debate
Four prospective randomized trials Balch - no overall 5 yr
difference, improved in
patients , 60 yrs with ELND, 1-2 mm tumors,
no ulceration, or both benefited, WHO trunk 1.5 mm or more
immediate or
delayed no significant survival benefit, however
was between ELND with occult metastasis andlater developers with
delayed LND
-
8/22/2019 Melanoma 0003
44/53
The Debate - PRO ELND
sequential dissemination theory 30% stage I & II occult
disease
Once palpable 70-80% distant disease, 10 yr
survival 15-25%, 5 yr 1-2 nodes
micrometastasis 65%
Balchs non-randomized study
-
8/22/2019 Melanoma 0003
45/53
The Debate - CON ELND
randomized trials 70% no occult disease
sequential dissemination only theory
-
8/22/2019 Melanoma 0003
46/53
Balchs recommendations
Three groups local, local plus micro, local plus distant
Thin - 95% cure rate no benefit to ELND
Intermediate - 60% regional, 20% distant,
benefit ELND
Thick - >60% regional, >70% distant, nobenefit
Should consider other factors as well
-
8/22/2019 Melanoma 0003
47/53
Sentinel Node Theory
Essence of debate to identify those withoccult metastasis
Morton- first node in group to receive flow
from tumor site
-
8/22/2019 Melanoma 0003
48/53
SLN - procedure
isosulfan blue injection at tumor site, followchannels to
node
studies with ELND 80% sensitivity, specificity
99% preoperative lymphscintigraphy, intra-
operative radiolymphoscintigrapy, and
isosulfan blue dye
69.5% SLN excised blue dye, 83.5% hot,
combined success 96%, location matters
-
8/22/2019 Melanoma 0003
49/53
SLN - Utility
prognostic indicator - study SLN statusmost significant
indicator of disease-free
and disease-specific survival
pathology H&E, S-100, HMB-45 limited by # sections
reverse transcription with polymerase chain
reaction (RT-PCR)- peripheral blood and
nodes, (mRNA tyrosinase) 29 ELND 38% path
positive, 66% RT-PCR positive
-
8/22/2019 Melanoma 0003
50/53
Adjuvant Therapy
Radiation high dose (400-500 cGy) bulky, residual,
recurrent, unresectable, ill
lentigo maligna 5 yr cure 80% (disfiguring,debilitating
location)
adjuvant- trend toward improved regional
control in N+ dissected necks palliate - especially bony
mets
-
8/22/2019 Melanoma 0003
51/53
Adjuvant Therapy
Chemotherapy response 25%, durable control 1%
consider in CSI with >1.5 mm, CSII with WLE,
TND no survival advantage demonstrated
single agent dacarbazine (DTIC)
multiple combinations carmustine, cisplatin,
DTIC, tamoxifen
-
8/22/2019 Melanoma 0003
52/53
Adjuvant Therapy
Immunotherapy unusual behavior, no survival benefit
Interferon
ECOG 1684, >4mm or N+, 6.9 yrs high dose
IFN-alpha-2b, improved disease-free and
overall survival approx. 1 yr. 26% dropout rate
toxicity
-
8/22/2019 Melanoma 0003
53/53
Summary
Incidence and deaths on rise Survival rates increasing due to
detection
and thorough treatment
Depth and nodal status most important
prognostic indicators
ELND still debated SLD useful
Other modalities therapy further research