Embed Size (px)
Citation preview

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 1/82
25/11/2014
1
Tratamiento farmacológico del melanomaavanzado: pasado, presente y futuro
José Antonio López Martín
Oncología MédicaHospital Uni ersitario 12 de Oct!"re
Madrid# $spa%a
2
Melanoma metastásico - 2010• Incidencia global en ascenso• Edad de inicio menor que otros tumores• Mal pronóstico, opciones limitadas de tratamiento:
– Supervivencia 1 año ~25% / 2 años ~10%1
• No tratamientos aprobados para pacientes previamentetratados
• Ningún estudio aleatorizado ha mostrado incremento enla supervivencia
1Korn EL et al. J Clin Oncol . 2008;26:527-534

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 2/82
25/11/2014
2
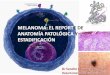
Survival curves of ,!"# patients $it% metastatic melanomas atdistant sites &stage '() su*grouped *y &+) t%e site of metastatic
disease and & ) serum lactose de%ydrogenase & ./) levels
Balch C M et al. JCO 2009;27:6199-6206 ©2009 by American Society of Clinical Oncology

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 3/82
25/11/2014
&
ármacos activos en melanoma en estudiosde fase 2-" &de(ita 3 4e 2011)
ármaco acientesevalua*les
Tasa 5espuestas3*6etivas &7)
4#78'&7)
+l9uilantes'acar"azina 2(4)0 1 1*+1,-e.ozolo.ida &50 1# 11+1,
;itrosoureasLo.!stina 2)0 1" ,+1)
ote.!stina 15& 2< 1)+&1+nálogos latino
isplatino 1 2" 1)+2,ar"oplatino 4& 1! 5+2)
+gentes interaccionan microt=*ulos
aclita3el 5 1" )+22'oceta3el 105 11 *+1,
incristina 52 12 &+20in"lastina *2 1" 5+21indesina 2)& 1< 10+1

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 4/82
25/11/2014
4
• Reacción del huésped ante el melanoma (Handley , 1907):incremento del número de células redondas infiltrantes
• Respuesta del huésped ante el melanoma: re!resionesespont"neas documentadas
• #ustancias citotó$icas anto%melanoma ex-vivo , en el suerode al!unos pacientes (&e'is)
.acar*azina &.T'8)
• 'A lo apr!e"a en 1,)5• o 6a7 est!dios 8rente a
trata.iento de soporte
• 'i ersos es9!e.as en.onoterapia 7 en co."inación
• -asa resp!esta: ; <20=• >!per i encia: ; .eses ?@

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 5/82
25/11/2014
5

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 6/82
25/11/2014
*
8onclusiones de revisiones sistemáticasy meta-análisis so*re el uso de .T'8
“… en conclusión, los datos obtenidos enlos últimos 30 años, y en particular en loúltimos 5, demuestran que el tratamientocon dacarbazina en monoterapiadacarbazina en monoterapiadacarbazina en monoterapiadacarbazina en monoterapia esequivalente al de las combinaciones dedicho fármaco con otros agentes, entérminos de eficacia antitumoral ysupervivencia…”

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 7/82
25/11/2014
)
.acar*azina• 'acar"azina estB indicado para el trata.iento de pacientes
con .elano.a .aligno .etastatizado#• 'acar"azina podrB ser ad.inistrado co.o agente Cnico en
dosis de 200 a 250 .g/.D/día i# # d!rante 5 días cada &se.anasEen "ol!s o en per8!sión rBpida ?de 15 a &0.in!tos #
• -a."ién es posi"le ad.inistrar 50 .g/.D de Brea des!per8icie corporal el pri.er día 7 desp!és !na ez cada &se.anas( en 8or.a de per8!sión intra enosa#
Temozolomida
• ro8Br.aco 9!egenera el .eta"olitoacti o de la
dacar"azina tras6idrólisis• ia oral• Atra iesa "arrera
6e.atoence8alica

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 8/82
25/11/2014
Temozolomida 1 4 meses
.T'8 1 # meses
/5 1 " > p?0 012
Temozolomida meses
.T'8 ! < meses
/5 1 1 &'8 4#7 0 42-1 #2)>
p?0 2
J Clin Oncol 18:158-166. 2000
J Clin Oncol 18:158-166. 2000

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 9/82
25/11/2014
,
EUROPEAN JOURNAL OF CANCER 47 (2011) 1476 –1483
Supervivencia glo*al mediana,#1* . ?-e.ozolo.ida,#&* . ?'acar"azina FHazard ratio G 1#00(,5= con8idence inter al ?0# *( 1#1) #
Supervivencia sin progresión2#&0 . ?-e.ozolo.ida2#1) . ?'acar"azina FHazard ratio G 0#,2(,5= con8idence inter al ?0# 0(1#0* #

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 10/82
25/11/2014
10
otemustina 1 4 meses
.T'8 1 meses
otemustina " meses
.T'8 # ! meses
p?0 0!
otemustina 22 meses.T'8 2 meses p?0 0#4
T'@M 3 /+ST+ .@S+553 3 .@ M@T+ST+S'S 8@5@ 5+ @S

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 11/82
25/11/2014
11
otemustina'ndicaciones terapAuticas
Melano.a .alignodise.inado( incl!idas laslocalizaciones cere"rales(para ad.inistración en.onoterapia#
Dosis recomendada: 100 mg/m2.
En monoquimioterapia simple el tratamiento comprende:Inducción: tres administraciones consecutivas con unasemana de intervalo, seguidas de un período de lavado de 4 a5 semanas,Mantenimiento: una administración cada 3 semanas.
FECHA DE AUTORIZACIÓN: 05/11/99
J Clin Oncol 17:2105-2116. 1999

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 12/82
25/11/2014
12
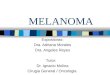
?IL2 gp100 : ,= ?IL2 : 1=
$ngl J Med 2011F&*4:211,<2)#
Respuestas globalesRespuestas objetivas

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 13/82
25/11/2014
1&
SupervivenciaSupervivencia global
Supervivencia glo*al de pacientes conmelanoma avanzado seg=n el tratamiento
Kar"e et al# -6e Oncologist 2011F1*:5<24
'-Iote.!stina

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 14/82
25/11/2014
14
*Datos recolectados mediante búsqueda PubMed “melanoma clinical trial.”
US National Library of Medicine and National Institutes of Health.
N total de Ensayos Clínicospublicados *: 3337
14 0 B 2010: Más de "000 @@88sin impacto clCnico real
0
50
100
150
200
250
1970 1995 2005 2010
N P u b l i c a
i o n e s
d e
E n s a y o s
C l í n i c o s
*
Año Publicación20001975 1980 1985 1990
Phase III Study Design
1:1 randomization stratified by:
• metastatic stage (M1a, M1b, and M1c)• region (Australia, North America, Western Europe)• baseline LDH (< 0.8 x ULN, 0.8–1.1 x ULN, >1.1-2 x ULN)
Planned N = 514
Chemo-naïveECOG PS 0-1Stage IV cutaneousMeasurable diseaseLDH levels ≤ 2.0 x ULNNo current brain mets
nab -Paclitaxel ( nab -P)150 mg/m 2 IV
days 1, 8, and 15, 28-day cycle
Dacarbazine (DTIC)1000 mg/m 2 IV, day 1, 21-day cycle
• CT scan every 8 weeks in both arms • Enrollment period April 2009 – June 2011; Data cut-off – June 30, 2012 • Treatment until disease progression or unacceptable toxicity, patient/investigator discretion
ECOG, Eastern Cooperative Oncology Group;LDH, lactate dehydrogenase; ULN, upper limit of normal
Hersh, et al. Phase 3 Study of nab ® -Paclitaxel vs Dacarbazine in Chemotherapy-naïve Patients with Metastatic Malignant Melanoma. Presented at: The Society ofMelanoma Reserach; November 8-11, 2012; Los Angeles, CA.

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 15/82
25/11/2014
15
Other Efficacy Endpoints
Blinded RadiologyAssessment
nab -Paclitaxel(n = 264)
Dacarbazine(n = 265)
Response RateRatio
(P na b-P /P DTIC)P -value
ORR, % (95% CI) 15 (10.5, 19.1) 11 (7.5, 15.1) 1.305 (0.837, 2.035) 0.239
DCR, % (95% CI) 39 (32.8, 44.5) 27 (21.5, 32.1) 1.442 (1.123, 1.852) 0.004PR, % 15 11SD ≥ 16 weeks, % 24 15
Best Response 0.0017*
PR, % 15 11SD, % 25 16PD, % 35 48 0.005**Not Evaluable, % 25 25
P, proportion of improved patients; PD, progressive, disease; SD,stable disease
* Includes confirmed PR + SD + PD ** Comparison of PD rate between arms
Hersh, et al. Phase 3 Study of nab ® -Paclitaxel vs Dacarbazine in Chemotherapy-naïve Patients with Metastatic Malignant Melanoma. Presented at: The Society ofMelanoma Reserach; November 8-11, 2012; Los Angeles, CA.
Target Tumor Responses by Patient
Hersh, et al. Phase 3 Study of nab ® -Paclitaxel vs Dacarbazine in Chemotherapy-naïve Patients with Metastatic Malignant Melanoma. Presented at: The Society ofMelanoma Reserach; November 8-11, 2012; Los Angeles, CA.

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 16/82
25/11/2014
1*
PFS by Independent Radiology Review
CI, confidence interval
Hersh, et al. Phase 3 Study of nab ® -Paclitaxel vs Dacarbazine in Chemotherapy-naïve Patients with Metastatic Malignant Melanoma. Presented at: The Society ofMelanoma Reserach; November 8-11, 2012; Los Angeles, CA.
OS: Planned Interim Analysis
Hersh, et al. Phase 3 Study of nab ® -Paclitaxel vs Dacarbazine in Chemotherapy-naïve Patients with Metastatic Malignant Melanoma. Presented at: The Society ofMelanoma Reserach; November 8-11, 2012; Los Angeles, CA.

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 17/82
25/11/2014
1)

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 18/82
25/11/2014
1
Subtipos clínico-moleculares demelanoma
15

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 19/82
25/11/2014
1,

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 20/82
25/11/2014
20
Melero … Ascierto. Clin Cancer Res 2013

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 21/82
25/11/2014
21
Paradigmas de tratamiento farmacológico
del melanoma avanzado
Diana=sistemainmune
Diana=tumorInmunoterapia TratamientoAnti-diana
Cortesía del Dr. Ribas

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 22/82
25/11/2014
22
'pilimuma* en melanoma avanzado:
Supervivencia en ensayos de ase 2
O´Day et al. ASCO 2009: 9033
44
@ventos adversos relacionadoscon activación linfocitaria &ir+@s)

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 23/82
25/11/2014
2&

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 24/82
25/11/2014
24

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 25/82
25/11/2014
25
50
Tremelimuma* +"! 1004:roteCna 8 reactiva y supervivencia
Mars6all A> O2010: 2*0,

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 26/82
25/11/2014
2*
os respondedores a 'pilimuma* muestran un perfil deeDpresión gAnica del tipo Einflamación citotóDicaF
Ji et al, 2011.
CXCL9, 10, 11CCL4, CCL5Granzima BPerforinaCD8a
No Beneficio Beneficio
Screening
Semana 12'ncremento inicialde la carga total
de tumor &mG/3 .)
5espuesta ala semana 1!
Semana 4!5espuesta duradera ;o ir+@s
ortesía de 8 # Har.anNa7a( iena
Har.anNa7a ( et al# resented at $A'O 200,( ienna( A!stria
8inAtica especial de la respuestaantitumoral a ipilimuma*

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 27/82
25/11/2014
2)
Hodi F S et al. PNAS 2003;100:4712-4717
;ecrosis tumoral inducida por 'pilimuma*Wolchok et al.Clin Cancer Res 2009;15(23):7412–20
-!.or necrosis it6 gran!loc7tesand l7.p6oc7tes
8.<H
8. H
8.20H cells
asc!lopat67 it6 peri asc!lar and intra.!ral l7.p6oidin8iltrates associated it6 l!.inal t6ro."osis
+nálisis de los patrones de respuesta
150125100
755025
0-25-50-75
-100-125
19,373
17,24215,111
12,98010,849
8,7186,5874,456
2,325194
-1,937
S P D
( mm
2 )
Relative week from first dose date
50
25
0
–25
–50
–75
–100
–125
C h a n g e
f r o m
b a s e l i n e
S P D ( % )
Relative week from first dose date
1,272
1,124975
827678
530
382233
85-64
-212
S P D
( mm
2 )
C h a n g e
f r o m
b a s e l i n e
S P D ( % )
-9 -3 3 9 15 21 27 33 39 45 51
Relative week from first dose date
C h a n g e
f r o m
b a s e l i n e
S P D ( % )
S P D
( mm
2 )
2,8942,5562,2181,8811,5431,206868530193-145-482
50
25
0
-25
-50
-75
-100
-125
Total tumourvolume
Index lesionsNew lesionsIpilimumabdosing
SPD = Sum of the Product of the perpendicular Diameters (a measure of tumour volume)
-9 -3 3 9 15 21 27 33 39 45 51
-9 -3 3 9 15 21 27 33 39 45 51
ISta*le diseaseI $it% slo$, steadydecline in total tumourvolume
Response after initial increasein total tumour volumeResponse in baseline lesions
C h a n g e
f r o m
b a s e l i n e
S P D ( % )
S P D
( mm
2 )
2,8102,4822,1541,8261,4981,171843515187-140-468
50
25
0
-25
-50
-75
-100
-125-9 -3 3 9 15 21 27 33 39 45 51
9 months
Relative week from first dose date
PD
PR
CR
5.2 months 6 months
9.4 months
Response in index and new lesionsAt or after the appearance of new lesions
Wolchok JD, et al. Clin Cancer Res 2009;15:7412–7420

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 28/82
25/11/2014
2
55
'pilimuma*: 5espuesta S;8&8+1 <-0<2: 8o%orte +)
asal Semana 1!
5 cere*ral H glo*al, de 11H meses duraciónHeller ( et al# A> O 2011# J linOncol 2011F2, ?s!pplF a"str 5 1

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 29/82
25/11/2014
2,

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 30/82
25/11/2014
&0
'pilimuma* H *evacizuma* &fase 1)
Hodi A> O 2011
'pilimuma* H JM-8S

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 31/82
25/11/2014
&1
3tras com*inaciones con ipilimuma*&clinicaltrials gov - marzo 201<)
H ot%er c%emo K targeted H ot%er immuno H ot%er agent8o.!stine ni ol!.a" "e aciz!.a"ge.cita"in cisplatin anti<OP40 radiationlo <dose c7clop6osp6a.ide anti< I lenolida.ide
e.!ra8eni" rIL<21 isolated li." in8!sion
da"ra8eni" tra.etini" KM< > cr7oa"lationQM><,0 **2 adopti e cell trans8er rit!3i.a"I.atini" a8ter allogeneic ste.
cell transplantradioe."olization
androgen<depri ation t6erap7 I <al8a 2"dasatini" a!tologo!s ' accinedo37c7cline te.ozola.ide I'O in6i"itorpaclita3el car"oplatin intrat!.oral IL<2car"oplatin etoposide Onco e3ge.cita"ine ni ol!.a"

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 32/82
25/11/2014
&2

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 33/82
25/11/2014
&&
+ctividad clCnica de nivoluma* B ase 1
65
Hodi ECCO 2013

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 34/82
25/11/2014
&4
>znol M( et al# resented at A> O 2010 J Clin Oncol 2 :15s( 2010 ?s!pplF a"str 250* #
@ficacia antitumoral de
;ivoluma* & MS-4"!## ) en melanoma

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 35/82
25/11/2014
&5

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 36/82
25/11/2014
&*

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 37/82
25/11/2014
&)

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 38/82
25/11/2014
&

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 39/82
25/11/2014
&,

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 40/82
25/11/2014
40
Pembrolizumab Pembrolizumab Pembrolizumab Pembrolizumab (MK (MK (MK (MK- -- -3475) 3475) 3475) 3475)

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 41/82
25/11/2014
41

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 42/82
25/11/2014
42
Seguridad de 'pilimuma* y de
;ivoluma* en monoterapia
Wolchock J Leuk Biol 2013Melero Clin Cancer Res 2013

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 43/82
25/11/2014
4&
[TITLE]
Presented By Jedd D. W olchok, MD, PhD at 2013 ASCO Annual Meeting
'pilimuma* H nivoluma*: 6ustificación preclCnica

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 44/82
25/11/2014
44
?E
22 months follow up for Cohorts 1-3
+S83 201< - 400" M Sznol et alSurvival, response duration, and activity *y 5+ mutation status ofnivoluma* &;'(3, anti- .-1, MS-4"!## , 3;3-<#" ) and ipilimuma*concurrent t%erapy in advanced melanoma

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 45/82
25/11/2014
45

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 46/82
25/11/2014
4*
+S83 201< - 400" M Sznol et alSurvival, response duration, and activity *y 5+ mutation status ofnivoluma* &;'(3, anti- .-1, MS-4"!## , 3;3-<#" ) and ipilimuma*concurrent t%erapy in advanced melanoma

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 47/82
25/11/2014
4)

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 48/82
25/11/2014
4

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 49/82
25/11/2014
4,

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 50/82
25/11/2014
50

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 51/82
25/11/2014
51

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 52/82
25/11/2014
52
Paradigmas de tratamiento farmacológicodel melanoma avanzado
Diana=sistemainmune
Diana=tumorInmunoterapia TratamientoAnti-diana
Cortesía del Dr. Ribas

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 53/82
25/11/2014
5&

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 54/82
25/11/2014
54
Melanoma $it% a*normal M+ L pat%$ay
Georgina Long 2011
BRAF inhibitorsVemurafenib
Dabrafenib/GSK2118436LGX818
MEK inhibitorsTrametinibGDC-0973PimasertibMEK162AZD6244TAK, BAY,
ERK inhibitorMERCK
mTOR
PI3K
Akt
PI3K inhibitorsmTOR inhibitors
PTEN

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 55/82
25/11/2014
55
RasGTP
Basal
pERK
cyclin D
Ki67
Día 15
Cyclin D
BRAFV600
MEK
ERK
P
P
Cell cycle(Ki67)
PLX4032
RTK
Y-PY-P
GF
Inhibición de la señal de MAPK en biopsias de pacientes conmelanoma con mutación en BRAFV600 tratados con Vemurafenib
MAPK = mitogen-activated protein kinase;pERK = phosphorylated extracellurar signal-regulated kinase.Adapted from Smalley et al, 2010; Flaherty et al, 2010b.
McDermott U et al. N Engl J Med 2011;364:340-350.
Respuesta metabólica precoz aVemurafenib

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 56/82
25/11/2014
5*

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 57/82
25/11/2014
5)
Flaherty et al, 2010; Chapman et al, 2011; Sosman et al, 2012.
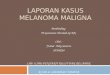
100908070605040302010
0 P r o g r e s s i o n -
f r e e s u r v i v a l ( %
)
0 6 12 18 24
338337
63186
2277
316
00
100269
37113
1449
03
No. at risk
1.6 6.9
Hazard ratio 0.38(95% CI: 0.32–0.46)
Log-rank p<0.001 (post-hoc)Dacarbazine
(n=338)
Vemurafenib (n=337)
Progression-free survival (February 01,2012 cut-off) censored at crossover
Time (months)
DacarbazineVemurafenib
Chapman. ASCO 2012

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 58/82
25/11/2014
5
100908070605040302010
0
O v e r a l l s u r v i v a l ( %
)
0 6 12 18 24
Vemurafenib (n=337)Median f/u 12.5 months
Dacarbazine (n=338)Median f/u 9.5 months
338337
173280
79178
2444
01
244326
111231
50109
47
9.7 13.6
Overall survival (February 01, 2012 cut-off)
censored at crossover
Hazard ratio 0.70(95% CI: 0.57–0.87)p<0.001 (post-hoc)
Time (months)
DacarbazineVemurafenib
No. at risk
Chapman. ASCO 2012

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 59/82
25/11/2014
5,
.a*rafeni* 5@+L-":rimary endpoint: S 'nvestigator-assessed
&cut-off: 14 .ecem*er 2011)
On randomized study treatment at cut-off: dabrafenib 57%, DTIC 27%Median follow-up time: 4.9 months (dabrafenib 5.1 mos, DTIC 4.8 mos.)
Ha!sc6ild A> O 2012

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 60/82
25/11/2014
*0
No prior brain treatment: BRAF V600E
maximal intracranial target lesion reduction
Cohort B
Cohort A
irN ood# A> O 2012
Selected adverse events (% of patients)
Vemurafenib, n= 336 Dacarbazine, n= 282
Adverse events All Grade 3 Grade ≥ 4 All Grade 3 Grade ≥ 4
Arthralgia 49 3 - 3 <1 -
Rash 36 8 - 1 - -
Fatigue 33 2 - 31 2 -
Photosensitivity 30 3 - 4 - -↑↑↑↑ LFTs 18 7 <1 5 1 -
Cutaneous SCC 12 12 - <1 <1 -
Keratoacanthoma 8 6 - - - -
Skin papilloma 18 <1 - - - -
Nausea 30 1 - 41 2 -
Neutropenia <1 - <1 11 5 3
Discontinuations due to AE: 6% Vemurafenib; 4% Dacarbazine
Chapman. ASCO 2012

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 61/82
25/11/2014
*1
Eventos adversos ocurridos en > 5%
pacientes
Fotosensibilidad: dabrafenib (3%), DTIC (5%)
otosensi*ilidad

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 62/82
25/11/2014
*2
ToDicidad cutánea por in%i*idores 5+
An8ort6# Lancet Oncol 201&F 14: e11+1
Carcinoma epidermoide/keratoacantomapiel por vemurafenib
– Incidencia: 26%
– Tiempo hasta aparición (mediana): 8 semanas (2–36)
– N mediano de episodios por paciente: 1 (range 1–7)
(cada punto es la semana hasta 1ª aparición de una lesión en unpaciente)
0 5 10 15 20 25 3530 40
Tiempo con Vemurafenib (semanas)
Mediana
Ribas et al, 2011.

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 63/82
25/11/2014
*&
.ifferential effects of 5+ in%i*ition in 5+ (!00mutant melanoma and 5+ $ild type cells
BRAF V600 mutant melanoma BRAF wild type cells
Modeled from Hatzivassiliou et al . Nature 2010, Heidorn et al . Cell 2010, Poulikakos et al . Nature 2010
CRAF
MEK1/2
ERK
P
P
BRAF V600
MAPKsignaling
CRAF
MEK1/2
ERK
P
P
BRAF V600
PLX4032
MAPKsignaling
CRAF
MEK1/2
ERK
P
P
BRAF
MAPK signaling
RAS
CRAF
MEK1/2
ERK
P
P
BRAF
PLX4032
MAPK signaling
RAS
aradoDical M+ L activation in /5+S mutantcuS88KL+s
BRAF wild type cells
CRAF
MEK1/2
ERK
P
P
BRAF
MAPK signaling
RAS
CRAF
MEK1/2
ERK
P
P
BRAF
PLX4032
MAPKsignaling
HRAS Q61
Fei Su, Amaya Viros, Carla Milagre, … Antoni Ribas*, Richard Marais*. NEJM 2012Oberholzer, …. Robert, Garraway, JCO 2011
ParadoxicalMAPK activation
with RAF inhibitors

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 64/82
25/11/2014
*4
010203040506070
CR+PR SD PD
Assessment of Tumor Response Rate tovemurafenib: Independent Review Committee
• ORR 53% by IRC• ORR 57% by investigator assessments (INV)
• RR, including unconfirmed, 69% (INV)
• PR in 4 of 10 BRAF V600K patients
R e s p o n s e r a
t e ( % )
n=70 n=38 n=18
53% CR+PR
5% CR
29%
14%
Error bars represent 95% confidence intervals

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 65/82
25/11/2014
*5
5esponse and 5elapse $it% vemurafeni*10/02/08 (Pre) 11/26/08 (2+ mo) 02/20/09 (4+ mo)
Pt #43, UCLA
melanoma
stroma
A# i"as
Mec%anisms of 5esistance to 5+ 'n%i*itors
Survival
BRAF V600E
MEK
ERK
P
P
BRAF inh
PDGFRb or IGF1R
PI3K
AKT
Nazarian et al.Nature 2010Villanueva et al.Cancer Cell 2010
MEK-independentprogression
Nazarian et al.Nature 2010
NRAS Q61
COTJohannessen et al.Nature 2010
CRAF
Wagle et al.JCO 2011
MEK-dependentprogression
Poulikakos et al.Nature 2012Shi et al.Nature Com 2012
MEKi
PI3Ki or AKTi
A# i"as

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 66/82
25/11/2014
**

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 67/82
25/11/2014
*)
Trametinib (GSK1120212)Highly selective, allosteric inhibitor of MEK1/MEK2
IC50 of 0.7-0.9 nM
Unique exposure profile provides constant target inhibition and
minimizes potential Cmax driven toxicities
TrametinibMEK1 Binding-Model
D a y
1 5 C
o n c e n t r a t i o n
( n g
/ m L )
Preclinical Target
Time (hours)
METRIC Overall Survival – ITT

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 68/82
25/11/2014
*

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 69/82
25/11/2014
*,
Enhanced Antitumor Activity with Combination
M e a n
t u m o r v o
l u m e
( m m
3 ) +
S E M
BRAFV600E human melanoma xenograft
2000
1500
1000
500
0
0 1 0 2 0 3 0 4 0 5 0 6 0 7 0 8 0 9 0Treatment period (days)
A375PF11
Untreated controlTrametinib (0.3 mg/kg)Dabrafenib (30 mg/kg)Dabrafenib(300 mg/kg)Dabrafenib+trametinib(30/0.3 mg/kg)
Re"er# A> O 2012
MEKi Blocks BRAFi-Induced Skin Lesions in Rats
Control BRAFi (150 mg/kg) BRAFi + MEKi (1.5 mg/kg)
BRAFi alone resultsin thickening &hyperkeratosis
Co-dosing with MEKiattenuates lesionformation
Re"er# A> O 2012

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 70/82
25/11/2014
)0
Key Treatment-Related Skin Toxicities
All Part B Patients(N = 135)
Grade ≥ 3,n (%)
Any grade event,n (%)
Rash/Skintoxicities 1 3 (2%) 61(45%)
Skin papilloma 0 (0%) 3 (2%)
Squamous cellcarcinoma 4 (3%) 4 (3%)
Actinic keratosis 0 (0%) 7 (5%)
Hyperkeratosis 0 (0%) 5 (4%)
1Skin toxicities include multiple terms

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 71/82
25/11/2014
)1
Treatment-Related AEs ≥ 20% of Patients4 dose levels
dabrafenib/trametinib (mg BID/mg QD) – 75/1, 150/1, 150/1.5, 150/2
Preferred Term
Full dose (n = 79)(150 mg BID dabrafenib/2 mg QD trametinib) All Part B
Patients(N = 135)
n (%)Grade ≥ 3n (%)
All graden (%)
Any event, n (%) 28 (35) 1 71 (90) 126 (93)
Pyrexia 6 (8) 46 (58) 70 (52)
Rash/Skintoxicities 2
0 33 (42) 61 (45)
Chills 1 (1) 29 (37) 51 (38)
Fatigue 1 (1) 30 (38) 50 (37)
Nausea 1 (1) 27 (34) 46 (34)
Dose reduction due to AEs in 39% of all Part B patients; most common are pyrexia (23%); chills (10%)
1Includes 1 Grade 5 event of ventricular arrhythmia2Skin toxicities include multiple terms

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 72/82
25/11/2014
)2

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 73/82
25/11/2014
)&

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 74/82
25/11/2014
)4

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 75/82
25/11/2014
)5

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 76/82
25/11/2014
)*
5as mutated melanoma

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 77/82
25/11/2014
))
J;+ KJ;+11 melanoma

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 78/82
25/11/2014
)
c-L'T activated melanoma

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 79/82
25/11/2014
),
Imatinib in KIT-abnormal melanoma
M1b M1cM1a
-80
-60
-40
-20
0
20
40
60
80
100
120
K!o J et al( A> O 2010
KIT status (Exon 9:11:13:17:18: amplif) 2:14:8:3:5:3
Correlations of response andKIT aberrations
KIT Status PR SD PR+SD
KIT Amp 1/3 0/3 1/3
Exon11 2/12 8/12 10/12Exon13 3/8 1/8 4/8
Exon17 0/3 1/3 1/3
Exon18 0/4 2/4 2/4
Multiple gene aberrations* 3/4 1/4 4/4
* 4 patients respectively harbored multiple KIT aberrations as following:(13)K642E+Amplification ; (13) I817T(T2450C); (18)F848L(T2542C) ;(11)L576P+Amplification ;
K!o J et al( A> O 2010
07

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 80/82
25/11/2014
0

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 81/82
25/11/2014
1

7/24/2019 Melanoma 2014
http://slidepdf.com/reader/full/melanoma-2014 82/82
25/11/2014
Le7endas !r"anas• Ipili.!.a" es tó3ico 7 de di8ícil .aneSo
– La 8or.ación delpaciente 7 del .édico es la cla e• Los trata.ientos antidianas de"erían reser arse
para pacientes sinto.Bticos o con en8er.edadrBpida.ente e ol!ti a – Los trata.ientos antidianas 8!ncionan en los
pacientes con la .!tación 7 tanto .eSor c!anto .Bs8a ora"le es la "iología de la en8er.edad
• o 6a7 s!per i encias prolongadas con lostrata.ientos antidiana ?Tplatea! – o 6a7 seg!i.iento s!8iciente# o lo sa"e.os#