Embed Size (px)
Citation preview
Metástasis hepáticas de Metástasis hepáticas de Metástasis hepáticas de Metástasis hepáticas de Cáncer colorrectal: Cáncer colorrectal: Cáncer colorrectal: Cáncer colorrectal: Su relevancia clínicaSu relevancia clínica
SESIÓN MULTIDISCIPLINARIA SEOM SEMNIMSESIÓN MULTIDISCIPLINARIA SEOM-SEMNIMDRA E. GONZÁLEZ-FLORES
ONCOLOGÍA MÉDICA GRANADAONCOLOGÍA MÉDICA. GRANADAMadrid-23 0ctubre 2012
Magnitude of diseaseMagnitude of diseaseMagnitude of diseaseMagnitude of diseaseColorectal cancer is one Colorectal cancer is one of the most common cancersof the most common cancers
Approximately 50% of patientsApproximately 50% of patientsApproximately 50% of patients Approximately 50% of patients have or will develop liver metastaseshave or will develop liver metastases
2020--30% of patients have liver30% of patients have liver--only only metastases at the time of initial evaluationmetastases at the time of initial evaluation
After primary tumor resection, at least 1After primary tumor resection, at least 1 in in 3 patients will develop recurrent liver 3 patients will develop recurrent liver diseasedisease
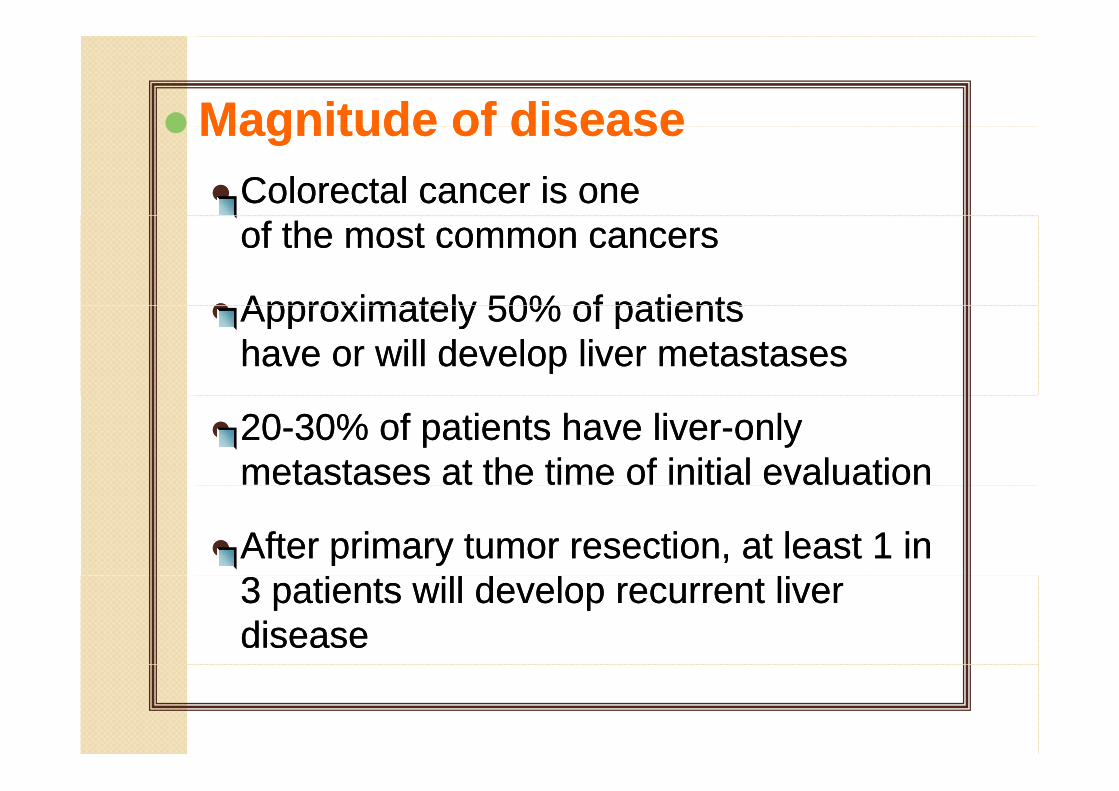
CANCER COLOCANCER COLO--RECTAL RECTAL CANCER COLOCANCER COLO--RECTAL RECTAL Sitios mas frecuentes de metástasis a distanciaSitios mas frecuentes de metástasis a distancia
Hígado 38-60%
Ganglios abdominales 39%g
Pulmón 38%
Peritoneo 28%
Ovario 18%
Glándulas adrenales 14%
Pleura 11%
Hueso 10%
Cerebro 8%
Adapted from Kemeny N, Seiter K. Handbook of chemotherapy in clinical oncology. SCI ed.1993;589-594.
TRATAMIENTOThe multidisciplinary teamThe multidisciplinary team
Strategic choices determine the therapeutic optionsSurgeon Oncologist
Strategic choices determine the therapeutic options
Cl i tiClose communication between members of multidisciplinary treatment team istreatment team is recommended
M. NuclearRadiologist
Nurse HistopathologistNCCN Guidelines v2 2010; Van Cutsem E, et al. Ann Oncol 2010;21 (Suppl. 6):vi1–vi10
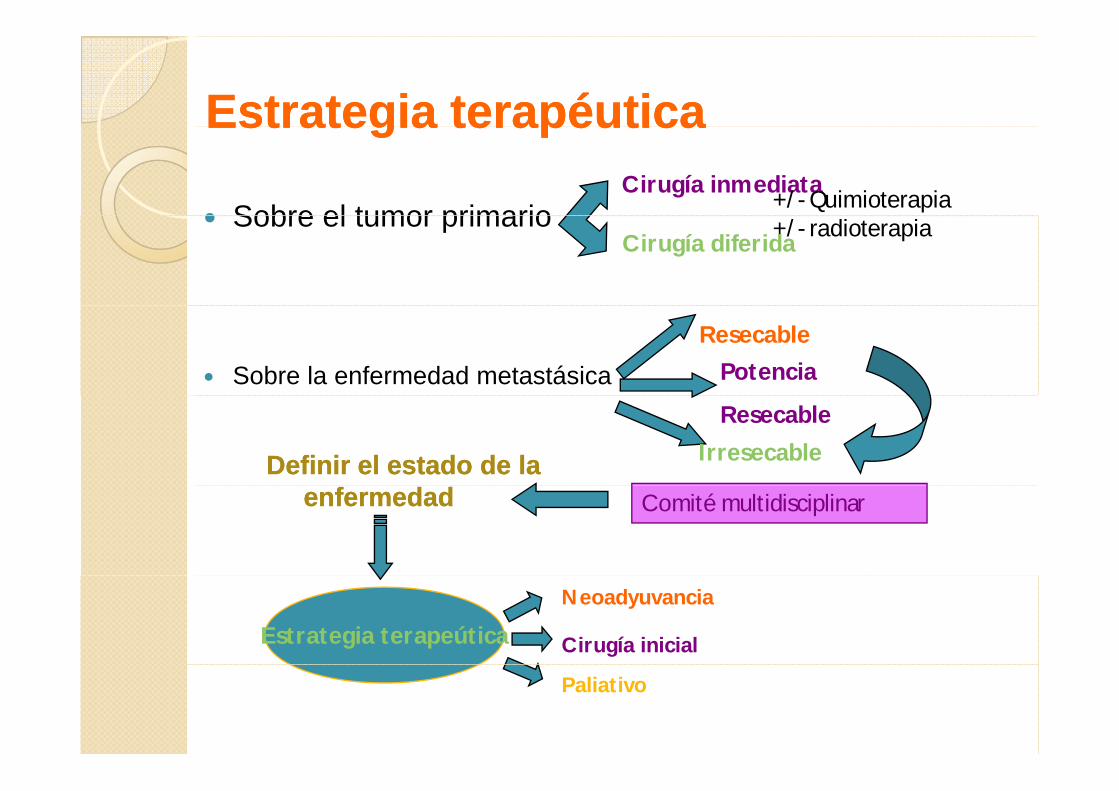
Estrategia terapéuticaEstrategia terapéuticaEstrategia terapéuticaEstrategia terapéutica
Sobre el tumor primarioCirugía inmediata
+/- QuimioterapiaSobre el tumor primarioCirugía diferida
+/- radioterapia
Sobre la enfermedad metastásicaResecable
Potencia
Resecable
IrresecableDefinir el estado de la Definir el estado de la Comité multidisciplinarenfermedadenfermedad
Estrategia terapeútica
Neoadyuvancia
Cirugía inicial
Paliativo
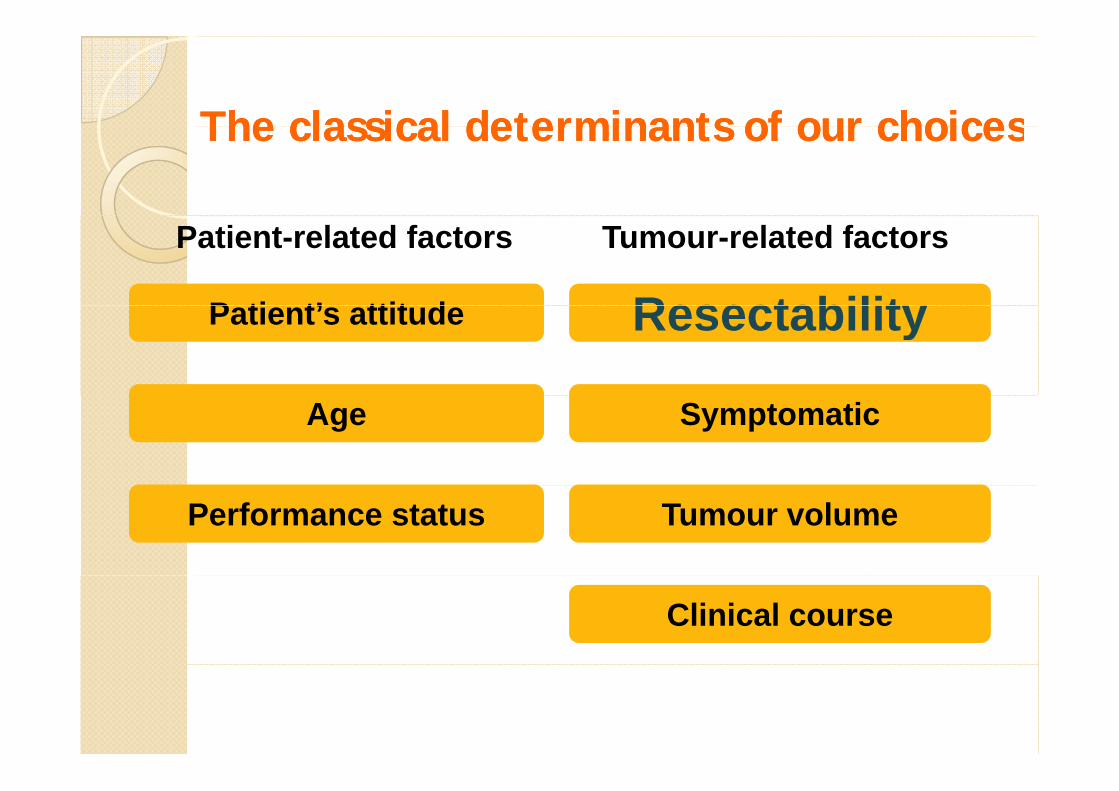
The classical determinants of our choicesThe classical determinants of our choicesThe classical determinants of our choicesThe classical determinants of our choices
Patient-related factors
P ti t’ ttit d ResectabilityTumour-related factors
Patient’s attitude Resectability
Age Symptomatic
Performance status Tumour volume
Clinical course
Liver MetastasesLiver MetastasesApproximately 80% of liver Approximately 80% of liver metastases are initially unresectablemetastases are initially unresectablemetastases are initially unresectablemetastases are initially unresectable
SizeSizeLocationLocationNumberNumberNumberNumber
Definitions of unresectablity Definitions of unresectablity yydiffer by surgeon and by institutiondiffer by surgeon and by institution
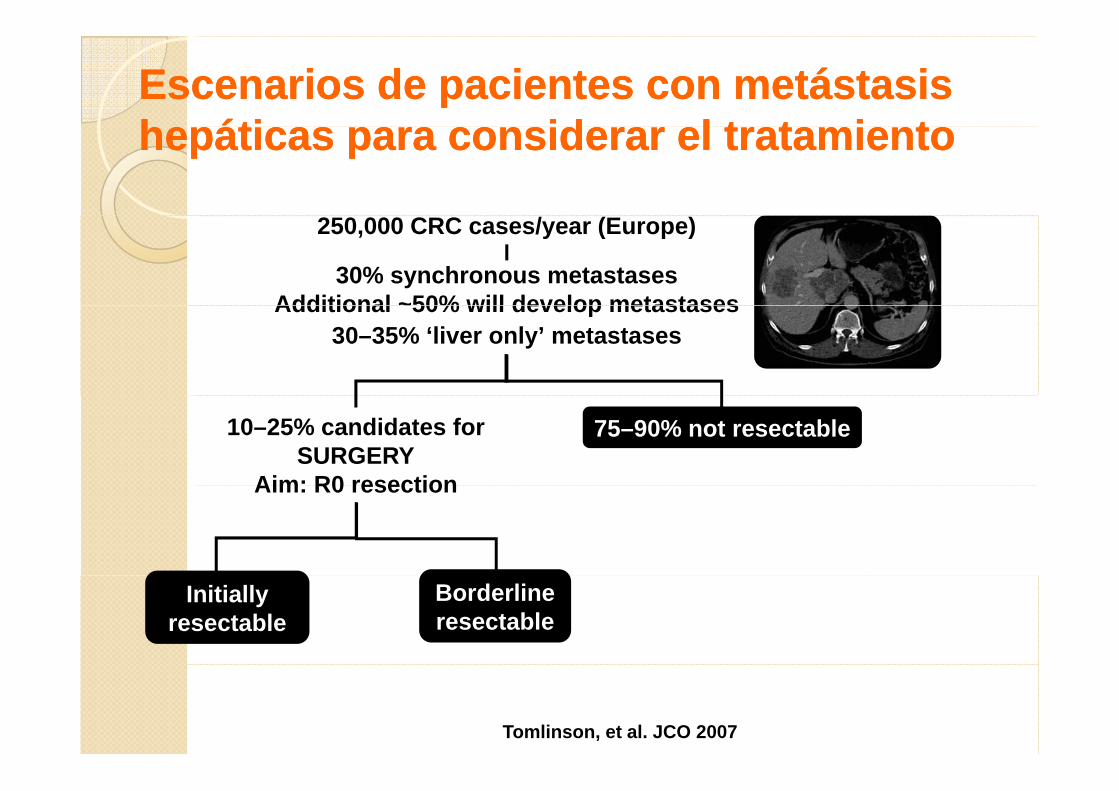
Escenarios de pacientes con metástasis Escenarios de pacientes con metástasis h áti id l t t i th áti id l t t i thepáticas para considerar el tratamientohepáticas para considerar el tratamiento
30% synchronous metastasesAdditional ~50% will develop metastases
250,000 CRC cases/year (Europe)
Additional ~50% will develop metastases 30–35% ‘liver only’ metastases
75–90% not resectable10–25% candidates for SURGERY
Aim: R0 resectionAim: R0 resection
Initially resectable
Borderline resectable
Chu, et al. Clin Colorectal Can 2006; Kemeny, et al. NEJM 1999; Kemeny, et al. Oncologist 2007; Leichman. Surg Oncol Clin N Am 2007;
Leonard, et al. JCO 2005; Tomlinson, et al. JCO 2007; Van Cutsem, et al. EJC 200;
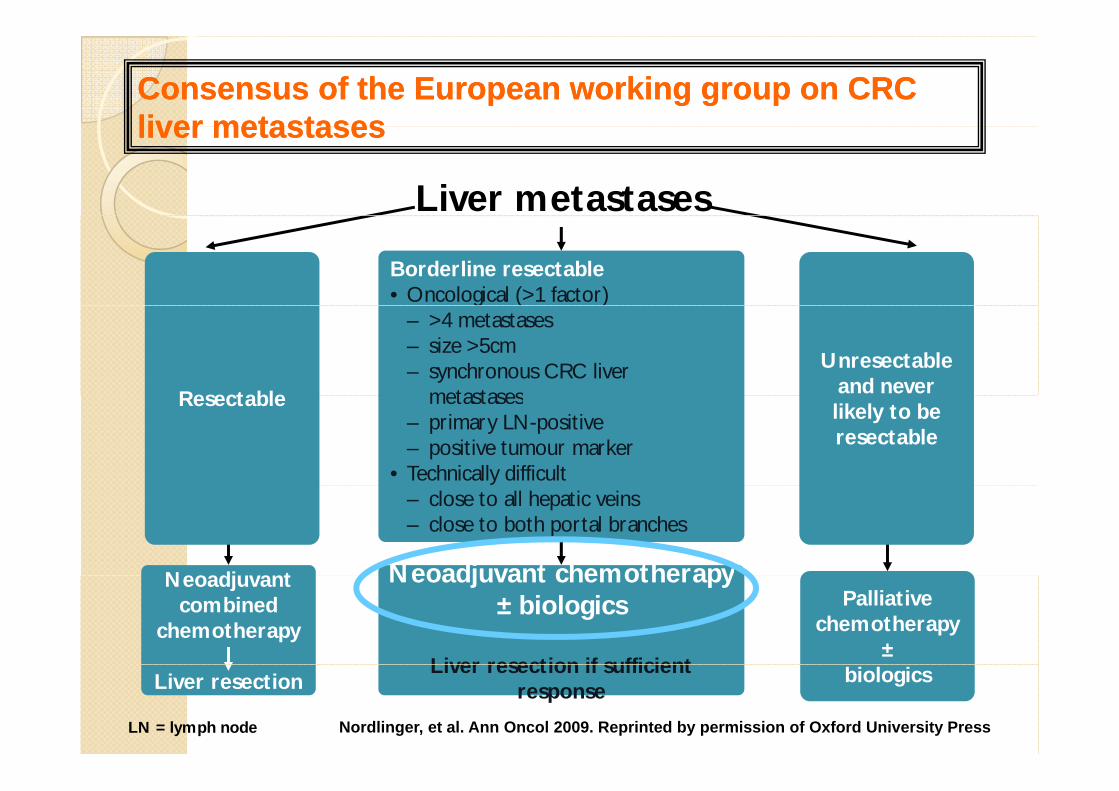
Consensus of the European working group on CRC Consensus of the European working group on CRC liver metastasesliver metastasesliver metastasesliver metastases
Liver metastases
Borderline resectable• Oncological (>1 factor)
Unresectableand neverR t bl
g ( )– >4 metastases– size >5cm– synchronous CRC liver
metastaseslikely to beresectable
Resectable metastases– primary LN-positive– positive tumour marker
• Technically difficult
Neoadjuvant chemotherapy
– close to all hepatic veins– close to both portal branches
N dj tPalliative
chemotherapy±
Neoadjuvant chemotherapy± biologics
Liver resection if sufficient
Neoadjuvantcombined
chemotherapy
biologicsLiver resection if sufficientresponseLiver resection
LN = lymph node Nordlinger, et al. Ann Oncol 2009. Reprinted by permission of Oxford University Press
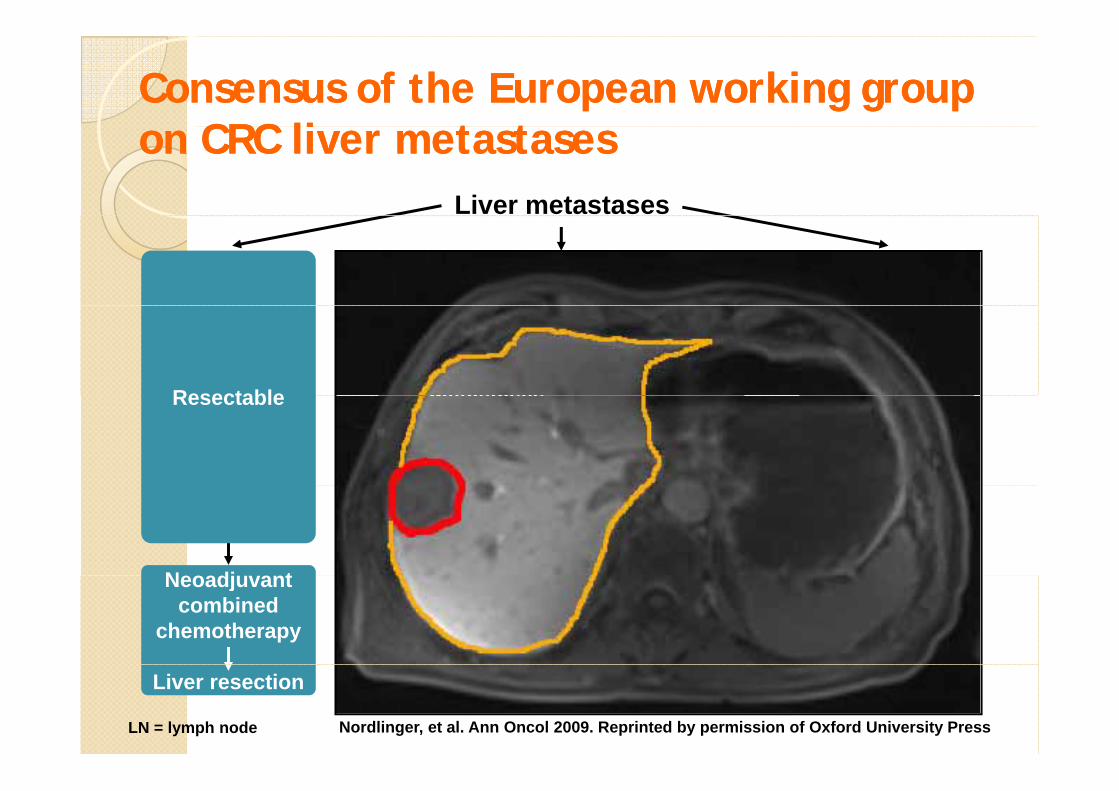
Consensus of the European working group Consensus of the European working group CRC li t t CRC li t ton CRC liver metastaseson CRC liver metastases
Liver metastases
Borderline resectable• Oncological (>1 factor)
Unresectableand neverResectable
g ( )– >4 metastases– size >5cm– synchronous CRC liver
metastaseslikely to beresectable
Resectable metastases– primary LN-positive– positive tumour marker
• Technically difficult
N dj t h th
– close to all hepatic veins– close to both portal branches
N dj tPalliative
chemotherapy±
Neoadjuvant chemotherapy± biologics
Liver resection if sufficient
Neoadjuvantcombined
chemotherapy
biologicsresponseLiver resection
LN = lymph node Nordlinger, et al. Ann Oncol 2009. Reprinted by permission of Oxford University Press
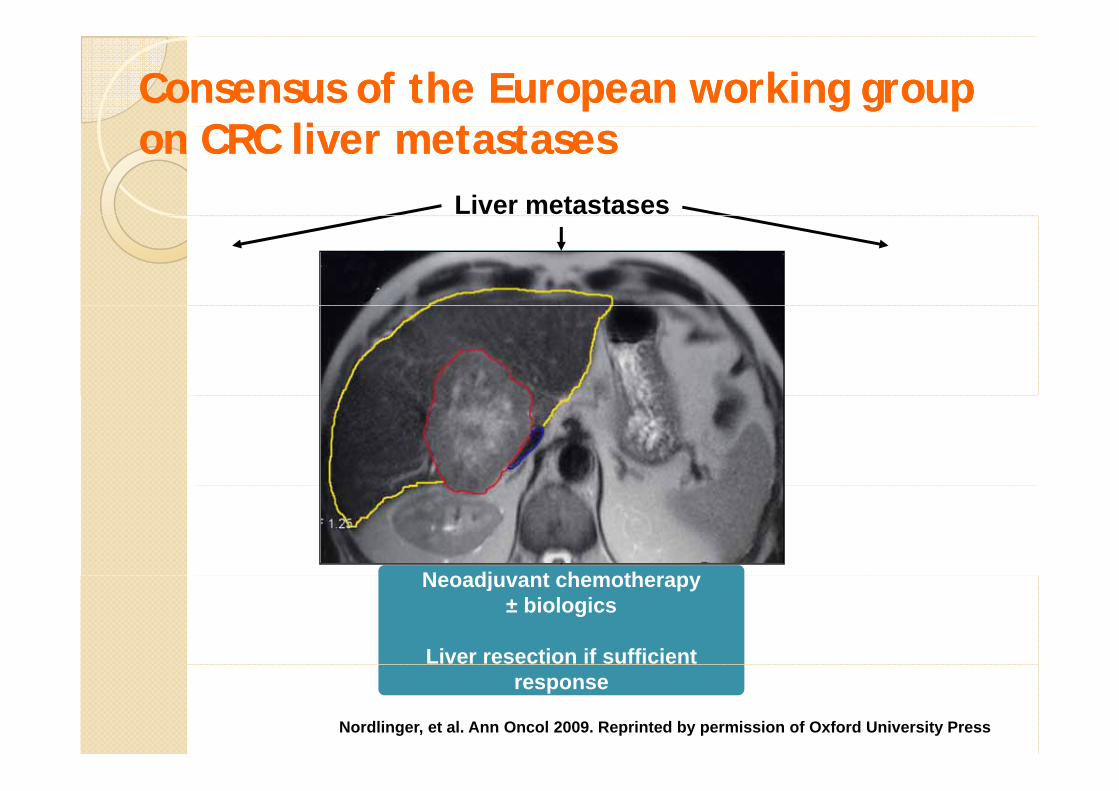
Consensus of the European working group Consensus of the European working group CRC li t t CRC li t ton CRC liver metastaseson CRC liver metastases
Liver metastases
Borderline resectable• Oncological (>1 factor)g ( )
– >4 metastases– size >5cm– synchronous CRC liver
metastasesmetastases– primary LN-positive– positive tumour marker
• Technically difficult
N dj t h th
– close to all hepatic veins– close to both portal branches
Neoadjuvant chemotherapy± biologics
Liver resection if sufficientresponse
Nordlinger, et al. Ann Oncol 2009. Reprinted by permission of Oxford University Press
NEOADJUVANT CHEMOTHERAPY:NEOADJUVANT CHEMOTHERAPY:
is advantageous…is advantageous…
Micro-metastases treatmentPreserves more liver tissueIs independent of the postoperative complicationsSelect a subgroup of less than 10% of patients with
i f h h d i poorer prognosis for whom we have to design new strategies
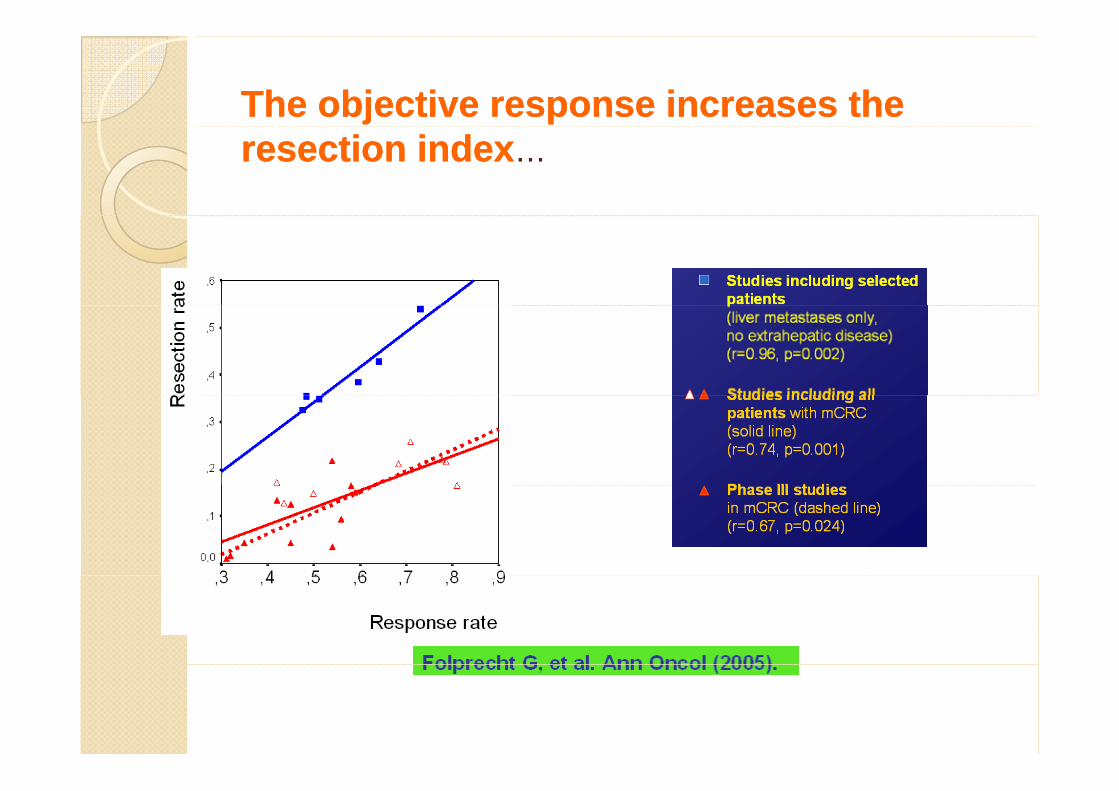
The objective response increases the The objective response increases the resection indexresection index……
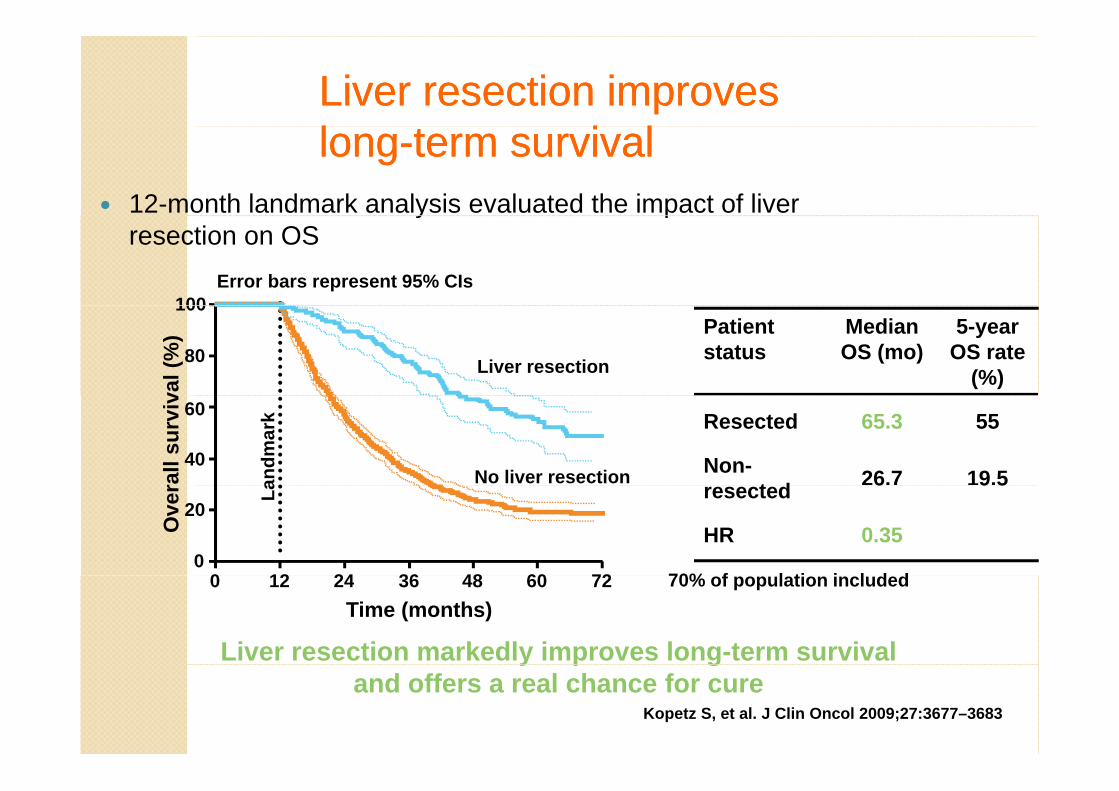
Liver resection improves Liver resection improves ll i li llonglong--term survivalterm survival
12-month landmark analysis evaluated the impact of liver y presection on OS
100Error bars represent 95% CIs
Patient status
Median OS (mo)
5-year OS rate
(%)80
100
val (
%)
Liver resection
Resected 65.3 55
Non-t d 26.7 19.5
40
60
rall
surv
iv
andm
ark
No liver resectionresected 6 9 5
HR 0.35
70% f l ti i l d d0
12 24 36 48 60 72
20
Ove
r La
0 70% of population included
Liver resection markedly improves long-term survival Time (months)
12 24 36 48 60 720
y p gand offers a real chance for cure
Kopetz S, et al. J Clin Oncol 2009;27:3677–3683
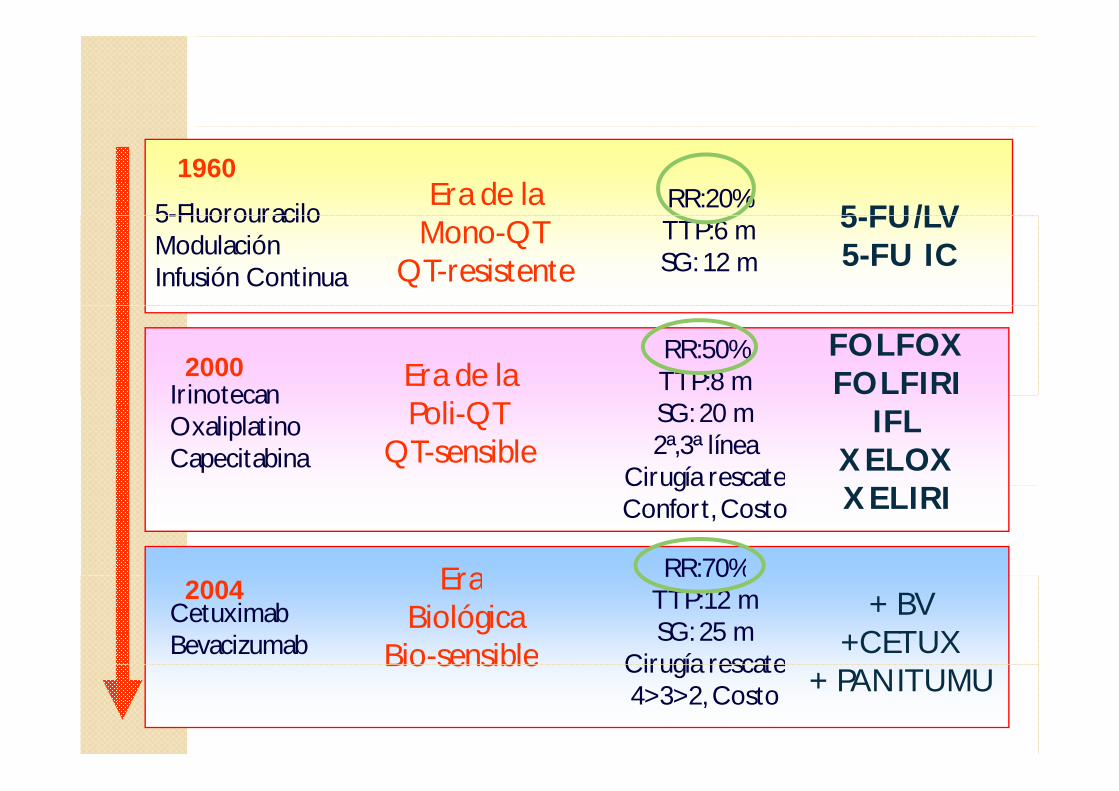
5-FluorouraciloEra de la RR:20%
5 FU/LV
1960
5-FluorouraciloModulación Infusión Continua
Mono-QTQT-resistente
TTP:6 mSG: 12 m
5-FU/LV5-FU IC
Era de laRR:50%TTP:8 m
FOLFOXFOLFIRIIrinotecan
2000
Poli-QTQT-sensible
SG: 20 m2ª,3ª línea
Cirugía rescate
IFLXELOX
IrinotecanOxaliplatinoCapecitabina
Cirugía rescateConfort, Costo XELIRI
Era RR:70%EraBiológica
Bio-sensible
RR:70%TTP:12 mSG: 25 m
Cirugía rescate
+ BV+CETUX
CetuximabBevacizumab
2004
Bio sensible Cirugía rescate4>3>2, Costo + PANITUMU
Personalized therapyPersonalized therapyPersonalized therapyPersonalized therapyOld: Clinical parametersOld: Clinical parameters◦ Patient-based
Age, performance status, co-morbidities, experience with prior therapies, financial implications…
◦ Tumor-based◦ Tumor-basedStage, biology, localization of metastases, number and sites of metastases…
New: Molecular biomarkers◦ Patient-based (pharmacogenomics)◦ Patient-based (pharmacogenomics)◦ Tumor-based
RESPUESTARESPUESTA S
RESPUESTA
SUP
ER
RESPUESTA RADIOLÓGICA
RV
IVENN
CIA
C it i d l OMSCriterios de la OMS
- WHO handbook for reporting results of cancer treatments. Geneva (Switzerland): World Health Organization Offset Publication. No 48: 1979
- Miller AB et al. Reporting results of cancer treatment. Cancer 1981: 47, 207-14
Criterios RECISTCriterios RECIST
- Therase P et al. New Guidelines to Evaluate the Response to Treatment in Solid Tumors. Journal of the National Cancer Institute 2000: 92 (3)Journal of the National Cancer Institute 2000: 92 (3)
- Eisenhauer EA et al. New response evaluation criteria in solid tumors: Revised RECIST guideline (version 1.1). European Journal of Cancer 2009: 45,
Quimioterapia sistémica y hepatectomía
Respuesta radiológica completa: significado83 % Presencia de tumor viable o recidiva in situ al año de la cirugíag
Bemoist S et al. J Clin Oncol 2006 (RC por TAC)
81 % Presencia de tumor viable en pieza qx o durante seguimiento
Tan et al. J GI Surg 2007 (RC por PET)
73 % Ausencia de recidiva in situ tras 31 meses de mediana de seguimientogElias D et al. J Surg Oncol 2004
Metástasis evanescente = potencial problema para el cirujano
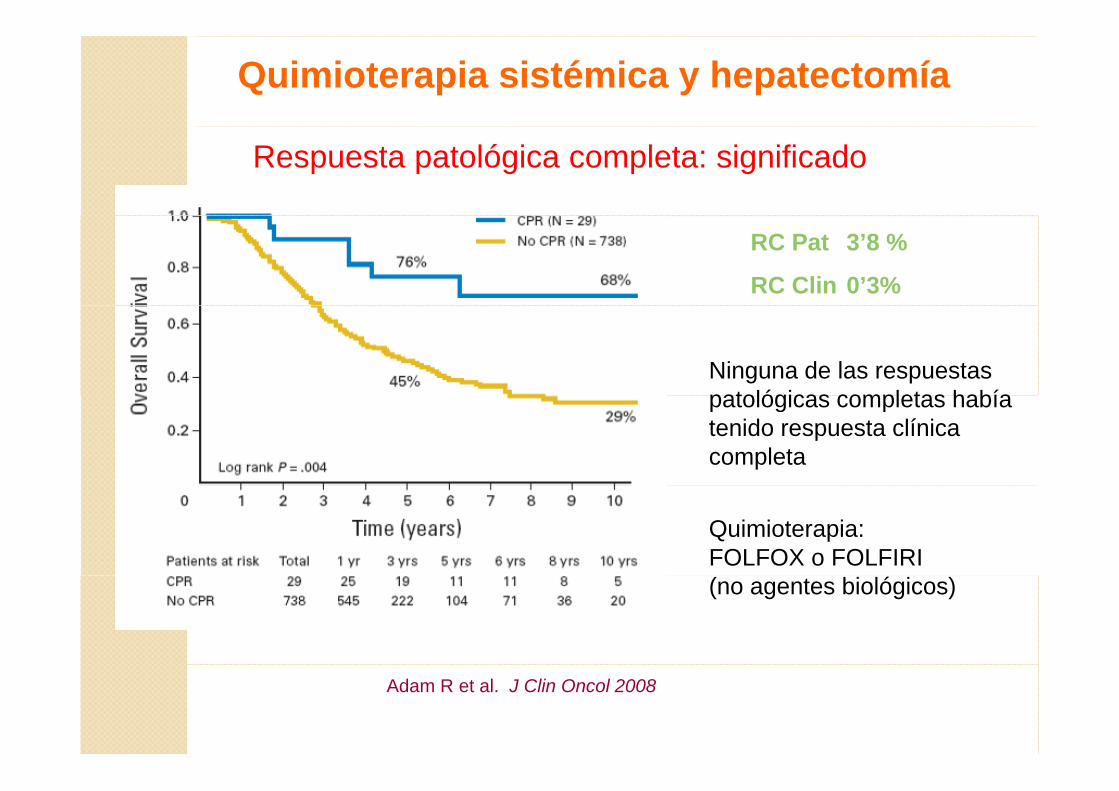
Quimioterapia sistémica y hepatectomía
Respuesta patológica completa: significado
RC Pat 3’8 %
RC Clin 0’3%
Ninguna de las respuestas patológicas completas habíapatológicas completas había tenido respuesta clínica completa
Quimioterapia: FOLFOX o FOLFIRI (no agentes biológicos)
Adam R et al. J Clin Oncol 2008
LIMITACIONESLIMITACIONES
Evaluación de nuevos Fármacos con diferentes mec de acción
Ejm. Inhibidores de angiogénesis, GIST, Hepatoca (SHARP trial)...
No siempre predictor de respuesta histológicaNo siempre predictor de respuesta histológicaEjm. Cáncer de pulmón, recto ...
RECIST: Mide únicamente tamaño no contemplaRECIST: Mide únicamente tamaño, no contempla cambios características de la ls
No es posible conocer viabilidad células tumorales
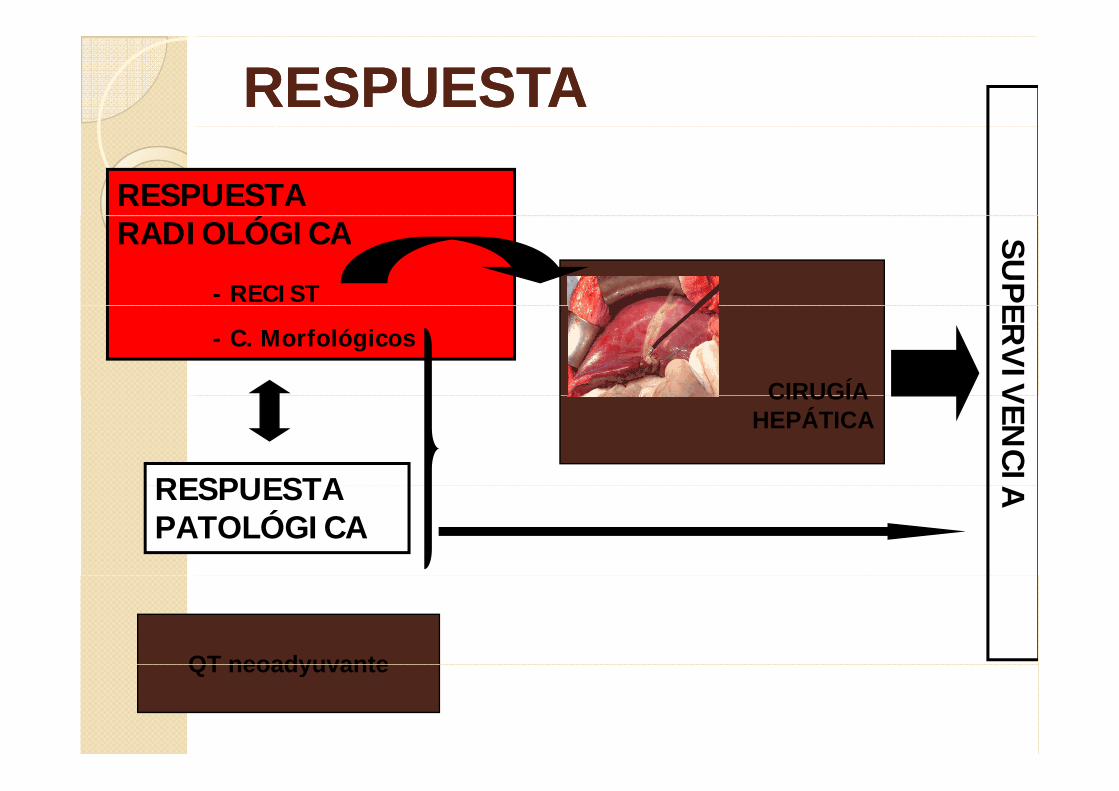
RESPUESTARESPUESTARESPUESTA
ÓRADIOLÓGICA
- RECIST
SUP
E
- C. Morfológicos
ERV
IVCIRUGÍA VEN
CI
CIRUGÍA HEPÁTICA
RESPUESTA ARESPUESTA PATOLÓGICA
QT neoadyuvanteQT neoadyuvante
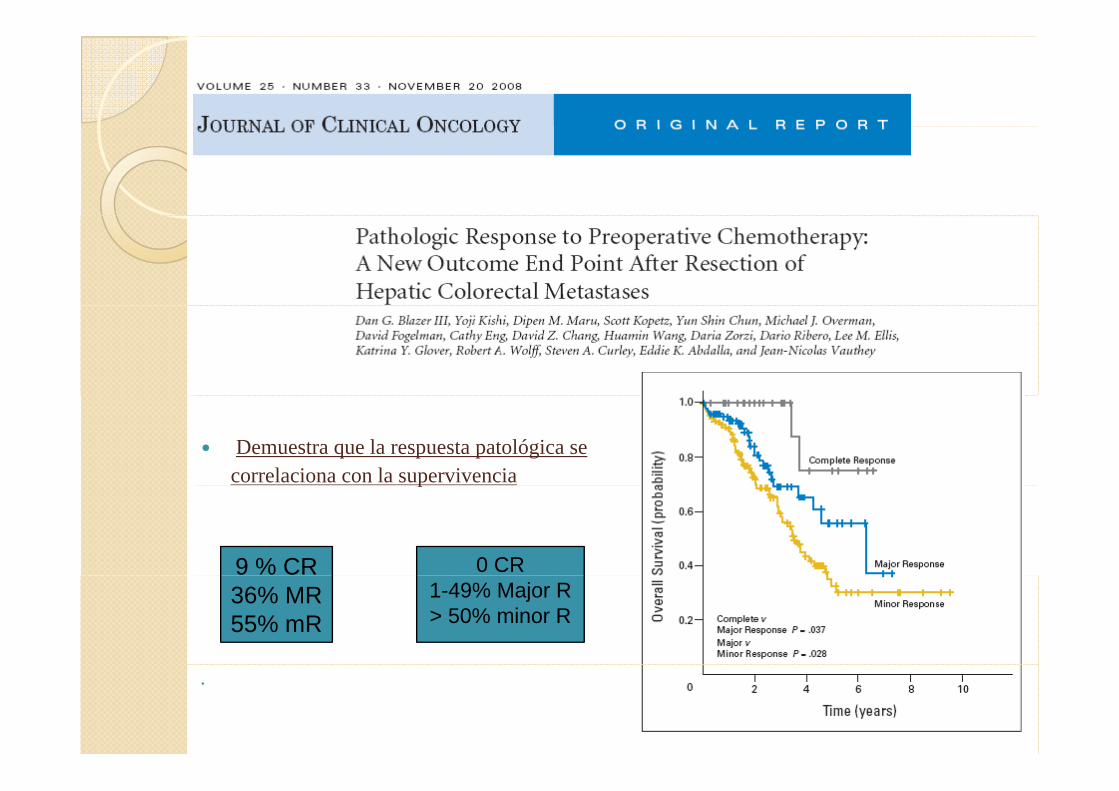
Relación entre respuesta histológica y
supervivencia (publ previa sólo respuesta)
- N 271 ( QT con/sin BV) (37% BV)
Demuestra que la respuesta patológica secorrelaciona con la supervivenciap
0 CR9 % CR1-49% Major R> 50% minor R
36% MR55% mR
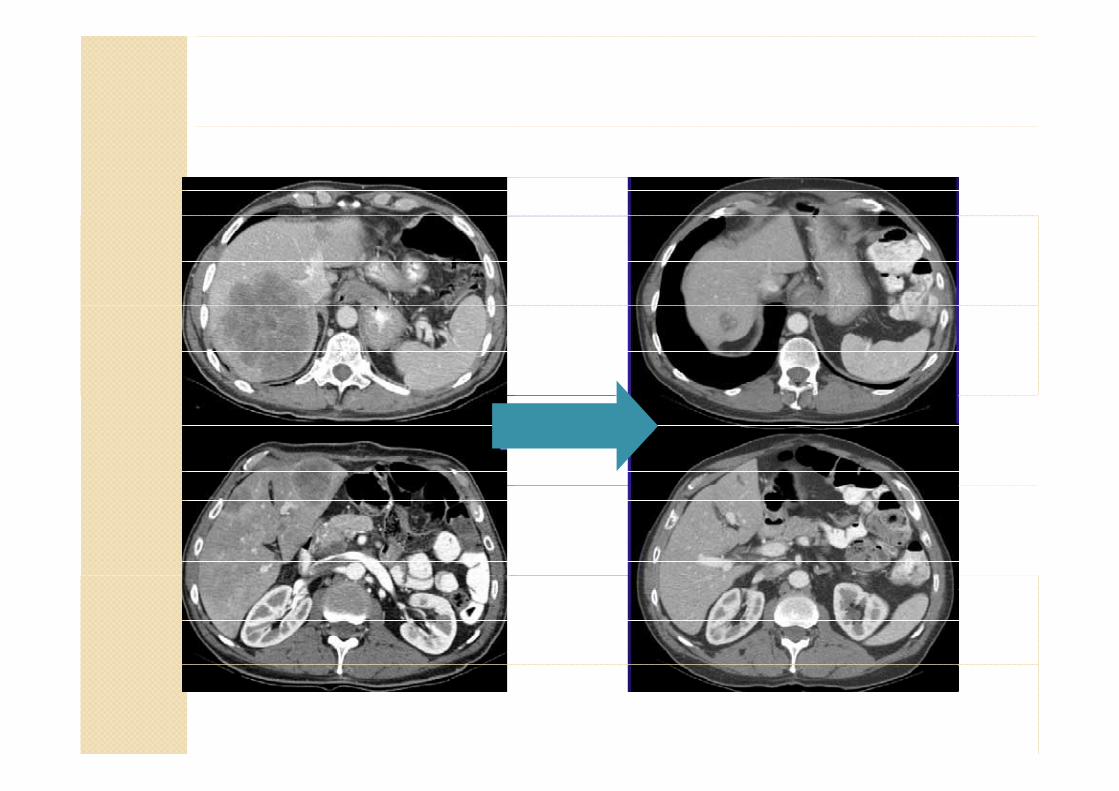
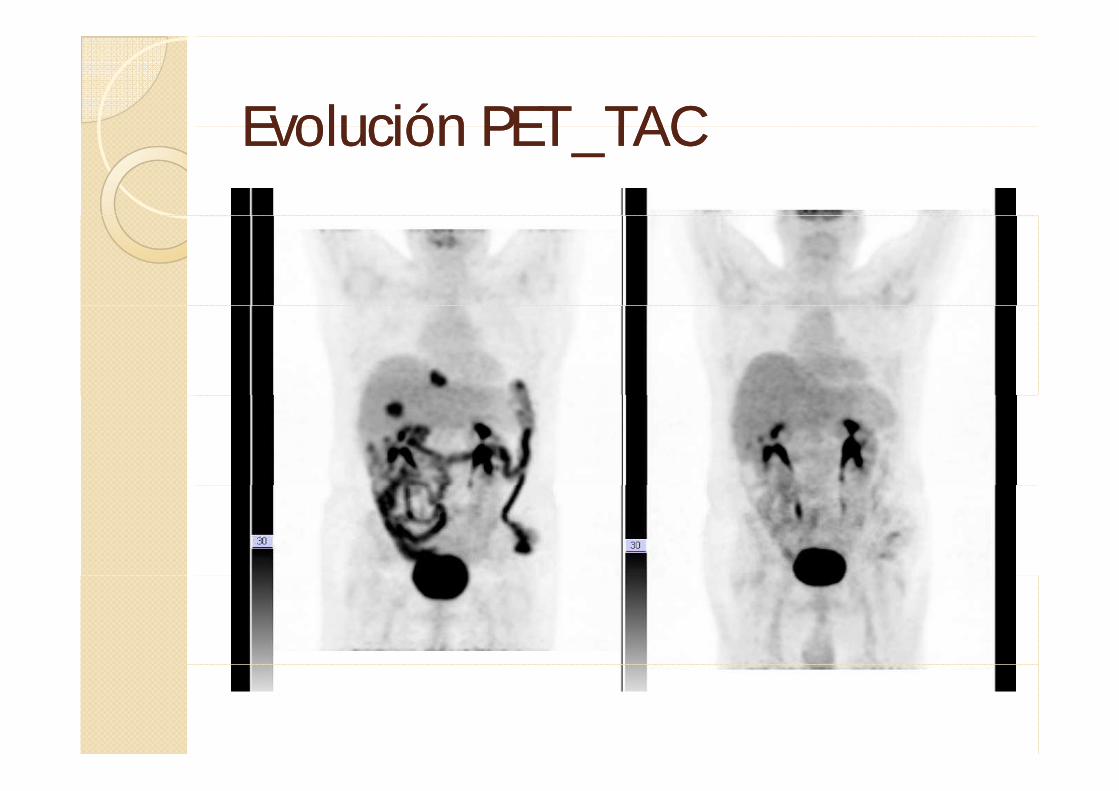
Evolución PET TACEvolución PET TACEvolución PET_TACEvolución PET_TAC
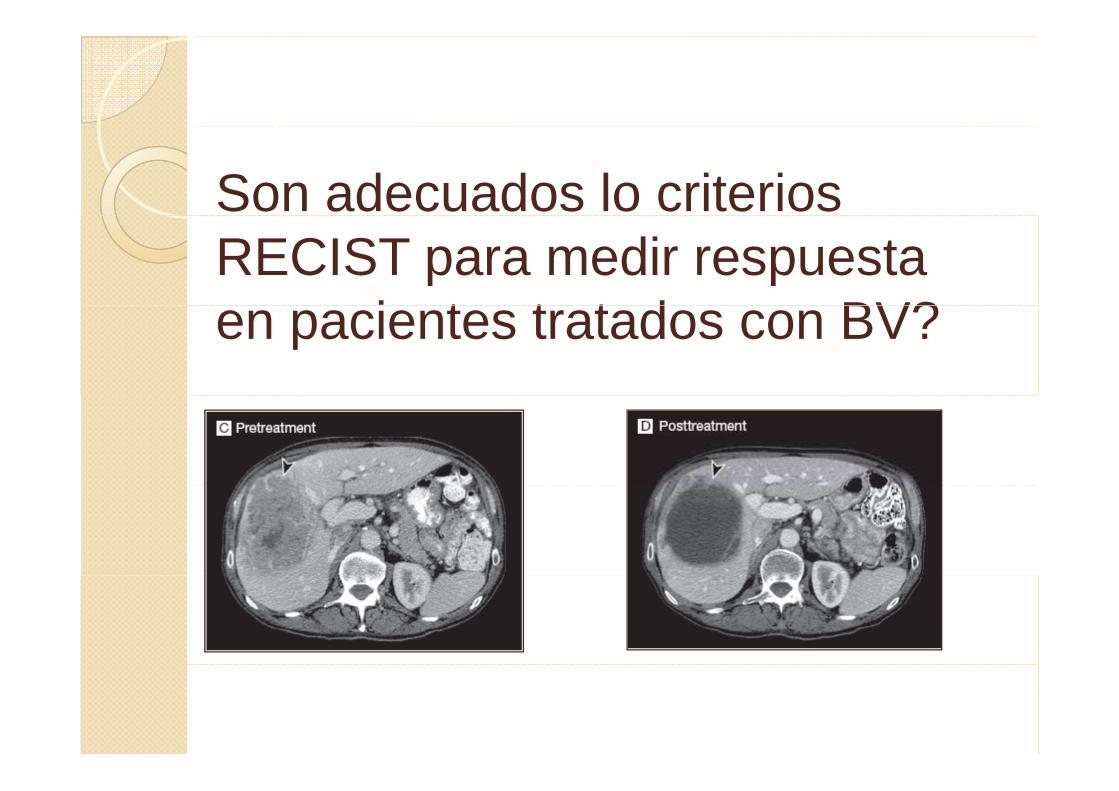
Son adecuados lo criterios RECIST para medir respuesta
i t t t d BV?en pacientes tratados con BV?
¿Debemos seguir usando la respuesta radiológica como método único de valoración previo a la cirugía?¿Cómo debemos evaluar la ¿respuesta radiológica?¿Cuándo debemos usar otros ¿Cuándo debemos usar otros métodos de valoración de respuesta?respuesta?Cúal es el mejor momento para evaluar la respuesta para evaluar la respuesta previo a la cirugia?Duración del tratamiento Duración del tratamiento neoadyuvante?





























