Embed Size (px)
Citation preview

Monitoring The Critically Ill Children
長庚兒童醫院 兒童加護科夏紹軒

• The goals and principles of ICU monitoring
• Characteristics of monitoring critically ill children
• Cardiovascular monitoring
• Respiratory monitoring
• Cerebral monitoring
• Conclusions

Principles and Philosophy in Critical
Care Medicine• Early diagnosis and identification of the
problem• Anticipation of possible events and
complications• The holistic approach to a critical illness• The considered use of technology• Primum non nocere• Recognition of the limits of critical care

The goals of monitoring the critically ills (I)
• DO2=CO CaO2=CO (1.34Hb SaO2+0.003PaO2)
• DO2=CBF (1.34Hb SaO2+0.003PaO2)
• PaCO2= ( VCO2×0.863 ) ÷VA
• CO depends on heart rate, preload, myocardium contractility and afterload
• CBFCPP=MAPICP
• Organ functions: CNS, liver, kidney…etc

Balance between demand and supply
• DO2=C.O. CaO2(supply)• VO2C.O. (SaO2-SvO2)(demand)• VO2 經常是一個常數,所以
C.O. 與 (SaO2-SvO2)成反比,同理,CBF與 (SaO2-SjvO2)成反比
• 因此,監測 DO2 與 VO2可以得知心血管系統供需平衡的狀況

Types of monitorings
• Clinical assessments: PE, CRT, GCS…
• Laboratory tests: ABG, lactate…
• Non-invasive monitoring: EKG, SpO2, NBP, Echo
• Invasive monitoring: ABP, CVP, Swan-Ganz
• Cardiac monitoring
• Respiratory monitoring
• Monitoring neurologic function
• Interactions of organ systems

監測之時機與項目• What?
• How?
• When? How frequent?
• Logical approach to monitorings
–功能決定目標–監測目標是否達成–監測是否有心肺腦及其他系統之併發症產生

• The goals and principles of ICU monitoring
• Characteristics of monitoring critically ill children
• Cardiovascular monitoring
• Respiratory monitoring
• Cerebral monitoring
• Conclusions

Characteristics of monitoring children• Children are smaller
– Every organs are smaller
– Difficult in obtaining invasive accesses
• Children are fragile– Barotrauma
– Complications of invasive procedures
• Structural problems– CHD– Airway stenosis
• Non-conventional therapies– HFOV– NO, surfactant, liquid,
ECMO
• Children are developing– Poor communicating– GCS– Different normal value

Patient (2yo) in Car Accident
• The patient developed following conditions:– Hemorrhagic shock
– Altered mental status
– Short of breath and desaturation

Patient (2yo) in Car Accident
• FiO2=1.0• pH=7.35• PaCO2=47• PaO2=50• SaO2=83%• PIP/PEEP=30/9
• BP=80/50(60)• CVP=10• CI=2.5• ICP=15• CPP=45• GCS=10

• The goals and principles of ICU monitoring• Characteristics of monitoring critically ill
children• Cardiovascular monitoring
– Perfusion– Hemodynamics
• Respiratory monitoring• Cerebral monitoring

Perfusion
• The blood flow and oxygen delivered to the tissue bed.
• Capillary refill time: weakly correlated
• Lactate: lactic acidosis
• Gastric intramural pH (tonometry)

Lactic acidosis and outcome of ECMO
Cheung et al. CCM 2002; 30:2135-2139

Gastric intramural pH (Tonometry)

Gastric tonometry and septic shock
Krafte-Jacobs et al. Chest 1995; 108:220-225

心輸出量的評估• 心輸出量=脈搏次數心搏容積• 心搏容積與以下三參數相關• Preload前負荷 =心臟收縮前內部血液容積• Myocardium Contractility心肌收縮力 =心臟幫浦的力量
• Afterload後負荷 =心臟射出血液所面對的阻力

Hemodynamic Monitoring
• Gold Standards: indicator dilution methods– Fick method: CO=O2 consumption/avDO2– Dye dilution: Indocyanine green– Thermodilution: Swan Ganz, PiCCO
• Alternatives:– Doppler techniques– Bioimpedance

Fick Method

非侵入性監測 NICO

Hemodynamic monitoring
• Pulse rate and strength, skin temperature, capillary refill time, core-peripheral temperature gap
• EKG monitor, CXR, NBP• Echocardiography, • ABP, CVP, SvO2• Pulmonary artery floating catheter, cardiac
catheterization,

如何測量 Hemodynamics?


Thermodilution and Cardiac Output


非侵入性監測: PiCCO

PiCCO: Gödje et al. Crit Care Med 2002 Vol. 30, No. 1


非侵入性監測: Hemosonics

非侵入性監測: Hemosonics

非侵入性監測:Impedance Cardiography
ECG
generator
measuring
measuringgenerator
ECG



Principle Method Advantages Disadvantages
Fick Colorimetry Accurate Require MVO2, error when ETT leak, PTX, FiO2>0.5
NICO Accurate, non-invasive
>20kg, hypercapnea
Dilution PA Accurate, semi-continuous
Affect by respiration, difficult for children, complications, RL CO
Trans-pulmonary
Easy for small p’t, continuous
Require dedicated A line, safe duration?
Dye Accurate Sequential measurement limited by dye clearance,
Lithium Accurate, use pre-existing CV/A line
Toxicity, blood sampling
Doppler Echo Structural and function Expertise, users variations
Trans-esophageal
Continuous, rapid insertion, less invasiv
Probe fixation, individual errors, tracked accurately
Bio-impedance
Non-invasive Doubtful accuracy in critical illness

Disadvantages of invasive cardiovascular monitoring
• Difficult to obtain access• Malposition: arterial puncture (2-16%). • Pneumothorax (incidence 2-4%)• Arrhythmias. • Knotting. • PA rupture with a mortality rate of 50%. • Infection• Thromboembolisms



非侵入性心輸出量之評估方法• 理學檢查
– Perfusion:微血管回填時間、肢端脈搏、尿量
–皮膚溫度、顏色(發紺、蒼白 )
• 心輸出之評估–心電圖– *血壓計– *超音波
• Perfusion– MvO2– Gastric
Tonometry


Tips for cardiovascular monitoring
• The influence of PEEP on PAOP (or CVP): Do we have to disconnect ventilator to measure CVP and PAOP?
• Can pressure represent volume (the true preload)? Or can any preload parameters predict the response to fluid challenge?

tPAOP = eePAOP [PEEPtot (PAOP/ Palv)]
Paw
cmH2O
PAP/PAOP mmHg
disconnection
Palv
PAOP
Nadir PAOP
Teboul et al. CCM 2000, 28(11); 3631-3636

CVP, PAOP and preload
• No correlation between CVP, PAOP and RVEDVI, LVEDVI or stroke volume index
• The post saline infusion changes of CVP and PAOP have no correlation with SVI
• SVI LVEDVI, SVI LVEDVI• Initial CVP does not correlate with PAOPPAOP CVP
• Kumar et al. CCM, 2004; 32:691-699

Response to fluid challenge
• Respiration variation in CVP predict response to fluid challenge
• Magder et al. J Crit Care 1992; 7:76-85
• Respiratory changes in arterial pulse pressure can predict response to fluid challenge
• Michard et al. Am J Respir CCM 2000; 162:134-138

Respiratory variations in CVP predict response to fluid challenge• 33 ICU patients
– 12 spontaneous ventilation– 21 positive-pressure ventilation
• Spontaneous inspiratory effort > 2mmHg decrease in PAOP
• Predictor: inspiration-associated decrease in Pra 1mmHg POSTIVE response– < 1mmHg NEGATIVE response
• Challenge: 250-500ml NS infused until Pra increased by 2 mmHg
• Positive response: increase in cardiac output > 250ml/min• Magder et al. J Crit Care 1992; 7:76-85

Respiratory Changes in Arterial Pulse Pressure and Fluid Responsiveness
Michard et al. Am J Respir Crit Care Med Vol 162. pp 134–138, 2000

• The goals and principles of ICU monitoring
• Characteristics of monitoring critically ill children
• Cardiovascular monitoring• Respiratory monitoring• Cerebral monitoring

Respiratory monitoring
• Oxygen content/Gas exchange• CaO2=(1.34HbSaO2+0.003PaO2)• 即使少量增加 Hb 與 SaO2 可以明顯影響 CaO2
• 增加 SaO2 可提高 CaO2 :例如可增加 FiO2, PEEP
• 監測 Hb, SaO2, PaO2

Respiratory monitoring
• 監測異常的 CaO2 與 CO2排除不能• 監測異常的肺換氣動力學• 監測併發症發生之可能性• 侵入性監測
ABG, IABG• 非侵入性監測
Pulse oximeter, SpO2, ETCO2, PtcO2, Ventrak mechanical graphics

How to interpret and use ABG
• pH, PaCO2, PaO2, HCO3, BE, SaO2
• PaCO2= ( VCO2×0.863 ) ÷VA
• A-a gradient=PAO2-PaO2=FiO2(PB-47)-PaCO2/k-PaO2
• CaO2=(1.34×Hb×SaO2)+(0.003×PaO2)
• pH=pK+log[HCO3/0.03(PaCO2)]
• IABG? CBG? VBG?

Yildizdas et al. Arch Dis Child, 2004; 89:176-180
R2=0.994
R2=0.995
R2=0.957
R2=0.975
R2=0.945
R2=0.981
R2=0.996
R2=0.990
116 patients in NICU and PICU, compare ABG, VBG (Central venous)and CBG

Pulse Oximetry


The limit of pulse oximetry
• Dyshemoglobinemias– COHb– metHb
• Light leakage• Dyes• Low SaO2 (<70%?)• Hb < 3g/dL• Hypotension
– < 30mmHg
• Nail polish– Blue and black 3-5%
• Venous pulsation• Probe mal position• Motion artifact• Skin pigmentation
– Melanin
– bilirubin

End-tidal CO2

Area p=q

X=alveolar ventilation, Y=alveolar dead space, Z=airway dead space,
Y+Z
X+Y+Z Vd/Vt=

Vd/Vt: Clinical for Extubation Hubble , CCM , 2000. Extubation determined by the clinical team using standard clinical assessment. Minimal vent settings for extubation: -FiO2 0.40 -PEEP 7cm H2O -PIP 30cm H2OPrior to extubation , Vd/Vt was calculated from a single breath CO2 waveform. (CO2SMO Plus Monitor , Novametrix Medical Systems)


Results: Individual Outcomes
Vd/Vt Successful
Extubation
Failed
Extubation
0.10-0.50 24/25(96%) NIV(1)
0.51-0.64 6/9(67%) NIV(3)
0.65-0.95 2/10(20%) NIV(6),PPV(2)
P<0.001

Transcutaneous pO2
Skin surface Epidermis Dermis
Artery
Vein
100 mmHg
0 mmHg
40-42C
30 C
27 C

The limit of transcutaneous blood gas
• Dissociate with arterial CO2 in shock or hypothermia
• The electrode is heated to 38-44C and increase local CO2 production, capillary CO2 solubility and diffusion through the stratum corneum,
• Risk of burn.• Adjunct to ABG , HFOV

Mechanical graphics
0 15 30 45
75
150
250
Airway Pressure(cmH2O)
Volu
me(m
l)
Vt=145ml
PEEP
PIP=42
2Y ARDS
Low compliance
Dynamic compliance=Vt/(PIP-PEEP)=3.9
Ins
Exp

Mechanical graphics
0 15 30 35Airway Pressure(cmH2O)
75
150
250
Volu
me(m
l)
Vt=145ml
PEEP
Dynamic compliance=Vt/(PIP-PEEP)=7.6
PIP=29
Exp
Ins

Tidal Volume DeterminationCannon , AJRCCM , 2000.
Population: PICU pts<16yrs old(n=98) Ventilator circuit: -infant: n=70 ; 2.8± 2.3mos -pediatric: n=28 ; 7.3± 5.6 yrs Ventilator:SV300(Siemens) Pneumotach -placed between ETT & vent circuit -CO2SMP Plus Monitor (Novametrix)Effective Vt = Vt at exp valve [circuit compliance ﹣ (PIP-PEEP)]

Results: Infant Circuit
Vt(ml) p
Exp valve Vt 70.4 ± 31.1
Calcuated Vt 59.2 ± 28.8 <0.0001
Pneumotach Vt 39.4 ± 21.5 <0.0001
The Vt as measured at the ETT was onaverage only 56% of that measured at theexpiratory valve of the ventilator.


Vt(ml) p
Exp valve Vt 185.4 ± 96.6
Calcuated Vt 167.8± 94.6 0.16
Pneumotach Vt 135.3± 75.8 0.03
Results: Pediatric Circuit
The Vt as measured at the ETT was onaverage 73% of that measured at the exp.valve of the ventilator.


• The goals and principles of ICU monitoring
• Characteristics of monitoring critically ill children
• Cardiovascular monitoring
• Respiratory monitoring
• Cerebral monitoring

腦監測 • 腦功能
– GCS, EEG, BIS
• 監測腦灌流供需功能– CBF, Autoregulation, CMRO2
• 防止二度傷害–避免腦缺血 Cerebral Ischemia–預防 /避免高危險狀況
ICP, °C, hypo or hyper-glycemia

腦監測
• 項目• Brain function
• CBF, CPP
• CMRO2
• ICP
• General clinical
• 方法• GCS, BIS, EEG
• TCD
• NIRS
• JV Saturations
• ICP monitor

腦功能之監測• Glasgow Coma Scale: different scoring
according to AGE, infants, children, adult
• Continuous EEG monitoring
• Processed electroencephalogram. Use a one lead EEG to evaluate the awareness of patients during anesthesia: BIS or AEP


Bispectral IndexHsia et al. Ped Neurol 2004; 31: 20-
23
R=0.8, p<0.05

腦血流量監測
0
1020
3040
5060
70
Reduced Normal Elevated
GR/MDSD/PVSDead
CBF Groups
% of Patients
CBF vs. Glasgow outcome score: 3 months post injuryRobertson et al. 1992

腦血流量監測
• CBFCPP(cerebral perfusion pressure)=MAP-ICP(CVP, if CVP>ICP)
• 經顱骨超音波都卜勒監測 -TCD
• 遠紅外線監測 -NIRS-Near Infrared Spectroscopy
• Jugular vein saturation monitoring

Impaired Pressure-Flow AutoregulationMaximal Normal MaximalVasodilation Autoregulation Vasoconstriction
0 25 50 75 100 125 150 CPP (mmHg)
CBFUnexpected Ischemia
Unexpected Hypermia
Normal AutoregulationDisrupted AutoregulationPartial Disrupted Autoreg

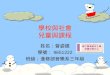
經顱骨超音波都卜勒監測 -TCD
• 優點:–非侵入性–可連續監測 *
–可知道腦血管阻力
• 缺點:–執行者之技術與探頭位置
–血流速度而非流量–定性而非定量–無法分辨 ICP與 CBF
監測血流速度改變頻率之訊號

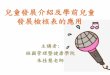
經顱骨超音波都卜勒監測 -TCD
腦血流速率
CPP遞減
Systolic velocity
Diastolic velocity
Reversal of diastolic flow
Reductions in CPP Diastolic Velocity Systolic Velocity Reversal of Diast Vel. Oscillating Pattern

經顱骨超音波都卜勒監測 -TCD
PulsatilityIndex (PI)
ICPPI = Vel(syst) - Vel(diast) / Vel(mean)
TCD Pulsatility Index is a Nonspecific Marker of ICP

遠紅外線監測 -NIRS
• 優點:–非侵入性–定量–可監測代謝率– HbO2
/DeoxyHb
• 缺點:–顱骨厚度不同–腦直徑大小不同
– Hb異常會影響結果
Pulse oximeter for the brain

遠紅外線監測 -NIRS
010203040506070
0 10 20 30 40 50 60 70
R2 = 0.83NIR
Xe 133 Clearance

腦代謝率 CMRO2 之監測• CMRO2=CBFAVDO2(CaO2-CjvO2)• CMRL=CBF AVDL(The difference of
lactate in artery blood and jugular venous blood)
• LOI= AVDL/AVDO2• 當 LOI<0.08 , CMRO2是恆定的,而
CBF 與 AVDO2成反比• 當 LOI0.08表示腦代謝增加,上述不
真。

腦代謝率 CMRO2 之監測
CMRO21.81.51.20.90.60.30
0 0.4 0.8 1.2
2.0
4.0
6.0
CBF(ml/gm/min)
AV
DO
2(m
ol/ml)
ischemia
infarction hyperemia
normal
hypo- perfusion
Robertson J of Neurosurg 1989

侵入性的 DO2 評估Jugular bulb catheter
Transverse sinus
Jugular bulb
At about the level of mastoid process Internal
jugular vein
SCM muscle


SjvO2 monitoring in PICU
• Total number: 20 • Major diagnoses :
– Close head injury :4/20 (20%)– Meningoencephalitis: 11 /20 (55%) – EV 71 with cardiopulmonary failure : 5/20
(25%)
• Oxygen extraction ratio (OER)=(SaO2-SjvO2)/SaO2, normal:24-42%

Episodes of Increased OER (I)
P’t No. OER>40% episodes/pt
Head injury 2/4 2/2
Meningoencephalitis
6/11 9/6
EV 71 with PE 2/5 3/2
Total number 10/20 14/10

Clinical Condition Correlated with Increased OER
• BP– 5 episodes : hypertension– 4 episodes : hypotension – 1 episode: normotensive

Restore OER
• 10ml/kg normal saline challenge or blood transfusion for each increased OER episodes when CVP 9 mmHg in ≦6 episodes
• Mannitol infusion in 2 episodes• Adjust intropic agents in 2 episodes• All patients restored OER after
managements

0
50
100
150
200
250
Time(Hr) 0
0.5
0.75 3.5
4.5
8.5
10.5
14.5
18.5
22.5 26 27 28
30.5
32.5
38.5
40.5
42.5 46 50
0
20
40
60
80
100
120
140HR
SaO2
GCS
SBP(mmHg)
CVP(mmHg)
SjvO2
1yo EV71 patient witbh jugular catheter in place
No difference in dopamine and epinephrine inf rate
NS 150ml at 0.75hr, 300ml at 22.5hr, 150ml+RBC1U at 40.5hr

顱內壓監測• 腦室內監測 : Gold Standard
–整體壓力 Global Pressure - mean of entire brain–治療 - drainage
• 腦實質內或硬腦膜下監測 : Fiberoptic–局部壓力 Regional Pressure - local tissue–無治療性 Not Therapeutic–併發症較少
bleeding (0.5 vs. 1-6%) infection rate


顱內壓順應性之變化曲線
顱內容積
顱內壓
危險區
高危險區
低順應性:
少許容積之變化即可能造成嚴重壓力變化!

顱內壓曲線P1 P2 P3
P1 P2 P3
正常順應性
順應性變低

Age SBP/DBP MAP CPP ICP
1-3 days 64/41 50 (38-62) 40 1.5-6 mmHg
1mo-2 yr. 95/58 72 (65-86) 62
2-5 yr. 101/57 74(65-85) 64 3-7 mmHg
6-7 yr. 104/55 71(65-91) 61
8-9 yr. 106/58 74(65-94) 64
10-11 yr. 108/60 76(65-96) 66 10–18 mmHg
12-13 yr. 112/62 79(65-98) 69
14-15 yr.Boys Girls16-18 yr.Boys Girls
116/66112/68121/70110/68
83(65-103)83(65-98)
87(65-104)82(65-98)
73737772

0
20
40
60
80
100
12019:40
21:25
21:50
00:30
01:00
03:00
05:00
07:49
10:00
13:00
15:05
17:00
21:00
01:00
09:00
09:10
09:40
11:00
13:00
14:30
17:00
19:00
21:00
01:00
03:00
05:00
07:00
09:00
11:00
15:00
17:50
19:00
21:00
23:00
01:00
03:00
05:00
07:00
09:00
11:00
13:00
15:00
17:00
21:00
01:00
03:00
05:00
09:00
11:00
12:00
13:00
15:00
17:28
20:00
01:00
03:00
05:00
09:00
11:00
13:00
15:00
17:00
19:00
21:00
01:00
05:00
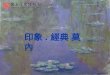
11 11月 日 11 12月 日 11 13月 日 11 14月 日 11 15月 日 11 16月 日 11 17月 日 11 18月 日
Midazolam before suction since Nov 13 9:00Dopamine 50mg in D5w20cc run 1ml/hrBomin 2mg in16cc run 0.1ml/hrHyperventilation on Nov.12 8:25am, off Nov.14 12:00Thiopental 84 mg in 16.6 cc run 1.5 cc/hr Nov.14 16:00
----ICP----CPP----MAP----CVP

腦監測應用於治療• 降低腦部代謝
– Mild hypothermia:– 33-35ºC–控制痙攣、減少刺激– Sedation/analgesics?
midazolam, morphine, phenobarbitalthiopental,注意 BP
• 增加氧氣運送–增加 FiO2–增加 Hb–增加心輸出量– Preload:CVP>10避免過高 CVP
– Contractility– Afterload

腦監測應用於治療• 減少顱內壓
–使用Mannitol/ furosemide以維持滲透壓 310-320mOsm以上
–控制換氣,維持 PaCO2:30-35mmHg
• 增加 CPP–增加心輸出量–當心輸出量足夠時,使用血管升壓素如norepinephrine以增加血壓

Conclusions
• Early diagnosis and identification of the problem• Anticipation of possible events and complications• The holistic approach to a critical illness: • The considered use of technology• Primum non nocere• Recognition of the limits of critical care