-
7/28/2019 Neumonia y Sistema Cardiovascular Lancet 13.pdf
1/10
Review
496 www.thelancet.com Vol 381 February 9, 2013
Acute pneumonia and the cardiovascular system
Vicente F Corrales-Medina, Daniel M Musher, Svetlana Shachkina,
Julio A Chirinos
Although traditionally regarded as a disease confined to the
lungs, acute pneumonia has important effects on thecardiovascular
system at all severities of infection. Pneumonia tends to affect
individuals who are also at highcardiovascular risk. Results of
recent studies show that about a quarter of adults admitted to
hospital with pneumoniadevelop a major acute cardiac complication
during their hospital stay, which is associated with a 60% increase
inshort-term mortality. These findings suggest that outcomes of
patients with pneumonia can be improved byprevention of the
development and progression of associated cardiac complications.
Before this hypothesis can betested, however, an adequate
mechanistic understanding of the cardiovascular changes that occur
during pneumonia,and their role in the trigger of various cardiac
complications, is needed. In this Review, we summarise
knowledgeabout the burden of cardiac complications in adults with
acute pneumonia, the cardiovascular response to thisinfection, the
potential effects of commonly used cardiovascular and
anti-infective drugs on these associations, andpossible directions
for future research.
IntroductionPneumonia an cariac isease are leaing causes
ofmorbiity an mortality worlwie.15 Community-acquire pneumonia
affects more than 5 million aults,an causes 11 million hospital
amissions an morethan 60 000 eaths every year in the USA.1,2
Cariacisease affects more than 30 million US aults an leasto 5
million hospital amissions an more than300 000 eaths every year.3,6
Disease burens in Europeare similar.4,5,7 Pneumonia an cariac
isease oftencoexist in the same patients.8 For example, more
thanhalf of elerly patients amitte to hospital withpneumonia also
have a chronic cariac isoreranassociation that will become more
prevalent as the
population continues to age.8
Investigators have reporte a high incience of
cariaccomplications uring the course of community-acquirepneumonia,
an have shown that these events areinepenently associate with
increase short-termmortality.9 In view of this association, full
appreciation ofthe magnitue of this problem an an unerstaning ofthe
cariovascular consequences of this infection areimportant. In this
Review, we summarise the presentknowlege about the buren of cariac
complications inault patients with pneumonia, the
cariovascularresponse to acute pneumonia, an the potential effects
ofcommonly use cariovascular an anti-infective rugson these
associations. We also iscuss potential areas for
future research.
Burden of cardiac complications in patients withpneumoniaFor
several ecaes, investigators have note that acuterespiratory
infections, incluing pneumonia, oftenprecee the evelopment of acute
cariac events, an acausal relation has been propose.10,11 For acute
coronarysynromes specifically, this association satisfies most
ofBrafor Hills criteria for causality an is iscusseelsewhere.11,12
The high prevalence of cariac arrhythmiasafter an episoe of
pneumonia an the temporality of thisassociation also suggest a
causal role for pneumonia in
cases of pneumonia-associate arrhythmias.9
Although asimilar argument can be mae for the association
betweenpneumonia an heart failure, this relation is probablymore
complex. Results of clinical stuies suggest thatpatients with heart
failure have reuce immunologicalresponses, an experimental evience
inicates thatpulmonary congestion can promote the growth ofcommon
bacteria such as Streptococcus pneumoniae(pneumococcus) an
Staphylococcus aureus in the lungs.1315Epiemiological ata also
suggest that pre-existing heartfailure is a risk factor for the
evelopment of pneumonia. 16Therefore, the causeeffect relation
between pneumoniaan heart failure might be biirectional. A causal
relationbetween infections in other organs, such as the urinary
or
gastrointestinal tracts, an acute cariac events has alsobeen
suggeste, but has not yet been characterise.17,18
Although acute cariac events have been recognise asimportant
complications in patients with pneumonia
Lancet 2013; 381: 496505
Published Online
January 16, 2012
http://dx.doi.org/10.1016/
S0140-6736(12)61266-5
Department of Medicine,
University of Ottawa, ON,
Canada (V F Corrales-Medina MD,
S Shachkina MD); Ottawa
Hospital Research Institute,
ON, Canada
(V F Corrales-Medina,
S Shachkina); Departments of
Medicine and Molecular
Virology and Microbiology,
Baylor College of Medicine,Houston, TX, USA
(Prof D M Musher MD); Medical
Care Line, Infectious Disease
Section, Michael E DeBakey VA
Medical Center, Houston, TX,
USA (D M Musher);Division of
Cardiology, University of
Pennsylvania,PA, USA
(J A Chirinos MD);and
Philadelphia VA Medical Center,
PA, USA (J A Chirinos)
Correspondence to:
Dr Vicente F Corrales-Medina,
Department of Medicine,
University of Ottawa,
1053 Carling Avenue, CPC 470,
Ottawa, ON, K1Y 4E9, [email protected]
Search strategy and selection criteria
We searched Medline (from 1946 to May 15, 2012), Scopus
(from 1950 to May 15, 2012), and Embase (from 1947 to
May 15, 2012) databases, using detailed search strategies
(appendix). We developed search methods to capture clinical
and experimental evidence of cardiac complications in
patients
with pneumonia, and the effects of pneumonia on the human
cardiovascular system, the consequences of commonly used
cardiovascular drugs on the outcomes of patients withpneumonia,
and the effects of available antibiotics on the
cardiovascular system. Only articles in English, Spanish,
Russian,
German, French, and Chinese were included. Articles in
languages other than English were translated by medical
doctors proficient in those languages. Then, relevant
articles
were reviewed in their entirety and discussed by the
investigators to establish their relevance to this
Review.When
appropriate, we preferred to cite comprehensive reviews of
the
literature rather than many individual reports. Similarly,
our
Review focuses on conceptual syntheses of data, rather than
detailed descriptions of original research.
See Online for appendix
-
7/28/2019 Neumonia y Sistema Cardiovascular Lancet 13.pdf
2/10
Review
www.thelancet.com Vol 381 February 9, 2013 497
since the early 20th century, the magnitue of this problemhas
only recently begun to be appreciate fully.19 A meta-analysis of 25
stuies reporting the incience of cariacevents within 30 ays of
pneumonia iagnosis reportecumulative rates of new or worsening
heart failure (14%,
range 733%), new or worsening arrhythmias (5%, range111%), an
the acute coronary synromes myocarialinfarction or unstable angina
(5%, range 111%) in patientsamitte to hospital with pneumonia.20
Most stuies,however, i not use clear efinitions for the
outcomesinvestigate, relie on retrospective chart review for
theirascertainment, or were restricte to high-risk populations(eg,
veterans, patients with iabetes, an elerly patients).In their 2012
analysis of a prospective multicentre cohortof 2344 unselecte
patients with community-acquirepneumonia (1343 inpatients an 944
outpatients), Corrales-Meina an colleagues reporte the 30-ay
incience ofwell-efine cariac complications.9 In this cohort, new
orworsening heart failure, new or worsening arrhythmias,
an myocarial infarction occurre in, respectively, 21%,10%, an 3%
of inpatients, an 14%, 10%, an 01% ofoutpatients. Overall, cariac
complications (efine as anyof the aforementione events) occurre in
27% of in-patients an 2% of outpatients.9 Cariac arrest occursin up
to 3% of patients amitte to hospital withcommunity-acquire
pneumonia.21
The occurrence of two or more types of cariac event ina patient
with pneumonia is not uncommon an hasbeen reporte in 2040% of
patients who evelop cariaccomplications.9,19 In this setting, the
recognition ofmyocarial infarction is usually precee by the
iagnosisof other cariac events (69% of patients). 9 Conversely,
new or worsening heart failure an arrhythmias are thefirst
recognise, or only, pneumonia-associate cariacevent in most cases
(85% an 69%, respectively).9
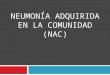
Risk for cariac complications is higher in the first feways
after a pneumonia iagnosis, with about 90% of
these events recognise within 7 ays of iagnosis, anmore than
half ientifie within the first 24 h (figure 1).9,22Risk factors for
cariac complications inclue oler age(about 86% of cariac
complications occur in peopleage 60 years), nursing home resience,
pre-existingcariovascular isease, an greater severity of
pneumoniaat presentation.9,22,23 Nonetheless, about a thir
ofpneumonia-associate cariac complications occur inpatients with no
history of clinical cariac isease, aquarter of cases are in
patients consiere to be at low riskon the basis of their pneumonia
severity inex score, anabout three-quarters of cases arise in
patients thought notto nee intensive care after their first
assessment.9,19,21,24
Cariac complications have an important effect on the
clinical course of patients with pneumonia. In patientsamitte to
hospital with pneumonia who experienceclinical failure to
treatment, about a thir o so because ofcariac complications.25
Diagnostic criteria for myocarialinfarction are present in as many
as 50% of patients withpneumonia who nee intensive care unit
treatmentwithin 24 h of amission to hospital. 23 Cariac
compli-cations are also the irect or unerlying cause of eath in27%
of pneumonia-associate eaths.26 Death within30 ays of pneumonia
iagnosis is five times morecommon in patients who evelop cariac
complicationsthan in those who o not.9 Even after ajustment
forbaseline risk, cariac complications are associate with a
Figure 1: Timing of cardiac complications in patients with
community-acquired pneumonia
Cardiac complications included any of the following cardiac
events: new or worsening heart failure, new or worsening
arrhythmias, or myocardial infarction. Data
from the Pneumonia Patient Outcomes Research Team cohort study.
Adapted from Corrales-Medina et al,9 with permission of Wolters
Kluwer Health.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
25 26 27 28 29 300
5
10
15
20
25
30
35
40
45
50
55
Patientswithcardiaccomplications(%;n=377)
Day of cardiac complications relative to day of pneumonia
diagnosis
-
7/28/2019 Neumonia y Sistema Cardiovascular Lancet 13.pdf
3/10
Review
498 www.thelancet.com Vol 381 February 9, 2013
60% increase in pneumonia-associate short-termmortality,9 an lea
to one in four reamissions afterhospitalisation for
pneumonia.27
Effects of pneumonia on the cardiovascularsystemThe present
unerstaning of the human cariovascularresponse to infections,
incluing pneumonia, is erivemainly from stuies of critically ill
patients with septicshock. This isorer is characterise by inability
of the
peripheral vasculature to constrict espite
increaseconcentrations of catecholamines an increase activityof the
reninangiotensinalosterone system;28 myo-carial systolic an
iastolic ysfunction, mainly of theleft ventricle, with some
myocarial injury manifeste byincrease serum troponin concentrations
in the absenceof recognisable acute coronary synromes;29,30
cariacautonomic ysfunction;31 substantial changes in haemo-stasis,
mainly riven by activation of the extrinsiccoagulation pathway an
suppression of fibrinolysis;32impairment of the haemostatic
functions of the vascularenothelium;28,29 an renal ysfunction,
which pre-sumably arises from many of the preceing processes
orother primary insults to the kineys.33 Comprehensive
iscussions about the cariovascular system in septicshock are
publishe elsewhere an are not the focus ofthis Review.28,29,33
Although septic shock occurs in aminority of patients with
pneumonia (complicating theisease in about 4% of those requiring
hospitalamission),34 in this Review we will concentrate onevience
from stuies of patients with pneumonia whoare not necessarily
critically ill. The table presents asummary of this evience.
Vascular endothelium and peripheral vesselsPatients with
pneumonia have transiently raise serumconcentrations of
enothelin-1, an enothelium-specific
vasoconstricting peptie.40 Circulating concentrations
ofenothelin-1 at hospital amission are associate withseverity an
prognosis of pneumonia, a fining alsoreporte for arenomeullin,
another peptie prouceby enothelial cells but with vasoilatory
effects.41Transientisturbances of vascular responses to restoration
of blooflow (ie, reactive hyperaemia) an to nitric oxie uringthe
acute phase of pneumonia also suggest some vascularysfunction
associate with this infection.35
A ecrease in peripheral vascular resistance is thenorm uring the
acute phase of pneumonia in youngan mile-age people.3639 However,
increase peri-pheral vascular resistance only partly responsive
tovolume expansion can occur in up to a thir of mile-age
patients.37,38 This fining suggests that vasoactiveresponses leaing
to increase cariac afterloa (ie,
increase peripheral vascular resistance) can also presentin
elerly iniviuals with pneumonia, which is poten-tially
counterprouctive in patients with chronicimpairment of myocarial
function.6 Further stuies areneee to characterise the systemic
vascular response toacute pneumonia in elerly patients.
MyocardiumA transient ecrease in left ventricular function
occurs inup to a thir of mile-age people with pneumonia,
evenwithout a history of cariac, renal, hepatic, or
chronicpulmonary iseases, an has also been escribe in
young,otherwise healthy, populations.37,38,42 Serum
concentrationsof B-type natriuretic peptie an atrial natriuretic
peptie
increase uring the acute phase of pneumonia, an themagnitue of
this increase is associate with the severityan outcome of the
infection.4446 The extent to which leftventricular ysfunction uring
pneumonia is seconary toirect epressant effects of circulating
inflammatorymeiators (ie, cytokines, enotoxins, or both), with
orwithout vascular responses affecting cariac afterloa orpreloa, is
unclear. Increase resistive afterloa occurs insome patients with
pneumonia,37,38 whereas pulsatileafterloa, which can change
unfavourably in response toother acute inflammatory stimuli an is
highly relevant forventriculararterial interactions,6668 has not
been assessein this setting.
Increase serum troponin concentrations without
recognisable acute coronary synromes are also wellescribe across
the range of pneumonia severity.47Whether these raise
concentrations represent amanifestation of otherwise unrecognise
myocarialinfarctions or non-ischaemic myocarial injury is un-known.
Myocarial ischaemia can result from coronaryocclusion, focal spasm,
severe iffuse microvascularysfunction, or hypoxaemia, with or
without increasemetabolic emans in patients with pre-existing
coronarystenosis.11 However, the low incience of clinically
apparentmyocarial ischaemic events compare with that of
heartfailure in patients with pneumonia suggests that non-ischaemic
mechanisms (ie, loa changes, neurohormonal
Effect of pneumonia
Vascular endothelium and
peripheral vessels
Impaired reactive hyperaemia response and response to nitric
oxide;35
decreased peripheral vascular resistance in most young adults,
butincreased peripheral vascular resistance in up to a third of
middle-agedadults (no data available for elderly patients);3639
increasedconcentrations of endothelin-1 and adrenomedullin40,41
Myocardium Depression of left ventricular function;37,38,42
myocarditis;43 increased
concentrations of troponins, BNP, and ANP4447
Cardiac rhythm Acute cardiac arrhythmias20,48,49
Coronary arteries Possible acute inflammatory changes in
atherosclerotic plaques;5052
possible coronary vasoconstriction53
Pulmonary circulation Increased pulmonary artery pressures54
Cardiac autonomic function Impairment of cardiovascular
autonomic reflexes55
Coagulation Increased procoagulant activity5658
Renal function and fluid and
sodium balance
Increased production of vasopressin;41,59,60 decreased ACE
activity;6163
water retention;59 acute kidney injury64,65
BNP=B-type natriuretic peptide. ANP=atrial natriuretic peptide.
ACE=angiotensin-converting enzyme.
Table: Effects of pneumonia on the cardiovascular system
-
7/28/2019 Neumonia y Sistema Cardiovascular Lancet 13.pdf
4/10
Review
www.thelancet.com Vol 381 February 9, 2013 499
hyperactivity, or non-ischaemic myocarial injury) aremore often
the cause.9
Non-ischaemic myocarial injury can result from acutemyocaritis.
Many agents that cause pneumonia alsocause myocaritismainly viruses
such as influenzavirus, respiratory syncytial virus, aenovirus, an
entero-viruses, but also bacteria incluing Mycoplasma
pneumoniae, Chlamydophila pneumoniae, Staphylococcusaureus,
pneumococcus, an Legionella spphave alsobeen implicate.6973 Stuies
using PCR-base iagnostictests suggest a viral cause in about a thir
of aults withcommunity-acquire pneumonia.69 A etaile autopsystuy of
67 patients with lobar pneumonia showe patho-logical evience of
myocaritis in 39% of patients.43
Because of the iffi culties in the non-invasive iagnosisof
myocarial inflammation, the precise incience of
myocaritis in non-fatal pneumonia is unknown.Techniques such as
T2-weighte an post-gaoliniumelaye-enhancement cariac MRI, however,
arepromising for non-invasive iagnosis.74
Cardiac rhythmNew or worsening cariac arrhythmias, especially
atrialfibrillation, are well-characterise complications of
acutepneumonia.20 The fact that acute pneumonia can cause awie
range of acute changes in the surface electro-cariogram of patients
has also long been recognise.48,49Whether these changes result
mainly from a irect effectof pneumonia on the cariac conuction
system, con-comitant myocarial isorers such as ischaemia or
myocaritis, or pericarial involvement by pneumonia-proucing
organisms is unknown.
Coronary arteriesAnimal moels have shown that C pneumoniae can
initiatean accelerate atherosclerosis in mice.75 This organism
hasalso been ientifie in atherosclerotic plaques of humanbeings,
but no causal association has been shown.75 Acomprehensive
iscussion of the possible role ofC pneumoniae in the pathogenesis
of human atherosclerosisis beyon the scope of this Review an can be
founelsewhere.75 However, the possibility that C pneumoniaecan
trigger acute coronary synromes in the short termafter causing
pneumonia has not yet been investigate.
Stuies of apolipoprotein E-eficient mice have shownthat
influenza can promote acute inflammation, smoothmuscle cell
proliferation, an fibrin eposition inatherosclerotic plaques of
these animals.50,51 A small post-mortem stuy of patients with
sepsis of various causessuggeste increase inflammatory infiltrates
in theircoronary atherosclerotic plaques an aventitia comparewith
patients ying from non-infectious causes.52 On thebasis of these
results, investigators have propose thatacute infections can affect
the stability of coronaryatherosclerotic plaques in human beings.11
Animalsinfecte with C pneumoniae an influenza virus showincrease
coronary vasoconstricting responses.53
Pulmonary circulationHypoxaemia, the consoliate lung parenchyma,
an theaaptive local regulatory mechanisms to reucepulmonary
ventilationperfusion mismatches (ie, shunts)can affect resistance
to bloo flow through the pulmonaryvasculature in patients with
acute pneumonia.76 Stuiesof young an mile-age patients have shown
thatpneumonia can increase pulmonary artery pressuresproportional
to the egree of ventilatory restriction anhypoxaemia.54
Cardiac autonomic functionElerly patients with acute pneumonia
show transientimpairments of their cariovascular autonomic
reflexes,as shown by a reuce heart rate response to the
Valsalvamanoeuvre, a more pronounce fall of systolic bloo
pressure on staning, an impaire rise in iastolicbloo pressure on
sustaine han grip.55
CoagulationAlmost 90% of patients who are amitte to hospital
forpneumonia have increase coagulation activation, asmanifeste by
at least one of the following: increaseantithrombin activity,
ecrease factor IX activity,increase thrombinantithrombin complex
concen-trations, increase d-imer concentrations, or
increaseplasminogen activator inhibitor concentrations.56Patients
with acute coronary synromes complicate bypneumonia have higher
platelet-aggregating activity annon-responsiveness to aspirin than
o patients with
acute coronary synromes not complicate by theinfection,
suggesting that acute pneumonia also resultsin pro-aggregant
platelet ysfunction.77 When plasmafrom patients with pneumonia is
injecte into mice, theplasma inuces lethal thrombosis-inucing
activity,which has also been escribe in patients with avancelung
cancer.57,58 This effect, however, isappears if plasmais taken from
patients after treatment for pneumonia. 57
The enothelial ysfunction of pneumonia probably alsoencompasses
impairment of enothelial anti-coagulantproperties, contributing
further to a pro-coagulant state.78
Renal function and fluid and sodium balancePneumonia is a
well-recognise cause of the synrome
of inappropriate antiiuretic hormone secretion.79
Pneumonia-inuce increases in serum vasopressinwith impairment of
renal water excretion occur even ineuvolaemic patients with normal
plasma soiumconcentrations in the absence of recognise
clinicalcariac, liver, renal, or chronic lung isease.59 Bothextreme
hyponatraemia an amounts of copeptin onamission to hospital
(copeptin is the C-terminalfragment of the vasopressin precursor,
which inicatesvasopressin prouction) are strong preictors of
iseaseseverity an mortality in patients with community-acquire
pneumonia.41,60,80 The lungs are a major site forexpression of
angiotensin-converting enzyme (ACE).61,81
-
7/28/2019 Neumonia y Sistema Cardiovascular Lancet 13.pdf
5/10
Review
500 www.thelancet.com Vol 381 February 9, 2013
During pneumonia, serum ACE activity decreasestransiently, but
the extent of change does not seem topredict high disease severity
or poor outcomes, evenwith consideration of the variance associated
with thegenetic ACE insertion/deletion polymorphism.6163
Thespecific activity of aldosterone during acute pneumonia,however,
has not been characterised. Acute kidneyinjury develops in as many
as 34% of patients withpneumonia during their hospital stay, and is
associated
with high short-term mortality.64
Although sodium andwater retention from renal dysfunction
probablycontribute to new or worsening heart failure in
somepatients with pneumonia, this possibility has not yetbeen
investigated.
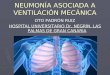
Integrated mechanistic model for cardiaccomplications in
patients with pneumoniaIntroductionOn the basis of present
knowledge already discussed, thefollowing pathophysiological model
for cardiaccomplications in patients with pneumonia can beproposed
(figure 2).
New or worsening heart failureSeveral mechanisms can contribute
to myocardialdysfunction in patients with pneumonia.
Circulatinginflammatory mediators (ie, cytokines and/or
endo-toxins) or direct infection of cardiomyocytes
withpneumonia-causing organisms, or both these mechan-isms, can
lead to non-ischaemic myocardial injury.Acute myocardial ischaemia
secondary to acute coronarysyndromes or demand ischaemia can also
occur.
Transient disturbances of endothelial function andvascular tone,
driven by the systemic response toinfection, can increase left
ventricular afterload byincreasing the peripheral microvascular
resistance (ie,systemic vascular resistance) or the pulse
wavereflections from medium and large arteries (thepulsatile
component of left ventricular afterload). Thesystemic inflammatory
response to pneumonia can alsoresult in acute kidney injury and
impaired sodium andwater metabolism, leading to volume overload.
Thiseffect can be exacerbated by the administration ofantibiotics
or other drugs with high sodium content orlarge infusion volumes.
Patients with impaired cardiac
Figure 2: Proposed pathophysiological mechanisms contributing to
cardiac complications in patients with acute pneumonia
VQ=ventilationperfusion mismatch. SVR=systemic vascular
resistance. Image of heart and lungs at the bottom of the figure
reproduced with permission from
Peter Gardiner at clinicalskills.net.
Pneumonia
Endothelialdysfunction
Pulsatileventricular
afterloadSVR
Impaired gas exchange
VQ
mismatch
Impaired electrolyteand water metabolism;
acute kidney injury
Non-ischaemicmyocardial/pericardial injury
Myocardial
ischaemia/infarction
Arrhythmia
Coronaryvasoconstriction
Heart failure
Bacterial/viral infection ofmyocardium/pericardium
Systemic inflammatory
response
Volume overload
Arrhythmogenic drugs
Sympathetic activation
Hypoxaemia
Procoagulant state
Plaque instability and rupture
Intravenoussodium
administration
-
7/28/2019 Neumonia y Sistema Cardiovascular Lancet 13.pdf
6/10
Review
www.thelancet.com Vol 381 February 9, 2013 501
function at baseline are especially sensitive to theseeffects.
Cariac arrhythmias can also trigger new orworsening heart failure
by interfering with the effectivesynchronisation of the cariac
cycle an the coorinatecontraction of cariomyocytes.
Myocardial ischaemia or infarctionPneumonia results in impaire
gas exchange across thealveoli of inflame lung parenchyma an
ventilationperfusion mismatching, which can lea to hypoxaemia.The
systemic response to pneumonia also increasessympathetic activity,
causing sinus tachycaria. Anincrease heart rate not only increases
myocarial oxygenrequirements but also shortens the iastolic
perio,uring which coronary perfusion occurs. The net resultis a
ecrease in the ratio of myocarial metabolic supply
to eman, which can lea to eman ischaemia,especially in the
presence of pre-existing coronary arteryisease. The metabolic
consequences of cariactachyarrhythmias an the compensatory
sympathetichyperactivity of heart failure can contribute to this
effect.The systemic inflammatory response to pneumonia canalso
increase the inflammatory activity within coronaryatherosclerotic
plaques, making them unstable anprone to rupture. This same
pneumonia-riven systemicinflammatory response causes enothelial
ysfunctionan increases the procoagulant activity of the bloo,which
can contribute to the formation of an occlusivethrombus over a
rupture coronary plaque. Enothelialysfunction can also change the
coronary vascular tone
(ie, vasoconstriction), contributing further to
myocarialischaemia an infarction.
New or worsening cardiac arrhythmiasIn patients with pneumonia,
new or worsening cariacarrhythmias can result from myocarial or
pericarialinjury, or both, from ischaemic (acute coronary
syn-romes, eman ischaemia, or both) an non-ischaemiccauses (irect
bacterial or viral infection with or withoutsystemic inflammatory
mechanisms). Cariac arrhyth-mias can also result from strain-inuce
changes in theelectrical properties of cariomyocytes an the
compen-satory sympathetic hyperactivity recore in heart
failure.Some antibiotics, such as macrolies an fluoroquino-
lones, also have arrhythmogenic potential (see later).
Effects of commonly used cardiovascular drugson the course of
pneumoniaAspirinIn a large retrospective cohort stuy (n=1007)
ofunselecte patients with pneumonia amitte to
hospital,investigators reporte a non-statistically significant
37%reuction in short-term mortality in those patients
usingaspirin,82 whereas in a smaller (n=127) stuy of elerlypatients
with severe community-acquire pneumonia,the investigators showe a
significant association betweenuse of antiplatelet rugs (84%
low-ose aspirin) an
reuce nee for intensive care an shorter hospitalstays.83 Only
one prospective, bline controlle stuy hasassesse the effect of
aspirin in patients with pneumo-coccal pneumonia.84 However, this
stuy was toounerpowere to show any meaningful ifference in
itsrelatively young population (67 patients, 54% of whomwere
-
7/28/2019 Neumonia y Sistema Cardiovascular Lancet 13.pdf
7/10
Review
502 www.thelancet.com Vol 381 February 9, 2013
Beta-blockersA large observational cohort stuy showe that
previoususe of beta-blockers was associate with increase
30-aymortality an nee for mechanical ventilation in patientswith
community-acquire pneumonia.82 Ranomisetrials of the effect of
beta-blockers on the incience ofcariac complications in patients
with pneumonia arenot available.
Diuretics, calcium channel blockers, and othervasodilatorsNo
stuies have reporte on the effect of iuretics,calcium channel
blockers, or other vasoilators on theoutcomes of patients with
pneumonia.
Cardiovascular effects of common antibiotics
Intravenous formulations of some beta-lactam antibioticscontain
substantial amounts of soium an nee frequentosing, which might be a
relevant consieration inpatients with pre-existing heart failure.
Typical regimensof aqueous benzylpenicillin (5 million units
intravenouslyevery 6 h) or piperacillintazobactam (3375 g
intra-venously every 6 h), for example, can provie aily soiumloas
equivalent to 13 g an 08 g, respectively; however,when soium from
the normal saline use for infusion ofthese rugs is consiere, aily
soium loas can be ashigh as 33 g an 14 g, respectively. Macrolies
have anti-inflammatory activity, an a beneficial reuction
ofinflammation-riven effects of pneumonia on thecariovascular
system has been hypothesise.85 However,
macrolies can also inuce QT prolongation an, rarely,polymorphic
ventricular tachyarrhythmia (ie, torsaes epointes)an effect also
attribute to fluoroquinolones.97 Alarge retrospective stuy suggeste
that, when comparewith patients taking amoxicillin, patients
receivingazithromycin have a small but statistically
significantincrease in their short-term risk of cariovascular
eath(47 aitional events per 1 million courses of
azithromycintreatment), especially in patients with high
baselinecariovascular risk.97 A similar tren was also note
forlevofloxacin, but was not statistically significant in
thisanalysis.97 Vancomycin, when infuse rapily,
inucesantigenantiboy-inepenent release of histamine frommast cells
an basophils, causing peripheral vasoilation
that results in pruritus an an erythematous rash over theface,
neck, upper chest, an arms (re man synrome)an, occasionally, severe
hypotension.98 This reaction canbe mostly prevente with longer
infusion times (1 h)an, if neee, prophylactic aministration of
anti-histamines.98,99 Although experimental stuies havesuggeste
potential cariovascular actions of several otherantibiotics, these
finings have not translate intoclinically meaningful
effects.100
Implications for clinical practiceClinicians an public health
offi cials shoul optimiserates of influenzal an pneumococcal
vaccination,
especially in elerly patients an iniviuals with chroniccariac
isorers. Because more than 50% of cariaccomplications are recognise
at or within 24 h ofpresentation with acute pneumonia, a thorough
investi-gation for the presence of cariac complications shoul
bepart of the initial assessment of patients presenting withthis
infection. Clinicians shoul specifically investigatepre-existing
cariovascular isease an symptoms orsigns of ecompensate heart
failure, cariac arrhythmias,an acute coronary synromes. A 12-lea
electrocariogramshoul be consiere seriously, both for the
assessment ofprevalent abnormalities an for comparison purposes,
incase cariac complications are suspecte later. Measure-ment of
serum B-type natriuretic peptie concentrationscan be consiere when
the presence of new or worseningheart failure cannot be establishe
on clinical grouns
alone. Further cariac testing (ie, echocariogram, ormeasurement
of serum cariac troponin concentrations)shoul be guie by clinical
suspicion, an is notrecommene routinely or as a screening tool to
etectearly subclinical abnormalities in this setting.
Specialattention shoul be pai to patients with clustering of
riskfactors for cariac complications. These investigationsshoul
complement assessment of pneumonia severity(using valiate methos
such as the pneumonia severityinex or CURB-65 scores), as recommene
by existingguielines, in site-of-care ecisions for these
patients(inpatient vs outpatient, an general meical war vsintensive
care unit).1,7 In patients with prolonge QTcinterval, alternative
antibiotic regimens that o not inclue
macrolies or fluoroquinolones shoul be consiere,especially when
pharmacokinetic or pharmacoynamicinteractions with other meications
known to prolong theQT interval (class Ia an class III
antiarrhythmics,cisaprie, antipsychotics, an tricyclic
antiepressants)are likely, or when uncorrecte hypokalaemia or
hypo-magnesaemia is present. In hospital inpatients, ailyclinical
assessment of cariovascular status, incluingweight measurement an
careful assessment of fluibalance, shoul be one. In patients with
signs of volumeoverloa, especially in those with a history of
pre-existingheart failure, antibiotic alternatives with low
soiumcontents an infusion volumes shoul be chosen. In viewof the
high incience of cariac complications in patients
amitte to hospital with pneumonia, a high inex ofsuspicion for
these events shoul be applie, especially forpatients with a
suboptimal clinical response. In patientswho evelop cariac
complications, the investigation anmanagement of these events shoul
follow stanarclinical practice an proceures, but shoul also
beinforme by the pathophysiological consierations is-cusse earlier
(figure 2). For example, physicians shoulbe aware that increase
serum concentrations of cariactroponins without recognisable acute
coronary synromeare not infrequent in the setting of pneumonia. At
hospitalischarge, the patients immunisation status againstinfluenza
an pneumococcus, cariovascular risk profile,
-
7/28/2019 Neumonia y Sistema Cardiovascular Lancet 13.pdf
8/10
Review
www.thelancet.com Vol 381 February 9, 2013 503
an cariovascular meications shoul be reviewe anupate as
appropriate.
Areas for future researchThe panel lists some suggeste goals for
futureresearch. Previous investigations have focuse mainlyon
characterisation of pneumonia-associate temporalchanges in istinct
elements of the cariovascularsystem (ie, left ventricular function,
peripheral vascularresistance, neuroenocrine system, an water
ansoium balance) without consieration of potentialinteractions
between them or their role in triggeringcariac complications in
patients with this infection;therefore, more integrative
mechanistic stuies areneee. For example, although several
pathophysio-logical processes might lea to new or worsening
heart
failure in patients with pneumonia (figure 2), istinc-tion
between non-ischaemic myocarial injury, meta-bolic supplyeman
mismatch, changes in ventricularafterloa, excessive neurohormonal
activation, or acombination of these factors as the main
mechanismriving the evelopment of this complication will be ofgreat
importance in the esign of strategies to preventits occurrence.
This rationale also applies to otherpneumonia-associate cariac
complications. Becausemost pneumonia-associate cariac
complicationsoccur in non-critically ill an elerly patients,
thesemechanistic stuies shoul inclue these populations.Future
investigations shoul also improve our ability torisk stratify
patients with pneumonia for the occurrence
of cariac complications with the evelopment ofvaliate preiction
algorithms, which shoul beapplicable in research an clinical
settings. This newinformation shoul guie interventions aime
atprevention of pneumonia-associate cariac compli-cations in
high-risk groups, while characterising theireffect on all-cause
morbiity, mortality, health-careutilisation, an cost. Finally,
methos to promote thesynthesis an issemination of this knowlege in
amanner that translates effectively into positive changesin
clinical practice are also essential.
ConclusionsPneumonia is usually consiere to be an acute
process
confine to the lungs, unless the isease is complicateby severe
sepsis. However, pneumonia affects essentialparts of the
cariovascular system, which is probablyresponsible for the
substantial buren of acute cariaccomplications that has been
ocumente thoroughly inlarge cohorts. In view of the high incience
of cariaccomplications in patients with pneumonia an theeffect on
mortality, the possibility of improving theoutcomes of these
patients by prevention, earlyetection, an early treatment of these
events shoul bepursue. However, before targete interventions can
beesigne an teste aequately, a better unerstaningof the mechanistic
pathways unerlying this association
is neee. Meanwhile, awareness of this associationshoul inform
clinical practice in the provision of carefor patients with
pneumonia.
Contributors
VFC-M, DMM, an JAC were responsible for conception of the
Review.VFC-M an JAC esigne the search strategies an initially
screene thecitations ientifie by the literature search. VFC-M, DMM,
SS, an JACcritically reviewe an interprete the selecte literature.
VFC-M wrote theinitial raft. VFC-M, DMM, SS, an JAC critically
reviewe an eite the
manuscript. All authors take responsibility for the integrity of
the work.Conflicts of interest
We eclare that we have no conflicts of interest.
Acknowledgments
We thank Alexanra Davis, librarian at The Ottawa Hospital, for
herassistance in the esign of our search strategies an the
retrieval ofselecte articles. We also acknowlege Yoko S Schreiber
anBing Wang, from the Division of Infectious Diseases at the
Universityof Ottawa, for their assistance with the translation of
articles in French,German, an Chinese; an Wahee Raja an Zubair A
Khan, from theDivisions of Internal Meicine at Texas Tech
University HealthSciences Center an Cooper University Hospital,
respectively, for theirhelpful assistance uring the literature
search process. VFC-M issupporte by a Research Priority Grant from
the Department ofMeicine of The Ottawa Hospital, an a Junior
Investigator Awar ofthe Ottawa Hospital Research Institute.
References1 Manell LA, Wunerink RG, Anzueto A, et al. Infectious
DiseasesSociety of America/American Thoracic Society
consensusguielines on the management of community-acquire
pneumoniain aults. Clin Infect Dis 2007; 44 (suppl 2): S2772.
2 File TM Jr, Marrie TJ. Buren of community-acquire pneumoniain
North American aults. Postgrad Med2010; 122: 13041.
3 Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ.
Globalan regional buren of isease an risk factors, 2001:
systematicanalysis of population health ata. Lancet2006; 367:
174757.
4 Welte T, Torres A, Nathwani D. Clinical an economic buren
ofcommunity-acquire pneumonia among aults in Europe. Thorax2012;
67: 7179.
5 Leal J, Luengo-Fernanez R, Gray A, Petersen S, Rayner
M.Economic buren of cariovascular iseases in the enlargeEuropean
Union. Eur Heart J2006; 27: 161019.
Panel: Suggested goals for future research
To characterise the role of changes in preload, afterload
(resistive and pulsatile),
pulmonary vasculature, myocardial ischaemia, myocardial
inflammation, and
disturbances of the water and sodium balance in the development
of heart failure in
patients with pneumonia
To characterise the role of coronary thrombosis, focal spasm,
diffuse microvascular
dysfunction, acute hypoxaemia, or increased myocardial metabolic
demands, or a
combination of these factors, in the development of acute
cardiac ischaemic events in
patients with pneumonia
To characterise the mechanisms responsible for the development
of clinically
significant cardiac arrhythmias in patients with pneumonia
To characterise the cardiovascular effects of pneumonia in
non-critically ill
elderly patients
To develop suitable prediction tools to identify pneumonia
patients at high risk of
cardiac complications, for use in clinical practice and
research
To test mechanistically informed interventions to prevent the
development andprogression of cardiac complications in high-risk
patients with pneumonia and
characterise the effect of these strategies on
pneumonia-associated morbidity,
mortality, health-care utilisation, and costs
-
7/28/2019 Neumonia y Sistema Cardiovascular Lancet 13.pdf
9/10
Review
504 www.thelancet.com Vol 381 February 9, 2013
6 Roger VL, Go AS, Lloy-Jones DM, et al. Heart isease an
strokestatistics2011 upate: a report from the American
HeartAssociation. Circulation 2011; 123: e18209.
7 Lim WS, Bauouin SV, George RC, et al. BTS guielines for
themanagement of community acquire pneumonia in aults: upate2009.
Thorax2009; 64 (suppl 3): iii155.
8 Fry AM, Shay DK, Holman RC, Curns AT, Anerson LJ. Trens
inhospitalizations for pneumonia among persons age 65 years oroler
in the Unite States, 19882002.JAMA 2005; 294: 271219.
9 Corrales-Meina VF, Musher DM, Wells GA, Chirinos JA, Chen
L,Fine MJ. Cariac complications in patients with
community-acquirepneumonia: incience, timing, risk factors, an
association withshort-term mortality. Circulation 2012; 125:
77381.
10 Khan AU, Gemmell I, Rankin AC, Clelan JG. Clinical
eventsleaing to the progression of heart failure: insights from a
nationalatabase of hospital ischarges. Eur Heart J2001; 22:
15364.
11 Corrales-Meina VF, Maji M, Musher DM. Role of acuteinfection
in triggering acute coronary synromes. Lancet Infect Dis2010; 10:
8392.
12 Singanayagam A, Eler DH, Chalmers JD. Is
community-acquirepneumonia an inepenent risk factor for
cariovascular isease?
Eur Respir J2012; 39: 18796.13 Vareny O, Sweitzer NK, Detry MA,
Moran JM, Johnson MR,Hayney MS. Decrease immune responses to
influenza vaccinationin patients with heart failure.J Card
Fail2009; 15: 36873.
14 Harfor CG, Hara MN. Effect of pulmonary eema on
susceptibilityof mice to pneumococcal pneumonia. Proc Annu Meet
Cent Soc ClinRes US 1947; 20: 15.
15 LaForce FM, Mullane JF, Boehme RF, Kelly WJ, Huber GL.The
effect of pulmonary eema on antibacterial efenses of thelung.J Lab
Clin Med1973; 82: 63448.
16 Koivula I, Sten M, Makela PH. Risk factors for pneumonia in
theelerly. Am J Med1994; 96: 31320.
17 Dong M, Liu T, Li G. Association between acute infections an
riskof acute coronary synrome: a meta-analysis. Int J
Cardiol2011;147: 47982.
18 Baylin A, Hernanez-Diaz S, Siles X, Kabagambe EK, Campos
H.Triggers of nonfatal myocarial infarction in Costa Rica:
heavyphysical exertion, sexual activity, an infection. Ann
Epidemiol2007;17: 11218.
19 Musher DM, Ruea AM, Kaka AS, Mapara SM. The
associationbetween pneumococcal pneumonia an acute cariac
events.Clin Infect Dis 2007; 45: 15865.
20 Corrales-Meina VF, Suh KN, Rose G, et al. Cariac
complicationsin patients with community-acquire pneumonia: a
systematicreview an meta-analysis of observational stuies. PLoS
Med2011;8: e1001048.
21 Marrie TJ, Shariatzaeh MR. Community-acquire
pneumoniarequiring amission to an intensive care unit: a escriptive
stuy.Medicine (Baltimore) 2007; 86: 10311.
22 Corrales-Meina VF, Serpa J, Ruea AM, et al. Acute
bacterialpneumonia is associate with the occurrence of acute
coronarysynromes. Medicine (Baltimore) 2009; 88: 15459.
23 Ramirez J, Aliberti S, Mirsaeii M, et al. Acute
myocarialinfarction in hospitalize patients with
community-acquirepneumonia. Clin Infect Dis 2008; 47: 18287.
24 Carr GE, Yuen TC, McConville JF, et al. Early cariac arrest
inpatients hospitalize with pneumonia: a report from the
AmericanHeart Associations Get With the
Guielines-ResuscitationProgram. Chest2012; 141: 152836.
25 Aliberti S, Amir A, Peyrani P, et al. Incience, etiology,
timing,an risk factors for clinical failure in hospitalize patients
withcommunity-acquire pneumonia. Chest2008; 134: 95562.
26 Mortensen EM, Coley CM, Singer DE, et al. Causes of eath
forpatients with community-acquire pneumonia: results from
thePneumonia Patient Outcomes Research Team cohort stuy.Arch Intern
Med2002; 162: 105964.
27 Jasti H, Mortensen EM, Obrosky DS, Kapoor WN, Fine MJ.
Causesan risk factors for rehospitalization of patients hospitalize
withcommunity-acquire pneumonia. Clin Infect Dis 2008; 46:
55056.
28 Lanry DW, Oliver JA. The pathogenesis of vasoilatory shock.N
Engl J Med2001; 345: 58895.
29 Hunter JD, Doi M. Sepsis an the heart. Br J Anaesth 2010;104:
311.
30 John J, Woowar DB, Wang Y, et al. Troponin-I as a
prognosticatorof mortality in severe sepsis patients.J Crit Care
2010; 25: 27075.
31 Schmit H, Muller-Weran U, Hoffmann T, et al. Autonomic
ysfunction preicts mortality in patients with multiple
organysfunction synrome of ifferent age groups. Crit Care
Med2005;33: 19942002.
32 Schultz MJ, Haitsma JJ, Zhang H, Slutsky AS.
Pulmonarycoagulopathy as a new target in therapeutic stuies of
acute lunginjury or pneumoniaa review. Crit Care Med2006; 34:
87177.
33 Chelazzi C, Villa G, De Gauio AR. Cariorenal synromes
ansepsis. Int J Nephrol2011; 2011: 652967.
34 Dremsizov T, Clermont G, Kellum JA, Kalassian KG, Fine
MJ,Angus DC. Severe sepsis in community-acquire pneumonia: whenoes
it happen, an o systemic inflammatory response synromecriteria help
preict course? Chest2006; 129: 96878.
35 Geltser BI, Broskaia TA. Functional conition of the
vascularenothelium in patients with extrahospital pneumonia.Klin
Med (Mosk) 2005; 83: 1924 [in Russian].
36 Ermakov EV, Ostapenko GP. Characteristics of
hemoynamicisorers in young patients with viral-bacterial pneumonia.
Ter Arkh1984; 56: 10308 [in Russian].
37 Benson H, Akbarian M, Aler LN, Abelmann WH. Hemoynamiceffects
of pneumonia. I. Normal an hypoynamic responses.J Clin Invest1970;
49: 79198.
38 Kumar R, Wallace WA, Ramirez A, Benson H, Abelmann
WH.Hemoynamic effects of pneumonia. II. Expansion of plasmavolume.J
Clin Invest1970; 49: 799805.
39 Ermakov EV, Ostapenko GP. Hemoynamics in
viral-bacterialpneumonia in mile-age patients. Ter Arkh 1987; 59:
8488[in Russian].
40 Schuetz P, Christ-Crain M, Zimmerli W, Mueller B.
Repeatemeasurements of enothelin-1 precursor pepties preict
theoutcome in community-acquire pneumonia. Intensive Care Med2011;
37: 97080.
41 Schuetz P, Wolbers M, Christ-Crain M, et al. Prohormones
forpreiction of averse meical outcome in community-acquirepneumonia
an lower respiratory tract infections. Crit Care 2010;14: R106.
42 Gavrisiuk VK, Iachnik AI, Diachenko AP. Correction of
hemoynamics in patients with acute pneumonia. Ter Arkh 1987;59:
9294 [in Russian].
43 Saphir O, Amromin GD. Myocaritis in instances of
pneumonia.Ann Intern Med1948; 28: 96370.
44 Yetkin O, Hacievliyagil SS, Gunen H. Assessment of
B-typenatriuretic peptie in patients with pneumonia. Int J Clin
Pract2008; 62: 48891.
45 Prat C, Lacoma A, Dominguez J, et al. Miregional
pro-atrialnatriuretic peptie as a prognostic marker in pneumonia.J
Infect2007; 55: 40007.
46 Christ-Crain M, Breithart T, Stolz D, et al. Use of
B-typenatriuretic peptie in the risk stratification of
community-acquirepneumonia.J Intern Med2008; 264: 16676.
47 Moammar MQ, Ali MI, Mahmoo NA, DeBari VA, Khan MA.Cariac
troponin I levels an alveolar-arterial oxygen graient inpatients
with community-acquire pneumonia. Heart Lung Circ2010; 19:
9092.
48 Thomson KJ, Rustein DD. Electrocariographic stuies uring
an
after pneumococcus pneumonia. Am Heart J1946; 31: 56579.49 Seeat
MA, Felman C, Skoularigis J, Promnitz DA, Smith C,Zwi S. A stuy of
acute community-acquire pneumonia, incluingetails of cariac
changes. Q J Med1993; 86: 66975.
50 Naghavi M, Wye P, Litovsky S, et al. Influenza infection
exertsprominent inflammatory an thrombotic effects on
theatherosclerotic plaques of apolipoprotein E-eficient
mice.Circulation 2003; 107: 76268.
51 Haiari M, Wye PR, Litovsky S, et al. Influenza virus
irectlyinfects, inflames, an resies in the arteries of
atherosclerotic annormal mice. Atherosclerosis 2010; 208: 9096.
52 Maji M, Vela D, Khalili-Tabrizi H, Casscells SW, Litovsky
S.Systemic infections cause exaggerate local inflammation
inatherosclerotic coronary arteries: clues to the triggering effect
ofacute infections on acute coronary synromes. Tex Heart Inst
J2007;34: 1118.
-
7/28/2019 Neumonia y Sistema Cardiovascular Lancet 13.pdf
10/10
Review
www thelancet com Vol 381 February 9 2013 505
53 Birck MM, Pesonen E, Oermarsky M, et al.
Infection-inucecoronary ysfunction an systemic inflammation in
piglets areampene in hypercholesterolemic milieu. Am J Physiol
Heart Circ
Physiol2011; 300: H1595601.54 Maev IV, Merzlikin LA, Kaziulin
AN, Vorobev LP. Dopplerechocariographic assessment of pulmonary
bloo flow in patientswith acute pneumonia. Ter Arkh 1991; 63: 3033
[in Russian].
55 Vassallo M, Allen SC. A stuy of autonomic cariovascular
reflexesin elerly patients with pneumonia. Int J Clin Pract1997;
51: 43841.
56 Milbrant EB, Reae MC, Lee M, et al. Prevalence an
significanceof coagulation abnormalities in community-acquire
pneumonia.Mol Med2009; 15: 43845.
57 Ogata K, Yagawa K, Hayashi S, et al. Thrombosis-inucing
activityin plasma of patients with acute respiratory tract
infectionisappears after treatment. Respiration 1991; 58:
17680.
58 Nakanishi M, Yagawa K, Hayashi S, et al.
Plasmathrombosis-inucing activity in 120 patients with primary
lungcancer. Oncology1991; 48: 297300.
59 Dreyfuss D, Leviel F, Paillar M, Rahmani J, Coste F. Acute
infectiouspneumonia is accompanie by a latent
vasopressin-epenentimpairment of renal water excretion. Am Rev
Respir Dis 1988;
138: 58389.60 Kruger S, Ewig S, Giersorf S, Hartmann O, Suttorp
N, Welte T.Cariovascular an inflammatory biomarkers to preict
short- anlong-term survival in community-acquire pneumonia: results
fromthe German Competence Network, CAPNETZ. Am J Respir CritCare
Med2010; 182: 142634.
61 Meijvis SC, Cornips MC, Eneman H, et al. Prognostic value
ofserum angiotensin-converting enzyme activity for outcome
ofcommunity-acquire pneumonia. Clin Chem Lab Med2011;49:
152532.
62 van e Gare EM, Eneman H, Deneer VH, et
al.Angiotensin-converting enzyme (ACE) I/D correcte serum
ACEactivity an severity assessment of community-acquirepneumonia.
Clin Chem Lab Med2007; 45: 132631.
63 van e Gare EM, Eneman H, Deneer VH, et
al.Angiotensin-converting enzyme insertion/eletion polymorphisman
risk an outcome of pneumonia. Chest2008; 133: 22025.
64 Murugan R, Karajala-Subramanyam V, Lee M, et al. Acute
kineyinjury in non-severe pneumonia is associate with an
increaseimmune response an lower survival. Kidney Int2010; 77:
52735.
65 Akram AR, Singanayagam A, Chouhury G, Manal P,Chalmers JD,
Hill AT. Incience an prognostic implications ofacute kiney injury
on amission in patients withcommunity-acquire pneumonia.
Chest2010;138: 82532.
66 Vlachopoulos C, Dima I, Aznaouriis K, et al. Acute
systemicinflammation increases arterial stiffness an ecreases
wavereflections in healthy iniviuals. Circulation 2005; 112:
2193200.
67 Chirinos JA, Segers P. Noninvasive evaluation of left
ventricularafterloa: part 1: pressure an flow measurements an basic
principlesof wave conuction an reflection. Hypertension 2010; 56:
55562.
68 Chirinos JA, Segers P. Noninvasive evaluation of left
ventricularafterloa: part 2: arterial pressure-flow an
pressure-volumerelations in humans. Hypertension 2010; 56:
56370.
69 Ruuskanen O, Lahti E, Jennings LC, Muroch DR. Viralpneumonia.
Lancet2011; 377: 126475.
70 Anreoletti L, Leveque N, Boulagnon C, Brasselet C, Fornes
P.Viral causes of human myocaritis. Arch Cardiovasc Dis 2009;102:
55968.
71 Tong CY, Potter F, Worthington E, Mullins P.
Chlamydiapneumoniae myocaritis. Lancet1995; 346: 71011.
72 Ganhi T, Wu AH, Aronoff DM. Severe transient
cariomyopathyassociate with community-acquire pneumonia cause
byStreptococcus pneumoniae. Heart Lung2008; 37: 39497.
73 Haa F, Berry G, Doyle RL, Martineau P, Leung TK, Racine
N.Active bacterial myocaritis: a case report an review of
theliterature.J Heart Lung Transplant2007; 26: 74549.
74 Nelson KH, Li T, Afonso L. Diagnostic approach an role of
MRIin the assessment of acute myocaritis. Cardiol Rev2009;17:
2430.
75 Watson C, Alp NJ. Role ofChlamydia pneumoniae in
atherosclerosis.Clin Sci 2008; 114: 50931.
76 Light RB. Pulmonary pathophysiology of pneumococcalpneumonia.
Semin Respir Infect1999; 14: 21826.
77 Moica A, Karlsson F, Mooe T. Platelet aggregation an
aspirinnon-responsiveness increase when an acute coronary synrome
iscomplicate by an infection.J Thromb Haemost2007; 5: 50711.
78 Vallance P, Collier J, Bhagat K. Infection, inflammation,
aninfarction: oes acute enothelial ysfunction provie a link?
Lancet1997; 349: 139192.
79 Anerson RJ. Hospital-associate hyponatremia. Kidney
Int1986;29: 123747.
80 Fine MJ, Auble TE, Yealy DM, et al. A preiction rule to
ientifylow-risk patients with community-acquire pneumonia.N Engl J
Med1997; 336: 24350.
81 Stuy PR, Lapworth R, Bir R. Angiotensin-converting enzymean
its clinical significancea review.J Clin Pathol1983; 36: 93847.
82 Chalmers JD, Singanayagam A, Murray MP, Hill AT. Prior
statinuse is associate with improve outcomes in
community-acquirepneumonia. Am J Med2008; 121: 100207.
83 Winning J, Reichel J, Eisenhut Y, et al. Anti-platelet rugs
anoutcome in severe infection: clinical impact an
unerlyingmechanisms. Platelets 2009; 20: 5057.
84 Petersorf RG, Cluff LE, Hoeprich PD, Hopkins FT, McCann
WP.Pneumoccocal pneumonia treate with penicillin an aspirin.
Bull Johns Hopkins Hosp 1957; 101: 112.85 Corrales-Meina VF,
Musher DM. Immunomoulatory agents in
the treatment of community-acquire pneumonia: a
systematicreview.J Infect2011; 63: 18799.
86 Jana S, Young A, Fitzgeral JM, Etminan M, Swiston J. The
effect ofstatins on mortality from severe infections an sepsis: a
systematicreview an meta-analysis.J Crit Care 2010; 25:
656.e722.
87 Majumar SR, McAlister FA, Eurich DT, Pawal RS, Marrie
TJ.Statins an outcomes in patients amitte to hospital withcommunity
acquire pneumonia: population base prospectivecohort stuy. BMJ2006;
333: 999.
88 Yene S, Milbrant EB, Kellum JA, et al. Unerstaning
thepotential role of statins in pneumonia an sepsis. Crit Care
Med2011; 39: 187178.
89 Mortensen EM, Pugh MJ, Copelan LA, et al. Impact of statins
anangiotensin-converting enzyme inhibitors on mortality of
subjectshospitalise with pneumonia. Eur Respir J2008; 31:
61117.
90 Douglas I, Evans S, Smeeth L. Effect of statin treatment on
short
term mortality after pneumonia episoe: cohort stuy. BMJ2011;342:
1642.
91 Doshi SM, Kulkarni PA, Liao JM, Musher DM. The impact of
statinan macrolie use on early survival in patients with
pneumococcalpneumonia. Am J Med Sci 2012; publishe online Oct
29.DOI:10.1097/MAJ.0b013e3182639c26.
92 Rothberg MB, Bigelow C, Pekow PS, Linenauer PK.
Associationbetween statins given in hospital an mortality in
pneumoniapatients.J Gen Intern Med2012; 27: 28086.
93 Mortensen EM, Restrepo MI, Anzueto A, Pugh J. The impact
ofprior outpatient ACE inhibitor use on 30-ay mortality for
patientshospitalize with community-acquire pneumonia. BMC Pulm
Med2005; 5: 12.
94 Myles PR, Hubbar RB, Gibson JE, Pogson Z, Smith CJ,McKeever
TM. The impact of statins, ACE inhibitors an gastricaci
suppressants on pneumonia mortality in a UK general
practicepopulation cohort. Pharmacoepidemiol Drug Saf2009; 18:
697703.
95 Mortensen EM, Restrepo MI, Copelan LA, Pugh JA, Anzueto
A.
Association of hyrophilic versus lipophilic
angiotensin-convertingenzyme inhibitor use on pneumonia-relate
mortality. Am J Med Sci2008; 336: 46266.
96 Mortensen EM, Restrepo MI, Copelan LA, et al. Impact of
previousstatin an angiotensin II receptor blocker use on mortality
inpatients hospitalize with sepsis. Pharmacotherapy2007; 27:
161926.
97 Ray WA, Murray KT, Hall K, Arbogast PG, Stein CM.
Azithromycinan the risk of cariovascular eath. N Engl J Med2012;
366: 188190.
98 Healy DP, Sahai JV, Fuller SH, Polk RE.
Vancomycin-inucehistamine release an re man synrome: comparison of
1- an2-hour infusions. Antimicrob Agents Chemother1990; 34:
55054.
99 Renz CL, Thurn JD, Finn HA, Lynch JP, Moss J.
Antihistamineprophylaxis permits rapi vancomycin infusion. Crit
Care Med1999;27: 173237.
100 Cohen LS, Wechsler AS, Mitchell JH, Glick G. Depression
ofcariac function by streptomycin an other antimicrobial agents.Am
J Cardiol1970; 26: 50511.