Embed Size (px)
Citation preview
5/20/2011
1
Presented By:
Joseph S. Ferezy, D.C.
Examination ComponentsI. History and mental status
II. Cranial nerve (special senses)
III Somatic motorIII.Somatic motor
IV.Somatic sensory
V. Reflex
VI.Tone, posture, station and movement
Ferezy’s MSR’SMotor
STV
Strength
Reflex
Deep
Superficial Strength
Tone
Volume
Sensory
Deep
Superficial
Superficial
Visceral
Pathologic
Serebellar
Station
Movement
5/20/2011
2
Basic Exam Organization
Sitting (Chair)History of Present Illness
Observe Mental Status Include Observe Mental Status ‐ Include
Cleanliness
Stream of Talk
Mood
Content of Thought
Intelligence
Sensorium (Cognitive)
Basic Exam Organization
StandingFree, Heel/toe, Tandem W lki /H i /K B dWalking/Hopping/Knee Bend
Romberg
Posture (observe – tremor, asymmetry, atrophy, Etc.)
T & L ROM’s
Basic Exam Organization• Sitting (Exam Table)▫ Cranial Nerve Examination.▫ Motor Tests ‐ Strength, Tone, and Volume ( t th th i l t )(most other then spinal extensors).
▫ Coordination Tests (Drift, Finger To Finger/Nose, Heel to Shin, Rapid Alternating Movements, Etc.).
▫ Intrathecal Tests.▫ Orthopedic Tests (Most).▫ Muscle stretch reflexes.
5/20/2011
3
The Examination of Station, Movement and Gait
Station ‐ The place at which someone is positioned or is assigned to remain, the act or manner of standing.
Gait ‐ a manner of walking or moving on foot.
Station and gait disorders are among the most common Station and gait disorders are among the most common reasons patients seek outpatient neurologic consultation.
A careful assessment of station and gait provides a quick, reliable snapshot of the integrated function of the patient's motor and sensory systems of both the central and peripheral nervous systems.
Often involved in both somatoform (psychogenic) disorders as well as mistaken as psychogenic in etiology.
The Examination of Station, Movement and Gait
A normal examination requires nervous system function at the highest level, integration and performance.
Disorders of motor or sensory systems of the peripheral or central nervous system may affect movement.
Each system will affect movement in a characteristic way.
Because it is a sensitive (but not specific) test, the good clinician will test movement in even a cursory neurologic examination.
Abnormal responses to the integrated testing of station and movement require additional testing to challenge each system independently in order to determine which system is failing and at what level.
The Examination of Station, Movement and Gait
Patient standing
Eyes open
Eyes closed
Broad base
Narrow base
Patient sitting (or standing)
Arms outstretched and supinated
5/20/2011
4
The Examination of Station, Movement and Gait Ask patient to walk
Free walk
Tandem (heel to toe) walk
Heel walkHeel walk
Toe walk
Ask patient to do a shallow to deep knee bend
Ask patient to hop on one foot in place (then the other)
Sit down
Get up from a seated position
Movement Requires extensive pre‐requisite knowledge about multiple motor and sensory systems and how the nervous system integrates function.
Brain is the “Puppet Master”.
C di t d t i i t d Coordinated movement requires sensory input and integration of four so‐called “motor systems”.
Superimposed on tone and posture
Tone and posture change instantly with superimposed movement.
Creates a sensory‐motor‐sensory‐motor continuous loop
Motor Systems ‐ Clinical Classifications Pyramidal (AKA: cotricospinal, UMN, Betz cell, long tracts) – direct influence on lower motor neurons involved in willfully directed muscular contractions.
Extrapyramidal – tone, posture, gait and other “pre‐programmed” movements. Modulates pyramidal system, does not travel in the pyramids.
Cerebellar – Balance, tone and fine coordination of willfully directed muscular contractions.
Reflex arc – (AKA: LMN, final common pathway) to target muscle.
ALL motor systems are useless unless they can affect the muscle.
5/20/2011
5
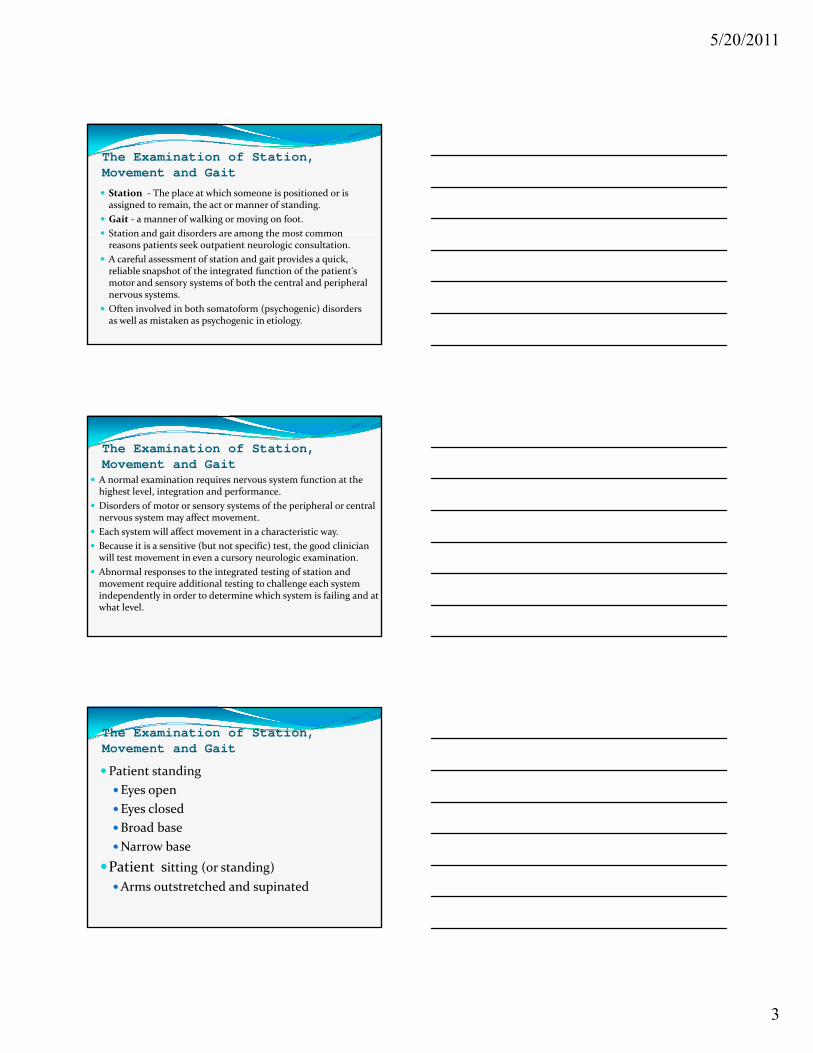
Basic clinical concepts of pyramidal system innervation Covered in “Examination of the Somatic Motor System”.
Voluntary movements are di t d th h th t mediated through the motor
cortex (UMN).
Each area of this cortex controls an area of the face and body
Extrapyramidal and cerebellar systems are also involved.
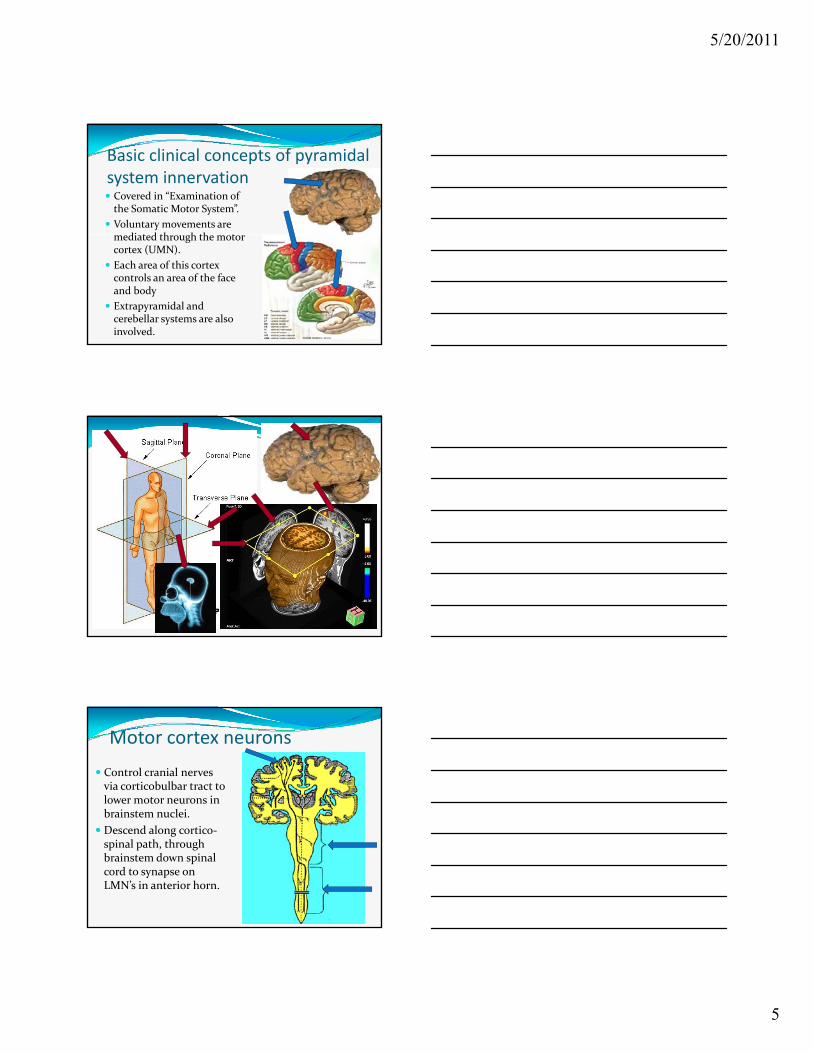
Motor cortex neurons
Control cranial nerves via corticobulbar tract to lower motor neurons in brainstem nuclei.
Descend along cortico‐spinal path, through brainstem down spinal cord to synapse on LMN’s in anterior horn.
5/20/2011
6
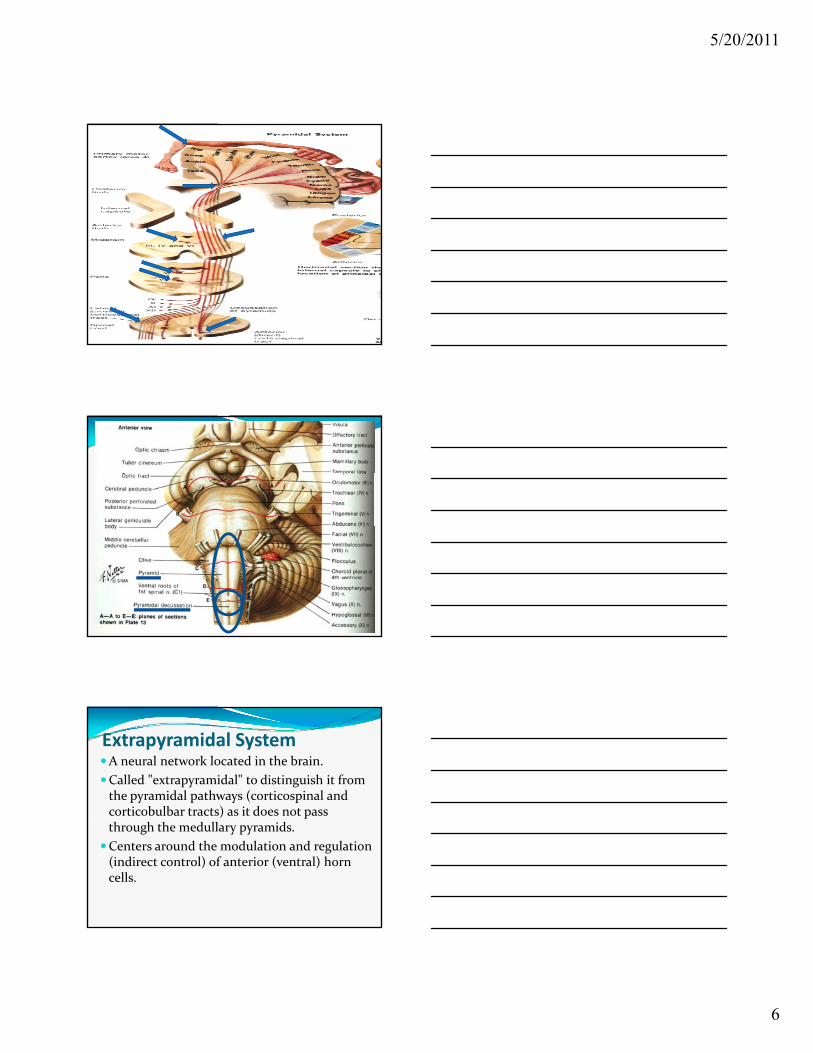
Extrapyramidal SystemA neural network located in the brain.
Called "extrapyramidal" to distinguish it from the pyramidal pathways (corticospinal and corticobulbar tracts) as it does not pass ) pthrough the medullary pyramids.
Centers around the modulation and regulation (indirect control) of anterior (ventral) horn cells.
5/20/2011
7
Extrapyramidal System Extrapyramidal tracts are chiefly found in the reticular formation of the pons and medulla, and target neurons in the spinal cord involved in reflexes, locomotion, complex movements, and postural control.
Deeply interconnected to and modulated by the Deeply interconnected to and modulated by the nigrostriatal pathway, the basal ganglia, the cerebellum, the vestibular nuclei, and different sensory areas of the cerebral cortex.
All of these regulatory components can be considered part of the extrapyramidal system, in that they modulate motor activity but we tend to discuss sensory and cerebellar areas separately.
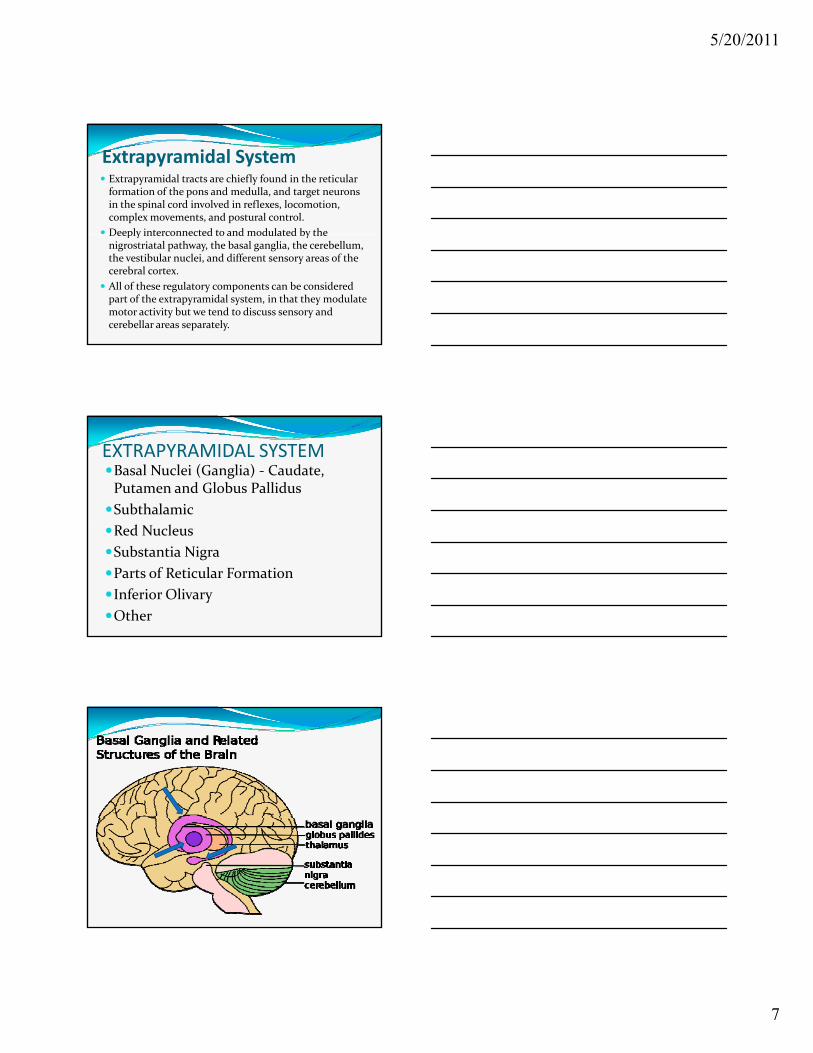
EXTRAPYRAMIDAL SYSTEMBasal Nuclei (Ganglia) ‐ Caudate, Putamen and Globus Pallidus
Subthalamic
R d N lRed Nucleus
Substantia Nigra
Parts of Reticular Formation
Inferior Olivary
Other
5/20/2011
8
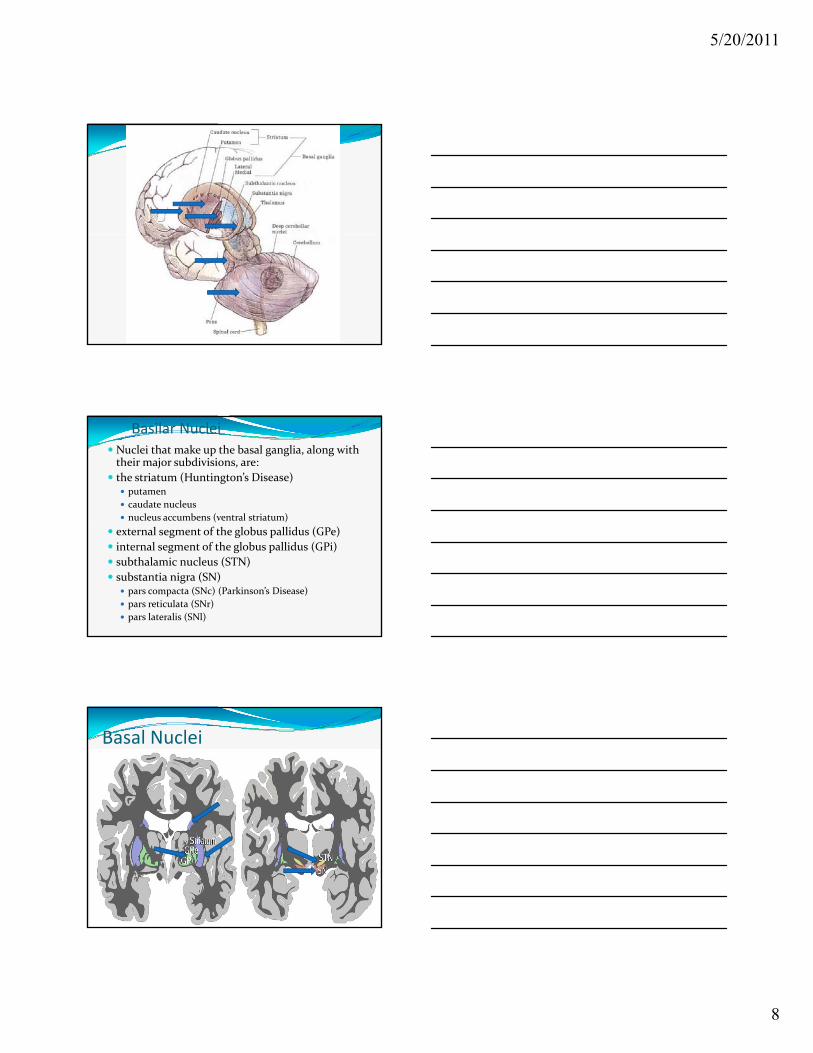
Basilar Nuclei Nuclei that make up the basal ganglia, along with their major subdivisions, are:
the striatum (Huntington’s Disease) putamen
caudate nucleus
nucleus accumbens (ventral striatum)
external segment of the globus pallidus (GPe)
internal segment of the globus pallidus (GPi)
subthalamic nucleus (STN)
substantia nigra (SN) pars compacta (SNc) (Parkinson’s Disease)
pars reticulata (SNr)
pars lateralis (SNl)
Basal Nuclei
5/20/2011
9
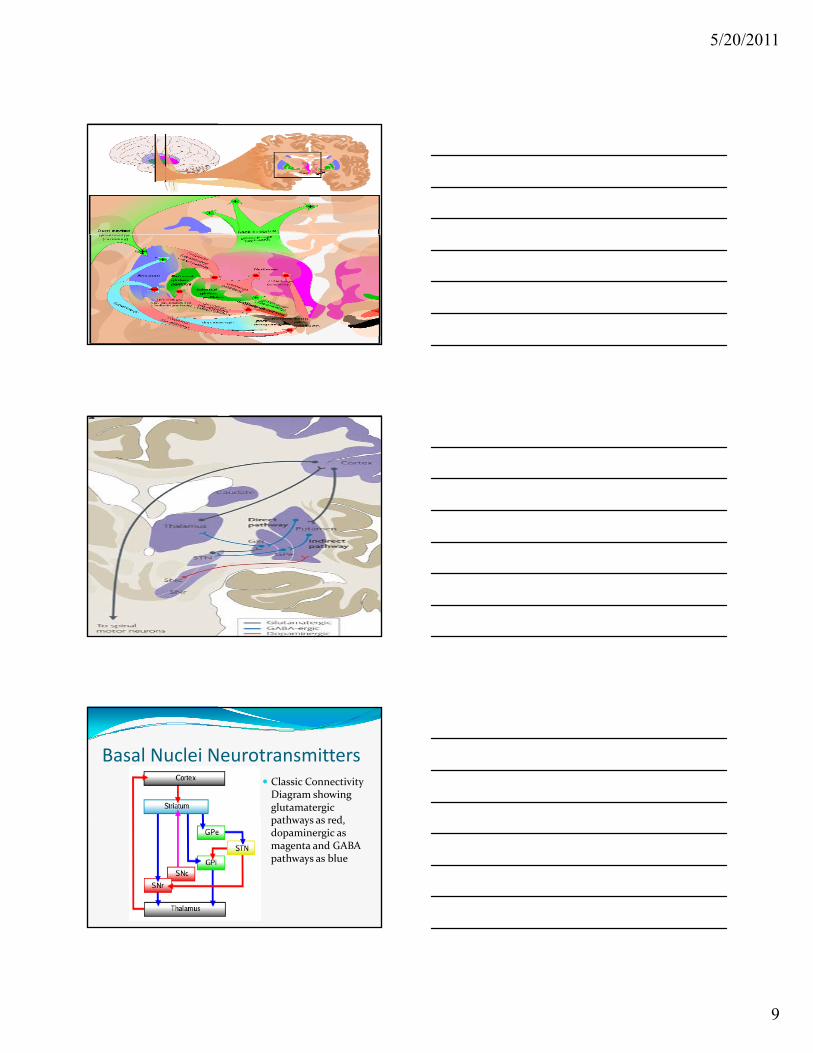
Basal Nuclei Neurotransmitters Classic Connectivity Diagram showing glutamatergic
th d pathways as red, dopaminergic as magenta and GABA pathways as blue
5/20/2011
10
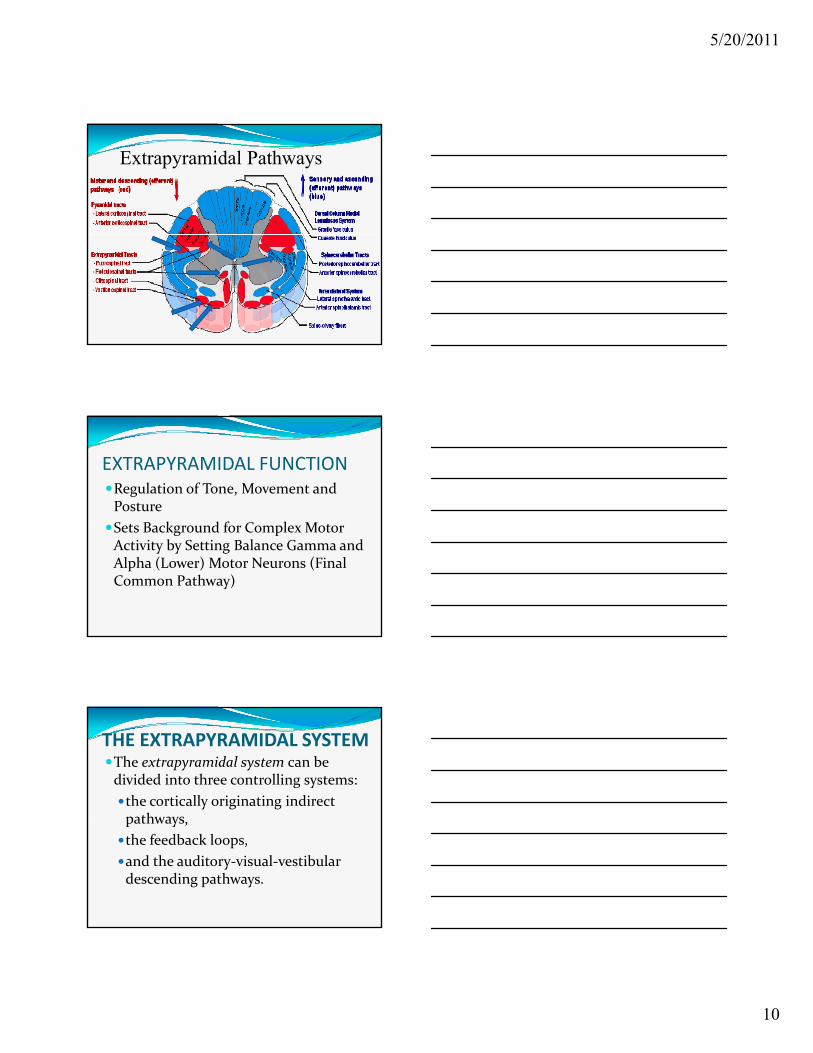
Extrapyramidal Pathways
EXTRAPYRAMIDAL FUNCTIONRegulation of Tone, Movement and Posture
Sets Background for Complex Motor Sets Background for Complex Motor Activity by Setting Balance Gamma and Alpha (Lower) Motor Neurons (Final Common Pathway)
THE EXTRAPYRAMIDAL SYSTEMThe extrapyramidal system can be divided into three controlling systems:
the cortically originating indirect pathways pathways,
the feedback loops,
and the auditory‐visual‐vestibular descending pathways.
5/20/2011
11
Cortically Originating Indirect Descending Pathways
Signals transmitted over the pyramidal system to produce voluntary movement are preceded by activity in neurons of the extrapyramidal system and relayed to the basal nuclei, red nucleus, and brainstem reticular formation (probably mechanism for reinforcement of formation (probably mechanism for reinforcement of MSR’s).
Basal nuclei contribute to background muscle tone and probably aid in fine tuning motor skills of the distal upper extremity.
The impulses projecting to the red nuclei influence spinal cord alpha and gamma motor neurons via
rubrospinal and other descending tracts.
Feedback Loops Neural circuits in which a signal sample is fed back to a "comparator," which can compare the signal with some pre‐programed desired condition and subsequently take steps to "adjust" or "modify" it.
The extrapyramidal system includes two such feedback py ysystems connecting from above and below:
cortically originating extrapyramidal system feedback loops (COEPS feedback loops) modifying feedback signals are returned to the cortex via the thalamocortical fibers.
proprioceptor originating extrapyramidal system feedback loops (POEPS feedback loops) modifying feedback signals through cerebellum to the spinal cord motor neurons.
Auditory Visual Vestibular Descending Pathways Postural adjustments in response to auditory (startle reflex – Jumping Frenchmen of Maine), visual (hands protect face), and vestibular signals (veering) is an additional face), and vestibular signals (veering) is an additional way to regulate the activity of spinal motor neurons.
Pathways explains why complex movements that can not be controlled voluntarily may occur spontaneously (e.g. A Parkinson patient who can not walk very well can run when frightened, or can catch a ball thrown at their face) as well as reflex balance movements.
5/20/2011
12
EXTRAPYRAMIDAL FUNCTION The basal ganglia have a “limbic” sector whose components are the nucleus accumbens (NA), ventral pallidum, and ventral tegmental area (VTA).
VTA efferents provide dopamine to the nucleus accumbens (ventral striatum) same as substantia nigra cells provive ( ) g pdopamine to the striatum.
Evidence suggests a central role in reward learning.
A number of highly addictive drugs, including cocaine, amphetamines, and nicotine, are thought to work by increasing the efficacy of the VTA→NA dopamine signal.
There is also evidence implicating over activity of the VTA dopaminergic projection in schizophrenia.
Clinical Signs of Basal Nuclei and Related Brainstem Dysfunction Chorea may be associated with dysfunction of the corpus striatum.
Sydenham's chorea, may be seen as a complication of rheumatic fever in children Recovery from this form of rheumatic fever in children. Recovery from this form of the disease is usually complete.
Huntington's chorea, is a hereditary disease which becomes progressively worse and often leads to severe mental debilitation loss of motor control and early death.
Athetosis is also associated with damage to the striatum and lateral parts of the globus pallidus.
5/20/2011
13
Clinical Signs of Basal Nuclei and Related Brainstem Dysfunction Ballismus, monoballismus and hemiballismus is generally associated with damage to the subthalamus and can occur spontaneously or be brought on by the initiation of a voluntary movement involving the initiation of a voluntary movement involving the affected limb.
Parkinson's disease (paralysis agitans) causes hypokinesia, tremor during rest and characteristic “pill‐rolling” principally involves the dopamine‐releasing fibers of the substantia nigra (nigro‐striatal pathway).
EXTRAPYRAMIDAL DISEASEDiffuse and Chronic
Acute, Well Circumscribed or Completely Destructive Lesions Rarely Cause Classic Picture
EXTRAPYRAMIDAL DISEASEGradual Onset
Hypertonia ( d )
Hyperkinesia
Emotional b l(Rigidity)
Bradykinesia
Hypokinesia
Lability
Dementia
5/20/2011
14
EXTRAPYRAMIDAL DISEASE Parkinson’s Disease
Parkinsonian Syndromes
Wilson’s Disease
Obsessive‐compulsive disorder
Attention‐deficit hyperactivity disorder
Congenital Athetosis
Sydenham’s Chorea
Huntington’s Chorea
Hemiballismus
Tourette’s Syndrome
hyperactivity disorder (ADHD)
Cerebral palsy: basal ganglia damage during second and third trimester of pregnancy
Tardive dyskinesia, caused by chronic antipsychotic treatment
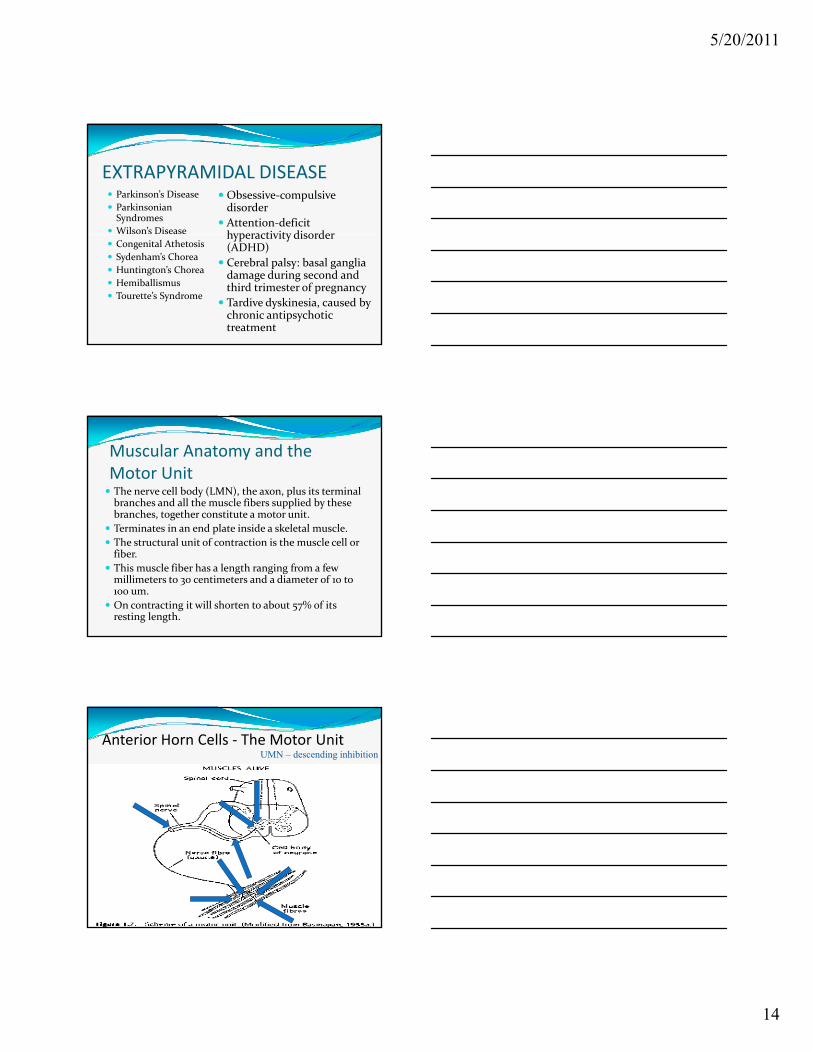
Muscular Anatomy and the Motor Unit The nerve cell body (LMN), the axon, plus its terminal branches and all the muscle fibers supplied by these branches, together constitute a motor unit.
T i t i d l t i id k l t l l Terminates in an end plate inside a skeletal muscle.
The structural unit of contraction is the muscle cell or fiber.
This muscle fiber has a length ranging from a few millimeters to 30 centimeters and a diameter of 10 to 100 um.
On contracting it will shorten to about 57% of its resting length.
Anterior Horn Cells ‐ The Motor UnitUMN – descending inhibition
5/20/2011
15
Functional Roles of Muscles Most muscles are capable of functioning in several different ways depending on
starting position
motion being performed
relation to gravity relation to gravity
direction of the motion
how much resistance it must overcome
As the variables change, so do the roles the muscle play.
All of these factors are “automatically” accounted for with every voluntary movement by reflex connections in the nervous system.
Functional Roles of MusclesFive primary roles
Agonist or prime mover
UMN – for “voluntary” movement selects ylmn’s to activate specific muscles.
Synergist
Antagonist
Stabilizer or fixator
Neutralizer
Functional Roles of MusclesAgonist – a muscle or group of muscles that causes the motion
Th l i i ll The muscle contracts isotonically to produce a motion or isometrically to maintain a position.
5/20/2011
16
Functional Roles of MusclesSynergistic – aids in the movement of a prime moverAssistive – assists in prime mover muscle actionmuscle action
Neutralizers ‐ prevents unwanted movements inherent in the action of the agonist (e.g. pronator teres contraction to stop bicep induced supination during elbow flexion).
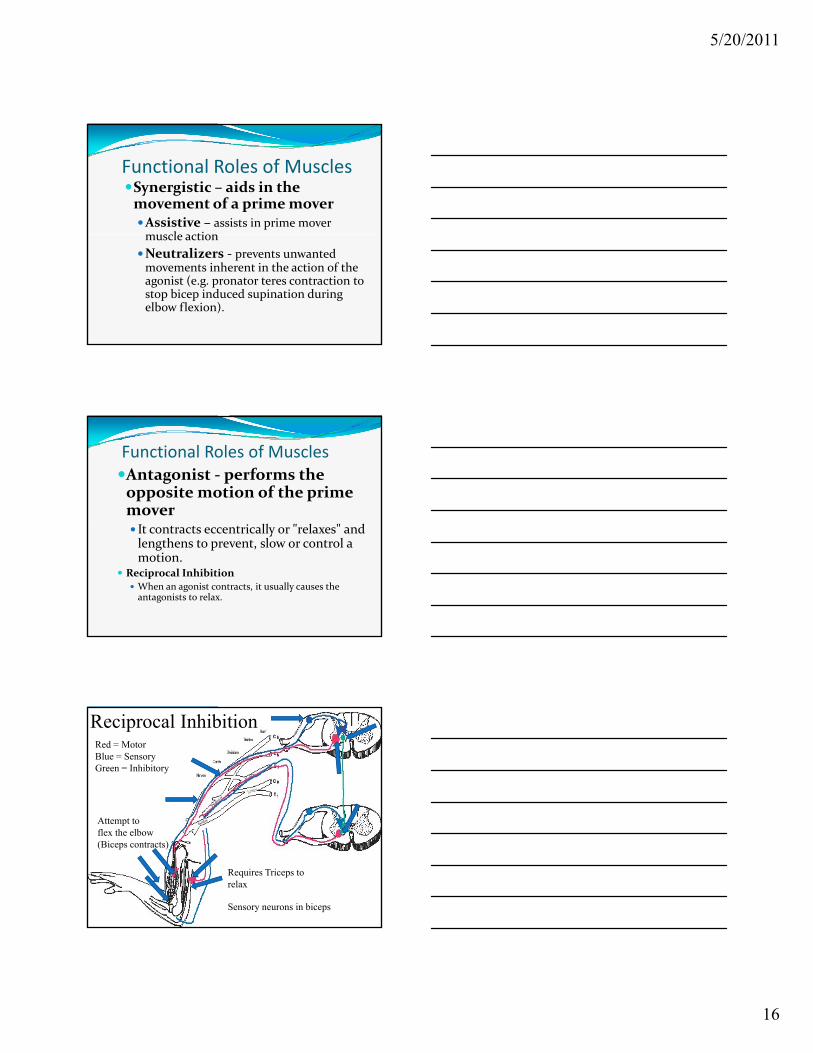
Functional Roles of MusclesAntagonist ‐ performs the opposite motion of the prime moverIt t t t i ll " l " d It contracts eccentrically or "relaxes" and lengthens to prevent, slow or control a motion.
Reciprocal Inhibition When an agonist contracts, it usually causes the antagonists to relax.
A
Reciprocal Inhibition Red = MotorBlue = SensoryGreen = Inhibitory
Attempt to flex the elbow(Biceps contracts)
Requires Triceps torelax
Sensory neurons in biceps
5/20/2011
17
Functional Roles of MusclesStabilizer – (AKA: fixators) the muscle may contract to hold a body part immobile while another body part is moving.
The sustained stabilizing contraction is The sustained stabilizing contraction is frequently isometric. In most normal activities, proximal joints are stabilized by muscle contractions during movement of more distal joints.
Functional Roles of Muscles
Stabilizers and Neutralizers both use co‐contraction to prevent motion.
Stabilizers are associated with joints;
Neutralizers are associated with muscle.
Testing MovementCrude.
Sensitive.
Specific?.
More Definitive Tests Isolate System Involved.
5/20/2011
18
Gait ObservationPhases of gait.Foot Placement Specific. Heel Striking First Controlled Placement of Foot and Big Toe.
Smooth and Rhythmic.Arm Swing Symmetrical and Natural.
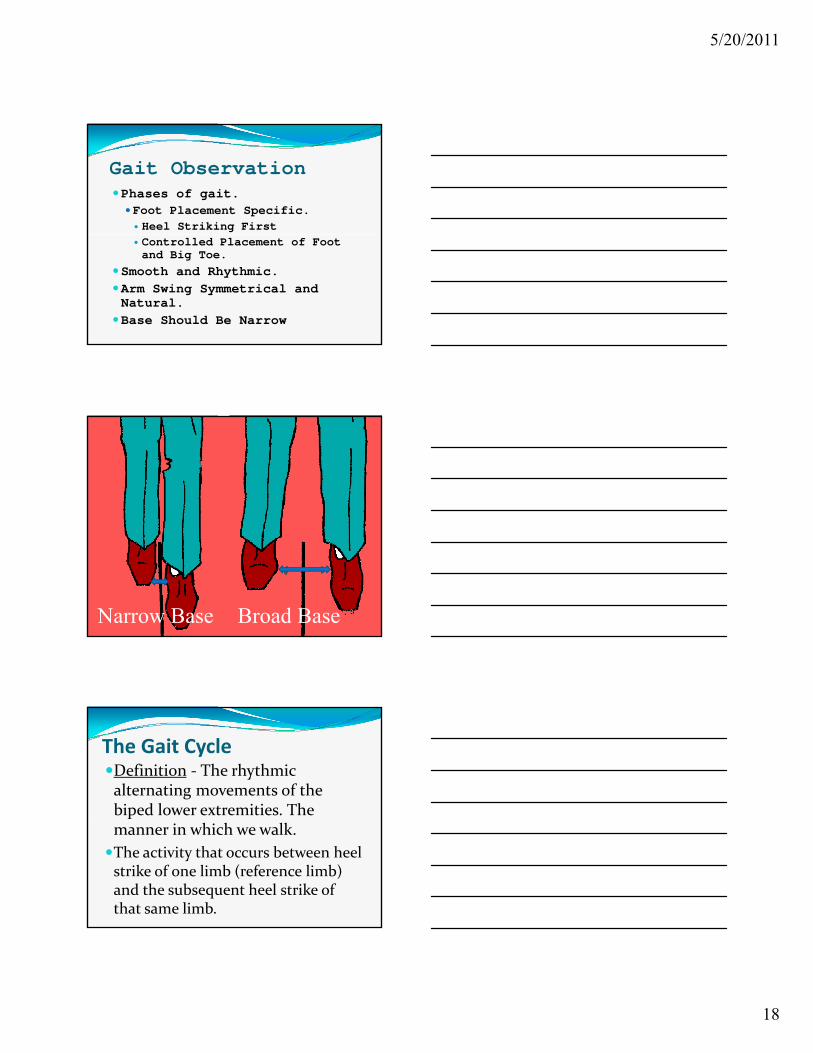
Base Should Be Narrow
Narrow Base Broad Base
The Gait CycleDefinition ‐ The rhythmic alternating movements of the biped lower extremities. The pmanner in which we walk.
The activity that occurs between heel strike of one limb (reference limb) and the subsequent heel strike of that same limb.
5/20/2011
19
The Gait CycleTwo Phases STANCE ( support) PHASE – Reference lower extremity is touching the ground
D i it l f t i t hi th d During gait only one foot is touching the ground for most of the cycle.
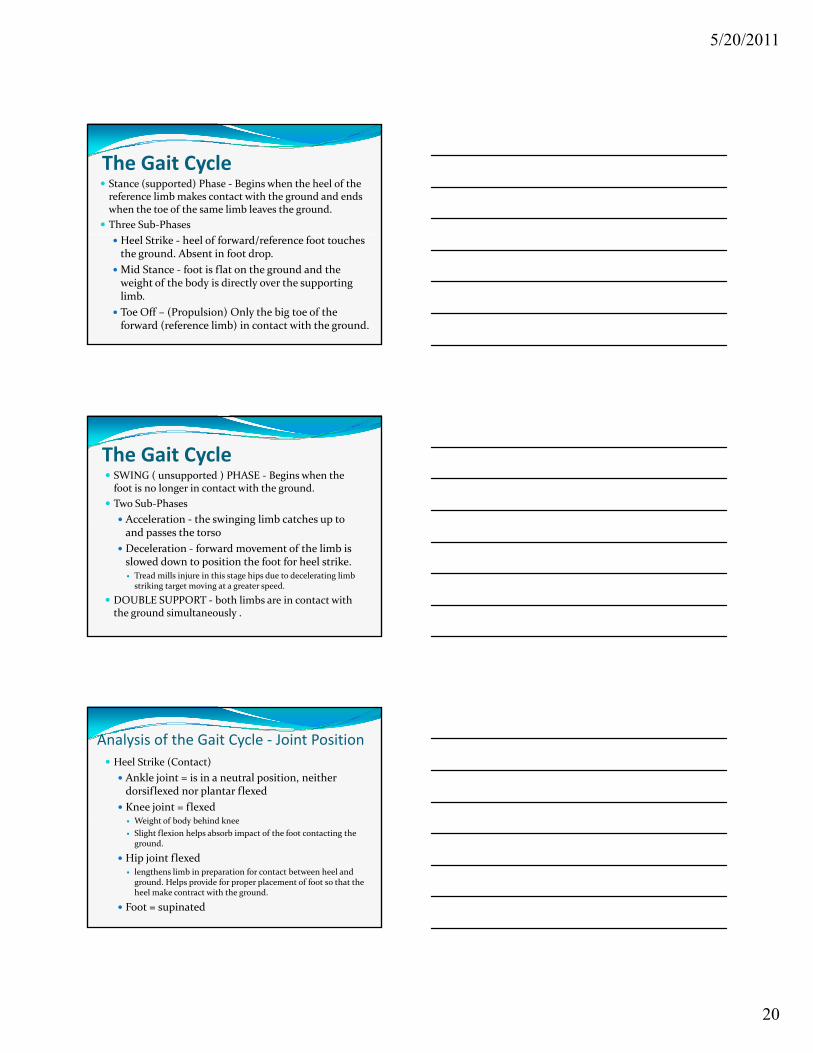
Each foot should touch the ground with a tripod of support due to the arches of the forefoot.
SWING PHASE ‐ Reference lower extremity is not touching the ground
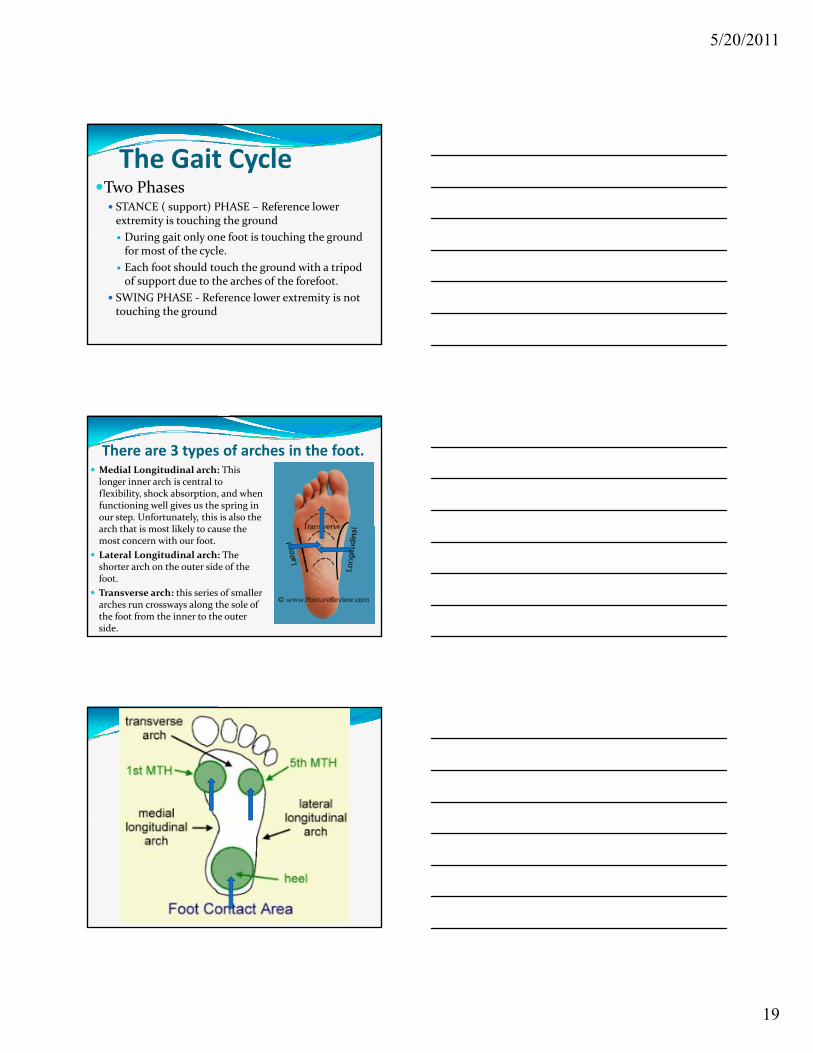
There are 3 types of arches in the foot. Medial Longitudinal arch: This longer inner arch is central to flexibility, shock absorption, and when functioning well gives us the spring in our step. Unfortunately, this is also the
h h i lik l h arch that is most likely to cause the most concern with our foot.
Lateral Longitudinal arch: The shorter arch on the outer side of the foot.
Transverse arch: this series of smaller arches run crossways along the sole of the foot from the inner to the outer side.
5/20/2011
20
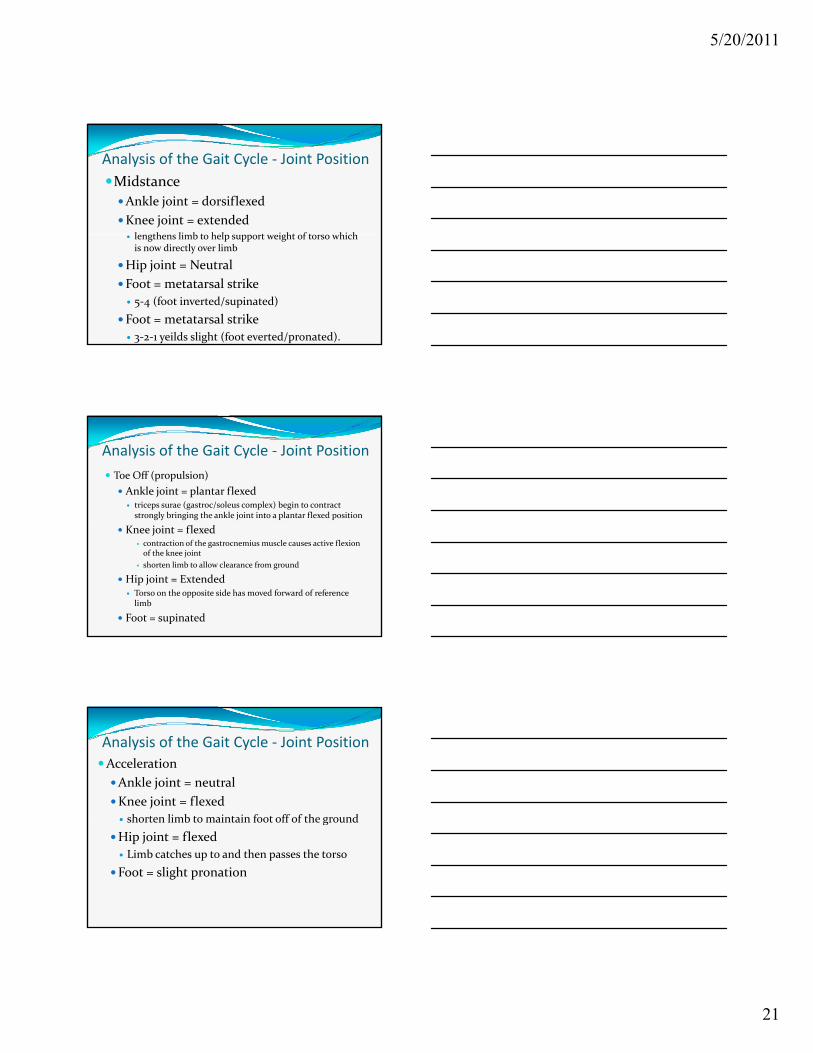
The Gait Cycle Stance (supported) Phase ‐ Begins when the heel of the reference limb makes contact with the ground and ends when the toe of the same limb leaves the ground.
Three Sub‐Phases
Heel Strike ‐ heel of forward/reference foot touches the ground. Absent in foot drop.
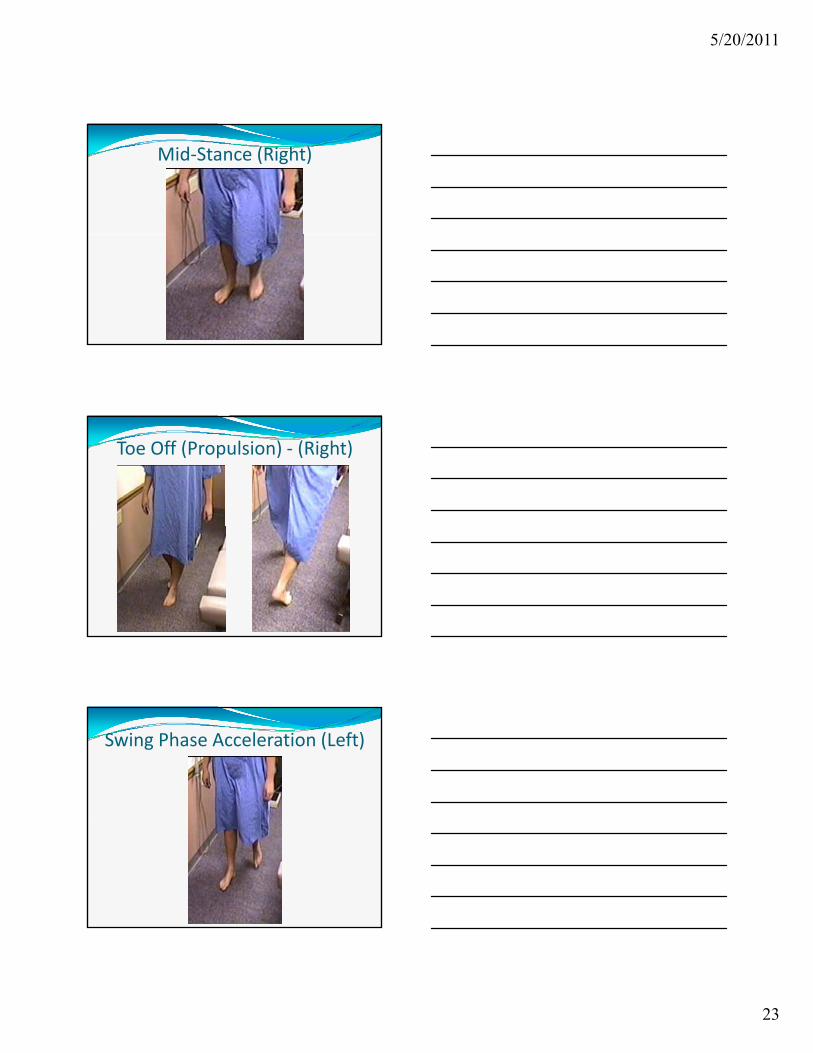
Mid Stance ‐ foot is flat on the ground and the weight of the body is directly over the supporting limb.
Toe Off – (Propulsion) Only the big toe of the forward (reference limb) in contact with the ground.
The Gait Cycle SWING ( unsupported ) PHASE ‐ Begins when the foot is no longer in contact with the ground.
Two Sub‐Phases
Acceleration ‐ the swinging limb catches up to and passes the torso
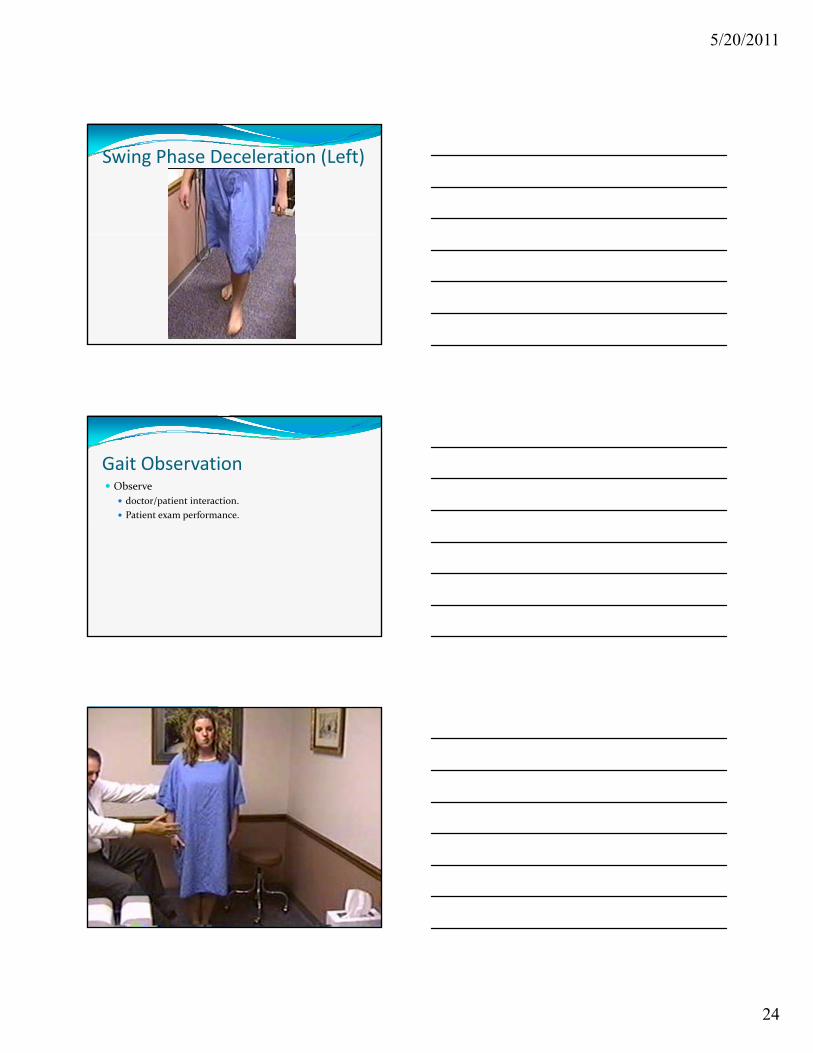
Deceleration ‐ forward movement of the limb is slowed down to position the foot for heel strike. Tread mills injure in this stage hips due to decelerating limb striking target moving at a greater speed.
DOUBLE SUPPORT ‐ both limbs are in contact with the ground simultaneously .
Analysis of the Gait Cycle ‐ Joint Position
Heel Strike (Contact)
Ankle joint = is in a neutral position, neither dorsiflexed nor plantar flexed
Knee joint = flexed W i h f b d b hi d k Weight of body behind knee
Slight flexion helps absorb impact of the foot contacting the ground.
Hip joint flexed lengthens limb in preparation for contact between heel and ground. Helps provide for proper placement of foot so that the heel make contract with the ground.
Foot = supinated
5/20/2011
21
Analysis of the Gait Cycle ‐ Joint Position
Midstance
Ankle joint = dorsiflexed
Knee joint = extended l th li b t h l t i ht f t hi h lengthens limb to help support weight of torso which is now directly over limb
Hip joint = Neutral
Foot = metatarsal strike
5‐4 (foot inverted/supinated)
Foot = metatarsal strike
3‐2‐1 yeilds slight (foot everted/pronated).
Toe Off (propulsion)
Ankle joint = plantar flexed triceps surae (gastroc/soleus complex) begin to contract strongly bringing the ankle joint into a plantar flexed position
K j i fl d
Analysis of the Gait Cycle ‐ Joint Position
Knee joint = flexed contraction of the gastrocnemius muscle causes active flexion of the knee joint
shorten limb to allow clearance from ground
Hip joint = Extended Torso on the opposite side has moved forward of reference limb
Foot = supinated
Acceleration
Ankle joint = neutral
Knee joint = flexed
shorten limb to maintain foot off of the ground
Analysis of the Gait Cycle ‐ Joint Position
shorten limb to maintain foot off of the ground
Hip joint = flexed
Limb catches up to and then passes the torso
Foot = slight pronation
5/20/2011
22
Heel Strike (Right)
5/20/2011
23
Mid‐Stance (Right)
Toe Off (Propulsion) ‐ (Right)
Swing Phase Acceleration (Left)
5/20/2011
24
Swing Phase Deceleration (Left)
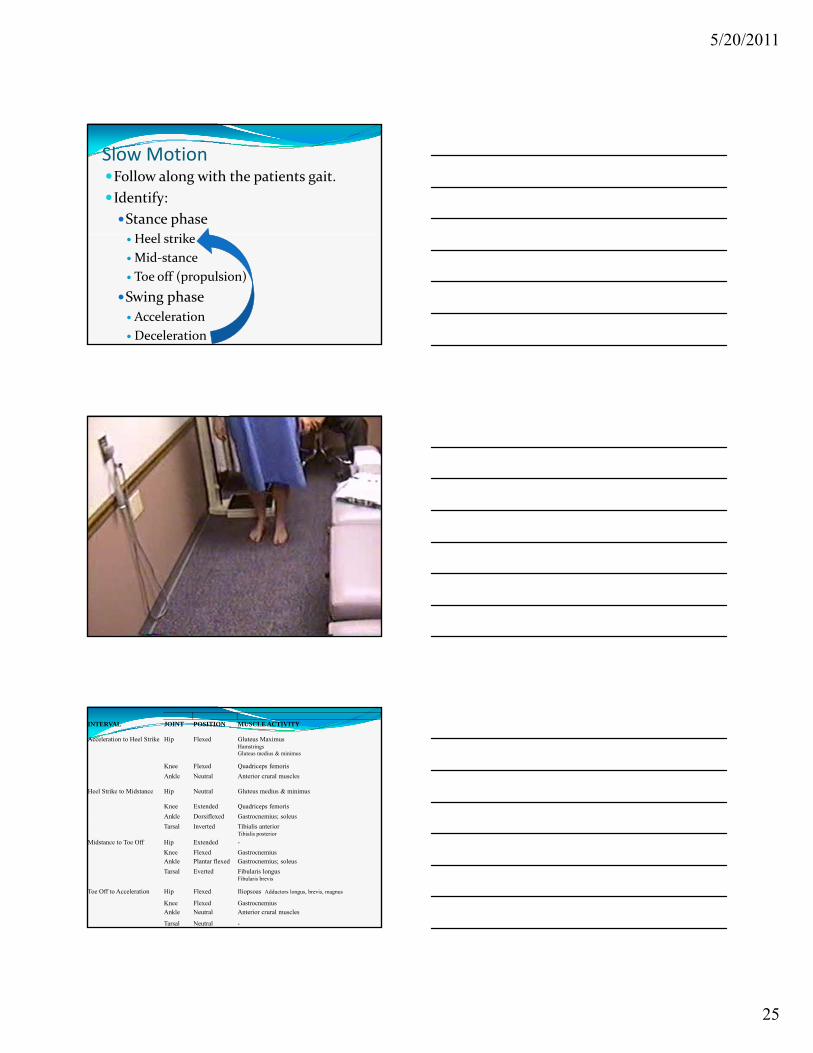
Gait Observation Observe
doctor/patient interaction.
Patient exam performance.
5/20/2011
25
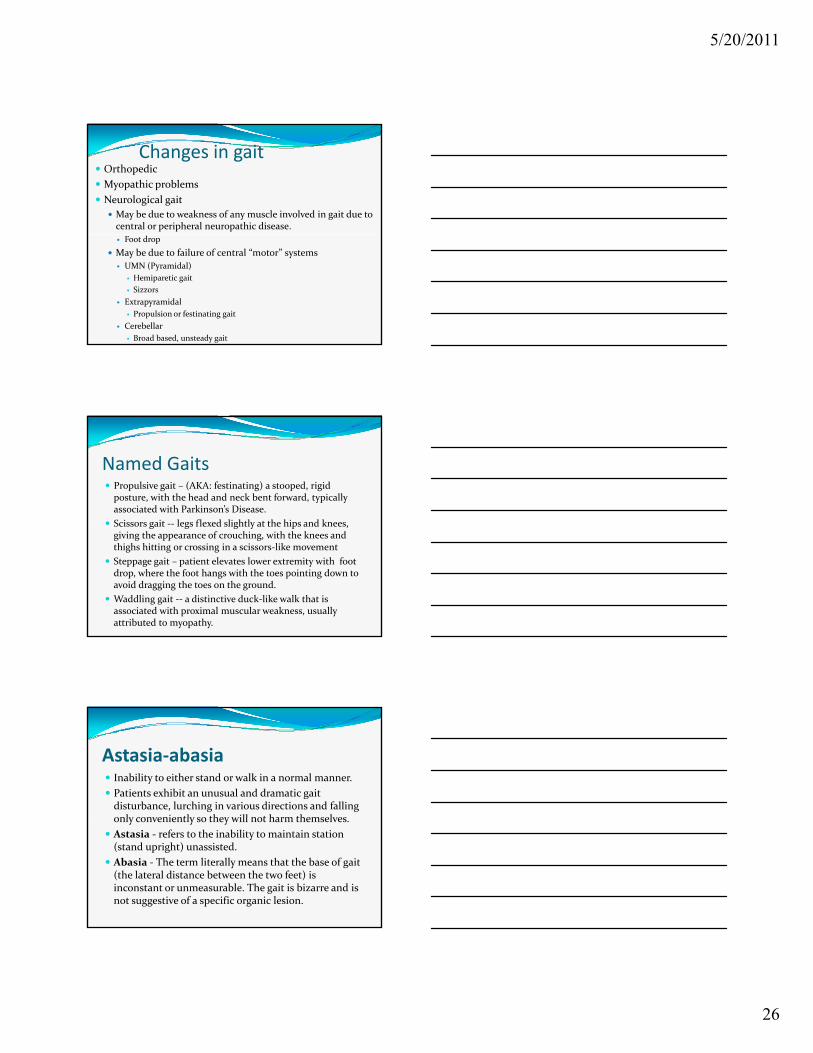
Slow MotionFollow along with the patients gait.
Identify:
Stance phase
H l ikHeel strike
Mid‐stance
Toe off (propulsion)
Swing phase
Acceleration
Deceleration
INTERVAL JOINT POSITION MUSCLE ACTIVITY
Acceleration to Heel Strike Hip Flexed Gluteus Maximus HamstringsGluteus medius & minimus
Knee Flexed Quadriceps femoris
Ankle Neutral Anterior crural muscles
Heel Strike to Midstance Hip Neutral Gluteus medius & minimus
Knee Extended Quadriceps femoris
Ankle Dorsiflexed Gastrocnemius; soleusAnkle Dorsiflexed Gastrocnemius; soleus
Tarsal Inverted Tibialis anterior Tibialis posterior
Midstance to Toe Off Hip Extended -
Knee Flexed GastrocnemiusAnkle Plantar flexed Gastrocnemius; soleus
Tarsal Everted Fibularis longusFibularis brevis
Toe Off to Acceleration Hip Flexed Iliopsoas Adductors longus, brevis, magnus
Knee Flexed GastrocnemiusAnkle Neutral Anterior crural muscles
Tarsal Neutral -
5/20/2011
26
Changes in gait Orthopedic
Myopathic problems
Neurological gait
May be due to weakness of any muscle involved in gait due to central or peripheral neuropathic disease.
Foot drop
May be due to failure of central “motor” systems
UMN (Pyramidal)
Hemiparetic gait
Sizzors
Extrapyramidal
Propulsion or festinating gait
Cerebellar
Broad based, unsteady gait
Named Gaits Propulsive gait – (AKA: festinating) a stooped, rigid posture, with the head and neck bent forward, typically associated with Parkinson’s Disease.
Scissors gait ‐‐ legs flexed slightly at the hips and knees, Scissors gait legs flexed slightly at the hips and knees, giving the appearance of crouching, with the knees and thighs hitting or crossing in a scissors‐like movement
Steppage gait – patient elevates lower extremity with foot drop, where the foot hangs with the toes pointing down to avoid dragging the toes on the ground.
Waddling gait ‐‐ a distinctive duck‐like walk that is associated with proximal muscular weakness, usually attributed to myopathy.
Astasia‐abasia Inability to either stand or walk in a normal manner.
Patients exhibit an unusual and dramatic gait disturbance, lurching in various directions and falling only conveniently so they will not harm themselvesonly conveniently so they will not harm themselves.
Astasia ‐ refers to the inability to maintain station (stand upright) unassisted.
Abasia ‐ The term literally means that the base of gait (the lateral distance between the two feet) is inconstant or unmeasurable. The gait is bizarre and is not suggestive of a specific organic lesion.
5/20/2011
27
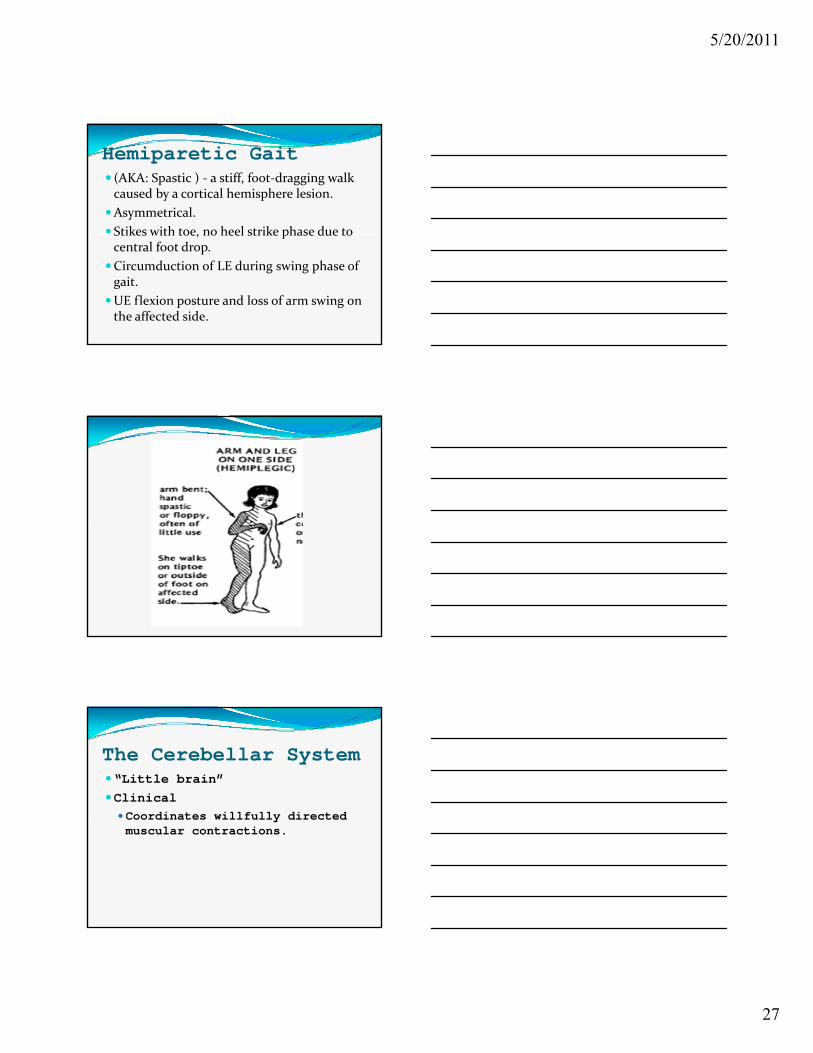
Hemiparetic Gait (AKA: Spastic ) ‐ a stiff, foot‐dragging walk caused by a cortical hemisphere lesion.
Asymmetrical.
Stikes with toe, no heel strike phase due to Stikes with toe, no heel strike phase due to central foot drop.
Circumduction of LE during swing phase of gait.
UE flexion posture and loss of arm swing on the affected side.
The Cerebellar System“Little brain”
ClinicalCoordinates willfully directedCoordinates willfully directed muscular contractions.
5/20/2011
28
The cerebellum Outgrowth of the vestibular system, sits atop the brainstem.
accounts for approximately 15‐25% of the brain.
i i h l ll i f h communicates with almost all regions of the neuroaxis, with the single exception of the striatum, and has been implicated in cognitive, emotional, sensory, motor and speech processing.
has been shown to display neuroplasticity and learning and memory and may serve as an integrative interface for cognition, emotion, motor functioning and memory.
The cerebellum Typically thought of as a motor center to coordinate fine motor control including speech and visual processing, including the visual guidance of movement.
Electrical‐electrode stimulation or damage to this structure can trigger rage reactions and hyperactivity including can trigger rage reactions and hyperactivity including “mania”.
Abnormalities in the cerebellum have also been implicated in the pathogenesis of schizophrenia and autism.
Monkeys reared under deprived conditions displayed abnormal activity in the cerebellum (dentate gyrus) and autistic behavior.
The cerebellum Exerts a tonic and stabilizing influence on motor function and can coordinate, smooth, fine tune, and exert a timing influence on motor movements.
Some cerebellar neurons become activated just thinking b ki about making a movement.
Not just associated with motor functioning, but classical conditioning and the learning of new complex motor programs.
The cerebellum may slowly assume control over learned movements, which become "automatic" and can be performed with little or no help from the cerebrum which is then free to do other things.
5/20/2011
29
The cerebellumConversely, cerebellar lesions slow or abolish the acquisition and retention of conditioned responses and compound movements more
l th i l t severely then simple movements.
These and other findings suggests that the cerebellum may act to integrate and combine different movements, and movement sequences.
The cerebellum
The cerebellum
5/20/2011
30
5/20/2011
31
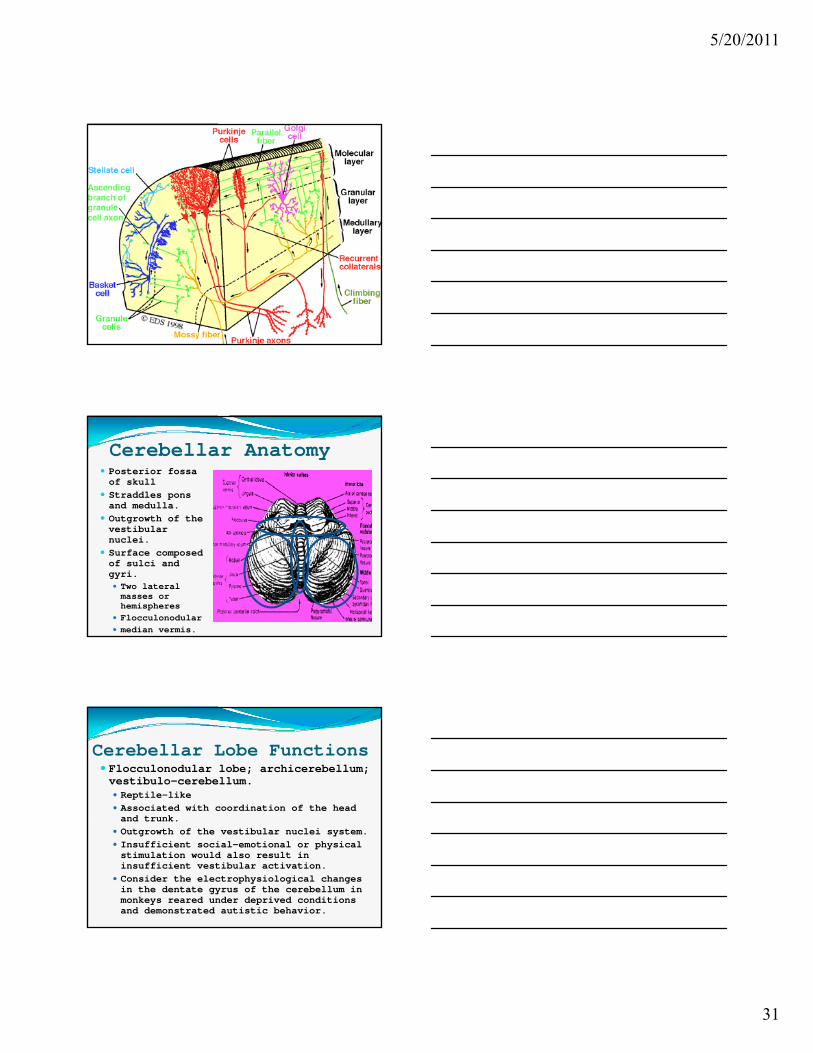
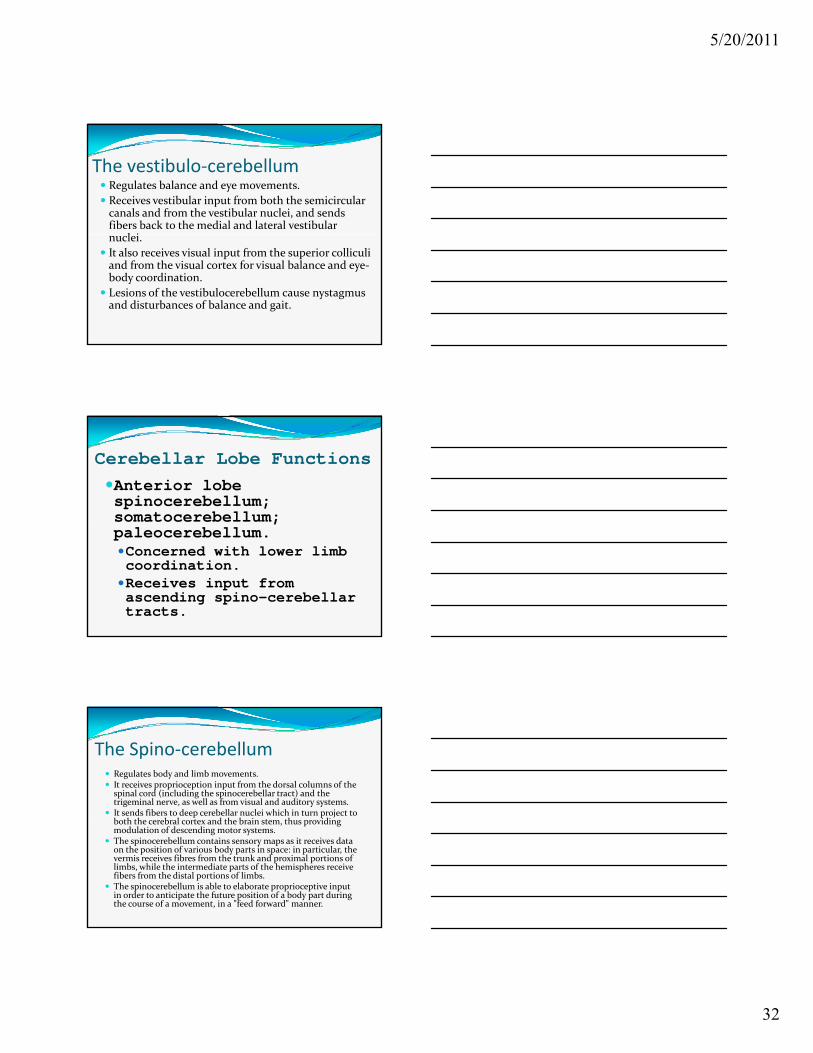
Cerebellar Anatomy Posterior fossa of skull
Straddles pons and medulla.
Outgrowth of the tib lvestibular
nuclei. Surface composed of sulci and gyri. Two lateral masses or hemispheres
Flocculonodular median vermis.
Cerebellar Lobe Functions Flocculonodular lobe; archicerebellum; vestibulo-cerebellum. Reptile-like Associated with coordination of the head and trunkand trunk.
Outgrowth of the vestibular nuclei system. Insufficient social-emotional or physical stimulation would also result in insufficient vestibular activation.
Consider the electrophysiological changes in the dentate gyrus of the cerebellum in monkeys reared under deprived conditions and demonstrated autistic behavior.
5/20/2011
32
The vestibulo‐cerebellum Regulates balance and eye movements.
Receives vestibular input from both the semicircular canals and from the vestibular nuclei, and sends fibers back to the medial and lateral vestibular
l i nuclei.
It also receives visual input from the superior colliculiand from the visual cortex for visual balance and eye‐body coordination.
Lesions of the vestibulocerebellum cause nystagmus and disturbances of balance and gait.
Cerebellar Lobe Functions
Anterior lobe spinocerebellum; somatocerebellum; paleocerebellum.Concerned with lower limb coordination.Receives input from ascending spino-cerebellar tracts.
The Spino‐cerebellum Regulates body and limb movements. It receives proprioception input from the dorsal columns of the
spinal cord (including the spinocerebellar tract) and the trigeminal nerve, as well as from visual and auditory systems.
It sends fibers to deep cerebellar nuclei which in turn project to b h h b l d h b h d
jboth the cerebral cortex and the brain stem, thus providing modulation of descending motor systems.
The spinocerebellum contains sensory maps as it receives data on the position of various body parts in space: in particular, the vermis receives fibres from the trunk and proximal portions of limbs, while the intermediate parts of the hemispheres receive fibers from the distal portions of limbs.
The spinocerebellum is able to elaborate proprioceptive input in order to anticipate the future position of a body part during the course of a movement, in a "feed forward" manner.
5/20/2011
33
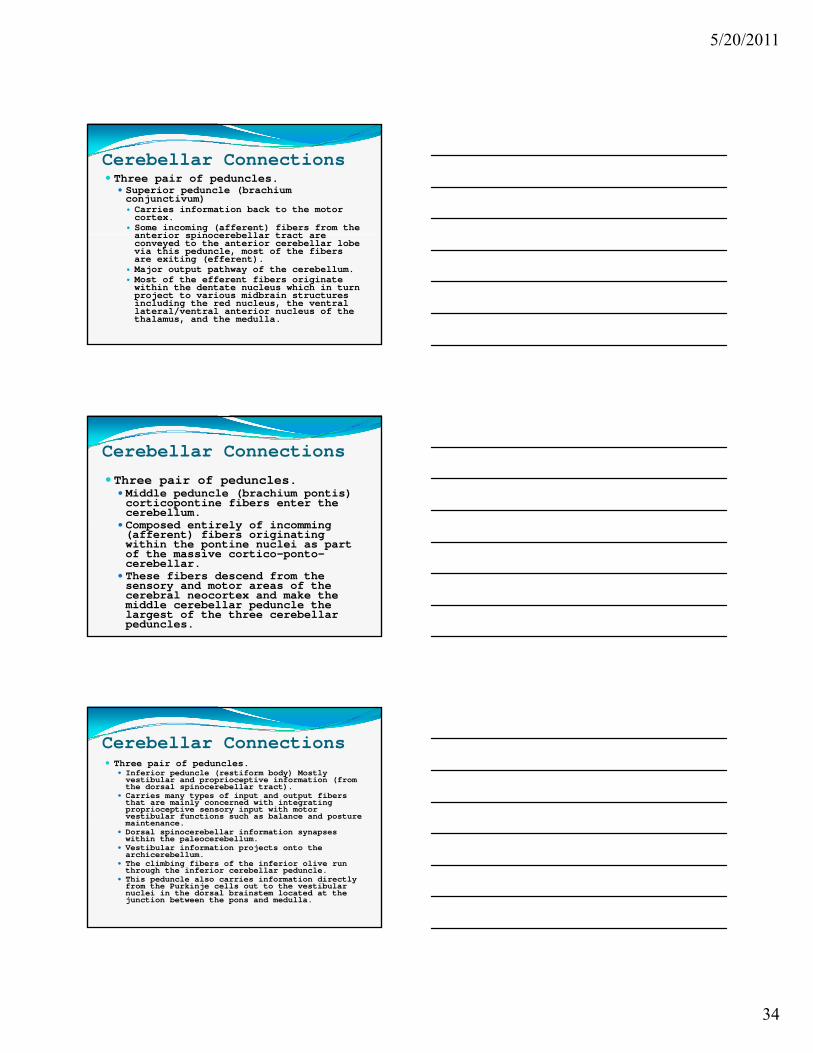
Cerebellar Lobe Functions The posterior lobe; hemispheres; cerebro-cerebellum; pontocerebellum; neocerebellum) Coordinates voluntary movement of the ipsilateral body side.
Input from and output to (feedback loop) to the contralateral cerebral motor areas from the Dentate nucleus.
The neocerebellum is involved in planning movement that is about to occur and has purely cognitive functions as well.
The Neocerebellum Involved in planning movement and evaluating sensory information for action.
Receives input exclusively from the cerebral cortex (parietal frontal) via the pontine nuclei (forming (parietal‐frontal) via the pontine nuclei (forming cortico‐ponto‐cerebellar pathways).
Sends fibers to the ventrolateral thalamus (connected to motor areas of the premotor and primary motor area of the cortex) and to the red nucleus (connected to inferior olivary nucleus, which links back to the cerebellar hemispheres).
5/20/2011
34
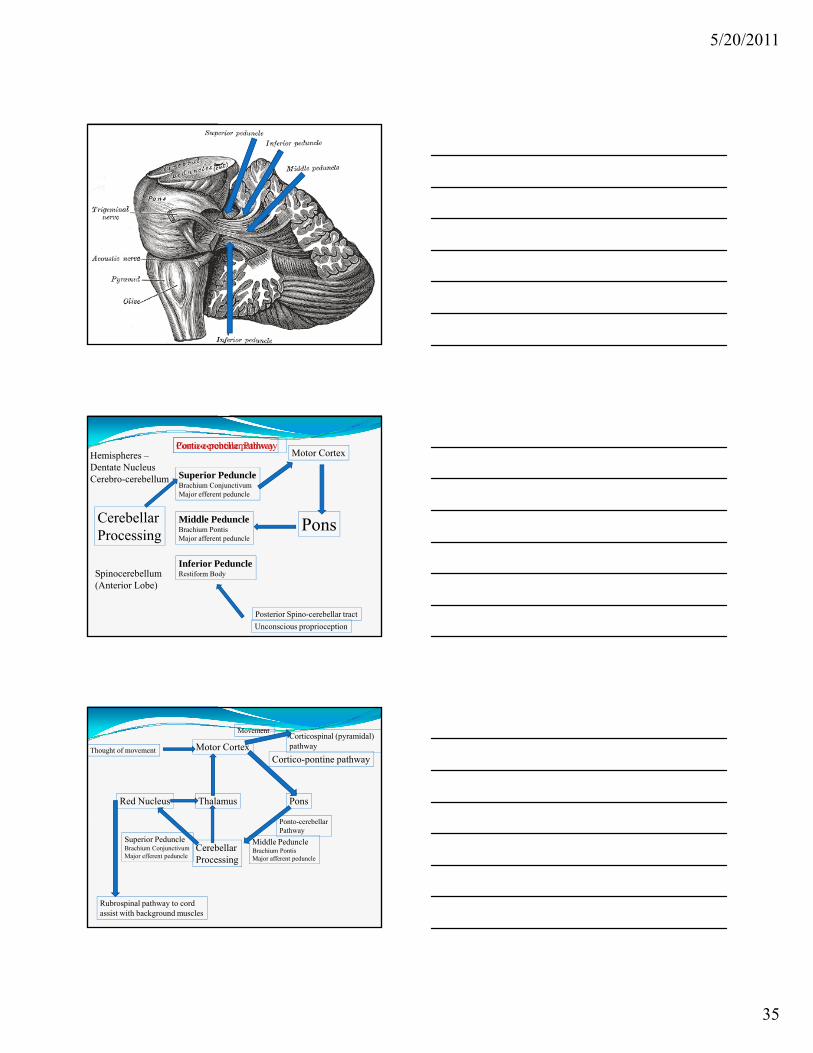
Cerebellar Connections Three pair of peduncles.
Superior peduncle (brachium conjunctivum) Carries information back to the motor cortex.
Some incoming (afferent) fibers from the anterior spinocerebellar tract areanterior spinocerebellar tract are conveyed to the anterior cerebellar lobe via this peduncle, most of the fibers are exiting (efferent).
Major output pathway of the cerebellum. Most of the efferent fibers originate within the dentate nucleus which in turn project to various midbrain structures including the red nucleus, the ventral lateral/ventral anterior nucleus of the thalamus, and the medulla.
Cerebellar Connections
Three pair of peduncles. Middle peduncle (brachium pontis) corticopontine fibers enter the cerebellum.
Composed entirely of incomming Composed entirely of incomming(afferent) fibers originating within the pontine nuclei as part of the massive cortico-ponto-cerebellar.
These fibers descend from the sensory and motor areas of the cerebral neocortex and make the middle cerebellar peduncle the largest of the three cerebellar peduncles.
Cerebellar Connections Three pair of peduncles.
Inferior peduncle (restiform body) Mostly vestibular and proprioceptive information (from the dorsal spinocerebellar tract).
Carries many types of input and output fibers that are mainly concerned with integrating proprioceptive sensory input with motor vestibular functions such as balance and posturevestibular functions such as balance and posture maintenance.
Dorsal spinocerebellar information synapses within the paleocerebellum.
Vestibular information projects onto the archicerebellum.
The climbing fibers of the inferior olive run through the inferior cerebellar peduncle.
This peduncle also carries information directly from the Purkinje cells out to the vestibular nuclei in the dorsal brainstem located at the junction between the pons and medulla.
5/20/2011
35
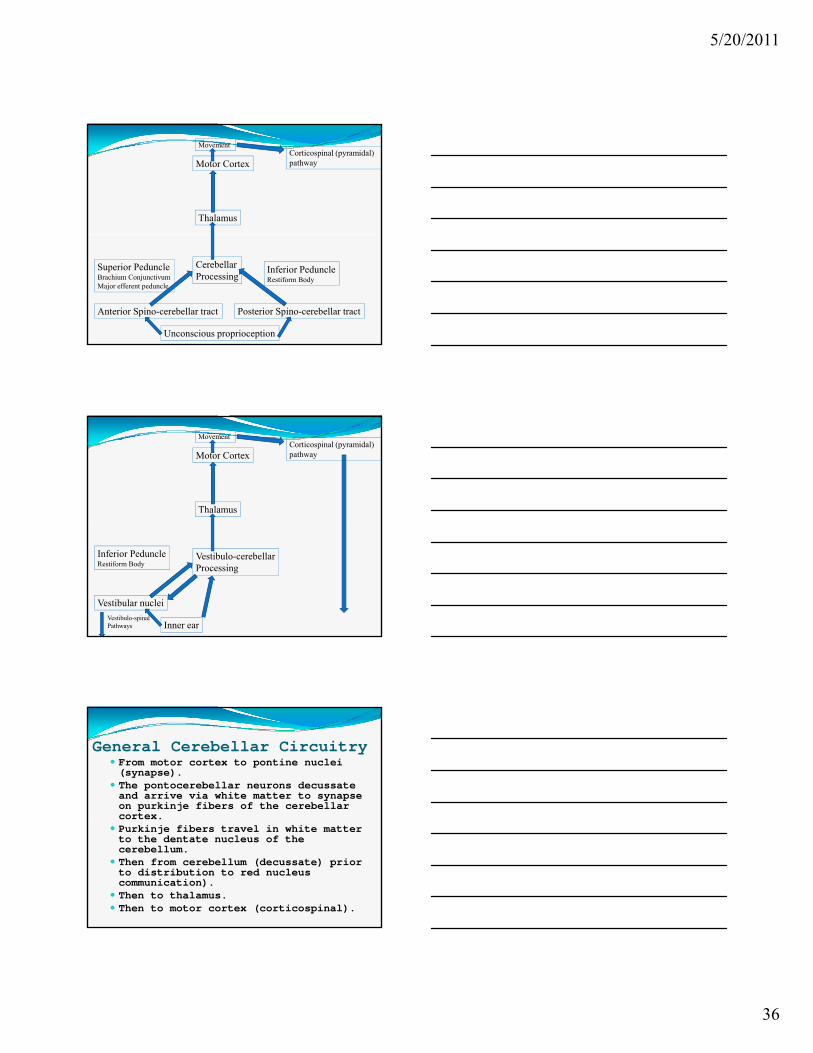
Motor Cortex
Cerebellar PonsMiddle Peduncle
Cortico-pontine pathwayPonto-cerebellar Pathway
Superior PeduncleBrachium ConjunctivumMajor efferent peduncle
Hemispheres –Dentate NucleusCerebro-cerebellum
Processing
Unconscious proprioception
Posterior Spino-cerebellar tract
PonsBrachium PontisMajor afferent peduncle
Inferior PeduncleRestiform BodySpinocerebellum
(Anterior Lobe)
Motor Cortex
Red Nucleus Thalamus Pons
Movement
Cortico-pontine pathway
Corticospinal (pyramidal)pathway
Thought of movement
CerebellarProcessing
Middle PeduncleBrachium PontisMajor afferent peduncle
Ponto-cerebellarPathway
Superior PeduncleBrachium ConjunctivumMajor efferent peduncle
Rubrospinal pathway to cordassist with background muscles
5/20/2011
36
Motor Cortex
Thalamus
Movement Corticospinal (pyramidal)pathway
CerebellarProcessing
Unconscious proprioception
Anterior Spino-cerebellar tract Posterior Spino-cerebellar tract
Inferior PeduncleRestiform Body
Superior PeduncleBrachium ConjunctivumMajor efferent peduncle
Motor Cortex
Thalamus
Movement Corticospinal (pyramidal)pathway
Vestibulo-cerebellarProcessing
Inner ear
Vestibular nuclei
Inferior PeduncleRestiform Body
Vestibulo-spinalPathways
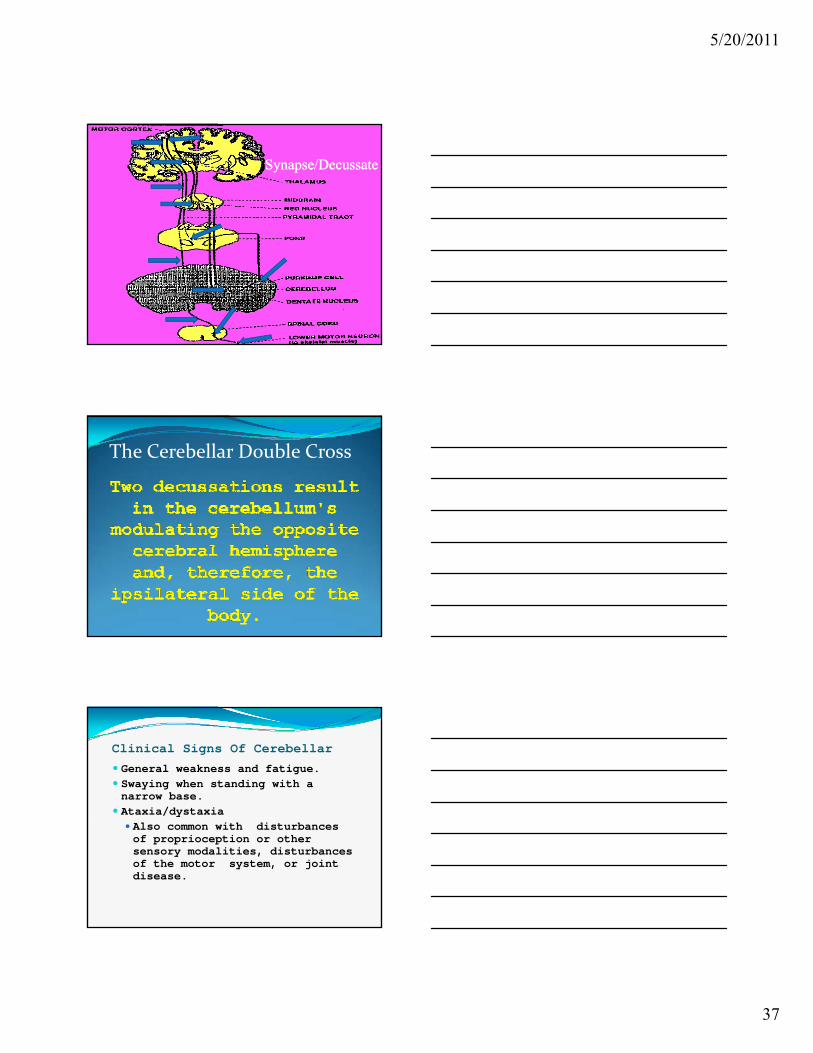
General Cerebellar Circuitry From motor cortex to pontine nuclei (synapse).
The pontocerebellar neurons decussate and arrive via white matter to synapse on purkinje fibers of the cerebellar cortexcortex.
Purkinje fibers travel in white matter to the dentate nucleus of the cerebellum.
Then from cerebellum (decussate) prior to distribution to red nucleus communication).
Then to thalamus. Then to motor cortex (corticospinal).
5/20/2011
37
Synapse/DecussateSynapse/Decussate
The Cerebellar Double Cross
Clinical Signs Of Cerebellar
General weakness and fatigue. Swaying when standing with a narrow base.
Ataxia/dystaxia Also common with disturbances of proprioception or other sensory modalities, disturbances of the motor system, or joint disease.
5/20/2011
38
Clinical Signs Of Cerebellar Dysfunction
Cerebellar Gait Broad based Broad-based
Clinical Signs Of Cerebellar Dysfunction Dysarthria (slurring of speech)
Listen for dysarthria of recent onset.
"Whosoever, whatsoever, or perfect pleasures" or any tongue twister.
Tremor
Nystagmus
5/20/2011
39
Clinical Signs Of Cerebellar Dysfunction Hypotonia.
“Rag doll” posture and gait.
Decomposition of movement.
" b h "Movement by the numbers”.
Dysdiadochokinesia Inability to perform rapidly alternating movements. Rapidly supinate and pronate the hands.
Thigh slap. Tap foot rapidly.
Clinical Signs Of Cerebellar DysfunctionThe pendular reflex?
5/20/2011
40
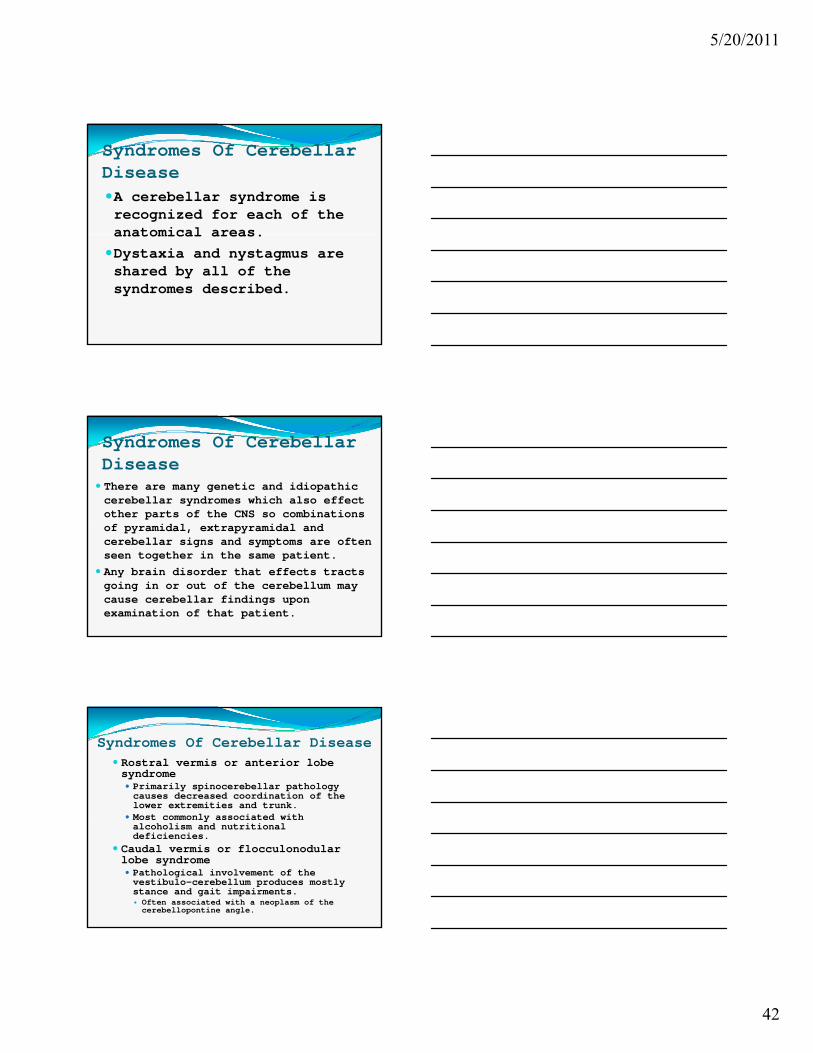
Overshooting And Undershooting Difficulty in measuring distances will overestimate or underestimate the distance to a particular point.
Eyes open.y p Finger-to-nose test. Observe for intention tremor More objective method is wrist slap test.
Lower extremity = heel-to-shin test.
The rebound sign test
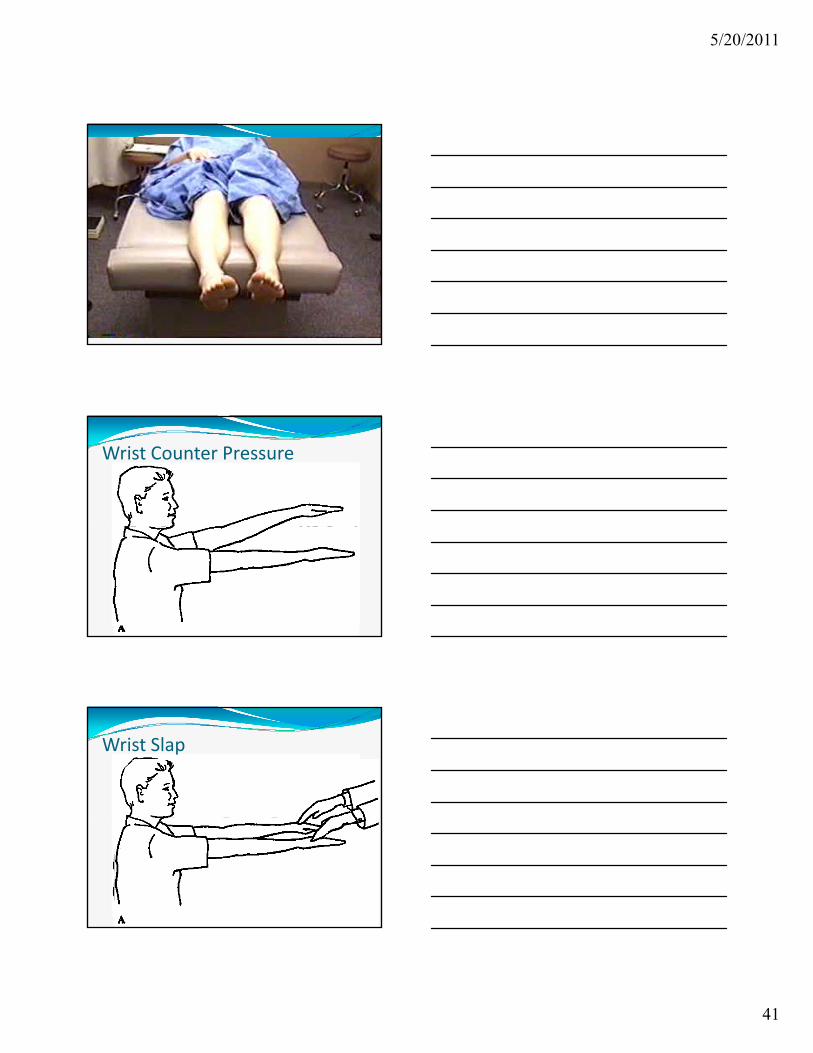
Patient Video Vignettes In the two following patients we will perform some cerebellar test.
As always, observe the doctors instructions and communication as well as the technical test communication, as well as the technical test performance by the patient.
In the second case you will see how removing visual clues from the patient causes the test to become a proprioceptive test.
5/20/2011
41
Wrist Counter Pressure
Wrist Slap
5/20/2011
42
Syndromes Of Cerebellar DiseaseA cerebellar syndrome is recognized for each of the anatomical areasanatomical areas.
Dystaxia and nystagmus are shared by all of the syndromes described.
Syndromes Of Cerebellar Disease There are many genetic and idiopathic cerebellar syndromes which also effect other parts of the CNS so combinations of pyramidal extrapyramidal andof pyramidal, extrapyramidal and cerebellar signs and symptoms are often seen together in the same patient.
Any brain disorder that effects tracts going in or out of the cerebellum may cause cerebellar findings upon examination of that patient.
Syndromes Of Cerebellar Disease Rostral vermis or anterior lobe syndrome Primarily spinocerebellar pathology causes decreased coordination of the lower extremities and trunk.
Most commonly associated with Most commonly associated with alcoholism and nutritional deficiencies.
Caudal vermis or flocculonodularlobe syndrome Pathological involvement of the vestibulo-cerebellum produces mostly stance and gait impairments. Often associated with a neoplasm of the cerebellopontine angle.
5/20/2011
43
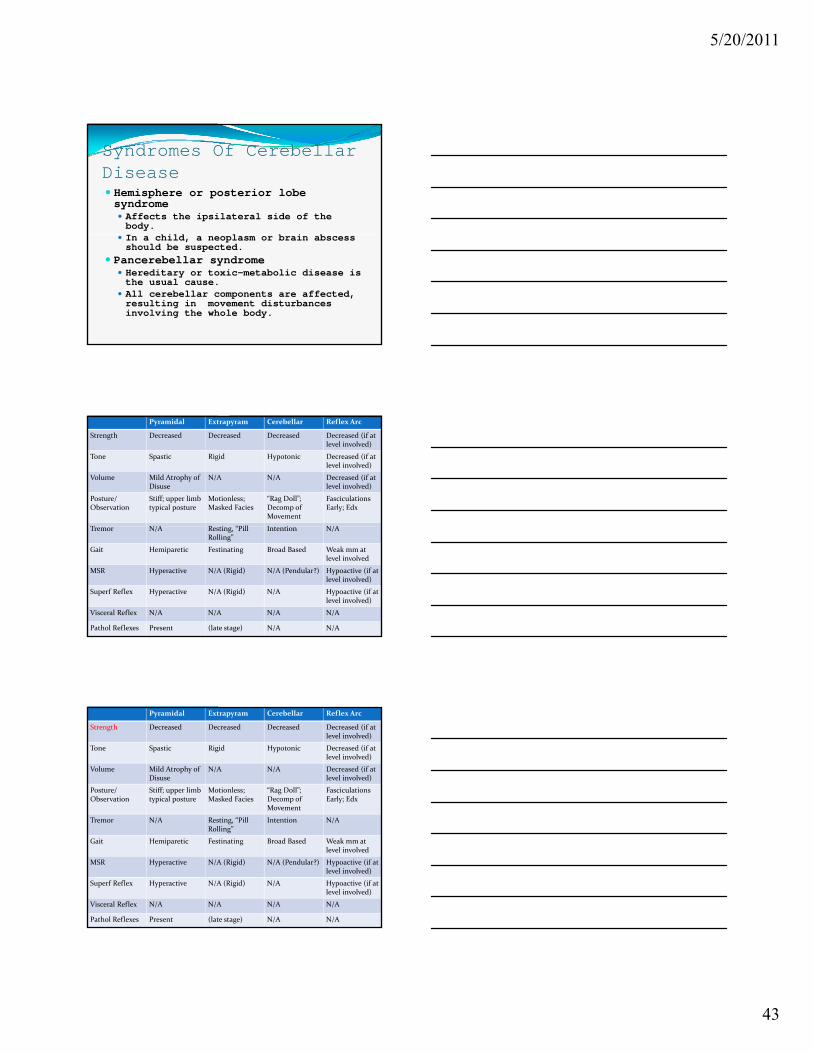
Syndromes Of Cerebellar Disease Hemisphere or posterior lobe syndrome Affects the ipsilateral side of the body.
hild l b i b In a child, a neoplasm or brain abscess should be suspected.
Pancerebellar syndrome Hereditary or toxic-metabolic disease is the usual cause.
All cerebellar components are affected, resulting in movement disturbances involving the whole body.
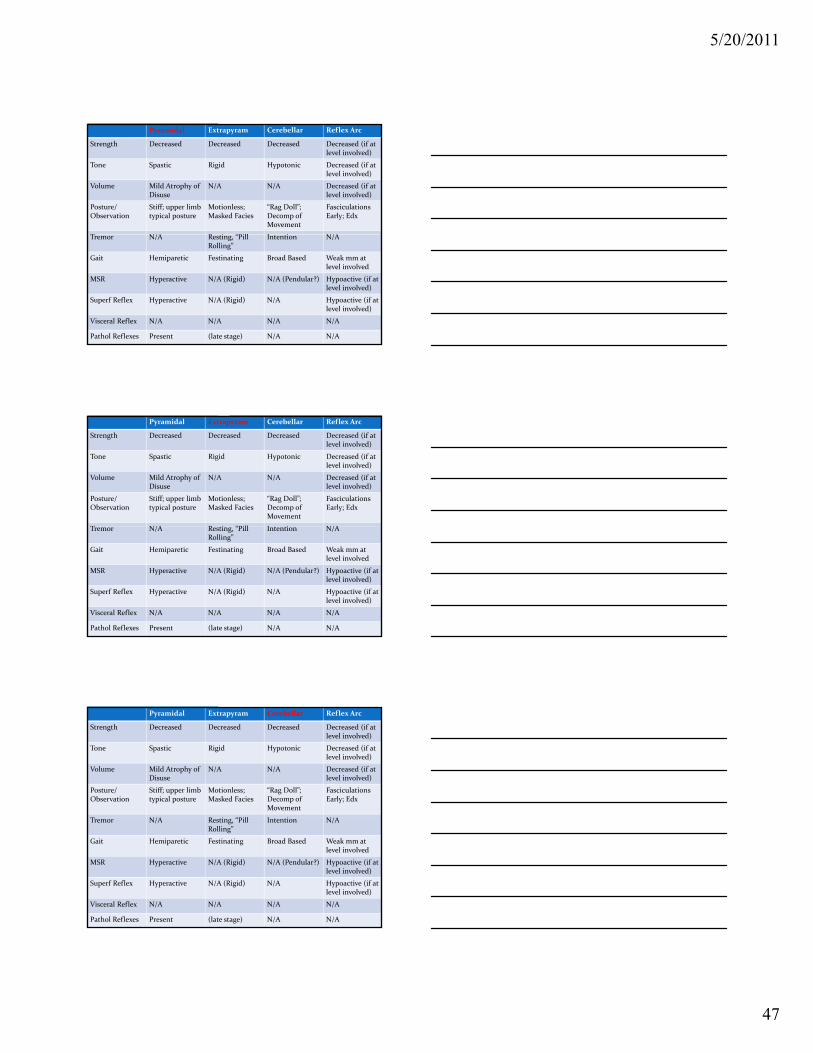
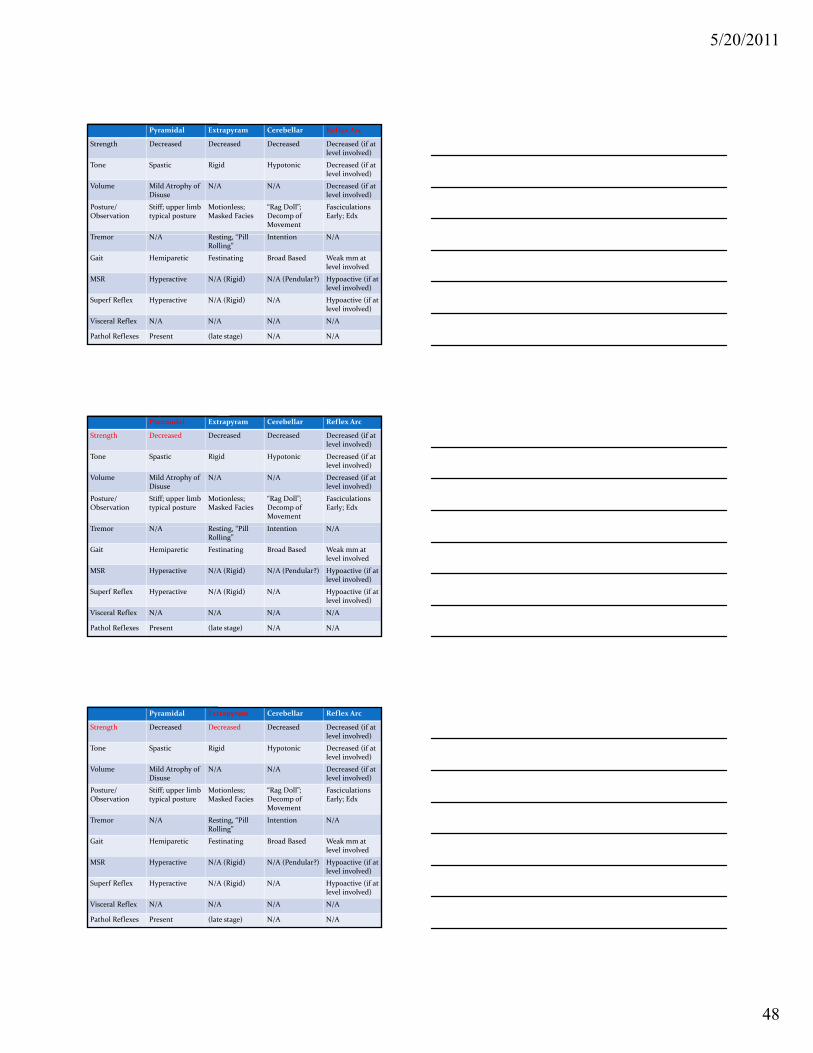
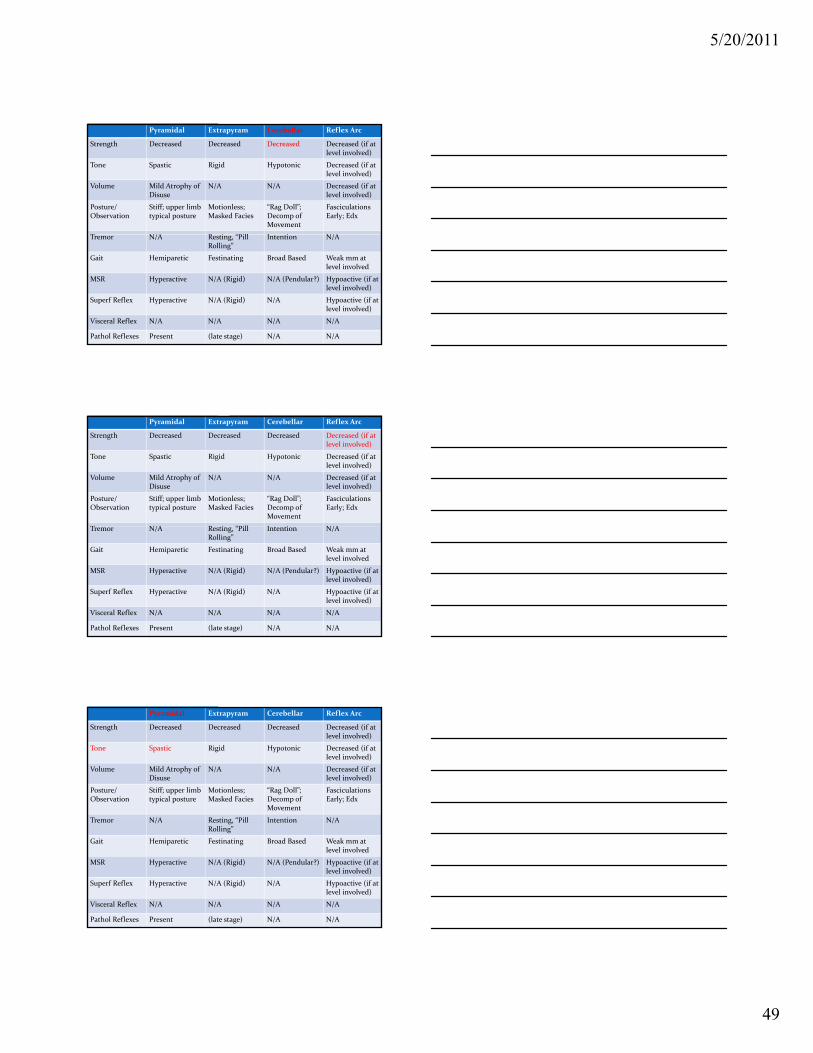
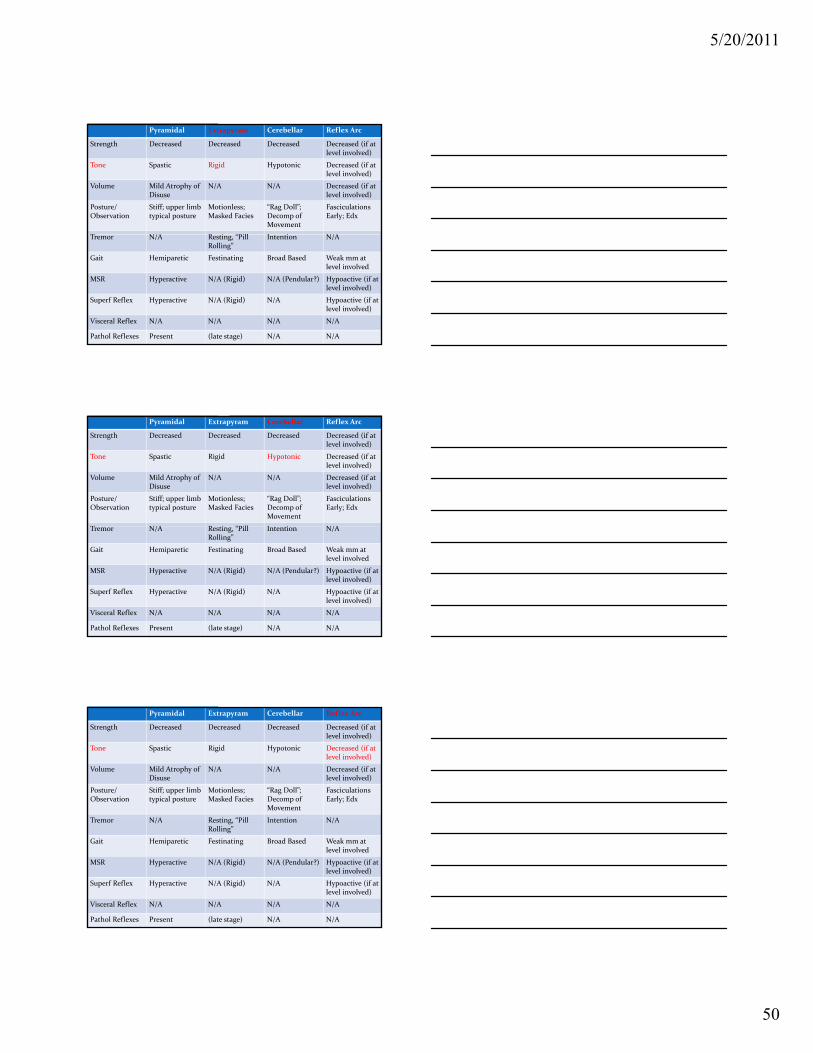
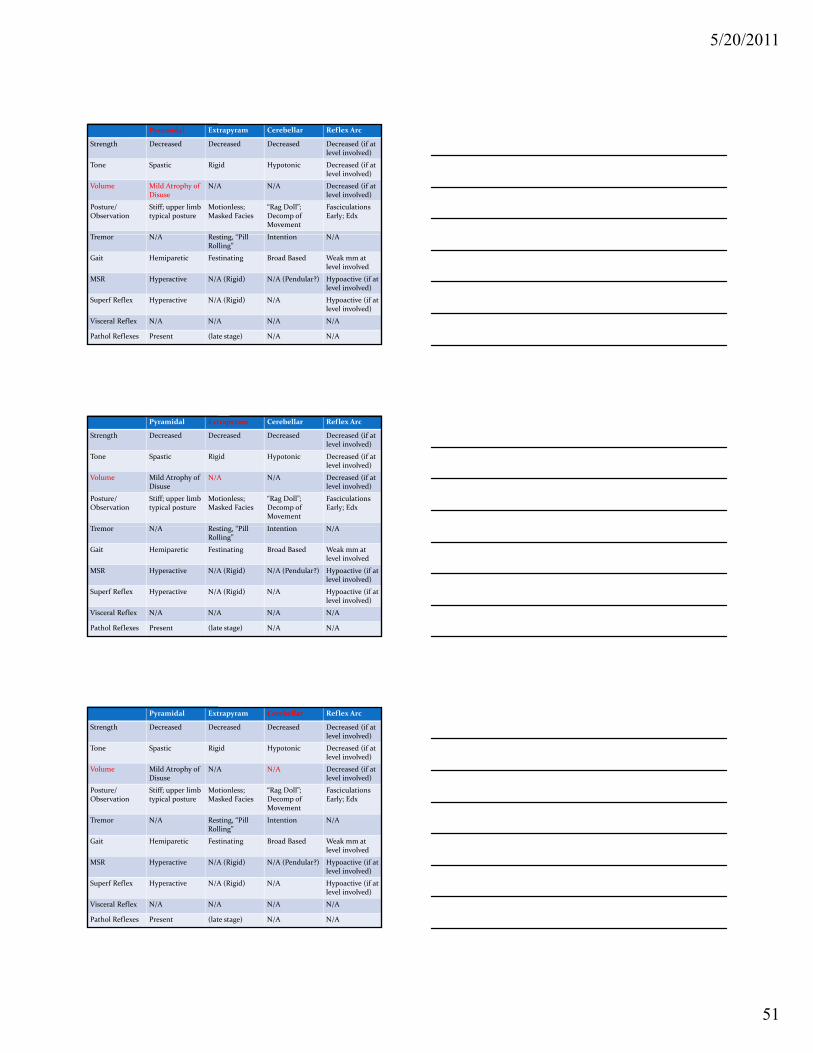
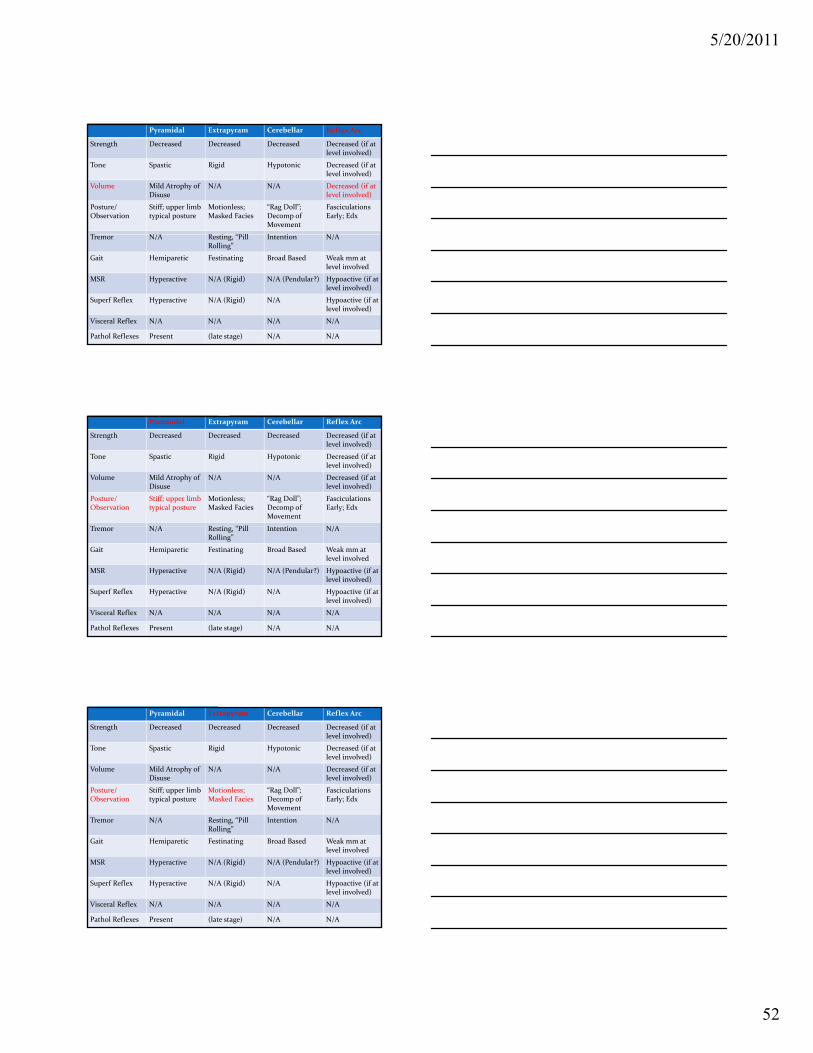
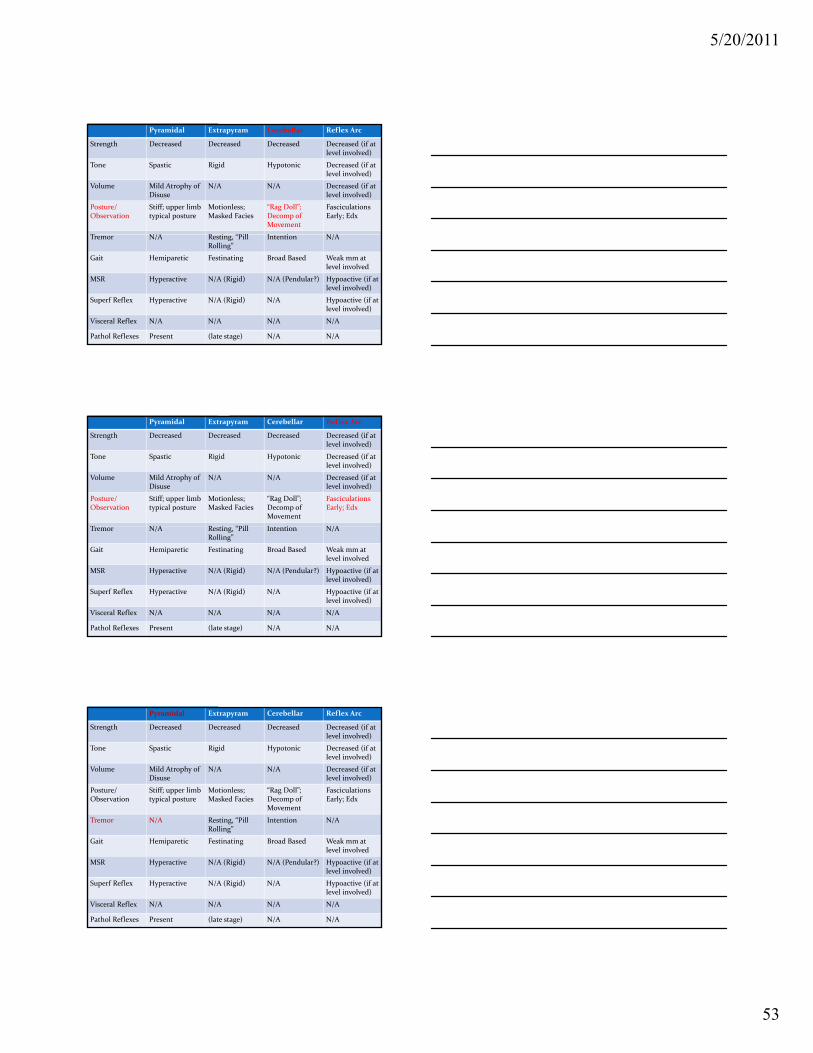
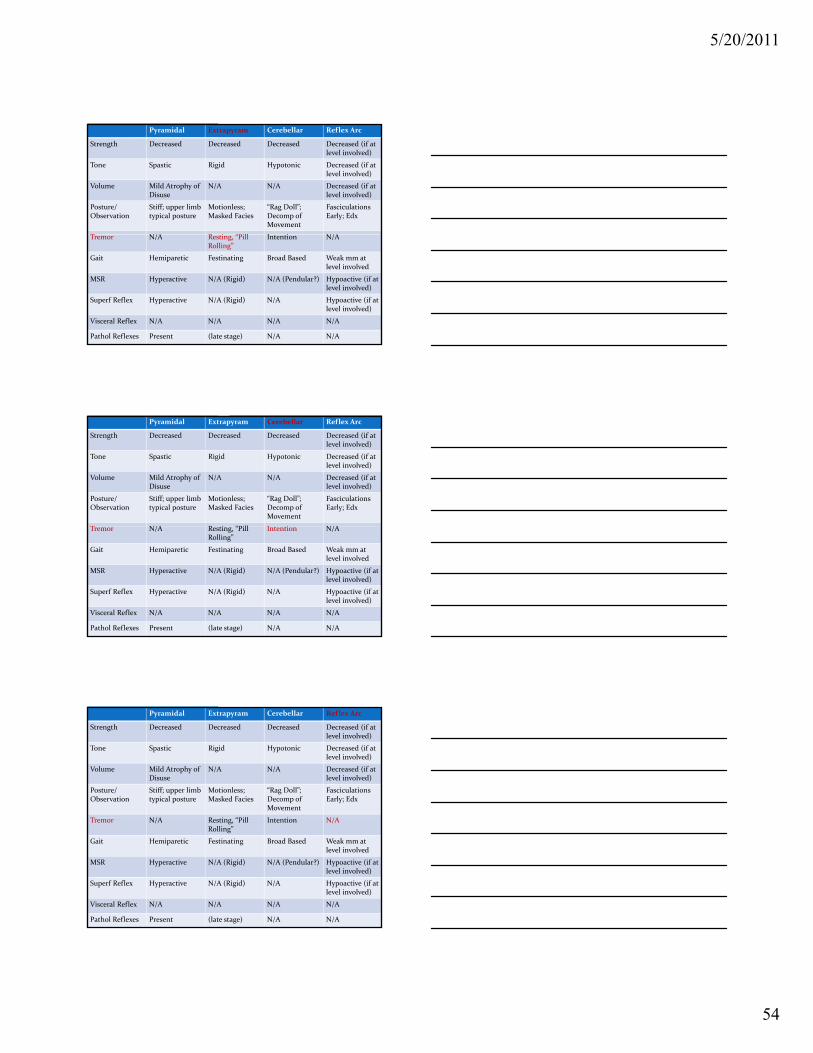
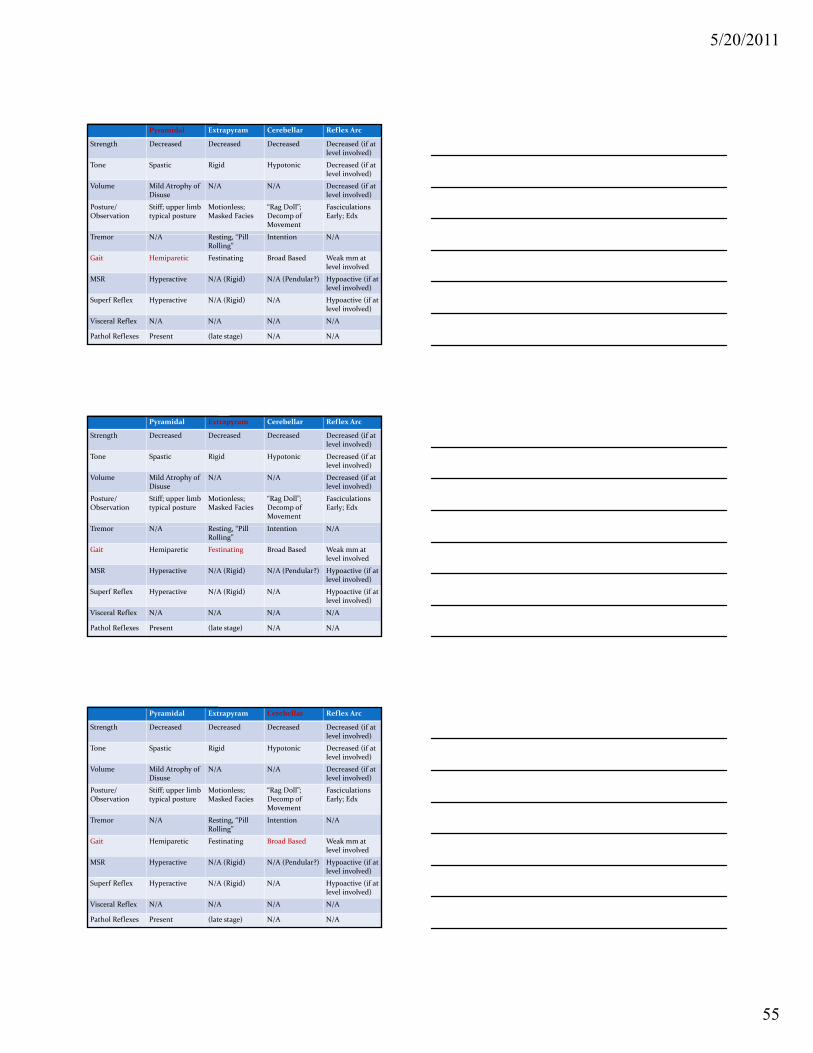
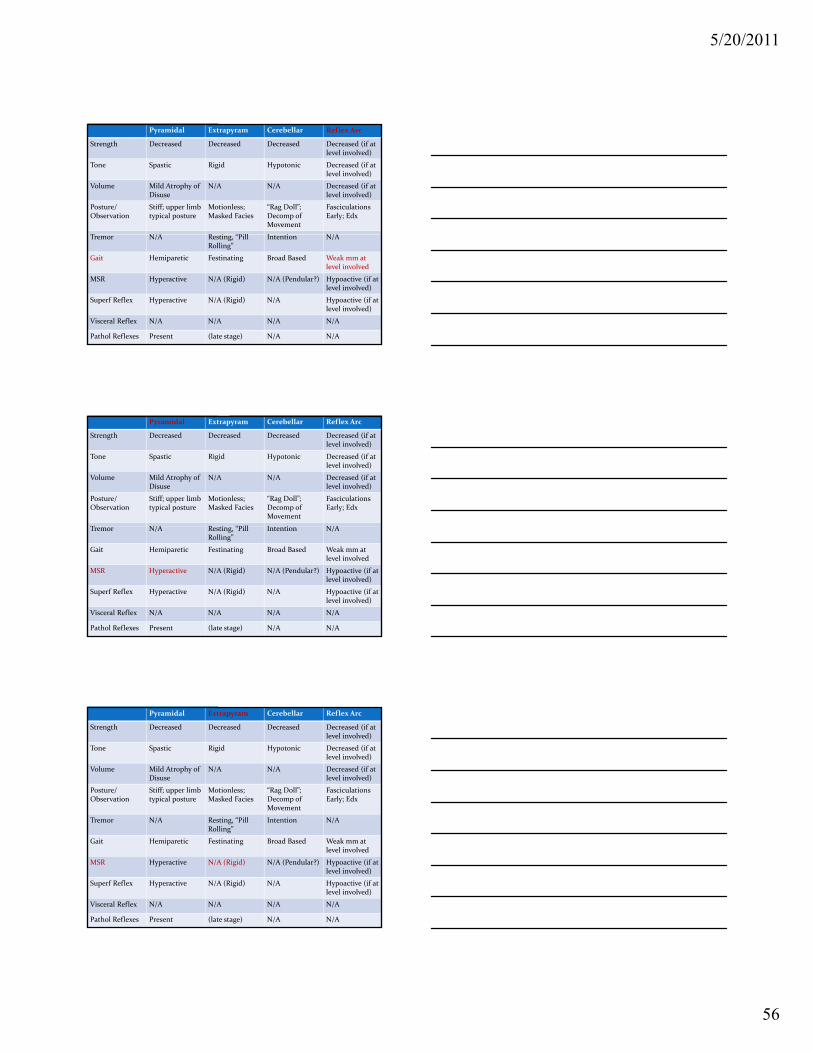
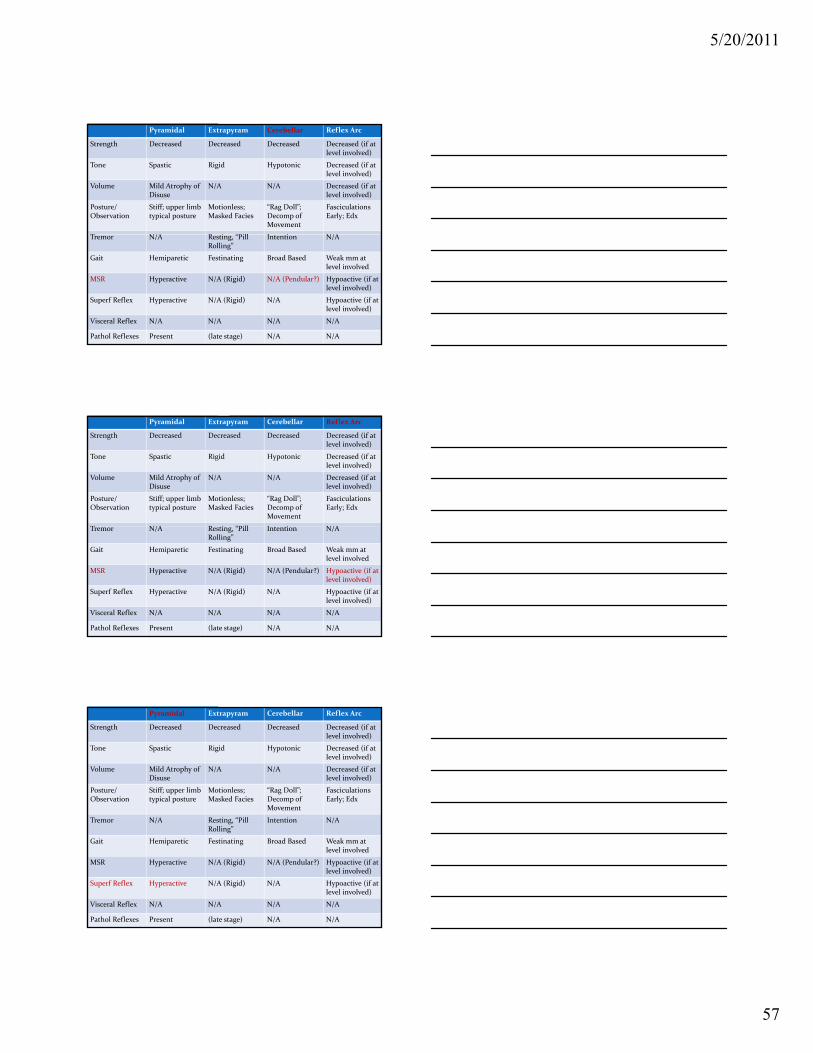
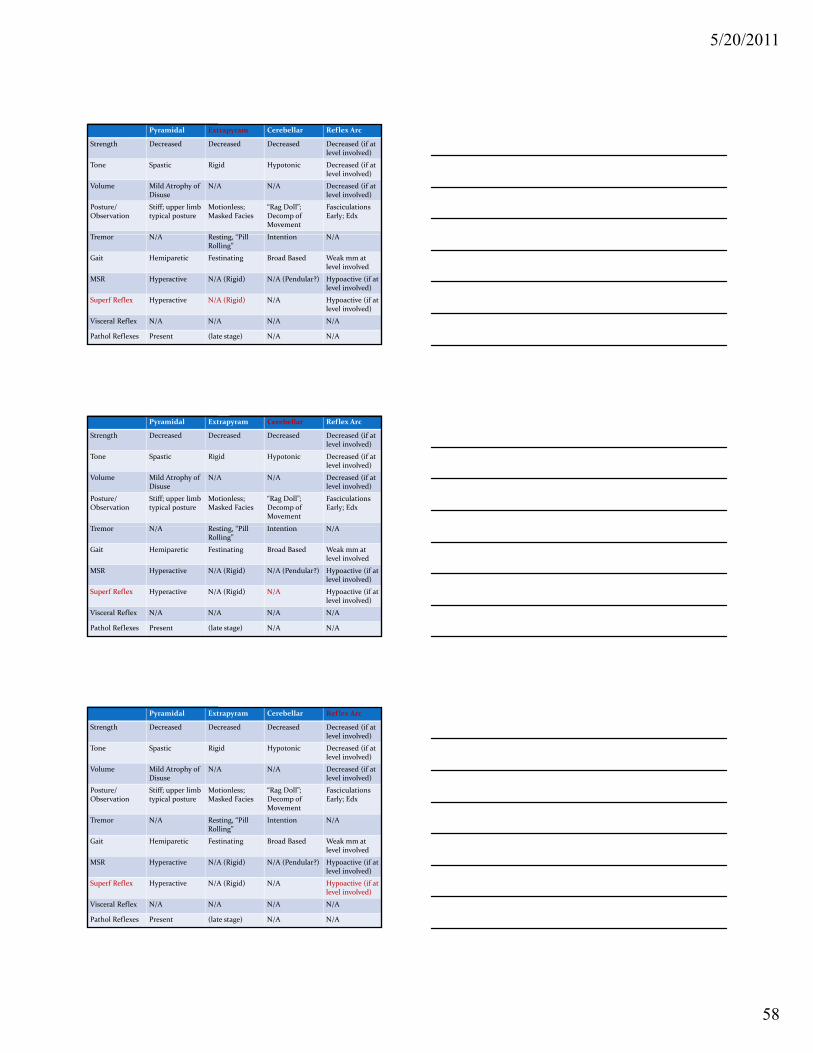
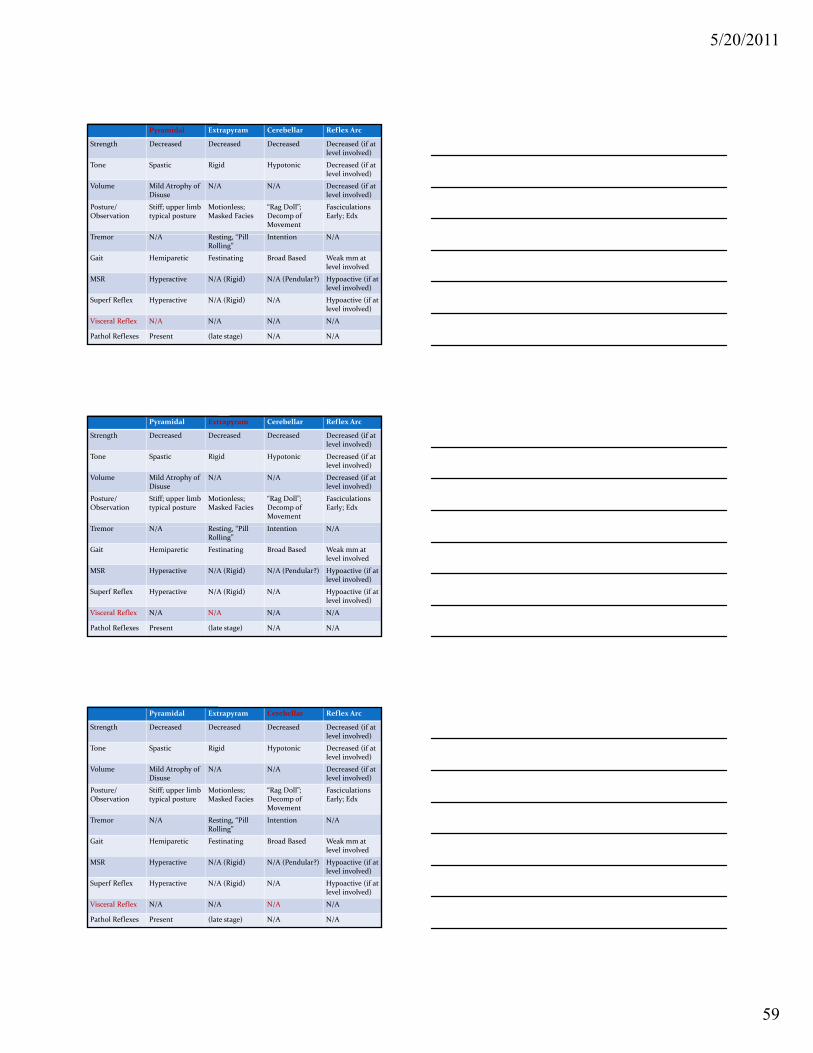
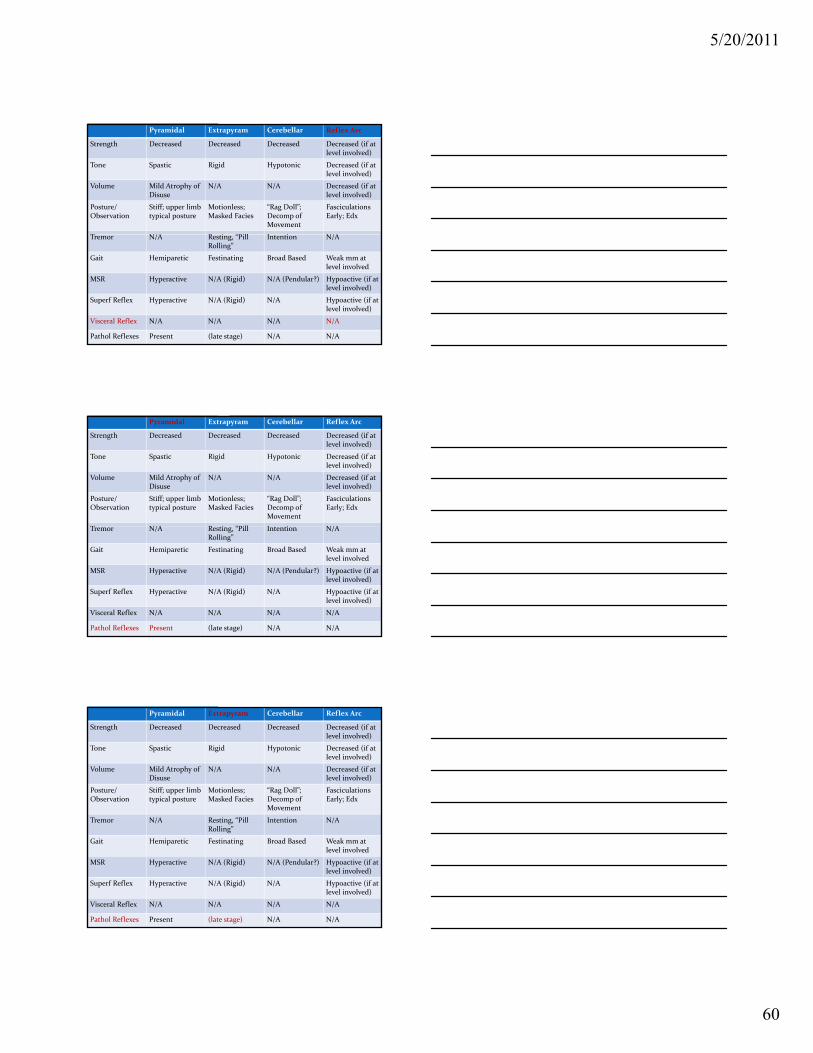
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
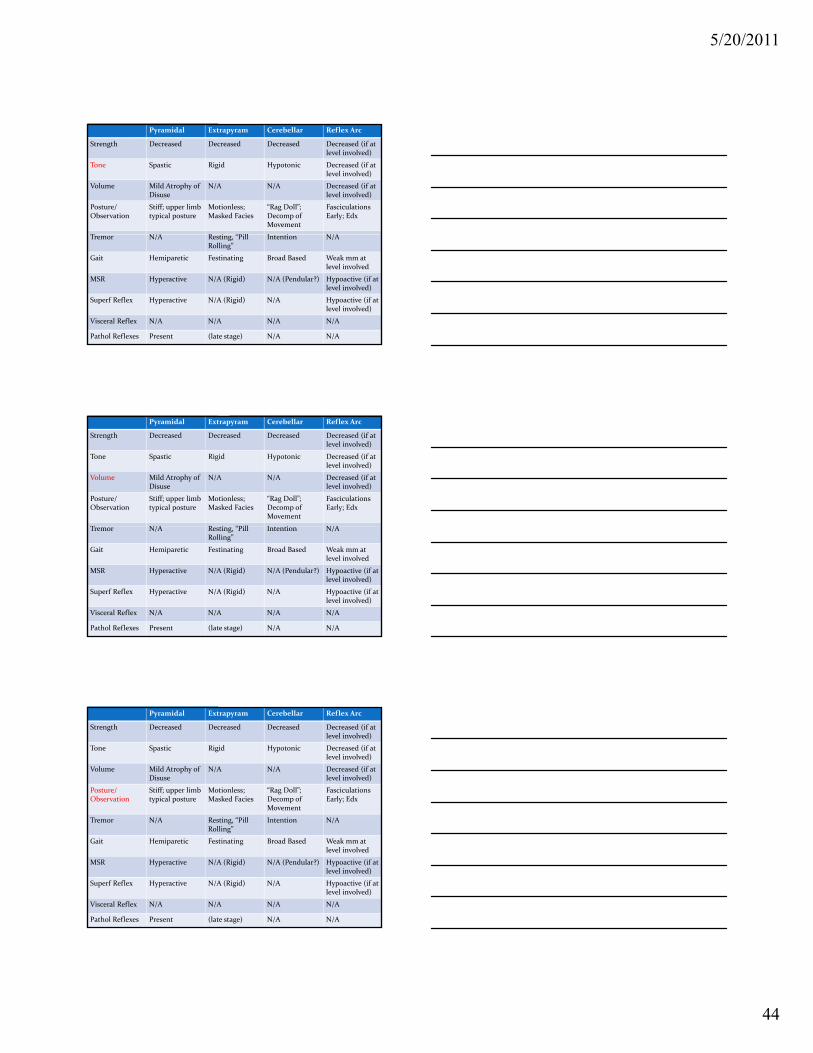
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
44
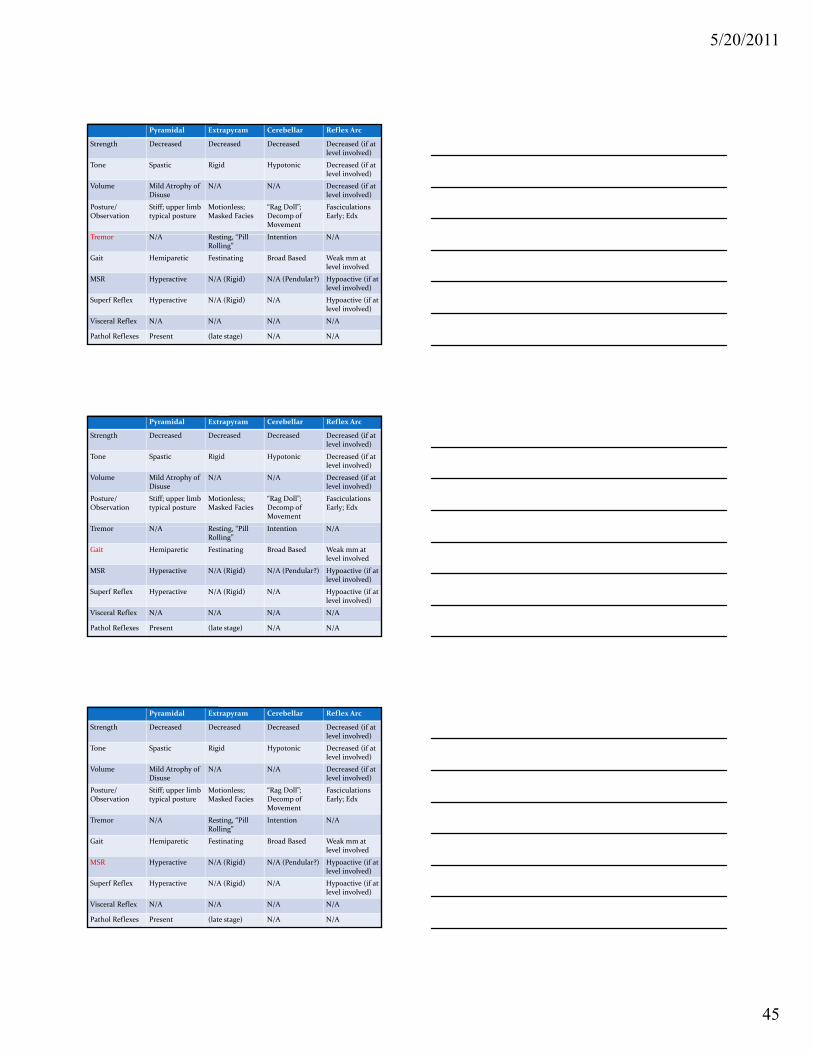
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
45
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
46
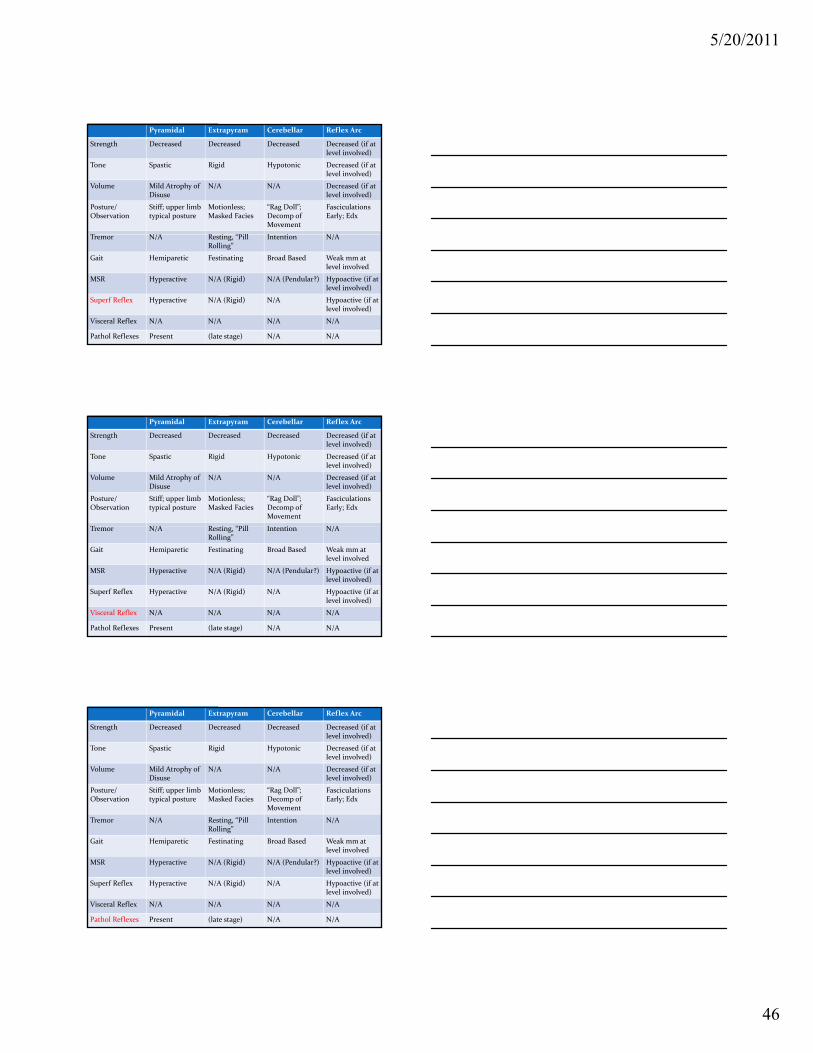
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
47
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
48
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
49
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
50
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
51
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
52
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
53
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
54
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
55
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
56
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
57
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
58
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
59
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
5/20/2011
60
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
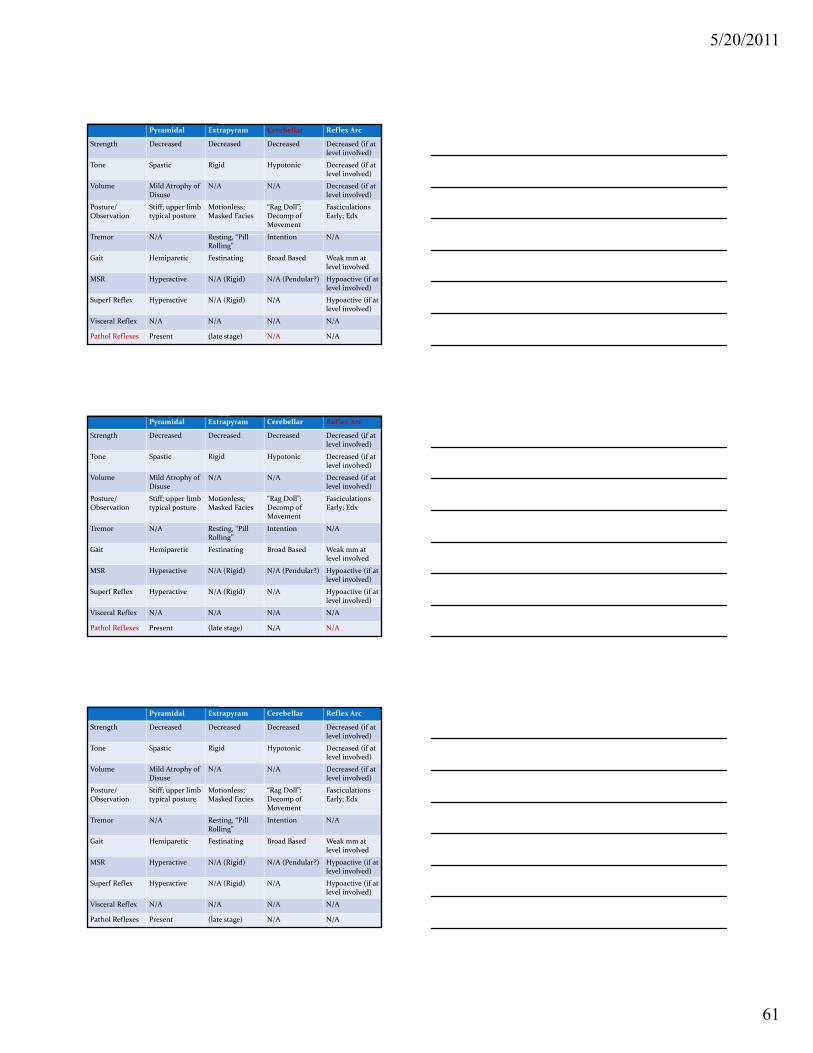
5/20/2011
61
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
Pyramidal Extrapyram Cerebellar Reflex Arc
Strength Decreased Decreased Decreased Decreased (if at level involved)
Tone Spastic Rigid Hypotonic Decreased (if at level involved)
Volume Mild Atrophy of Disuse
N/A N/A Decreased (if at level involved)
Posture/Observation
Stiff; upper limb typical posture
Motionless; Masked Facies
“Rag Doll”; Decomp of Movement
Fasciculations Early; Edx
T N/A R i “Pill I i N/ATremor N/A Resting, “Pill Rolling”
Intention N/A
Gait Hemiparetic Festinating Broad Based Weak mm at level involved
MSR Hyperactive N/A (Rigid) N/A (Pendular?) Hypoactive (if at level involved)
Superf Reflex Hyperactive N/A (Rigid) N/A Hypoactive (if at level involved)
Visceral Reflex N/A N/A N/A N/A
Pathol Reflexes Present (late stage) N/A N/A
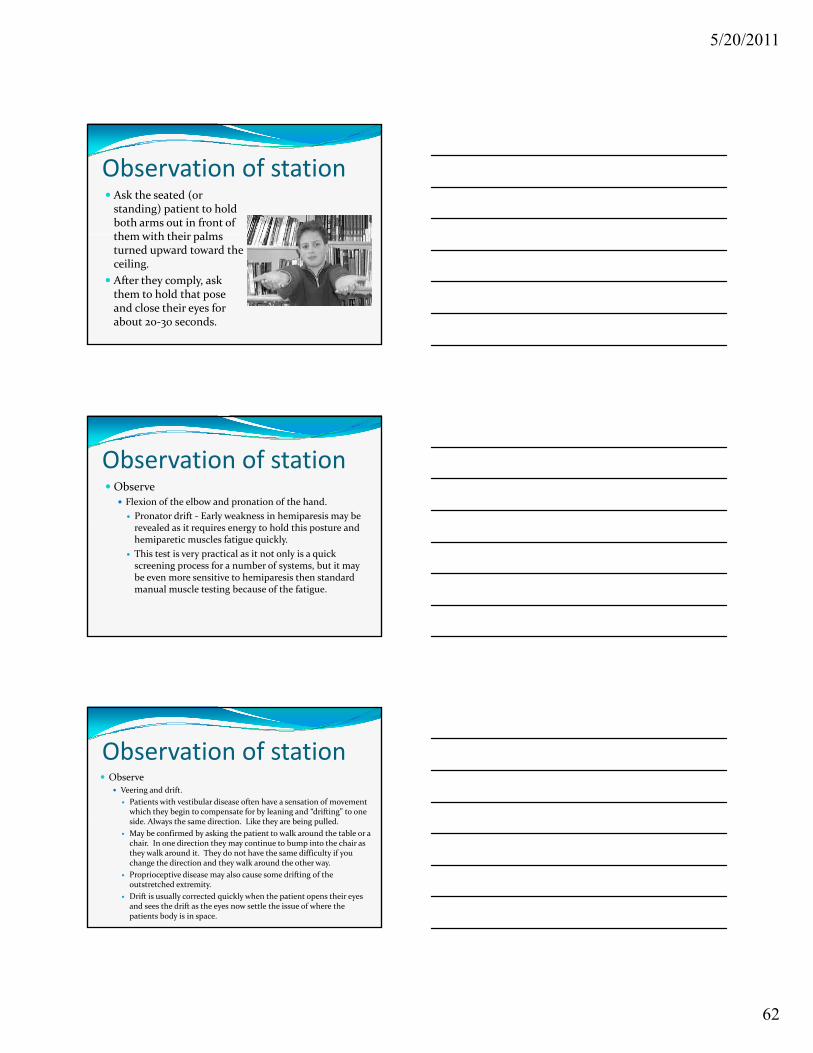
5/20/2011
62
Observation of station Ask the seated (or standing) patient to hold both arms out in front of th ith th i l them with their palms turned upward toward the ceiling.
After they comply, ask them to hold that pose and close their eyes for about 20‐30 seconds.
Observation of stationObserve
Flexion of the elbow and pronation of the hand.
Pronator drift ‐ Early weakness in hemiparesis may be l d it i t h ld thi t d revealed as it requires energy to hold this posture and
hemiparetic muscles fatigue quickly.
This test is very practical as it not only is a quick screening process for a number of systems, but it may be even more sensitive to hemiparesis then standard manual muscle testing because of the fatigue.
Observation of station Observe
Veering and drift.
Patients with vestibular disease often have a sensation of movement which they begin to compensate for by leaning and “drifting” to one side. Always the same direction. Like they are being pulled.
May be confirmed by asking the patient to walk around the table or a chair. In one direction they may continue to bump into the chair as they walk around it. They do not have the same difficulty if you change the direction and they walk around the other way.
Proprioceptive disease may also cause some drifting of the outstretched extremity.
Drift is usually corrected quickly when the patient opens their eyes and sees the drift as the eyes now settle the issue of where the patients body is in space.
5/20/2011
63
Observation of station Observe
Veering and drift
In proprioceptive disease the extremity may drift but it is not quite the same as the veering which involves both extremities quite the same as the veering which involves both extremities as well as the trunk.
You may differentiate by testing proprioceptive function in the extremity separately. A simple method of doing this is to grab one of the patients upper extremities and with the patients eyes closed elevate the extremity and bend it into a certain position. Ask the patient to move the other extremity into the same position. This rapidly checks both sides proprioceptive function.
Observation of station Observe
Drift or veering.
If one extremity drifts up and laterally, it may be a problem with one of the cerebellar hemispheres. Observe for intention
d f h b ll h fi tremor and perform other cerebellar tests such as finger to nose for confirmation.
Placing the head and neck in various positions, particularly rotation or extension rotation, while doing this test, may cause drift in vertebral artery disease; particularly in cases of where it is cervical spondylosis compressing the vertebral arteries.
Asking the patient to shake their head in a “no” fashion may cause some drift in cervicogenic disequilibrium due to confusion from cervical proprioceptors.
Patient Video VignettesCases with various normal and abnormal gait examples.
ObserveObserve
doctor/patient interaction.
Patient exam performance.
5/20/2011
64
Discussion Was the gait normal?
What did you notice?
No.
Foot drop.
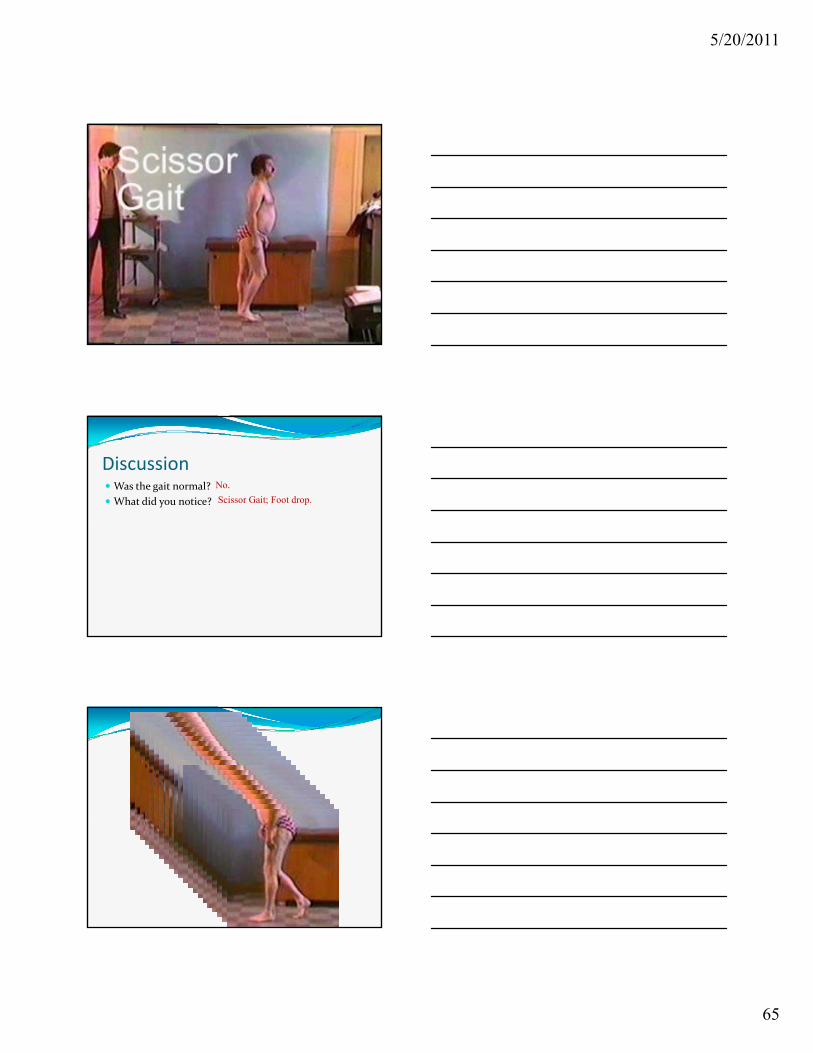
5/20/2011
65
Discussion Was the gait normal?
What did you notice?
No.
Scissor Gait; Foot drop.
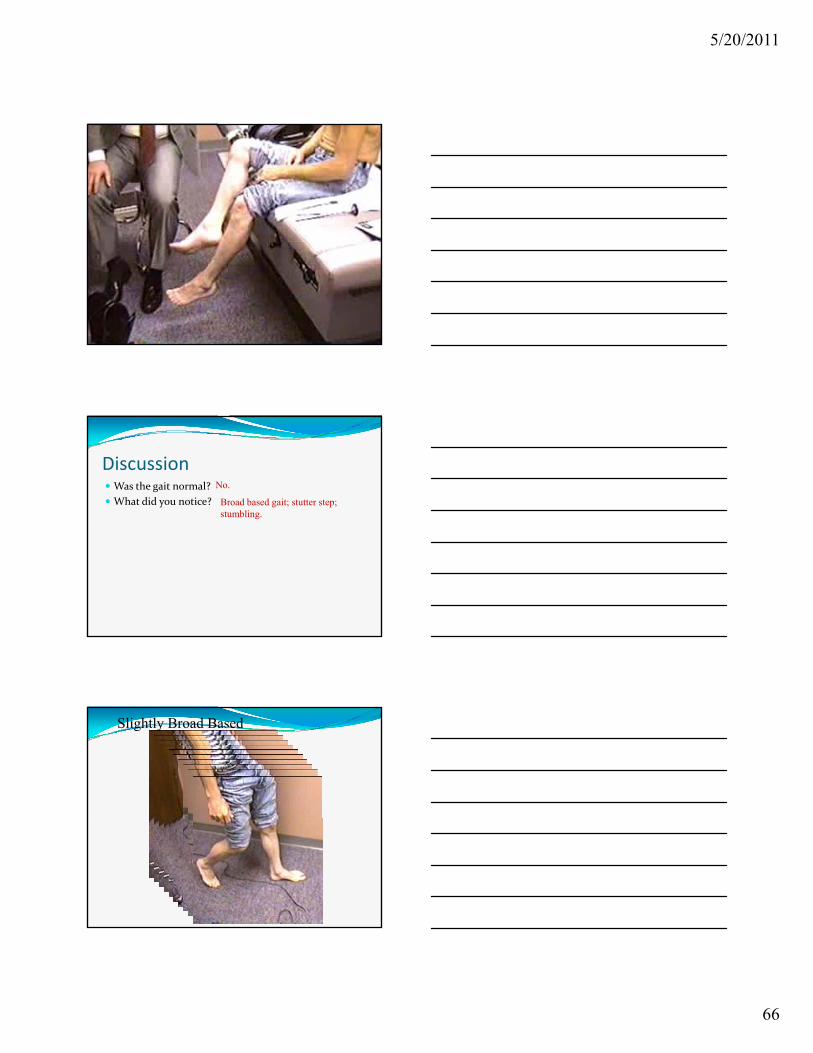
5/20/2011
66
Discussion Was the gait normal?
What did you notice?
No.
Broad based gait; stutter step; stumbling.
Slightly Broad Based
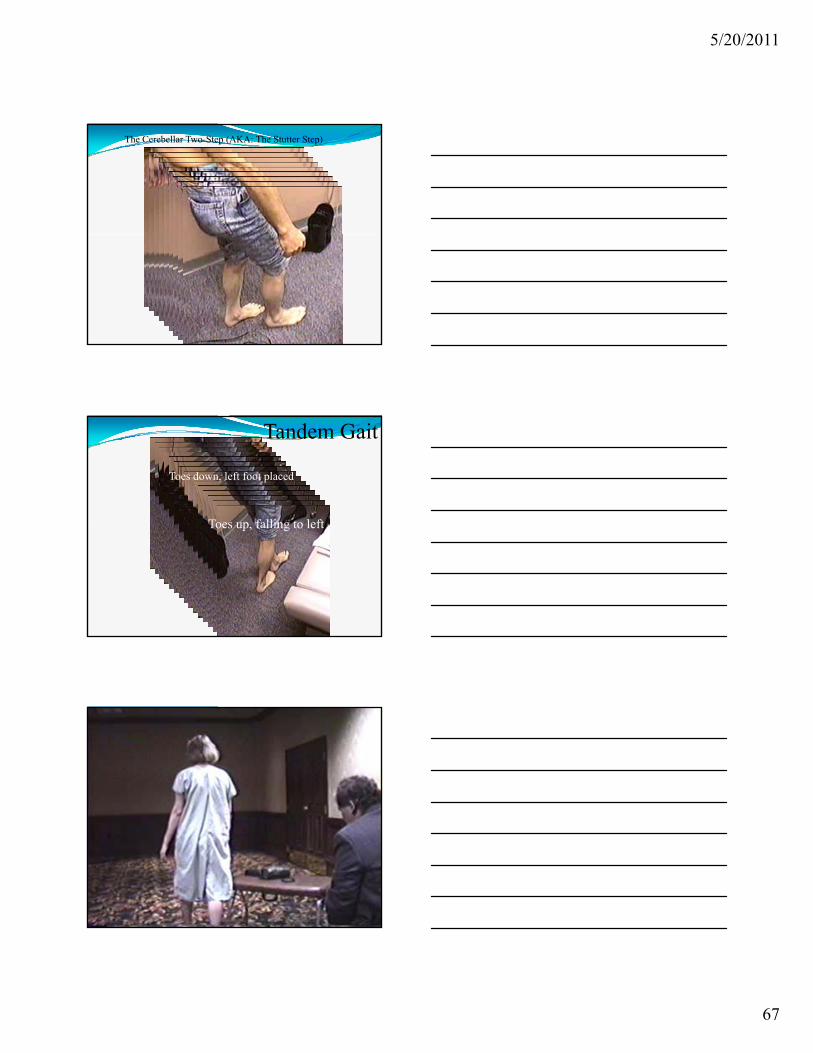
5/20/2011
67
The Cerebellar Two-Step (AKA: The Stutter Step)
Toes up falling to left
Toes down, left foot placed
Tandem Gait
Toes up, falling to left
Hysterical Gait ‐ Ataxia
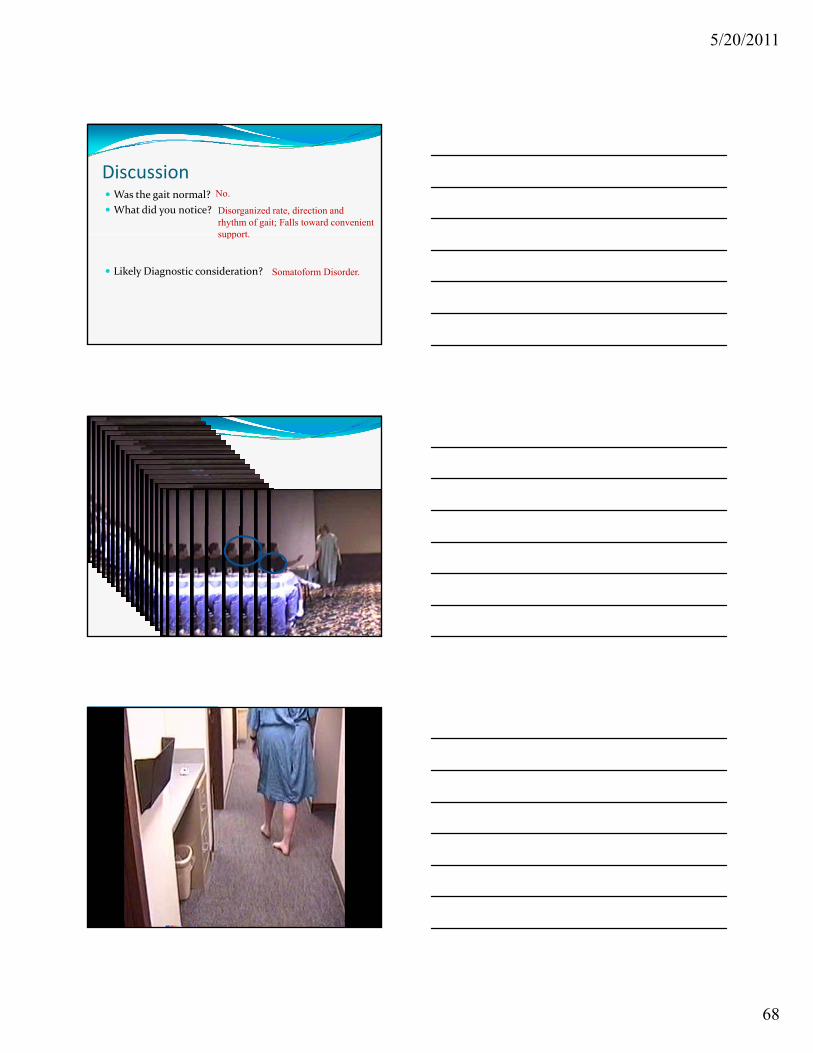
5/20/2011
68
Discussion Was the gait normal?
What did you notice?
No.
Disorganized rate, direction and rhythm of gait; Falls toward convenient support
Likely Diagnostic consideration?
support.
Somatoform Disorder.
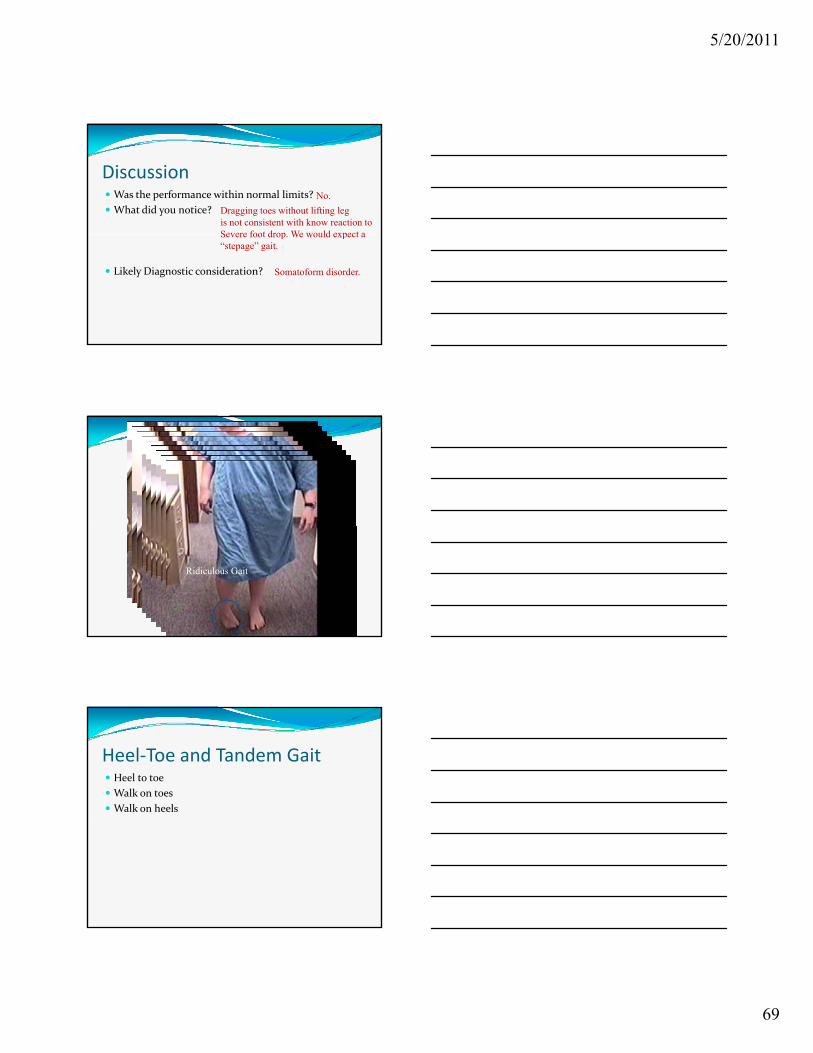
5/20/2011
69
Discussion Was the performance within normal limits?
What did you notice?
No.
Dragging toes without lifting legis not consistent with know reaction to Severe foot drop We would expect a
Likely Diagnostic consideration?
Severe foot drop. We would expect a “stepage” gait.
Somatoform disorder.
Ridiculous Gait
Heel‐Toe and Tandem Gait Heel to toe
Walk on toes
Walk on heels
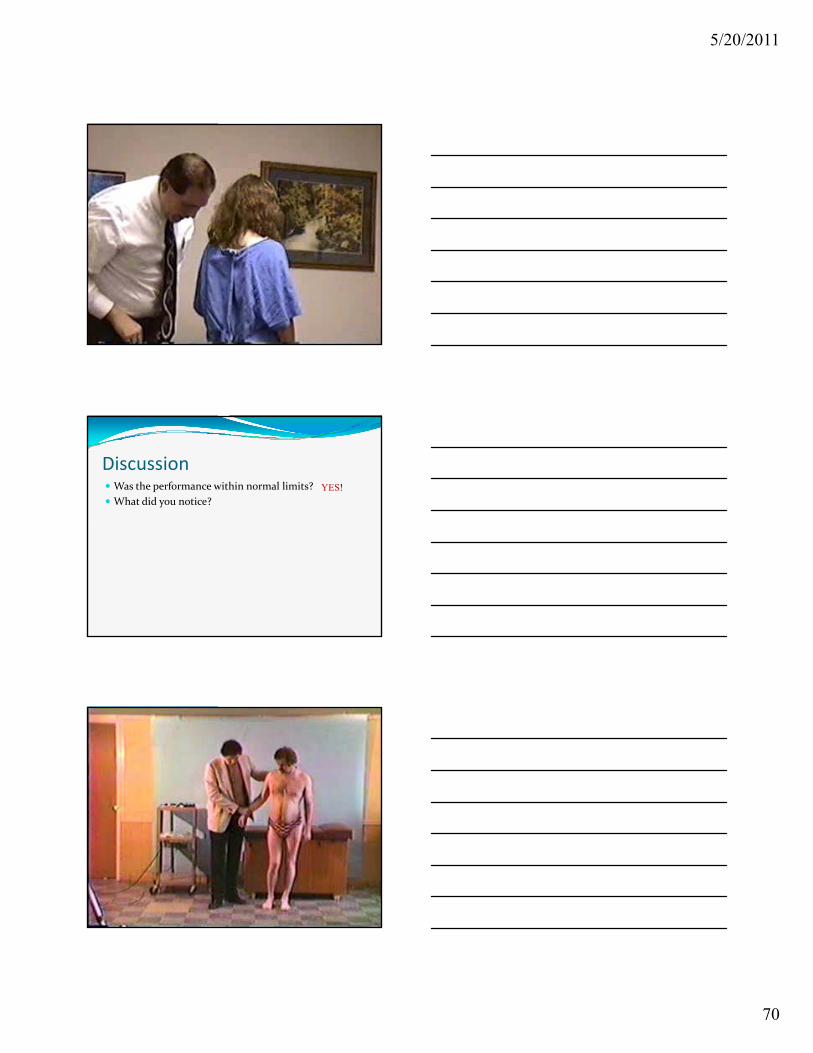
5/20/2011
70
Discussion Was the performance within normal limits?
What did you notice?
YES!
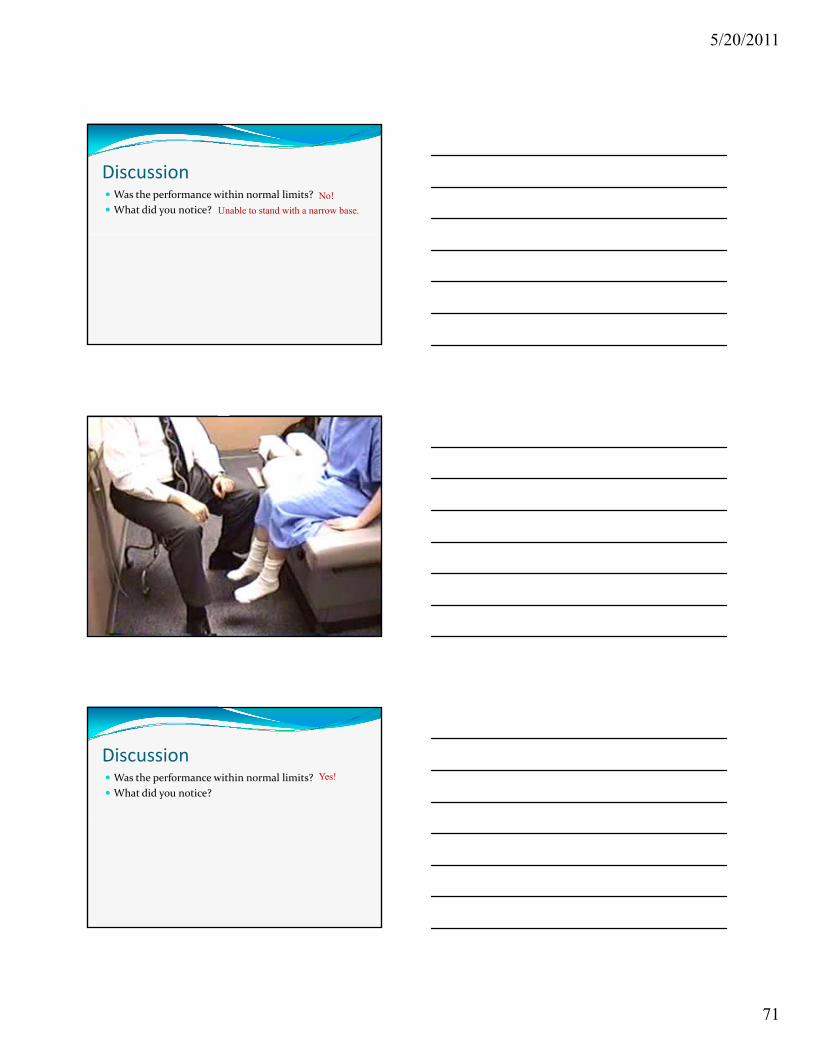
5/20/2011
71
Discussion Was the performance within normal limits?
What did you notice?
No!
Unable to stand with a narrow base.
Discussion Was the performance within normal limits?
What did you notice?
Yes!
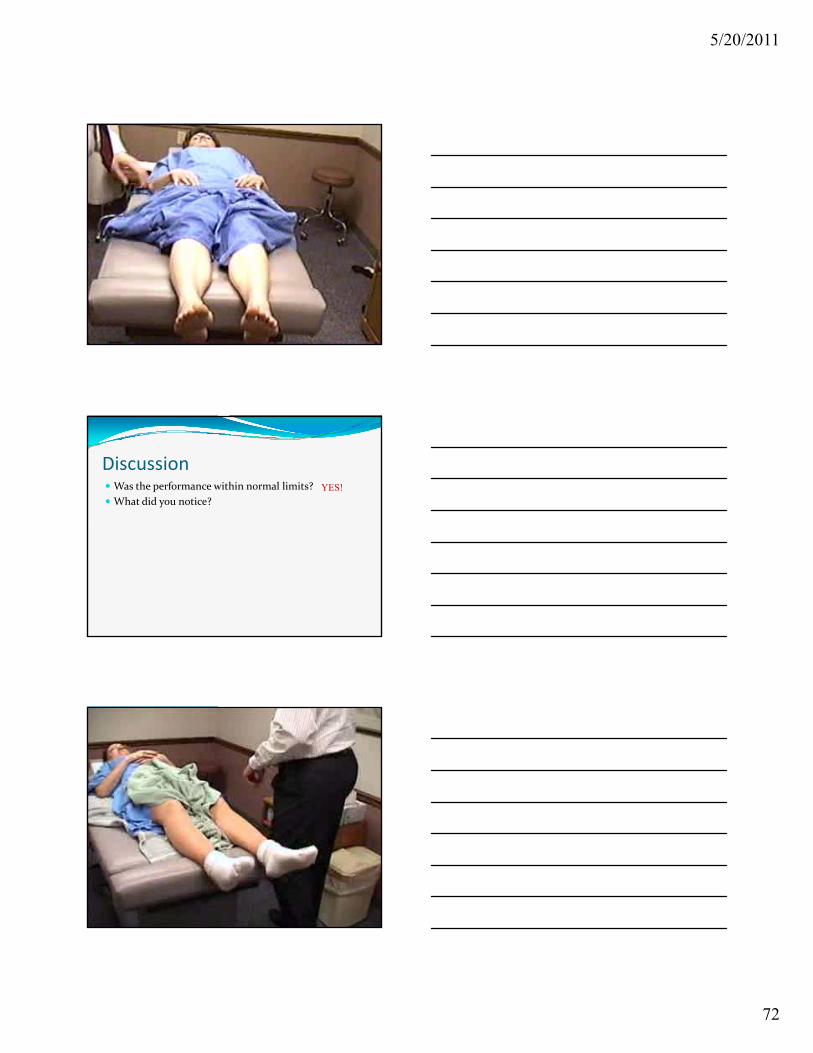
5/20/2011
72
Discussion Was the performance within normal limits?
What did you notice?
YES!
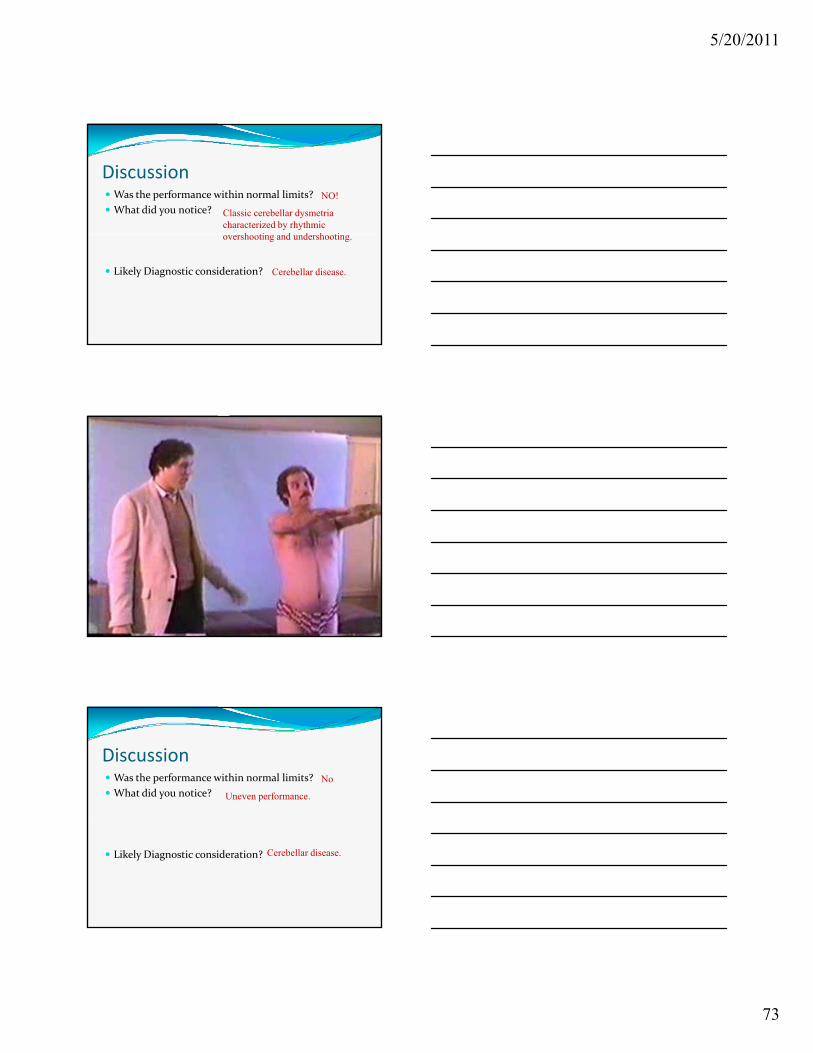
5/20/2011
73
Discussion Was the performance within normal limits?
What did you notice?
NO!
Classic cerebellar dysmetria characterized by rhythmic
h ti d d h ti
Likely Diagnostic consideration?
overshooting and undershooting.
Cerebellar disease.
Discussion Was the performance within normal limits?
What did you notice?
No
Uneven performance.
Likely Diagnostic consideration? Cerebellar disease.
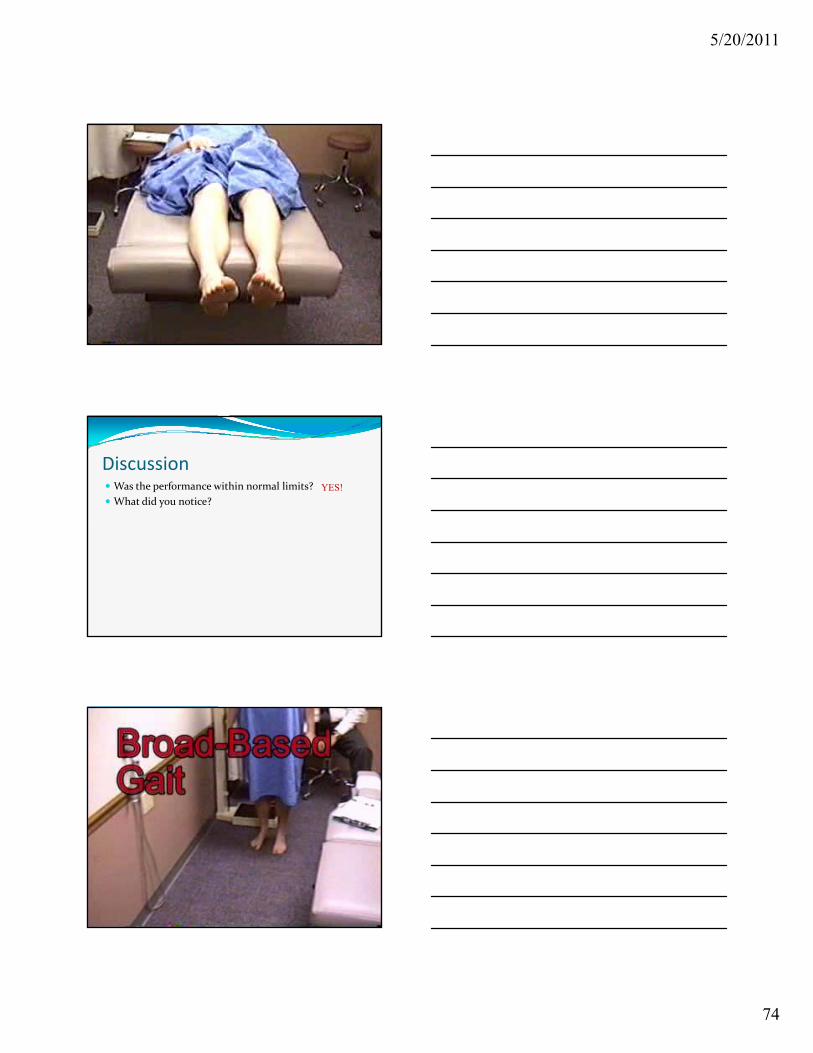
5/20/2011
74
Discussion Was the performance within normal limits?
What did you notice?
YES!
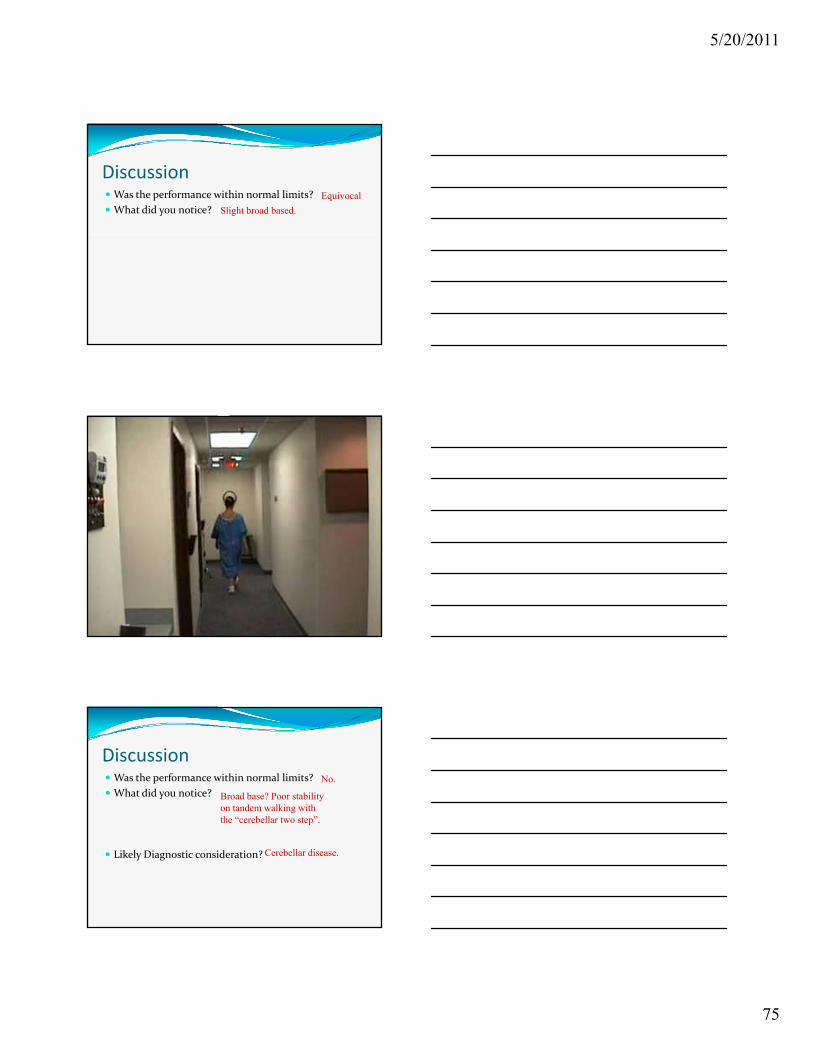
5/20/2011
75
Discussion Was the performance within normal limits?
What did you notice?
Equivocal
Slight broad based.
Discussion Was the performance within normal limits?
What did you notice?
No.
Broad base? Poor stability on tandem walking with th “ b ll t t ”
Likely Diagnostic consideration?
the “cerebellar two step”.
Cerebellar disease.
5/20/2011
76
Balance step
Heel strike
Presented By:
Joseph S. Ferezy, D.C.
Examination of station and gait Routine part of examination.
Disorders affecting balance and movement can be challenging due to complex sensory and motor systems interactionssystems interactions.
When any of these systems fail the nervous system displays predictable deficits.
Recognizing and testing the nervous system reveals these deficits and is a pre‐requisite to arriving at a diagnosis which is a pre‐requisite for proper management.