-
7/30/2019 Obat Pada Anak2
1/8
Oral Lichenoid Drug Eruption: A Report of aPediatric Case and
Review of the Literature
Victoria Woo, D.D.S.,* Julia Bonks, D.M.D., Lyubov Borukhova,
D.M.D.,
and David Zegarelli, D.D.S.
*School of Dental Medicine, University of Nevada, Las Vegas,
Nevada, Columbia University College of Dental
Medicine, New York, New York
Abstract:Lichenoid drug eruptions are seen most frequently on
the
skin and seldomly affect the mucosal surfaces. Oral
involvementknown as
oral lichenoid drug eruptionis more common in the adult
population and
has been associated with numerous medications. Pediatric-onset
oral lich-
enoid drug eruption is an exceptionally rare finding with only
isolated cases
published in the literature. The nonspecific appearance and
latent presen-
tation of pediatric oral lichenoid drug eruption can cause
confusion in
diagnosis and treatment. We report a case of oral lichenoid drug
eruption
occurring in a 15-year-old and explore challenges in the
clinical and histo-
logic recognition of this condition.
Drug eruptions represent a spectrum of cutaneous
and mucosal changes related to oral, parenteral, orinhaled
exposure to medications (1,2). The clinical pre-
sentation of drug eruptions is variable and may mimic
the immune-mediated mucosal diseases including lichen
planus, pemphigus vulgaris, mucous membrane pem-
phigoid, and lupus erythematosus (LE) (3). A well-
recognized form of chronic drug reaction is the lichenoid
drug eruption (LDE), which may manifest on the skin,
oral mucosa, or both sites (4); of the two, oral LDE
(OLDE) is less common than cutaneous LDE (57) and
may occur independently of skin lesions (4). The intra-
oral sites of predilection of OLDE include the posterior
buccal mucosa, tongue, floor of mouth, palate, and
alveolar ridges (810). There appears to be a preferencefor
unilateral distribution (1113). Clinically, lesions of
OLDE are morphologically identical to those of idio-
pathic oral lichen planus (OLP). They can exhibit a
classic reticular pattern or a predominantly erosive pat-
tern, depending on the drug implicated (14). Further-more,
thehistologic appearance andimmunologic profile
of drug-induced lichenoid lesions are nearly identical to
their idiopathic counterpart (6,1517).
Oral lichenoid drug eruptions have been reported in
association with an extensive list of medications. The
most commonly implicated drug classes include: peni-
cillamine (5,18), antimalarials (19), gold salts (5,12),
antihypertensives, including b-blockers (4,5,18,20,21)
and angiotensin inhibitors (5,6,2123), nonsteroidal
antiinflammatory drugs (5,24,25), and HIV medications
(5,26,27). The time from initial medication intake to
lesion appearance is variable, ranging from weeks to
months with an average delay in onsetof 23 months
(6).Demographically, OLDEs tend to be seen in adult
patients and are rare findings in the pediatric population
(7), which the authors consider to be patients 15 years of
Address correspondence to Victoria Woo, D.D.S.,
ColumbiaUniversityDivision of Oral Pathology, 630 W. 168th
Street,PH15W-1562 New York, NY 10032, or e-mail:
[email protected].
DOI: 10.1111/j.1525-1470.2009.00953.x
458 2009 The Authors. Journal compilation 2009 Wiley
Periodicals, Inc.
Pediatric Dermatology Vol. 26 No. 4 458464, 2009
-
7/30/2019 Obat Pada Anak2
2/8
age or younger. The disparity in prevalence is likely due
to the more frequent use of medications and to the
multiplicity of medications used in older individuals in
our older population. Moreover, the majority of medi-
cations associated with OLDE are used for the treatment
of predominantly adult-onset conditions (7).
In this article, we present a pediatric patient with
OLDE who demonstrated dramatic improvement on
discontinuation of his systemic medications.
CASE REPORT
A 15-year-old male was referred for evaluation of bilat-
eral buccal mucosal and tongue lesions of more than
1-yearduration.Thepatientreportedthathislesionswere
painful, particularly when exposed to certain foods and
liquids. A past medical history revealed that he was under
treatment by a psychiatrist for insomnia and mood
swings. His medications included risperidone (Risper-dal) and
carbamazepine (Tegretol), which he had been
taking for2 years. Further questioningrevealed no other
medical conditions, no family history of lichen planus
(LP), no history of hepatitis B vaccination, and no sig-
nificant exposure to cinnamon-containing products or
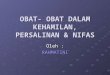
foodstuffs. On intraoral examination, erosivelesionswith
white striatedperipheral borderswereobserved involving
the right and left buccal mucosa (Fig. 1A) and lateral
tongue borders (Fig. 1B). The ulcers corresponded to the
occlusal planes, suggestive of a Koebner phenomenon. A
predominantly reticular lesion was also evident upon the
lower labial mucosa. There were no adjacent dental res-torations
and no cutaneous involvement was noted. The
clinical differentialdiagnosis includedOLP versus an oral
mucosal lichenoid reaction. A biopsy was performed of
the left buccal mucosa and revealed hyperparakeratosis
with an underlying lichenoid infiltrate containing scat-
tered neutrophils. Interface mucositis, characterized by
intraepitheliallymphocytic exocytosisandcolloidbodies,
was also evident (Fig. 2). A histopathologic diagnosis of
hyperkeratosis and lichenoid mucositis was made. The
patient was provided with a topical steroid mouthrinse
(dexamethasone suspension 0.5 mg5mL). On follow-up
2 weeks later the lesions were unchanged. An OLDE re-
lated to the patients medications was stronglysuspected.Upon
consultation with the patients psychiatrist, both
medications were stopped. On follow-up 1 month later,
the patient reported 100% subjective improvement in his
symptoms. Clinically, there was almost complete resolu-
tion of the ulcerations although residual white striations
were noted involving the right and left posterior buccal
mucosa (Fig. 3A). The bilateral tongue borders were
clinically normal (Fig. 3B). A drug re-challenge was
offered but refused by his parents due to discomfort
A
B
Figure 1. (A) Oral lichenoid eruption: Erosions associated
with white striations of left buccal mucosa. (B) Oral
lichenoideruption: Large erosion with white, striated periphery of
leftlateral tongue border.
Figure 2. Photomicrograph of oral biopsy demonstrating
alichenoid infiltrate with intraepithelial lymphocytes and
colloidbodies (hematoxylin and eosin, magnification 100).
Woo et al: Oral Lichenoid Drug Eruption 459
-
7/30/2019 Obat Pada Anak2
3/8
associated with his initial lesions. At 1-year follow-up,
there were persistent reticular lesions of the bilateral
buccal mucosa butno evidence of ulceration. The patient
has been placed on annual oral pathology recall and
continues to be followed closely by his psychiatrist.
DISCUSSION
Pediatric LDE is infrequent due to the relative uncom-
mon use of systemic medications in this age group. A
review of the current literature revealed several cases of
cutaneous LDE in children (28,29). However, reports of
OLDE are extremely rare and may be related to lack ofrecognition
or misdiagnosis as other clinical entities,
including idiopathic LP. We performed a Medline and
PubMed search for pediatric OLDE cases published in
the English-language literature andfound onlytwo cases,
presented in Table 1 (29,30). The patients listed in this
table fulfilled the criteria for OLDE, including a history
of systemic medication intake, clinical and histologic
evidence of lichenoid mucositis, and resolution of lesions
with drug cessation. It is noteworthy that formal analysis
of documented cases was often difficult due to a wide
variation in reporting techniques and diagnostic criteria.
A complete listing of OLDE-causing medicationsused in the
pediatric population is beyond the scope of
this paper. However, an abbreviated list is provided in
A
B
Figure 3. (A) Appearance of oral mucosa 1 month following
drug withdrawal: Residual white striations of left buccalmucosa.
(B) Appearance of oral mucosa 1 month followingdrug withdrawal:
Left lateral tongue border with no clinicalevidence of disease.
TABLE 1. Reported Cases of Pediatric Oral Lichenoid Drug
Eruption
AuthorNo.cases Agesex Drug implicated Site
Clinicalfeatures
Time onset*time resolve Comments
Ridola et al (29) 1 20 mosM Dactinomycin Lips, face trunk, limbs
Reticular,papular
12 d1 mo Topical steroids given;resolution despitecontinued
vincristine
Kanwar et al (30) 1 4 yrsM Dactinomycin Oral NS, axillae,
groinpubic region, chest
NS 7 d1 mo
Present case 1 15 yrsM Risperidone,carbamazepine
BM, tongue Erosive ?mo1 mo
*Time of lesional onset after drug administration, Time of
lesional resolution after drug withdrawal.M, male; NS, not
specified; BM, buccal mucosa.
TABLE 2. OLDE-Associated Systemic Medications Used inthe
Pediatric Population
Antianxietypsychotropic agents (clonazepam, diazepam,lorazepam,
temazepam, tricyclic antidepressants)
Antibiotics (tetracycline)Anticonvulsants (carbamazepine,
lorazepam, oxcarbazepine,
phenytoin, valproate sodium)Antidiabetics
(insulin)Antidiarrheals (bismuth)
Antinflammatory agents (aspirin, fenclofenac,
ibuprofen,naproxen, rofecoxib)
Antifungals (amphotericin B, ketoconazole)Antimalarials
(chloroquine, hydroxychloroquine, pyrimethamine,quinidine,
quinine)Antituberculosisantimycobacterial agents (isoniazid,
streptomycin, rifampin)Antiulcer agents (cimetidine, ranitidine,
omeprazole)Bipolar agents (lithium)Chemotherapeutic agents
(dactinomycin)Thyroid replacement agents (thyroxine)
OLDE, oral lichenoid drug eruption.
460 Pediatric Dermatology Vol. 26 No. 4 JulyAugust 2009
-
7/30/2019 Obat Pada Anak2
4/8
Table 2 (8,3134). Of note, several of these medications
have been implicated in both oral and cutaneous
lichenoid eruptions.
The diagnosis of OLDE may be challenging due to its
nonspecific clinical findings and rarity in the pediatric
population. A clear temporal relationshipbetween lesion
onset and drug intake is not always obvious due to
variable latent periods, which ranges from an average of
12 months (29) to reportedly 2 years in duration
(6,24,35,36). Therefore, extended latency from initial
drug exposure does not preclude thediagnosis of OLDE.
Furthermore, oral lesions have presented after medica-
tion withdrawal in exceptional cases (37). In this setting,
a high index of clinical suspicion is required to prompt
evaluation of a drug-inducedetiology. Lastly, identifying
the causal agent can also become problematic in patients
taking multiple medications, although the most recently
administered drug should be suspected first.
Further complicating the diagnosis of OLDE is thewide array of
oral conditions that can present with lich-
enoid-appearing lesions. The differential diagnosis for
OLDE in a child should include OLP, lichenoid amal-
gam reaction, and cinnamon stomatitis; less likely con-
siderations include lesions of LE, oral manifestations of
chronic graft-versus-host disease, and erythema multi-
forme. The latter five conditions can be excluded by
evaluating the following: direct contact with amalgam
restorations,exposure to cinnamon containing products;
systemic involvement and positive serologic tests for LE;
history of bone marrow transplant; and characteristic
clinical findings such as hemorrhagic crusted lips andtarget
skin lesions (Table 3) (8,12). Hepatitis B vaccina-
tion (3840) and liver disorders, such as chronic active
hepatitis (41), have also been associated with oral
lichenoid lesions but can be appropriately eliminated
during history taking. Therefore, the main diagnostic
dilemma involves differentiating OLDE from OLP, the
latter being a rare but documented condition in children
(4246). Clinical, microscopic, and immunologic simi-
larities make distinction between OLDE and OLP diffi-
cult if not impossible in certain cases. This is
compounded by the lack of clearly defined and stan-
dardized criteria in the diagnosis of OLDE. Attempts at
identifying histologic features specific to OLDE have
been met with variable success. Purported histologic
features favoring the diagnosis of OLDE include a deep
and diffuse subepithelial infiltrate composed of
lymphocytes, plasma cells, neutrophils with or without
eosinophils; perivascular inflammation; and intraepi-
thelial colloid bodies (4,12,13,15,4749). However, most
authors agree that these findings are not exclusive to
OLDE and can also be seen in OLP as well as other
mucocutaneous conditions (e.g., discoid LE) (15,47,50).
In contrast to traditional histology, immunofluorescenceanalysis
may be of help in distinguishing OLDE from
OLP. While both conditions show similar findings on
direct immunofluorescence studiesnamely, a shaggy
deposition of fibrinogen along the basement membrane
zone and immunoglobulin M-positive colloid bodies
(5,8,51)detection of circulating basal cell cytoplasmic
autoantibodies (BCCA) by indirect immunofluorescence
may favor a diagnosis of OLDE (11). A positive BCCA
test, characterized by a distinct string of pearls pattern
on serum analysis, has been documented in OLDE by
many authors (11,52,53) and may be a useful ancillary
test to support a drug-induced etiology.
Furthermore,immunofluorescence testing also serves to rule out
other immune-mediated vesiculobullous diseases, such
as LE, pemphigus vulgaris, and mucous membrane
pemphigoid.
TABLE 3. Differential Diagnosis of OLDE
Condition Agesex Sites Oral lesions Diagnosis
Oral lichen planus Middle-aged;elderlyF
Skin: flexor surfacesOral: BM, tongue, gingival
Bilateral, symmetric;reticular > erosive;exacerbations
Clinical; histology; DIF
Lichenoid amalgam
reaction
AnyM = F BM, lateralventral tongue;
contact with amalgam
White or atrophic
striations; persistent
Clinical; histology; ?mercury
patch testSystemic lupuserythematosus
Avg. 30 yrsF Multisystem: skin, kidney,cardiac
Oral: BM, palate, gingiva
Reticular; atrophic;nonspecific erosions
Clinical; histology; DIF;serology for ANA, dsDNA
Graft-versus-hostdisease
AnyM = F Multisystem: skin, GI, liverOral: BM, tongue, Lips
Reticular; papular;atrophic nonspecificerosions
History of bone marrowtransplant; clinical; histology
Erythema multiforme 2030 yrsM = F Skin: hands, feet,
genitalOcular: conjunctivaOral: Lips, BM, tongue, FOM,
soft palate
Hemorrhagic crustingof lips; nonspecificulcers; rapid onset
Clinical; histology to rule outother ulcerative processes
F, female; M, male; BM, buccal mucosa; FOM, floor of mouth; DIF,
direct immunofluorescence; ANA, antinuclear antibodies;
dsDNA,double-stranded DNA antibodies; OLDE, oral lichenoid drug
eruption.
Woo et al: Oral Lichenoid Drug Eruption 461
-
7/30/2019 Obat Pada Anak2
5/8
Although thereare no universally acceptedcriteria for
the diagnosis of OLDE, recent efforts by McCartan et al
(17) have provided a more structured system for
reporting cases. These authors suggest that reports
should include: (1) an accurate clinical description of
lesions with a defined temporal relationship with drug
exposure, (2) evidence of histologic verification, and (3)
documented lesion resolution on drug withdrawal.
Moreover, lesion recurrence on drug re-challenge
(provocation testing) and supportive immunofluores-
cence testing will also help to confirm a medication-re-
lated cause (5,54). Lastly, some authors have used patch
testing as an auxiliary tool in diagnosis (55), while others
contend that a negative patchtest cannot reliablyrule out
OLDE (56).
The ideal treatment for OLDE consists of drug
withdrawal or substitution with an alternate medication
following consultation with the patients physician (18).
Lesion resolution is typically observed within weeks tomonths
after drug cessation although delayed responses
may result in lesion persistence (57). Furthermore, faint
residual striations or milder forms of erosive lesions
are commonly observed following elimination of the
medication (12), as seen in our patient.In many instances
however, the severity of the medical condition for which
the patient is being treated precludes drug discontinua-
tion. In such cases, topical steroid therapy has been used
but with variable to little success (24). Reportedly, select
adult patients have benefited from systemic corticoste-
roid therapy (18), topical tacrolimus (58), and topical
acetretin (59), although such treatments should be usedwith
appropriate caution in children. Palliative remedies
such as temporary mucosal protectants (e.g., milk of
magnesia) may provide symptomatic relief (18). In
addition, good oral hygiene practices are to be encour-
aged to prevent superimposed bacterial and fungal
infections (18).
In this report, the patient was taking risperidone and
carbamazepine as prescribed by his psychiatrist. Ris-
peridone is an antipsychotic agent used to manage
schizophrenia and bipolar disorder. This medication is
most often associated with central nervous system side
effects such as agitation, somnolence, and dizziness (60).
Carbamazepine is an anticonvulsant primarily indicatedfor
treatment of epilepsy with similar neurologic side-
effects as risperidone. To our knowledge, risperidone has
been associated with lichenoid dermatitis (60) but is nota
documented cause of OLDE. In contrast, carbamaze-
pine has been implicated in OLDEs (8,11,31,61), cuta-
neous LDEs (61,62), lupus erythematosus-like drug
eruptions (8,63,64) and fixed drug eruptions (8,65).
Although it cannot be stated with certainty which agent
caused the OLDE in our patient, carbamazepine is
favored due to its more extensive history of drug
reactions.
In summary, the presentation of lichenoid lesions in
the pediatric population should prompt evaluation for
OLP and other conditions with intraoral lichenoid
manifestations. A thorough history of systemic drug in-
take over the previous 12 months should be documented
as a means to eliminate or support a diagnosis of OLDE
(5). Dueto the increasing recognitionandpharmacologic
management of childhood-onset illnesses, including
attention deficithyperactivity disorder (66), it is possible
that drug-related side-effects and oral complications may
become more prevalent in the younger population.
Therefore, it is important for clinicians to recognize the
spectrum of medication-induced conditions, including
OLDE, in order to avoid delays in diagnosis and
treatment.
REFERENCES
1. Boyd AS, King LE. Lichenoid drug reaction fromisotretinoin
therapy. Cutis 2001;68:301303.
2. Kaur S, Bhalla M, Thami GP.Subacute lichenoid eruptiondue to
L-thyroxine overdosage. Dermatology 2003;206:346347.
3. Scully C, Bagan JV.Adversedrug reactions in the
orofacialregion. Crit Rev Oral Biol Med 2004;15:221239.
4. Korstanje MJ. Drug-induced mouth disorders. Clin ExpDermatol
1995;20:1018.
5. McCartan BE, McCreary CE. Oral lichenoid drug erup-tions.
Oral Dis 1997;3:5863.
6. Gu nes AT, Fetil E, Ilknur T et al. Naproxen-inducedlichen
planus: report of 55 cases. Int J Dermatol 2006;45:709712.
7. Tilly JJ, Drolet BA, Esterly NB. Lichenoid eruptions
inchildren. J Am Acad Dermatol 2004;51:606624.
8. Neville BW, Damm DD, Allen CM et al. Allergies andimmunologic
diseases. In: Neville BW, Damm DD, AllenCM, Bouquot JE, eds. Oral
& maxillofacial pathology,2nd edn. New York: W.B. Saunders
Company, 2002:300303.
9. Hay KD, Reade PC. Methyldopa as a cause of oralmucous
membrane reactions. Br Dent J 1978;145:195203.
10. Wiesenfeld D, Scully C, MacFadyen EE. Multiple liche-noid
drug reactions in patients with Ferguson-Smithdisease. Oral Surg
Oral Med Oral Pathol 1982;54:527529.
11. Lamey PJ, McCartanBE, MacDonald DGet al.Basalcell
cytoplasmic autoantibodies in oral lichenoid reactions.Oral Surg
Oral Med Oral Pathol Oral Radiol Endod1995;79:4449.
12. Robinson NA. Lichenoid tissue reactions of the oralmucosa.
Singapore Dent J 2000;23(Suppl. 1):5663.
13. Campisi G, Florena AM, Franco V et al. Oral lichenoiddrug
reaction by lithium in a patient with bipolar disorder.J Oral
Pathol Med 2005;34:124126.
14. Potts AJ, Hamburger J, Scully C. The medication ofpatients
with oral lichen planus and the association ofnonsteroidal
anti-inflammatory drugs with erosive lesions.Oral Surg Oral Med
Oral Pathol 1987;64:541543.
462 Pediatric Dermatology Vol. 26 No. 4 JulyAugust 2009
-
7/30/2019 Obat Pada Anak2
6/8
15. Van den Haute V, Antoine JL, Lachapelle JM.
Histopath-ological discriminant criteria between lichenoid
drugeruption and idiopathic lichen planus: retrospective studyon
selected samples. Dermatologica 1989;179:1013.
16. Halevy S, Shai A. Lichenoid drug eruptions. J Am
AcadDermatol 1993;29(2 pt 1):249255.
17. McCartan BE, McCreary CE, Healy CM. Studies of drug-induced
lichenoid reactions: criteria for case selection. OralDis
2003;9:163164.
18. ZelicksonBD, Rogers RS III. Drug reactions involving
themouth. Clin Dermatol 1986;4:98109.
19. Van Beek MJ, Piette WW. Antimalarials. Dermatol
Clin2001;19:147160.
20. Hawk JLM. Lichenoid drug eruption induced by propan-olol.
Clin Exp Dermatol 1980;5:9396.
21. Robertson WD, Wray D. Ingestion of medication amongpatients
with oral keratoses including lichen planus. OralSurg Oral Med Oral
Pathol 1992;74:183185.
22. Breathnach S. Drug reactions. In: Burns T, Breathnach S,Cox
N, Griffiths C, eds. Rooks textbook of dermatology,Vol. 4, 7th edn.
Oxford: Blackwell Science, 2004:1180.
23. Firth NA, Reade PC. Angiotensin-converting enzymeinhibitors
implicated in oral mucosal lichenoid reactions.Oral Surg Oral Med
Oral Pathol 1989;67:4144.
24. Hamburger J, Potts AJ. Non-steroidal anti-inflammatorydrugs
and oral lichenoid reactions. Br Med J (Clin Res
Ed)1983;287:1258.
25. Baga n JV, Thongprasom K, Scully C. Adverse oralreactions
associated with the COX-2 inhibitor rofecoxib.Oral Dis
2004;10:401403.
26. Scully C, Diz Dios P. Orofacial effects of
antiretroviraltherapies. Oral Dis 2001;7:205210.
27. Ficarra G, Flaitz CM, Gaglioti D et al. White
lichenoidlesions of thebuccal mucosa in patientswith
HIVinfection.Oral Surg Oral Med Oral Pathol 1993;76:460466.
28. Bu yu kgebiz B, Arslan N, Ostu rk Y et al. Drug reaction
to
ursodeoxycholic acid: lichenoid drug eruption in an infantusing
ursodeoxycholicacidfor neonatal hepatitis. J PediatrGastroenterol
Nutr 2002;35:384386.
29. Ridola V, Mahe E, Fawaz O et al. Dactinomycin-inducedsevere
lichenoid eruption in a child. Pediatr Dermatol2006;23:503506.
30. Kanwar VS, Gajjar A, Ribeiro RC et al. Unusualcutaneous
toxicity following treatment with dactinomycin:a report of
twocases. MedPediatr Oncol1995;24:329333.
31. Parks ET. Lesions associated with drug reactions. Derma-tol
Clin 1996;14:327337.
32. Wright JM. Oral manifestations of drug reactions. DentClin
North Am 1984;28:529543.
33. Tack DA, Rogers RS. Oral drug reactions. Dermatol
Ther2002;15:236250.
34. Pua VS, Scolyer RA, Barnetson RS.
Pravastatin-inducedlichenoid drug eruption. Australas J Dermatol
2006;47:5759.
35. Ellgehausen P, Elsner P, Burg G. Drug-induced lichenplanus.
Clin Dermatol 1998;16:325332.
36. Al-Hashimi I, Schifter M, Lockhart PB et al. Oral
lichenplanus and oral lichenoid lesions: diagnostic and
thera-peutic considerations. Oral Surg Oral Med Oral PatholOral
Radiol Endod 2007;103(Suppl. 1):S25S31.
37. Felder RS, Millar SB, Henry RH. Oral manifestations ofdrug
therapy. Spec Care Dentist 1988;8:119124.
38. Usman A, Kimyai-Asadi A, Stiller MJ et al. Lichenoideruption
following hepatitis B vaccination: first NorthAmerican case report.
Pediatr Dermatol 2001;18:123126.
39. Agrawal S, Garg VK, Joshi A et al. Lichen planus afterHBV
vaccination in a child: a case report from Nepal.J Dermatol
2000;27:618620.
40. Limas C, Limas CJ. Lichen planus in children: a
possiblecomplication of hepatitis B vaccines. Pediatr
Dermatol2002;19:204209.
41. Cottoni F, Ena P, TeddeG et al. Lichen planus in children:a
case report. Pediatr Dermatol 1993;10:132135.
42. Kanwar AJ, Handa S, Ghosh S et al. Lichen planus
inchildhood: a report of 17 patients. Pediatr
Dermatol1991;8:288291.
43. Kumar V, Garg BR, Baruah MC et al. Childhood lichenplanus
(LP). J Dermatol 1993;20:175177.
44. Sharma R, Maheshwari V. Childhood lichen planus: areport of
fifty cases. Pediatr Dermatol 1999;16:345348.
45. Nanda A, Al-Ajmi HS, Al-Sabah H et al. Childhoodlichen
planus: a report of 23 cases. Pediatr Dermatol2001;18:14.
46. Alam F, Hamburger J. Oral mucosal lichen planus inchildren.
Int J Paediatr Dent 2001;11:209214.
47. Winer LH, Leeb AJ. Lichenoid eruptions. a histopatho-logical
study. AMA Arch Derm Syphilol 1954;70:274281.
48. Beckman KA, Chanes L, Kaufman SR. Lichen planusassociated
with topical beta-blocker therapy. Am J Op-thalmol
1995;120:530531.
49. Powell ML, Ehrlich A, Belsito DV. Lichenoid drug erup-tion
to salsalate. J Am Acad Dermatol 2001;45:616619.
50. Schidt M. Oral lupus erythematosus. III. A histopatho-logic
study of sixty-six patients. Oral Surg Oral Med OralPathol
1984;57:281293.
51. Helander SD, Rogers RS III. The sensitivity andspecificityof
direct immunofluorescence testing in disorders of
mucous membranes. J Am Acad Dermatol 1994;30:6575.52. Van Joost
T. Incidence of circulating antibodies reactivewith basal cells of
skin in drug reactions. Acta DermVenereol Suppl (Stockh)
1974;54:183187.
53. McQueen A, Behan WMH. The string of pearls phe-nomenon an
immunofluorescent serological finding inpatients screened for
adverse drug reactions. Am JDermatopathol 1982;4:155159.
54. Kurumaji Y, Miyazaki K. Tiopronin-induced lichenoideruption
in a patient with liver disease and positive patchtest reaction to
drugs with sulfhydryl group. J Dermatol1990;17:176181.
55. Sharma VK, Vatve M, Sawhney IM et al. Clinicalspectrum of
drug rashes due to antiepileptics. J AssocPhysicians India
1998;46:595597.
56. PenneysNS,Ackerman AB,Gottlieb NL.Gold dermatitis.Arch
Dermatol 1974;109:372376.57. Savage NW. Oral lichenoid drug
eruptions. Oral Dis
1997;3:5557.58. Lozada-Nur FI, Sroussi HY. Tacrolimus powder
in
Orabase 0.1% for the treatment of oral lichen planus andoral
lichenoid lesions: an open clinical trial. Oral SurgOral Med Oral
Pathol Oral Radiol Endod 2006;102:744749.
59. Dalmau J, Peramiquel L, Puig L et al.
Imatinib-associatedlichenoid eruption: acitretin treatment allows
maintained
Woo et al: Oral Lichenoid Drug Eruption 463
-
7/30/2019 Obat Pada Anak2
7/8
antineoplastic effect. Br J Dermatol 2006;154:12131216.
60. Thomson Healthcare, Inc. Physicians desk reference,59th ed.
New Jersey: Thomson Healthcare, Inc., 2005.p. 17421747,
23772380.
61. Roberts DL, Marks R. Skin reactions to carbamazepine.Arch
Dermatol 1981;117:273275.
62. Atkin SL, Mckenzie TM, Stevenson CJ. Carbamazepine-induced
lichenoid eruption. Clin Exp Dermatol 1990;15:382383.
63. Jain KK. Systemic lupus erythematosus (SLE)-like syn-dromes
associated with carbamazepine therapy. Drug Saf1991;6:350360.
64. Simpson JR. Collagen disease due to carbamazepine(Tegretol).
Br Med J 1966;2:1434.
65. Shuttleworth D, Graham-Brown RA. Fixed drugeruption due to
carbamazepine. Clin Exp Dermatol 1984;9:424426.
66. Goldstein S. Is ADHD a growth industry. J Atten
Disord2006;9:461464.
464 Pediatric Dermatology Vol. 26 No. 4 JulyAugust 2009
-
7/30/2019 Obat Pada Anak2
8/8









![[7]. Obat Obat Pada Gangguan Sistem Sirkulasi](https://img.pdfslide.tips/doc/110x75/55cf8eae550346703b948000/7-obat-obat-pada-gangguan-sistem-sirkulasi.jpg)