Embed Size (px)
Citation preview

On-scene Trauma care

เนอหาและแนวทางของ PHTLS
• มความเปนปจจบน (Up-to-date)
• มหลกการทางวทยาศาสตร (Scientific base)
• ใชหลกการเดยวกนกบ ATLS


การปองกนอบตเหต(Prevention)
ระบบการแพทยฉกเฉน
(EMS)
การรกษาใน รพ(definitive
care)

การผาตด(operation)

ประวตการเปลยนแปลงปรบปรง หลกการดแลผบาดเจบนอกโรงพยาบาล
การรบผปวยแลวน าสง รพ โดยไมใหการรกษาทจดเกดเหต—either in the field or en route, with rapid transport to
the hospital, frequently without anyone in the patient care compartment— system prior to the 1950s
การรกษาทจดเกดเหตบางอยาง This period began with the publication of the National Standard
Curriculum and continued until the late 1970s
การรกษาทจดเกดเหตอยางเตมท กอนเคลอนยาย(Stay and play). the trauma patient and the cardiac patient
were treated exactly alike; that is, attempts were made to stabilize the patient in the field, often for
prolonged amounts of time.
การรกษาทจดเกดเหตเฉพาะทจ าเปน. Beginning in the mid-to late 1980s, it was recognized that the critical
trauma patient could not be “Stabilized” in the field but rather required rapid assessment and intervention
in an OR to control hemorrhage. This realization led to the change in prehospital management of the
trauma patient of minimizing the on-scene time and rapid extrication and transport to an appropriate


การปองกนการบาดเจบ (Injury prevention)หลกการและแนวคด : ลดการเกดอบตเหต สามารถลดการเสยชวตได

กระบวนการท าใหเกด Injury Prevention (Prevention as the solution)
• การปองกนอปบตเหตสามารถท าไดในระบบ EMS (EMS role on prevention)• การเรยนรหรอแนะน าแบบตวตอตว (One-0n-0ne Intervention)• การผลกดนหรอน าเสนอผานระดบชมชน (Community wide intervention)• ปองกนอบตเหตในบคลากร EMS (Injury prevention to EMS provider :
most important person in trauma incident)

ทฤษฎ (Principles or the science of medicine) หลกการหรอองคความร ทจะน าไปสผลลพททคาดหวง
การปรบใช (Preferences or the art of medicine) กระบวนการน าความรมาใช ใหเกดผลไดจรง ขนกบหลายปจจย เชน
เหตการณแตละครงแคกรตางกน (Situation that currently exists)
ผ ปวยแตละรายแตกตางกน (Condition of the patient)
การใชความรหรอทฤษฎ และประสบการณ (Knowledge and experience)
การมอปกรณเครองมอทพรอม (Equipment available)
การใชความรใหไดผลจรง (How to use the Knowledge)
ทฤษฎ กบ ชวตจรง

พยาธวทยาของการด ารงชวตและเสยชวต (PHYSIOLOGY OF LIFE AND DEATH)

การด ารงชพของมนษย
• กน
• ขบถาย
• นอน
• หายใจ

ทางเดนอากาศ (Airway)

หายใจเพอ ????
ตองมตองการ

ระบบไหลเวยนโลหต
ขนสง oxygen

การหายใจและสรางพลงงานระดบเซลล
ตองมตองการ
กระบวนการทไมม O2Anaerobic respiration
ตนเหตของปญหา
กระบวนการม O2Aerobic respiration

SHOCK #### ค ำทเรำไมอยำกไดยน ######
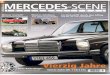
Figure 4-6 Organ Tolerance to Ischemia
Organ Warm Ischemia Time
Heart, brain, lungs 4-6 minutes
Kidneys, liver, gastrointestinal tract 45-90 minutes
Muscle, bone, skin 4-6 hours
• HYPOPERFUSION
• INADEQUET TISSUE PERFUSION
• INADEQUET CELLULAR CIRCULATION AND RESPIRATION

ความดนโลหต Blood pressureCardiac output x peripheral vascular resistant(PVR) = BP
HR x stroke volume x PVR = BP
ปม แทงก ทอ

ชนดของภำวะ SHOCK• ภาวะชอคจากการขาดเลอด Hypovolemic shock
#Vascular volume smaller than normal vascular sizeo Loss of fluid and electrolytes (dehydration)o Loss of blood and fluid (hemorrhagic shock)
• Distributive shock#Vascular space larger than normalo Neurogenic "shock" (hypotension)o Psychogenic shocko Septic shock
o Anaphylactic shock
• Cardiogenic shock#Pump failure
Intrinsicextrinsic
ปม แทงก ทอ

Hypovolemic shock
หลกการรกษา• หามเลอด (Stop bleed External/Internal)• ใหเลอด (Replace blood component)• ใหสารน า (Replace fluid)

Distributive shock
หลกการรกษา
• Replace fluid
• Vasoconstrictive agent

Cardiogenic shock• Intrinsic : MI/Arrhythmia
• ExtrinsicTension pneumothorax >> needle thoracostomyCardiac tamponade >> Pericardiocentesis

หลกทฤษฎท PHTLS น ามาใช

1.กระบวนการคดวางแผนดแลผบาดเจบวกฤตหรอรนแรง(Component of Critical Thinking in Emergency Medical Care)
1. ประเมนสถาณการณ ( situation.)2. ประเมนผ ปวย (patient.)3 ประเมนทรพยากร (resources.)4 วเคราะหผลลพธทตองการ (possible solutions.)5 เลอกแนวทางหรอวธการทจะรกษา( manage the situation).6 วางแผนการรกษา (plan of action.)7 เรมใหการรกษาและประเมนผลเบองตน (response of the patient to plan )8 การประเมนและตดสนใจระหวางท าการรกษา( Decision the plan of action.)9 ปฏบตตามขนตอนท 7 8 จนการรกษาไดผลส าเรจ

2.ขนตอนการประเมนหรอตดสนใจในภาวะวกฤต (Steps in Critical Thinking)
AssessmentWhat is going on? What needs to be done? What are the resources to achieve the goal? Analysis will involve : ประเมนจดเกดเหต Scene Assessment. ประเมนภาวะเสยงหรอสงอนตรายในจดเกดเหต ( hazards to either the patient or provider.) ประเมนอาการผ ปวย (Condition of the patient.) ภาวะเรงดวนทตองรบแกไข (Rapidity required for resolution.) สถานทจะน าสงผ ปวย (Location of the care) จ านวนผ ปวยในจดเกดเหต (Number of patients on the scene.) จ านวนยานพาหนะทตองการ ( Number of transport vehicles required.) ตองการการน าสงทเรงดวนกวาหรอไม ( more rapid transport : aero-medical).

ขนตอนการปฏบต
1 วเคราะหสถาณการณและอาการผ ปวย ( Analysis)
2 วางแผนการรกษา ( Construction the plan )
3 ลงมอท า ใหการรกษา ( Action )
4 การประเมนซ า ( Reassessment )

Analysis- คดวเคราะหสถานการณและอาการผ ปวยอยางรวดเรว จากขอมลทไดรบ ทงจากการสงการ การประเมนจดเกดเหต การซกประวต การตรวจรางกาย ( Primary Assessment ) โดยอาศยความรและทฤษฎ ประสบการณ ค าสงการทางการแพทย
- วเคราะหความเปนไปไดในการรกษา และการประเมนทรพยากรทม
Construction of a Plan - วางแผนการรกษาจากการวเคราะห เพอเลอกแผนการรกษาทไดผลลพธดทสด ทเหมาะกบสถานการณทเจอ ทรพยากรทมขณะนน เวลาทจ ากด ความสามารถของทม

Action- การใหการรกษาตามแผน รวมทงการปฏบตการเปนทม การปฏบตตามค าสงจากหวหนาทม และจากการตดสนใจรวมกน - การสงเกตอาการตอเนอง และการเปลยนแปลงของสถานการณ ผานการท างานเปนทม - มการแบงหนาทอยางชดเจนภายในทม ระหวาง หวหนาทมผสงการหรอตดสนใจ และลกทม
Reassessment- การประเมนซ าและการสงเกตอาการตอเนอง ทงการเปลยนแปลงของสถานการณ และการเปลยนแปลงของอาการผ ปวย พรอม
ทงการวเคราะหและวางแผนการรกษาใหม

การประเมนและรกษาผปวย (Patient assessment and management)

Primary survey A-B-C-D-Eแตกตางจาก ATLS อยางไร
“ประเมนและรกษาอยางรวดเรว แลวรบน าสง = SAVE and RUN ”

Definitive Care
Reevaluation
Adjuncts
Adjuncts
Primary Survey
Resuscitation
Reevaluation
Detailed
Secondary Survey
หลกการ Initial Assessment เหมอนกบ ATLS

หลกการ Secondary survey เหมอนกบ ATLS : Head to toe
ท าการตรวจเมอผ ปวยมอาการคงทหรอหลงจาก Primary survey and Resuscitation

หลกการส าคญ : Concept of Transport
ผ ปวยบาดเจบอาการวกฤต การรกษาจ าเพาะ ทเหมาะสมและส าคญทสดคอ การน าสงโรงพยาบาลทสามารถรกษาภาวะบาดเจบนนได ใหเรวทสด
หตถการหรอการกษาทไมจ าเปน หรอสามารถรอไดโดยไมเกดอนตราย ควรชะลอไวกอนและสามารถกระทไดบนรถ หรอเมอโอกาสอ านวย เชน
- การดามกระดกหก ทไมใชภาวะคกคามชวต
- การปดแผลขนาดเลก ทไมใชแผลอนตราย

หลกการ Appropriate ongoing Assessment เหมอนกนผ ปวยสามารถอาการเปลยนแปลงไดตลอดเวลา (Time change ,everything change)
Similar concept of Communication : MIST
M : Mechanism of injury/sceneI : Injury partS : Sign > vital sign , sign and symptomT : Treatment

CPR in Traumatic patient
ขอแตกตางของภาวะ Cardiac Arrest ในผ ปวย Trauma กบผ ปวยทวไป
- ผ ปวยอาจตองการเลอด ( Need blood ?)
- ผ ปวยตองไดรบการผาตด (Need Surgical intervention)
- โอกาสรอดเพยง 4%

ผปวยบาดเจบรนแรงทไมจ าเปนตอง CPR(Withhold CPR should be done)
- อวยวะส าคญฉกขาด
- พบลกษณะของการเสยชวตมานาน เชน lividity , rigor mortis, decomposition.
- ผ ปวย Blunt Trauma ททราบวามภาวะหยดหายใจ หรอหวใจหยดเตนนานแลว กอนทมไปถง (pulseless and apneic on arrival of prehospital care providers.)
- ผ ปวย Penetrating trauma ทไมพบสญญาณของการรอดชวต เชน รมานตาไมตอบสนอง (no pupillary reflexes) , ไมมลกษณะคลนไฟฟาหวใจของการมโอกาสรอดชวต ( no organized cardiac rhythm on ECG greater than 40 beats/minute).

Any questions?