Embed Size (px)
Citation preview
![Page 1: Passage of a δ-Opioid Receptor Selective Enkephalin, [d-Penicillamine2,5]Enkephalin, Across the Blood-Brain and the Blood-Cerebrospinal Fluid Barriers](https://reader038.pdfslide.tips/reader038/viewer/2022100510/5750243f1a28ab877eadf13a/html5/thumbnails/1.jpg)
Journal c~fNeurochemistryLippincott—Raven Publishers, Philadelphia© 1996 International Society for Neurochemistry
Passage of a ó-Opioid Receptor Selective Enkephalin,[D-Penicillamine2’5]Enkephalin, Across the Blood—Brain
and the Blood—Cerebrospinal Fluid Barriers
Sarah A. Williams, Thomas J. Abbruscato, *Victor J. Hruby, and Thomas P. Davis
Departments of Pharmacology and *Chemjsz~j..y University of Arizona, Tucson, Arizona, U.S.A.
Abstract: [D-Penicillamine2’5]enkephalin(DPDPE) is anenzymatically stable, cS-opioid receptor-selective peptide,which produces analgesia when given intracerebroven-tricularly. However, because only modest analgesic ef-fects were seen after subcutaneous administration ofDPDPE, it has been inferred that it does not cross theblood—brain barrier well. In this present study, a vascularbrain perfusion technique in anesthetized rats was usedto measure directly whether [3H]DPDPEcould cross theblood—brain and/or the blood—CSF barriers. The resultsindicated that the brain uptake of [3H]DPDPEwas sig-nificantly greater than that of [14C]sucrose,a vascularmarker (p < 0.01), and than that of [3H]DPDPEinto theCSF (p < 0.01). Furthermore, HPLC analysis confirmedthe integrity of the 3H to DPDPE and demonstrated thatintact [3H]DPDPEentered the brain. Although 1 mM eu-cine-enkephalin failed to inhibit uptake of [3H]DPDPE,unlabeled DPDPE (100 pM) caused a significant inhibitionof the brain uptake (p < 0.01) but not the CSF uptakeof [3H]DPDPE. These data provide evidence that intact[3H]DPDPE enters the CNS of anesthetized rats by satu-rable and nonsaturable mechanisms. In addition, the sat-urable mechanism is likely to be found at the blood—brainbarrier, with the blood—CSF barrier playing only a minorrole in the brain uptake of this peptide. Key Words:Blood—brain barrier—Blood—CSF barrier—[D-Penicilla-mine25] enkephalin — Peptide — Brain perfusion — En-kephalin.J. Neurochem. 66, 1289—1299 (1996).
[D-Penicillamine2’5lenkephahn (DPDPE; tyrosine-D - penicillamine - glycine - phenylalanine - D - penicilla -
mine) is a 6-opioid receptor-selective enkephalin ana-logue (Mosberg et a!., 1983; Emmerson et a!., 1994;Vanderah et a!., 1994), which, in contrast to endoge-nous enkephalins, is conformationally restricted by adisulfide bridge and therefore enzymatically stable(Hambrook et al., 1976; Weber et al., 1991, 1992;Brownson et al., 1994). DPDPE was developed byour research group in an attempt to design receptor-selective opioid peptide drugs, which could be usedclinically to produce favorable pharmacological ef-
fects, such as analgesia, without eliciting multiple sideeffects (Mosberg et al., 1983; Hruby et al., 1991). Inaddition, it was hoped that these peptide analoguescould be used to determine the physiological and phar-macological roles of the opioid receptor types (j.t, 6,and K) (Pert and Snyder, 1973; Martin et a!., 1976;Lord et al., 1977).
Substances can enter the brain either directly acrossthe blood—brain barrier (BBB), found at the level ofthe cerebral capillary endothelium and/or indirectlyacross the choroid plexuses and the arachnoid mem-brane (blood—CSF barrier) into the CSF and then bydiffusion into the brain. Although initially it wasthought that peptides could not enter the CNS, it isnow generally accepted that some peptides can enterand exit the CNS, and several recent reviews have beenpublished (Broadwell, 1989; Audus et al., 1992; Bankset al., 1992; Brownlees and Williams, 1993; Podusloet al., 1994). At least five methods have been postu-lated by which peptides can enter the CNS: transmem-brane diffusion (Banks and Kastin, 1985), fluid-phaseendocytosis (Broadwell, 1989), absorptive-mediatedendocytosis (Kumagai et al., 1987; Terasaki et al.,1989), receptor-mediated transport (Pardridge et al.,1985; Fishman et al., 1987), and carrier-mediatedtransport (Banks and Kastin, 1987).
The transport of DPDPE into the CNS has pre-viously been investigated by our laboratory using bothin vivo and in vitro techniques. Distribution studiesexamining brain uptake after intraperitoneal, intrave-nous, subcutaneous, and oral administration showedthat naloxone-displaceable [3HJDPDPE could accu-mulate in the brain, suggesting that there is a significantCNS uptake (Weber et al., 1991, 1992). In addition,
Received August 8, 1995; revised manuscript received October18, 1995; accepted October 24, 1995.
Address correspondence and reprint requests to Dr. T. P. Davisat Department of Pharmacology, University of Arizona, 1609 NorthWarren Street, Tucson, AZ 85724, U.S.A.
Abbreviations used: BBB, blood-~brain barrier; DPDPE, [o-penicillamineS I enkephalin.
1289
![Page 2: Passage of a δ-Opioid Receptor Selective Enkephalin, [d-Penicillamine2,5]Enkephalin, Across the Blood-Brain and the Blood-Cerebrospinal Fluid Barriers](https://reader038.pdfslide.tips/reader038/viewer/2022100510/5750243f1a28ab877eadf13a/html5/thumbnails/2.jpg)
1290 S. A. WILLIAMS ET AL.
experiments using a primary cell culture model of theBBB indicated that DPDPE could cross the BBB (We-ber et a!., 1993).
Analgesia, produced by 6-opioid receptors, isthought to be a centrally mediated event; therefore,only those agonists that can pass through the BBB andblood—CSF barrier, after peripheral administration, arelikely to induce this biological effect (Frederickson etal., 1981; Ward and Takemori, 1983; Galligan et a!.,1984; Shook et a!., 1987). Several studies measuredsignificant analgesia after intravenous, intracerebro-ventricular, and intrathecal administration of DPDPE,thus suggesting CNS uptake (Galligan et a!., 1984;Porreca et al., 1984; Heyman et al., 1987; Weber etal., 1991). In contrast, subcutaneous administration ofDPDPE elicited no analgesic effect, and from thisstudy it has been inferred that this peptide does notcross the BBB and enter the brain very effectively(Shook et al., 1987). However, it is known that theroute of administration plays an important role in thebioavailability of drugs to the brain, and it is likelythat, after subcutaneous administration, the amountreaching the circulation is decreased by tissue seques-tration, lack of absorption into the circulation, and evencatabolism. Thus, the inability of DPDPE to cross theBBB and produce a biological effect after subcutane-ous administration may actually reflect too low a con-centration of peptide in the plasma (Rapoport et a!.,1980).
A clearer understanding of the passage of opiatesand their analogues across membrane systems such asthe BBB is essential in clarifying their physiologicalor phannacological role, their roles in pathologicalconditions such as drug addiction, and the developmentof therapeutic approaches. With this in mind the aimof this study was to investigate the uptake of [3H1-DPDPE into the CNS, more directly than previousmethods, using an in situ brain perfusion technique inanesthetized rats (Z!okovic et al., 1986; Williams etal., 1993; Preston et a!., 1995). This technique hasbeen specifically developed to measure the uptake ofslowly permeating molecules across both the BBB andthe blood—CSF barrier and, in this study, was alsoused to determine whether uptake was by nonsaturableand/or by specific saturable transport mechanisms.This information concerning the uptake of [3H]-DPDPE across the BBB and blood—CSF barrier willbe used to direct future enkephalin analogue develop-ment and research.
EXPERIMENTAL PROCEDURES
Perfused rat brainThe experimental protocol was approved by the Institu-
tional Animal Care and Use Committee at the University ofArizona. Adult Sprague—Dawley rats (weighing 250—350g) were anesthetized and heparinized with intrapentonealinjections of sodium pentobarbital (64.8 mg kg ) and hepa-
nfl (10,000 U kg’). The neck vessels were exposed, andthe right common carotid artery was cannulated with finesilicone tubing connected to a perfusion system. The erythro-cyte-free perfusion fluid (Preston et a!., 1995) consisted ofa modified Krebs—Henseleit Ringer’s solution [117.0 mMNaCl, 4.7 mM KC1, 0.8 mM MgSO.r3H
2O, 24.8 mMNaHCO3, 1.2 mMKH2PO4, 2.5 mMCaCl2~6H2O,10mMn-glucose, 39 g L’ of dextran (MW 70,000), and I gof bovine serum albuminI that had been thoroughly gassedwith 5% CO2 in 02 (P02, 640—730 mm Hg) and warmed to37°C.With the start of perfusion the right jugular vein wassevered to allow drainage of the perfusion medium. Oncethe correct perfusion pressure of 90.8 ±5.3 mm Hg and aperfusion flow rate of 3.1 ml mm -‘ had been achieved forthe right carotid artery, the contralateral carotid artery wascannulated and perfused in a similar manner. The remainingjugular vein was then severed. The
3H-!abeled DPDPE, inthe absence and presence of unlabeled DPDPE, leucine-en-kephalin, or [14CI sucrose, the vascular space marker, wasthen infused via a slow-drive syringe pump (model 22; Har-vard Apparatus, South Natick, MA, U.S.A.) into the in-flowing mammalian Ringer’s solution. After the set perfu-sion time (2.5—30 mm), a cisternamagnaCSF sample (‘—50gil) was taken, and perfusionwas terminated by decapitation.The brain was removed, choroid plexuses were excised, andthe brain was homogenized. Perfusion fluid was collectedfrom the carotid cannulae immediately at the end of theperfusion period.
Brain tissue samples (‘-~50mg wet weight) together withthe CSF and lOO-jel perfusate samples were prepared forliquid scintillation counting. To ensure uniformity all sam-ples were treated in a similar manner and solubilized over-night in 1 ml of tissue solubilizer (TS-2; Research Products,Mount Pleasant, IL, U.S.A.). After solubilization, 30 ~slofglacial acetic acid was added to the samples to eliminatechemiluminescence. Four milliliters of Budget Solve LiquidScintillation Cocktail (Research Products) was added, andthe samples were counted for radioactivity (model LS 5000TD counter; 43% efficiency for 3H and 93% for 4C; Beck-man Instruments, Fullerton, CA, U.S.A.). The 3H and ‘4Cactivities were converted from cpm to dpm, with the use ofinternal stored quench curves.
Capillary depletion stepAfter the brain had been removed and the choroid plexuses
were excised, the brain was subjected to thecapillary deple-tion procedure as previously reported (Triguero et al., 1990;Zlokovic et al., 1992). In brief, brain (0.5 g) was homoge-nized (Polytron homogenizer; Brinkmann Instruments,Westbury, NY, U.S.A.) in 3.5 ml of ice-cold physiologicalbuffer (pH 7.4; 10 mM HEPES, 141 mM NaCl, 4 mM KC1,2.8 mM CaC1
2, 1 mM MgSO4, 1 mM NaH2PO4, and 10mM D-glucose (Triguero et al., 1990). Four milliliters ofice-cold 26% dextran (MW 60,000) solution was then addedto achieve a final dextran concentration of 13%, and thesample was rehomogenized with 3 strokes (Bowman et al.,1983). An aliquot of homogenate was removed, and theremainder was centrifuged at 5,400 g for 15 mm in a micro-fuge (Beckman Instruments). The capillary-depleted super-natant and vasculature-containing pellet were carefully sepa-rated. Homogenate, pellet, and supernatant were then so!ubi-lized, as described above, before the addition of scintillationfluid to enable radioactive counting. To assess the percentcontamination of the supernatant with the blood vessels,
J. Neurochem., Vol. 66, No. 3, 1996
![Page 3: Passage of a δ-Opioid Receptor Selective Enkephalin, [d-Penicillamine2,5]Enkephalin, Across the Blood-Brain and the Blood-Cerebrospinal Fluid Barriers](https://reader038.pdfslide.tips/reader038/viewer/2022100510/5750243f1a28ab877eadf13a/html5/thumbnails/3.jpg)
BRAIN AND CSF ENTRY OF DPDPE 1291
(1)
(2)
(3)
which failed to pellet, the specific activity of the vascularenzyme marker alkaline phosphatase was measured using a
Octanol/saline partition coefficientsPartition coefficients for [3HI DPDPE and [14C]sucrose
Sigma assay kit (procedure no. 104; Sigma Chemical Co., St. in 1-octanol/saline were determined by the method of Col-Louis, MO, U.S.A.). The alkaline phosphatase supernatant! lins et al. (1988). In brief, 1 ~tCiof the test compound waspellet ratio was found to be 4.61 ± 0.86%, which is in placed in a saline solution (pH 7.4) at room temperature.agreement with the value published by Triguero et a!. Equal volumes of saline and octano! were shaken vigorously(1990), indicating that there is very little contamination of andthen centrifuged at 1,000 g for 5 mm. The upper octanolthe supernatant by cerebral capillary endothelium. phase and lower aqueous phase were separatedand analyzed
by liquid scintillation counting. Thepartition coefficient wasHPLC analysis
To establish the integrity of the tnitiated label to DPDPEand the stability of DPDPE, samples from the arterial perfu-
calculated as the ratio of labeled substance in the octanolphase to concentration in the aqueous phase. For each corn-pound triplicate determinations were made.
sate, venous outflow, andbrain were analyzed using a series410 HPLC gradient system (Perkin-Elmer, Norwalk CTU.S.A.) as described previously (Davis, 1990). Perfusionmedium samples were prepared for analysis by addition ofan equal volume of acetonitrile, mixing, and centrifugationat 13,000 g for 5 mm. The supernatant was removed anddiluted to produce a sample for HPLC analysis with a finalacetonitrile concentration of <10%. Brain extractions were
•
MaterialsRadiolabeled substances. [3H
2I Tyr1DPDPE (18.1 Ci!
mmol) wasprovided by Chiron Mirnotopes Peptide Systems(San Diego, CA, U.S.A.) under thedirection of theNationalInstitute on Drug Abuse. [‘4CISucrose (0.44 Ci/rnmol) waspurchased from NEN Research Products (Boston, MA,U.S.A.).
performed using a modified method of Erchegyi et al.(1991). In brief, rats were perfused with [3H1DPDPE asdescribed previously. At theend of 30-mm (n 2) perfusionperiods, the animal was decapitated, and the brain was re-
Unlabeled substances. DPDPE was provided by ChironMimotopes Peptide Systems under the direction of the Na-tional Institute on Drug Abuse. Leucine-enkephalin was pun-chased from Sigma.
moved and placed in 7.5 ml of ice-cold 10% trifluoroaceticacid. The sample was taken for homogenization (Polytronhomogenizer) and then centrifuged at 27,820 g for 20 mm(Sorval! RC2-B centrifuge; Du Pont Medical Products, Wi!-mington, DE, U.S.A.). The supernatant was collected, anequal volume of ether was added, and the samples weregently agitated. The samples were recentrifuged at 200 g for
Expression of resultsThe amount of 3H or ‘4C radioactivity in thebrain (whole
brain, homogenate, supernatant, or pellet) and CSF (CT~~SU.;
dpm g -‘ or dpm ml 1) was then expressed as a percentageof that in the artificial perfusate (Cr
1 dpm ml andtermedthe RTimue% (ml g’ or ml ml ‘):
20 mm, and the supernatant was discarded. The sampleswere then pooled, lyophilized, and diluted to 500 j.tl with10% acetonitrile before being taken for HPLC analysis.
R % = < 100Tn~ue
All samples were eluted from a 0.46- x 15-cm InertsilODS-21.t column (Metachem Technologies, Torrance, CA, The percent inhibition of uptake by an inhibitor can beU.S.A.) with alinear gradient of 10—40% 0.1% trifluoroace- expressed by the following equation:tic acid in acetonitrile versus 0.1% aqueous trifluoroaceticacid over a 20-mn period at 1.5 ml!min and 37°C.Afterseparation on the column the outflow from the HPLC was
I h~b — RTissue — RlflhlbitlOn 100C n 1 ition — ~ X
directed to an A200 Flo-One Radioactive Detector (PackardRadiomatic Instruments and Chemicals, Tampa Bay, FL, where R1flhfbt~I0. is the RTIS~U. uptake in the presence of anU.S.A.) and mixed with Flo-Scint 111 (Packard), beforepassing through the 0.5-rn! capacity flow-cell for real-time
inhibitor in the plasma perfusate.Brain unidirectional transfer constant, ~ values can then
analysis of the radioactive sample. be determined from multiple-time uptakedata (2.5—30 mm)as previously described by Gjedde (1981, 1982), Patlak et
Protein bindingDrug binding to bovine albumin at 37°Cwas determined
al. (1983), and Zlokovic eta!. (1986). The following equa-tion describes K1~:
by ultrafiltration centrifugal dialysis (Paulus, 1969; Bane eta!., 1985). Ultrafiltration of [
3HIDPDPE (4.09 nM) dis-solved in 1 ml of warmedperfusion medium was carriedoutwith the use of the Centrifree micropartition device (Ami-
j.T
I C~(t)dtCBrain ( T) + vC~,
1( T) m
con, Beverly, MA, U.S.A.). Approximately 400 ~zlof ultra-filtrate was obtained, when the sample was centrifuged at1,978 g for 10 mm (Sorvall RC2-B). The total concentration
where C~rajn(T) and C~1(T) are radioactivities per unitweight of brain (dpm g ~‘) and plasma (dpm ml ~‘) at time
(T) of [3HIDPDPE introduced into the system and that T, with T being the time of perfusion in minutes. V, is the
found in the ultrafiltrate (F) were determined by scintillation initial volume of distribution of the test solute in the rapidlycounting. The percentage of [3H]DPDPE bound to albumin equilibrating space, which may include the vascular space,could then be expressed as follows: [(T — F) ITI x 100. In the capillary endothelial volume, andbr compartments inaddition, to confirm that bovine albumin was not found in parallel with the BBB (Blasberg et al., 1983; Zlokovic ettheultrafiltrate, the protein concentration was determined by al., 1986; Begley et a!., 1990). Because under the presentthemethod of Lowry et al. (1951) using bovine serum albu- experimental conditions the concentration of [3H]DPDPEmm as the standard and was found to be negligible, in the arterial inflow (Cr
1) is constant, then
J. Neurochem., Vol. 66, No. 3, 1996
![Page 4: Passage of a δ-Opioid Receptor Selective Enkephalin, [d-Penicillamine2,5]Enkephalin, Across the Blood-Brain and the Blood-Cerebrospinal Fluid Barriers](https://reader038.pdfslide.tips/reader038/viewer/2022100510/5750243f1a28ab877eadf13a/html5/thumbnails/4.jpg)
1292 S. A. WILLIAMS ET AL.
CT
J C~(t)dt
cpl
CCSF(T)K
1,, =
I C~dtJo
(4)
and Eq. 3 simplifies to
CBn(T) = K1, T + V~ (5)
C~(T)Equation 5 defines a straight line with a slope K,0 (ml
min’ g~)and ordinate intercept V, (ml g’). Because theequation includes the vascular space (V,), direct comparisonscan be made between brain and CSF rate constants (K,0).Backflux transport of the test solute from brain to blood isindicated by a departure from linearity of the experimentalpoints.
Several assumptions are made about this transport mode!and are fully described in the study by Patlak et al. (1983).In brief, they include that there is a single source for the testsolute in the system, i.e., the plasma; its concentration in theplasma may vary with time; there is a reversible compart-ment from which the compound can leave and return to theplasma or enter an irreversible compartment; movement bythis test solute within these compartments obeys first-orderkinetics; the test solute does not alter the system; the testsolute is not initially present in either the reversible or irre-versible compartments; the test solute is only metabolizedwithin the irreversible compartment, and any resultant me-tabolite is trapped within this compartment.
The CSF does not meet all of the above criteria; for exam-ple, it cannot contain an irreversible compartment. Thus,this model is not appropriate for determining blood to CSFunidirectional transfer constants. B!ood-to-CSF transfer con-stants can be determined by means of the following equationdeveloped by Collins and Dedrick (1983) and Smith andRapoport (1986):
(6)
This two-compartment/single-time uptake analysis can beapplied if entry of the test solute into the CSF is proportionalto its plasma concentration and theconcentration in the CSF(CCSF) is less than the concentration in the plasma (Cr1);thus, efflux (CSF to blood) is much smaller than influx(blood to CSF) of the test solute and therefore can be ig-nored. In addition, the uptake time must be less than thehalf-time for ventricular CSF turnover, so that loss of thetest solute due to bulk flow can be ignored. In the rat, theCSF turnover rate is —4 h (Bradbury, 1979), much longerthan the time course of the current experiments (up to 30mm). Under the present experimental conditions, the con-centration of the test solute in the perfusion medium remainsconstant; thus, f~C~~dt= C~1 T. Simple two-compartmentanalysis has also been used to determine unidirectional rateconstants from blood to brain (Ohno et al., 1978; Blasbergeta!., 1983; Zlokovic et al., 1986). Blood-to-brain unidirec-tional transfer constants determined in this manner must becorrected for vascular space. In this study this was achievedby subtracting [‘
4CI sucrose (RBran,) from [3HI DPDPE(RBrai,~)
Data analysisFor all experiments, the data are presented as mean
±SEM values. The correlation coefficients (r), slopes (K~0),
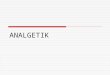
FIG. 1. Brain (top) and CSF (bottom) uptake of [3H]DPDPE
(U) and [14C]sucrose(A) plotted against time. Uptake is ex-pressed as a percent ratio of tissue to perfusate radioactivities(RT~
0000ml g or ml mi-1). Data are mean ±SEM (bars) values
of three to seven animals.
and intercepts (1,7,) of curves were determined by leastsquares linear regression analysis, and the slopes were com-pared by ANOVA. Student’s t test wasused for the compari-son of two means. Statistical significance was taken as p<0.05.
RESULTS
Figure 1 illustrates multiple-time uptake plots for[3H]DPDPE and the vascular space marker [‘4C]-sucrose into the CNS. These results indicate a progres-sive uptake of [3HJDPDPE, which is significantlygreater than that of [‘4C I sucrose into the brain (p<0.0!) and CSF (p < 0.05). In addition, after consid-ering [‘4C] sucrose/vascular space, [3H]DPDPE up-take into the brain is ‘-—57% greater than that into theCSF(p <0.01).
Table I shows the brain unidirectional transfer con-stants (K~
0)and the initial volume of distribution (V,)for [
3HIDPDPE and [‘4Clsucrose, which were deter-mined from the computed lines of regression in Fig. I,i.e., multiple-time uptake analysis/three-compartmentmodel. Table 1 also shows the blood-to-brain and theblood-to-CSF transfer constants derived by the two-compartment/single-time uptake model. As shown, the
J. Neurochem., Vol. 66, No. 3, 1996
![Page 5: Passage of a δ-Opioid Receptor Selective Enkephalin, [d-Penicillamine2,5]Enkephalin, Across the Blood-Brain and the Blood-Cerebrospinal Fluid Barriers](https://reader038.pdfslide.tips/reader038/viewer/2022100510/5750243f1a28ab877eadf13a/html5/thumbnails/5.jpg)
BRAIN AND CSF ENTRY OF DPDPE 1293
TABLE 1. Calculated unidirectional transfer constants(K,,,) and initial volumes ofdistribution (V,) for
[3H]DPDPE and [‘4C]sucrose into brain and CSF
Brain CSF
K,,,K
0 V,
Isotope (©l min~g~) (ml 100 g~) (jsl min~g’)
[‘4ClSucrose 0.16 ±0.080 1.66 ±0.15 —
— — 0.70 ±026°[~H]DPDPE 1.46 ±0.310
2.26 ±0.20’3.60 ±0.58
—
—
0.99 ±0.29°
Data are mean ±SEM values.“Determined by multiple-time uptake analysis (Fig. 1). n = 27
animals.Determined by single-time uptake analysis at a perfusion time
of30 mm (brain value is corrected for vascular space). n = 3 animals.Determined by single-time uptake analysis as described above.
n = 5 animals.
brain K0 value determined by single-time uptake anal-
ysis was similar to that determined by multiple-timeuptake analysis. In addition, the K10 value for [
3H] -
DPDPE into the CSF is only 68% of its rate of uptake(three-compartment model) into the brain. It is inter-esting to note that the initial volume of distribution(V,) is approximately two times higher for [3H] -
DPDPE (MW 645.8) than for [‘4C]sucrose (MW342.3).
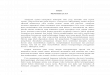
The effect of an excess of unlabeled DPDPE or!eucine-enkephalin on the uptake of [3HIDPDPE intothe brain and the CSF is illustrated in Fig. 2. Theseresults indicate that [3H] DPDPE is significantly self-inhibited by 26% into the brain (p <0.01 by Student’s
FIG. 2. Uptake of [3H]DPDPEin the absence (LI) and presenceof 100 ©M unlabeled DPDPE (U) or 1 mM unlabeled leucine-enkephalin (~)into the brain and CSF. Uptake is expressed asa percent ratio of tissue to perfusate radioactivities (Rr,suoe orRIflh~b~~,OO;ml g~or ml ml), and [14C]sucrose/vascularspacehas been subtracted from the brain values. Perfusion time was20 mm. Data are mean ±SEM (bars) values for three to sevenanimals. “p < 0.01 by Students’ t test for the difference betweenlabeled only and 100 ©M unlabeled DPDPE.
TABLE 2. Contribution of the vascular component tototal brain uptake of [3H]DPDPE
RT~,,0,(%)
[3H]DPDPE Supernatant Homogenate Pellet
Only (n = 6) 4.31 ±0.74 5.06 ±0.74°+ 100
1jM DPDPE(n = 7) 2.60 ±0.32 3.17 ±0.290
0.63 ±0.53°
0.55 ±0.58’
RT,,0, (%) represents the ratio of tissue to plasma radioactivities>< 100. Supernatant is brain homogenate, which has undergone dcx-tran density centrifugation to produce the cerebral capillary-enrichedpellet. Data are mean ±SEM values. Perfusion time is 20 mm, andn is the number of experiments.
The supernatant means were compared by paired Stu~6nt’st testto the homogenate and pellet means: 0 not significantly differentfrom each other, “p < 0.001, ‘p < 0.01.
t test). However, there is no significant difference inthe uptake of [
3H] DPDPE into the CSF in the absenceor presence of 100 ,uM unlabeled DPDPE. In addition,there was no effect on the uptake of radiolabeledDPDPE with 1 mM leucine-enkephalin being presentin the perfusion medium.
To ensure that the measured radioactivity in the
FIG. 3. HPLC/Flo-One Radioactive Detector chromatograms of[3H]DPDPEfrom the arterial perfusion medium (top) and thevenous outflow (bottom). Venous outflow samples were takenat 20 mm after the start of perfusion.
.1. Neurochem., Vol. 66, No. 3, 1996
![Page 6: Passage of a δ-Opioid Receptor Selective Enkephalin, [d-Penicillamine2,5]Enkephalin, Across the Blood-Brain and the Blood-Cerebrospinal Fluid Barriers](https://reader038.pdfslide.tips/reader038/viewer/2022100510/5750243f1a28ab877eadf13a/html5/thumbnails/6.jpg)
1294 S. A. WILLIAMS ET AL.
the brain sample (Fig. 4). A percentage of the radioac-tivity was also detected in the solvent front of both thestandard and brain samples, i.e., 3 and 7%, respec-tively.
Octanol/saline partition coefficients for [3HI-DPDPE were 0.076 ±0.002 compared with a valueof 0.00050 ±0.00003 for [‘4C]sucrose. Bovine serumalbumin binding of [3H I DPDPE was negligible, with>97% remaining in the free form, and as was expected
li’4C]sucrose did not bind to bovine serum albumin
(Table 3).
DISCUSSION
FIG. 4. HPLC/Flo-One Radioactive Detector chromatograms ofa radioactive standard (top) and an acid/ether extraction ofpooled brains (n = 2) that had been in situ-perfused with [3H]-DPDPE for 30 mm (bottom).
brain was actually due to brain uptake of [3HIDPDPEand notjust [3HI DPDPE accumulation within the cere-bral vasculature, a capillary depletion step was carriedout. As can be seen inTable 2, there was no significantdifference in the amount of radioactivity for [3H1-DPDPE found in the brain homogenate and in the su-pernatant in either the absence or the presence of unla-beled DPDPE. In addition, the amount of radioactivitydetected in the vasculature-enriched pellets was smalland significantly lower than that detected in the super-natants.
Figure 3 illustrates the extraction of [3H]DPDPE inthe perfusion medium before (arterial inflow) and after(venous outflow) it had passed through the cerebralcirculation. As can be seen, both samples eluted as asingle peak, with the retention times matching eachother as well as radioactive standards for this peptide.The extraction of intact [3HI DPDPE in the brain wasalso important in determining if the multiple-time up-take data actually represented intact peptide and notsolely metabolites or free radioactive counts (Fig. 4).After the longest experimental perfusion period, 30mm, ‘—~90%of the brain sample eluted as intact [3H]-DPDPE. A small radioactive peak was detected at 15.5mm and accounted for 3% of the total radioactivity in
Figure 1 illustrates the uptake of [‘4CI sucrose intothe brain and CSF determined using the in situ brainperfusion technique in anesthetized rats. These [‘4CI-sucrose experiments are in full agreement with thoseof Zlokovic et a!. (1992) and Ohno et al. (1978),where the brain unidirectional transfer constant, K,
0,and cerebral blood volume/vascular space were deter-mined as 0.28 ±0.08 p1 min~g
1 and 1.14 ±0.22 ml100 g ~, respectively (Table 1; multiple-time uptakeanalysis). This indicates that this highly water-soluble,nonmetabolizable carbohydrate, with an octanol/salinepartition coefficient of 0.00050 ± 0.00003, remainsmainly within the cerebral vascular space and confirmsthe integrity of the BBB during these experiments. Inaddition, the perfusion parameters, in terms of Po
2 andperfusion pressure, are similar to the values of Prestonet a!. (1995). The uptake of [
3HIDPDPE into thebrain, also illustrated in Fig. 1, is linear with time andis significantly greater than that for the vascular spacemarker [‘4CI sucrose. Furthermore, the blood-to-braintransfer constants (K
10 ~l mm — g~1) for [3HIDPDPE,
determined using multiple- and single-time uptakeanalysis, were relatively similar, being 1.46 ± 0.31and 2.26 ±0.20, respectively (Table 1).
When considering these results, it was importantto assess the data from the ultrafiltration centrifugaldialysis study, because it is known that protein bindingcan play a major factor in determining the CNS uptakeof certain peptides (Banks et al., 1990). As can be
TABLE 3. The percentage ofprotein-bound [3HJDPDPEand [‘4C]sucrose in theperfusion medium determined
using the levels of radioactivity found in the sample andultrafiltrate produced by ultrafiltration centrifugal dialysis
Perfusion medium (dpmlml)
[‘4C]Sucrose [3H]DPDPE
Sample 308,400 272,692Ultrafiltrate 307,650 264,658
% protein bound 0.25 ±0.05 2.95 ±0.29
The levels of radioactivity are the means of triplicate determina-tions. The percent protein bound data are mean ±SEM values.
J. Neurochem., Vol. 66, No. 3, 1996
![Page 7: Passage of a δ-Opioid Receptor Selective Enkephalin, [d-Penicillamine2,5]Enkephalin, Across the Blood-Brain and the Blood-Cerebrospinal Fluid Barriers](https://reader038.pdfslide.tips/reader038/viewer/2022100510/5750243f1a28ab877eadf13a/html5/thumbnails/7.jpg)
BRAIN AND CSF ENTRY OF DPDPE 1295
seen in Table 3, because [3HIDPDPE and [‘4CI-sucrose remained predominantly unbound to the bo-vine serum albumin in the perfusion medium, it wouldappear that the data in Fig. 1 are not underestimationsof the true uptake values.
Owing to their lipophilicity, peptide molecules mayenter into endothelia! cells without leaving them at theabluminal side, or they may be otherwise anchored atcellular components (Ermisch et a!., 1993; Z!okovicet al., 1993). The capillary depletion technique devel-oped by Triguero et a!. (1990) and used previously byZlokovic et a!. (1992), in combination with the insitu brain perfusion technique, allows examination of[3H]DPDPE accumulation by the capillary endothe-hum cells. In the present study (Table 2), it was foundthat after 20 mm of vascular brain perfusion, theamount of radioactivity in the brain homogenates wasnot significantly different from that obtained in thesupernatants and was much higher than that found ac-cumulated within the capillary endothelium-enrichedpellets. In conclusion, it would appear that [3H]-DPDPE accumulation within the cerebral capillary en-dothelial cells is negligible, in comparison with theoverall brain uptake.
The in situ brain perfusion technique reduces thepossibility of tritium exchange with water influencingthe [3H] DPDPE uptake data, by the use of an enzyme-free artificial plasma perfusate and also by preventingrecirculation of the perfusion medium. The resultsfrom this study (Fig. 3) also confirm that there is littledissociation of the 3H label from DPDPE during itsrapid passage through the cerebral circulation. In addi-tion, HPLC analysis has also revealed that the majority,i.e., 90%, of II3HIDPDPE remains intact in the brainafter an intracarotid artery perfusion period of 30 mm(Fig. 4). It is interesting to note that although a smallradioactive peak, i.e., 3%, was detected at 15.5 mm inthe brain sample, the majority of the radioactivity notassociated with intact [3H I DPDPE eluted with the sol-vent front, i.e., 7%, which does suggest the presenceof tritiated water. However, it is not known where thisdisplacement of tritium occurred. It is plausible that inthis present study, intact [3HI DPDPE actually crossedthe BBB and b!ood-CSF barrier (Fig. 3), and the tn-tium was displaced once it had reached the brain.
Figures 3 and 4 also indicate that DPDPE is predom-inantly notmetabolized in its passage through the cere-bral circulation, nor once it has actually reached thebrain. This confirms previously published studies fromthis laboratory, which demonstrated the inherent stabil-ity of 3H I DPDPE in the kidney, liver, small intestine,serum, and cytosolic endothelial space of the in vitroBBB (Weber et a!., 1991, 1992; Brownson et a!.,1994).
Together the results discussed above provide evi-dence that this radiolabeled enkephalin analogue cancross the BBB. This conclusion is in contrast to thatof Shook et a!. (1987), whereby no analgesic effect
was elicited after subcutaneous administration ofDPDPE (10 mg/kg), and it was inferred that this pep-tide could not cross the BBB. It should be emphasizedthat the analgesia study by Shook et al. (1987) usedmice and the present work has used rats; therefore,species differences may exist, making extrapolationdifficult. For example, although analgesia is producedby DPDPE administration in rats, the density of opioidbinding sites selective for DPDPE is smaller in brainsfrom the rat than the mouse, and this, in turn, parallelsthe potency of DPDPE in the two species (Yoburn eta!., 1991). However, Weber et a!. (1991) found thatsignificant analgesia was only produced after intrave-nous administration of high doses of DPDPE in mice(30 and 60 mg/kg), suggesting that at least some intactDPDPE crossed the BBB. Thus, it is likely that thelack of BBB penetration observed by Shook et a!.(1987) has more to do with too low a concentration ofDPDPE reaching the plasma than species differencesbetween the studies. This low bioavailability may bethe result of a rapid disappearance of DPDPE from thesite of administration to other organs, for example, thekidney and liver (Weber et al., 1992). It could alsobe due to a lack of absorption of DPDPE into thecirculation, although previous work in this laboratoryfound that there were similar concentrations of [3H I -
DPDPE in the blood, 15 and 120 mm after intravenousand subcutaneous administration, respectively (Weberet a!., 1992). In fact, there were significantly higherlevels of radiolabeled DPDPE in the blood, 60 mmafter the subcutaneous injection. Catabolism of thecompound could also be afactor; however, consideringthe inherent stability of DPDPE, this seems unlikely(Figs. 3 and 4) (Weber et a!., 1991, 1992; Brownsonet a!., 1994).
The initial volume of distribution (V,) is approxi-mately two times higher for [3HIDPDPE (MW 645.8)than for [14CI sucrose (MW 342.3) (Table 1). As therewas no large difference in the amounts of [3H]DPDPEor [‘4Clsucrose found accumulated within the mi-crovessel compartment of the brain (Table 2) or in theamounts that were protein bound (Table 3), it wouldappear that these differences in the V
1 values mayreflect differences in lipid solubility. The octanol/sa-line partition coefficient for [
3H] DPDPE was 0.076±0.002 compared with a value of 0.00050 ±0.00003for [14Cj sucrose.
In contrast to the brain uptake of [‘4Clsucrose,which represents both the vascular space and diffusionthrough the paracellular pathways of the cerebral endo-thelium, the CSF uptake of [14CI sucrose only repre-sents diffusion through the paracellular pathways ofthe choroid plexus. The uptake of [3HIDPDPE intothe CSF was significantly greater (p < 0.05) than theCSF uptake of [14C]sucrose (Fig. 1). However, afterconsidering vascular space, brain uptake of [3H] -
DPDPE is still significantly greater than the CSF up-take of this peptide by ‘-—57%. Although it is appreci-
J. Neurochem., Vol. 66, No. 3, 1996
![Page 8: Passage of a δ-Opioid Receptor Selective Enkephalin, [d-Penicillamine2,5]Enkephalin, Across the Blood-Brain and the Blood-Cerebrospinal Fluid Barriers](https://reader038.pdfslide.tips/reader038/viewer/2022100510/5750243f1a28ab877eadf13a/html5/thumbnails/8.jpg)
1296 S. A. WILLIAMS ET AL.
ated that in this in situ study the total separation acrosseither the BBB or the blood—CSF barrier is not possi-ble, it would appear unlikely that the blood—CSF routecould supply the brain with enough DPDPE to producethe level of 3H activity observed in these experiments.This conclusion is reached because it has been calcu-lated that the surface area of the BBB is greater thanthat of the blood—CSF barrier at the choroid plexuses,suggesting a greater importance of the BBB in control-ling the environment of the brain (Bradbury, 1979;Pardnidge, 1983; Keep and Jones, 1990). In addition,the rate of bulk flow of the CSF out of the ventriclesis considered faster than the diffusion kinetics fromthis fluid into the brain (Collins and Dedrick, 1983).Thus, the CSF is more likely to act as a sink to thebrain than the brain acting as a sink to the CSF (Davsonet al., 1961). In addition, if the CSF is the exclusivesource of a substance, high solute levels may be pro-duced at the ependymal—CSF surface, but there is asharp decrease in tissue concentrations as close as 0.2cm from the surface (Blasberg et a!., 1975). Thus, itis unlikely that DPDPE could penetrate to deep brainsites if, as Rapoport et al. (1980) postulated, theblood—CSF barrier was the main route for the uptakeof peptides into the brain. This is partly due to thevery slow turnover of brain extracellular fluid (Cserret a!., 1981; Szentesvanyi et a!., 1984) but can also berelated to uptake or receptor binding by the brain cellsclose to the ependyma. This is likely to occur in thecase of DPDPE a~there is a high density of 6-opioidreceptors in the caudate putamen (Mansour et a!.,1995).
It is known that peptides can enter and exit the CNSby several methOds that can be nonsaturable, such astransmembrane diffusion or fluid-phase endocytosis,as we!! as saturable, absorptive-, carrier-, or receptor-mediated transcytosis (Poduslo et a!., 1994). By farthe most common of the saturable transport systemsare carrier and receptor mediated (Brownlees and Wil-liams, 1993).
Several independent saturable mechanisms thattransport peptides from blood to brain have been char-acterized. Leucine-enkephalin, glutathione, delta sleep-inducing peptide, and arginine-vasopressin uptake atthe luminal membrane of the BBB has been shown tobe saturable (Zlokovic et a!., 1989a,b, 1990, 1994;Kannan et a!., 1992). In addition, studies have identi-fied saturable carrier systems for blood to brain trans-port of D- [Ala’ I -peptide T-amide and bidirectionaltransport of luteinizing hormone-releasing hormone(Barrera et a!., 1987, 1991). Receptor-mediated trans-port systems have been suggested at the BBB for insu-lin (Pardridge et a!., 1985) and transfernn (Fishmaneta!., 1987). In addition, absorptive-mediated endocy-tosis has also been indicated for a dynorphin-like anal-gesic peptide, E-2078 (Terasaki et a!., 1989), an adre-nocorticotropic hormone analogue, ebiratide (Shimuraet al., 1991), and cationized albumin (Kumagai eta!.,
1987). Saturable systems, which could be for the bloodto CSF transport of leucine-enkephalin, arginine-vaso-pressin, and 6 sleep-inducing peptide, have also beendescribed at the blood—tissue interface of the choroidplexus and may provide a pathway for passage of pep-tides from blood to the brain tissue (Zlokovic et al.,1988a,b, 1991).
To determine whether or not any part of the brainor CSF uptake of [3H I DPDPE was by a saturable com-ponent, the effect of an excess of unlabeled DPDPEwas examined. These self-inhibition studies revealedthat although the uptake of [3H I DPDPE into the braincould be inhibited by 26%, the CSF uptake was notaffected (Fig. 2). This would suggest that tritiatedDPDPE can use a saturable transport system to enterthe brain, and because entry into the CSF is purely bya nonsaturable process, this saturable system is mostlikely to be found at the BBB.
Because no saturable system could be identified forthe CSF uptake of this enkephalin analogue (Fig. 2)and there is a significant difference between the uptakeof [3H]DPDPE and [‘4Clsucrose into the CSF (Fig.1), it is likely that [3H I DPDPE can enter the CSF bydiffusion through the choroid plexus epithelial cell.This ability can be related to the higher octanol salinepartition coefficient of [3H] DPDPE compared with[‘4C]sucrose, as it has been shown that lipophilicityis extremely important in determining the penetrationof substances, including peptides, across the BBB(Banks and Kastin, 1985). An example of the effectof lipophilicity is also thought to explain the larger V
1value determined for [
3H I DPDPE in this present study(Table 1). However, although there is a significantdifference in the uptake of DPDPE and sucrose intothe CSF, it is smaller than might be expected consider-ing the >10-fold difference in lipophilicity. This couldbe related to the lower molecular size of sucrose andthe higher permeability of the choroidal epitheliumover the cerebral endothelium (Bouldin and Krigman,1975).
Saturable systems usually transport a group ofclosely related compounds, and it was possible that thesystem identified in our present study for [3H I DPDPEwas in fact the carrier, which was identified for theblood-to-brain transport of the endogenous leucine-en-kephalin (Z!okovic et al., 1989a; Banks and Kastin,1990). A earner for leucine-enkephalin has also beenidentified at the luminal membrane of the choroidplexus of the sheep (Zlokovic eta!., 1988a). However,Fig. 2 indicates that [3HI DPDPE does not use the samesaturable transport system as leucine-enkephalin to en-ter the CNS. This is also confirmed by the self-inhibi-tion study for [3H I DPDPE because no saturable uptakesystem could be identified at the blood—CSF barrier,in contrast to the previous study for leucine-enkephalin(Zlokovic et al., 1988a).
This laboratory has previously studied the passageof DPDPE across the BBB using both in vitro and
J. Neurochem., Vol. 66, No. 3, 1996
![Page 9: Passage of a δ-Opioid Receptor Selective Enkephalin, [d-Penicillamine2,5]Enkephalin, Across the Blood-Brain and the Blood-Cerebrospinal Fluid Barriers](https://reader038.pdfslide.tips/reader038/viewer/2022100510/5750243f1a28ab877eadf13a/html5/thumbnails/9.jpg)
BRAIN AND CSF ENTRY OF DPDPE 1297
in vivo methods (Weber et al., 1991, 1992, 1993).Assuming that the surface area of the cerebral capillar-ies is -—100cm2g~’,thena cerebrovascular permeabil-ity constant (P; cm min’) can be determined fromthe unidirectional transfer constants, K,
0, in Table I(Bradbury, 1979). The rate of uptake of [
3H I DPDPEinto the brain (Table I) can thus be expressed as apermeability constant with a value of 1.46 X l0~ cmmm’. In contrast, Weber et al. (1993) determined apermeability coefficient of 4.92 X l0~ cm min~ forthe passage of DPDPE across the in vitro BBB. This336-fold difference is somewhat larger than the 150-fold difference between in vivo and in vitro valuesobserved by Pardridge et a!. (1990). However, thislatter study did indicate that this correlation was onlyvalid for drugs that penetrated the BBB via lipid medi-ation, and, as shown in Fig. 2, the uptake of DPDPEinto the brain is by a saturable transport mechanism.In addition, this difference between the in vitro/in vivocorrelations is likely to be due to the different methodsused, for example, continuous versus primary cell cul-ture methods. As another comparison, a blood-to-brainK,. value was determined from the whole animal distri-bution study of Weber et al. (1991) and found to be0.48 ±0.24 j.tl min~g’. Although it is not the sameas that determined for [3H]DPDPE using the in situbrain perfusion method (Table 1), it is within a similarrange.
To summarize the conclusions obtained from thispresent study, it would seem that [3H]DPDPE entersthe CNS of anesthetized rats by both saturable andnonsaturable mechanisms. It would appear that the sat-urable mechanism is most likely to be found at theBBB, with theblood—CSF barrier playing only a minorrole in the brain uptake of this enkephahin analogue.In addition, this saturable system for [3H 1 DPDPE doesnot transport leucine-enkephalin. Future studies areplanned, both to characterize this saturable mechanismand to develop DPDPE analogues, which can take ad-vantage of the systems identified in this study.
Acknowledgment: This work is supported by grant DA06284 from the National Institutes of Health. SAW, wouldlike to thank The Wellcome Trust, London, U.K. for provid-ing a travel award to allow this work to be undertaken. Theauthors would like to thank Mr. Vincent Hau for his technicalassistance in determining the octanol-saline partition coeffi-cients.
REFERENCES
Audus K. L., Chikhale P. J., Miller D. W., Thompson S. E., andBorchardt R. T. (1992) Brain uptake of drugs: the influence ofchemical and biological factors. Adv. Drug Res. 23, 1—64.
Banks W. A. and Kastin A. J. (1985) Peptides and the blood—brainbarrier: lipophilicity as a predictor of permeability. Brain Res.Bull. 15, 287—292.
Banks W. A. and Kastin A. J. (1987) Saturable transport of peptidesacross the blood—brain barrier. Life Sci. 41, 1319—1338.
Banks W. A. and Kastin A. J. (1990) Peptide transport systems for
opiates across the blood—brain barrier. Am. J. Physiol. 259,El-ElO.
Banks W. A., Schally A. V., Barrera C. M., Fasold M. B., DurhamD. A., Csernus V. J., Groat K., and Kastin A. J. (1990) Perme-ability of the murine blood—brain barrier to some octapeptideanalogs of somatostatin. Proc. Natl. Acad. Sci. USA 87, 6762—6766.
Banks W. A., Kastin A. J., and Davis T. P. (1992) Permeability ofthe blood—brain barrier to peptides: an approach to the develop-ment of therapeutically useful analogs. Peptides 13, 1289—1294.
Barré J., Chamouard J. M., Houin G., and Tillement J. P. (1985)Equilibrium dialysis, ultrafiltration and ultracentrifugation com-pared for determining the plasma-protein-binding characteris-tics of valproic acid. Gun. Chem. 31, 60—64.
Barrera C. M., Kastin A. J., and Banks W. A. (1987) D-[Ala’]-peptide T-amide is transported from brain to blood by a satura-ble mechanism. Brain Res. Bull. 19, 629—633.
Barrera C. M., Kastin A. J., Fasold M. B., and Banks W. A. (1991)Bi-directional saturable transport of LHRH across the blood—brain barrier. Am. J. Physiol. 261, E3l2—E318.
Begley D. J., Squires L. K., Zlokovi~B. V., Mitrovi~D. M., HughesC. C. W., Revest P. A., and Greenwood J. (1990) Permeabilityof the blood—brain barrier to the immunosuppressive cyclicpeptide cyclosporin A. J. Neurochem. 55, 1222—1230.
Blasberg R., Patlak C. S., and Fenstermacher J. D. (1975) Intrathecalchemotherapy: brain tissue profiles after ventriculo-cisternalperfusion. J. Pharmacol. Exp. Thor. 195, 78—83.
Blasberg R. G., Fenstermacher J. D., and Patlak C. S. (1983) Trans-port of a-aminoisobutyric acid across brain capillary and cellu-lar membranes. J. Cereb. Blood Flow Metab. 3, 8—32.
Bouldin T. W. and Krigman M. R. (1975) Differential permeabilityof cerebral capillary and choroid plexus to lanthanum ion. BrainRes. 99, 444—448.
Bowman P. D., Ennis S. R., Rarey K. E., Betz A. L., and GoldsteinG. w. (1983) Brain microvessel endothelial cells in tissue cul-ture: a model for study of blood—brain barrier permeability.Ann. Neurol. 14, 396—402.
Bradbury M. W. B. (1979) The Concept ofa Blood—Brain Barrier.Wiley, Chichester.
Broadwell R. D. (1989) Transcytosis of macromolecules throughthe blood—brain barrier: a cell biological perspective and criticalappraisal. Acta Neuropathol. (Ben.) 79, 117—128.
Brownlees J. and Williams C. H. (1993) Peptidases, peptides, andthe mammalian blood—brain barrier. J. Neurochem. 60, 793—803.
Brownson E. A., Abbruscato T. J., Gillespie T. J., Hruby V. 1., andDavis T. p. (1994) Effect of peptidases at the blood—brainbarrier on the permeability of enkephalin. J. Pharmacol. Exp.Thor. 270, 675—680.
Collins 1. M. and Dedrick R. L. (1983) Distributed model for drugdelivery to CSF and brain tissue. Am. J. Physiol. 245, R303—R3l0.
Collins 1. M., Klecker R. W., Kelley J. A., Roth J. S., McCullyC. L., Balis F. M., and Poplack D. 0. (1988) Pyrimidine di-deoxynucleosides: selectivity of penetration into cerebrospinalfluid. J. Pharmacol. Exp. Thor. 245, 466—470.
Cserr H. F., Cooper D. N., Sun P. K., and Patlak C. 5. (1981)Efflux of radiolaheled polyethylene glycols and albumin fromrat brain. Am. J. Physiol. 240, F319—F328.
Davis T. P. (1990) Methods of measuring neuropeptides and theirmetabolism, in The Roles ofNeuropeptides in Stress Pathogene-sis and SystemicDisease (Kaufman P. G., McCubbin J. A., andNemeroff C. B., eds), pp. 149—177. Academic Press, Orlando,Florida.
Davson H., Kleeman C. R., and Levin E. (1961) Blood—brain barrierand extracellular space. J. Physiol. (Lond.) 159, 67P—68P.
Emmerson P. J., Liu M.-R., Woods J. H., and Medzihradsky F.(1994) Binding affinity and selectivity of opioids at mu, deltaand kappa receptors in monkey brain membranes. J. Pharma-col. Exp. Thor. 271, 1630—1637.
J. Neurochem., Vol. 66, No. 3, /996
![Page 10: Passage of a δ-Opioid Receptor Selective Enkephalin, [d-Penicillamine2,5]Enkephalin, Across the Blood-Brain and the Blood-Cerebrospinal Fluid Barriers](https://reader038.pdfslide.tips/reader038/viewer/2022100510/5750243f1a28ab877eadf13a/html5/thumbnails/10.jpg)
1298 S. A. WILLIAMS ET AL
Erchegyi J., Kastin A. J., Zadina J. E., and Qiu X.-D. (1991) Isola-tion of a heptapeptide Val-Val-Tyr-Pro-Trp-Thr-Gln (valor-phin) and some opiate activity. mt. J. Pept. Protein Res. 39,477—488.
Ermisch A., Brust P., Kretzschmar R., and Ruhle H.-J. (1993) Pep-tides and the blood—brain barrier. Physiol. Rev. 73, 489—527.
Fishman J. B., Rubin J. B., Handrahan J. V., Connor J. R., andFineR. E. (1987) Receptor-mediated transcytosis of transferrinacross the blood—brain barrier. J. Neurosci. Res. 18, 299—304.
Frederickson R. C. A., Smithwick E. L., Shuman R., and BemisK. G. (1981) Metkephamid, a systemically active analog ofmethionine enkephalin with potent opioid d-receptor activity.Science 211, 603—605.
Galligan J. J., Mosberg H. I., Hurst R., Hruby V. J., and Burks T. F.(1984) Cerebral delta opioid receptors mediate analgesia butnot the intestinal motility effects of intracerebroventricularlyadministered opioids. J. Pharmacol. Exp. Ther. 229, 641—648.
Gjedde A. (1981) High- and low-affinity transportof D-glucose fromblood to brain. J. Neurochem. 36, 1463—1471.
Gjedde A. (1982) Calculation of cerebral glucose phosphorylationfrom brain uptake of glucose analogues in vivo: a re-examina-tion. Brain Ret. 4, 237—274.
Hambrook J. M., Morgan B. A., Rance M. J., and Smith C. F.(1976) Mode of deactivation of the enkephalins by rat andhuman plasma and rat brain homogenates. Nature 262, 782—783.
Heyman J. S., Mulvaney S. A., Mosberg H. I., and Porreca F. (1987)Opioid 6-receptor involvement in supraspinal and spinal anti-nociception in mice. Brain Ret. 420, 100—108.
Hruby V. J., Toth G., Gehring C. A., Kao L.-F., Knapp R., LuiG. K., Yamamura H. I., Galligan J. J., Kramer T. H., DavisT. P., and Bunks T. F. (1991) Topographically designed ana-logues of ED-Pen 2,D-Pen5] enkephalin. J. Med. Chem. 34,1823—1830.
Kannan R., Kuhlenkamp J. F., Cokhtens M., and Kaplowitz N.(1992) Transport of glutathione at blood—brain barrier of therat: inhibition by glutathione analogs and age dependence. J.PharmacoL Esp. Ther. 263, 964—970.
Keep R. F. and Jones H. C. (1990) A morphometric study on thedevelopment of the lateral ventricle choroid plexus, choroidplexus capillaries and ventricular ependyma in the rat. Dev.Brain Res. 56, 47—53.
Kumagai A. K., Eisenberg J. B., and Pardridge W. M. (1987) Ab-sorptive-mediated endocytosis of cationized albumin and a /3-endorphin-cationized albumin chimeric peptide by isolatedbrain capillaries. J. Biol. Chem. 262, 15214—15219.
Lord J. A. H., Waterfield A. A., Hughes J., and Kosterlitz H. W.(1977) Endogenous opioid peptides: multiple agonists and re-ceptors. Nature 267, 495 —499.
Lowry 0. H., Rosebrough N. J., Fan A. L., and Randall R. J. (1951)Protein measurements with the Folin phenol reagent. J. Biol.Chem. 193, 265—275.
Mansour A., Fox C. A., Akil H., and Watson S. J. (1995) Opioid-receptor mRNA expression in the rat CNS: anatomical andfunctional implications. Trends Neurosci. 18, 22—29.
Martin W. R., Eades C. G., Thompson J. A., Huppler R. E., andGilbert P. E. (1976) The effects of morphine and nalorphine-like drugs in the non-dependent and chronically dependentchronic spinal dog. J. Pharmacol. Exp. Ther. 197, 517—532.
Mosberg H. I., Hurst R., Hruby V. J., Gee K., Yamamura H. I.,Galligan J. J., andBurks T. F. (1983) Bis-penicillamine enkeph-alms possess highly improved specificity toward delta opioidreceptors. Proc. Nail. Acad. Sci. USA 80, 5871—5874.
Ohno K., Pettigrew K. D., and Rapoport S. I. (1978) Lower limitsof cerebrovascular permeability to non-electrolytes in the con-scious rat. Am. J. Physiol. 235, H299—H307.
Pandridge W. M. (1983) Brain metabolism: a perspective from theblood—brain barrier. Physiol. Rev. 63, 1481—1535.
Pardridge W. M., Eisenberg J., and Yang J. (1985) Human blood—brain barrier insulin receptor. J. Neurochem. 44, 1771—1778.
Pardridge W. M., Triguero D., Yang J., and Cancilla P. A. (1990)Comparison of in vitro and in viva models of drug transcytosisthrough theblood—brain barrier. J. Pharmacol. Exp. Ther. 253,884—891.
Patlak C. S., Fenstermacher J. D., and Blasberg R. G. (1983) Graphi-cal evaluation of blood—brain barrier transfer constants frommultiple-time uptake data. .1. Cereb. Blood Flow Metab. 3, 1—7.
Paulus H. (1969) A rapid and sensitive method for measuring thebinding of radioactive ligands to proteins. Anal. Biochem. 32,91— 100.
Pert C. B. and Snyder S. H. (1973) Opiate receptor: demonstrationin nervous tissue. Science 179, 1011—1014.
Poduslo J. F., Curran G. L., and Berg C. T. (1994) Macromolecularpermeability across the blood—nerve and blood—brain barriers.Proc. NatI. Acad. Sci. USA 91, 5705—5709.
Porreca F., Mosberg H. I., Hurst R., Hruby V. J., and Burks R. F.(1984) Roles of mu, delta and kappa opioid receptors in spinaland supraspinal mediation of gastrointestinal transit effects andhot-plate analgesia in the mouse. J. Pharmacol. Exp. Ther. 230,341—348.
Preston J. E., Al-Sarraf H., and Segal M. B. (1995) Permeability ofthe developing blood—brain barrier to 4C-mannitol using therat in situ brain perfusion technique. Dev. Brain Res. 87, 69—76.
Rapoport S. I., Klee W. A., Pettigrew K. D., and Ohno K. (1980)Entry of opioid peptides into the central nervous system. Science207, 84—86.
Shimura T., Tabata S., Ohnishi T., Terasaki T., and Tsuji A. (1991)Transport mechanism of a new behaviorallyhighly potent adre-nocorticotropic hormone (ACTH) analog, ebiratide, through theblood—brain barrier. J. Pharmacol. Exp. Ther. 258, 459—465.
Shook J. E., Pelton J. T., Hruby V. J., and Bunks T. F. (1987)Peptide opioid antagonist separates peripheral andcentral opioidantitransit effects. J. Pharmacol. Exp. Thor. 243, 492—500.
Smith Q. R. and Rapoport S. I. (1986) Cerebrovascular permeabilitycoefficients to sodium, potassium and chloride. J. Neurochem.46, 1732—1742.
Szentesvanyi I., Patlak C. S., Ellis R. A., and Cserr H. F. (1984)Drainage of interstitial fluid from different regions of the ratbrain. Am. J. Physiol. 246, F835—F844.
Terasaki T., Ichihirai K., Sato H., Kang Y. S., and Tsuji A. (1989)Absorptive-mediated endocytosis of a dynorphin-like analgesicpeptide, E-2078, into the blood—brain barner. J. Pharmacol.Exp. Ther. 251, 35 1—357.
Triguero D., Buciak J., and Pardnidge W. M. (1990) Capillary deple-tion method for quantification of blood—brain barrier transportof circulating peptides and plasma proteins. J. Neurochem. 54,1882—1888.
Vanderah T., Takemori A. E., Sultana M., Portoghese P. S., MosbergH. I., Hruby V. J., Haaseth R. C., Matsunaga T. 0., and PorrecaF. (1994) Interaction of [D-Pen2,D-Pen5lenkephalin and [o-Ala2,G1u4] deltorphin with 6-opmoid receptor subtypes in vivo.Eur. J. Pharmacol. 252, 133—137.
Ward S. J. and Takemori A. E. (1983) Relative involvement ofmu, kappa and delta receptor mechanisms in opiate-mediatedantinociception in mice. J. Pharmacol. Exp. Ther. 224, 525—530.
Weber S. J., Greene D. L., Sharma S. D., Yamamura H. I., KramerT. H., Burks T. F., Hruby V. J., Hersh L. B., and Davis T. P.(1991) Distribution and analgesia of [3H] ED-Pen2,D-Pen 5]~
enkephalin and two halogenated analogs after intravenous ad-ministration. J. Pharmacol. Exp. Ther. 259, 1109—1117.
Weber S. J., Greene D. L., Hruby V. J., Yamamura H. I., PorrecaF., and Davis T. P. (1992) Whole body and brain distributionof [3HIcyclic ED-Pen2,o-Pen5 ] enkephalmn after intrapenitoneal,intravenous, oral and subcutaneous administration. J. Pharma-col. Exp. Ther. 263, 1308—1316.
Weber S. J., Abbruscato T. J., Brownson E. A., Lipkowski A. W.,Polt R., Misicka A., Haaseth R. C., Bartosz H., Hruby V. J.,
.1. Neurachem., Vol. 66, No. 3, 1996
![Page 11: Passage of a δ-Opioid Receptor Selective Enkephalin, [d-Penicillamine2,5]Enkephalin, Across the Blood-Brain and the Blood-Cerebrospinal Fluid Barriers](https://reader038.pdfslide.tips/reader038/viewer/2022100510/5750243f1a28ab877eadf13a/html5/thumbnails/11.jpg)
BRAIN AND CSF ENTRY OF DPDPE 1299
and Davis T. P. (1993) Assessment of an in vitro blood—brainbarrier model using several [Met
5 I enkephalin opioid analogs.J. Pharmacol. Exp. Thor. 266, 1649—1655.
Williams S. A., Davson H., and Segal M. B. (l993)Thymidine entryinto the brain and cerebrospinal fluid (CSF) of the anaesthetizedguinea-pig using the in situ brain perfusion technique. J. Phys-iol. (Lond.) 459, 178P.
Yoburn B. C., Lutfy K., and Candido J. (1991) Species differencesin p- and 6-opioid receptors. Eur. J. Pharmacol. 193, 105—108.
Zlokovic B. V., Begley D. J., Djuri6i~iB. M., and Mitrovic D. M.(1986) Measurement of solute transport across the blood—brainbarr~rin the perfused guinea-pig brain: method and applicationto N-methyl-a-aminoisobutynic acid. J. Neurochem. 46, 1444—1451.
Zlokovic B. V., Segal M. B., Dayton H., and Mitrovic D. M. (I 988a)Unidirectional uptake of enkephalins at the blood—tissue inter-face ofthe blood—cerebrospinal fluid barrier: a saturable mecha-nism. Regul. Pept. 20, 33—44.
Zlokovic B. V., Segal M. B., Davson H., and Jankov R. M. (1988b)Passage of delta sleep-inducing peptide (DSIP) across theblood—cerebrospinal fluid barrier. Peptides 9, 533—538.
Zlokovic B. V., Mackic J. B., Djunicic B. M., andDayton H. ( 1989a)Kinetic analysis of leucine-enkephalin cellular uptake at theluminal side of the blood—brain barrier of an in situ perfusedguinea-pig brain. J. Neurochem. 53, 1333—1340.
Zlokovic B. V., Susie V. T., Dayton H., Begley D. J., Jankov R. M.,Mitrovic D. M., and Lipovac M. N. (1989b) Saturable mecha-nism for delta-sleep-inducing peptide (DSIP) at the blood—brain barrier of the vascularly perfused guinea-pig brain. Pep-tides 10, 249—254.
Zlokovic B. V., Hyman S., McComb J. 0., Lipovac M. N., TangG., and Dayton H. (1990) Kinetics of arginine-vasopressinuptake at theblood—brain barrier. Biochim. Biophys. Acta 1025,191— 198.
Zlokovic B. V., SegalM. B., McComb J. G., Hyman S., WeissM. H.,and Davson H. (1991) Kinetics of circulating vasopressin bychoroid plexus. Am. J. Physiol. 260, F216—F224.
Zlokovic B. V., Banks W. A., Kadi H. E., Erchegyi J., Mackic J. B.,McComb J. G., and Kastin A. J. (1992) Transport, uptake andmetabolism of blood-bourne vasopressin by the blood—brainbarrier. Brain Res. 590, 213—218.
Zlokovic B. V., Ghiso J., Mackic J. B., McComb J. G., Weiss M. H.,and Frangione B. (1993) Blood—brain barrier transport ofcircu-lating Alzheimer’s amyloid /3. Biochem. Biophys. Res. Com-mun. 197, 1034—1040.
Zlokovic B. V., Mache J. B., McComb J. G., Weiss M. H., Kaplo-witz N., and Kannan R. (1994) Evidence for transcapillarytransport of reduced glutathione in vascular perfused guinea-pig. Biochem. Biophys. Res. Commun. 201, 402—408.
i. Neurochem., Vol. 66, No. 3, 1996