Embed Size (px)
Citation preview

1
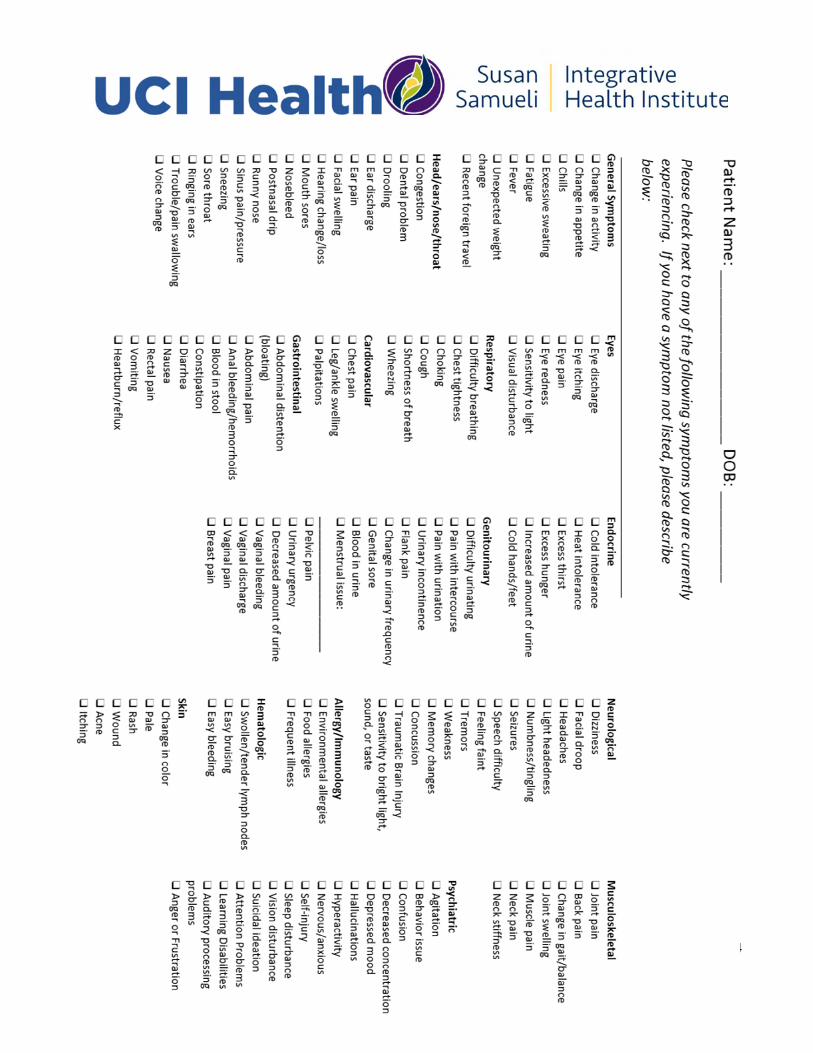
Patient History Form
Name: ______________________________ DOB: / / Age: ______
Preferred Pronouns (Circle all that apply): She, her, hers / he, him, his / they, them, theirs / Other: __________
How did you discover the Susan Samueli Integrative Health Institute? (Please check all that apply)
☐ Internet Search (Google) ☐ Social Media (Instagram, Facebook, etc.) ☐ Advertisement
☐ Insurance’s Provider Finder ☐ Reading an article ☐ Mail
☐ Event:______________ ☐ Friends, family member or colleague
☐ Referred by health provider: ________________ ☐ Other (please specify): ______________ Health Concerns to address today (in order of importance): Duration:
1. ____________________________________________ ________________ 2. ____________________________________________ ________________ 3. ____________________________________________ ________________
Providers currently involved in your care: Specialty: Phone: PCP: __________________ (___)_____________ Other: __________________ (___)_____________ Other: __________________ (___)_____________
Have you worked with integrative providers in the past? Yes _____ No ______ If yes, please list any treatments you’ve tried: _______________________________________________________ Are you currently taking prescription medications, vitamins, or nutritional supplements? Yes ___ No___
If yes, please complete attached sheet
PERSONAL & FAMILY HEALTH HISTORY
Date of most recent screening
(approximate if exact date is unknown)
Results Normal? (Y/N) If no, please provide brief information on findings
General physical exam
Lab work & urine test
Male – Prostate exam
Female – PAP & pelvic exam
Female – Breast imaging
Female – DEXA/bone density scan
Colonoscopy

2
Allergies (food, drug, or environmental) Please circle any that are life‐threatening
Allergen Reaction
______________________________________ ______________________________________ ______________________________________
______________________________________ ______________________________________ ______________________________________
Major Illnesses, hospitalizations, and/or surgical procedures (Including elective or cosmetic procedures)
Illness, Hospitalization or Procedure ______________________________________ ______________________________________ ______________________________________
Date ______________________________________ ______________________________________ ______________________________________
Please indicate if you or a family member has or has history of any of the following conditions: Family members include: Mother, Father, Daughter, Son, Maternal Grandmother, Maternal Grandfather, Paternal Grandmother, Paternal Grandfather, Sister, Brother, Other
Please check the box if you don’t know your family history
Assigned Female at birth patients: Last menstrual period: ___________ Age of first menstrual period: _____ Currently pregnant? ________ Currently breastfeeding? __________ Cycle length: ___________ Days of bleeding: ____ No. of pregnancies: ____ No. of children: ____ No. of miscarriages: ____ No. of abortions: ___
Condition Self Family Member Specify
from above list
Condition Self Family Member Specify
from above list
Current Previous Condition
Current Previous Condition
Allergies Epilepsy Alcoholism Heart attack Alzheimer’s Disease/Dementia
Heart disease
Anemia High cholesterol Anxiety Hypertension
Arthritis – rheumatoid/osteo Kidney disease
Autoimmune disorder Mental health disorder Blood disorder Obesity Cancer (type of cancer) Osteoporosis Depression Stroke Diabetes Thyroid disorder
(High/Low)

3
All patients: Average energy level (1‐10, 10 is highest): _____ Average stress level (1‐10, 10 is highest): ______ Sources of stress: __________________________________ Average hours asleep: ________ Typical bedtime: _________ Typical wake time: __________ Do you have issues with (circle): Falling asleep ∙ Staying asleep ∙ Frequent waking Do you exercise? _______ If so, how many times per week? _______ Approx. how long (minutes) ____________ Type of exercise: ____________________________________________________________________ Sample diet recall: Frequency of bowel movements ____________ Breakfast ______________________________ Consistency of stool: ______________________ Lunch: _________________________________ Dinner: ________________________________ Dietary Restrictions: ______________________ Snacks: ________________________________ Beverages: _____________________________ Pain: Do you experience frequent pain? Yes___ No___ If yes, please mark the areas on diagram and rate severity of the pain from 1‐10 (10 is most painful) ______ Please indicate if the pain is dull or sharp.
SOCIAL HISTORY (circle all that apply) Sexual Activity: Yes___ No___ Birth Control: ______________________________ Partners: Male___ Female ___ Do you drink alcohol: Never, Occasionally, Daily If yes: Beer, Wine, Liquor Number of drinks per day? ______ Do you consume Tobacco? Yes___ No____ If yes, how many years? ______ What form of tobacco: Cigarettes, Vaporizer, Chew, Cigar Number per day? _______ Quit date? __________ Recreational Drug use: Never, No current use, Occasional, Daily Uses per week? ______ What level of change to your lifestyle habits are you willing to make to improve your health & well‐being? Whatever it takes ∙ Significant change ∙ Some change ∙ No change
4

5
Prescription Medication, Vitamin & Supplement Information
Medication/supplement
Dose (include most recent dose adjustment if applicable)
Start date
Reason for taking
Frequency (approximately how many times do you
take it?)
Pharmacy: _______________________________________ ( )________________________ Name Telephone Number
Compound Pharmacy ___________________________________________ ( )___________________________ Name Telephone Number
6
Billing Providers
Insurance plans categorize acupuncturist, massage therapist, dietitians, and naturopathic doctors as allied health professionals. Allied health professionals must have a supervising physician in order to have their services covered by insurance and claims sent to the insurance must show them as the billing provider. Our office uses three different physicians to satisfy this requirement. Patients can expect to see, either on their bills or EOB, one of these three providers instead of the allied health professional seen in office.
Supplements
Nutritional supplements are not covered by insurance plans, as such our office is unable to bill insurances for them. Patients can use their FSA or HSA for payment provided that there are sufficient funds at the time of purchase and covered per your FSA or HSA guidelines. Our office encourages patients to keep their detailed receipts readily available in case the FSA or HSA plan requests documentation of purchase.
Laboratory Testing
Our providers will frequently order specialty labs to provide the best tailored care. These labs are processed by outside laboratories that are not directly affiliated with UCI Health or the Susan Samueli Integrative Health Clinic, as such our office does not bill for testing or sample analysis. When these tests are recommended, we advise that patients reach out directly to the company that processed your labs to receive the most accurate billing and insurance coverage information. All questions regarding payment and billing issues for these tests will have to be addressed to the company that processed your labs.





























