Embed Size (px)
Citation preview

Pediatric Palliative Care Waiver
Workgroup Meeting June 11, 2018
1
Agenda Welcome and Introductions
Purpose of Meeting
Pediatric Palliative Care (PPC) Waiver Overview Overview of Early and Periodic Screening, Diagnostic, and Treatment ( EPSDT) Services Transition Plan – Specific Elements
Open Discussion and Breakout Session
Final Comments and Next Steps
2

Welcome and Introductions
Sarah Eberhardt-Rios Chief, Integrated Systems of Care Division Department of Health Care Services
3

Purpose of Meeting
Sarah Eberhardt-Rios Chief, Integrated Systems of Care Division Department of Health Care Services
4

Purpose of Meeting
Today, we will be discussing Pediatric Palliative Care (PPC) Waiver services Understanding EPSDT services Understanding PPC services in Medi-Cal Managed Care and fee-for-service (FFS) delivery systems Planning and discussing a transition strategy for current waiver participants
5

Purpose of Meeting (continued)
Current PPC Waiver status
Department of Health Care Services (DHCS) discussions with Centers for Medicare and Medicaid Services (CMS) regarding PPC Waiver
Termination of PPC Waiver and transition of services to appropriate Medi-Cal Managed Care and FFS providers
6

Pediatric Palliative Care Waiver Overview
Sarah Eberhardt-Rios Chief, Integrated Systems of Care Division Department of Health Care Services
7

Pediatric Palliative Care Waiver Overview
PPC Waiver first approved by CMS in December 2008
Began as a t hree-year demonstration pilot program on April 1, 2009
Renewed for an additional five-year waiver term on December 27, 2012
8

The PPC Waiver was approved for 1,800 slots and to o perate within 12 counties
There are ten participating counties, with four active providers Participating counties: Alameda, Los Angeles, Marin,
Monterey, Orange, San Francisco, Santa Clara, Santa Cruz, Sonoma, and Ventura
Ventura is withdrawing from waiver participation; San Diego previously withdrew
Pediatric Palliative Care Overview (continued)
Enrollment has been historically low and r emains at around 200 participants at any given time
9

Pediatric Palliative Care Waiver Overview (continued)
process to identify proposed changes to the waiver to be addressed through the PPC Waiver renewal application
DHCS held three in-person stakeholder meetings to facilitate input: August 31, 2016 – PPC Waiver Renewal Kick-off Meeting April 14, 2017 – Northern California Technical Advisory Workshop May 2, 2017 – Southern California Technical Advisory Workshop
DHCS engaged in an extensive stakeholder
10

The PPC Waiver renewal application was submitted for CMS’ review on September 29, 2017
DHCS submitted three temporary extension (TE) requests to facilitate CMS’ review of the PPC Waiver renewal application First TE submitted October 12, 2017 extended current waiver term from December 27, 2017 through December 31, 2017 to align new waiver term with the new year (January 1, 2018)
Second TE approved by CMS on February 1, 2018 extended the current waiver term through May 15, 2018
Third TE approved by CMS on May 3, 2018 extends the current waiver term through August 13, 2018 11
Pediatric Palliative Care Waiver Overview (continued)

Pediatric Palliative Care Waiver Overview (continued)
Discussions with CMS included case management and assessment approaches per CMS Technical Guidance as applicable to all States
Separations for conflict of interest between assessing and care planning entities
Service delivery design challenge
12

Pediatric Palliative Care Waiver Overview (continued)
As a result of these challenges, DHCS has determined the best direction is to end the PPC Waiver and transition current beneficiaries into other systems of care
Transition will occur over a period of time, through a streamlined process including a warm handoff
The transition approach is what we are here to discuss today and will occur by January 1, 2019
13

History
PPC waiver established with Assembly Bill 1745, 2006
Need for a program to provide supportive care at the same time as curative care
PPC enrolled first patient in 2010
14

Affordable Care Act (ACA) Concurrent care, provision of ACA that permits concurrent hospice and curative care
Began 2011
PPC continued for some children requiring palliative care and curative services because: Not eligible for hospice care Do not have access to State palliative care services as described in Numbered Letter (NL) 04-0207, or
Required services not available under the state plan
15

Pediatric Palliative Care Options Waiver Concurrent Care
Age Under 21 Under 21
Geographic Limited counties: Alameda, Statewide Los Angeles, Marin, Monterey, Orange, San Francisco, Santa Clara, Santa Cruz, Sonoma, Ventura
Medical Eligibility Life threatening California Children’s Medical doc tor certification Services (CCS) eligible condition, of life expectancy less than expected 30 days in hospital i n six months coming year
Insurance FFS Medi-Cal Medi-Cal, Healthy Families
Agency Partners for Children (PFC) approved Hospice hospice or home health agency (HHA)
Palliative Care Agency-based nurse, social worker, Hospice physician, nurse, Service Provider licensed vocational nurse (LVN), social worker, LVN, CNA,
certified nursing assistant (CNA) chaplain
16
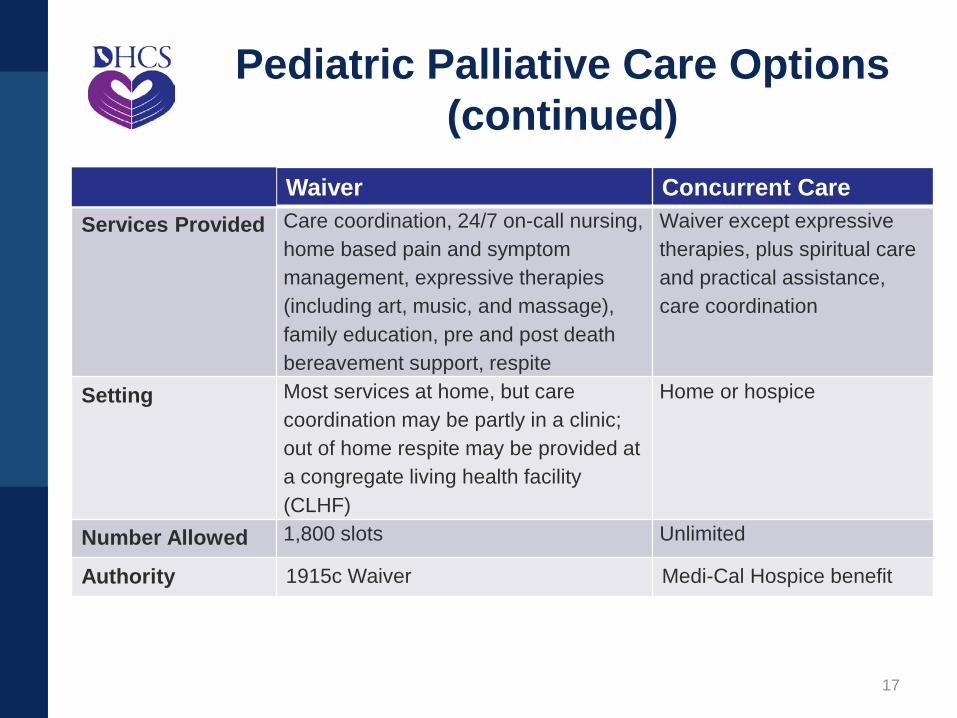
Pediatric Palliative Care Options (continued)
Waiver Concurrent Care Services Provided Care coordination, 24/7 on-call nur sing, Waiver except expressive
home based pain and symptom therapies, plus spiritual care management, expressive therapies and practical assistance, (including art, music, and massage), care coordination family education, pre and post death bereavement support, respite
Setting Most services at home, but care coordination may be partly in a clinic;
Home or hospice
out of home respite may be provided at a congregate living health facility (CLHF)
Number Allowed 1,800 slots Unlimited
Authority 1915c Waiver Medi-Cal Hospice benefit
17

Overview of Early and Periodic Screening, Diagnostic, and
Treatment Services
Lisa Albers Medical Consultant
Department of Health Care Services
18

EPSDT services are a benefit of the State’s Medicaid program (Medi-Cal) that provides comprehensive, preventive, diagnostic, and treatment services to eligible children under the age of 21, as specified in Section 1905(r) of the Social
Security Act.
19

EPSDT is designed to ensure thatchildren receive early detection and care,so that health problems are averted ordiagnosed and treated as early as
possible.
EPSDT has always been a benefit of both the managed care and FFS delivery
systems.
20

EPSDT
Early: Assessing and identifying problems early, starting at birth
Periodic: Checking children’s health at periodic, age-appropriate intervals
Screening: Providing physical, mental, developmental, dental,hearing, vision, and other screening tests to detect potentialproblems
Diagnostic: Performing diagnostic tests to follow up when a risk is identified
Treatment: Control, correct, or reduce identified health problems
21

EPSDT Services Screening Services Comprehensive health and developmental history Comprehensive unclothed physical exam Appropriate immunizations (according to the Advisory Committee on Immunization Practices)
Laboratory tests (including lead toxicity screening Health education (anticipatory guidance including child development, healthy lifestyles, accident and disease prevention)
Vision Services Hearing Services Dental Services
22

EPSDT Services (continued)
Other necessary health care, diagnostic services, treatment, and other measures described in section 1905(a) to correct or ameliorate defects and physical and mental illnesses and conditions discovered by the screening services, whether or not such services are covered under the State plan, if those services can be covered under Medicaid.
Other necessary services would include palliative care for children under the age of 21 when medically necessary to ameliorate their underlying condition.
23

EPSDT Services (continued)
EPSDT includes services that are medically necessary, regardless of whether such services are covered under Medi-Cal.
Service does not need to cure a condition. Services that maintain, sustain or support the child’s current health condition, prevent a condition from worsening, or prevent development of additional health problems are covered because they “ameliorate” a condition.
24

EPSDT Medicaid Requirements
State Medicaid agencies are required to: Inform all Medicaid-eligible individuals under age 21 that EPSDT services are available, and of the need for age-appropriate immunizations
Provide or arrange for the provision of screening services for all children
Arrange (directly or through referral) for corrective treatment as determined by child health screenings, and
Report EPSDT performance information annually via Form CMS-416
25

EPSDT All Plan Letter DHCS recently released All Plan Letter (APL) 18-007 on the requirements for coverage of EPSDT services for Medi-Cal members under the age of 21
APL does not represent a change in policy but rather reinforces existing regulations regarding the provision of EPSDT services
DHCS is amending Title 22 to eliminate references to ‘EPSDT supplemental services’ as there is no distinction between EPSDT services and ‘supplemental services’
26

EPSDT APL (continued) There are exceptions to services that managed care health plans (MCPs) are required to provide (carved out of the contract): Dental services provided by dental personnel Non-medical s ervices provided by Regional C enters (e.g., respite care) Alcohol and substance use disorder treatment services Specialty mental health services CCS services (not included in the capitated rate and excluding Whole Child Model counties)
However, MCPs are required to coordinate the provision of services with other entities, including providing appointment assistance, and transportation to medically necessary care
27

Transition Plan – Specific Elements
Lisa Albers Medical Consultant
Department of Health Care Services
28

Transition Plan
As of January 1, 2019, due to the end of the PPC Waiver, children enrolled in PPC Waiver will transition to MCPs or FFS
A majority of these children are already enrolled in managed care
MCPs have experience providing palliative care for adults as a result of Senate Bill 1004
29

Transition Plan - Members Noticing to Members DHCS will send notices to members 60 and 30 days prior to the transition date Informing members of the pending transition How to continue the benefit Continuity of care requirements
Many of these children are already enrolled in MCPs
DHCS will share pertinent data files for these children with MCPs prior to transition date
30
Continuity of Care Continuity of care requirements to assist Medi-Cal members who transition into Medi-Cal managed care are outlined in APL18-008 Members transitioning into an MCP have the right to request continuity of care in accordance with state law and the MCP contracts, with some exceptions
All MCP members with pre-existing provider relationships who make a continuity of care request to an MCP must be given the option to continue treatment for up to 12 months with an out-of-network Medi-Cal provider
31

PPC Waiver Counties/MCPs County MCPs
Alameda Alameda Alliance for Health, Anthem Blue Cross
Fresno CalViva, Anthem Blue Cross
Los Angeles LA Care, Health Net
Monterey Central California Alliance for Health
Orange CalOptima
San Francisco San Francisco Health Plan, Anthem Blue Cross
Santa Clara Santa Clara Family Health Plan, Anthem Blue Cross
Santa Cruz Central California Alliance for Health
Sonoma Partnership Health Plan
Ventura Gold Coast Health Plan
32

Transition Plan - MCPs APL Update Palliative Care APL MCPs to submit updated polices and procedures for palliative care to DHCS MCP contract amendments to reflect the benefit Updates to Member Handbooks Monitoring Current palliative care reporting template is under review for potential updates
33
Outlined in APL 17-015 for managed care: Current APL requires MCPs to authorize palliative care, regardless of patient-age, when general eligibility criteria are met, as well as, at least one of four disease-specific eligibility criteria Disease-specific criteria are adult-focused and will have to be modified
Palliative Care in Managed Care
34

Palliative Care APL Seven basic services: Advance Care Planning PC Assessment and Consultation Plan of Care Palliative Care Team Care Coordination Pain and Symptom Management Mental Health and Medical Social Services Includes psychotherapy, bereavement counseling, medical social services, and discharge planning
35

Palliative Care APL (continued)
MCPs may authorize additional palliative care not described in the APL at their discretion and cost For example, a 24/7 telephonic palliative care support line, separate from a routineadvice line Expressive therapies
RN
36

Open Discussion and Breakout Session
37

Final Comments and Next Steps
Sarah Eberhardt-Rios Chief, Integrated Systems of Care Division Department of Health Care Services
38

Final Comments and Next Steps
Continue working with CMS on transition approach and timeline based on today’s conversation
Prepare a transition plan to be submitted to CMS for review and approval
Request a final temporary extension from CMS for PPC Waiver through December 31, 2018
Work with MCPs to ensure each beneficiary receives the necessary care
Will closely monitor the provision of the benefit in the first six months and then traditional monitoring ongoing
39

Thank you!
40










![[PPT]KONSEP DASAR KEPERAWATAN KOMUNITAS · Web view... Hospital with aged care facilities Hostels Aged Care Assessment Team Community Family/older people Day care Respite care Support](https://img.pdfslide.tips/doc/110x75/5b3fec937f8b9a91078ca937/pptkonsep-dasar-keperawatan-komunitas-web-view-hospital-with-aged-care.jpg)