-
7/27/2019 perikard izliv uvod
1/20
Assessment of pericardial effusionOverview
Summary
Aetiology
Emergencies
Urgent considerations
DiagnosisStep-by-step
Differential diagnosis
Guidelines
Resources
References
Images
Patient leaflets
Credits
Email
Print
Feedback
ShareAdd to Portfolio
Bookmark
Add notes
SummaryPericardial effusion is a frequent finding that occurs
due to primary pericardial disease or in relation to a myriad
of systemic disease processes. The significance of effusions
lies in their relationship to an underlying disease
state and in their potential to affect a patient's
haemodynamics.
Epidemiology
Data from the Framingham cohort suggest that pericardial
effusion may be present in up to 6.5% of the adult
population. In the Framingham cohort, the incidence increased
with age, with only 1.2% of patients
-
7/27/2019 perikard izliv uvod
2/20
although once the pericardial pressure-volume relationship
reaches its non-compliant stage, expansion is limited
and small increases in volume produce a dramatic increase in
pericardial pressure, severely impairing
ventricular filling.
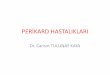
Diagram
showing the anatomy of the pericardium; the stippled area
represents the subfascial connective tissue planeFrom: Marchand
P. Thorax. 1951;6:359-368
Types of pericardial effusion
The mechanism of abnormal fluid collection depends on the
underlying aetiology, but is typically due to injury of
the pericardium and may be classified as acute or chronic, and
small or large. Chronic effusion has been defined
as an effusion that persists for >3 months; and acute, as
-
7/27/2019 perikard izliv uvod
3/20
The fluid may be serous, purulent, haemorrhagic, chylous, or
serosanguineous, but the nature of the effusion
adds little to the characterisation of the aetiology. Effusions
are categorised as transudates or exudates.
Exudative effusions may be idiopathic, iatrogenic, or due to
infection, malignancy, trauma, cardiorespiratory, and
autoimmune processes. Exudative effusions result from acute or
chronic pericardial inflammation, with high
levels of protein.
Cardiac tamponade occurs when pericardial pressure increases and
limits cardiac filling. The severity of
tamponade is determined by its effect on cardiac output and
haemodynamics, but even when hypotension is not
present, tamponade is a serious condition that may rapidly
progress and requires urgent evaluation. Effusions
that are small and thought to be transudative are unlikely to be
clinically significant.
Pericardial constriction
Chronic pericardial effusion may share similar clinical symptoms
and signs with pericardial constriction. The 2
conditions may co-exist, or constriction may develop as a later
consequence of the underlying aetiology of the
pericardial effusion, particularly following tuberculous
pericarditis or after cardiac surgery. Differentiating these 2
conditions may be difficult and requires advanced imaging
techniques.
AetiologyThere are many causes of pericardial effusion, with
varyingprevalence.[4] [5] The most common causes are typically
idiopathic andviral.[2] Other causes include bacterial, collagen
vascular disorders,vasculitis, Dressler's syndrome, certain
medicines, malignancy, CHF, MI,trauma, surgery, uraemia,
hypothyroidism, and amyloidosis.
The likelihood that an effusion will lead to tamponade depends
on the size,rapidity of formation, and nature of the effusion. For
instance, when bloodrapidly fills the pericardium as a result of
aortic dissection, much less fluid isneeded to produce tamponade
than in a gradually increasing effusion, inwhich the pericardium
has time to grow.
Idiopathic effusions are the most common single cause of
effusion, and thusthey seem to be a frequent cause of tamponade.
However, the likelihood thatan idiopathic or viral effusion will
produce tamponade is low. In contrast,
malignant effusions and tuberculous effusions are likely to
producetamponade. In a study of moderate-to-large effusions, 60% of
malignant and7% of tuberculous effusion eventually led to
tamponade.[4]
Aside from effusions producing tamponade, effusions that are the
result ofbacterial infection deserve special note because of the
high mortalityattributed to this disease. Purulent pericarditis was
uniformly fatal in the pre-antibiotic era, and even modern reports
cite mortality rates of 40%.[6]
http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-4http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-4http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-4http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-5http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-5http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-2http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-2http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-2http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-4http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-4http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-4http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-6http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-6http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-6http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-4http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-5http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-2http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-4http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-6
-
7/27/2019 perikard izliv uvod
4/20
IdiopathicIdiopathic effusions are those in which a definitive
diagnosis cannot beobtained. It is generally assumed that most
cases are due to viral infection,either acute or chronic. As in
viral pericarditis, patients generally present withfeatures typical
of acute pericarditis and experience a self-limiting, benigncourse.
However, idiopathic effusions may persist, recur, and, when
large,progress to tamponade.[3]Evaluation of fluid tends to
demonstrate bloody fluid, a low WBC count with amonocyte
predominance, normal glucose, and low specific gravity.[7]
InfectiousViral
Viral pericarditis rarely produces effusions large enough to
cause tamponade.
Viral infection is the most common cause of acute pericarditis
and is specifically identified in up to 50%
of cases. Coxsackie, echovirus, adenovirus, cytomegalovirus,
Epstein-Barr, mumps, rubella, parvovirus B19,
and HIV are among the many viral causes of acute
pericarditis.
Associated clinical history, such as time of year, exposures,
and acute onset, help distinguish viral
aetiologies from other causes. Evaluation of fluid reveals
characteristics similar to idiopathic effusion.[7]
Bacterial
Uniformly fatal if untreated. The mortality is 40% in
appropriately treated patients.[8] Bacterial pericarditis is a
fulminant condition with an acute onset, but up to 50% of patients
do not report
chest pain, and thus the condition needs to be considered in all
ill patients who present with pericardial effusion
and fever.[6]
Patients at higher risk for bacterial pericarditis include those
on dialysis, immunosuppressed patients,
alcoholic people, and patients who have recently had cardiac
surgery.
The most likely causes include Staphylococcus aureus,
Streptococcus pneumoniae,
andNeisseria species, although more modern reports note an
increase in anaerobic infections particularly in the
setting of head and neck infections.
Fluid analysis often is purulent, and has a very elevated WBC
with a neutrophil predominance.[7]
Tuberculous
Rare (4%) in developed countries, but is responsible for up to
70% of pericarditis in certain countries.
Tuberculous pericarditis remains the most common cause of
pericarditis in Africa.
http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-3http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-3http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-3http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-8http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-8http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-8http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-6http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-6http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-6http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-3http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-8http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-6http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7
-
7/27/2019 perikard izliv uvod
5/20
The diagnosis should be suspected in patients with acute
pericarditis that does not have the expected
rapid resolution of symptoms with supportive care.
Mortality is 85% in untreated cases and as high as 40% in
treated cases. Between 30% and 50% of
patients develop constrictive pericarditis.[8] [9]
Fungal
Reports of histoplasmosis and Candida-related pericarditis with
subsequent effusions have been
reported, but they are rare. In nearly all reported cases,
patients had a known predisposing condition for fungal
infection.[10]
Parasitic
Trypanosoma cruziinfection (Chagas' disease) may rarely be
associated with acute Chagas myocarditis
or chronic Chagas cardiomyopathy.
Although acute Chagas myocarditis is rare, pericardial effusion
is seen commonly (42%) when it
occurs.[11]
Immune-mediatedCollagen vascular disorders
SLE: pericardial disease is common in lupus and is part of the
diagnostic criteria. While autopsy studies
show that the pericardium is affected in 62% of patients,
clinically evident pericarditis occurs in 25% of patients
over the course of their disease. Typically, pericarditis occurs
in the setting of generalised serositis and, in
patients with pericardial effusion, a pleural effusion is
present in 76% of cases. In patients with clinically
recognised pericarditis, tamponade develops in 13% of
cases.[12]
Wegener's granulomatosis: pericarditis is the most common
cardiac manifestation in this systemic
inflammatory vasculitic disease. Mild subclinical pericardial
effusions occur in 55% of patients, and tamponade
may occur, although rarely. It is often difficult to determine
whether effusion is primarily related to Wegener's or
is a consequence of pathology in other organs, such as the
kidneys.[13]
Dressler's phenomenon
This syndrome was first described in the 1950s as a syndrome of
pericardial chest pain and fever in the
weeks to months following an acute myocardial infarct. It is now
known that this condition and others similar to it,
including post-pericardiotomy and post-commissurotomy syndrome,
are caused by antibodies to heart antigens.
The course is characteristically benign and the effusion has
exudative characteristics. Once a common disease,
in the era of reperfusion therapy the incidence of Dressler's
phenomenon has dramatically decreased.[14]
Drug-induced
Hydralazine, procainamide, and isoniazid are the most common
drugs identified as a cause of drug-
induced lupus erythematosus.
http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-8http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-8http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-8http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-9http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-9http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-10http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-10http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-10http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-11http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-11http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-11http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-12http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-12http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-12http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-13http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-13http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-13http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-14http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-8http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-9http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-10http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-11http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-12http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-13http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-14
-
7/27/2019 perikard izliv uvod
6/20
Pericarditis occurs in a similar proportion to idiopathic lupus,
but reports of tamponade are rare.
Typically, the disease and its manifestations resolve following
cessation of the offending agent.[15]
Amyloid
Cardiac involvement is common in systemic amyloidosis and
pericardial effusion occurs in as many as
58% of patients with cardiac amyloid. In all but a few cases,
the size of the effusion is small or moderate andtamponade is
rare.[16]
EndocrineHypothyroidism
Myxoedematous effusions accumulate very slowly as a result of
capillary leak. As a result, effusions
rarely lead to tamponade and have high protein content.
Typically, effusions resolve within weeks to months following
institution of hormone replacement
therapy.[17]
NeoplasticMalignant effusions
Are among the most likely to cause tamponade, in which lung
cancer, breast cancer, lymphomas, and
leukaemias are the most prevalent underlying malignancies.
Malignant effusion due to metastatic cancer is
rarely the presenting finding, although it may be the first sign
of metastases; thus, a history of known malignancy
increases clinical suspicion.
Primary malignancies (rare)
Angiosarcoma is the most common form of malignant cardiac
tumour.[18] It typically originates in the
right atrium, but may also exist separately or extend into the
pericardium.
Others include mesothelioma and malignant teratoma.[19] [18]
Accumulation of pericardial fluid may be gradual or rapid when
erosion intothe pericardial blood vessels occurs. Effusions are
exudative in quality, andcytological analysis of pericardial fluid
will be positive in 65% to 85% of
patients.[20]
CardiacAortic dissection
http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-15http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-15http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-15http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-16http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-16http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-16http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-17http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-17http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-17http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-18http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-18http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-18http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-19http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-19http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-19http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-18http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-18http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-20http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-20http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-20http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-15http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-16http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-17http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-18http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-19http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-18http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-20
-
7/27/2019 perikard izliv uvod
7/20
Pericardial haemorrhage occurs in the setting of proximal type A
dissection and can rapidly produce
tamponade with small volumes of pericardial blood. The mortality
is 60% and accounts for most deaths of
patients with type A dissection.[21]
CHF
Pericardial fluid has been noted to accumulate in patients with
CHF as part of generalised volumeoverload. The volume of fluid is
generally small and tamponade is not a recognised complication.
Pleural
effusions are present in 92% of heart failure patients with
pericardial effusion.[22] The fluid is characteristically
transudative, but they may be misclassified as exudates in the
setting of diuresis.[23]
Post cardiac surgery
Post-cardiac surgery effusion occurs in up to 85% of
patients.[24] In a study of 803 post-cardiac surgery
patients who had echocardiography performed on post-operative
day 8, effusion was common, but only 1.6% of
patients had large effusions. Valve surgery was significantly
associated with the presence of large effusion and
tamponade. Most patients were receiving anticoagulation that was
thought to contribute to the effusion.[25]
The clinical characteristics of post-operative effusions differ
from medical effusion. In a retrospective
review of 208 post-operative patients with symptomatic effusion
requiring intervention, malaise (90%) was the
most common symptom, followed by dyspnoea (65%) and chest pain
(33%). Hypotension and pulsus paradoxus
were present in only 27% and 17% of patients, although
hypotension was more common in early effusions,
which were predominantly due to bleeding complications, also
associated with anticoagulation.[26]While typical
circumferential effusions occur post-operatively, up to 58% are
loculated. Fever is a common finding (40%) and
is usually part of a post-cardiotomy syndrome, but
post-operative infection must always be considered.
Pericardial constriction post-surgery is a rare but important
occurrence, which usually presents many
months to years after cardiac surgery, often in patients where
signs of post-cardiotomy syndrome were noted
peri-operatively. Echocardiography, CT imaging, and cardiac
catheterisation may all be necessary to confirm the
diagnosis.
Post cardiac intervention
The incidence of percutaneous cardiac intervention-related
effusions has increased significantly in
recent decades, consistent with the increase in the frequency of
coronary intervention and introduction of new
interventional procedures such as ablation and valvuloplasty. In
a review of 1127 patients requiring
pericardiocentesis over 21 years, intervention-related effusions
accounted for 14% of all patients requiring
pericardiocentesis in the last 7 years of the study, making it
the third most common aetiology.[27]
Non-cardiac physicians are unlikely to encounter these patients,
as symptoms develop
rapidly.[28] While the incidence of cardiac perforation is
exceedingly low overall (0.08%), there is variability with
regard to particular interventions. The incidence of cardiac
perforation following diagnostic catheterisation is
0.006%, whereas in valvuloplasty it is 1.9%.
Traumatic
http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-21http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-21http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-21http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-22http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-22http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-22http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-23http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-23http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-23http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-24http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-24http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-24http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-25http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-25http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-25http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-26http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-26http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-26http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-27http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-27http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-27http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-28http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-28http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-28http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-21http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-22http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-23http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-24http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-25http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-26http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-27http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-28
-
7/27/2019 perikard izliv uvod
8/20
Direct penetrating injuries of the heart are usually the result
of stab wounds orgunshots and have a high pre-hospital mortality.
For patients who reach ahospital, emergency department
echocardiography is 96% accurate in thediagnosis of traumatic
effusion.[29]
Radiation-relatedIn the course of radiotherapy for thoracic
malignancies such as Hodgkin'slymphoma and breast cancer, the heart
and pericardium may be exposed tohigh doses of radiation.
Pericarditis related to radiation may be acute ordelayed.
The acute variety presents just following therapy, and typically
manifests similar to acute pericarditis of
other forms.
Delayed pericarditis may present as acute pericarditis or as an
asymptomatic effusion. Reports on theincidence of pericarditis vary
depending on the total dose of radiation given, but as many as 20%
of patients
receiving radiation to the entire pericardium and as few as 2%
of patients with subcarinal blocks develop
disease.
Those receiving >40 Gy of radiation without subcarinal blocks
are at thegreatest risk of significant pericardial pathology.
Tamponade is not infrequent and some evidence of tamponade has
beenreported to occur in up to one half of all cases. Pericardial
constriction may
also be seen as a longer-term consequence of mediastinal
irradiation.
RenalUraemia
Pericardial effusion in renal disease has been described in
uraemia related to acute renal failure and as
a consequence of inadequate dialysis in patients with chronic
renal failure. Features of acute pericarditis are
common in uraemic pericarditis and can occur in dialysis-related
effusions. A pericardial friction rub in a patient
with acute renal failure warrants an echocardiogram to evaluate
for pericardial effusion. These effusions are
characteristically transudative with low protein
content.[30]
Urgent considerationsSee Differential Diagnosis for more
details
Cardiac tamponade
Tamponade is present when pericardial effusion increases the
intrapericardial pressure, compressing the
cardiac chambers so that cardiac filling is impaired, leading to
hypotension and cardiovascular collapse.
http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-29http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-29http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-29http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-30http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-30http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-30http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-29http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-30http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html
-
7/27/2019 perikard izliv uvod
9/20
Tamponade exists as a haemodynamic spectrum ranging from trivial
compression with minimal effects on
cardiac output to fatal cardiovascular collapse.
Normally the pericardial pressure is lower than the heart
chamber pressures so that the transmyocardial
pressure gradient (pressure inside the heart minus pressure in
the pericardium) favours cardiac filling. As
pericardial pressure increases with a growing effusion, the
pericardial pressure equalises initially with the rightatrium,
producing diastolic collapse of the right atrium. The body attempts
to compensate by increasing central
venous pressures in order to prevent further collapse, and by
increasing sympathetic nervous system output to
maintain stroke volume and cardiac output. The effect is
tachycardia and jugular venous distension. As effusion
progresses, pericardial pressures increase to >10 mmHg and
surpass right ventricular diastolic pressure, which
is demonstrated on echocardiography as collapse of the right
ventricular free wall. When pericardial pressures
approach 25 mmHg, catheter-based pressure measurements reveal
equalisation of diastolic pressure in each
cardiac chamber and a transmyocardial pressure that is
essentially zero. All 4 chambers in the heart are
collapsed and tamponade is severe, with signs of reduced cardiac
output and hypotension. At this stage, the
pericardial volume is fixed and the heart can only be filled if
blood is leaving the heart. Thus, atrial filling occurs
in systole when the ventricles are evacuating. Furthermore,
increases in the volume of one chamber must
produce a corresponding decrease in the other chamber's volume
by a phenomenon known as ventricular
interdependence. During inspiration, when the stroke volume of
the right ventricle is increased, the left ventricle
stroke volume is decreased, producing a fall in blood pressure.
The opposite occurs during expiration. This
phenomenon of increased ventricular interdependence produces the
examination finding of pulsus
paradoxus.[31] [32]
The presence or absence of pulsus paradoxus is very important in
assessing pericardial effusion. A value >12
mmHg has a sensitivity of 98% and specificity of 83% for the
detection of tamponade.[33]
Pulsus paradoxus is an increase (>10 mmHg) of the normal
inspiratory decrease in systemic blood pressure. To
measure pulsus paradoxus, the blood pressure cuff is inflated
above systolic blood pressure. The cuff is deflated
slowly, listening for the first Korotkoff sound, which will be
intermittent and heard during quiet expiration. The
difference (in mmHg) between this first Korotkoff sound and the
pressure at which a Korotkoff sound is heard
with each beat is the pulsus paradoxus. Normal value is
-
7/27/2019 perikard izliv uvod
10/20
Pulsus paradoxus >10 mmHg
Increased jugular venous pressure.
Hypotension and increased jugular venous pressure are
relative.
DiagnosisWhen tamponade is suspected, the presence or absence of
pulsus paradoxus is very important. A value >12
mmHg has a sensitivity of 98% and specificity of 83% for the
detection of tamponade (although 10 mmHg is
often given as evidence of pulsus paradoxus).[33]However, pulsus
paradoxus is often absent in the early stages
of tamponade and may not be present in the presence of other
common conditions including hypovolaemia,
post-operative effusion, haemorrhage, pulmonary hypertension,
pulmonary embolus, right ventricular infarct, and
asthma. Pulsus paradoxus may also be difficult to measure in an
acutely unwell patient, and simply noting
disappearance of the pulse on palpation during inspiration
suggests significant tamponade.
Thus, a transthoracic echocardiogram is obtained in all patients
with suspected effusion based on history or
examination. A study of 110 patients with moderate or large
pericardial effusion attempted to determine the utility
of common echocardiography findings in patients with clinical
findings of tamponade.[34] Right atrial collapse
was the most sensitive finding for tamponade (90%), whereas
abnormal systolic venous flow was the most
specific finding in tamponade (92%). The combination of collapse
of the right atrium and ventricle plus abnormal
systolic venous flow was 98% specific for tamponade. Marked
variation in atrioventricular inflow velocities is also
an important echocardiographic finding in patients with
pericardial effusion that may either confirm clinical
tamponade or suggest an intermediate stage before overt
tamponade.[35] Of note, 10% of patients with clinical
tamponade did not have any echocardiographic findings of
collapse. Furthermore, collapse of any cardiac
structure was present in 34% of patients without clinical
tamponade, representing echocardiographic
tamponade.[34] Thus, the physical examination is especially
important in the evaluation of tamponade.
Management
The cornerstone of treatment of tamponade is emergency drainage
of the pericardial fluid. Pericardiocentesis is
traditionally performed in the catheterisation laboratory, but
bedside echocardiography-assisted
pericardiocentesis is widely employed in some
centres.[27]Surgical drainage with creation of a pericardial
window is indicated for recurrent effusions or in cases of
traumatic haemopericardium.[8]
Red flags
Metastatic malignancy
Bacterial pericarditis
Tuberculous pericarditis
Fungal pericarditis
Angiosarcoma
Mesothelioma
Malignant teratoma
http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-33http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-33http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-33http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-34http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-34http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-34http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-35http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-35http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-35http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-34http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-34http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-34http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-34http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-27http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-27http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-27http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-8http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-8http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-8http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html#expsec-6http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html#expsec-3http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html#expsec-4http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html#expsec-5http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html#expsec-7http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html#expsec-8http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html#expsec-9http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-33http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-34http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-35http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-34http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-27http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-8http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html#expsec-6http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html#expsec-3http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html#expsec-4http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html#expsec-5http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html#expsec-7http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html#expsec-8http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html#expsec-9
-
7/27/2019 perikard izliv uvod
11/20
-
7/27/2019 perikard izliv uvod
12/20
Cough
Fever: high fever and toxic appearance suggest bacterial
aetiology and should prompt urgent pericardial
drainage
Dyspnoea
Lethargy
Medical history (e.g., collagen vascular disease, amyloidosis,
cancer)
Medicine history (drug immune-mediated effusion)
Examination findings suggestive of pericardial effusion:
A pericardial friction rub, which is a high-pitched scratching
sound best heard over the left sternal border
with the patient leaning forwards at end-expiration. Rubs may be
1, 2, or 3 parts, corresponding to the periods of
greatest heart movement in the cardiac cycle. The pericardial
friction rub may also be transient, and thus it is
useful to examine patients suspected of pericarditis on multiple
occasions.
Distant heart sounds with a quiet precordium is a common finding
in pericardial effusion, although in
patients with pulmonary hypertension or dilated cardiomyopathy,
an anterior impulse is often present.
The presence or absence of pulsus paradoxus is very important. A
value >12 mmHg has a sensitivity of
98% and specificity of 83% for the detection of
tamponade.[33]
Pericardial constriction may produce similar examination
findings totamponade with pulsus paradoxus and elevated jugular
venous pressure. Apericardial knock may be evident during palpation
and/or auscultation, andconstriction is also often associated with
gross liver enlargement and ascites.
ImagingPatients with suspected pericardial effusion and symptoms
of acutepericarditis should receive an ECG and CXR. In most
circumstances, patientsshould have an echocardiogram for detection
of pericardial effusion, but
when examination findings suggest tamponade, a
transthoracicechocardiogram is essential.
When inflammation involves the epicardium, the ECG may show
diffuse ST-segment elevation and PR depression signalling
generalised epicardialinjury. View image If the pericardial
effusion is large enough, the heart mayswing in the pericardial
fluid, producing beat-to-beat variation of theventricular, and
occasionally the atrial, axis on the ECG known as electrical
http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-33http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-33http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-33http://bestpractice.bmj.com/best-practice/monograph/458/resources/images/print/6.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-33http://bestpractice.bmj.com/best-practice/monograph/458/resources/images/print/6.html
-
7/27/2019 perikard izliv uvod
13/20
alternans. CXR may show a water bottle-shaped cardiac silhouette
with adistinct, fat pericardial fat stripe suggesting a large
pericardial effusion. ViewimageWhen effusion is suspected on
examination, the preferred test to confirm thediagnosis is
transthoracic echocardiogram. It is a non-invasive and
effective
diagnostic modality that detects effusion when >50 mL of
fluid is present.Circumferential effusions are easily visualised as
an echo-dense space. ViewimageView imageView image Observed
diastolic collapse of the rightventricle or right atrium,
predominantly systolic inferior vena caval flow, andmarked
variation in mitral and tricuspid inflow velocities with
respiration are allsigns of tamponade.
Pericardial constriction should be suspected when clinical
features of aneffusion are present but imaging demonstrates no or
minimal effusion.Pericardial thickening may be noted on
echocardiography or CT imaging.
Marked respiratory variation in mitral and tricuspid inflow
velocities is also afeature of pericardial constriction.
Laboratory evaluationThe aetiology of pericardial effusion is
found in up to 60% of patients on initialevaluation.[4]Thus, all
patients require a thorough history and physicalexamination. The
utility of routine laboratory evaluation, including FBCs,chemistry,
rheumatoid factors, antinuclear antibodies, and serum
C-reactiveprotein, is not well established, as they lead to a
specific diagnosis in only
10% to 15% of cases.[37] It is more useful to order laboratory
tests asdetermined by the clinical picture.
FBC: a very elevated leukocyte count may suggest bacterial
pericarditis.
Chemistry: findings such as an elevated creatinine are sensitive
for renal failure and may suggest a
uraemic aetiology.
Thyroid-stimulating hormone: when elevated, it suggests that
hypothyroidism may be contributing to
pericardial effusion.
Serum C-reactive protein: is elevated in most cases of acute
pericarditis and so may not be helpful in
determining the underlying aetiology.
Erythrocyte sedimentation rate: is often elevated in acute
pericarditis and so may also be unhelpful in
determining the underlying aetiology.
Rheumatoid factor: when rheumatoid arthritis is suspected, this
is a useful test.
http://bestpractice.bmj.com/best-practice/monograph/458/resources/images/print/4.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/resources/images/print/4.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/resources/images/print/3.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/resources/images/print/3.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/resources/images/print/2.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/resources/images/print/1.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-4http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-4http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-4http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-37http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-37http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-37http://bestpractice.bmj.com/best-practice/monograph/458/resources/images/print/4.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/resources/images/print/4.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/resources/images/print/3.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/resources/images/print/3.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/resources/images/print/2.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/resources/images/print/1.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-4http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-37
-
7/27/2019 perikard izliv uvod
14/20
Antinuclear antibody: when SLE is suspected, this is a useful
test.
Troponin: troponin levels are often elevated in pericarditis and
do not portend a worse prognosis.
Blood cultures: when bacterial pericarditis is suspected, this
is an essential test.
Viral cultures: although positive cultures may aid in the
diagnosis of viral pericarditis, there is little clinical
utility in ordering them, as most cases of viral pericarditis
are benign and self-limiting, and a positive test would
not change management.
HIV: when evidence of immunosuppression is present on
examination, or the patient has risk factors for
infection, this test may alter the differential diagnosis.
PericardiocentesisWhen initial tests do not reach a diagnosis,
invasive pericardiocentesis may
be necessary for further diagnostic evaluation. The diagnostic
yield of fluid ortissue analysis obtained by either percutaneous or
surgical methods is verylow when performed for strictly diagnostic
purposes in patients without anobvious cause on initial
evaluation.[38] The balance of current opinionrecommends drainage
in the following circumstances:
Tamponade
Large effusion (>2.0 cm) with evidence of tamponade on
echocardiogram
Large effusion (>2.0 cm) without evidence of tamponade that
persists for >3 months
Suspected tuberculous or bacterial pericarditis.[2] [3] [34]
[39]
In the analysis of pericardial fluid, the first step should be
to separateeffusions into transudates and exudates by determining
the following:
LDH >200 U/decilitre (sensitivity 98%)
Total protein >30 g/L (3.0 g/dL) (sensitivity 97%)
Fluid to serum LDH >0.6 (sensitivity 94%, diagnostic accuracy
87%)
Fluid to serum protein >0.5 (sensitivity 96%).
If any one of these criteria is met, the patient has an exudate.
The mostaccurate test to distinguish transudative from exudative
effusion is a fluid toserum LDH >0.6 with an accuracy of 87%.[7]
[23]
http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-38http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-38http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-38http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-2http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-2http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-2http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-2http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-3http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-3http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-34http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-34http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-39http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-39http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-23http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-23http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-38http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-2http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-3http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-34http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-39http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-7http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-23
-
7/27/2019 perikard izliv uvod
15/20
The ability to separate pericardial effusions into exudates and
transudateshas been disputed. In a study of 120 patients undergoing
pericardiocentesisfor effusion of various aetiologies, there were
no differences in the absoluteor relative LDH and protein contents
among any of the various causes ofeffusion.[40] In the study, 118
of 120 patients would have been classified as
having exudates according to Light's criteria. Thus, while the
biochemicalcharacteristics of pericardial effusion may suggest a
particular entity, theyremain only one aspect in the overall
diagnosis.Other tests are used to provide a definitive diagnosis of
an underlyinginfectious or neoplastic cause:[22]
Viral cultures of pericardial fluid: culture and virus-specific
staining techniques may identify a specific
pathogen. These methods can be used to confirm the presence of
viral pericarditis and have a yield of
approximately 14%.[41]
Viral PCR is used to identify specific viral elements, and has a
diagnostic yield of 40%.[41]
Gram stain and culture: culture is more sensitive than Gram
stain for bacterial infections, but when either
reveals a specific pathogen it is very helpful. In fungal
infections, a positive fungal pericardial fluid culture
confirms the diagnosis and provides guidance when selecting
antifungal medication.
Pericardial adenosine deaminase activity (ADA) >667 nkat/L
(40 U/L) suggests tuberculous pericarditis.
The sensitivity is 88% and specificity 83%. As cultures are less
sensitive, this indirect test has become the
standard test in the diagnosis of pericardial tuberculosis.
Pericardial interferon-gamma (IFN-gamma) >200 picograms/L
suggests tuberculous pericarditis. Early
reports suggest that this test is 100% sensitive and specific.
However, its utility has not yet been demonstrated in
a large trial and it is not widely employed.
Cytology: required to confirm the diagnosis and subtype of
tumour. Metastatic malignancy is the most
common cause. Cytology is positive in up to 85% of cases of
pericardial metastases.[20] Cytology is also
required to identify the rare primary tumours (angiosarcoma,
mesothelioma, and malignant teratoma). Patients
with SLE have lupus erythematous cells, polymorphonuclear white
blood cells that have ingested another cell's
nuclear material, which may be seen in the pericardial
fluid.
Pericardial biopsyWhen fluid evaluation is non-diagnostic and
obtaining a diagnosis isnecessary, pericardial biopsy increases the
likelihood of obtaining a diagnosisunder select circumstances.
Pericardial biopsy is most useful whenneoplastic or tuberculous
effusions are suspected.[5][38]Although thediagnostic yield is
historically low and complicated by a high degree of false-negative
results, recent advances in pericardioscopy, which allows
directvisualisation of the pericardium, has improved the yield (40%
diagnostic yield)
http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-40http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-40http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-40http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-22http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-22http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-22http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-41http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-41http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-41http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-41http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-41http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-41http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-41http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-20http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-20http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-20http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-5http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-5http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-5http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-38http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-38http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-40http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-22http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-41http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-41http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-20http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-5http://bestpractice.bmj.com/best-practice/monograph/458/resources/references.html#ref-38
-
7/27/2019 perikard izliv uvod
16/20
and improved on the rate of false-negative samples (6.7%
false-negatives).[42] Biopsy is generally indicated in the course
of surgicaldrainage, when large effusions recur without a previous
diagnosis, and whentuberculous or malignant aetiologies are
suspected.[8]
Differential diagnosisSort by:
common/uncommonorcategoryCommonhide allIdiopathic
History Exam 1st test
chest pain, low-grade fever, cough,
dyspnoea
distant heart sounds, cardiac dullness CXR: pericardial
effusion
ECG: variable
Viral pericarditis
see our comprehensive coverage of Pericarditis
History Exam 1st test O
chest pain, low-grade fever,
cough, and other non-
specific symptoms - for
example, sore throat and
malaise
pericardial rub, a low-grade temperature
-
7/27/2019 perikard izliv uvod
17/20
with low ejection fraction; diastolic heart fa
ventricular ejection fraction normal but LV
abnormal diastolic filling patternsMore
Post-cardiac surgery
History Exam 1st test
post-cardiac surgery, malaise, dyspnoea; any change in
post-operative clinical status should prompt consideration
of an echocardiogram
hypotension mainly in early post-
operative tamponade, pulsus
paradoxus, fever
transthoracic
echocardiogr
effusionMore
Post cardiac intervention
History Exam 1st test
rapid progress to overt tamponade or haemodynamic
collapse in the interventional laboratory; may also present
as a delayed complication
hypotension rapidly progressing to
cardiovascular collapse or overt
tamponade is the rule
transthoraci
echocardiog
effusionMore
Uraemia
History Exam 1st test
hx of kidney disease, non-compliance with dialysis, and
pleuritic thoracic pain consistent with acute pericarditis;
associated symptoms of uraemia such as nausea, vomiting,
mental status changes, and uraemic frost may be present
a pericardial friction rub
indicates pericardial
inflammation
CXR: pleural effusion; m
signs of pulmonary oede
cardiomegalyMore
ECG: peaked T waves, i
PR interval, widened QR
chemistry-renal: elevate
creatinine levelsMore
Uncommonhide allBacterial pericarditis
see our comprehensive coverage of Pericarditis
History Exam 1st test O
hx of concomitant infection, for example, pleural
empyema/adjacent pneumonia/bacteraemia; hx of direct
cardiac trauma, immunosuppression, chronic disease, and
alcoholism; high-grade fever; absence of chest pain
toxic appearance with
high fever,
tachypnoea, and
tachycardia
blood
cultures: positiveMore
CXR: pleural effusionMore
ECG: diffuse ST-segment
elevation and PR
depressionMore
Tuberculous pericarditis
see our comprehensive coverage of Pericarditis
History Exam 1st test Other
hx of tuberculosis, pericarditis that does not
resolve as expected; subacute onset in
conjunction with constitutional complaints
distant heart sounds, cardiac
dullness, elevated neck veins,
hepatomegaly, pericardial
CXR: upper lobe
infiltrationMore
http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/243.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/243.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/243.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/243.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html
-
7/27/2019 perikard izliv uvod
18/20
including fever, night sweats, weight loss, and
fatigue; signs of heart failure predominate in
black patients
knock ECG: normalMore
Fungal pericarditis
see our comprehensive coverage of Pericarditis
History Exam 1st test
hx of chronic disease or
suppressed immune system,
fever
may be normal or reveal pericardial friction rub, distant
heart sounds; there are no specific signs suggestive of a
fungal aetiology
blood culture: positiveMore
CXR: pleural effusionMore
ECG: diffuse ST-segment ele
and PR depressionMore
Chagas disease
see our comprehensive coverage of Chagas disease
History Exam 1st test
hx exposure to Triatoma species, blood
transfusion, organ transplantation,
immunosuppression, health care or laboratory
occupations, travel to or residence in endemic
areas, ingestion of contaminated food or drink;
symptoms of myocarditis: palpitations,
syncope or pre-syncope
prolonged fever (7 to 30 days)
with nocturnal elevation,
hepatosplenomegaly,
lymphadenopathy, tachycardia
FBC: leukopenia or leukocytosis
with a left shift and
lymphocytosis; hypochromic
anaemia; low platelets
ECG: T wave alteration,
prolonged PR interval, sinus
tachycardia, low QRS voltage
CXR: enlargement of cardiac
area, pleural effusion
microscopy of fresh blood or
thick blood smear: visualisation
of trypomastigotes
Angiosarcoma
History Exam 1st test O
chest pain, symptoms of
heart failure
cardiac murmur, signs of
heart failure
transthoracic echocardiogram:intracardiac or
pericardial tumourMore
Mesothelioma
see our comprehensive coverage of Mesothelioma
History Exam 1st test
http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/243.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/1160.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/1184.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/243.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/1160.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/1184.html
-
7/27/2019 perikard izliv uvod
19/20
male predominance, third to fifth
decades, hx of asbestos exposure,
symptoms of heart failure
possible vena caval obstruction with
swelling and plethora of the upper
extremities, neck, and head
transthoracic
echocardiogram:pericardial stu
massMore
Malignant teratoma
History Exam 1st test
typically occurs in children with a
mean age of presentation of 16 weeks,
may present as heart failure
signs of heart failure predominate
due to compression of cardiac
structures
transthoracic
echocardiogram:intracardiac or
pericardial tumourMore
SLE
see our comprehensive coverage of Systemic lupus
erythematosus
History Exam 1st test Other tests
fatigue, arthralgia,
malar rash, oral ulcers,
and synovitis
malar rash, oral ulcers, arthritis,
photosensitivity rash, discoid rash and
seizures may be present
CXR: pleural effusionMore
ECG: diffuse ST-segment
elevation and PRdepressionMore
pe
an
ant pe
ce
Wegener's granulomatosis
see our comprehensive coverage of Wegener's granulomatosis
History Exam 1st test Other te
nose bleeds, recurrent sinusitis, haemoptysis,
and dyspnoea; constitutional complaints such
as fever, fatigue, and weakness
mucosal inflammation CXR: pleural effusion, pulmonary
infiltratesMore
ECG: diffuse ST-segment
elevation and PR
depressionMore
Dressler's phenomenon
History Exam 1st test Oth
hx of transmural infarct, hx of
cardiac pericardiotomy
typical pericardial chest pain
with low-grade fever
CXR: pleural effusionMore
ECG: diffuse ST-segment elevation and
PR depressionMore
Drug-induced
History Exam 1st test Ot
hx of hydralazine, procainamide,
isoniazid 1 month duration; fatigue,
arthralgia
may be normal or reveal
pericardial friction rub, distant
heart sounds
CXR: pleural effusionMore
ECG: diffuse ST-segment elevation
and PR depressionMore
http://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/103.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/327.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/103.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/327.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html
-
7/27/2019 perikard izliv uvod
20/20
Amyloidosis
see our comprehensive coverage of Amyloidosis
History Exam 1st test O
Hx of known amyloid, multiple myeloma,
monoclonal gammopathy, or chronic
illness such as rheumatoid arthritis; easy
bruising, fatigue, and weight loss
hepatomegaly ECG: low-voltage ECG with a pseudo-infarct
patternMore
transthoracic echocardiogram:left
ventricular hypertrophy, granular appearance
of myocardium, restrictive transmitral filling
patternMore
Hypothyroidism
see our comprehensive coverage of Primary hypothyroidism
History Exam 1st test
hx of hypothyroidism, thyroid surgery,
lethargy, constipation, cold intolerance
evidence of thyroid surgery, myxoedematous skin
changes, bradycardia, diminished tendon reflexes
TSH: elevatedMore
Aortic dissection
see our comprehensive coverage of Aortic dissection
History Exam 1st test Other test
tearing chest pain radiating to the back with
sudden onset, stroke symptoms due to
accompanying carotid artery dissection
blowing diastolic murmur,
pulse differential between
right and left arms
CXR: widened
mediastinumMore
th
ha
tra
di
ef
Direct penetrating injury
History Exam 1st test
gunshot and stab wounds
to the thorax
gunshot entrance wounds, stab wounds, hypotension often
without elevated neck veins, or pulsus paradoxus
transthoracic echocar
fluidMore
Radiation exposure
History Exam 1st test
hx of chest radiation,
especially without
subcarinal blocks
signs of volume overload with clear lung fields suggests
tamponade; a pericardial rub may be present, which
suggests acute pericarditis
CXR: pleural effusionMore
ECG: diffuse ST-segment e
and PR depressionMore
1
http://bestpractice.bmj.com/best-practice/monograph/444.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/535.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/445.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/444.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/535.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/445.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.htmlhttp://bestpractice.bmj.com/best-practice/monograph/458/diagnosis/differential-diagnosis.html