Embed Size (px)
Citation preview

19‐3‐2019
1
Hypercoagulopathie
Peter Verhamme
Vasculaire Geneeskunde & Hemostase
UZ Leuven

19‐3‐2019
2
Hypercoagulopathie
• Arteriele / Veneuze / Microvasculaire Trombose
• Aangeboren vs. Verworven
Cutane Manifestaties van hypercoagulopathie
• Post‐trombotische chronische veneuze insufficientie
• Oppervlakkige tromboflebitis
• Purpura (fulminans)
• Livedo reticularis / racemosa
• Livedo vasculopathie

19‐3‐2019
3
VaV
IXaIX
XIa
XII
XI
XIIa
X Xa
VIICa2+
PL
Ca2+
Ca2+VIIIaVIII
X
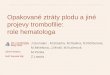
VIIa/Tissue Factor
Initiation of coagulation
PLCa2+
Prothrombin Thrombin (Iia)
XIII
XIIIa
Fibrinogen
Fibrin Monomer
Fibrin Polymer
Cross-linked Fibrin Polymer
Positivefeedback
Phospholipids (PL)Tissue Factor Pathway Inhibitor (TFPI)Prekallikrein (PK)High-molecular-weight kininogen (HK)
TFPI
(autocatalysis)TFPI
PKHK
HK
Sustainedhemostasis
Factor XIIa
Bradykinin
Complement

19‐3‐2019
4
Tissue Factor Pathway Inhibitor
Anti‐trombine
Thrombomoduline
Proteine CProteine S
Erfelijke trombofilie
● Overactiviteit stollingsfactoren ● Factor V Leiden (aPC‐resistentie)
● Prothrombine genmutatie (G20210A)
● Deficiëntie anticoagulantia ● Proteïne C deficiëntie● Proteïne S deficiëntie● Antitrombine deficiëntie

19‐3‐2019
5
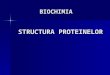
bron: inherited thrombophilia: a double-edged sword
Inherited thrombophilia: prevalence and risk for thrombosis

19‐3‐2019
6
Verworven aandoeningen
● Antifosfolipiden syndroom● Hematologische aandoeningen
● Myeloproliferatieve aandoeningenParoxysmale nachtelijke hemoglobinurie
● Oncologische aandoeningen● Zwangerschap● OAC ‐ HRT
● Nefrotisch syndroom ● Inflammatory Bowel Disease● Heparin‐inducedthrombocytopenie
● Hyperhomocysteïnemie● …
Antifosfolipiden syndroom
● Frequente verworven trombofilie○ Prevalentie 2‐4% ‐ incidentie 5/100.000/jaar
● Klinische criteria○ Trombose
■ Arterieel – veneus ‐microvasculair■ Massieve trombose / Ongewone plaats / Catastrofaal■ Hoog risico recurrente VTE
○ Obstetrische complicaties■ Premature geboorte■ Abortus

19‐3‐2019
7
Antifosfolipiden syndroom
● Labo criteria○ Auto‐immuunaandoening○ Antistoffen tegen fosfolipiden/proteïnen gebonden aan fosfolipiden
■ Lupus anticoagulans■ Anticardiolipine (IgG/IgM)■ Anti‐beta2‐glycoproteïne1 (IgG/IgM)
● Maar! ○ 2‐5% algemene populatie○ Gestegen bij infectie, andere auto‐immuunaandoeningen
Antifosfolipiden syndroom
● Etiologie○ Primair○ Secundair
■ SLE, andere auto‐immuunziekten■ Lymfoproliferatieve ziekten■ Acute of chronische infectie
● R/ voortgezette anticoagulatie○ Ernstige trombose○ Blijvend hoge levels antistoffen

19‐3‐2019
8
COUMARINE VAN MARC
Prof. Marc Verstraete, 1925‐2018

19‐3‐2019
9
Warfarine
Synthesis of Non-Functional
Coagulation Factors
Antagonismof
Vitamin K
Coumarins: Mechanism of action?
Vitamin K
VIIIXXII
PSPC
6h T1/2
18-24h
40-50h
48-60h
6-8h48h

19‐3‐2019
10
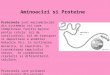
Clearance of Vitamin K‐dependent Proteins
0 20 40 60 80
100
40
60
80
30
Time after administration of warfarin (hours)
Activity (%
)
50
70
90
Prothrombin
Factor XFactor IXProtein CFactor VII
Warfarin‐induced Skin Necrosis

19‐3‐2019
11
PP
PP
UFH (MW 15 000) Xa = IIa
LMWH (MW < 8000) Xa >> IIa
Depolymerized
Heparin and LMWH : activation of antithrombin
Heparine‐induced trombocytopenie (HIT)
● Immuungemedieerde reactie○ Antistoffen tegen complex heparine ‐ platelet factor 4
● Trombocytopenie● Trombose

19‐3‐2019
12
Nieuwe Bloedverdunners
DABIGATRAN (PRADAXA)RIVAROXABAN (XARELTO)APIXABAN (ELIQUIS)EDOXABAN (LIXIANA)
VIIa
Xa
IXa
XIa
XIIa
DOACs: Factor Xa of Trombine‐inhibitoren
Tissue factor
Fibrinogen Fibrin clot
Factor II(prothrombin)
RivaroxabanApixabanEdoxaban
×Daibgatran

19‐3‐2019
13
www.phri.ca
Antiphospholipid antibody (triple positive): Rivaroxaban versus warfarin
Pengo V, et al. Blood 2018; 132: 1365‐71.