-
8/6/2019 Predicting Incomplete Uterine Rupture With
Vaginal.22[1]
1/5
Predicting Incomplete Uterine Rupture With
Vaginal Sonography During the Late SecondTrimester in Women With
Prior Cesarean
HIDEO GOTOH, MD, HIDEAKI MASUZAKI, MD, ATSUSHI YOSHIDA, MD,
SHUICHIRO YOSHIMURA, MD, TSUNETAKE MIYAMURA, MD, AND
TADAYUKI ISHIMARU, MD, PhD
Objective: To evaluate the usefulness of serial transvaginal
ultrasonographic measurement of the thickness of the lower
uterine segment in the late second trimester for predicting
the risk of intrapartum incomplete uterine rupture in
women with previous cesarean delivery.
Methods: Serial transvaginal ultrasonography with full
bladder was performed in 374 women without previous cesar-
ean delivery (control group) and 348 women with previous
cesarean delivery (cesarean group) from 19 to 39 weeks
gesta-
tion. The thickness of the lower uterine segment was
measured
in the longitudinal plane of the cervical canal.
Results: The thickness of the lower uterine segment de-
creased from 6.7 2.4 mm (mean standard deviation [SD]) at
19 weeks gestation to 3.0 0.7 mm at 39 weeks gestation in
the control group, but the thickness was more than 2.0 mm
throughout this period in each control subject. In the
cesareangroup, the thickness decreased from 6.8 2.3 mm at 19
weeks
to 2.1 0.7 mm at 39 weeks gestation and was significantly
thinner than that of the control group after 27 weeks
gestation
(P
-
8/6/2019 Predicting Incomplete Uterine Rupture With
Vaginal.22[1]
2/5
measurements) with previous cesarean delivery (cesar-ean group).
Only a single measurement was made foreach fetus. Between January
1995 and December 1998,722 women were examined prospectively by
transvag-inal ultrasonography between 19 and 39 weeks gesta-tion to
measure the thickness of the lower uterinesegment and to detect the
presence of any uterine defectwith a full bladder. All mothers were
healthy, withuncomplicated singleton pregnancies. Patients
repre-sented all women with uncomplicated pregnancies whoattended
the antenatal clinic at our department within
the above time periods. None of the patients reported inthis
study attempted vaginal birth after cesarean(VBAC).
The thickness of the lower uterine segment wasmeasured after the
bladder was identified in the longi-tudinal plane of the cervical
canal at transvaginal ultra-sonography (Figure 1). Ultrasonography
was per-formed by using Mochida equipment with a
7.5-MHztransvaginal transducer (Sonovista Ex model
meu-1581,Mochida, Japan). This system provides clear freeze-frames
and the use of on-screen calipers for directmeasurements. All
subjects were delivered after 37
weeks gestation. Measurement of the lower uterinesegment was
repeated at least three times in eachexamination, and the minimal
value was reported (to-tal: 722 measurements; control: 374;
cesarean delivery:348). Intraobserver and interobserver
variabilities in thecalculation of the thickness of the lower
uterine seg-ment obtained for the first 50 women in the
controlgroup were 4.7% and 5.5%, respectively. The sonogra-phers
were masked to the type of patient (controlcompared with cesarean)
to eliminate any possible bias.
Sonographic results at antepartum were comparedwith direct
intraoperative observation at cesarean de-livery. Incomplete
uterine rupture represented separa-tion of the uterine wall and
visceral peritoneum cover-ing the uterus.11 We examined differences
in thethickness of the lower uterine segment between
controlpregnant women and those with previous cesarean
delivery at each gestational week, as well as the patternof
change in the lower uterine segment during preg-nancy in each
group. We also used the antenatal andintraoperative data to examine
whether incompleteuterine rupture during delivery could be
predictedfrom lower uterine segment measurement during preg-nancy.
The surgeons were masked to the sonographicfindings at the time of
cesarean delivery.
The study protocol was approved by the EthicsReview Committee of
our institution, and a signedconsent form was obtained from each
subject. Datawere expressed as mean standard deviation (SD),
ormedian and range. Student t test and Mann-Whitney Utest were used
for comparison of continuous variables.Differences in uterine
thickness between control groupand cesarean group were evaluated by
unpaired t test,and those between the second and third trimesters
wereevaluated by paired t test. Fisher exact test was used
toexamine the association between ultrasonographicallydetermined
thickness of the lower uterine segment atdifferent stages of
pregnancy and incomplete uterinerupture at the time of cesarean.
Significance was con-sidered P .05. The sample size was sufficient
to detectdifferences at 5% level of significance with 80%
power.
Results
Patients in the cesarean group did not differ signifi-cantly
from those in the control group with respect tomaternal age,
parity, gestational age at delivery, infant
birth weight, and 1-minute and 5-minute Apgar scores(Table 1).
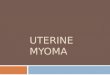
The thickness of the lower uterine segment inthe control group
decreased steadily from 6.7 2.4 mmat 19 weeks gestation to 3.0 0.7
mm at 39 weeksgestation, but the thickness was greater than 2.0 mm
inall cases (Figure 2). In the cesarean group, the thicknessof the
lower uterine segment decreased from 6.8
2.3 mm at 19 weeks gestation to 2.1 0.7 mm at 39weeks gestation
(Figure 2). Whereas the thickness ofthe lower uterine segment was
not different betweenthe two groups at 1926 weeks and 28 weeks
gesta-tion, it was significantly thinner in the cesarean than inthe
control group at 27 weeks and every week after 29weeks gestation (P
.05). Serial measurements of thelower uterine segment during
pregnancy showed thatin a subgroup of women with previous cesarean
deliv-ery, the uterine wall was persistently thin from the
Figure 1. Transvaginal ultrasonography showing the lower
uterine
segment and bladder full. Open arrow indicates uterine wall;
solid arrow
indicates bladder wall.
VOL. 95, NO. 4, APRIL 2000 Gotoh et al Measurement of Uterine
Thickness 597
-
8/6/2019 Predicting Incomplete Uterine Rupture With
Vaginal.22[1]
3/5
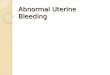
second trimester until the termination of pregnancy(thin group:
lower uterine segment was less thanmean 1 SD, n 12, Figure 3). In
another group of
women with previous cesarean delivery, the uterinewall decreased
in thickness progressively, in a mannersimilar to that of the
control group (nonthin group:lower uterine segment was mean 1 SD or
greater, n27, Figure 3). Eleven of the 12 women (91%) with alower
uterine segment less than the mean control 1SD in the late second
trimester had a surprisingly verythin uterine wall at cesarean
delivery; the fetal hair wasvisible through the amniotic membrane.
In all 27women with lower uterine segment greater than themean
control 1 SD, an intrapartum incomplete uter-
ine rupture at cesarean delivery did not develop (non-
thin group, P .001, Table 2).
Further analysis of transvaginal ultrasonographic
findings at 7 days before cesarean delivery (4 3 days)
and those at cesarean delivery showed that 17 of 23
women (74%) with lower uterine segment less than
2.0 mm before repeat cesarean delivery had an incom-
plete uterine rupture at cesarean delivery. On the other
hand, none of the 45 women with lower uterine seg-
ment of 2.0 mm or greater thickness demonstrated an
incomplete uterine rupture at cesarean delivery (P
.001, Table 2).
Figure 2. The mean thickness of the lower uterine segment in
controls
and women who have had a previous cesarean delivery. The
thickness
of the lower uterine segment was not different between the two
groups
at 1926 weeks and 28 weeks gestation (*). The lower uterine
segment
was significantly thinner in the cesarean group than in the
control
group at 27 weeks and 29 weeks gestation (P .05, unpaired t
test)
(**). The lower uterine segment was significantly thinner in
the
cesarean group than in the control group at every week after 30
weeks
gestation (P .01, unpaired t test) (***). SD standard
deviation.
Figure 3. Correlation between thickness of the lower uterine
segment
at late second trimester and third trimester in the thin group
and the
nonthin group. Note that in subjects in whom the lower
uterine
segment was thin from the late second trimester, intrapartum
incom-
plete uterine rupture was more likely to develop. NS not
significant.
Table 1. Characteristics of Controls and Women WithPrevious
Cesarean Delivery
Control Cesarean P
n 374 348
Maternal age (y) 28.9 5.3 31.9 4.6 NS*
Parity 1.9 0.9 1.4 0.8 NS*
Gestational age at
delivery (wk)
38.9 1.5 38.2 1.2 NS*
Birth weight (g) 3121 458 2953 483 NS*Apgar score 1-min 9 (8 10)
8 (710) NS
Apgar score 5-min 9 (8 10) 9 (8 10) NS
NS not significant.Data are presented as mean standard
deviation, or median
(range).* Student t test. Mann-Whitney U test.
Table 2. Association Between UltrasonographicallyDetermined
Thickness of the Lower UterineSegment at Different Stages of
Pregnancy andIntrapartum Incomplete Uterine Rupture atCesarean
Thickness of lower uterine
segment(mm)
Intrapartum incomplete
uterine rupture
Yes(%) No (%)
At second trimester
Mean control 1 SD 11 (91) 1 (9)
Mean control 1 SD 0 (0) 27 (100)
Within 7 d (4 3 d) of
cesarean
2 mm 17 (74) 6 (26)
2 mm 0 (0) 45 (100)
SD standard deviation.(At second trimester and within 7 d of
cesarean: P .001).
598 Gotoh et al Measurement of Uterine Thickness Obstetrics
& Gynecology
-
8/6/2019 Predicting Incomplete Uterine Rupture With
Vaginal.22[1]
4/5
Discussion
In 1988, ACOG recommended that carefully selected
patients be encouraged to have a trial of labor after a
single previous cesarean delivery.19 Several investiga-
tors have emphasized the efficacy and safety of vaginal
birth after cesarean delivery in a large series of stud-
ies.20,21 The most common complication of vaginal
delivery after a previous cesarean delivery is uterine
rupture, and the frequency varies between 0.5 to 0.8%
with previous lower uterine segment incision, as re-
ported in a recent study.22 Although maternal mortality
is rare, rupture of the uterus may be associated with
significant morbidity for the mother and fetus in
women with a history of low transverse cesarean deliv-
ery. Jones et al23 and Scott24 reported four perinatal
deaths among 20 cases of uterine rupture with a previ-
ous low-segment cesarean scar. Two of these infants
had long-term neurologic impairment, and three
women required hysterectomy.
Several investigators have examined the accuracy of
various diagnostic procedures in the detection of uter-ine
rupture in women with previous cesarean delivery.Hysterography,12
pelvic examination,13 and amniogra-phy14 have been used, but their
usefulness has not beenconfirmed. Hebisch et al25 compared the
results ofultrasonography with those of magnetic resonance im-aging
(MRI). They demonstrated that vaginal ultra-sonography provided
more accurate information aboutthe condition of the scarred
myometrium of the isthmusthan MRI. Other studies have shown that
ultrasonogra-phy may predict uterine rupture in women with
previ-
ous cesarean delivery. Rozenberg et al17 indicated thatthe risk
of uterine rupture in the presence of a defectivescar was related
directly to the degree of thinning of thelower uterine segment as
measured by transabdominalultrasonography at or near 37 weeks
gestation. Inparticular, they demonstrated that this risk
increasedsignificantly when the thickness was 3.5 mm or less.The
use of this cutoff value showed an excellent sensi-tivity (88.0%)
for ultrasonography, with a negativepredictive value of 99.3%. On
the other hand, Fukuda etal18 examined 41 low-segment transverse
cesarean de-livery scars by transperineal and transvaginal
longitu-
dinal scans. A wall thickness of 2 mm or less wasconsidered a
sign of poor healing. At operation, theymeasured the thickness of
the lower uterine segment byophthalmic calipers just after incising
the uterus and
before rupture of the membranes, and reported nofalse-positive
or false-negative results when using ul-trasonography.
Our results showed that when the thickness mea-sured by
transvaginal ultrasonography is less than2 mm within 1 week of
delivery, the lower uterine
segment may show an incomplete uterine rupture. Thepositive and
negative predictive values were 73.9% and100%, respectively.
Furthermore, a thickness of lessthan the control mean-SD at the
second trimester ishighly predictive of the development of
incompleteuterine rupture at delivery. The positive and
negativepredictive values were 91.7% and 100%, respectively. A
careful examination of our results showed that thepredictive
value at full term was lower than that at thesecond trimester. This
finding is probably due to furtherthinning of the lower uterine
segment at term as thewall is stretched by the presenting part.
Although thedefects of the lower uterine segment can be detected
inthe second trimester, our results showed that the mostclinically
useful information regarding the status of thelower uterine segment
is obtained when ultrasonogra-phy is performed before 36 weeks
gestation. Measure-ments obtained at that time avoid problems
associatedwith engagement of the presenting part in the pelvis
orthe physiologic reduction in the volume of amnioticfluid
occurring at later stages of pregnancy. Previousstudies that
examined the importance of detecting uter-ine rupture by
ultrasonography emphasized the valueof such evaluation at
term,17,18 but our study stressesthe importance of performing such
measurement dur-ing the late second trimester. We showed that
serialmeasurements of the lower uterine segment by trans-vaginal
ultrasonography during the second trimestermight predict incomplete
uterine rupture at term.
Although none of our cases with incomplete uterinerupture
progressed to a complete uterine rupture dur-ing labor, incomplete
uterine rupture represents a high
risk for complete uterine rupture because in some caseswith
incomplete uterine rupture, uterine contents areseparated from the
peritoneal cavity only by the vis-ceral peritoneum covering the
uterus.
In women with previous cesarean delivery, uterinerupture may
occur after labor even in those withlower-uterine segmental
incision. Thus, early predictionof uterine rupture before the onset
of labor should alsoreduce the frequency of uterine rupture after
delivery.Transvaginal ultrasonography could therefore be
con-sidered the standard diagnostic procedure that canpredict
accurately intrapartum uterine rupture in
women with previous cesarean delivery. Our resultsemphasize the
importance of measuring the uterine scarin the late second
trimester in women with previouscesarean delivery.
References
1. Chew SY. Uterine rupture in labor: A 10-year review.
Singapore
Med J 1984;25:249.
VOL. 95, NO. 4, APRIL 2000 Gotoh et al Measurement of Uterine
Thickness 599
-
8/6/2019 Predicting Incomplete Uterine Rupture With
Vaginal.22[1]
5/5
2. Megafu U. Factors influencing maternal survival in
ruptured
uterus. Int J Gynaecol Obstet 1985;23:47580.
3. Rachagan SP, Raman S, Balasundram G, Balakrishnan S.
Rupture
of the pregnant uterusa 21-year review. Aust N Z J Obstet
Gynaecol 1991;31:3740.
4. Saglamtas M, Vicdan K, Yalcin H, Yilmaz Z, Yesilyurt H,
Gokmen
O. Rupture of the uterus. Int J Gynaecol Obstet 1995;49:9
15.
5. Phelan JP, Clark SL, Diaz F, Paul RH. Vaginal birth after
cesarean.
Am J Obstet Gynecol 1987;157:15105.
6. Flamm BL, Lim OW, Jones C, Fallon D, Newman LA, Mantis
JK.Vaginal birth after cesarean section: Results of a multicenter
study.
Am J Obstet Gynecol 1988;158:107484.
7. Nielsen TF, Ljungbald U, Hagberg H. Rupture and dehiscence
of
cesarean section scar during pregnancy and delivery. Am J
Obstet
Gynecol 1989;160:56973.
8. Meehan FP, Burke G, Kehoe JT, Magani IM. True
rupture/scar
dehiscence in delivery following prior section. Int J
Gynaecol
Obstet 1990;31:24955.
9. Chazotte C, Cohen WR. Catastrophic complications of
previous
cesarean section. Am J Obstet Gynecol 1990;163:738 42.
10. Leung AS, Leung EK, Paul RH. Uterine rupture after
previous
cesarean section delivery: Maternal and fetal consequences. Am
J
Obstet Gynecol 1993;169:94550.
11. Cunningham FG, MacDonald PC, Gant NF, Leveno KJ,
Gilstrap
LC, Hankins GDV, et al. Williams obstetrics. 20th ed.
Norwalk,
Connecticut: Appleton & Lange, 1997.
12. Baker K. Vaginal delivery after lower uterine cesarean
section.
Surg Gynecol Obstet 1955;100:6903.
13. Meehan FP, Moolgaoker AS, Stallworthy J. Vaginal delivery
under
caudal analgesia after cesarean section and other major
uterine
surgery. BMJ 1972;2:7402.
14. Caterini HR, Rubino SM, Kaminetzky HA. Amniography
during
subsequent pregnancy for evaluating the post-cesarean
section
uterine scar. Obstet Gynecol 1972;39:71720.
15. Thubisi M, Ebarahim A, Moodley J, Shweni PM. Vaginal
delivery
after previous cesarean section: Is X-ray pelvimetry necessary?
Br J
Obstet Gynaecol 1993;100:4214.
16. Michaels WH, Thompson HO, Bout A, Schreiber FR, Michaels
SL,
Karo J. Ultrasound diagnosis of defects in the scarred lower
uterinesegment during pregnancy. Obstet Gynecol 1988;71:11220.
17. Rozenberg P, Goffinet F, Philippe HJ, Nisand I.
Ultrasonographic
measurement of lower uterine segment to assess risk of defects
of
scarred uterus. Lancet 1996;347:2813.
18. Fukuda M, Shimizu T, Ihara Y, Fukuda K, Natsuyama E,
Mochi-
zuki M. Ultrasound examination of caesarean scars during
preg-
nancy. Arch Gynecol Obstet 1991;248:12938.
19. American College of Obstetrics and Gynecologists. Maternal
and
fetal medicine: Guideline for vaginal delivery after previous
cesar-
ean birth. ACOG committee opinion no. 64. Washington, DC:
American College of Obstetrics and Gynecologists, 1988.
20. Flamm BL, Newman LA, Thomas SJ, Fallon D, Yoshida MM.
Vaginal birth after cesarean section delivery: Results of a
5-year
multicenter collaborative study. Obstet Gynecol 1990;76:7504.21.
Miller DA, Diaz FG, Paul RH. Vaginal birth after cesarean: A
10-year experience. Obstet Gynecol 1994;84:2558.
22. Flamm B, Goings JR, Liu Y, Wolde-Tsakid G. Elective
repeat
cesarean delivery versus trial of labor: A prospective
multicenter
study. Obstet Gynecol 1994;83:92732.
23. Jones RO, Nagashima AW, Hatnett-Goodman MM, Goodlin RC.
Rupture of low transverse cesarean scars during trial of
labor.
Obstet Gynecol 1991;77:8157.
24. Scott JR. Mandatory trial of labor after cesarean delivery:
Alterna-
tive viewpoint. Obstet Gynecol 1991;77:8114.
25. Hebisch G, Kirkienen P, Haldemann R, Paakkoo E, Huch A,
Huch
R. Comparative study of the lower uterine segment after
cesarean
section using ultrasound and magnetic resonance tomography.
Ultraschall Med 1994;15:1126.
Address reprint requests to:
Hideo Gotoh, MDDepartment of Obstetrics and GynecologyNagasaki
University School of Medicine1-7-1 SakamotomachiNagasaki,
852-8501
Japan
Received June 21, 1999.
Received in revised form October 5, 1999.Accepted October 15,
1999.
Copyright 2000 by The American College of Obstetricians and
Gynecologists. Published by Elsevier Science Inc.
600 Gotoh et al Measurement of Uterine Thickness Obstetrics
& Gynecology