Embed Size (px)
Citation preview

DOACs: QUANDO DOSARNE L’ATTIVITA’ E COME INTERPRETARE I RISULTATI
Sophie Testa Centro Emostasi e Trombosi
Dipartimento di Medicina di Laboratorio e Radiologia ASST Cremona
PUNTI DI DISCUSSIONE
• Perché parliamo di misurazione dell’attività anticoagulante dei DOACs
• Quando misurare
• Come misurare
• Come interpretare i risultati
DOACs
At present, DOACs are administered at fixed dose in relation to clinical
indications, individual characteristics and renal function without need for
laboratory monitoring, because:
1. Pharmacologycal studies have shown that DOAC have predictable
anticoagulant response in “standard” clinical condition
2. Clinical trials have been successfully conducted at fixed-dose regimen, without
laboratory controls and without the availability of specific antidotes, in two
clinical conditions (NVAF and VTE)

DOAC CHARACTERISTICS
Gosselin R et al, Thromb Haemost 2018

DOACs DOSAGE
DOSING ADJUSTEMENT IS
BASED ON PHARMACOKINETIC CONSIDERATIONS
(Clinical characteristics and
renal function)
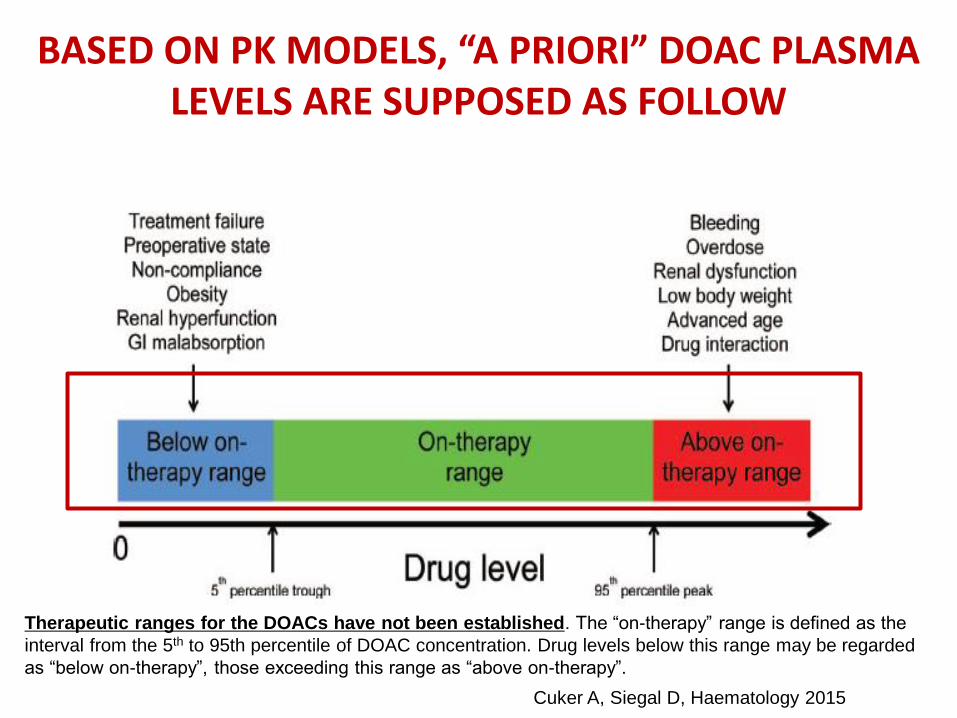
BASED ON PK MODELS, “A PRIORI” DOAC PLASMA LEVELS ARE SUPPOSED AS FOLLOW
Therapeutic ranges for the DOACs have not been established. The “on-therapy” range is defined as the
interval from the 5th to 95th percentile of DOAC concentration. Drug levels below this range may be regarded
as “below on-therapy”, those exceeding this range as “above on-therapy”.
Cuker A, Siegal D, Haematology 2015
BUT, THE REALITY IS THAT …
• High inter/intra individual variability has been demonstrated in the real
world patient population
• Pharmacological modifications have been showed in relation to: drug
interaction, liver and renal function, age , weight, comorbidities….
• After DOAC introduction in clinical practice specific antidotes have been
requested and are now available
• Laboratory measurements are recommended, at the moment, at least in
particular clinical conditions
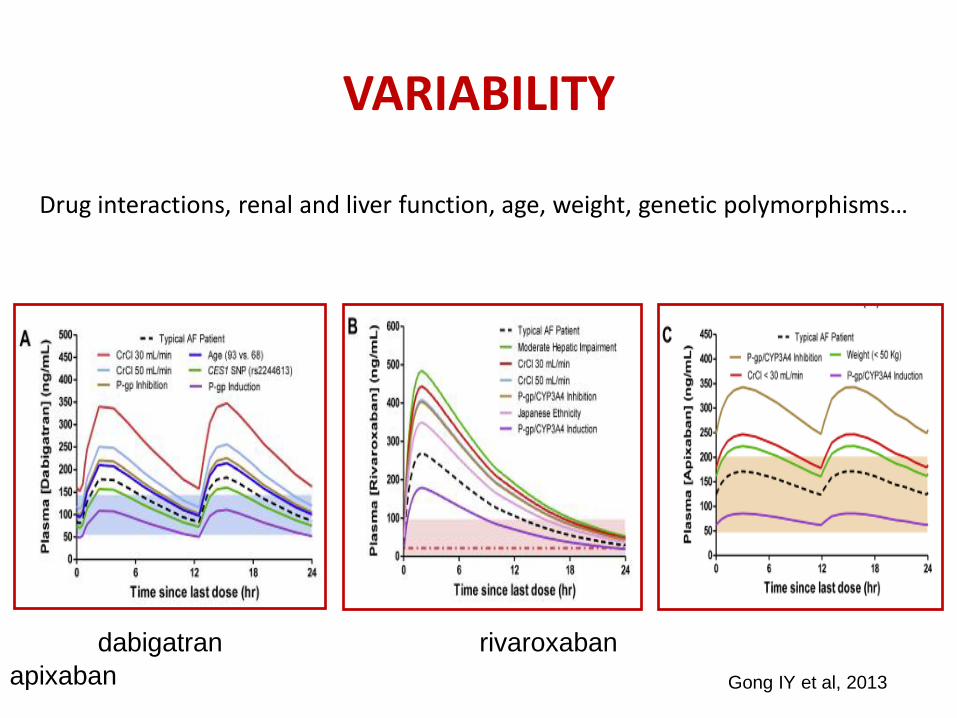
VARIABILITY
Drug interactions, renal and liver function, age, weight, genetic polymorphisms…
dabigatran rivaroxaban
apixaban
Gong IY et al, 2013

EXPECTED PEAK AND TROUGH DOAC LEVELS IN NVAF AND VTE PATIENTS ENROLLED
IN PHASE II-III CLINICAL STUDIES
Gosselin R et al, Thromb Haemost 2018
aMean (25th–75th percentile); bMean (5th–95th percentile); cMedian (5th–95th percentile); dMedian (1.5 x IQR); eMedian (IQR).

DOACs INTER-INDIVIDUAL VARIABILITY
Population CV%
Healthy and young volunteers ~ 20
Phase III randomized clinical studied ~ 40
“Real world” patients ~ up to 100
Testa S et al, Thromb Res 2016, 2019
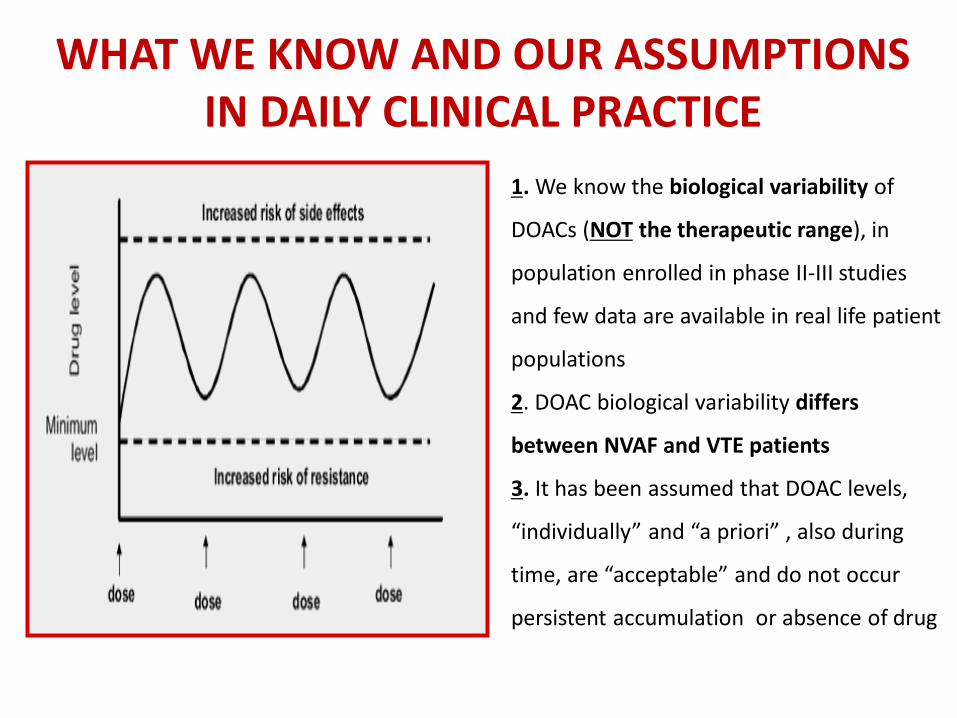
WHAT WE KNOW AND OUR ASSUMPTIONS IN DAILY CLINICAL PRACTICE
1. We know the biological variability of
DOACs (NOT the therapeutic range), in
population enrolled in phase II-III studies
and few data are available in real life patient
populations
2. DOAC biological variability differs
between NVAF and VTE patients
3. It has been assumed that DOAC levels,
“individually” and “a priori” , also during
time, are “acceptable” and do not occur
persistent accumulation or absence of drug
ARE THESE PHARMACOLOGICAL
INFORMATIONS USEFUL FROM A
CLINICAL POINT OF VIEW?
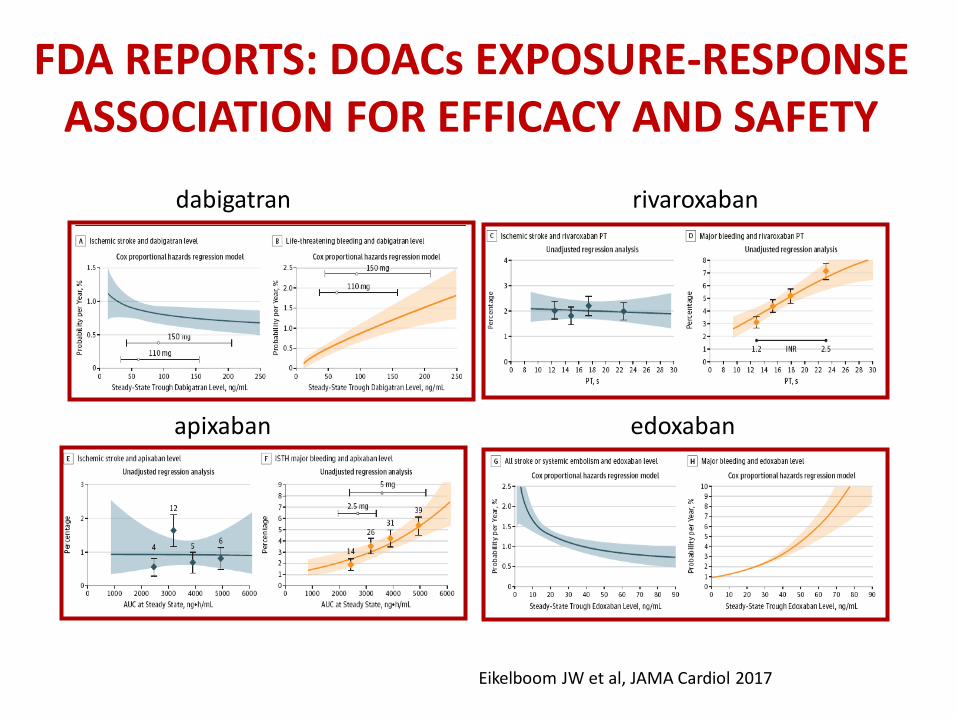
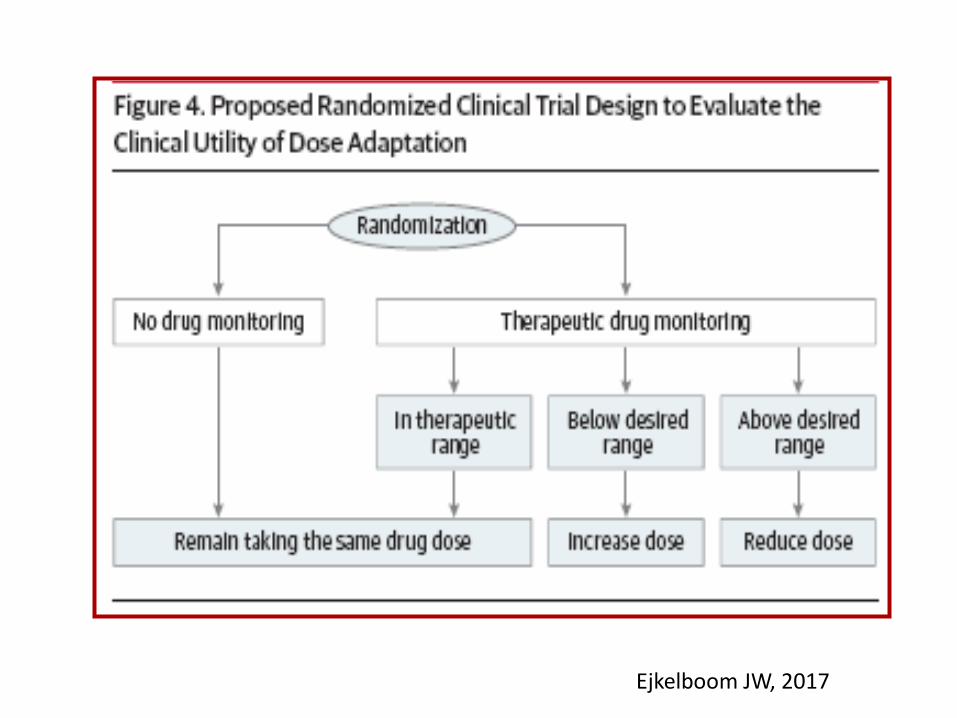
FDA REPORTS: DOACs EXPOSURE-RESPONSE ASSOCIATION FOR EFFICACY AND SAFETY
dabigatran rivaroxaban
apixaban edoxaban
Eikelboom JW et al, JAMA Cardiol 2017

DOACs AND THE LAB
Test Recommendation Comments
ClCr 1.Before starting DOACs and in the follow up to continue treatments (or adapt posology).
2. CrCl is also considered as surrogate of good anticoagulant action
- ClCr not validated in older population
- CrCl>30ml/min not correlate with aXa drugs
AST/ALT 1. Before starting DOACs and in the follow up to continue treatments
No clear timing of controls
Blood Cell Count
Should be recommended Before starting and during the follow up
PT/aPTT Not recommended to assess levels of anticoagulation
Should be recommended before starting DOAC to assess haemostatic status
DOAC specific
test
In special clinical conditions There is still no unanimous consensus
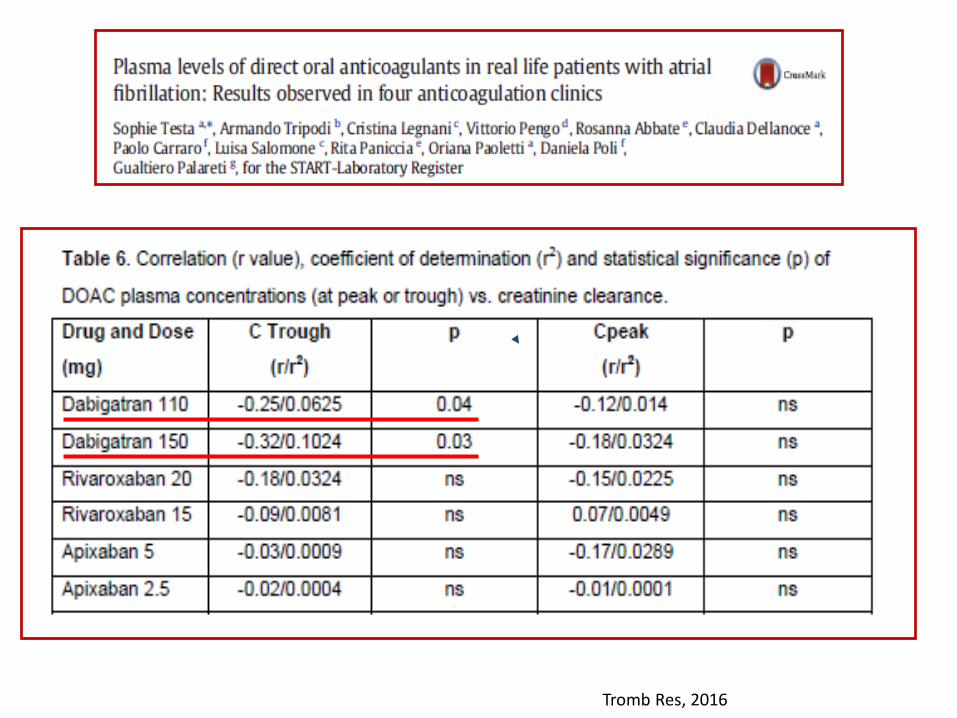
Tromb Res, 2016

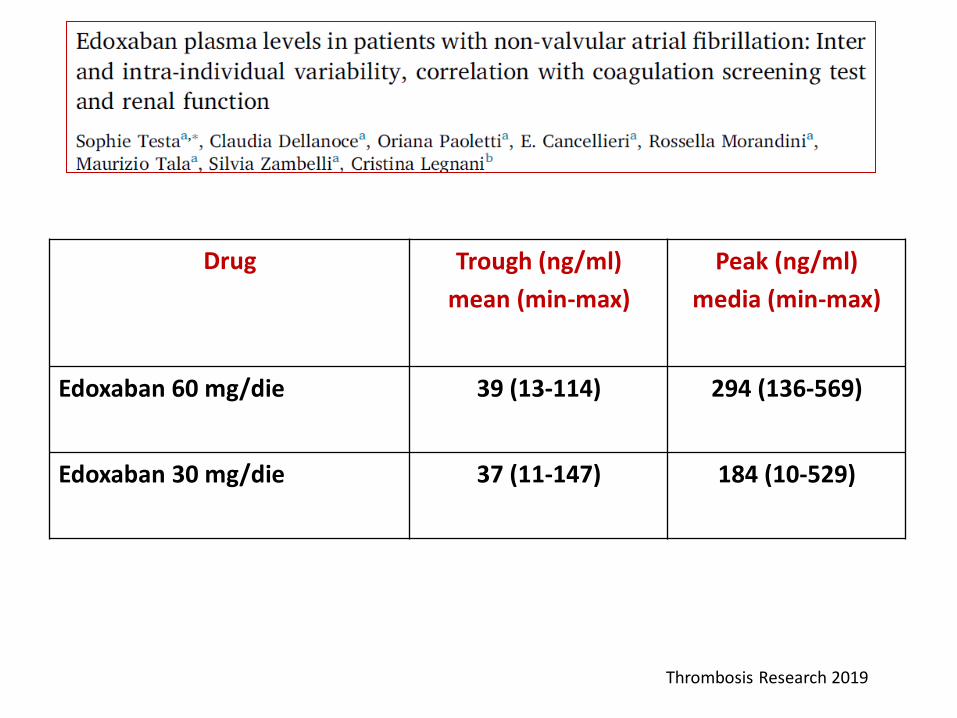
EDOXABAN PLASMA LEVELS IN PATIENTS WITH NON-VALVULAR ATRIAL FIBRILLATION: INTER AND INTRA-INDIVIDUAL VARIABILITY, CORRELATION WITH
COAGULATION SCREENING TEST AND RENAL FUNCTION
Thromb Res, 2019

DOACs MEASUREMENT
1. PERIODICAL MEASUREMENT (MONITORING) TO FREQUENT DOSE-
ADJUSTEMENT (currently no evidences…)
2. MEASUREMENT (CONTROL) TO HIGHLIGHT UNDER/OVER ANTICOAGULATION IN RELATION TO RISK OF BLEEDING AND THROMBOSIS
3. MEASUREMENT IN SPECIAL CLINICAL CONDITIONS (Patients presenting in emergency with bleeding/thrombosis, immediate reverse of anticoagulation, perioperative management, renal disease, liver disease, suspicion or known interaction with other drugs, elderly patients, under/over weight….but no still unanimous consensus)
Eikelboom JW et al, 2017

IN RECENT LITERATURE

These retrospective observational studies, conducted on small cohort of patient
population, highlighted :
1. A role in drug monitoring in the management of patients in selected
circumstances (surgery, bleeding thromboembolic complications, renal
failure, drug interactions, overweight)
2. No current indications in routine (frequent) drug level monitoring because it
rarely affected clinical management
3. The necessity of studies to further establish association between drug-
specific DOAC levels and clinical outcomes, to define appropriate indications
for testing
Thromb Res 2016; Int J Lab Hem 2017; JTH 2018
1. PERIODICAL MEASUREMENTS
(MONITORING) TO
DRUG DOSE-ADJUSTMENT


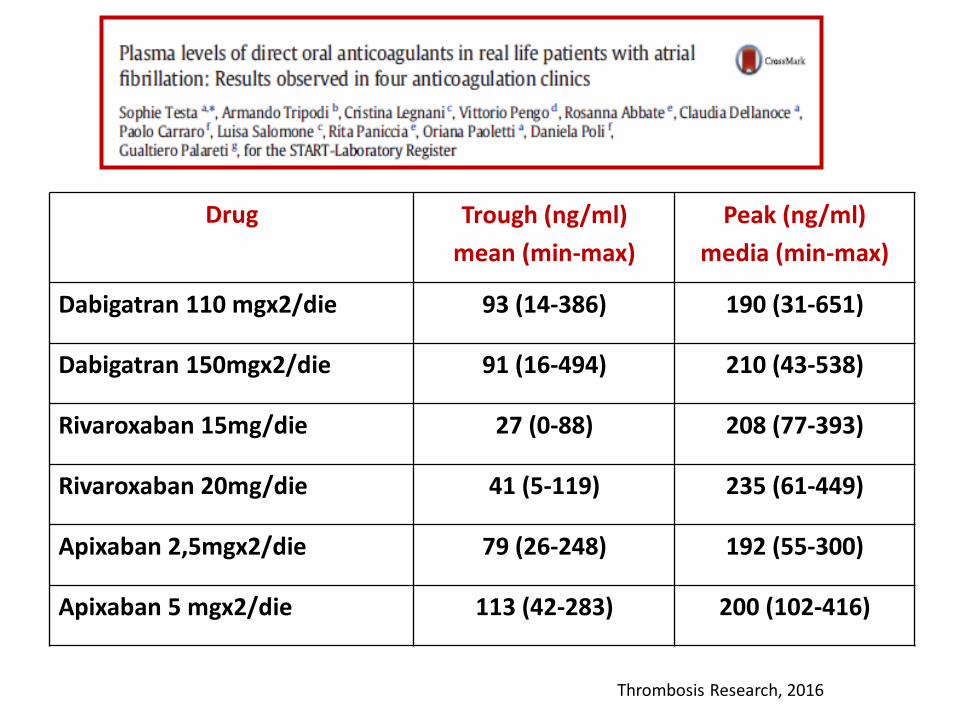
Drug Trough (ng/ml)
mean (min-max)
Peak (ng/ml)
media (min-max)
Dabigatran 110 mgx2/die 93 (14-386) 190 (31-651)
Dabigatran 150mgx2/die 91 (16-494) 210 (43-538)
Rivaroxaban 15mg/die 27 (0-88) 208 (77-393)
Rivaroxaban 20mg/die 41 (5-119) 235 (61-449)
Apixaban 2,5mgx2/die 79 (26-248) 192 (55-300)
Apixaban 5 mgx2/die 113 (42-283) 200 (102-416)
Thrombosis Research, 2016
Drug Trough (ng/ml)
mean (min-max)
Peak (ng/ml)
media (min-max)
Edoxaban 60 mg/die 39 (13-114) 294 (136-569)
Edoxaban 30 mg/die 37 (11-147) 184 (10-529)
Thrombosis Research 2019

Ejkelboom JW, 2017
Ejkelboom JW, 2017

2.
PERIODICAL MEASUREMENT
(CONTROL) TO HIGHLIGHT
UNDER/OVER ANTICOAGULATION
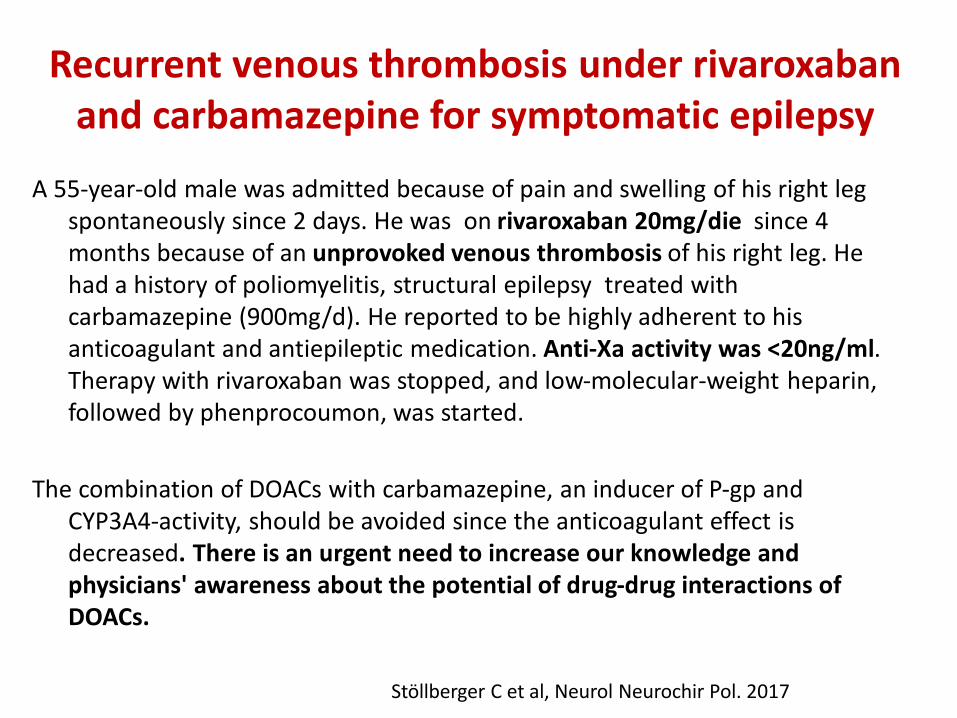
Recurrent venous thrombosis under rivaroxaban and carbamazepine for symptomatic epilepsy
A 55-year-old male was admitted because of pain and swelling of his right leg spontaneously since 2 days. He was on rivaroxaban 20mg/die since 4 months because of an unprovoked venous thrombosis of his right leg. He had a history of poliomyelitis, structural epilepsy treated with carbamazepine (900mg/d). He reported to be highly adherent to his anticoagulant and antiepileptic medication. Anti-Xa activity was <20ng/ml. Therapy with rivaroxaban was stopped, and low-molecular-weight heparin, followed by phenprocoumon, was started.
The combination of DOACs with carbamazepine, an inducer of P-gp and CYP3A4-activity, should be avoided since the anticoagulant effect is decreased. There is an urgent need to increase our knowledge and physicians' awareness about the potential of drug-drug interactions of DOACs.
Stöllberger C et al, Neurol Neurochir Pol. 2017

Breuer L, N Engl J Med 2013
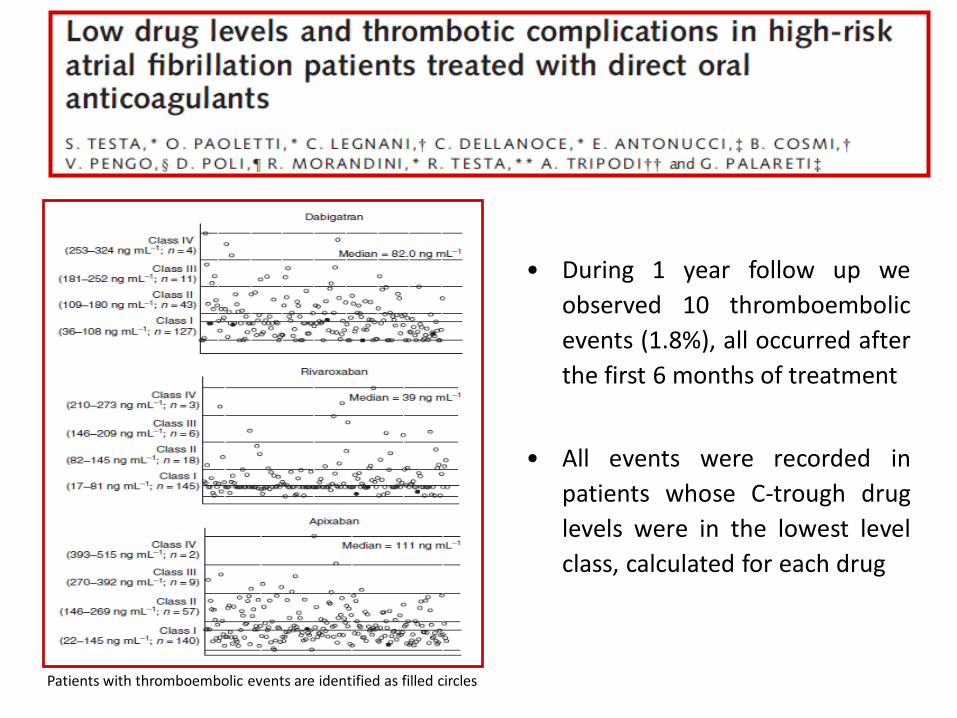
LEVELS
• During 1 year follow up we
observed 10 thromboembolic
events (1.8%), all occurred after
the first 6 months of treatment
• All events were recorded in
patients whose C-trough drug
levels were in the lowest level
class, calculated for each drug
Patients with thromboembolic events are identified as filled circles

THROMBOEMBOLIC RISK IN PATIENTS WITH LOW DOACs LEVEL AND HIGHER CHA2DS2-VASc
CHA2DS2-VASc >3.0
(291/595pts; 51.5%)
Class I n°
(Lower drug levels)
Class II, III,IV n°
(Highest drug levels)
Total
(n)
Thrombosis
10
0
10
No Thrombosis
117
164
281
10/127
(7.9%)
0/164
(0%)

CONCLUSION
• Our data show a relationship between low DOACs trough plasma levels and subsequent thrombotic events
• Especially in high cardiovascular risk patients with low DOACs levels
• DOACs measurement seems particularly indicated in these patients

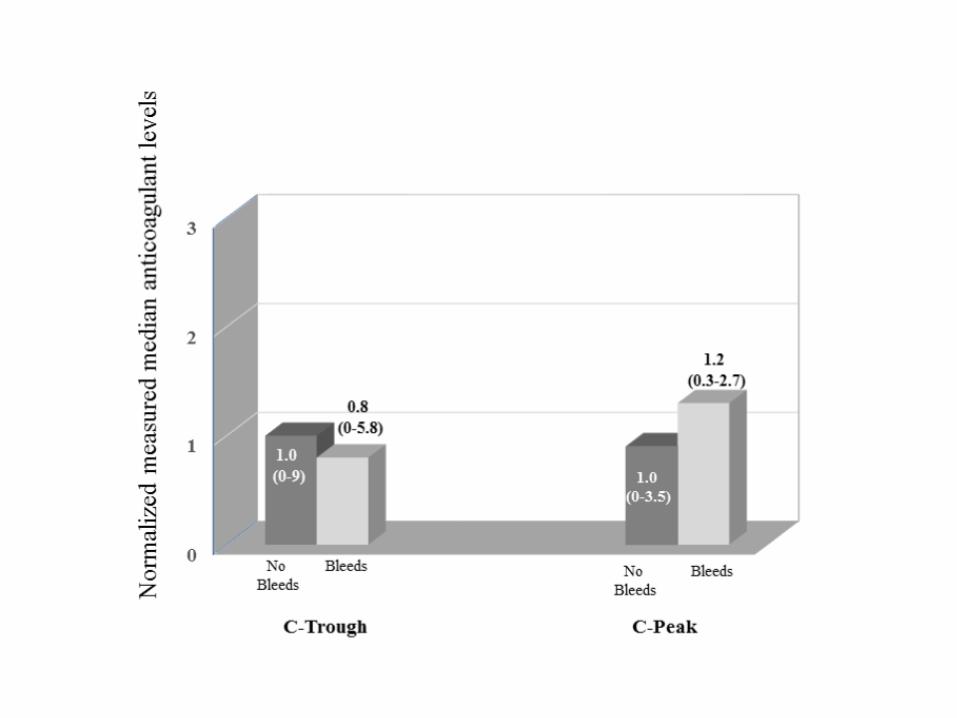
DRUG LEVELS AND BLEEDING COMPLICATIONS
IN ATRIAL FIBRILLATION PATIENTS TREATED WITH DIRECT ORAL ANTICOAGULANTS
• To evaluate a possible relationship between DOACs C-trough and C-
peak anticoagulant levels, measured at steady state within the first
month of treatment, and bleeding events observed during one year
follow up.
JTH, 2019

The MAS study (“Measure And See”)
Measurement of the anticoagulant levels in patients treated with Direct
Oral Anticoagulants (DOACs) and observation of bleeding and thrombotic complications during follow up.
Promoted and funded by the «Arianna Anticoagulazione Foundation» (Bologna, Italy), Coordinator: prof. Gualtiero Palareti In collaboration with: FCSA (Federation of Italian Anticoagulation Clinics)
To confirm this preliminary results a large prospective, multicenter, observational study - The MAS (Measure And See) Study, conducted within FCSA and the START Registry- has been planned and is started in June 2018.
The question: Is DOAC testing usefull to highlight patient at higher risk of complication? The answer: The MAS Study
Powell JR, JAMA 2015
• Patients presenting in emergency with adverse events (Thrombosis, Bleeding)
• Immediate reverse of anticoagulation
• Perioperative management
• Renal Disease
• Liver Disease
• Suspicion or known interaction with other drugs
• Elderly patients
• Under/over weight
3. DOAC MEASUREMENT IN SPECIAL
CLINICAL CONDITIONS
Pengo V et al, 2011
DOACs MEASUREMENT
=
HELPFUL TO GUIDE APPROPRIATE
MANAGEMENT

Caso 1: Stroke ischemico in donna di 58 anni trattata con dabigatran 150 mg 1cpx2/die per FANV, ultima dose assunta 1 ora prima del ricovero. Dosaggio dabigatran (dTT) <15 ng/mL a due controlli successivi. Si procedeva quindi a terapia trombolitica, profilassi eparinica e terapia con AVK. Caso 2: Emorragia cerebrale post-traumatica in pz trattato con dabigatran 150mgx2die per FANV . Dosaggio dabigatran = 189 ng/mL (6 ore dopo l’ultima assunzione del farmaco). Praticata infusione di idarucizumab (Praxbind®) 2.5 g 1flx2. Al termine dell’infusione dosaggio dabigatran (dTT)=2.28 ng/mL ( sempre negativo nelle 24 ore successive). TC encefalo a distanza di un mese evidenziava pressochè completo riassorbimento dell’emorragia.Ripresa terapia con dabigatran.


• Laboratory measurements were performed centrally and were
not used to guide therapy.
• dTT results were normal in ¼ of the study population. This group
of patients would not be expected to benefit from the
administration of idarucizumab.
• It will be useful to have activity measurements available for the
various direct oral anticoagulants in real time to help guide the
treatment of such patients and to prevent overutilization of
what will surely be a costly medication
Bauer KA , N Engl J Med 2015

PERIOPERATIVE MANAGEMENT: THE GUIDELINES
Schulman S, J Intern Med 2013
PERIPROCEDURAL MANAGEMENT OF DOAC SHOULD BE GUIDED BY
ACCURATE LABORATORY TESTS
Interruption of DOAC should not be based only on their respective
half-life but also on the residual drug concentration
• Poor correlation between renal function and plasma
concentration of apixaban and rivaroxaban was found except
dabigatran measured at trough (Testa S et al, TR 2016)
• Mass spectrometry measured dabigatran level greater than
20ng/ml in nearly 16% of patients undergoing high bleeding risk
procedures (Douketis JD et al JT&H 2016)
Douxfils J et al, Reg Anesthesia and Pain Medicine, Sept 2016

Douketis J et al, Jama Intern Med 2019

COMMENTS on JAMA • Altogether the study showed 3.43% of major and clinically
relevant, plus 5% of minor bleeding complications
• The adopted management algorithm was based on the DOACs pharmacokinetics, CrCl and the procedure-associate bleeding risk.
• However, DOACs plasma levels have a high inter-individual variability; furthermore, the drug elimination rate may not be constant in all patients
• Our question is: may we be really confident that a standardized model, which never takes into consideration the high drug level variability or the high risk of bleeding both from individual patients or from anesthesiology procedures, may be the best strategy to be adopted in all patients?
Testa S et al, JAMA 2019

1. At the beginning of DOAC treatment to confirm adsorption
and to know patient’s individual anticoagulant levels
2. Over-under weight
3. In case of potential interferences with co-medications
4. Co-morbidities
5. Bleeding and thromboembolic complications
6. Surgical and invasive procedures
Blood Transfusion, 2017


HOW TO MEASURE? 1. PT and aPTT react differently with DOACs in relation to type of
drug and type of reagent
2. Patients having the same DOAC plasma concentration may show
different PT or aPTT results
3. Normal PT/aPTT results cannot exclude significantly high
concentrations of DOACs, such as abnormal prolongation could
be caused by defects of coagulation other than those stemming
from the drug being taken by the patients
4. Specific test are easily available (dTT, Ecarin Tests, specified
calibrated aXa)
5. The use of PT or aPTT in clinical practice to evaluate DOAC
anticoagulant activity could cause dangerous misinterpretations.
Kitchen S et al, BJH 2015; Douxfils 2012, Douxfils 2013, Testa S et al, JTH 2016, Gosselin R 2018

COME INTERPRETARE I RISULTATI (I) • Considerare : tipo di farmaco, mono/bi-somminitrazione giornaliera,
orario dell’ultima assunzione
• Il laboratorio deve riportare sul referto i valori relativi all’assenza di farmaco, cioè i limiti inferiori di sensibilità analitica del test in uso
Test Negativo (ng/mL)*
dabigatran < 15
apixaban < 25
edoxaban < 20
rivaroxaban < 20 *ASST Cremona
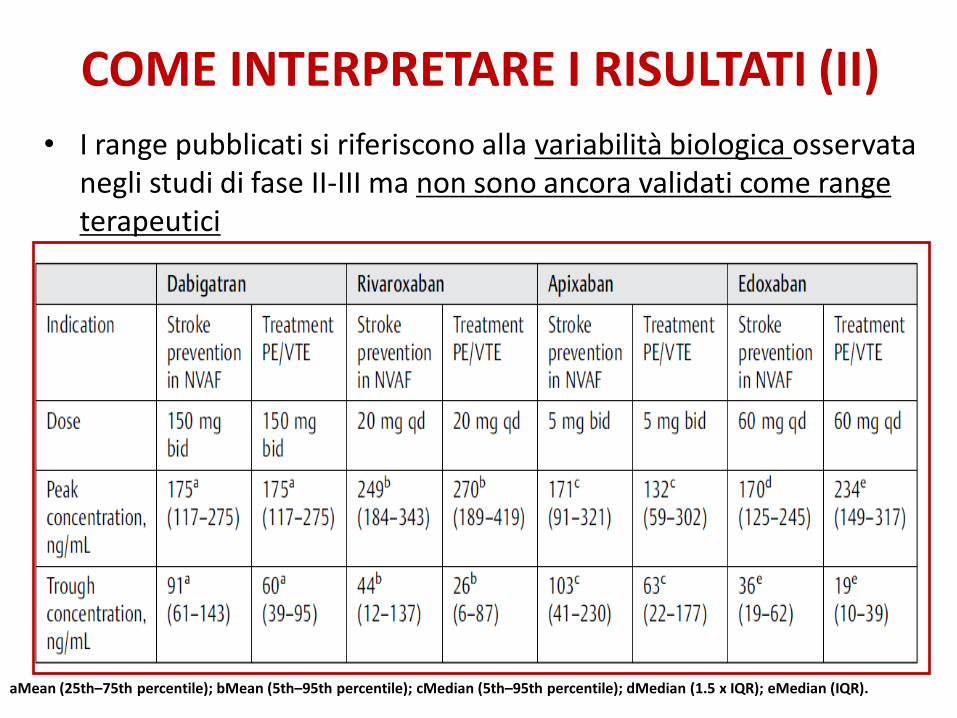
COME INTERPRETARE I RISULTATI (II)
• I range pubblicati si riferiscono alla variabilità biologica osservata negli studi di fase II-III ma non sono ancora validati come range terapeutici
aMean (25th–75th percentile); bMean (5th–95th percentile); cMedian (5th–95th percentile); dMedian (1.5 x IQR); eMedian (IQR).

COME INTERPRETARE I RISULTATI (III)
In attesa dei risultati degli studi in corso, pragmaticamente :
1. DOACs Livelli bassi : valori compresi tra il limite inferiore di sensibilità analitica e 50 ng/ml
2. Livelli al di fuori del 10/90 percentile sono rispettivamente espressione di basse o elevate concentrazioni di farmaco.
3. Valori di valle attesi (Derivati dagli studi fase IV 2016, 2019):
Farmaco Mean 10-90% (ng/ml)
Media Negativo (ng/mL)
dabigatran 50-170 80 < 15
apixaban 60-200 110 < 25
edoxaban 0-40 32 < 20
rivaroxaban 0-100 40 < 20

COME INTERPRETARE I RISULTATI (IV)
3. Livelli <50ng/ml consentono di procedere a Chirugia in Urgenza (According to ISTH, a drug concentration>30 ng mL in patients requiring an urgent intervention associated with a high risk of bleeding is likely to be sufficiently high to warrant antidote administration, whereas in patients with serious bleeding, antidote administration should be considered if the drug concentration exceeds 50 ng mL)
4. Livelli < 30 ng/ml sono auspicabili nella Chirugia Elettiva
5. La definizione dei cut-off per la trombolisi per i diversi DOAC non è ancora condivisa (In those requiring thrombolysis, plasma concentrations of 10 (apixaban), 50 (dabigatran) and 100 (rivaroxaban) ng/mL have been proposed as cut-offs)
Douxfils H et al, JTH 2017

CONCLUSIONI

• Il dosaggio dei DOACs è raccomandabile in molte situazioni cliniche • In considerazione dell’elevata variabilità dell’effetto anticoagulante, il dosaggio dei DOACs potrebbe essere auspicabile per ottimizzarne le posologie


Drug Trough (ng/ml)
mean (min-max)
Peak (ng/ml)
media (min-max)
Dabigatran 110 mgx2/die 93 (14-386) 190 (31-651)
Dabigatran 150mgx2/die 91 (16-494) 210 (43-538)
Rivaroxaban 15mg/die 27 (0-88) 208 (77-393)
Rivaroxaban 20mg/die 41 (5-119) 235 (61-449)
Apixaban 2,5mgx2/die 79 (26-248) 192 (55-300)
Apixaban 5 mgx2/die 113 (42-283) 200 (102-416)
Thrombosis Research, 2016

Drug Trough (ng/ml)
mean (min-max)
Peak (ng/ml)
media (min-max)
Edoxaban 60 mg/die 39 (13-114) 294 (136-569)
Edoxaban 30 mg/die 37 (11-147) 184 (10-529)
Thrombosis Research 2019
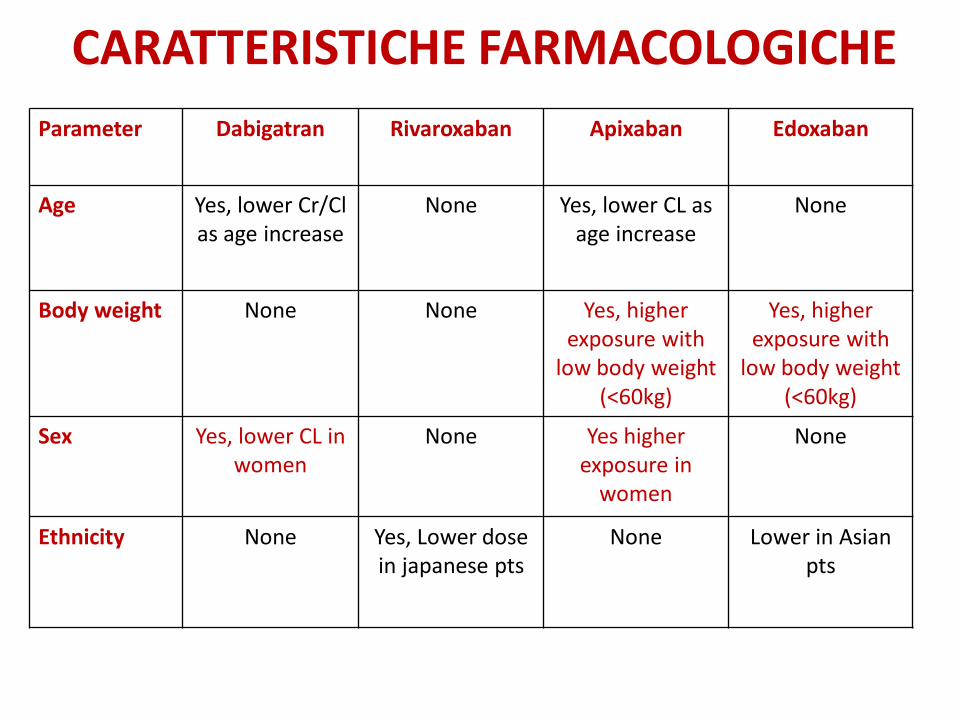
CARATTERISTICHE FARMACOLOGICHE
Gong IY et al 2013
Parameter
Dabigatran
Rivaroxaban
Apixaban
Edoxaban
Age
Yes, lower Cr/Cl as age increase
None
Yes, lower CL as age increase
None
Body weight
None None
Yes, higher exposure with
low body weight (<60kg)
Yes, higher exposure with
low body weight (<60kg)
Sex
Yes, lower CL in women
None
Yes higher exposure in
women
None
Ethnicity
None Yes, Lower dose in japanese pts
None Lower in Asian pts

DOACs AND WEIGHT: PHARMACOKINETIC AND PHARMACODYNAMIC STUDIES
DOAC PK/PD REFERENCES
DABIGATRAN Trough levels <21% for high body weight (>100 Kg) Reilly PA et al, J Am Coll Cardiol 2014
APIXABAN For body weight > 120 kg and BMI > 30: - Mean peak level < 31% - 24% higher volume of distribution and 23% lower drug
exposure - Mean half life 8.8 h ±3.2 vs 12±5.4
Upreti VV et al, Br J Clin Pharmacol 2013
EDOXABAN Body weight affected the non-renal clearence , with non renal decreasing with lower body weight (31-165kg)
Yin OQ et al, Eur J Clin Pharmacol 2014
RIVAROXABAN 1. Healthy volunteers with body weight > 120kg: No differencies for peak level and half life
2. No differencies in peak levels; volume of distribution directly correlated with body weight with a decrease of 0.8% per kg < 56 kg and increased Vd in higher weight pts .
1. Kubitza D et al, J Clin Pharmacol 2007
2. Mueck W et al, Clin Pharmacokinet 2011
Obese patients can show reduced DOAC exposure, but it doesn’t
mean that drug levels are “ a priori” low.

















![DUDAS FRECUENTES: AGENTE DE REVERSIÓN...2. EMA. Ficha técnica de Praxbind 2,5 g/ 50 ml solución inyectable y para perfusión [consultado el 8 de agosto del 2019]. 2015. 3. Eikelboom](https://img.pdfslide.tips/doc/110x75/5f7784ee5df04303935a033c/dudas-frecuentes-agente-de-reversin-2-ema-ficha-tcnica-de-praxbind-25.jpg)