Embed Size (px)
Citation preview
Současný stav poznatků o léčbě MM: co znamenají pro klinickou praxi? (Výstupy z klinických studií vs. klinická praxe)
Roman Hajek Department of Haematooncology, University Hospital Ostrava and Faculty of Medicine, University of Ostrava, Czech Republic
Mikulov 2014
© 2013 Millennium Pharmaceuticals, Inc.
Tato prezentace vznikla za finanční podpory společnosti Janssen-Cilag s.r.o.
Úvod
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
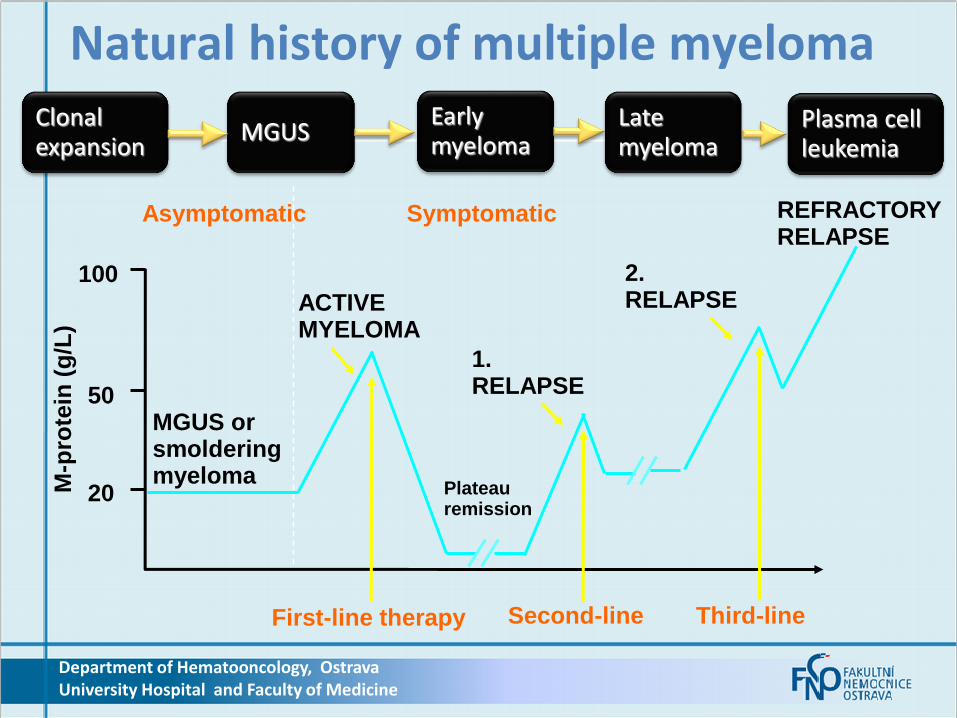
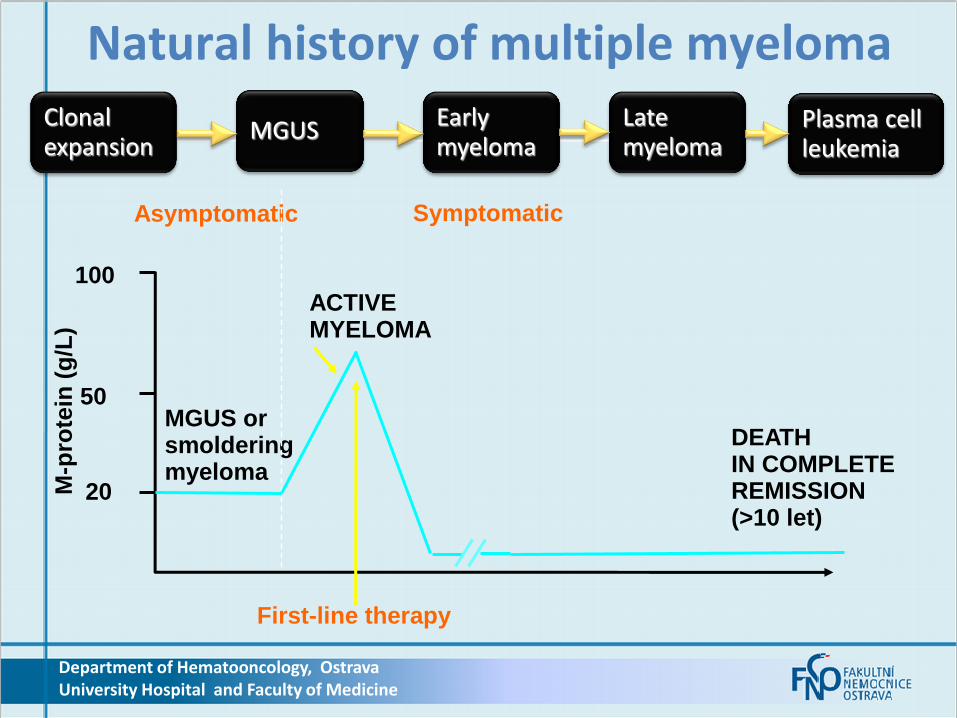
Natural history of multiple myeloma
MGUS or smoldering myeloma
Asymptomatic Symptomatic
ACTIVE MYELOMA
M-p
rote
in (
g/L
)
20
50
100
1. RELAPSE
2. RELAPSE
REFRACTORY RELAPSE
First-line therapy
Plateau remission
Second-line Third-line
Clonal expansion
MGUS Late myeloma
Plasma cell leukemia
Early myeloma
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
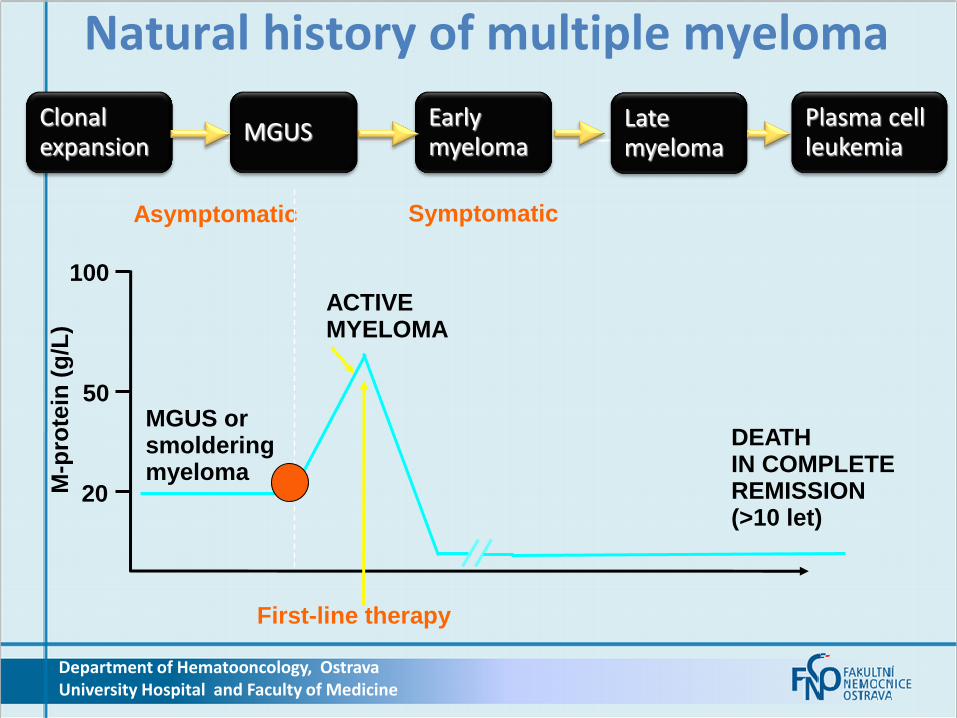
Natural history of multiple myeloma
MGUS or smoldering myeloma
Asymptomatic Symptomatic
ACTIVE MYELOMA
M-p
rote
in (
g/L
)
20
50
100
First-line therapy
Clonal expansion
MGUS Late myeloma
Plasma cell leukemia
Early myeloma
DEATH IN COMPLETE REMISSION (>10 let)
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
Natural history of multiple myeloma
MGUS or smoldering myeloma
Asymptomatic Symptomatic
ACTIVE MYELOMA
M-p
rote
in (
g/L
)
20
50
100
First-line therapy
Clonal expansion
MGUS Late myeloma
Plasma cell leukemia
Early myeloma
DEATH IN COMPLETE REMISSION (>10 let)
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
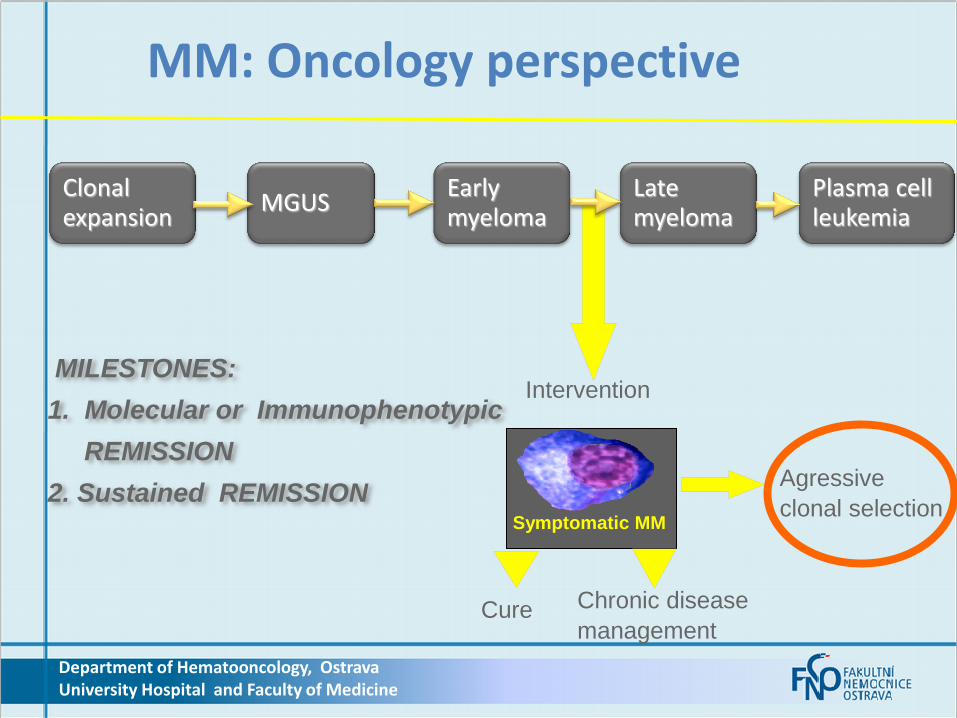
MM: Oncology perspective
Symptomatic MM
Intervention
Clonal expansion
MGUS Late myeloma
Plasma cell leukemia
Early myeloma
MILESTONES:
1. Molecular or Immunophenotypic
REMISSION
2. Sustained REMISSION
Cure Chronic disease
management
Agressive
clonal selection

Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
Personalised medicine
&
„targeted“ treatment?
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
We need novel therapeutic strategies
Personalised medicine
&
„targeted“ treatment?

Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
From diagnosis to treatment
ALL (TWO) novel drugs +
glucocorticoids and alkylating agents
upfront
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
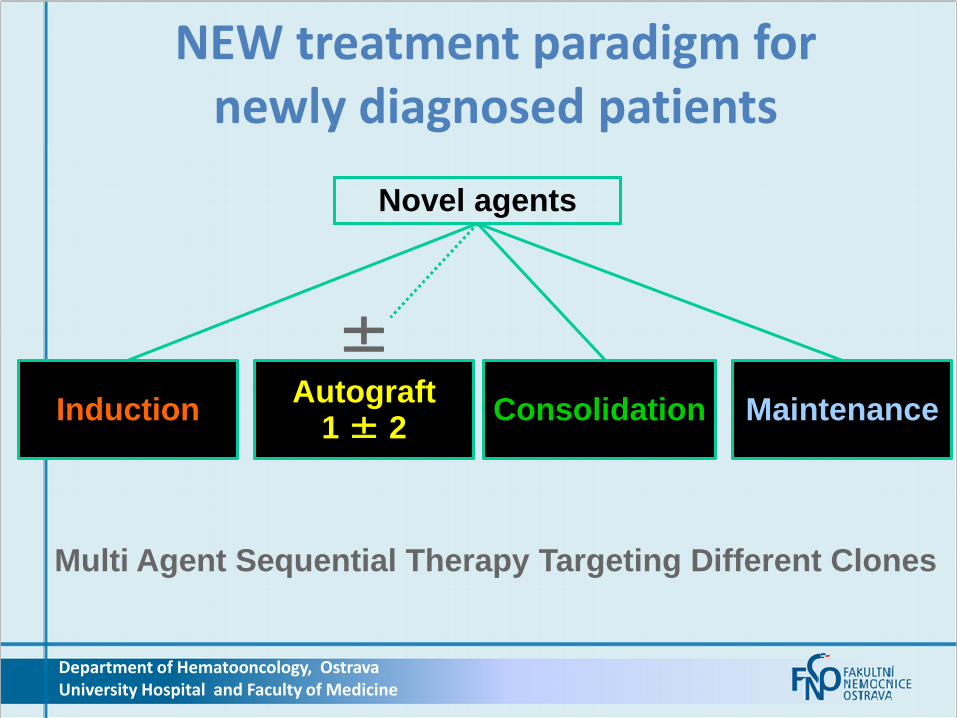
NEW treatment paradigm for newly diagnosed patients
Novel agents
Induction Autograft
1 ± 2 Consolidation Maintenance
±
Multi Agent Sequential Therapy Targeting Different Clones
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
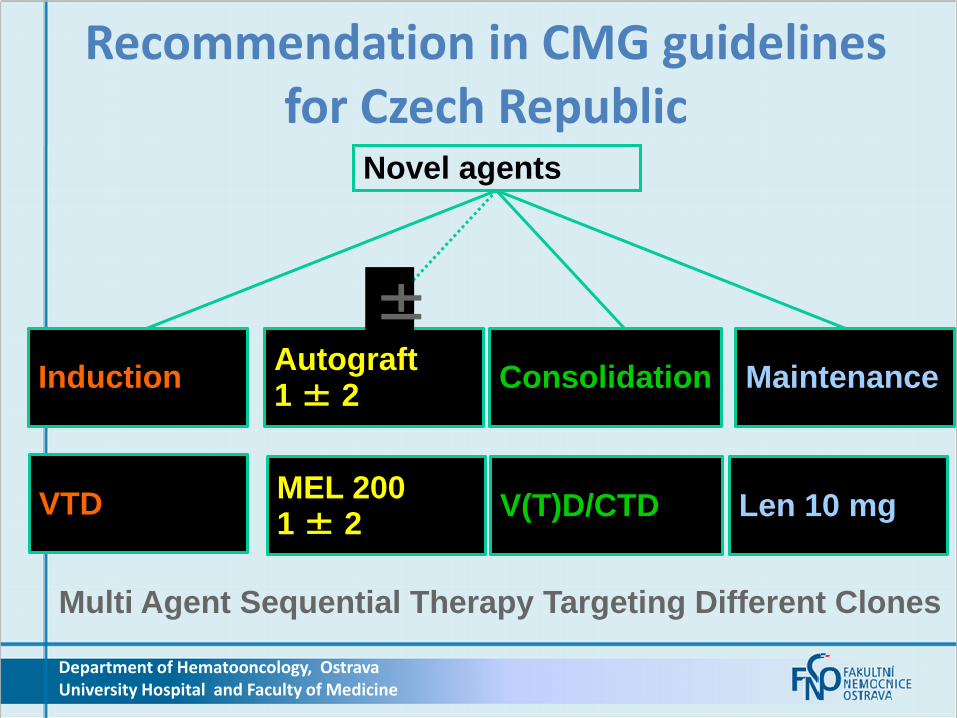
Recommendation in CMG guidelines for Czech Republic
Novel agents
Induction Autograft 1 ± 2
Consolidation Maintenance
±
Multi Agent Sequential Therapy Targeting Different Clones
VTD MEL 200 1 ± 2
V(T)D/CTD Len 10 mg
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
13
Klíčové účinné léky u MM
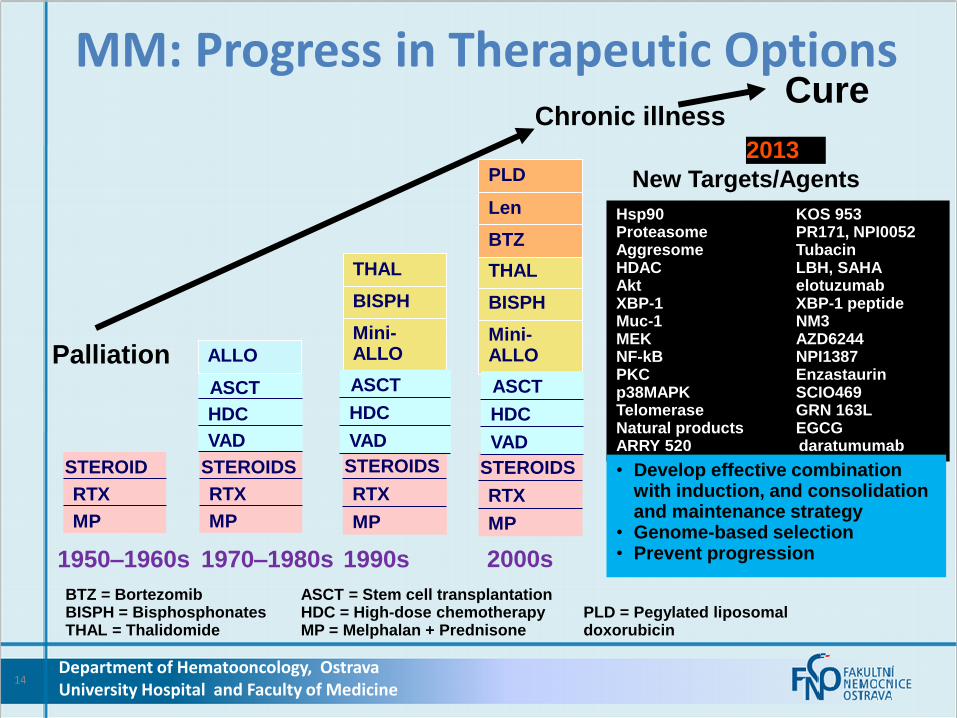
MM: Progress in Therapeutic Options
14
1950–1960s
MP
RTX
STEROID
1970–1980s
MP
RTX
STEROIDS
VAD
HDC
ASCT
1990s 2000s
MP
RTX
STEROIDS
BTZ = Bortezomib ASCT = Stem cell transplantation BISPH = Bisphosphonates HDC = High-dose chemotherapy PLD = Pegylated liposomal THAL = Thalidomide MP = Melphalan + Prednisone doxorubicin
ALLO
Mini-ALLO
BISPH
THAL
MP
RTX
STEROIDS
Mini-ALLO
BISPH
THAL
BTZ
Len
Palliation
Chronic illness Cure
Hsp90 KOS 953 Proteasome PR171, NPI0052 Aggresome Tubacin HDAC LBH, SAHA Akt elotuzumab XBP-1 XBP-1 peptide Muc-1 NM3 MEK AZD6244 NF-kB NPI1387 PKC Enzastaurin p38MAPK SCIO469 Telomerase GRN 163L Natural products EGCG ARRY 520 daratumumab
New Targets/Agents PLD
2013
• Develop effective combination with induction, and consolidation and maintenance strategy
• Genome-based selection • Prevent progression
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
VAD
HDC
ASCT
VAD
HDC
ASCT
15
MM:Progress in Therapeutic Options Key effective drugs
Alkylating agens
Glucocorticoids
IMIDs
Proteasome inhibitors
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
16
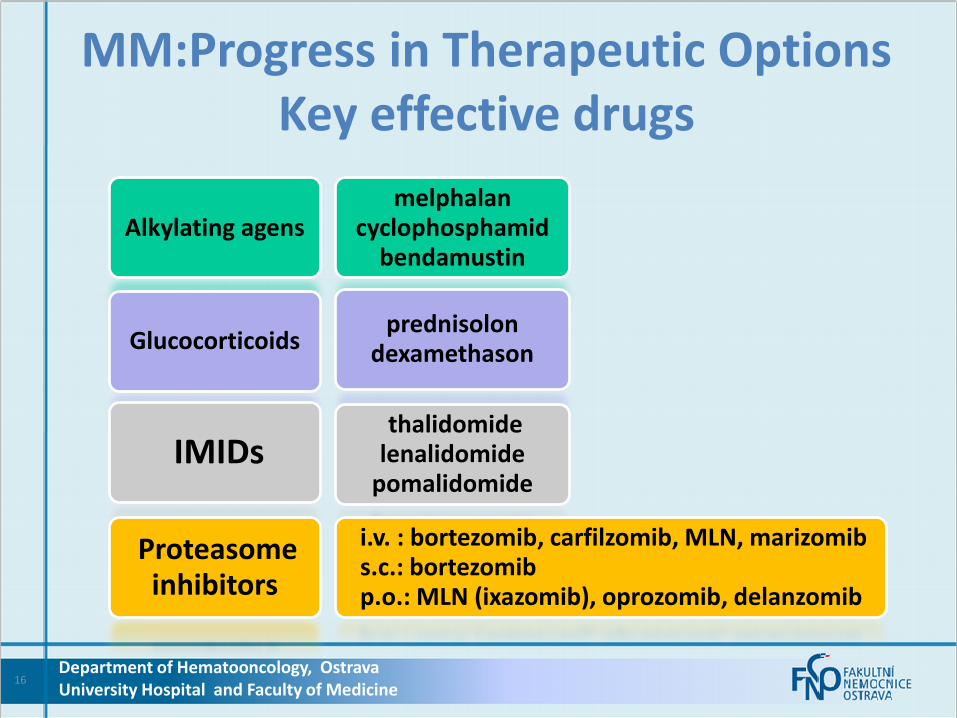
MM:Progress in Therapeutic Options Key effective drugs
Alkylating agens
Glucocorticoids
IMIDs
Proteasome inhibitors
melphalan cyclophosphamid
bendamustin
prednisolon dexamethason
thalidomide lenalidomide
pomalidomide i.v. : bortezomib, carfilzomib, MLN, marizomib s.c.: bortezomib p.o.: MLN (ixazomib), oprozomib, delanzomib
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
17
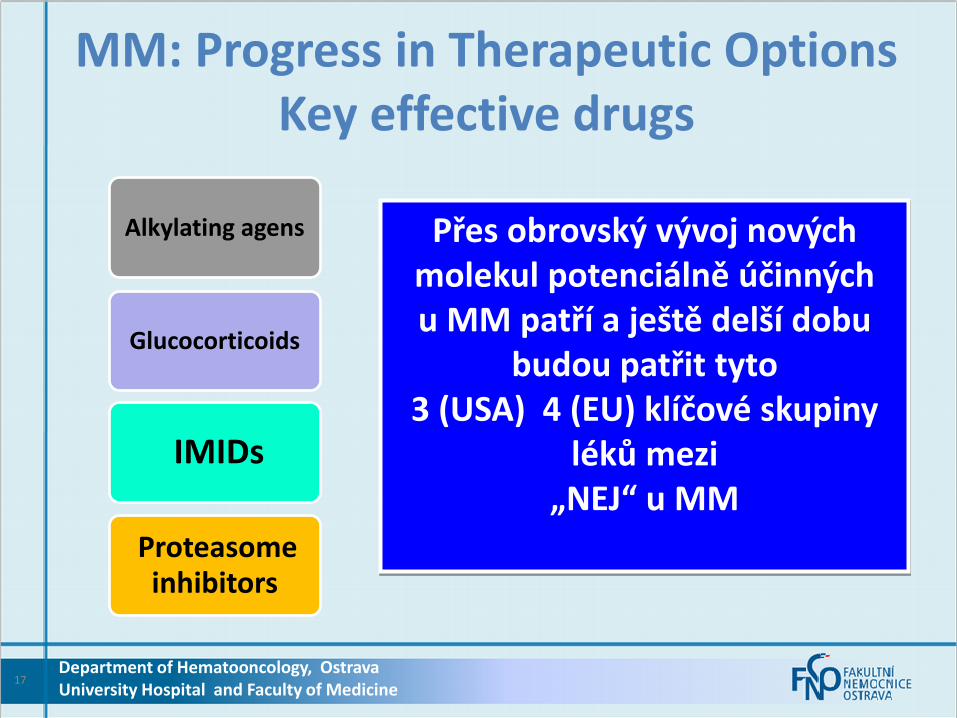
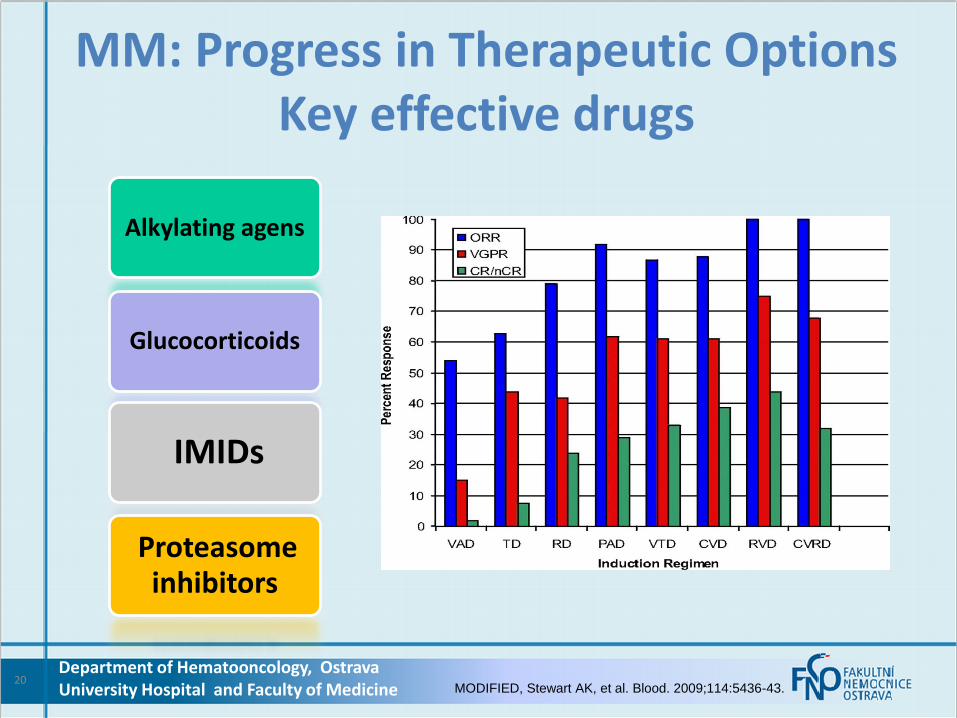
MM: Progress in Therapeutic Options Key effective drugs
Alkylating agens
Glucocorticoids
IMIDs
Proteasome inhibitors
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
Přes obrovský vývoj nových molekul potenciálně účinných u MM patří a ještě delší dobu
budou patřit tyto 3 (USA) 4 (EU) klíčové skupiny
léků mezi „NEJ“ u MM
IMIDs and Proteasome inhibitors
• Multiple mechanisms of action
• Strong anti-myeloma effect
• Non targeted drugs
• No predictors of sensitivity/resistance
1. Kupperman E, et al. Cancer Res 2010; 70(5): 1970-80 2. Chauhan D, et al. Clin Cancer Res 2011;17(16):5311–21 3. Lee EC, et al. Clin Cancer Res 2011; 17(23): 7313-23 4. Chattopadhyay N et al. AACR 2011, Orlando, FL, USA (Abstract 2828)
18 Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
Možnosti stávající léčby
© 2013 Millennium Pharmaceuticals, Inc.
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine 19
20
MM: Progress in Therapeutic Options Key effective drugs
Alkylating agens
Glucocorticoids
IMIDs
Proteasome inhibitors
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine MODIFIED, Stewart AK, et al. Blood. 2009;114:5436-43.
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine MODIFIED, Stewart AK, et al. Blood. 2009;114:5436-43.
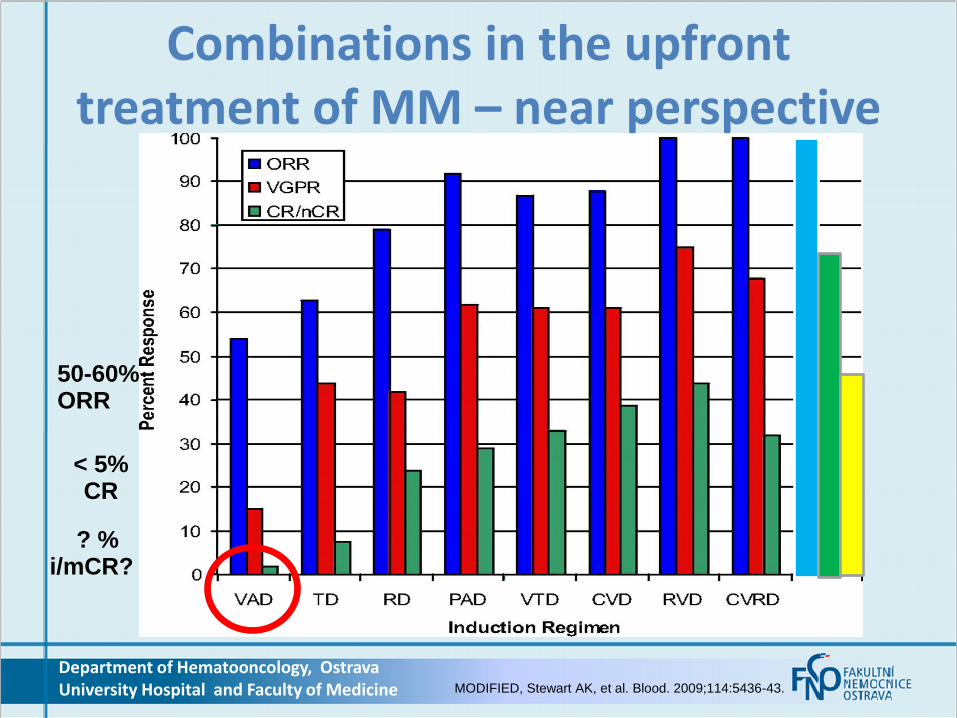
Combinations in the upfront treatment of MM – near perspective
50-60% ORR
< 5% CR
? % i/mCR?

Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine MODIFIED, Stewart AK, et al. Blood. 2009;114:5436-43.
Combinations in the upfront treatment of MM – near perspective
50-60% ORR
< 5% CR
? % i/mCR?
100% ORR
70-80% CR
30-40% i/mCR?
MM
-
Kombinace IMIDs a PIs
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
23

Bortezomib Combinations as Induction Therapy for Elderly NDMM Patients (Phase 3 UPFRONT Trial): Final analysis
N = 502 Transplant-ineligible
NDMM patients
VD (n = 168)* BORT: 1.3 mg/m2, D 1, 4, 8, 11 DEX: 20 mg, D 1, 2, 4, 5, 9, 11, 12; Cycles 1–4; D 1-2, 4-5; Cycles 5–8 8 cycles
VTD (n = 167)* BORT as per VD THAL 100 mg, D 1–21 DEX as per VD 8 cycles
VMP (n = 167) BORT as per VD MEL: 9 mg/m2, D 1–4 every other cycle PRED: 60 mg/m2, D 1–4 every other cycle 8 cycles
Maintenance* BORT: 1.6 mg/m2, D1, 8, 15, 22 5 cycles
VD, bortezomib, dexamethasone; VMP, bortezomib, melphalan, prednisone; VTD, bortezomib, thalidomide, dexamethasone
Niesvizky R, et al. Blood. 2013;122:abstract 1966. Updated data presented at ASH 2013.
• Primary end-point: PFS, secondary end-points: ORR, OS, TTNT
*Jediným aktuálně schváleným režimem s bor v primoléčbě u netransplantabilních pacientů je režim VMP (dle SPC Velcade v01/2014).
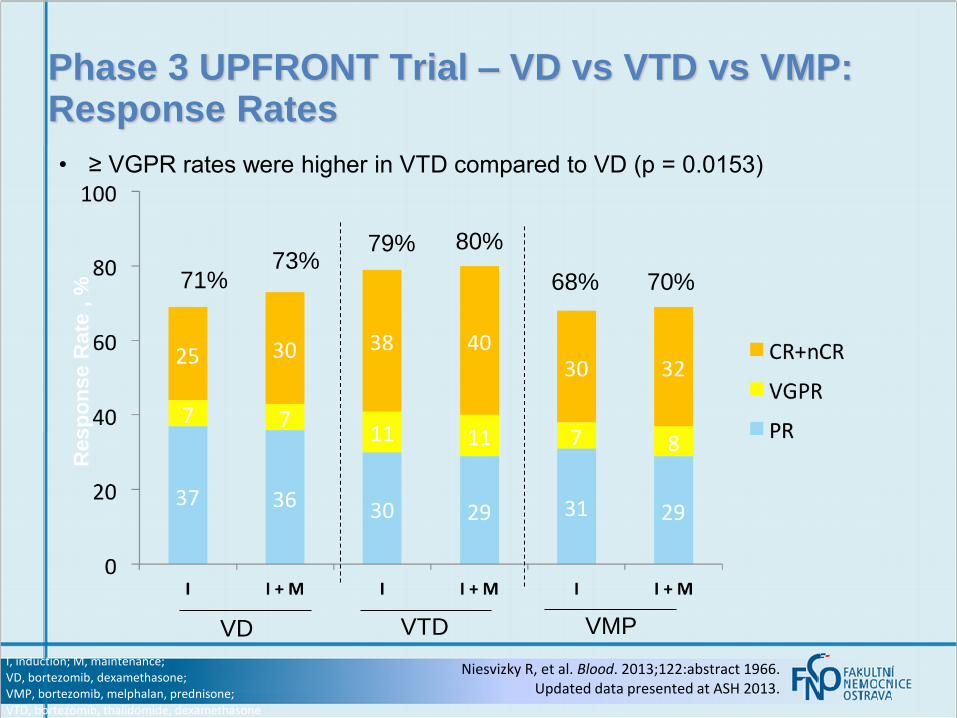
Phase 3 UPFRONT Trial – VD vs VTD vs VMP: Response Rates
Niesvizky R, et al. Blood. 2013;122:abstract 1966. Updated data presented at ASH 2013.
I, induction; M, maintenance; VD, bortezomib, dexamethasone; VMP, bortezomib, melphalan, prednisone; VTD, bortezomib, thalidomide, dexamethasone
• ≥ VGPR rates were higher in VTD compared to VD (p = 0.0153)
Resp
on
se R
ate
, %
71% 73%
79% 80%
68% 70%
VD VTD VMP
Nestačí zvláště u fragilních
a starších nemocných
jen IMID nebo PI
s dexametazonem?
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
26

Continuous Lenalidomide and Low-dose Dexamethasone Demonstrates a Significant PFS and OS Advantage in Transplant Ineligible NDMM Patients – The FIRST Trial: MM-020/IFM 0701
• Thierry Facon, Meletios A. Dimopoulos, Angela Dispenzieri, John V. Catalano, Andrew R. Belch, Cyrille Hulin, Michele Cavo, Antonello Pinto, Katja Weisel, Heinz Ludwig, Nizar J. Bahlis, Anne Banos, Mourad Tiab, Michel Delforge, James D. Cavenagh, Catarina Geraldes, Je-Jung Lee, Christine I. Chen, Albert Oriol, Javier De La Rubia, Lugui Qiu, Darrell J. White, Daniel Binder, Kenneth C. Anderson, Philippe Moreau, Michel Attal, Robert Knight, Guang Chen, Jason Van Oostendorp, Christian J. Jacques, Annette Ervin-Haynes, Lotfi Benboubker
Facon T, et al. Continuous Lenalidomide and Low-dose Dexamethasone Demonstrates a Significant PFS and OS Advantage in Transplant Ineligible NDMM Patients – The FIRST Trial: MM-020/IFM 0701. Plenary presentation at: American Society of Hematology. 2013; December 7-10; New Orleans, LA.
Abstract 2
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
RA
ND
OM
IZA
TIO
N 1
:1:1
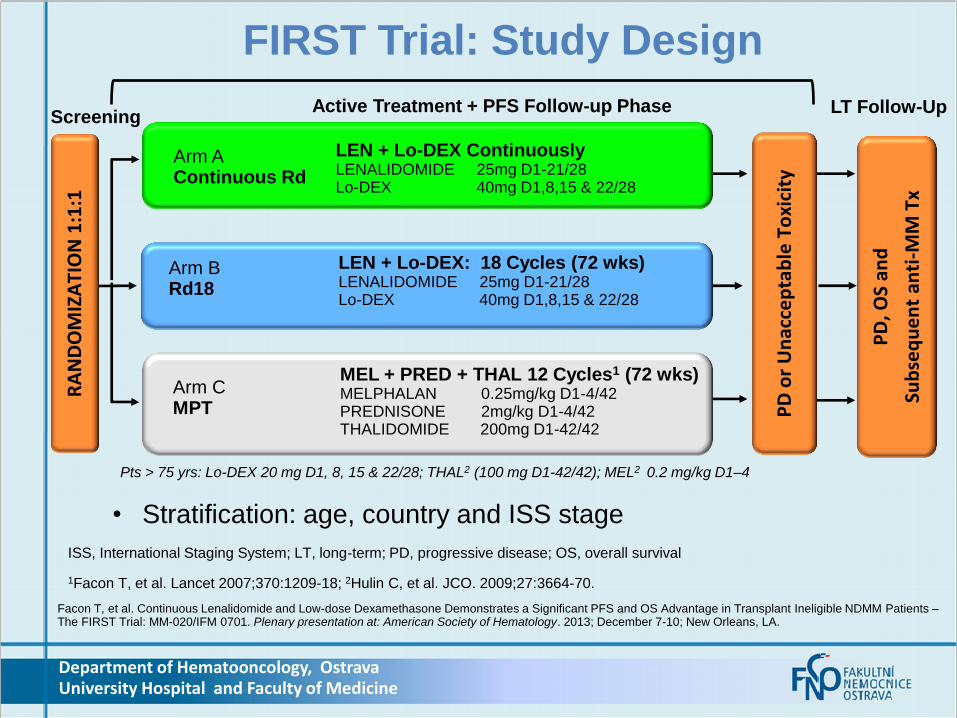
Arm B Rd18
Arm C MPT
LEN + Lo-DEX: 18 Cycles (72 wks) LENALIDOMIDE 25mg D1-21/28 Lo-DEX 40mg D1,8,15 & 22/28
MEL + PRED + THAL 12 Cycles1 (72 wks) MELPHALAN 0.25mg/kg D1-4/42 PREDNISONE 2mg/kg D1-4/42 THALIDOMIDE 200mg D1-42/42
PD
, OS
and
Sub
seq
ue
nt
anti
-MM
Tx
PD
or
Un
acce
pta
ble
To
xici
ty
Active Treatment + PFS Follow-up Phase Screening
LT Follow-Up
Pts > 75 yrs: Lo-DEX 20 mg D1, 8, 15 & 22/28; THAL2 (100 mg D1-42/42); MEL2 0.2 mg/kg D1–4
• Stratification: age, country and ISS stage
1Facon T, et al. Lancet 2007;370:1209-18; 2Hulin C, et al. JCO. 2009;27:3664-70.
FIRST Trial: Study Design
LEN + Lo-DEX Continuously LENALIDOMIDE 25mg D1-21/28 Lo-DEX 40mg D1,8,15 & 22/28
Arm A Continuous Rd
ISS, International Staging System; LT, long-term; PD, progressive disease; OS, overall survival
Facon T, et al. Continuous Lenalidomide and Low-dose Dexamethasone Demonstrates a Significant PFS and OS Advantage in Transplant Ineligible NDMM Patients – The FIRST Trial: MM-020/IFM 0701. Plenary presentation at: American Society of Hematology. 2013; December 7-10; New Orleans, LA.
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
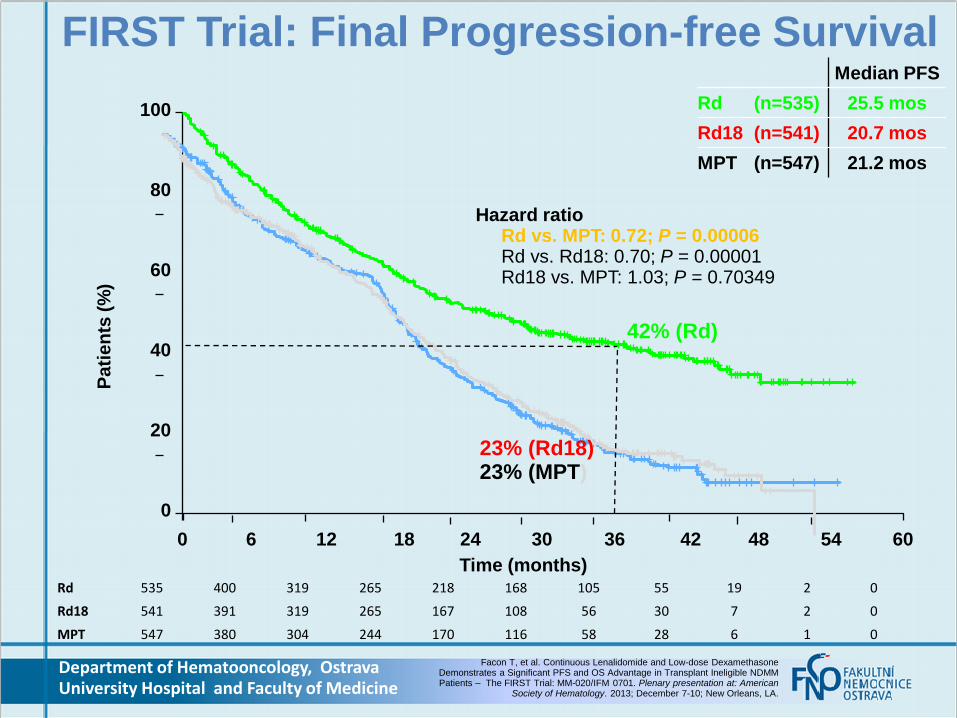
Median PFS
Rd (n=535) 25.5 mos
Rd18 (n=541) 20.7 mos
MPT (n=547) 21.2 mos
Rd 535 400 319 265 218 168 105 55 19 2 0
Rd18 541 391 319 265 167 108 56 30 7 2 0
MPT 547 380 304 244 170 116 58 28 6 1 0
Hazard ratio Rd vs. MPT: 0.72; P = 0.00006 Rd vs. Rd18: 0.70; P = 0.00001 Rd18 vs. MPT: 1.03; P = 0.70349
Time (months)
Pa
tie
nts
(%
) 100
80
60
40
20
0
0 6 12 18 24 30 36 42 48 54 60
42% (Rd)
23% (Rd18) 23% (MPT)
FIRST Trial: Final Progression-free Survival
Facon T, et al. Continuous Lenalidomide and Low-dose Dexamethasone Demonstrates a Significant PFS and OS Advantage in Transplant Ineligible NDMM Patients – The FIRST Trial: MM-020/IFM 0701. Plenary presentation at: American
Society of Hematology. 2013; December 7-10; New Orleans, LA.
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine

Nové přístupy
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
30

Sequential vs Alternating VMP and Rd in NDMM
Mateos MV, et al. Blood. 2013;122:abstract 403. Updated data presented at ASH.
a During the first cycle (6 weeks), bortezomib is given on D1, 4, 8, 11, 22, 25, 29, and 32.
Rd: Len: 25 mg/day, D1–21 Dex: 40 mg, D1, 8, 15, 22 Nine 4-week cycles
MPVRdMPV… for 18 cycles
MPV: Mel: 9 mg/m2, D1–4 Pred: 60 mg/m2, D–4 Bort: 1.3 mg/m2, D1, 8, 15, 22a One 6-week cyclea followed by eight 4-week cycles
Alternating therapy
N = 231 transplant- ineligible NDMM aged > 65 years
RdMPVRd… for 18 cycles
• Randomized phase 2 study to compare the efficacy and safety of two treatment schemes (MPV followed by Rd or MPV alternating with Rd)
• Primary end-points: TTP, safety; secondary end-points: RR, DOR, OS • Subanalysis in patients with high-risk cytogenetics
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine

Sequential vs Alternating VMP and Rd: Response
• Median number of 13 cycles (1-18)
Subanalysis:
• CR rates were similar across different subgroups for both arms, including
– pts aged < vs ≥ 75 yrs
– ISS stage I/II vs III
– cytogenetic abnormalities
Mateos MV, et al. Blood. 2013;122:abstract 403. Updated data presented at ASH.
ORR 89% ORR 94%
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
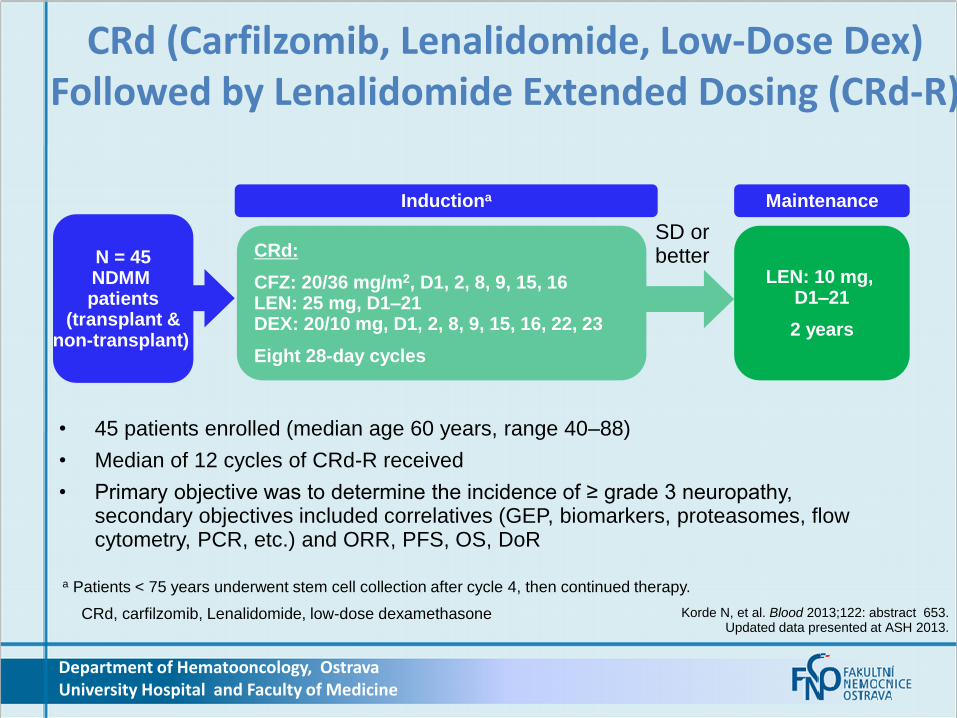
Korde N, et al. Blood 2013;122: abstract 653. Updated data presented at ASH 2013.
CRd (Carfilzomib, Lenalidomide, Low-Dose Dex) Followed by Lenalidomide Extended Dosing (CRd-R)
CRd, carfilzomib, Lenalidomide, low-dose dexamethasone
N = 45 NDMM patients
(transplant & non-transplant)
CRd:
CFZ: 20/36 mg/m2, D1, 2, 8, 9, 15, 16 LEN: 25 mg, D1–21 DEX: 20/10 mg, D1, 2, 8, 9, 15, 16, 22, 23
Eight 28-day cycles
LEN: 10 mg, D1–21
2 years
Inductiona Maintenance
SD or better
a Patients < 75 years underwent stem cell collection after cycle 4, then continued therapy.
• 45 patients enrolled (median age 60 years, range 40–88)
• Median of 12 cycles of CRd-R received
• Primary objective was to determine the incidence of ≥ grade 3 neuropathy, secondary objectives included correlatives (GEP, biomarkers, proteasomes, flow cytometry, PCR, etc.) and ORR, PFS, OS, DoR
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
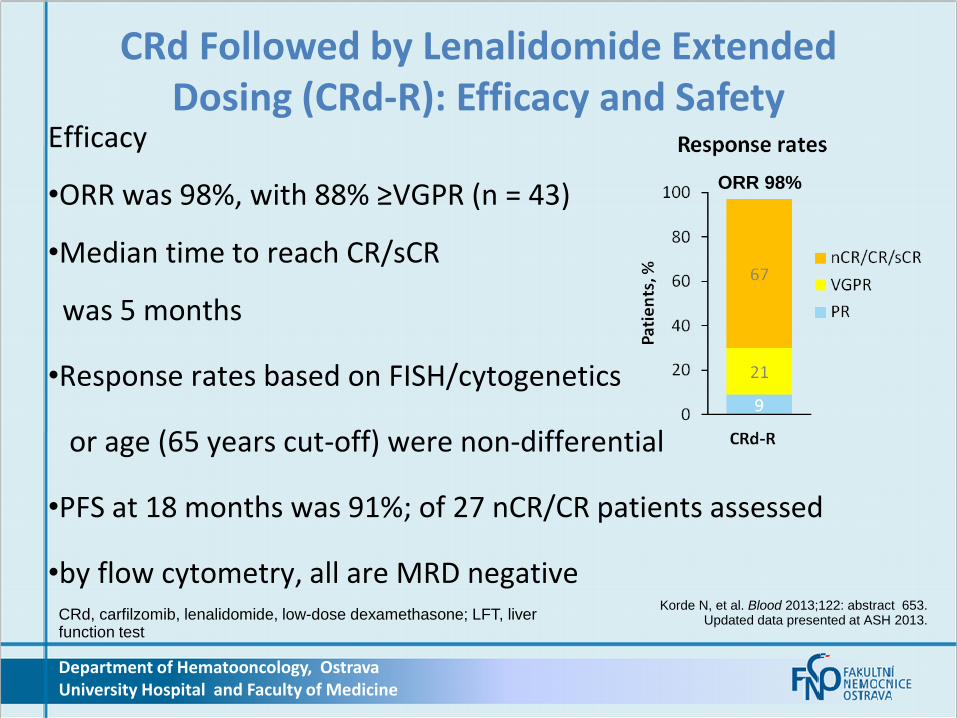
Efficacy
•ORR was 98%, with 88% ≥VGPR (n = 43)
•Median time to reach CR/sCR
was 5 months
•Response rates based on FISH/cytogenetics
or age (65 years cut-off) were non-differential
•PFS at 18 months was 91%; of 27 nCR/CR patients assessed
•by flow cytometry, all are MRD negative
CRd Followed by Lenalidomide Extended Dosing (CRd-R): Efficacy and Safety
ORR 98%
Korde N, et al. Blood 2013;122: abstract 653. Updated data presented at ASH 2013. CRd, carfilzomib, lenalidomide, low-dose dexamethasone; LFT, liver
function test
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
Závěr
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
35

36
MM:Progress in Therapeutic Options Key effective drugs
Alkylating agens
Glucocorticoids
IMIDs
Proteasome inhibitors
melphalan cyclophosphamid
bendamustin
prednisolon dexamethason
thalidomide lenalidomide
pomalidomide i.v. : bortezomib, carfilzomib, MLN, marizomib s.c.: bortezomib p.o.: MLN (ixazomib), oprozomib, delanzomib
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine

37
MM: Future in Therapeutic Option IMIDs and PI combo regimens
100% - ORR; 1/3 of mCR/iCR
Alkylating agens
Glucocorticoids
IMIDs
Proteasome inhibitors
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
38
MM: Futurein Therapeutic Option IMIDs and PI combo regimens for
several treatment lines
Glucocorticoids thalidomid bortezomib
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
VTD
39
MM: Future in Therapeutic Option IMIDs and PI combo regimens for
several treatment lines
Glucocorticoids thalidomid bortezomib
Glucocorticoids lenalidomide carfilzomib
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
VTD
CRD

40
MM: Future in Therapeutic Option IMIDs and PI combo regimens for
several treatment lines
Glucocorticoids thalidomid bortezomib
Glucocorticoids lenalidomide carfilzomib
Glucocorticoids pomalidomide ixazomib
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
VTD
CRD
IPD

41
MM: Future in Therapeutic Option IMIDs and PI combo regimens for
several treatment lines
Glucocorticoids thalidomid bortezomib
Glucocorticoids lenalidomide carfilzomib
Glucocorticoids pomalidomide ixazomib
pomalidomide oprozomib Glucocorticoids
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
VTD
CRD
IPD
OPD
42
Glucocorticoids thalidomid bortezomib
Glucocorticoids lenalidomide carfilzomib
Glucocorticoids pomalidomide ixazomib
pomalidomide oprozomib Glucocorticoids
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
VTD
CRD
IPD
OPD
Combinations of IMIDs and PIs with Glucocorticoids are the most
effective regimens There is not cross resistance thus rotation of different members from IMIDs and PIs is
possible in RRMM
Moreover some of regimens are
fully „per os“ regimen

43
MM: Progress in Therapeutic Options Key effective drugs
Alkylating agens
Glucocorticoids
IMIDs
Proteasome inhibitors
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
Despite many novel agens evaluation in the clinical
trials phase I/II
IMIDs and PIs
remain key players & backbone of myeloma
treatment on NDMM, as well as RRMM for this decade

Babak Myeloma Group Dept. of Pathological Physiology, Faculty of Medicine, MU
Grešliková Henrieta
Kryukov Fedor
Kubiczková Lenka
Kupská Renata
Mikulášová Aneta
Muthu Raja K.R.
Mužíková Jana
Němec Pavel
Perutka Tomáš
Piskacek Martin
Potáčová Anna
Sáblíková Barbora
Smejkalová Jana
Smetana Jan
Ševčíková Sabina
Šváchová Hana
Department of Clinical Hematology
University Hospital Brno
Penka Miroslav
Almáši Martina
Hanáková Božena
Kyjovská Drahomíra
Říhová Lucie
Suská Renata
Štouračová Marcela
Varmužová Tamara
Zarbochová Pavla
Department of Haematooncology
University Hospital Ostrava
Laura Adámková, Cecília Bodzásová,
Juraj Ďuráš, Jaromír Gumulec,
Zdeněk Kořístek, Tomáš Jelínek,
Michal Kaščák, Milan Matuška,
Milan Navrátil, Hana Plonková,
Zahradová Lenka, Jana Zuchnická,
Lenka Martinková , Eva Jarošová,
Eva Jakšíková, Petra Vrublová Laboratory of molecular
cytogenetic, Department of
Experimental Biology, Faculty of Science, MU
Kuglík Petr
Institute of Biostatistics and Analyses
Faculty of Medicine, MU
Jarkovský Jiři Budinská Eva
Ihnatová Ivana
Acknowledgement
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine

Thank you for your attention.
Department of Hematooncology, Ostrava University Hospital and Faculty of Medicine
45
CMGCMGCZ
EC
H
GR
OU
P
M Y E L O M AM Y E L O M A





























