Embed Size (px)
DESCRIPTION
Reproductive Endocrinology Related Diseases 生殖内分泌相关疾病. Zhejiang University School of Medicine, Women ’ s Hospital Wu Ruijin. Reproductive Endocrinology Related Diseases. Dysfunctional Uterine Bleeding 功能失调性子宫出血(功血) Amenorrhea 闭经 Polycystic Ovarian Syndrome ( PCOS ) 多囊卵巢综合征 - PowerPoint PPT Presentation
Citation preview

Reproductive Endocrinology Related Diseases生殖内分泌相关疾病
Zhejiang University School of Medicine,Women’s Hospital
Wu Ruijin

Reproductive Endocrinology Related Diseases
Dysfunctional Uterine Bleeding 功能失调性子宫出血(功血) Amenorrhea 闭经 Polycystic Ovarian Syndrome ( PCOS ) 多囊卵巢综合征
Premenarche Syndrome( 经前期综合征 ) Perimenopause Syndrome( 围绝经期综合征 ) Hyperprolactinemia( 高催乳激素血征 )

Mechanism of Normal Menses
▷ 下丘脑-垂体-卵巢轴(hypothalamic-pituitary-ovarian axis,
HPOA) 调节和反馈正常▷ 卵巢正常(有足够始基卵泡和对 Gn 正常的反应性)▷ 子宫完整,子宫内膜对雌、孕激素有正常反应性▷ 下生殖道通畅


Abnormal Uterine Bleeding (AUB)
Any bleeding that deviated from regular, cyclic (28+/- 7 days) bleeding of normal amount (≤80ml) and duration (2-8 days).
Includes abnormal menstrual bleeding and bleeding due to other causes such as pregnancy, systemic diseases, or cancer.
The diagnosis and management present some of the most difficult problems in gynecology.
In childbearing women, a complication of pregnancy must always be considered, and more than one entity may be present, eg, uterine myomas and cervical cancer.

异常子宫出血(一)
月经过多( menorragia )经量过多( hypermenorrhea )子宫不规则过多出血( menometrorrhagia )子宫不规则出血( metrorrhagia )
周期 经期 经量规则 延长 过多
( > 7 天) ( >80ml )规则 正常 过多
不规则 延长 过多
不规则 可延长 不太多
Menorrhagia: Excessive uterine bleeding at regular intervalsMetrorrhagia: bleeding between regular menstrual periods

异常子宫出血(二)月经频发( polymenorrhea ):周期少于 21 天。月经稀发( oligomenorrhea ):周期长度超过 35 天。月经过少( hypomenorrhea ):月经稀疏,出血少于 2 天。接触性出血( contact bleeding) :性交后出血,排除宫颈癌等。
Polymenorrhea: Irregular bleeding at infrequent intervals

Dysfunctional uterine bleeding (DUB)
功能失调性子宫出血(功血)

Definition
Abnormal bleeding without clear anatomic c
ause.
调节生殖的神经内分泌机制失常引起的异常子宫出血,无全身及内外生殖器质性病变。

PathogenesisPathogenesis
Anovulatory dysfunctional uterine bleeding
( 无排卵性功血 ) ( 85% ) Puberty ( 20% ): unstable HPOA regulation with gro
wing follicle but no LH peak and ovulation does not occur.
Perimenopause ( 50% ): ovary becomes low responsive to Gn and its function declines.
Child bearing period ( 30% ): inside/outside interference, such as psychologic factor, environment, stress,etc.

Anovulatory( 1 ) breakthrough bleeding( 雌激素突破出血 ) : 子宫内膜受单一 E 刺激而无孕酮对抗引起 ;
( 2 ) withdrawal bleeding( 雌激素撤退出血 ) : 子宫内膜在单一 E 的刺激下持续增生,因一批卵泡闭锁 导致 E ,内膜失去 E 支持剥脱出血。
内膜过厚,脆性↑ 内膜修复困难
血管结构功能异常 子宫内膜出血自限性机制缺陷 局部因子异常: PGs
凝血、纤溶异常

Ovulatory menstrual dysfunction
( 排卵性月经失调 ) ( 15% ) Luteal phase defect (LPD) ( 黄体功能不全 )
Abnormal FSH/LH or ratio, low LH peak or following pulse defect.
Irregular shedding of endometrium( 子宫内膜不规则脱落)
HPOA dysfuction and corpus luteum degenerate uncompletely

PathologyAnovulatory Endometrial hyperplasia ( 子宫内膜增生症 ):1994, WHO simple hyperplasia ( 单纯型增生 ) complex hyperplasia ( 复杂型增生 ) atypical hyperplasia ( 不典型增生 ) Proliferative phase endometrium ( 增生期子宫内膜 ) Atrophic hyperplasia ( 萎缩型子宫内膜 )
Ovulatory menstrual dysfunction LPD : P↓→ 分泌期腺体分泌不良 Irregular shedding of endometrium ( 子宫内膜不规则脱
落 ) : P 低量持续→不规则脱落,混合型

Clinical FindingsClinical Findings
Anovulatory Symptoms: Irregular uterus bleeding (metrorrhagia) Characteristic of bleeding:
( 1 ) irregular cycle and duration
( 2 ) not stop by oneself
( 3 ) irregular amount
( 4 ) no menalgia ( 痛经 )
( 5 ) anaemia
“ 三不一无一贫”

Ovulatory menstrual dysfunction Luteal phase defect (LPD) ( 黄体功能不全 ) ( 1 ) shorten cycle, luteal phase <11d, frequently cycle
( 2 ) infertility
( 3 ) repeating spontaneous abortion
( 4 ) D & C : luteal phase endometrium defected and backward 2d to standard phase
Irregular shedding of endometrium( 子宫内膜不规则脱落)( 1 ) prolonged and heavy menses( 2 ) D & C: proliferative and secretary endometrium coexist in cycle d5
( 3 ) BBT high temperature phase prolonged to next menstruation
(4) Serum E2,P and BBT,D&G, cervix mucus score help to diagnosis

Diagnosis
History Physical examination and pelvic examination Auxiliary examination
( 1 ) Blood/live/clotting function test
( 2 ) HCG
( 3 ) Endometrial biopsy /Dilatation and Curettage (D&C) : stop bl
eeding and pathologic diagnosis
( 4 ) Ultrasound or Hysteroscopy: exclude intracavity diseases
(( 55 )) Ovulation function examination Ovulation function examination
(( 66 )) OOthers : cervical cytologic examination

Ovulation function examination Ovulation function examination
1. B ultrasound detects follicles and ovulation
2. BBT ( 基础体温测定 )
3. Vagina cells smear
4. Cervical mucus score ( 宫颈粘液评分 )
5. Endometrial biopsy
6. Serum hormone: E2, P
7. Urine and serum LH
8. Laproscope

ultrasound detects follicles and ovulation

2. 基础体温测定
双相体温



Low E2 state High E2 state

Insler 宫颈评分法 -- ―――――――――――――――――- -- --
项目评分 0 1 2 3
粘液量 无 颈管内 颈管口见粘液 溢出宫颈口 拉丝度 无 <4 cm 4~10 cm >10 cm 结晶 无 少量细条状 羊齿状 典型结晶
宫颈口 闭 裂隙 部分开放 开张 ( 瞳孔样 ) -- ―――――――――――――――――――――
宫颈粘液拉丝度


Proliferative EndometriumProliferative Endometrium
(( 增生期子宫内膜增生期子宫内膜 ))
Secretory EndometriumSecretory Endometrium
(( 分泌期子宫内膜分泌期子宫内膜 ))

分泌期内膜-示核下空泡分泌期内膜-示核下空泡


Differential Diagnosis
Pregnancy related diseases Hemorrhagic diseases Genital tract diseases Endocrinal diseases Drugs

Treatment to anovulative DUB General treatment: antiinflammatory, retrieve anaemia ( 纠正贫血 ), enhance
nutrition as the time stop bleeding. Drug treatment : hormonal therapy Principle of treatment: ( 1 ) stop bleeding, ( 2 ) cycl
e regulation, ( 3 ) induce ovulation (or reduce bleeding).
( 1 ) stop bleeding ( 止血 ) :8h 见效、 24-48h 基本止血,超过 96h 考虑诊断更改 ; 合理剂量,渐减量,
持续无出血 20 天 。雌激素:适于无排卵型青春期功血。 常用药物及方法:妊马雌酮、乙烯雌酚、戊酸雌二醇孕激素:体内有一定 E 水平,药物性刮宫,甲羟孕酮、炔诺酮雄激素:增强收缩,单用效差,适于绝经过渡期功血。联合用药:避孕药、三合激素

( 2 ) cycle regulation( 调整周期 ) : 雌、孕序贯法(人工周期):青春期、生育期,低 E2 雌、孕联合法(避孕药):生育期高 E2 、绝经过渡期 后半周期法(孕激素):青春期、绝经过渡期
( 3 ) induce ovulation (促进排卵 ) : to women desire bearing children Clomiphene citrate, CC (氯米芬 ) Human chorionic gonadotropin, HCG ( 绒绒绒绒 ) Human menopausal gonadotropin, HMG (尿促性素 ) Follicle stimulating hormone , FSH ( 卵泡刺激素 ), FSH-HP , r-FS
H Gonadotropin releasing hormone agonist, GnRHa (促性腺激素释
放激素激动剂 )

Operation treatment: Diagnosis Curettage: often used in acute heavy
bleeding or exist high risk of endometrial cancer Endometrial ablation( 子宫内膜切除术): Peri-
menopause heavy bleeding, hormone therapy does not work and no child-bearing request
Hysterectomy( 子宫切除术): medicine therapy does not work and patient choose

Treatment to menstrual dysfunction
Induce follicles development — CC, HMG+ hCG, Ergolactin (溴隐停 )
Promote LH peak — hCG 5000-10000U Increase luteal function — progestogen, 10mg Induce luteal resolve —progestogen


Amenorrhea
闭 经

Definition
primary amenorrhea (原发性闭经): 5%
No period by age 16 regardless of the presence of normal grow
th and development or the appearance of 2nd sexual characteristi
cs.(≥16岁,第二性征已发育,尚无月经来潮; ) 或
No period by age 14, absence of growth or development of 2nd
sexual characteristics;(≥14岁,无第二性征,无月经来潮 )
secondary amenorrhea (继发性闭经):95% No period for a length equivalent to at least 3 x previous cycles in
tervals or no periods for 6 months. ( 月经停止 6个月,或自身 3个周期以上 )

Classification Classic Hormonal ( 1 ) Gonadotropins (按 FSH 水平分) ▷ 高 FSH 闭经:血清 FSH>30IU/L ,提示卵巢功能衰退 ▷ 低 FSH 闭经: FSH 、 LH<5IU/ ,提示病变在下丘脑或垂体 ( 2 ) Estrogen (按雌激素水平分) ▷ Ⅰ度闭经:子宫内膜已受一定雌激素影响,用孕激素后有撤退性出血(黄
体酮试验) ▷ Ⅱ度闭经:体内雌激素水平低落,子宫内膜菲薄或萎缩,用孕激素后不出现撤退性出血
( 3 ) Prolactin :高泌乳素血症
“4- Compartment” (按解剖部位分 ) Outflow tract——Ovary——Anterior pituitary——Hypothalamus 中枢神经 - 下丘脑-垂体-卵巢-子宫

FSH LH Estradiol Classification Examples
H-P failure Pre-Puberty, Stress, xs.exercise
NL NL NL H-P dysfunction
Anovulation/ PCOS
Ovarian failure
Menopause/
POF
Hormonal Approach

PathogenesisPathogenesis
Primary Amenorrhea (原发性闭经 ) 多由遗传学原因或先天性缺陷引起 体内有一定雌激素水平则第二性征发育正常或接近
正常 体内无雌激素分泌第二性征缺乏

Secondary Amenorrhea 继发性闭经
1.Hypothalamic amenorrhea 下丘脑性闭经 ( 55% ):最常见 , 功能性为主, GnRH 脉冲分泌频率、幅度、量的异常均可致闭经。
①精神应急性( psychogenic stress ) :创伤、紧张、环境改变 ②体重下降、神经性厌食( weight loss , anorexia nervosa )
③长期 过剧运动 : 体脂减少 Leptin 下降 ④药物: 可逆性 利血平、氯丙嗪 下丘脑多巴胺 垂体 PRL 避孕药 抑制下丘脑 GnRH
⑤颅咽管瘤: 瘤体压迫垂体柄,下丘脑 GnRH 和多巴胺运送受抑制⑥Kallmann 综合征(嗅觉缺失综合症) 下丘脑 GnRH先天性分泌缺陷伴有嗅觉丧失或减退 低促性腺激素性性腺功能减退 原发闭经、无性征发育、内生殖器分化正常

2. Pituitary Amenorrhea 垂体性闭经( 20% ):
① hypophyseal tumor( 垂体肿瘤 ): 催乳激素细胞肿瘤 , 致闭经溢乳综合征
②hypophyseal infarct ( 垂体梗死 ) ( Sheehan syndrome):
由于产后出血和休克导致垂体急性梗塞和坏死,使腺垂体丧失正常功能引起一系列腺垂体功能低下的症状,包括 :
产后无乳、脱发、低促性腺激素闭经 , 生殖器官萎缩,以及肾上腺皮质、甲状腺功能减退症状如低血压、畏寒、嗜睡等。
③empty sella syndrome( 空蝶鞍综合征 ) :蝶鞍隔破坏,蛛网膜下腔向蝶鞍延伸,蝶鞍充满脑脊液

3. Ovarian amenorrhea 卵巢性闭经( 20% ) XO syndrome or absence (先天性性腺发育不全或缺如 ) : Turn
er’s syndrome
premature ovarian failure , POF( 卵巢早衰 )
Ovaries histoclasia or resection ( 卵巢组织破坏或切除 )
Ovaries functional tumor ( 卵巢功能性肿瘤 )
polycystic ovary syndrome, PCOS( 多囊卵巢综合征 )

性腺先天性发育不全 占原发性闭经 35%性腺发育不全 、卵泡缺如、性征幼稚、雌激素水平低下, 属高促性腺激素闭经,75%染色体异常, 25%染色体正常 ①染色体异常最常见 Turner’s syndrome X染色单体 45,XO :性腺发育不全、第二性征发育不良;特殊体型:身材矮小( <150CM),盾胸、蹼颈、后发际低 ;继发性闭经见于嵌合体 45, XO/46XX ,或X短臂、长臂缺失等
②单纯性腺发育不全(染色体正常)46 , XX 条索状性腺46 , XY 条索状性腺( Swyer 综合征)

对抗性卵巢综合征 : 卵巢具有始基卵泡和初级卵泡,形态饱满 卵巢对 FSH 不敏感,可能存在 FSH 受体缺陷 卵泡无分泌雌二醇功能,血 FSH升高 女性第二性征接近正常,女性维持性征的雌激素来自
卵巢间质在高 LH 刺激下产生雄烯二酮外周转化

POF:
定义: 在 40岁以前出现的高促性腺激素( FSH≥40IU/L )伴随低性激素水平 (E2≤30pg/ml),临床表现为原发或继发闭经。
发生率: Coulam 检查 1858例POF ,发现 40岁妇女 1/100 发生 POF , 30岁 1/
1000 原发闭经 POF 10%~28% 继发闭经 POF 4%~18%病因:• 卵泡耗竭:卵泡起源数缺乏,卵泡闭锁加速• X染色体异常 • 半乳糖血症• 卵泡功能紊乱:酶缺陷,讯号缺陷• 免疫作用

4.Uterine amenorrhea 子宫性闭经( 5%)Congenital absence of uterus 先天性无子宫或发育不全 (米勒管
发育不全综合征) ▷染色体 46 , xx ,内分泌正常,有排卵,第二性征正常 ▷ 无子宫、无阴道,少部分始基子宫 ▷ 宫内胚胎发育副中肾管中、尾段未发育
子宫内膜损伤:如Asherman syndrome绒绒绒绒绒绒绒绒绒绒绒绒绒绒绒绒绒绒绒绒
5.Congenital hypogenital dysplasia先天性下生殖道发育异常:处女膜闭锁、阴道缺如
6. Pathocrinia 其它内分泌功能异常:甲低、甲亢等

Diagnosis (etiological diagnosis)
History: exclude pregnancy for secondary amenorrhea Physical examination and pelvic examin
ation Auxiliary examination

评估雌激素水平宫颈评分法阴道脱落细胞检查孕激素试验阳性为 I 度闭经
雌激素试验方法:雌孕激素序贯试验有撤退性出血为 II 度闭经重复试验仍无撤退性出血为子宫性闭经

子宫功能测定子宫内膜活检子宫输卵管碘油造影( HSG )宫腔镜药物撤退性试验
卵巢功能测定BBT
B 超监测卵泡激素测定: E2 、 P ( >15.9nmol/l,提示有排卵 ),T;
FSH>40IU/L提示卵巢功能衰竭宫颈评分法阴道脱落细胞检查

绒绒绒绒绒绒▷ 垂体兴奋试验 (GnRH 刺激试验):静脉注射GnRH 刺激垂体,观察血 FSH 和 LH 变化垂体功能正常者刺激后 30 分钟比基值升高 2 - 4倍反应低下或无反应—垂体功能减退反应亢进- PCOS
▷ 激素: PRL<25ug/L 、 FSH 、 LH
▷头颅X片、 CT
其它检查 : 染色体 , 甲状腺 ,肾上腺功能 ,腹腔镜 , 宫腔镜等

闭经的诊断步骤

Treatments
System treatments : diet regulation, psychotherapy Medicine : hormone supplemented or anti-excess 1 ) suppress PRL : Ergolactin 2 ) induce ovulation: CC 、 GnRH 、 GnRHa 、 HMG 3 ) HRT
▷ artificial cycle :用于 II 度闭经患者,目的维持性征,引起月经,防止骨质疏松
▷progestogen :适用于Ⅰ度闭经患者,目的保护子宫内膜 ▷contraceptives : effective to PCOS

Operation : structural disease 1 ) rectify malformation: atresia hymenalis ( 处女膜闭
锁 )
2 ) Asherman syndrome : adhesions isolation
3 ) tumor resection : ovaries functional tumor, pituit
ary tumor
ART

Polycystic Ovary Syndrome (PCOS)
多囊卵巢综合症

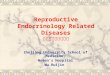
PCOS an outlineDefinition : 以持续性无排卵、高雄激素或胰岛素抵抗为特征的内分泌紊乱的症候群。 妇科内分泌临床常见疾患,占生育年龄妇女 5-10% ,我国的发病率尚缺少
全国性、大样本、多中心研究。 PCOS 临床表现异质性,严重影响生殖功能,且雌激素依赖性肿瘤如子宫
内膜癌发病率增加,相关的代谢失常包括高雄激素血症、胰岛素抵抗、糖代谢异常、脂代谢异常、心血管疾病危险也增加。
病因至今未明,诊断标准不统一,药物治疗方案混乱,对远期并发症缺乏合理防治措施。
Origins of PCOS : 1935 Stein-Leventhal 描述闭经、多毛和双卵巢囊性增大的无排卵相关综合症( S-L 征)。
1990NIH 制定 PCOS 诊断标准 2003 鹿特丹标准 Obesity, fertility and PCOS

Genetic aspects
Intra-uterine Obesity Androgens
Environmental aspects
Single gene Polygenic
Steroid enzymes
Gonadotrophins
Cytokines
Fat hormones
Insulin gene
Insulin receptor
Interactions of many factors
Birthweight Genetic Ovary genes Placental factors Dietary Placental
Imprinting Leptin Aromatisation
Etiological factors of PCOS

Hot topics in aetiology of PCOS
Genetic studies Role of insulin in origins Androgens and prenatal exposure Prenatal growth and PCOS Obesity, inflammation and environmental Disorders of appetite and eating

PCOS – perspective on phenotype
Oligo- amenorrhea Infertility Obesity Hirsutism (多毛) Acne (痤疮) Acanthosis nigricanes
(黑棘皮症 ) Type 2 diabetes Precocious puberty ( 性早熟 ) Other
Endocrinologist Gynaecologist Internist Dermatologist Fertility expert
from Fauser 2004


Ultrasound of ovaries

PCOS – a problem of perspective
Testosterone
LH:FSH ratio
Anovulation
Insulin resistance

PCOS diagnostic criteria - 1990 NIH consensus
Chronic anovulation Hyperandrogenism
(clinical or biochemical)exclusion of other etiologies
Dunaif. PCOS. 1992. Blackwell ScientificFauser 2004
未将 PCO作为诊断的主要症状

Rotterdam consensus on PCOS 2003 ESHRE/ASRM meeting 20 people with expertise on PCOS Discussed diagnostic criteria for PCOS Consensus reached – published 2004

oligoanovulation/anovulation hyperandrogenism
(clinical and/or biochemical) polycystic ovaries
exclusion other aetiologies 2 out of 3 criteria wider criteria for family studies
Fauser 2004
Rotterdam consensus criteria for PCOS


Ultrasound consensus definitions
Balen et al Hum Reprod 9:505, 2003
Technical issues: transvaginal, state of art equipment, well trained staff, D3-5 or following progestin bleed, repeat scan if dominant follicle, calculate ovarian volume, count antral follicles, diameter 3 dimensions
• Either 12 or more follicles 2-9mm or ovarian volume over 10ml
• Subjective assessment follicle distribution should be ignored as well as stroma
• Only one ovary is adequate for diagnosis
• Does not apply to OCP users: PCO does not mean PCOS

What is the relationship between PCO and PCOS?
Since 20-25% of women have PCO, we should not equate PCO with PCOS clinically as yet BUT
PCO women get hyperstimulation like PCOS women Evidence of similar degree of metabolic problems in women
with PCO (no hyperandrogenaemia) (Norman et al 1995) Siblings of PCOS more hyperinsulinaemic (Norman et al
1995) Siblings of PCOS more insulin resistant, hyperandrogenaemic
and more likely to get diabetes mellitus (Legro et al 2002, Yildiz et al 2003)
More likely PCO is part of a spectrum

WHO IIWHO II
WHO II Anovulatory Infertility:Paradigm Shift
Irregular CyclesIrregular Cycles
LHLH
AndrogensAndrogensInsulinInsulin
& & ObesityObesity
PCOPCO
PCOSPCOS
Laven,Ob Gyn Surv 2002
Fauser 2004

Fem
ale
% o
bese
34 23.5 19.3 9.9 7
27.7 21 17.2 9 820
21.7
Mal
e %
obe
seObesity rates worldwide

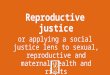
Weight affects fertility and menstrual cycles
0
0.5
1
1.5
2
2.5
3
Infertility Menstrual irregularity
<16
16-18
18-20
20-22
22-24
24-26
26-28
28-30
30-32
>32
Rel
ativ
e R
isk
BMI kg/m2
(referent RR 1.0 for BMI 20-22 kg/m2)
** **
*
***
*
*
(Rich-Edwards et al, Am J Obstet Gynecol 171: 171, 1994)

Obesity and reproduction – bad synergies
• Related to early puberty and menarche
• Central obesity more significant than peripheral obesity
• PCOS can be anticipated to be worse than obesity alone

Obesity and reproduction – bad synergies
Prior to pregnancy Increases length of time to pregnancy, menstrual disorders, miscarriage and may require more drugs
During pregnancy
Increases gestational diabetes, congenital abnormalities, high blood pressure, instrumental and operative delivery
After pregnancy Increases diabetes mellitus, high blood pressure, endometrial cancer, cardiovascular disease, musculoskeletal problems

Treatments
降低 LH 水平 (1) 短效避孕药或 Diane-35 (2)GnRHa
改善 PCOS 的 胰岛素抵抗状态( 1 )降低体重( 2 ) metformin ( 甲福明 ) ,双胍类, 1g-1.5g/d( 3 ) dizoxide ( 二氮嗪 ):300mg/d( 4 ) TZDs 噻唑烷二酮类,格列酮类

降低雄激素水平及其受体活性 促排卵: CC\HMG\HCG 等 代谢紊乱相应处理 手术处理:多点穿刺、楔形切除等