Embed Size (px)
Citation preview

www.MRCPass.com
Respiratory
شكر خاص
رياض السيد رياضالدكتور شكر خاص ألخي وزميلي الفاضل
صاحب الفضل في ھذا الملف
أشرف شيخونكذلك البد أن أشكر أخي الفاضل وزميل العمل الدكتور
خالد يوسف الزھري
مصر –مستشفى سوھاج التعليمي
https://www.facebook.com/elzohryxp
May 2012
www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 2
Respiratory Q001 A man presents with symptoms suggestive of a pneumonia. The CXR confirms this.
Which of the following features suggests poor prognosis?
A. Respiratory rate of 20
B. Temperature 38°C
C. Age 60
D. Urea of 10
E. MTS score of 9 out of 10
Answer: d) urea of 10.
The CURB‐65 score for poor prognosis in pneumonia are :
* confusion (defined as an AMT of 8 or less)
* urea greater than 7 mmol/l
* respiratory rate of 30 breaths per minute or greater
* blood pressure less than 90 systolic or diastolic blood pressure 60 or less
* age 65 or older

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 3
Respiratory Q002
A 60 year old lady presents with shortness of breath. A chest X ray confirms that she has
a right sided pleural effusion. An Aspirate was taken and the sample was sent for several
tests.
Which one of the following is an indication for a chest drain?
A. High protein
B. Low glucose
C. Low LDH
D. PH <7.2
E. Blood stains
Answer: D) pH < 7.2
Although a high protein also points tow ards an exudates, a low pH is the best marker of
infection in an effusion requiring chest drain insertion.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 4
Respiratory Q3
A 75 year old heavy smoker presents to the hospital with breathlessness, wheezing and
a cough with yellow sputum.
He has the following investigations: Hb 18 g/dl, WCC 12 x 10^9/l, ABGs show a pH of
7.38, pO2 of 8.5 kPa, pCO2 of 7 kPa.
What is the diagnosis?
A. Bronchiectasis
B. Chronic obstructive pulmonary disease
C. Mesothelioma
D. Tuberculosis
E. Cryptogenic fibrosing alveolitis
Answer: b) chronic obstructive pulmonary disease.
This patient has type II respiratory failure, without an acidosis, suggesting chronic CO2
retention. He also is a heavy smoker and has polycythaemia, making COPD most likely.
www
Dr. K
Re
A 45
yello
infe
coa
Whi
Ans
The
thic
HRC
w.MRCPass.c
Khalid Yusuf
spiratory
5 year old m
ow sputum
ection. On e
rse crepitat
ich investig
A. Chrom
B. Bronc
C. Sweat
D. Maxil
E. High r
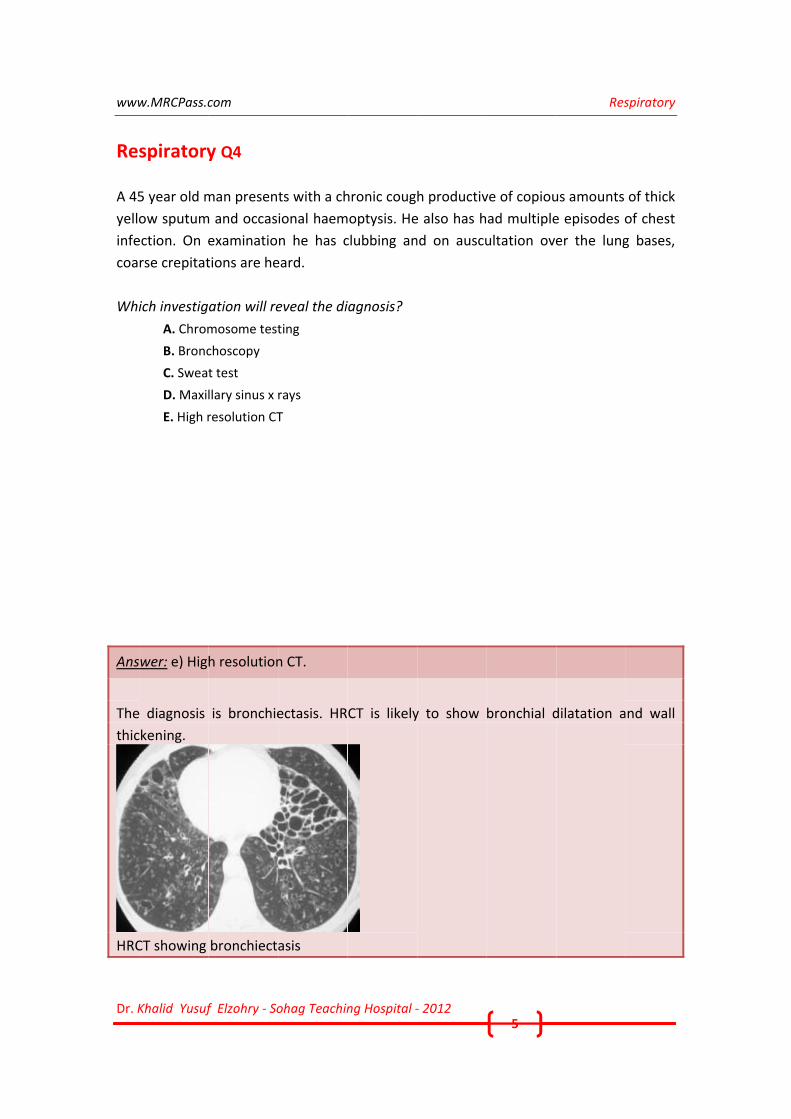
wer: e) Hig
e diagnosis
ckening.
CT showing
com
f Elzohry ‐ So
y Q4
man presen
m and occas
examinatio
tions are he
ation will re
mosome test
choscopy
t test
llary sinus x
resolution CT
h resolution
is bronchie
bronchiect
ohag Teachin
ts with a ch
ional haem
n he has c
eard.
eveal the di
ting
rays
T
n CT.
ectasis. HR
asis
ng Hospital ‐
hronic coug
optysis. He
clubbing an
iagnosis?
CT is likely
‐ 2012
h productiv
e also has h
nd on auscu
y to show
5
ve of copiou
ad multiple
ultation ove
bronchial d
Res
us amounts
e episodes o
er the lung
dilatation a
spiratory
of thick
of chest
g bases,
nd wall

www
Dr. K
Re
A 40
Wha
Ans
The
are
w.MRCPass.c
Khalid Yusuf
spiratory
0 year old m
at is his alp
A. 10%
B. 15%
C. 25%
D. 50%
E. 75%
wer: D) 50%
e normal ge
MS (75%),
com
f Elzohry ‐ So
y Q5
man has em
ha 1 antitry
%.
notype is M
MZ (55%), S
ohag Teachin
mphysema. H
ypsin level li
MM and leve
SS (50%) ZZ
ng Hospital ‐
He is found
ikely to be?
els of enzym
(15%.)
‐ 2012
to have the
?
me is (100%
6
e SS phenot
%). The relev
Res
type.
vant enzym
spiratory
me levels

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 7
Respiratory Q6
A 70 year old man with known chronic obstructive pulmonary disease (COPD) is
admitted with symptoms of worsening breathlessness and confusion. Following a dose
of 200mg iv hydrocortisone and two doses of salbutamol and atrovent nebulisers,
arterial blood gases were taken.
His arterial blood gases are as follows: pH 7.18, PO2 6.6 kPa , PCO2 12.0 kPa.
What should be done next?
A. Repeat dose of corticosteroids
B. Mechanical ventilation
C. 2 litres oxygen
D. Monteleukast
E. Magnesium infusion 2g
Answer: b) Mechanical ventilation.
This patient has type II respiratory failure with acidosis, and hence should be considered
for ventilation, either straight away or with a trial of NIPPV beforehand.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 8
Respiratory Q7
A 40 year old woman has been breathless and is undergoing investigations for the
cause. She has a previous history of being a smoker and has a dry cough as well. Her
ABGs show a pO2 of 9 kPa and pCO2 of 5 kPa. Lung function tests show reduced vital
capacity, reduced TLCO but increased KCO.
What is the likely diagnosis?
A. COPD
B. Bronchial obstruction from a tumour
C. Kyphoscoliosis
D. Obstructive sleep apnoea
E. Fibrosing alveolitis
Answer: c) kyphoscoliosis.
In this scenario, the lung function indicates that the surface area for exchange are
inadequate (low TLCO) hence suggesting that lung expansion is reduced. How ever,
cardiac output is increased to compensate, and henced KCO is increased. Kyphoscoliosis
would restrict lung expansion, or a neuromuscular disorder (eg spina bifida) could cause
this.
www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 9
Respiratory Q8
A 50 year old woman is admitted with infective exacerbation of asthma. She responds to
medical treatment but Aspergillus fumigatus is eventually cultured from her sputum.
Further investigations show serum total IgE level was elevated at 350 ng/ml (normal 40‐
180 ng/ml), RAST to Aspergillus fumigatus was class III, Aspergillus fumigatus precipitins
are negative.
What is the most appropriate management?
A. No change in medication
B. High dose oral corticosteroids
C. CT scan of the chest
D. Chest X ray
E. Itraconazole
Answer: a) No change in medication.
With negative Aspergillus fumigatus precipitins and serum total IgE less than 1000
ng/ml, this patient is unlikely to have Allergic Bronchopulmonary Aspergillosis (ABPA).
Features which are found commonly in asthmatics without ABPA include:
Positive immediate skin reactivity to Aspergillus fumigatus, which is present in 20‐30%
of asthmatics Positive serum precipitins to Aspergillus, which occur in 10% of asthmatics
without ABPA Recurrent mucoid impaction and atelectasis Peripheral blood eosinophilia
and elevation of serum total IgE.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 10
Respiratory Q9
A 60 year old man presents with small amounts of haemoptysis and breathlessness. He
does not have pleuritic chest pains and has normal oxygen saturations.
In considering the potential diagnosis, haemoptysis can occur with which of the
following diagnosis?
A. Pulmonary fibrosis
B. Melanoma
C. Goitre
D. Thymoma
E. Aspergilloma
Answer: e) Aspergilloma.
Haemoptysis can be caused by pulmonary embolus, tuberculous infection, aspergilloma,
bronchial carcinoma, Goodpasture's syndrome and Wegener's granulomatosis.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 11
Respiratory Q10
A 30 year old man gives a six‐month history of worsening breathlessness and coughs up
half a cupful of sputum daily. He was occasionally wheezy with viral illnesses as a young
child, works in a factory and has smoked 25 cigarettes per day for the last four years.
The most likely diagnosis is:
A. Lung carcinoma
B. Bronchiectasis
C. Asthma Asbestosis
D. Chronic obstructive pulmonary disease
E. Rheumatoid lung
Answer: b) Bronchiectasis.
Bronchiectasis is most likely due to the extensive amounts of sputum production. In a
young person, cystic fibrosis and hypogammaglobulinaemia should be considered.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 12
Respiratory Q11
A 60 year old man has smoked for 10 years. He has a longstanding dry cough and
expiratory wheeze.
Examination reveals scattered rhonchi and reduced lung expansion.
The most likely diagnosis is:
A. Asthma
B. Lung carcinoma
C. Chronic bronchitis
D. Bronchiectasis
E. Extrinsic allergic alveolitis
Answer: c) chronic bronchitis.
The heavy smoking history and wheeze suggests chronic bronchitis.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 13
Respiratory Q12
A 14 year old boy develops red eye and rhinitis frequently during the start of the
summer.
What is the likely triggering agent?
A. House dust mite
B. Grass pollen
C. Willow pollen
D. Isocyanates
E. Coal dust
Answer: B) grass pollen.
Grass pollen is released late May till August, and willow pollen is released from March
till June. As the allergic rhinitis is triggered during the start of summer, this is most likely
to be due to grass pollen.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 14
Respiratory Q13
A 65 year old man presents with breathlessness that has got gradually worse over three
months. He has long‐standing atrial fibrillation, for which he takes warfarin and
amiodarone.
On examination his pulse is 100/min in AF, oxygen saturation was 90% on air. His JVP
was not raised and he has fine bibasal crackles. Arterial blood gas saturation showed
mild hypoxia and a pulmonary function test revealed a moderate restrictive picture.
The most likely diagnosis is:
A. Bronchiectasis
B. Pulmonary embolism
C. Pulmonary haemorrhage
D. Amiodarone induced interstitial lung disease
E. Congestive cardiac failure
Answer: d) amiodarone induced interstitial lung disease .
The case scenario would fit amiodarone induced interstitial lung disease or pulmonary
fibrosis. This may take several months or years to develop. Lung function tests may
show a restrictive picture with reduced transfer factor. A high resolution CT in this case
is likely to show diffuse "ground glass" opacities or interlobular septal thickening.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 15
Respiratory Q14
A 65 year old man has been confirmed to have lung cancer.
Which form of cancer has the worst prognosis?
A. Small cell
B. Squamous cell
C. Adenocarcinoma
D. Large cell
E. Prostate metastasis
Answer: a) small cell.
Small cell lung cancer has the worst prognosis out of all lung cancers and is rarely
suitable for surgical resection. Even when diagnosed early the 2‐year survival is in the
order of 20‐25%. The main form of therapy is chemotherapy.
Small cell cancer is associated with syndrome of inappropriate antidiuretic hormone
(ADH) and squamous cell cancer is associated with paraneoplastic hypercalcaemia
through increased parathyroid‐related hormone. 75% of small cell cancers arise in the
proximal airways.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 16
Respiratory Q15
A 22 year old female presents with a chest infection. She is unable to complete a
sentence and her peak flow rate was 40% of her normal level. She is treated with high
flow oxygen, nebulised bronchodilators and oral steroids but this is associated with little
change in her condition.
Which of the following treatments, given intravenously, would be the most appropriate
for this patient?
A. Aminophylline
B. Augmentin
C. Hydrocortisone
D. Magnesium
E. Salbutamol
Answer: D) Magnesium.
IV magnesium is recommended by the British Thoracic Society in severe exacerbation of
asthma. A dose of 2g (8 mmol) is given as a bolus iv dose in the acute presentation
period.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 17
Respiratory Q16
A 60 year man has been a smoker of 20 a day for 30 years. He has a cough and difficulty
in breathing for 3 days which has worsened and he presents to hospital. He has home
nebulisers but not home oxygen.
On examination, his oxygen saturations are 95%, blood pressure 110 / 60 mmHg and
respiratory rate 32. He has diffuse wheezes and is using his respiratory muscles. Arterial
blood gases done on 6 litres of oxygen show :
pH 7.25
P02 16 kPa
PCO2 8.2 kPa
What should be the next management step?
A. Non invasive ventilation
B. Intravenous antibiotics
C. Intubation and ventilation
D. Reduce inspired oxygen concentration
E. Increase oxygen concentration
Answer: d) reduce inspired oxygen concentration.
This man with Chronic Obstructive Pulmonary Disease (COPD) has blood gases showing
type II respiratory failure with acidosis. He has been placed on 6 litres of oxygen, which
is too much for a patient with severe COPD as the history of home nebuliser use
suggests.
His respiratory drive is suppressed by too much oxygen inspired, and hence reduction to
a lower concentration (e.g. 1 ‐ 2 litres) to maintain a pO2 above 8.5 kPa is
recommended.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 18
Respiratory Q17
A 70 year woman has a history of dry cough for 2 months. She has lost 5 kg of weight
over the 2 months. Her chest X ray shows a left apical shadowing. Blood tests reveal a
raised white cell count of 16. She has not managed to cough up any sputum.
Which test should be performed?
A. CT scan of the chest
B. Serum ANCA
C. Ultrasound of the chest
D. Kveim test
E. Bronchoscopy
Answer: e) bronchoscopy.
This patient is likely to have TB due to the apical shadowing. In a patient who is unable
to expectorate sputum, bronchoscopy with lavage (send for AFB) should be performed
to confirm the diagnosis.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 19
Respiratory Q18
A 65 year old man with emphysema presented with increasing dyspnoea and left‐sided
pleuritic chest pain. A chest radiograph reveals a left‐sided pneumothorax with a lung
edge measured 5 cm away from the chest wall.
The most appropriate management of his condition is:
A. Review with daily chest radiographs
B. Intercostal tube drainage
C. Refer to a respiratory outpatient clinic
D. CT chest
E. Simple aspiration
Answer: b) Intercostal tube drainage.
The lung edge measurement suggests a greater than 50% pneumothorax. A smaller
pneumothorax may be amenable to aspiration. In the context of chronic underlying
respiratory disease such as chronic obstructive pulmonary disorder and a large
pneumothorax, patients are best managed by pleural drainage.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 20
Respiratory Q19
A 70 year old man attends the hospital with a history of proximal muscle weakness. He
also gives a history of cough of 12 weeks duration and complains of pain of the small
joints of the hands. He has small haemorrhages in the nail folds, but is not clubbed. On
examination of the chest he has bibasal crackles, and a chest radiograph reveals diffuse
reticular infiltrates. Lung function tests confirm a restrictive pattern.
What is the likely cause of his interstitial lung disease?
A. SLE
B. Dermatomyositis
C. Ankylosing spondylitis
D. Cryptogenic fibrosing alveolitis
E. Amiodarone induced fibrosis
Answer: b) Dermatomyositis.
In polymyositis and dermatomyositis patients often develop proximal muscle weakness
and of pain in the small joints of the fingers. They may have ragged cuticles and
haemorrhages at the finger nail folds. Interstitial lung disease can occur. Underlying
malignancy (lungs, ovaries, breasts and stomach) is present in 5% of cases.

www
Dr. K
Re
A 4
desc
feve
sym
Whi
Ans
The
or K
dila
Bro
w.MRCPass.c
Khalid Yusuf
spiratory
40 year old
cribes long
er or night s
mptoms. Che
ich is the m
A. High
B. Exerc
C. Echoc
D. Bronc
E. Serum
wer: a) high
e likely diag
Kartagener'
ted central
nchiectasis‐
com
f Elzohry ‐ So
y Q20
d man is re
standing s
sweats, and
est X ray sho
ost appropr
resolution CT
cise tolerance
cardiography
choscopy an
m precipitins
h resolution
nosis is bro
s syndrome
tubular bro
‐ Airw ay di
ohag Teachin
eferred for
sputum pro
d he does no
ows mild bi
riate investi
T
e test
y
d biopsy
n CT.
onchiectasis
e. HRCT wil
onchi and m
latation on
ng Hospital ‐
investigati
oduction wh
ot smoke. H
ilateral lowe
igation?
s, and a fam
ll help to co
mosaic oliga
the HRCT
‐ 2012
ion of the
hich is strea
How ever th
er zone sha
mily history
onfirm the
emia were
21
cause of c
aked with
here is a fam
dowing.
is suggestiv
diagnosis,
seen.
Res
chronic cou
blood. The
mily history
ve of cystic
if changes
spiratory
ugh. He
re is no
of such
fibrosis
such as

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 22
Respiratory Q21
A 40 year old man has a 3 month history of cough and dyspnoea. He smokes 20 a day.
There is no history of asbestos exposure.
His WBC count is 24 x 10^9/l with 70% neutrophils and 3.0 x 10^9/l (5%) eosinophils. IgE
level is elevated.
He has decreased breath sounds corresponding to parenchymal infiltrates on the CXR.
Which is the best test to confirm the diagnosis?
A. Sputum for Acid Fast Bacilli
B. HIV test
C. Autoimmune screen
D. Aspergillus RAST
E. Stool for ova, cysts, parasites
Answer: d) Aspergillus RAST.
The condition described is Allergic Broncho Pulmonary Aspergillosis, which is
commoner among asthmatics and cystic fibrosis patients. Eosinophilia and high IgE
levels are suggestive of this condition. RAST test for antibodies tow ards Aspergillus
confirms the diagnosis.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 23
Respiratory Q22
A 45 yearold woman is admitted with a 2‐day history of fever, rigors and breathlessness.
She looks extremely unwell and is confused, cyanosed, has a respiratory rate of 24/min
and a systolic blood pressure of 85 mmHg.
There is bronchial breathing at her right base, where a chest radiograph reveals
consolidation.
Which would be the most appropriate antibiotic regimen?
A. Intravenous ceftazidime and intravenous gentamicin
B. Oral erythromycin
C. Intravenous cefotaxime and oral erythromycin
D. Intravenous amoxicillin and oral clarithromycin
E. Oral amoxicillin and oral clarithromycin
Answer: c) Intravenous cefotaxime and oral erythromycin.
Severe pneumonia as defined by the British Thoracic Society guidelines, is diagnosed
when there are two of the following features: confusion, urea >7mmol/l, respiratory
rate >30/min, and hypotension (SBP <90mmHg, DBP <60mmHg).
Appropriate treatment is with intravenous antimicrobials: cefuroxime 1.5g three times
daily or cefotaxime 1g three times daily daily PLUS erythromycin 500 mg four times daily
or clarithromycin 500mg twice daily.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 24
Respiratory Q23
A 72 year old man presents with a history of worsening breathlessness and cough. His
arterial blood gases show the following recordings when taken at room air:
pH 7.25
pO2 6.4kPa
pCO2 8.9 kPa
Bicarbonate 31mmol/L
What is the most likely diagnosis?
A. Acute exacerbation of chronic obstructive pulmonary disease
B. Obstructive sleep apnoea
C. Pulmonary oedema
D. Pulmonary embolus
E. Pulmonary fibrosis
Answer: a) Acute exacerbation of chronic obstructive pulmonary disease.
The blood gas result would be most compatible with a patient with severe COPD and
chronic type 2 respiratory failure with an acute exacerbation (Hypoxia, respiratory
acidodis with raised CO2 and metabolic compensation).

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 25
Respiratory Q24
A 70 year old man presents with a chronic cough. He is a heavy smoker of over 40
cigarettes a day. CXR shows a peripheral right‐sided lesion. A biopsy which was taken
shows squamous cell carcinoma. No regional lymph nodes are involved. Lung function
tests show a FEV1 of less than 1.5 litres.
The recommended treatment is:
A. Chemotherapy
B. Radiotherapy
C. Lobectomy
D. Pneumectomy
E. Lung transplant
Answer: b) Radiotherapy.
Although surgical treatment is possible in non small cell lung carcinoma, a FEV1 of less
than 1.5 litres contraindicates surgery. Hence, radiotherapy is recommended.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 26
Respiratory Q25
A 55 year old gentleman has pickw ickian syndrome. He has poor exercise tolerance of
50 yards and often feels lethargic at work.
Which of the following is the best investigation?
A. Echocardiography to assess cor pulmonale
B. CT scan of the chest
C. Blood gas
D. Sleep study
E. Exercise tolerance test
Answer: d) sleep study.
The diagnosis of obstructive sleep apnoea can be made with a sleep study
(polysomnography). In sleep apnoea, there is gross obesity and airways obstruction,
occasionally leading to type II respiratory failure. During the sleep study, > 10 episodes
of apneic episodes (pauses in breathing) satisfies the criteria for obstructive sleep
apnoea.
www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 27
Respiratory Q26
A 60 year old man smoker of 35 pack years presents with a 6 month history of shortness
of breath. His past medical history includes diabetes and cervical spondylosis.
Spirometry shows FEV1 of 1 litre ‐ 65% predicted
FVC 1.03 litres ‐ 57% predicted
FEV1/FVC ratio of 95.
How would you interpret the spirometry results?
A. Normal
B. Mixed defect
C. Obstructive defect
D. Restrictive defect
E. Suggestive of haemorrhage
Answer: d) Restrictive defect.
Reduced FEV1 and FVC with normal FEV1 ratio is compatible with restrictive defect.
Causes of restrictive lung defect are :
‐ neurogenic or psychogenic causes
‐ abnormalities of the thoracic wall
‐ stiff parenchyma (pulmonary fibrosis)
‐ loss of lung tissue, e.g. pneumonectomy
‐ displacement

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 28
Respiratory Q27
A 65 year old man has worsening breathlessness. He has a past medical history of
arthritis and palpitations. On admission his oxygen saturations were 90% on air.
ABGs show pO2 9 kPa. pCO2 3.5 kPa, pH 7.36.
His chest X ray shows patchy shadowing in both lung peripheries.
Which one of the following drugs is likely to be responsible?
A. Codeine
B. Tramadol
C. Simvastatin
D. Amiodarone
E. Prednisolone
Answer: d) amiodarone.
The hypoxia and X ray changes suggest pulmonary fibrosis. Out of the list of
medications, amiodarone is the most likely candidate. A lung function test with transfer
factor and also high resolution CT will help to confirm the diagnosis of amiodarone
related pulmonary fibrosis.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 29
Respiratory Q28
A 65 year old man has been diagnosed with chronic obstructive pulmonary disease
(COPD). Spirometry confirms severe COPD with a FEV1 of less than 25% predicted. In the
last year he has been admitted to hospital on 6 occasions with COPD exacerbation.
Which one of the following can help to reduce hospital admissions?
A. Tiotropium
B. Monteleukast
C. Oral theophyllines
D. Salmeterol
E. Hydrocortisone
Answer: a) Tiotropium.
Severe COPD is diagnosed if the FEV1 is less or equal to 30% predicted. Studies have
shown that patients treated with long acting anticholinergic (e.g. tiotropium) have few
er exacerbations per year.
www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 30
Respiratory Q29
An 13 year old male has recent onset breathlessness. He has a history of wheezing
particularly during the summer when the pollen count is high.
Which of these tests would help to confirm the diagnosis?
A. Trial of inhaled corticosteroids
B. Trial of anticholinergics
C. Serial peak flow measurements
D. Lung function tests
E. Chest X ray
Answer: c) serial peak flow measurements.
The history of wheezing during pollen exposure suggests asthma. The best diagnostic
test for asthma would be demonstration of variable airways obstruction with serial peak
flow measurements. Asthmatic patients with exacerbation will demonstrate peak flows
lower than their predicted peak flow, and also a morning dip. There is also reversibility if
a bronchodilator (e.g. salbutamol) is administered.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 31
Respiratory Q30
A 27 year old man presents with sudden onset left sided pleuritic chest pain and
breathlessness.
On examination he is distressed, tachypnoeic and has tracheal displacement to the right
together with a hyper‐resonant percussion note on the left side. There were no breath
sounds on the left. Chest x ray shows a < 2 cm left sided pneumothorax.
What is the best management procedure?
A. High dose oxygen
B. Intercostal drainage tube
C. Chemical pleurodesis
D. Aspiration of pneumothorax
E. Repeat chest x ray in 6 hours
Answer: d) aspiration of pneumothorax.
Treatment of a pneumothorax of < 2 cm margin would be initial aspiration.
This is less painful, leads to a shorter duration of admission, reduces the need for
pleurectomy.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 32
Respiratory Q31
A 65 year year old lady presents with weight loss and haemoptysis and is admitted to
hospital. She has been a heavy smoker for 25 years. A Chest X ray shows a mass in the
right upper lobe.
Which is the best test to investigate at present?
A. Sputum cytology
B. CT scan of the lung
C. Transbronchial biopsy
D. Lymph node biopsy
E. Pleural biopsy
Answer: a) sputum cytology.
The mass seen on the CXR is likely to be a malignancy in view of the history of smoking,
haemoptysis and weight loss. The initial test should be sputum cytology, as the
diagnosis can be confirmed most easily. Staging CT scans can then be done to guide
further management after this.
www
Dr. K
Re
A 70
set
Whi
Ans
An
mal
spre
synd
Left
w.MRCPass.c
Khalid Yusuf
spiratory
0 year old
of investiga
ich one of th
A. FEV1
B. Horne
C. Histo
D. Hype
E. Neuro
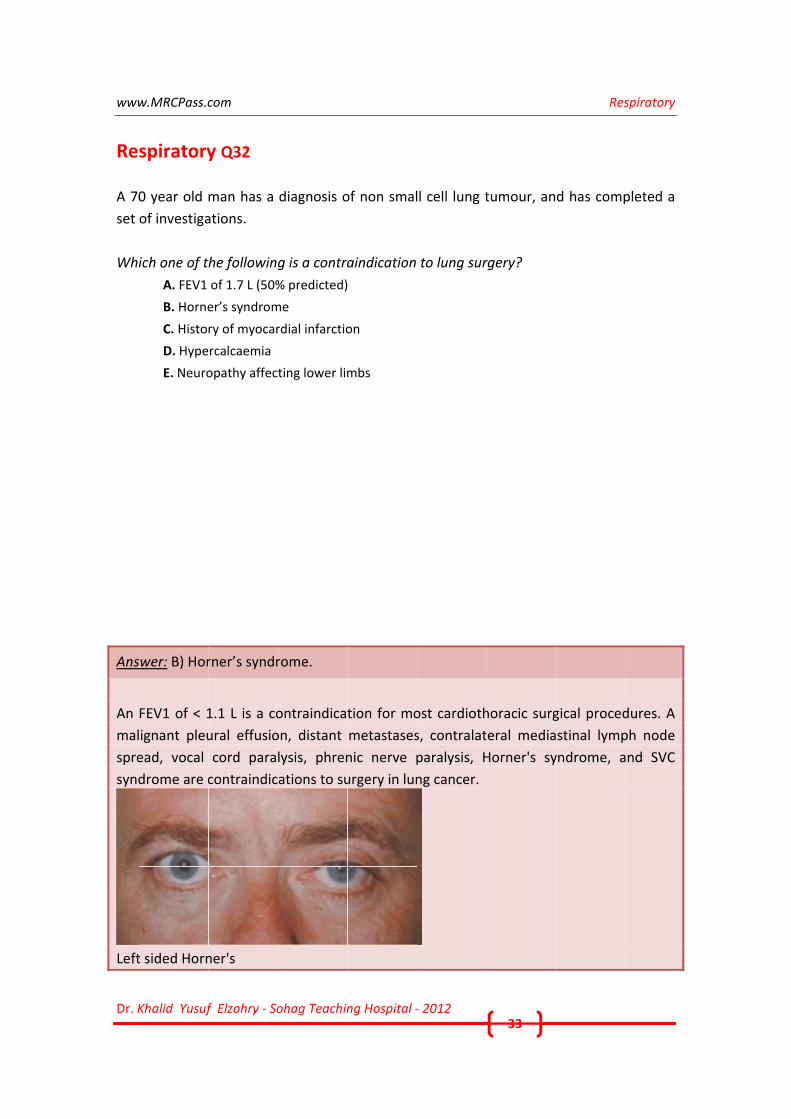
wer: B) Hor
FEV1 of < 1
ignant pleu
ead, vocal
drome are c
t sided Horn
com
f Elzohry ‐ So
y Q32
man has a
ations.
he following
of 1.7 L (50%
er’s syndrom
ry of myocar
rcalcaemia
opathy affect
rner’s syndr
1.1 L is a co
ural effusio
cord para
contraindic
ner's
ohag Teachin
diagnosis o
g is a contra
% predicted)
me
rdial infarctio
ting lower lim
rome.
ontraindicat
on, distant
lysis, phren
ations to su
ng Hospital ‐
of non smal
aindication
on
mbs
tion for mo
metastases
nic nerve p
urgery in lun
‐ 2012
l cell lung t
to lung sur
ost cardioth
s, contralat
paralysis, H
ng cancer.
33
tumour, an
rgery?
horacic surg
eral media
Horner's sy
Res
d has comp
gical proced
stinal lymp
yndrome, a
spiratory
pleted a
dures. A
ph node
nd SVC

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 34
Respiratory Q33
A 20 year old male presents with breathlessness and wheezing.
Which of the following is most likely to suggest asthma?
A. Increased serum IgE
B. Wheezing induced by smoking
C. Obstructive picture in the lung function tests
D. Response to prednisolone
E. Diurnal PEFR variation > 20%
Answer: e) diurnal PEFR variation of >20%.
In asthma, diurnal PEFR variability is due to various degrees of bronchial hyperreactivity.
This is the best indicator of likely asthma. A raised IgE indicates atopy but is not
diagnostic of asthma.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 35
Respiratory Q34
A 70 year old patient with COPD presents with cough and breathlessness which has
worsened over 2 months.
On admission, he has the following arterial blood gas results.
pH 7.32, pO2 7 kPa, pCO2 8 kPa, HCO3 34 mmol/l, Base Excess ‐1.
Which one of the following biochemical states fits best?
A. Chronic respiratory acidosis
B. Chronic respiratory alkalosis
C. Chronic metabolic acidosis
D. Chronic metabolic alkalosis
E. Acute metabolic acidosis
Answer: a) chronic respiratory acidosis.
There is a mild respiratory acidosis (pH < 3.5 and pCO2 > 6) and base excess is also not
elevated (in this case only ‐1). There is metabolic compensation, as indicated by a high
bicarbonate ( >30). The patient's history of COPD suggests that he has chronic hypoxia
and chronic CO2 retention, hence causing the picture of chronic respiratory acidosis.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 36
Respiratory Q35
A breathless 35 year old woman has the following lung function tests:
FEV1 1.2 L (65%)
FVC 1.4 L (60%)
FEV1/FVC ratio = 82%predicted
TLC = 65% predicted
RV = 60% predicted
TLCO = 57% predicted
KCO = 105% predicted
What is the most likely diagnosis?
A. COPD
B. Bronchiectasis
C. Cystic fibrosis
D. Scoliosis
E. Pneumonia
Answer: d) Scoliosis.
The lung function tests show a significant restrictive defect. Only kyphoscoliosis or a
pneumonitis may fit this picture but given the normal/high KCO (i.e. after correcting for
alveolar volumes), the most likely answer is kyphoscoliosis as the gas exchange after
correcting for the alveolar volume is high.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 37
Respiratory Q36
A 70 year old man presented with shortness of breath. On examination, he had the signs
of a large right‐sided pleural effusion.
Investigations revealed: Pleural fluid analysis ‐ protein 65 g/L
What is the most likely cause?
A. Congestive cardiac failure
B. Nephrotic syndrome
C. Non specific pericarditis
D. Liver cirrhosis
E. Mesothelioma
Answer: e) Mesothelioma.
It is a case of exudative pleural effusion (protein >30 g/l). Mesothelioma is the most
likely cause in this case. Other causes are: malignancies, infection, autoimmune
conditions.
www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 38
Respiratory Q37
A 75 year old man with COPD is on long‐term oxygen therapy (LTOT). He complains of
persistent leg swelling during a routine review .
His ABG on a supplemental oxygen flow rate of 2 l/min, shows:
pH of 7.35, pCO2 of 5.7kPa, pO2 of 7.8kPa and HCO3 of 28 mmHg
What should be done?
A. CXR
B. Overnight oxygen saturation monitoring
C. Echocardiogram
D. Repeat ABG on air
E. CT scan of the chest
Answer: b) Overnight oxygen saturation monitoring.
The presence of persistent oedema or secondary polycythaemia suggests that the
correction of overnight SaO2 may be inadequate. Nocturnal hypoxaemia may be evident
during an overnight SaO2 monitoring.
www
Dr. K
Re
A 5
exa
of h
A ch
hyp
Wha
Ans
The
crep
retic
che
HRC
opa
w.MRCPass.c
Khalid Yusuf
spiratory
50 year ma
mination he
his lungs.
hest X ray r
oxia with a
at is the bes
A. Lung
B. Trans
C. Serum
D. High
E. Serum
wer: d) high
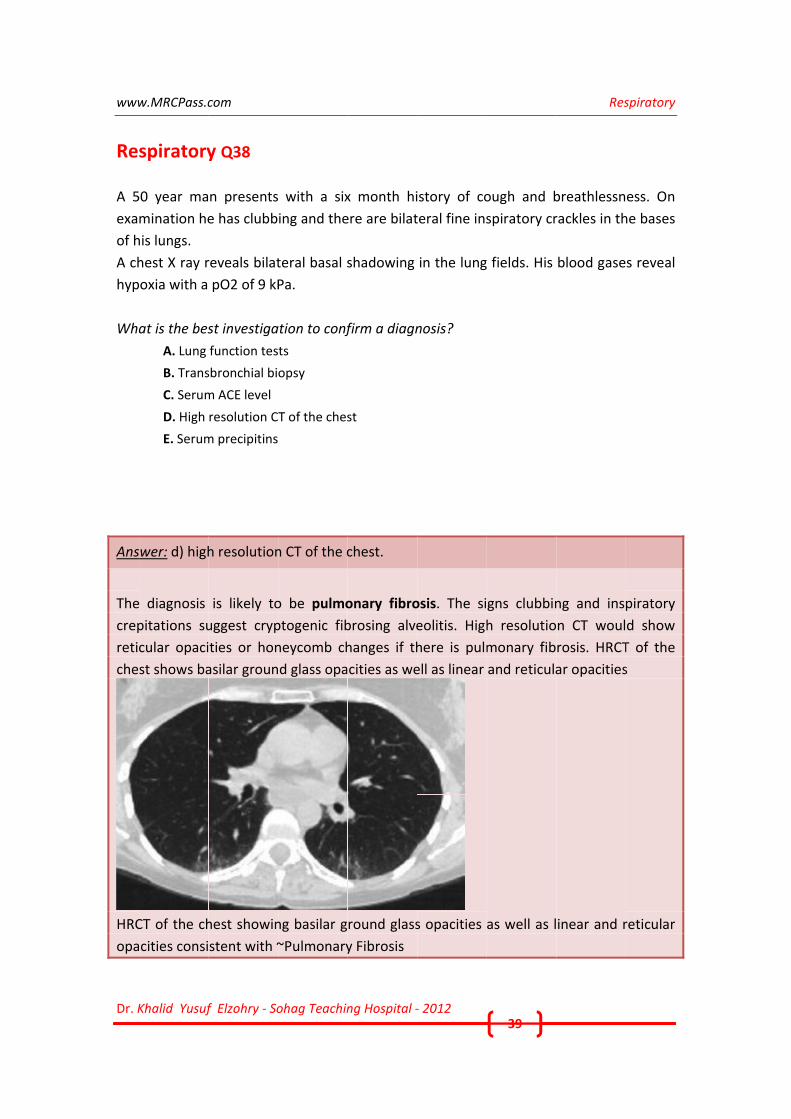
e diagnosis
pitations su
cular opaci
st shows ba
CT of the ch
cities consi
com
f Elzohry ‐ So
y Q38
n presents
e has clubb
reveals bilat
pO2 of 9 kP
st investiga
function tes
sbronchial bi
m ACE level
resolution C
m precipitins
h resolution
is likely to
uggest cryp
ties or hon
asilar groun
hest showin
stent with ~
ohag Teachin
with a six
ing and the
teral basal s
Pa.
ation to conf
ts
opsy
T of the ches
n CT of the c
o be pulmo
ptogenic fib
neycomb ch
d glass opa
ng basilar g
~Pulmonary
ng Hospital ‐
x month hi
ere are bilat
shadowing
firm a diagn
st
chest.
onary fibro
brosing alve
hanges if th
cities as we
round glass
y Fibrosis
‐ 2012
istory of co
teral fine ins
in the lung
nosis?
osis. The si
eolitis. High
here is pulm
ell as linear
s opacities
39
ough and b
spiratory cr
fields. His
gns clubbin
h resolutio
monary fib
and reticula
as well as l
Res
breathlessn
rackles in th
blood gase
ng and ins
n CT woul
rosis. HRCT
ar opacities
inear and r
spiratory
ess. On
he bases
s reveal
piratory
d show
T of the
s
reticular

www
Dr. K
Re
A 40
bee
with
Wha
Ans
Asp
Hae
fung
alle
Asp
w.MRCPass.c
Khalid Yusuf
spiratory
0 year old m
en treated f
hin a cavity
at is the dia
A. Chlam
B. Capla
C. Extrin
D. Asper
E. Legion
wer: d) Asp
pergillomas
emoptysis i
gals or exci
rgic bronch
ergilloma
com
f Elzohry ‐ So
y Q39
man presen
for tubercu
in the right
agnosis?
mydia pneum
an's syndrom
nsic allergic a
rgilloma
nella infectio
pergilloma.
are masse
s a commo
sion surger
opulmonar
ohag Teachin
nted with h
losis. Chest
t upper lobe
monia
me
alveolitis
on
es of funga
on symptom
ry if large. T
ry aspergillo
ng Hospital ‐
history of re
t x ray show
e with an ai
al mycelia
m. They m
They are no
osis).
‐ 2012
ecurrent Ha
wed a roun
r crescent.
that grow
may require
ot associate
40
aemoptysis.
nded soft t
in preexis
treatment
ed with bro
Res
He has pre
issue mass
sting lung c
t with eith
onchiectasis
spiratory
eviously
is seen
cavities.
er anti‐
s (unlike

www
Dr. K
Re
A 5
hem
unit
Dur
seps
inte
pres
Wha
Ans
Res
vasc
con
ARD
w.MRCPass.c
Khalid Yusuf
spiratory
55 year old
morrhage an
t.
ring the foll
sis persistin
erstitial tissu
ssure was 1
at is the dia
A. Conge
B. Pneum
C. Pulmo
D. Adult
E. Comm
wer: d) adu
piratory di
cular perm
dition from
DS
com
f Elzohry ‐ So
y Q40
d man who
nd post‐ope
owing wee
ng over sev
ues and he
13 mmHg.
agnosis?
estive cardia
mocystis pne
onary embol
t respiratory
munity acqui
ult respirato
istress syn
eability (ca
m pulmonary
ohag Teachin
o had two
erative seco
ks this was
veral weeks
became mo
ac failure
eumonia
lism
distress syn
red pneumo
ory distress
drome is
ausing a V/
y oedema. I
ng Hospital ‐
episodes o
ondary hem
followed b
s. Chest x
ore significa
drome
onia
syndrome.
associated
/Q mismatc
t does not
‐ 2012
of hemorrh
morrhage, w
by bronchop
ray showed
antly hypox
with profo
ch). A norm
respond to
41
hagic shock
was admitte
pneumonia
d progressi
ic. Pulmona
ound hypo
mal PCWP
steroids.
Res
k due to in
d to intens
with symp
ive changes
ary capillary
xia and in
differentia
spiratory
ntestinal
ive care
toms of
s in the
y wedge
creased
ates the

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 42
Respiratory Q41
A 40 year old man is HIV positive. He presents with breathlessness to the hospital. Chest
XR shows bilateral interstitial lung markings. His oxygen levels desaturate upon
mobilising.
What should be commenced?
A. Amoxycillin
B. Amoxycillin and clarithromycin
C. Iv co‐trimoxazole
D. Doxycycline
E. Quadruple TB therapy
Answer: c) iv co‐trimoxazole.
The diagnosis is PCP. Silver staining rather than auramine should be done. Mortality is
10%. Iv co‐trimoxazole or pentamidine can be used. Desaturation is typical with exercise
in PCP. Other bacterial infections such as TB are more common among Africans.
www
Dr. K
ReA 2
wor
bud
salb
For
cou
Exa
Res
Inve
Neu
0.44
The
Wha
Ans
ABP
trea
fung
add
Spu
the
CXR
w.MRCPass.c
Khalid Yusuf
spiratory5 year old
rsening of a
desonide m
butamol inh
the past 2
gh and prod
mination a
piratory exa
estigations
utrophils 6
4) x 10^9/l.
e chest X‐ray
at is the like
A. Chron
B. Allerg
C. Pulmo
D. Extrin
E. Meso
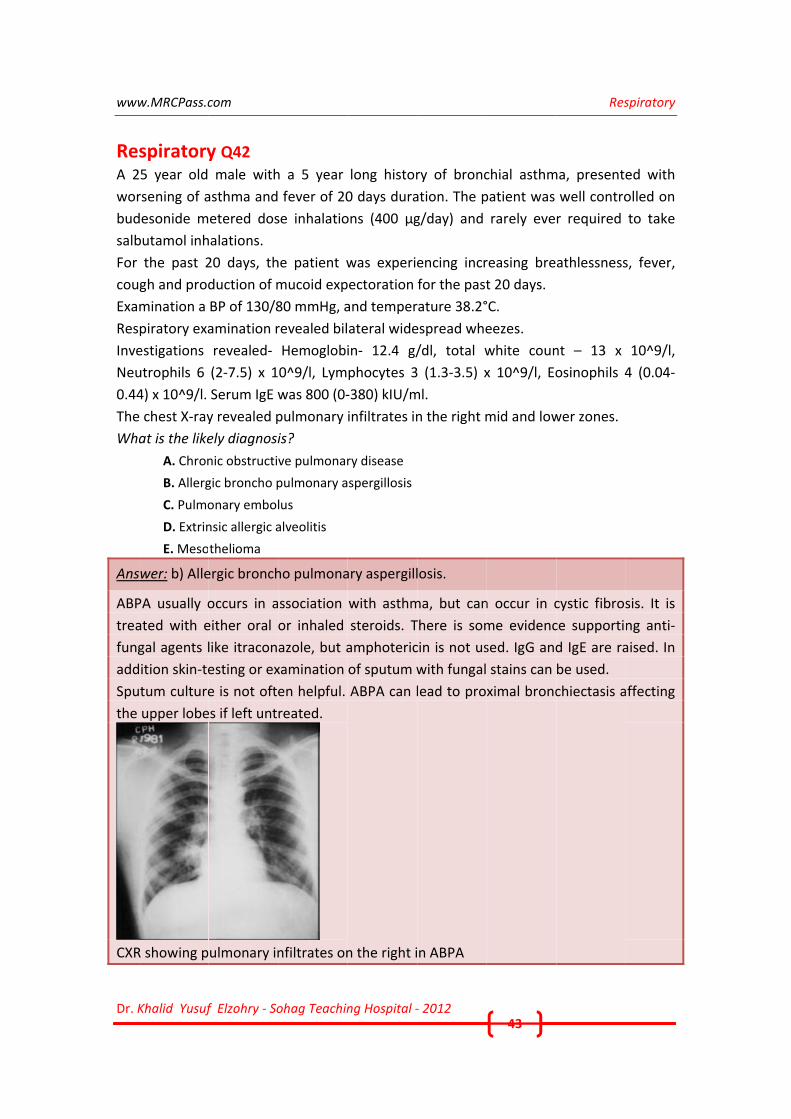
wer: b) Alle
PA usually o
ated with e
gal agents l
ition skin‐te
tum culture
upper lobe
R showing p
com
f Elzohry ‐ So
y Q42 male with
asthma and
etered dos
halations.
20 days, th
duction of m
BP of 130/8
amination r
revealed‐
(2‐7.5) x 1
Serum IgE w
y revealed p
ely diagnosi
nic obstructi
gic broncho p
onary embol
nsic allergic a
thelioma
ergic bronch
occurs in a
either oral
like itracon
esting or ex
e is not ofte
es if left unt
ulmonary in
ohag Teachin
h a 5 year
fever of 20
se inhalatio
he patient w
mucoid exp
80 mmHg, a
revealed bil
Hemoglobi
0^9/l, Lym
was 800 (0‐
pulmonary
is?
ve pulmonar
pulmonary a
lus
alveolitis
ho pulmona
ssociation
or inhaled
azole, but a
xamination
en helpful.
reated.
nfiltrates on
ng Hospital ‐
long histor
0 days dura
ons (400 μg
was experie
ectoration
and temper
ateral wide
in‐ 12.4 g/
phocytes 3
‐380) kIU/m
infiltrates in
ry disease
spergillosis
ary aspergill
with asthm
steroids. T
amphoteric
of sputum w
ABPA can l
n the right i
‐ 2012
ry of bronc
ation. The p
g/day) and
encing incr
for the past
rature 38.2°
espread whe
/dl, total w
3 (1.3‐3.5) x
ml.
n the right m
losis.
ma, but can
There is som
cin is not us
with fungal
lead to pro
n ABPA
43
chial asthm
patient was
rarely eve
reasing bre
t 20 days.
°C.
eezes.
white coun
x 10^9/l, Eo
mid and low
n occur in c
me evidenc
sed. IgG and
stains can
ximal bronc
Res
ma, presente
well contro
r required
athlessness
nt – 13 x
osinophils 4
wer zones.
cystic fibros
ce supporti
d IgE are ra
be used.
chiectasis a
spiratory
ed with
olled on
to take
s, fever,
10^9/l,
4 (0.04‐
sis. It is
ng anti‐
aised. In
affecting

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 44
Respiratory Q43
A 16 year girl with know n cystic fibrosis presents with cough and fevers. Chest X ray
shows right lower zone consolidation.
What antibiotic should be commenced?
A. Amoxycillin
B. Metronidazole
C. Ceftazidime
D. Gentamicin
E. Piperacillin
Answer: C) Ceftazidime
Patients with cystic fibrosis often have pseudomonas as a pathogenic infection.
Ceftazidime and ciprofloxacin would cover the organism, and sometimes gentamicin or
meropenem may be required due to resistance.

www
Dr. K
ReA 50
rash
che
Whi
Ans
Skin
Chu
affe
The
synd
The
Hyp
and
Pulm
w.MRCPass.c
Khalid Yusuf
spiratory0 year old a
h. His routi
st radiograp
ich blood te
A. Total
B. Antin
C. Anti G
D. Asper
E. Anti‐n
wer: b) Ant
n rash and
urg‐Strauss
ects small‐ t
e presence
drome.
ese criteria a
(1) asthma
(2) eosinop
(3) paranas
(4) pulmon
(5) histolog
(6) monone
pergammag
positive AN
monary Infi
com
f Elzohry ‐ So
y Q44 asthmatic tr
ne blood te
ph is norma
est should b
Ig E level
eutrophil cy
GBM antibod
rgillus fumig
nuclear antib
tineutrophil
renal dysf
syndrome,
o medium‐
of 4 or
are:
philia of mo
sal sinusitis
ary infiltrat
gical proof o
euritis mult
lobulinemia
NCA are usu
ltrates in Ch
ohag Teachin
reated with
ests shows
al.
be done nex
toplasmic an
dy
ates precipit
body (ANA)
l cytoplasm
function in
, or allergic
sized arteri
more crite
re than 10%
tes (may be
of vasculitis
iplex or pol
a, increased
ually presen
hurg Straus
ng Hospital ‐
high dose o
mild renal
t?
ntibodies
tins
ic antibodie
an asthma
c granulom
es.
eria indicat
% in periphe
transient)
with extrav
yneuropath
d immunog
nt.
s syndrome
‐ 2012
of inhaled c
dysfunctio
es.
atic suggest
matous angi
tes a high
eral blood
vascular eos
hy.
lobulin E (Ig
e
45
corticostero
n and bloo
ts Churg–
iitis, is a ra
likelihood
sinophils
gE) levels, r
Res
oids develop
od eosinoph
Strauss syn
are syndrom
of Churg‐
rheumatoid
spiratory
ps a skin
hilia. His
ndrome.
me that
‐Strauss
d factor,

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 46
Respiratory Q45
A 70 year old man with chronic obstructive lung disease presents with a cough, fevers
and green sputum.
What is the antibiotic of choice?
A. Teichoplanin
B. Cefotaxime
C. Erythromycin
D. Amoxicillin
E. Ciprofloxacin
Answer: D) amoxicillin.
In COPD, the 3 bacterial species account for most isolates are : Haemophilus influenzae,
Streptococcus pneumoniae and Moraxella cattarhalis. First line treatment should be
with amoxicillin, but if the patient is allergic, a tetracycline should be used.

www
Dr. K
Re
A 60
had
synd
Whi
Ans
Res
mul
narc
failu
ARD
w.MRCPass.c
Khalid Yusuf
spiratory
0 year old p
been in IT
drome.
ich of these
A. CT sca
B. Oesop
C. Pulmo
D. Requ
E. Arteri
wer: c) pulm
piratory di
ltiple blood
cotics. Ches
ure. Hence t
DS
com
f Elzohry ‐ So
y Q46
patient was
TU not long
e would help
an of the che
phageal man
onary capilla
irement for
ial blood gas
monary cap
istress synd
transfusion
st XR would
the best tes
ohag Teachin
involved in
g before th
p to confirm
est
nometry
ary wedge pr
ventilatory s
ses
pillary wedg
drome can
ns, drow ni
d show bila
st would be
ng Hospital ‐
n a car accid
here was a
m the diagno
ressure
support
ge pressure.
n be caused
ng and aspi
teral infiltr
e PCWP, wh
‐ 2012
dent and su
suspicion o
osis?
d by sever
iration, and
ates, and th
ich would b
47
stained mu
of severe r
re trauma,
d drugs such
he presenta
be normal (<
Res
ultiple fractu
respiratory
smoke inh
h as salicyla
ation mimic
<18mmHg)
spiratory
ures. He
distress
halation,
ates and
cs heart
.
www
Dr. K
Re
A 6
lesio
Ans
Squ
bro
Squ
mas
thei
A ca
w.MRCPass.c
Khalid Yusuf
spiratory
8 year old
on. Out of t
A. Meso
B. Small
C. Squam
D. Aden
E. Large
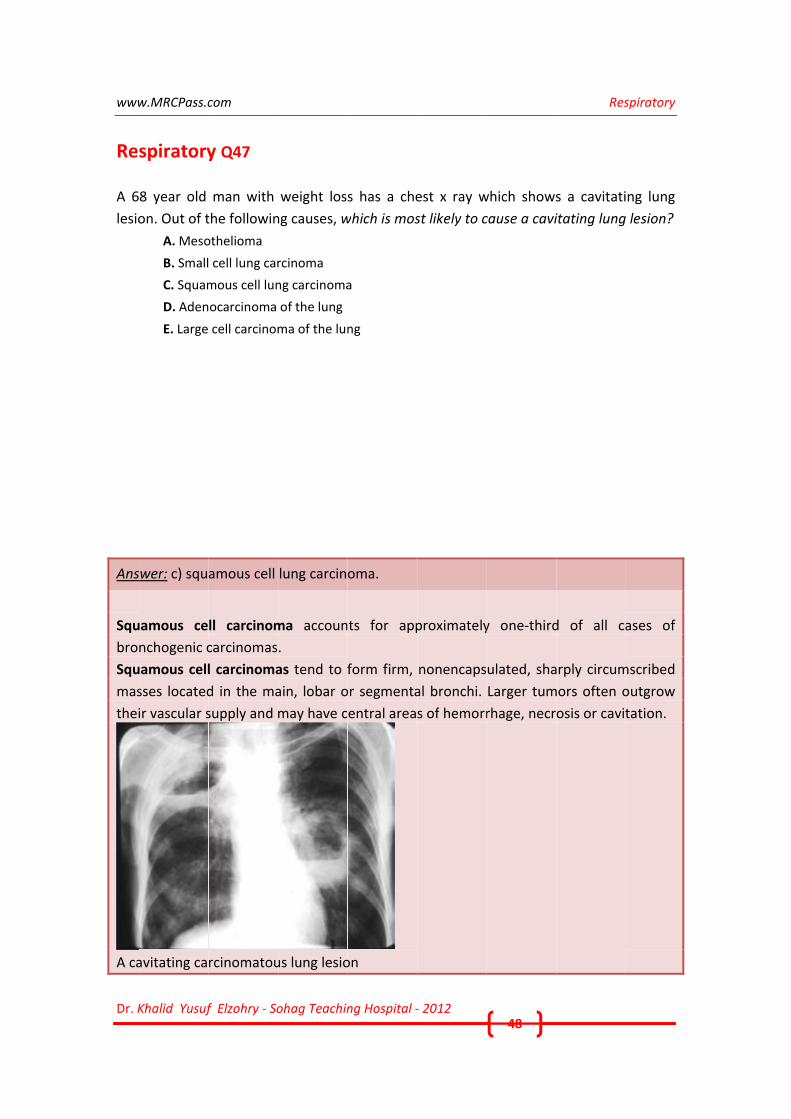
wer: c) squ
uamous ce
nchogenic c
uamous cell
sses located
ir vascular s
avitating ca
com
f Elzohry ‐ So
y Q47
man with
the followin
othelioma
cell lung car
mous cell lun
ocarcinoma
cell carcinom
amous cell
ll carcinom
carcinomas
l carcinoma
d in the ma
supply and m
rcinomatou
ohag Teachin
weight loss
ng causes, w
rcinoma
ng carcinoma
of the lung
ma of the lun
lung carcin
ma accoun
.
as tend to f
ain, lobar o
may have c
us lung lesio
ng Hospital ‐
s has a che
which is mos
a
ng
oma.
ts for app
form firm,
or segmenta
entral area
on
‐ 2012
est x ray w
st likely to c
proximately
nonencaps
al bronchi.
s of hemorr
48
which shows
cause a cavi
y one‐third
ulated, sha
Larger tum
rhage, necr
Res
s a cavitati
itating lung
d of all ca
arply circum
mors often o
osis or cavit
spiratory
ng lung
lesion?
ases of
mscribed
outgrow
tation.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 49
Respiratory Q48
A 45 year man has a long history of productive cough. He had complained of frequent
chest infections.
Examination reveals bilateral inspiratory crackles in the bases of the lungs and clubbing
of the fingers.
Which of following treatments is likely to reduce the frequency of exacerbations?
A. Prophylactic antibiotics
B. Inhaled corticosteroids
C. Oral corticosteroids
D. Postural drainage
E. Lung transplant
Answer: D) postural drainage.
The patient has bronchiectasis, in which the common complication is difficulty
expectorating, postural drainage of secretions is helpful.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 50
Respiratory Q49
A 60 year old man, ex‐smoker (20 pack‐years), was admitted to the hospital because of
a prolonged fever of up to 38.5°C over a period of 10 days, associated with a
progressively worsening shortness of breath, a nonproductive cough, weakness, and
fatigue.
The chest radiograph, showed consolidations at the base of both lungs, prominent
interstitial markings in the middle lung fields, and hazy infiltrates in the right upper lung
field.
A bronchoscopy was done and BAL fluid analysis showed alveolitis with macrophages of
65%, lymphocytes of 25%, and neutrophils of 10%.
Which drug is most likely to be responsible?
A. Sulphasalazine
B. Penicillamine
C. Gold
D. Methotrexate
E. Azathioprine
Answer: d) methotrexate.
The diagnosis is interstitial pneumonitis. Methotrexate is associated with interstitial
pneumonitis. This is rare but a serious complication. Diagnosis is based on the clinical
setting, clinical manifestations, radiographic abnormalities, bronchoalveolar lavage
(BAL), and lung histology.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 51
Respiratory Q50
A 40 year old woman has a history of cough with copious phlegm with intermittent
haemoptysis. She also gets recurrent chest infections and has a long history of joint
pains. She is on non‐steroidal anti‐inflammatory drugs.
Her chest radiograph shows linear radioluciences at both bases. A high‐resolution
computed tomography scan (HRCT) of the chest confirms bronchiectasis.
What is the likely cause?
A. Old tuberculosis
B. Hypogammaglobulinaemia
C. Rheumatoid arthritis
D. Cystic fibrosis
E. Kartagener's syndrome
Answer: c) Rheumatoid arthritis.
The case scenario suggests rheumatoid arthritis. 4 % of patients with rheumatoid
arthritis develop bronchiectasis. Other causes are chronic infection (TB, measles,
whooping cough etc), foreign body aspiration, hypogammaglobulinaemia, Kartagener's
syndrome, Young's syndrome, cystic fibrosis, allergic bronchopulmonary aspergillosis.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 52
Respiratory Q51
A 35 year old lady has a headache, cough and myalgia.
On examination, she has a pyrexia and scattered crackles bilaterally on auscultation of
the chest. Rapid cold agglutinins was positive.
What is the likely diagnosis?
A. Tuberculosis
B. Staphylococcal pneumonia
C. Streptococcal pneumonia
D. Mycoplasma pneumonia
E. Legionella pneumonia
Answer: d) mycoplasma pneumonia.
Mycoplasma pneumonia is the commonest atypical pneumonia.
Approximately 15% of pneumonias in adults are due to Mycoplasma pneumoniae.
Transmission occurs from person to person by infected droplets. The incubation period
is 9‐21 days. The incidence is higher during the winter months. Fever, chills, cough and
headache are early symptoms. Dyspnoea, chest pain and haemoptysis are rare.
Small pleural effusions may occur but are rare. Cold agglutinins are usually present in a
titre greater than 1:32.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 53
Respiratory Q52
A 32 year old man is admitted to hospital with a history of breathlessness of 4‐6 weeks
duration. He initially had flu‐like symptoms and was treated by his doctor with a 5‐day
course of amoxicillin. How ever, he then started coughing up blood, leading to urgent
referral.
On examination he was dyspnoeic at rest, with bilateral crackles on auscultation of the
lungs.
Investigation revealed anaemia and impaired renal function (creatinine 250 micromol/l).
Pulmonary function tests were normal apart from an abnormally high diffusion factor.
Urine dipstick testing showed the presence of red blood cells.
What is the most likely diagnosis?
A. Goodpasture's syndrome
B. Farmer's lung
C. Invasive Aspergillosis
D. Extrinsic allergic alveolitis
E. Chronic eosinophilic pneumonia
Answer: a) Goodpasture's syndrome.
The clinical picture of pulmonary and renal involvement is typical of Goodpasture's
syndrome. The condition is due to the presence of circulating anti‐glomerular basement
membrane antibodies (anti‐GBM antibodies. Other causes of pulmonary haemorrhage
and renal failure include Wegener's granulomatosis, microscopic polyangiitis and
systemic lupus erythematous (SLE).
www
Dr. K
Re
A 40
has
and
bec
The
Wha
Ans
ARD
diffe
shad
ven
w.MRCPass.c
Khalid Yusuf
spiratory
0 year old
a temperat
fever desp
ome much
WCC is 18 x
CRP is 220
PO2 is 6.5k
Pulmonary
e chest X‐ray
at is the like
A. Pulm
B. Pneum
C. Sever
D. Pulm
E. Adult
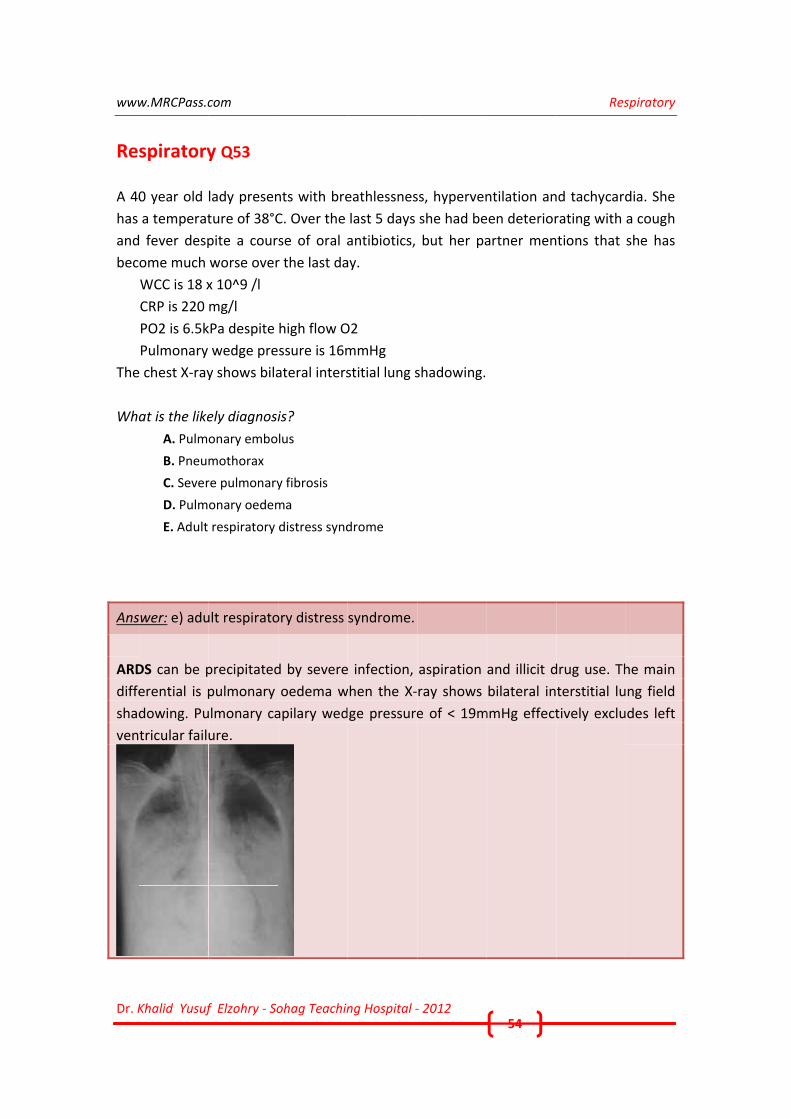
wer: e) adu
DS can be p
erential is p
dowing. Pu
tricular fail
com
f Elzohry ‐ So
y Q53
lady presen
ture of 38°C
pite a cour
worse over
x 10^9 /l
mg/l
kPa despite
wedge pre
y shows bila
ely diagnosi
onary embo
mothorax
re pulmonary
onary oedem
respiratory
ult respirato
precipitated
pulmonary
ulmonary ca
ure.
ohag Teachin
nts with bre
C. Over the
se of oral a
r the last da
high flow O
ssure is 16m
ateral inters
is?
lus
y fibrosis
ma
distress synd
ory distress
d by severe
oedema w
apilary wed
ng Hospital ‐
eathlessnes
last 5 days
antibiotics,
ay.
O2
mmHg
stitial lung s
drome
syndrome.
e infection,
when the X‐
ge pressure
‐ 2012
ss, hyperven
she had be
but her pa
shadowing.
aspiration
ray shows
e of < 19m
54
ntilation an
een deterior
artner men
and illicit d
bilateral in
mmHg effect
Res
nd tachycard
rating with
tions that
drug use. Th
terstitial lu
tively exclu
spiratory
dia. She
a cough
she has
he main
ng field
des left
www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 55
Respiratory Q54
A 30 year old man with bronchial asthma was admitted to hospital for reassessment of
his recurring dry cough, chest tightness and wheezing.
Investigations show:
Neutrophils 6 (2‐7.5) x 10^9/l
Lymphocytes 3 (1.3‐3.5) x 10^9/l
Eosinophils 9 (0.04‐0.44) x 10^9/l
CXR shows reticulonodular shadowing
Investigations to look for causes of the eosinophilia (e.g., parasitosis, immunodeficiency
and malignant disease) included stool microscopy, tumour marker assays (for
carcinoembryonic antigen and cancer antigen (CA) 125, CA 19‐9, CA 15‐3 and CA 72‐4),
mammography, gastroduodenoscopy, bronchoscopy, abdominopelvic ultrasonography,
and vaginal and pelvic examination; all yielded normal findings.
Pulmonary function tests revealed a mild obstructive and moderate restrictive pattern
[FEV1] 46%,[FVC] 55%, ratio of FEV1 to FVC 72, peak expiratory flow 53%, [DLCO] 46%.
What is the likely diagnosis?
A. Tuberculosis
B. Loeffler's syndrome
C. Sarcoidosis
D. Pulmonary embolism
E. Wegener's granulomatosis
Answer: b) Loeffler's syndrome.
Hypereosinophilic syndrome is a rare condition where there is an idiopathic eosinophil
count of > 15 x 10^9/dl.
It is associated with Loeffler's syndrome which is a transient pulmonary reaction with
nodular or reticular shadowing (diffuse, fanshaped shadowing) on chest radiology and
eosinophilia.
Hypereosinophilic syndrome generally affects young men ages 20‐50. Thrombotic
tendency, neurological involvement (loss of intellect, depressed mood and poor
coordination) and restrictive cardiomyopathy occur. There is response to steroids.
The lung involvement results in nocturnal cough, productive sputum, wheezing and
dyspnea, which raises the
suspicion of bronchial hyperreactivity. Patients may be misdiagnosed as having asthma.
However, pulmonary function tests typically reveal no airflow limitation.

www
Dr. K
Re
A 40
has
uns
Whi
Ans
Kart
(tra
bro
Sym
rheu
sub
ano
Dex
w.MRCPass.c
Khalid Yusuf
spiratory
0 year old m
recurrent
uccessful in
ich one of th
A. Hypo
B. Alpha
C. Defec
D. Karta
E. Asthm
wer: d) Kart
tagener's
nsposition)
nchiectasis,
mptoms and
umatoid art
clavian arte
osmia or clu
xtrocardia in
com
f Elzohry ‐ So
y Q55
man has a h
episodes o
n having chi
he following
gammaglobu
a 1 antitrypsi
ct in CFTR ge
aganer's synd
ma variant
tagener's sy
syndrome
of the v
, and immo
d signs are
thritis, rena
ery. There
bbing.
n Kartagene
ohag Teachin
history of lo
of chest inf
ldren. He a
g is likely?
ulinaemia
in deficiency
ne
drome
yndrome.
is heredi
viscera, ab
bility of the
dyspnoea,
al abnormal
is also oti
er's syndrom
ng Hospital ‐
ng standing
fections and
lso has hea
y
itary. It c
bnormal fro
e cilia.
productive
ities, malfo
itis media,
me
‐ 2012
g cough wit
d sinusitis.
ring difficul
comprises
ontal sinus
cough, rec
ormations of
nasal spee
56
th sputum p
He is mar
lty.
a triad o
ses produc
current resp
f renal vess
ech, conduc
Res
production.
ried but ha
of: situs i
cing sinusi
piratory inf
sels and ano
ctive heari
spiratory
He also
as been
nversus
tis and
fections,
omalous
ng loss,

www
Dr. K
Re
A 40
that
doe
pur
Wha
Ans
The
diag
out
Seru
mon
Sarc
w.MRCPass.c
Khalid Yusuf
spiratory
0 year old w
t have not
es not have
ple / red no
at is the app
A. Lung
B. Arran
C. Arran
D. Start
E. Arran
wer: e) arra
e combinat
gnostic of s
patients wi
um angiote
nitor diseas
coidosis
com
f Elzohry ‐ So
y Q56
woman is r
responded
any other s
odules on he
propriate m
Biopsy
nge CT scan o
nge bronchos
prednisolon
ge outpatien
ange outpat
tion of bil
sarcoidosis.
ith full lung
ensin‐conve
se. Worseni
ohag Teachin
eferred wit
to a course
symptoms,
er shins. A c
managemen
of the lungs
scopy and br
e
nts appointm
tients appo
ateral hila
. This is usu
g function
erting enzym
ng disease
ng Hospital ‐
th a history
e of fluclox
and has ne
chest radiog
nt?
ronchoalveo
ment for follo
intment for
ar lymphad
ually self‐lim
tests inclu
me (ACE) le
can be trea
‐ 2012
y of red, pai
xacillin given
ever smoked
graph show
lar lavage to
ow up
r follow up.
denopathy
miting. She
ding transf
evel and lu
ted with pr
57
inful legs of
n for celluli
d. Examinat
ws prominen
exclude ma
and eryth
should ho
fer factor a
ung function
rednisolone
Res
f 3 weeks d
itis. She is a
tion reveals
nt hilar regio
lignancy
hema nodo
w ever be
and lung v
ns can be
e.
spiratory
duration
afebrile,
s tender
ons.
osum is
seen in
olumes.
used to

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 58
Respiratory Q57
A 50 year old patient has become more breathless over several days. He was assessed
with a spectrum of tests. The chest X ray was normal. In the interpretation of his arterial
blood gases on air the following results were obtained:‐
pO2: 8.0 kPa
pCO2: 9.2 kPa
pH: 7.40
Base Excess +2
What disease is likely to have caused this?
A. Community acquired pneumonia
B. Bronchiectasis
C. Tuberculosis
D. Guillain barre syndrome
E. Small cell carcinoma
Answer: d) guillain barre syndrome.
The raised CO2 and hypoxia demonstrate type II respiratory failure. The causes of this
could be obstructive lung disease, neurogenic, or musculoskeletal (kyphoscoliosis).
www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 59
Respiratory Q58
A 40 year lady presents with a 6 month history of intermittent haemoptysis. She
describes episodes of cutaneous flushing, which typically affects the head and neck. The
episodes are often associated with an unpleasant warm feeling, itching feeling. They last
for half an hour.
She is slightly breathless but has had no evidence of leg swelling or chest pain. She
smokes 10 cigarettes a day.
She has lost 3 kg of weight in the past two months and has been experiencing night
sweats. A Chest x ray shows sail sign in the left lower lobe, but no visible consolidation.
Which one of the following is the most likely diagnosis?
A. Wegener's granulomatosis
B. Goodpasture's syndrome
C. Carcinoid tumour
D. Sarcoidosis
E. Tuberculosis
Answer: c) carcinoid tumour.
A sail sign on the CXR indicates collapse of the left lower lobe. The likely diagnosis is a
carcinoid tumour, which is associated with smoking.
An early and frequent (94%) symptom of carcinoid tumors is cutaneous flushing, which
typically affects the head and neck. Episodes are often associated with an unpleasant
warm feeling, itching, palpitation, upper‐body erythema and edema, salivation,
diaphoresis, lacrimation, and diarrhea. Exercise, stress, or certain foods (eg, cheese)
may trigger an attack. Initial attacks are short, lasting only a few minutes. With time, the
duration increases to hours. Flushes are reported to be longest in association with
bronchial carcinoids.
Carcinoid tumours are neuroendocrine tumours arising from Kultchitzsky cells. They can
be central or peripheral, and are classified as typical or atypical depending on their
histology. They are slow growing tumours of lung with a peak incidence around age 40.
Bronchial obstruction is common. Diagnosis is by bronchoscopy and biopsy.

www
Dr. K
Trea
Sail
w.MRCPass.c
Khalid Yusuf
atment is us
sign (straig
com
f Elzohry ‐ So
sually with
ght line arou
ohag Teachin
lobectomy.
und the hea
ng Hospital ‐
.
art border)
‐ 2012 60
Resspiratory

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 61
Respiratory Q59
A 68 year old man with emphysema is referred to a chest clinic for consideration of
oxygen therapy. Despite maximal treatment with bronchodilators, his exercise tolerance
is reduced to about 25 yards.
Physical examination and pulmonary function test was consistent with emphysema.
There was no evidence of heart failure. ECG was normal. CXR showed hyperinflated lung
fields.
Oxygen saturation was 90%. ABG showed ph of 7.36, pCO2 of 3.7kPa, pO2 of 7.6 kPa.
What should be recommended?
A. Overnight SaO2 monitoring
B. Course of steroids
C. Walking test with a trial of oxygen
D. Repeated ABG in 6 weeks time
E. Long‐term oxygen therapy
Answer: c) Walking test with a trial of oxygen.
This patient does not meet the criteria for long term oxygen therapy, which is indicated
when the paO2 is persistently below 7.3 kPa on air. Clinical stability is defined as the
absence of exacerbation of chronic lung disease for the previous 5 weeks.
Patients without chronic hypoxaemia and not on LTOT, should be considered for
ambulatory oxygen therapy if they show evidence of exercise oxygen desaturation (a fall
of SaO2 of at least 4% below 90%), improvement in exercise capacity with ambulatory
oxygen therapy and motivation to use the ambulatory oxygen outside the house.
Assessment should be performed on both air and supplemental oxygen with the patient
blinded as to the content of the cylinder.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 62
Respiratory Q60
A 50 year old woman presents with breathlessness that has been getting gradually
worse over a few weeks and she has difficulty mobilising. On physical examination she is
found to have a large left sided pleural effusion.
The presence of the effusion is confirmed by chest radiography.
The most appropriate initial investigation would be:
A. Diagnostic aspiration of pleural fluid
B. Sputum cytology
C. CT chest
D. Pleural biopsy
E. Mantoux test
Answer: a) Diagnostic aspiration of pleural fluid.
The first investigation should be diagnostic aspiration of pleural fluid.
Light’s criteria can be used to distinguish transudates from exudates: in exudates at
least one of the following three criteria are met:
pleural fluid protein concentration greater than 50% of that in plasma;
pleural fluid LDH greater than 60% of that in plasma;
pleural fluid LDH more that two thirds the upper limit of normal in plasma
In general, if the protein is < 30 g then it is considered to be a transudate, if > 30 g then
it is an exudate.

www
Dr. K
Re
A 38
is H
doc
Wha
Ans
PCP
alve
The
3 w
pati
dea
Pne
w.MRCPass.c
Khalid Yusuf
spiratory
8 year old m
HIV positive
tor makes a
at treatmen
A. AZT
B. IV me
C. IV co‐
D. IV flu
E. IV am
wer: c) IV c
P patients a
eolar infiltra
e patient sho
weeks as w
ients with m
th by over 5
eumocystis p
com
f Elzohry ‐ So
y Q61
man is adm
. His chest
a diagnosis
nt should be
etronidazole
‐trimoxazole
conazole
mphotericin
o‐trimoxazo
re usually h
ates.
ould receive
well as gluc
moderate to
50%.
pneumonia
ohag Teachin
itted to the
radiograph
of Pneumo
e started?
ole.
hypoxic and
e intraveno
cocorticoids
o severe hy
ng Hospital ‐
e hospital w
h shows bil
cystis carin
d chest radi
us co‐trimo
s (IV methy
ypoxia, dec
‐ 2012
with a one‐w
ateral alveo
ii pneumon
iograph cha
oxazole in a
ylpred for
reases the
63
w eek histo
olar infiltra
nia (PCP).
aracteristica
dose of 12
3 days). Th
risk of resp
Res
ry of dyspn
tes. The ad
ally shows b
0mg/kg for
his, when
piratory fail
spiratory
oea. He
dmitting
bilateral
at least
used in
ure and

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 64
Respiratory Q62
A 40 year old man has a 3 month history of cough, dyspnoea and sputum production. He
smokes 20 cigarettes a day and has a history of asthma. There is no history of asbestos
exposure.
His WBC count is 24 x 10^9/l with 70% neutrophils and 3.0 x 10^9/l (5%) eosinophils. IgE
level is elevated. He has decreased breath sounds corresponding to parenchymal
infiltrates on the CXR.
Which is the best test to confirm the diagnosis?
A. HIV test
B. Stool for ova,cysts,parasites
C. Autoimmune screen
D. Aspergillus precipitins
E. Sputum for Acid Fast Bacilli
Answer: d) Aspergillus precipitins.
The condition described is Allergic Broncho Pulmonary Aspergillosis, commoner among
asthmatics and cystic fibrosis patients. Wheeze, shortness of breath and productive
cough are symptoms.
Allergic bronchopulmonary aspergillosis results from an allergic reaction to Aspergillus
fumigatus which actually grow s in the walls of the bronchi.
Eosinophilia and high IgE levels are suggestive of the condition. Aspergillus precipitins
(lab test to detect antibodies) the diagnosis. The chest radiograph often shows evidence
of proximal bronchiectasis.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 65
Respiratory Q63
A 55 year old woman is admitted with a history of syncopal episodes and
breathlessness. There is no prior history of recent travel.
On examination she looks distressed. Her pulse rate is 120 beats per minute, blood
pressure 85/60, JVP is elevated by 5 cm. Respiratory rate 26 per minute, there is a soft
systolic murmur at the left sternal edge. Breath sounds are clear.
Investigations show : HB 12.4 g/dL, Blood gases pH 7.42, Pa CO2 3.3 kPa, Pa O2 8.5 kPa.
She was put on high flow oxygen and given low molecular weight heparin.
The next step in management of this patient should be:
A. High dose aspirin
B. Coronary angiography
C. Urgent CTPA and consider thrombolysis
D. Intravenous unfractionated heparin
E. VQ scan
Answer: c) urgent CTPA and consider thrombolysis.
The diagnosis massive central pulmonary embolus as the patient is hypoxic and
hypotensive. The best management is to obtain an urgent CTPA and then thrombolyse if
there are no contraindications (e.g. high risk of bleeding).

www
Dr. K
Re
A 50
past
mar
Whi
Ans
The
exp
alte
and
Var
the
Flow
w.MRCPass.c
Khalid Yusuf
spiratory
0 year old l
t year. She
rked stridor
ich of the fo
A. FEV1
B. FVC
C. Resid
D. Flow
E. Funct
wer: d) flow
e flow volum
iration at d
erations in t
expiratory
iable intrat
expiratory
w Volume L
com
f Elzohry ‐ So
y Q64
ady has bee
has previo
r.
ollowing is h
ual volume
volume loop
tional residua
w volume lo
me loop is a
different lu
the airway r
limbs of th
horacic lesi
limb.
Loop showin
ohag Teachin
en complai
ously been
helpful in in
p
al capacity
oop.
a graphic re
ng volumes
resistance.
e flow volu
ions are ch
ng airways o
ng Hospital ‐
ning of wor
diagnosed
vestigating
ecording of
s, and may
Fixed lesion
me loop.
aracterized
obstruction
‐ 2012
rsening diff
with a goit
g the extent
f airflow du
y be affecte
ns cause pla
d by expirat
66
iculty with
tre. On exa
of airways
uring maxim
ed in a cha
ateaus in b
tory slowing
Res
breathing o
amination, s
obstruction
mal respirat
aracteristic
oth the ins
g and flatte
spiratory
over the
she had
n?
tion and
way by
piratory
ening of

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 67
Respiratory Q65
A 60 year old lady has arthritic changes on her hand joints of ulnar deviation and
Butonniere's defomirty. She has chronic breathlessness.
Which of the following is a likely association?
A. Aspergillosis
B. Pulmonary fibrosis
C. Empyema
D. Lung carcinoma
E. Pulmonary emboli
Answer: b) pulmonary fibrosis.
The pulmonary complications of rheumatoid arthritis are :
pulmonary fibrosis (interstitial lung disease)
bronchiolitis obliterans with organizing pneumonia
bronchiectasis
interstitial pneumonitis secondary to drugs
www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 68
Respiratory Q66
A 35 year old man has significant wheezing and breathlessness. Recordings of peak
flows shows diurnal variation. He was prescribed with salbutamol but continues to have
frequent wheezy episodes.
What is the next step in management?
A. Phosphodiesterase inhibitors
B. Leukotriene antagonists
C. Oral antibiotics
D. Inhaled corticosteroids
E. Oral steroids
Answer: d) inhaled corticosteroids.
Diurnal PEFR variation points tow ards a diagnosis of asthma. First line treatment are
short acting B agonists such as salbutamol and Patients who do not respond to B
agonists should be treated with inhaled corticosteroids (becotide or flixotide) which
help to reduce exacerbations in the long term.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 69
Respiratory Q67
A 55 year old lady presents with worsening breathlessness. She has a history of
Raynaud’s phenomenon, heartburn and reflux.
On examination, the skin over her fingers is tight and shiny. She has multiple
telangiectasia over her face and nail‐fold capillary loops are seen. Her investigations
show she has Anticentromere antibodies.
What respiratory complication may occur?
A. Churg Strauss syndrome
B. Metastatic adenocarcinoma
C. Pulmonary hypertension
D. Allergic bronchopulmonary aspergillosis
E. Mesothelioma
Answer: c) pulmonary hypertension.
The patient has the clinical features of limited cutaneous scleroderma (LcSScformerly
CREST syndrome). Anticentromere antibodies occur in 70‐80% of these patients. A
significant respiratory complication is pulmonary hypertension. Treatment is with
prostaglandin analogues e.g. iloprost (intravenous infusions) or bosentan (oral).

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 70
Respiratory Q68
A 16 year old boy was brought to the A&E with wheeze and extensive rash whilst eating
at a Chinese takeaway.
On examination, he had extensive wheezes in his chest, stridor, as well as urticaria
covering his upper and lower limbs. His BP is 82/50 mmHg.
What is the most likely diagnosis?
A. C1 Esterase Deficiency
B. Salmonella infection
C. Idiopathic urticaria
D. Asthma
E. Allergy
Answer: E) allergy
The scenario is consistent with a food allergy, e.g. nuts, leading to an anaphylactic
reaction. The patient should be treated with hydrocortisone (iv or im) as well as
chlorpheniramine.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 71
Respiratory Q69
A 40 year old man with pneumonia is being examined.
Which one of the following positive auscultatory signs is diagnostic of bronchial
breathing?
A. Rhonchi
B. Increased vocal resonance
C. Aegophony
D. Whispering pectoriloquy
E. Fine inspiratory crepitations
Answer: d) Whispering pectoriloquy.
Whispering pectoriloquy is a diagnostic sign for bronchial breathing.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 72
Respiratory Q70
A 16 year old boy with previous tuberculosis had a 7‐day history of progressive cough,
wheeze and tachypnoea, despite 4 days of intravenous flucloxacillin and cefotaxime
therapy.
Total serum IgE titre was 1600 IU (normal range, 0–180 IU) and the skin prick test was
positive for Aspergillus fumigatus.
What should he be treated with?
A. Praziquantel
B. Aciclovir
C. Itraconazole
D. Rifampicin
E. HAART
Answer: c) itraconazole.
Allergic bronchopulmonary aspergillosis (ABPA) is a diagnosis which can be confirmed by
significantly elevated serum IgE titre, positive skinprick tests for aspergillus, positive IgG
aspergillus precipitins.
Treatment is with antifungals. Steroids may be required in patients with respiratory
distress.

www
Dr. K
Re
A 35
arriv
brea
He
read
Res
dev
Wha
Ans
The
into
As t
a la
Larg
w.MRCPass.c
Khalid Yusuf
spiratory
5 year old m
ved 30 min
athlessness
is cyanosed
ding 81%, d
piratory ex
viation of th
at immedia
A. Pleur
B. Insert
C. Arran
D. Check
E. Conta
wer: b) Inse
e diagnosis
o a tension p
the patient
rge bore ne
ge right side
com
f Elzohry ‐ So
y Q71
man whose
nutes earlie
s. He collaps
d and has a
despite high
xamination
e trachea to
ate course of
odesis
t large bore n
nge for urgen
k arterial blo
act ITU to arr
ert large bo
is a right s
pneumotho
is unstable,
eedle would
ed pneumot
ohag Teachin
condition h
er with a 2
sed while aw
a pulse 130/
flow oxyge
reveals re
ow ards the
of action sho
needle into r
nt portable c
ood gases an
range for the
re needle in
sided spont
orax.
, there is no
d reduce the
thorax
ng Hospital ‐
has suddenl
2‐hour hist
w aiting CX
/min and B
en via a re‐b
duced brea
e left.
ould be take
right hemith
hest XR
d commence
e patient to b
nto right he
taneous pn
o time to ar
e pressure i
‐ 2012
y deteriora
tory of cen
R.
BP of 85/45
breathe mas
ath sounds
en?
orax
e BIPAP
be ventilated
emithorax.
eumothora
rrange for p
n the right
73
ted is broug
ntral pleurit
5 mmHg. Ox
sk.
in the rig
d
ax, which h
portable che
hemithorax
Res
ght to A&E.
tic chest pa
xygen satur
ght lung fie
as now dev
est XR, inse
x.
spiratory
. He had
ain and
ration is
eld with
veloped
ertion of

www
Dr. K
Re
A 4
feve
prev
Ove
sam
His
Wha
Ans
Prev
wei
exp
Silic
w.MRCPass.c
Khalid Yusuf
spiratory
5 year old
ers and ha
viously trea
er the past
mples are AF
chest X‐ray
at is the like
A. Silico
B. React
C. Cadm
D. Histio
E. Asbes
wer: a) silic
vious TB p
ght loss. C
osure to sil
cosis
com
f Elzohry ‐ So
y Q72
man devel
s lost half
ated tubercu
ten years h
FB negative
y shows nod
ely diagnosi
sis
tivation of TB
mium lung
ocytosis X
stosis
cosis.
redisposes
Coal miners
ica are at ri
ohag Teachin
ops breath
f a stone i
ulosis. He w
he and his p
.
dular shadow
is?
B
to silicosis
s, quarry w
sk.
ng Hospital ‐
lessness an
n weight o
works as a ta
partner wen
wing in the
s, which ca
workers and
‐ 2012
nd a non pr
over the p
axi driver.
nt fossil hu
upper zone
n present
d people w
74
roductive c
ast six mo
nting in old
e.
as fever, b
whose hobb
Res
ough. He h
onths. He h
d quarries.
breathlessne
bies predisp
spiratory
has mild
has had
Sputum
ess and
pose to

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 75
Respiratory Q73
A 70 year retired sandblaster has worsening symptoms of cough, wheeze and
breathlessness. He has been keeping parrots for 15 years as a hobby.
Serum precipitins for M faeni are negative.
Chest X ray shows hyperinflated lungs.
His lung function tests show :
FEV1 1.8L (predicted 2.6)
FVC 3.0L (predicted 3.2)
FEV1/FVC 60%
Which of the following is the likely diagnosis?
A. Silicosis
B. Chronic obstructive airways disease
C. Farmer's lung
D. Allergic bronchopulmonary aspergillosis
E. Pigeon fancier's lung
Answer: b) chronic obstructive airways disease.
The lung function tests show an obstructive picture (reduced FEV1/FVC ratio).
Interestitial lung diseases are more likely to cause a restrictive picture on the lung
function test.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 76
Respiratory Q74
A 60 year old asthmatic lady is admitted with sudden onset left sided pleuritic chest pain
accompanied by shortness of breath.
Arterial blood gases are as follow s: pH of 7.30, p02 of 7.5kPa, and pCO2 of 3.8 kPa.
Chest XR is normal. She is commenced on oxygen.
What is the most appropriate immediate action?
A. Request a chest XR in expiration
B. Request D‐dimer
C. Start low molecular weight heparin and request CT pulmonary angiography
D. Start low molecular weight heparin and request a V/Q scan
E. Broad spectrum antibiotics
Answer: c) Start low molecular weight heparin and request CT pulmonary angiography.
The symptoms and findings clearly point out tow ards pulmonary embolism (PE). As the
clinical probability of PE is high, measurement of D‐dimer should not be performed,
since the result would not alter the need for definitive investigation. Measurement of D‐
dimer should only be performed when the probability of PE is low , when a normal value
would be taken as reassuring and further investigation would not be pursued.
V/Q scan less likely to be unhelpful in view of her asthma; hence a CT pulmonary
angiogram would be the imaging procedure of choice.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 77
Respiratory Q75
A 65 year old man has had 5 kg weight loss over 6 months. He is an ex smoker of 25
cigarettes a day for 40 years and used to work in a coal mine.
A Chest X ray shows a large right sided pleural effusion and several pleural plaques in
both lung peripheries.
Pleural aspiration reveals an exudate with 42 g of protein.
What investigation should be recommended?
A. Bronchoscopy
B. Lung function tests
C. Spiral CT of the chest
D. Thoracoscopy and biopsy
E. Sputum for AFB
Answer: d) thoracoscopy and biopsy.
This patient probably has a malignant effusion as demonstrated by the exudate from the
pleural effusion. As he is symptomatic, the best option would be to drain the fluid as
well as confirm a diagnosis simultaneously.
A video assisted thoracoscopy would help to do this. In this procedure, an illuminated
tube is inserted through a small incision made betw een the ribs. It allows the operator
to visualize structures inside the chest and to perform simple procedures such as biopsy
and nodule excision.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 78
Respiratory Q76
A 65 year old man with a smoking history of 50 a day for many years has been a chest
radiograph showing a lung mass. He is presently waiting a bronchoscopy.
Which one of the following supports a diagnosis of small cell lung cancer?
A. Disseminated intravascular coagulation
B. Hypertrophic pulmonary osteoarthropathy (HPOA)
C. Syndrome of inappropriate antidiuretic hormone secretion (SIADH)
D. Thrombocytosis
E. Hypercalcaemia
Answer: c) Syndrome of inappropriate antidiuretic hormone secretion (SIADH).
SIADH is most comonly seen with small cell carcinoma rather than non‐small cell
carcinoma. HPOA, hypercalcaemia without bone metastasis is more common in
squamous cell carcinoma. DIC and thrombocytosis are more common with
adenocarcinoma.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 79
Respiratory Q77
A 60 year old woman presents with a 6‐month history of progressive shortness of
breath. Her past medical history is unremarkable apart from Raynaud’s syndrome for
which she takes a calcium channel blocker.
On examination she has telangiectasia.
Her chest radiograph shows clear lung fields, prominent pulmonary arteries and mildly
enlarged heart. Spirometry is normal, but gas transfer is reduced by 40% of predicted.
What is the most likely diagnosis?
A. Cor pulmonale
B. Pulmonary arterial hypertension
C. Sarcoidosis
D. Pulmonary emboli
E. Pulmonary oedema
Answer: b) Pulmonary arterial hypertension.
The patient is likely to have scleroderma from the clinical history.
There is also associated pulmonary hypertension which such patients are at risk of.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 80
Respiratory Q78
A 75 year old lady is admitted with an acute exacerbation of chronic obstructive
pulmonary disease (COPD). One hour after admission she remains distressed with a
respiratory rate of 35 per minute and is peripherally cyanosed. Repeated arterial blood
gases show a severe respiratory acidosis with a pH of <7.2.
Which of the following treatments is recommended?
A. Give intravenous infusion of aminophylline
B. Give intravenous hydrocortisone
C. Repeat bronchodilator therapy and arrange repeat arterial gases
D. Arrange for noninvasive positive pressure ventilation
E. High flow oxygen
Answer: d) Arrange for noninvasive positive pressure ventilation.
Non invasive positive pressure ventilation should be considered, especially in COPD
patients when there is a need for ventilatory assistance as indicated by worsening
dyspnoea, acute respiratory acidosis and worsening oxygenation. If this does not work
then intubation and ventilation may be necessary.

www
Dr. K
Re
A 65
of t
Whi
airw
Ans
The
with
Flow
w.MRCPass.c
Khalid Yusuf
spiratory
5 year old m
he trachea
ich of the f
ways obstru
A. Flow
B. Force
C. Force
D. Peak
E. Resid
wer: A) flow
e flow volum
h a retroste
w volume lo
com
f Elzohry ‐ So
y Q79
man presen
by a retrost
following in
uction?
volume loop
ed expiratory
ed vital capac
expiratory fl
ual volume
w volume lo
me loop is t
ernal mass.
oop showing
ohag Teachin
nts with ins
ternal goitr
nvestigation
p
y volume
city
low rate
oop
the best me
g airways o
ng Hospital ‐
piratory str
e.
ns is the m
ethod of as
bstruction
‐ 2012
ridor. A che
most useful
ssessing ext
81
est X‐ray sho
to assess
tent of obst
Res
owed comp
the severity
truction ass
spiratory
pression
y of his
sociated

www
Dr. K
Re
A 2
hist
65%
sim
Whi
Ans
α1
(obs
phe
Smo
w.MRCPass.c
Khalid Yusuf
spiratory
5 year old
ory of recu
%, reduced
ilar present
ich is the lik
A. Eosin
B. Asthm
C. α1 an
D. Fibro
E. Rheum
wer: c) α1 a
antitrypsin
structive p
enotypes are
oking cessat
com
f Elzohry ‐ So
y Q80
man who
urrent chest
FEV1, FVC
tation.
kely diagnos
ophilic granu
ma
ntitrypsin def
sing alveolit
matoid lung
antitrypsin d
n deficienc
icture) on
e M S or Z.
tion is essen
ohag Teachin
smokes, h
t infections
and KCO o
sis?
uloma
ficiency
is
deficiency.
cy is autos
the lung f
ZZ has the w
ntial.
ng Hospital ‐
has progres
s. His lung f
of 45% pred
somal rece
function te
worse outco
‐ 2012
sive breath
function te
dicted. He
essive and
ests, with r
ome.
82
hlessness. H
sts show a
also has an
causes an
reduced tra
Res
He has had
FEV1/FVC
n uncle who
n emphyse
ansfer fact
spiratory
d a long
ratio of
o had a
ematous
or. The

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 83
Respiratory Q81
A 55 year old woman with rheumatoid arthritis is referred with a history of recurrent
chest infections, intermittent wheeze and production of half a teacupful of sputum
daily, on occasions with blood stained.
What is the most likely diagnosis?
A. Pulmonary fibrosis
B. Bronchiectasis
C. Emphysema
D. Tuberculosis
E. Squamous lung carcinoma
Answer: b) Bronchiectasis.
Bronchiectasis is associated with rheumatoid arthritis, occurring in 3‐4% of patients with
this condition. As with all other causes of bronchiectasis, it presents with recurrent
chest infections and excessive sputum. Recurrent haemoptysis is a common feature.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 84
Respiratory Q82
A 38 year old man with a history of depression is brought to the accident and
emergency department after being found unconscious in a garage. A friend said that he
complained of a headache, then had nausea and vomiting.
He then became unrousable.
Oxygen saturations are 95% on air and breath sounds are clear on auscultation.
What is the likely diagnosis?
A. Pulmonary eosinophilia
B. Pulmonary embolus
C. Adult respiratory distress syndrome
D. Pneumocystis pneumonia
E. Carbon monoxide poisoning
Answer: e) Carbon monoxide poisoning.
Carbon monoxide poisoning is produced by the incomplete combustion of carbon
containing fuels such as gas, coal, oil, wood and coke.
Headache is the most common symptom (90%) followed by nausea & vomiting, vertigo,
alteration in consciousness and weakness.
The cherry red skin colour occurs when COHb concentration exceeds 20% but it is rarely
seen in life. Pulse oximetry gives falsely high oxygen saturation sand it is not
recommended.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 85
Respiratory Q83
A 45 year man has breathlessness and a dry cough. On examination, there are bilateral
basal crepitations in his lungs. Oxygen saturations are 95% on air. Circulating precipitins
towards Micropolyspora faeni are positive.
What is the likely diagnosis?
A. ABPA
B. Bagassosis
C. Farmer's lung
D. Bird fancier's lung
E. Cheese worker's lung
Answer: c) farmer's lung.
This is a form of hypersensitivity pneumonitis. Farmer's lung is caused by the
actinomycetes Micropolyspora faeni, and bagassosis is caused by Thermoactinomyces
sacchari.

www
Dr. K
Re
A 4
feve
prev
Ove
sam
His
Wha
Ans
Prev
wei
exp
Silic
w.MRCPass.c
Khalid Yusuf
spiratory
5 year old
ers and ha
viously trea
er the past
mples are AF
chest X‐ray
at is the like
A. Silico
B. Cadm
C. Histio
D. React
E. Asbes
wer: a) silic
vious TB p
ght loss. C
osure to sil
cosis‐ Mid a
com
f Elzohry ‐ So
y Q84
man devel
s lost half
ated tubercu
ten years h
FB negative
y shows nod
ely diagnosi
sis
mium lung
ocytosis X
tivation of TB
stosis
cosis.
redisposes
Coal miners
ica are at ri
nd Upper Z
ohag Teachin
ops breath
f a stone i
ulosis. He w
he and his p
.
dular shadow
is?
B
to silicosis
s, quarry w
sk.
Zone linear a
ng Hospital ‐
lessness an
n weight o
works as a ta
partner wen
wing in the
s, which ca
workers and
and reticulo
‐ 2012
nd a non pr
over the p
axi driver.
nt fossil hu
upper zone
n present
d people w
onodular sh
86
roductive c
ast six mo
nting in old
e.
as fever, b
whose hobb
hadowing,
Res
ough. He h
onths. He h
d quarries.
breathlessne
bies predisp
spiratory
has mild
has had
Sputum
ess and
pose to

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 87
Respiratory Q85
A 70 year old man who has previously worked in the building trade presents with a
history of chest pain and dyspnoea. On examination he has evidence of a right‐sided
pleural effusion. Pleural aspiration is performed and a pleural biopsy taken. Histology
from the biopsy shows mesothelioma.
What should be done?
A. The diagnosis should be queried
B. Radiotherapy should be given to prevent seeding of tumour cells
C. Surgery
D. Chemotherapy should be given to prevent seeding of tumour
E. Curative radiotherapy should be given
Answer: b) Radiotherapy should be given to prevent seeding of tumour cells.
In mesothelioma no treatment has been shown to influence the universally fatal
outcome. After obtaining a positive biopsy, radiotherapy should be given in an attempt
to prevent seeding of tumour cells, around the area of the biopsy.

www
Dr. K
Re
A 50
to c
swe
and
CXR
The
Ans
TB i
Red
w.MRCPass.c
Khalid Yusuf
spiratory
0 year old i
casualty. He
eats. On exa
there are c
R shows fibr
investigati
A. CT ch
B. Gastr
C. Sputu
D. Mant
E. Fibreo
wer: c) Spu
s likely. In a
d coloured A
com
f Elzohry ‐ So
y Q86
v drug user
e has a chr
amination h
crepitations
rosis and ca
on most like
hest
ric lavage
um for acid a
toux test
optic bronch
tum for aci
a patient wi
AFB
ohag Teachin
r has been r
ronic cough
he is unkem
s over the a
vitation in t
ely to confir
and alcohol f
hoscopy
d and alcoh
th a produc
ng Hospital ‐
referred to
h productiv
pt and ema
pex of the l
the left ape
rm the diag
ast bacilli
hol fast baci
ctive cough,
‐ 2012
the medica
ve of sputu
aciated. His
left lung.
x.
gnosis would
illi.
, AFBs shou
88
al ward afte
um, loss of
trachea is d
d be:
uld be positi
Res
er being bro
weight, an
deviated to
ive in the sp
spiratory
ought in
nd night
the left
putum.

www
Dr. K
Re
A 5
nod
and
mul
Whi
Ans
Mul
can
sugg
A m
w.MRCPass.c
Khalid Yusuf
spiratory
5 year old
dules presen
transbron
ltinucleated
ich of the fo
A. Histo
B. Asper
C. Tuber
D. Small
E. Silicos
wer: c) tube
ltinucleated
be present
gests either
multinucleat
com
f Elzohry ‐ So
y Q87
smoker has
nt in the p
nchial biop
d giant cells
ollowing is l
plasmosis
rgillosis
rculosis
l cell carcino
sis
erculosis.
d giant cells
t in viral inf
r sarcoid, TB
ed giant ce
ohag Teachin
s a history
erihilar reg
psy is don
.
likely?
ma
s are very la
ections (e.g
B or Wegen
ll
ng Hospital ‐
of breathle
gion. His se
ne. This s
arge epider
g. herpes), T
ner's granulo
‐ 2012
essness and
rum calcium
shows non
rmis cells th
TB or lymph
omatosis.
89
d a dry cou
m is norma
n necrotic
hat have mu
homa. Gran
Res
gh. He has
al. A bronch
granulom
ultiple nucle
ulomatous
spiratory
several
hoscopy
as and
ei. They
disease

www
Dr. K
Re
A 3
and
Whi
Ans
Disc
ison
Urin
w.MRCPass.c
Khalid Yusuf
spiratory
0 year old
is about to
ich drug ma
A. Pyraz
B. Eryth
C. Rifam
D. Isonia
E. Etham
wer: c) Rifa
coloration o
niazid is an e
ne discolour
com
f Elzohry ‐ So
y Q88
woman wi
o be started
ay cause uri
zinamide
romycin
mpicin
azid
mbutol
ampicin.
of urine is
enzyme inh
ration in a p
ohag Teachin
th epilepsy
on quadru
ine discolou
due to rifa
hibitor.
patient taki
ng Hospital ‐
y has been
ple therapy
uration?
ampicin. Ri
ng Rifampic
‐ 2012
diagnosed
y.
ifampicin is
cin
90
with pulm
s a liver en
Res
onary tube
nzyme indu
spiratory
erculosis
ucer but

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 91
Respiratory Q89
A 30 year old male patient presents with worsening rhinitis, cough and wheezing, which
has occurred for the past 2 years. On admission, his lung function tests show FEV1 of
55% predicted and FVC of 65% predicted and a chest X ray showed bilateral infiltrates.
He had an eosinophil count of 5 x 10^9/l (0.04‐0.4) and sputum eosinophilia of 80% was
also found. There was also elevated IGE levels of >1000 kU/L. Serum ANCA was positive
at a dilution of 1:1024.
A nasal biopsy showed chronic inflammation, with some areas suggestive of vasculitis,
and eosinophilic infiltration.
Which diagnosis is most likely?
A. COPD
B. Mesothelioma
C. Churg Strauss syndrome
D. Tuberculosis
E. Extrinsic allergic alveolitis
Answer: c) Churg Strauss syndrome.
There are many causes of pulmonary symptoms with eosinophilia including Loeffler's
syndrome, Churg Strauss syndrome, pulmonary eosinophilic syndrome and ABPA.
Extrinsic allergic alveolitis does not cause a wheeze and also does not cause
eosinophilia.
Churg‐Strauss syndrome is an uncommon condition characterised by asthma and blood
eosinophilia together with an eosinophilic vasculitis. The initial phase of the disorder is
one of asthma and allergic rhinitis, often followed by peripheral blood eosinophilia with
eosinophilic tissue disease. The vasculitic phase that follows is life‐threatening; how
ever, it can often be treated effectively with immunosuppression. It is associated with
granuloma formation and vasculitis affecting several organs e.g. skin, pericardium,
kidney and lung.

www
Dr. K
Seru
tissu
pati
w.MRCPass.c
Khalid Yusuf
um eosinop
ue biopsy a
ients have c
com
f Elzohry ‐ So
philia and e
and the ant
cANCA and
ohag Teachin
levated IgE
tineutrophi
about 50%
ng Hospital ‐
levels are
il cytoplasm
have pANC
‐ 2012
typical. Lab
mic antibod
CA.
92
boratory dia
y (ANCA) t
Res
agnosis is b
est. About
spiratory
ased on
25% of

www
Dr. K
Re
A 44
mas
Wha
Ans
The
may
prec
Asp
w.MRCPass.c
Khalid Yusuf
spiratory
4 year old m
sses with ai
at is the like
A. tuber
B. Asper
C. Actino
D. Extrin
E. Coal w
wer: B) asp
e air halo si
y be predisp
cipitins are
ergilloma
com
f Elzohry ‐ So
y Q90
man has pr
r halo arou
ely diagnosi
rculosis
rgillosis
omycosis
nsic allergic a
worker’s lung
ergillosis.
ign is partic
posed to by
towards as
ohag Teachin
resented wi
nd them in
is?
alveolitis
g
cularly asso
y previous T
pergillus.
ng Hospital ‐
ith haemop
the upper z
ociated wit
TB infection
‐ 2012
ptysis. He ha
zones. He h
h the funga
leading to c
93
ad a chest
as positive
al infection
cavitation. T
Res
X ray which
serum prec
n aspergillos
The positive
spiratory
h shows
cipitins.
sis, This
e serum

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 94
Respiratory Q91
A 55 year lady has had a long history of productive cough and shortness of breath. She
often coughs up whitish sputum and is prone to chest infections. On examination her
temperature is 36° C, chest expansion is reduced and there are bilateral wet inspiratory
crackles.
Which one of the following treatments is most helpful?
A. Intravenous antibiotics
B. B agonist inhalers
C. Postural drainage
D. Morphine
E. Prednisolone
Answer: c) postural drainage.
This lady has bronchiectasis. There is no suggestion of a chest infection during this
episode of admission, hence postural drainage is the best treatment option.
www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 95
Respiratory Q92
A 55 year old farmer has had progressive breathlessness over the past 2 years. He
presents with a severe episode of dyspnea and productive cough which occurred 6
hours after he started working. He mentions that these episodes are typical but today is
more severe. On admission, his O2 saturations are 94% on air.
CXR shows bilateral interstitial shadowing in upper zones.
Which of the following is the most useful test?
A. Precipitins to aspergillus
B. Sputum for AFB
C. Kveim test
D. Precipitins to Micropolyspora faeni
E. Bronchoscopy
Answer: d) precipitins to Micropolyspora faeni.
This patient is likely to have extrinsic allergic alveolitis. The classic presentation of
farmer's lung results from inhalational exposure to thermophilic Actinomyces species.
Patients with extrinsic allergic alveolitis may present acutely with a flulike illness with
cough. They can also present subacutely with recurrent pneumonia or chronically with
exertional dyspnea, productive cough, and weight loss.
The onset of symptoms after acute exposure is usually betw een 4 and 12 hours. Some
antigens provoke symptoms after repeated exposure; these include bioaerosols of
microbial or animal antigens and a few reactive chemicals.
Thermophilic actinomycetes species which can cause EAA include Saccharopolyspora
rectivirgula (formerly Micropolyspora faeni), Thermoactinomyces vulgaris,
Thermoactinomyces viridis, and Thermoactinomyces sacchari.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 96
Respiratory Q93
A 60 year old woman had a CXR showing pulmonary fibrosis. Upon review , of her drug
history, which of the following drugs might she have been on in the past?
A. Clarithromycin
B. Amoxicillin
C. Busulphan
D. Omeprazole
E. Ciprofloxacin
Answer: C) busulphan.
Busulphan, bleomycin, amiodarone and nitrofurantoin are drugs which commonly cause
pulmonary fibrosis.

www
Dr. K
Re
A 6
The
afte
An X
in t
faen
Wha
Ans
Extr
cou
EAA
or c
In
acti
bird
zon
w h
EAA
w.MRCPass.c
Khalid Yusuf
spiratory
5 year old
ese symptom
er. He is a no
X‐ray of the
he lower p
ni.
at is the dia
A. Tube
B. Wege
C. Churg
D. Extrin
E. Pulmo
wer: d) ext
rinsic allerg
nt is norma
A is a delaye
cell mediate
Extrinsic
nomycetes
d fancier's l
e fibrosis ca
eeze.
A causing up
com
f Elzohry ‐ So
y Q94
farmer has
ms occur d
on smoker.
e chest reve
arts of the
agnosis?
rculosis
ener's granul
g Strauss syn
nsic allergic a
onary eosino
rinsic allerg
gic alveoliti
al. Bronchoa
ed hypersen
ed (type IV)
Allergic A
and avian p
ung. Precip
auses audib
pper zone fi
ohag Teachin
s been gett
during work
ealed intens
lung. He a
lomatosis
ndrome
alveolitis
ophilia
gic alveolitis
is causes a
alveolar lava
nsitivity rea
in chronic d
lveolitis, t
proteins, an
pitins to mic
ble crackles.
ibrosis
ng Hospital ‐
ing worsen
k and are o
sified interst
lso had rais
s.
neutrophil
age shows l
ction which
disease.
the most
nd the most
cropolyspor
. Symptoms
‐ 2012
ning breathl
often worse
titial lung m
sed serum
lia due to c
lymphocyte
h may be im
common
t common d
ra faeni are
s are typical
97
lessness for
e for appro
markings and
precipitins
cell mediat
es and mast
mmune com
antigens
diseases are
seen in far
lly of breath
Res
r the past 4
oximately 1
d reticular c
to micropo
ion but eo
t cells.
mplex (III) m
are therm
e farmer's lu
rmer’s lung
hlessness bu
spiratory
4 years.
0 hours
changes
olyspora
sinophil
mediated
mophilic
ung and
g. Upper
ut not

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 98
Respiratory Q95
A 22 year old woman has asthma for which she is using her salbutamol inhaler two or
three times a day.
What should be the next step in her management if she worsens?
A. Advise her to use the salbutamol inhaler regularly three times a day
B. Add regular inhaled steroid, e.g. beclometasone 100 microg twice daily
C. Add regular salmeterol twice daily
D. Add regular inhaled steroid, e.g. beclometasone 1000 microg twice daily
E. Add regular inhaled steroid, e.g. beclometasone 1000 microg twice daily, plus regular
long‐acting inhaled beta agonist
Answer: b) Add regular inhaled steroid, e.g. beclometasone 100 microg twice daily.
The British Thoracic Society Asthma guidelines are as follows:
Step 1: PRN use of inhaled short‐acting beta agonists
Step 2: regular inhaled steroids
Step 3: high‐dose inhaled steroids, or low ‐dose inhaled steroids plus long‐acting beta
agonist
Step 4: high‐dose inhaled steroid and regular bronchodilators (sustained release
theophylline, inhaled ipatropium, oral long‐acting beta agonist, high‐dose
inhaled bronchodilators, cromoglycate / nedocromil) Step 5: addition of regular
steroid tablets

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 99
Respiratory Q96
A 60 year old woman with know n COPD is referred with a 4‐month history of morning
headaches. She describes a dull headache which is generalised, worst upon waking up.
She has home nebuliser (salbutamol and atrovent) but is not on home oxygen.
A routine arterial blood gas on admission showed a pH of 7.34 pCO2 of 6.2 kPa, pO2 of
8.8 kPa and HCO3 30 mmHg.
What should be done?
A. Long‐term oxygen therapy
B. Ambulatory oxygen therapy
C. CT chest
D. Overnight SaO2 and CO2 monitoring
E. Repeat ABG
Answer: d) Overnight SaO2 and CO2 monitoring.
Morning headaches are often ascribed to patients with nocturnal hypoxia or early
morning hypercapnia. They are often associated with sleep apnea or a chronic
respiratory disease such as COPD.
The admission blood gases show mild hypoxia, and hypercapnia. There is respiratory
acidosis with metabolic compensation. It suggests that there is a high likelihood of
chronic hypoxia.
If oxygen monitoring confirmed nocturnal hypoxia (defined as O2 sats of < 90% for
more than 30% of sleep time), she may require nocturnal oxygen supplementation.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 100
Respiratory Q97
A couple attend the GP surgery with their 2 year old daughter. She has a history of
repeated chest infections, failure to thrive, and steatorrhoea (fatty stools). They also
have an 8 year old child who is fit and well.
What is the likely diagnosis?
A. Pulmonary Eosinophilia
B. Asthma
C. Cystic fibrosis
D. Congenital Tuberculosis
E. Bochdalek Hernia
Answer: c) Cystic fibrosis.
The gene defect in cystic fibrosis is in a mutation on chromosome 7. The inheritance is
autosomal recessive so the other child without symptoms has not inherited two CF
genes. Pulmonary disease develops over a few months after birth. Common infective
organisms are pneumoccocus, Haemophilus influenzae and Pseudomonas aeruginosa.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 101
Respiratory Q98
A 45 year old man complains of wheeziness which is worse. He has a history of asthma.
His current medication consists of a low dose of inhaled corticosteroids and inhaled
short‐acting beta 2 agonist taken three to four times a day.
What should be done next?
A. Add oral steroids
B. Add an inhaled long‐acting beta 2 agonist
C. Add a long‐acting anticholinergic
D. Add a short acting anticholinergic
E. Add a leucotriene receptor antagonist
Answer: b) Add an inhaled long‐acting beta 2 agonist.
According to the British Thoracic Society guidelines the next step would be to add an
inhaled long‐acting beta 2 agonist (LABA) and then assess the situation. If there is a
good response to LABA, this medication should be continued. If there is benefit from
LABA but control is still inadequate, LABA should be continued, and the inhaled
corticosteroids should be increased to a high dose.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 102
Respiratory Q99
A 65 year old heavy smoker is admitted with a history of increasing breathlessness. This
has been precipitated by the development of a cough with yellow purulent sputum.
The organisms that are likely to cause infective exacerbations of COPD are:
A. Streptococcus pneumoniae, Legionella pneumophilia, Mycoplasma pneumoniae
B. Streptococcus pneumoniae, Klebsiella pneumoniae, E coli
C. Streptococcus pneumoniae, Haemophilus influenzae, Moxarella catarrhalis
D. Streptococcus pneumoniae, Pseudomonas aeruginosa, Staphylococcus aureus
E. Streptococcus pneumoniae, Haemophilus influenzae, Legionella pneumophilia
Answer: c) Streptococcus pneumoniae, Haemophilus influenzae, Moxarella catarrhalis.
In infective exacerbations of COPD, Streptococcus pneumoniae and Haemophilus
influenzae, as well as Moraxella are the commonest organisms.
www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 103
Respiratory Q100
A 65 year old man has longstanding breathlessness on exertion. He has been smoking 20
cigarettes a day over a period of 30 years.
On examination, the patient is breathless with use of accessory muscles and resting
activation of the abdominal muscles. The chest is barrel shaped.
With regards to this case, which one of the following is know n to be a predictor of
mortality?
A. Spirometry
B. Fibrotic changes
C. Body Mass Index
D. Arterial blood gases
E. How many cigarettes were smoked
Answer: c) Body Mass Index.
A low body mass index is a known predictor of mortality in patients with chronic
obstructive pulmonary disease.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 104
Respiratory Q101
A 40 year man presents with shortness of breath. On admission he is unw ell and has a
respiratory rate of 32 breaths per minute. His chest is wheezy on auscultation.
Arterial blood gases show :
pO2 9.5 kPa, pCO2 3.5 kPa, pH 7.48, HCO3 25, BE +2.
What is the likely clinical scenario?
A. Lactic acidosis secondary to metformin
B. Anxiety disorder
C. Asthma attack
D. Chronic bronchitis
E. Pneumothorax
Answer: c) asthma attack.
The patient has a respiratory alkalosis (pH > 7.45) which is acute since the bicarbonate
levels are normal (22‐28). There is hypoxia and the patient is hyperventilating in
response and blowing off CO2.
This would be consistent with an asthma attack.
In an anxiety attack, hypoxia would not be present.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 105
Respiratory Q102
A 30 year old man is admitted with a history of haemoptysis, cough and dyspnoea. He
has been previously fit and has smoked 25 cigarettes a day for the last 10 years. A chest
XR shows diffuse alveolar infiltrates. He has a microcytic, hypochromic anaemia, urine
dipstick confirms haematuria and proteinuria. His lung function tests shows a normal
spirometry and a TLCO of 125% predicted.
What is the most likely diagnosis?
A. Pulmonary emboli
B. Chest trauma
C. Goodpasture's syndrome
D. Pulmonary tuberculosis
E. Pneumonia
Answer: c) Goodpasture's syndrome.
Goodpasture's syndrome is characterised by diffuse alveolar haemorrhage and
glomerulitis. Men are commonly affected with most cases occurring betw een the ages
of 20‐30 years. It is more likely to occur in smokers. The anti glomerular basement
antibody (Anti‐GBM) is present in up to 90% of the patients. Renal histology usually
shows a focal segmental necrotizing glomerulitis with crescent formation. The TLCO is
increased during active bleeding and can be used to monitor disease activity. An
increase above 30% of baseline is suggestive of an intra‐alveolar bleed.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 106
Respiratory Q103
A 60 year old man presents with sever breathlessness following an upper respiratory
tract infection.
Which of the following would support a diagnosis of acute respiratory distress syndrome
(ARDS)?
A. High protein content of pulmonary oedema fluid
B. Normal chest Xray
C. High pulmonary capillary wedge pressure
D. Increased lung compliance
E. High CO2 levels
Answer: a) High protein content of pulmonary oedema fluid.
Acute respiratory distress syndrome is characterised by hypoxaemia, reduced lung
compliance, pulmonary hypertension and pulmonary infiltrates on chest X ray. There is
damage to the capillary endothelial cell linings resulting in oedema leakage of proteins
cells into interstitial alveolar spaces.
A high pulmonary capillary wedge pressure suggests heart failure. High CO2 reflect type
II respiratory failure and are non specific.
www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 107
Respiratory Q104
A 60 year old man had a transbronchial biopsy confirming squamous cell carcinoma of
the lung.
Which of the following is a contraindication tow ards surgical resection?
A. Hypercalcaemia
B. Superior vena caval obstruction
C. Previous radiotherapy
D. Metastasis to local lymph nodes
E. Pleural effusion
Answer: b) superior vena caval obstruction.
Extensive nodal spread, distal metastases, stage IIIB or more, and superior vena caval
obstruction are contraindications tow ards surgery for lung cancer.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 108
Respiratory Q105
In which of the following have randomised controlled trials shown that long‐term oxygen
therapy (LTOT) reduces mortality?
A. Asthma
B. Chronic obstructive lung disease
C. Cryptogenic fibrosing alveolitis
D. Cystic fibrosis
E. Pulmonary sarcoidosis
Answer: B) Chronic obstructive lung disease.
There is evidence for a small reduction in mortality in patients with COPD and resting
hypoxia. Although indications for LTOT are largely based on mortality data, some studies
have also suggested improvements in other outcome measures, including depression,
cognitive function, quality of life, exercise capability, and frequency of hospitalisation.

www
Dr. K
Re
A 50
She
Wha
Ans
Cau
Rais
w.MRCPass.c
Khalid Yusuf
spiratory
0 year old w
has had no
at is the like
A. Vagus
B. Horne
C. Hiatu
D. Phren
E. Hepat
wer: d) phr
uses of phre
pneumonia
pleurisy
aortic aneu
substernal
neoplasms
thoracic su
herpes zost
vasculitis
diabetes
sed Left hem
com
f Elzohry ‐ So
y Q106
woman has
o history of
ely diagnosi
s nerve palsy
er's syndrom
s hernia
nic nerve pal
tomegaly
renic nerve
enic nerve p
a
urysm
goiter
rgery
ter infection
midiaphragm
ohag Teachin
an incident
cardiothora
is?
y
me
lsy
palsy.
palsy are :
n
m
ng Hospital ‐
tal finding o
acic surgery
‐ 2012
of raised lef
y or trauma
109
ft hemidiap
to the ches
Res
hragm on t
st.
spiratory
the CXR.
www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 110
Respiratory Q107
A 35 year old man has symptoms of wheezing and has been diagnosed as having late
onset asthma. How ever, his GP measured routine blood tests and found that he had a
creatinine of 250 umol/l.
What antibody is likely to be helpful in confirming the diagnosis?
A. Antinuclear antibody
B. Anti phospholipids antibody
C. Anti Ro antibody
D. Anti nuclear cytoplasmic antibody
E. Anti gliadin antibody
Answer: D) anti nuclear cytoplasmic antibody.
The clinical diagnosis is likely to be an ANCA positive small vessel vasculitis such as
polyarteritis nodosa, as there is pulmonary and renal involvement. Churg Strauss
syndrome should also be considered (only a small proportion of patients with Churg
Strauss have a positive ANCA)

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 111
Respiratory Q108
A 60 year old man has a long history of smoking and COPD. His resting PO2 is 7.2 kPa
and his continues to be breathless despite being on home nebulisers. He is assessed for
long term oxygen therapy (LTOT).
When is LTOT indicated?
A. PO2 <7.2 kPa
B. PO2 <7.8 kPa
C. PO2 <8 kPa
D. PO2 <8.5 kPa
E. PO2 <9 kPa
Answer: a) pO2 <7.2 kPa.
When there is polycythaemia or pulmonary hypertension, Long Term Oxygen Therapy is
indicated when pO2 < 8kPa. In uncomplicated COPD, it is indicated when pO2 < 7.2kPa

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 112
Respiratory Q109
A 60 year old woman with asthma presents with a history of acute breathlessness and
pleuritic chest pain. Her arterial blood gases show the following readings:
pH 7.35, pO2 6.8 kPa, pCO2 4 kPa, bicarbonate 25 mmol/L
Which test is most specific to acute pulmonary embolism?
A. MRI of the chest
B. CT pulmonary angiogram
C. Chest x‐ray
D. D‐Dimers
E. V/Q scan
Answer: b) CT pulmonary angiogram.
Most of the tests are helpful but a CT pulmonary angiogram remains the gold standard
diagnostic test for pulmonary embolism.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 113
Respiratory Q110
A 35 year old man presents with swelling of his lips and around the throat following
consumption of prawns. His
investigations show :
serum IgE 150 kU/L (0‐120)
C3 level is 77 mg/dL (65‐190)
C4 level is 45 mg/dL (15‐50)
Which of the following diagnosis is likely?
A. C1 esterase inhibitor deficiency
B. Allergic reaction
C. Systemic mastocytosis
D. Moon face
E. Cellulitis
Answer: b) allergic reaction.
Mildly elevated IgE concentration suggests an allergic reaction to praw ns. In
angioneurotic oedema due to C1 esterase inhibitor deficiency, a low C4 with normal C3
level is seen (C2 is also low but not commonly measured).

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 114
Respiratory Q111
A 40 year old man has with a 2 year history of increasing shortness of breath. This is
worse with exertion e.g. climbing the stairs at home and is even slightly so at rest. He is
a non‐smoker.
On examination, his pulse is 95 beats/min and his blood pressure is 140/95 mmHg. He
has finger clubbing and a crackling noise at the end of inspiration over the bases of the
lungs. There was no ankle oedema Lung function tests show :
FVC 2.5 l (predicted 3.2 )
FEV1 2.1 l (predicted 2.4)
FEV1 % 76% (predicted 75%)
Diffusing Capacity: Gas Transfer Factor for carbon monoxide: DLCO 17
ml/min/mmHg (predicted) 25
Which one of the following diagnosis is likely?
A. Aspergilloma
B. Guillain‐Barre syndrome
C. Cryptogenic fibrosing alveolitis
D. Asthma
E. Congestive cardiac failure
Answer: c) cryptogenic fibrosing alveolitis.
A reduced FVC, with normal FEV1, FEV1% and PEF usually indicates restriction of lung
volume . KCO (transfer factor) is also reduced in fibrotic lung disease, as in this case. The
additional findings of inspirational crackles and clubbing suggests the diagnosis of
cryptogenic fibrosing alveolitis.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 115
Respiratory Q112
A 60 year old man has severe COPD requiring home nebulisers and home oxygen. He is
admitted with an infective exacerbation.
Which of the following results would be expected on the arterial blood gases?
A. PH 7.25 paCO2 7 paO2 7.5 HCO3 30
B. PH 7.10 paCO2 7 paO2 4 HCO3 24
C. PH 7.30 paCO2 4 paO2 8.5 HCO3 30
D. PH 7.40 paCO2 4 paO2 4 HCO3 22
E. PH 7.45 paCO2 3 paO2 12 HCO3 24
Answer: a) pH 7.25 paCO2 7 paO2 7.5 HCO3 30.
A long standing COPD patient would be expected to have a high bicarbonate. However
this patient is unwell with type II respiratory failure (high CO2) and hence has
uncompensated respiratory acidosis.

www
Dr. K
Re
A 60
and
Che
bac
Whi
tube
Ans
Slat
mac
Silic
w.MRCPass.c
Khalid Yusuf
spiratory
0 year old m
breathless
est XR show
illi.
ich of the
erculosis?
A. Beryl
B. Cadm
C. Coal
D. Silica
E. House
wer: d) silic
te workers,
crophage fu
cosis
com
f Elzohry ‐ So
y Q113
miner has b
ness.
ws diffuse in
following
lium
mium
e dust
ca.
stonemas
unction, and
ohag Teachin
been in the
nterstitial sh
dusts is
ons and m
d in particul
ng Hospital ‐
occupation
hadowing. A
most likely
miners are e
lar, predisp
‐ 2012
n for 20 yea
A sputum s
y to have
exposed to
oses to TB i
116
ars. He pres
ample is po
predispose
o silica dus
infection.
Res
sents with a
ositive for a
ed the pat
t. Silicosis
spiratory
a cough
acid fast
tient to
impairs

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 117
Respiratory Q114
A 34‐year‐old woman presented with a dry cough, thorax constriction, and generalised
weakness. During the preceding 5 months, she had experienced these dry cough
episodes tw ice a week. A lung function test showed a restriction of the vital capacity
(71% of the adjusted reference value), and the diffusion capacity was also reduced (66
to 68%).
Bronchoalveolar lavage specimens were obtained, the lymphocytes were increased up
to 41% (norm, <10%), and neutrophils were increased up to 6% (norm, <2%) with a
normal total cell count.
What is the likely diagnosis?
A. Asthma
B. Pulmonary embolus
C. Tuberculosis
D. Extrinsic allergic alveolitis
E. Alpha 1 antitrypsin deficiency
Answer: d) extrinsic allergic alveolitis.
Extrinsic Allergic Alveolitis is a type III or type IV response. There is no eosinophilia. IgG
and lymphocytes are involved in immune response. Antigens of micropolyspora faeni
and thermoactinomyces are 0.5‐5 microns . These antigens which may be detected as
serum precipitins.
The acute form takes about 6 hours for sensitisation to the inhaled antigen. The chronic
form may take weeks.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 118
Respiratory Q115
A 65 year old patient with COPD is on maximal treatment.
Which one of the following is likely to prevent further disease progression?
A. Steroids
B. Beta agonist inhalers
C. Stopping smoking
D. Tiotropium
E. Home oxygen
Answer: C) stopping smoking.
In COPD, discontinuation of smoking is the only features which has been shown to
reduce disease progression.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 119
Respiratory Q116
A 60 year old male smoker has emphysema.
His lung function tests show :
FEV1 is 0.5 (20% predicted)
FVC is 2.2 (61% predicted)
FEV1:FVC ratio of 26%
His arterial blood gases show a PO2 of 7.5 and 7.2 on two separate occasions. He is
mildly breathless at rest, but severely breathless on exertion.
What is the best measure of his respiratory function?
A. TLCO
B. FEV1
C. FVC
D. KCO
E. TLC
Answer: b) FEV1.
The breathlessness worsens considerably without much change in oxygen tension,
suggesting that the cause of his dyspnoea is hyperinflation of his chest which worsens
on exertion.
Severity of emphysema is defined by the British Thoracic Society (BTS) in relation to
FEV1, not FEV1:FVC ratio. Mild is 60‐80% predicted; moderate 40‐60% and severe <40%.

www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 120
Respiratory Q117
A 40 year old lady was admitted to hospital with fevers and cough productive of
sputum.
Chest X‐ray shows diffuse patchy consolidation around the left lung. She has had a flu
like illnes 4 weeks ago, and has a past medical history of asthma. She also smokes 10
cigarettes a day.
Which organism is likely to be responsible?
A. Mycoplasma
B. Pseudomonas
C. Klebsiella
D. Staphylococcus
E. Tuberculosis
Answer: d) staphylococcus.
Following a viral infection, patients are predisposed to staphylococcal infection. The
chest XR changes suggest staphlococcus rather than streptococcus (which would cause
lobar consolidation).

www
Dr. K
Re
A 50
apy
His
mm
(0.8
Che
Wha
Ans
Sarc
hila
effu
Bila
w.MRCPass.c
Khalid Yusuf
spiratory
0 year old m
rexial on ad
blood sho
mol/l, potass
8‐1.4)mmol/
est X ray sho
at is the like
A. Extrin
B. Tuber
C. Sarco
D. Allerg
E. Leiom
wer: c) sarc
coidosis can
r lymphade
usions and n
teral hilar ly
com
f Elzohry ‐ So
y Q118
man presen
dmission.
w ESR 60
sium 4.1 mm
/l.
ows bilatera
ely diagnosi
nsic allergic a
rculosis
idosis
gic bronchop
myoma
coidosis.
n cause ma
enopathy,
nodules.
ymphadeno
ohag Teachin
ts with a 3
mm/hr, ur
mol/l, corre
al hilar lymp
is?
alveolitis
pulmonary as
ny changes
diffuse par
opathy in sa
ng Hospital ‐
month hist
rea 7 μmo
ected calciu
phadenopat
spergillosis
s on the CXR
renchymal
arcoidosis
‐ 2012
ory of coug
l/l, creatin
m 2.75 (2.2
thy and egg
R. Among th
changes, e
121
gh and brea
ine 100 μm
2‐2.7) mmo
gshell calcifi
hese are un
eggshell ca
Res
thlessness.
mol/l, sodiu
l/l, phospha
cation.
nilateral or b
alcification,
spiratory
He was
um 137
ate 0.82
bilateral
pleural
www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 122
Respiratory Q119
A 40 year old woman presents with breathlessness, cough and fever. On examination,
she has basal crackles in the lung fields. Circulating precipitans to Micropolyspora faeni
are positive.
Which of the following is the most likely diagnosis?
A. Pigeon fanciers' lung
B. Allergic Bronchopulmonary Aspergillosis
C. Farmers' lung
D. PCP infection
E. Pulmonary fibrosis
Answer: c) Farmers' lung.
Farmer's lung is the most common type of hypersensitivity pneumonitis.
Hypersensitivity pneumonitis, also known as extrinsic allergic alveolitis, is associated
with intense or repeated exposure to inhaled biologic dusts. The classic presentation of
farmer's lung results from inhalational exposure to thermophilic Actinomyces species
and occasionally from exposure to various Aspergillus species.
Acute farmer's lung develops after large exposure to moldy hay or contaminated
compost. Symptoms often spontaneously resolve within 12 hours to days if antigen
exposure is eliminated or avoided. It manifests as new onset of fever, chills,
nonproductive cough, chest tightness, dyspnea, headache, and malaise.
www.MRCPass.com Respiratory
Dr. Khalid Yusuf Elzohry ‐ Sohag Teaching Hospital ‐ 2012 123
Respiratory Q120
A 50 year old meat factory worker has been unw ell with fever, cough, sweats and
lethargy. On examination, he had a purpuric rash and hepatosplenomegaly.
What is the likely diagnosis?
A. Pulmonary embolism
B. Respiratory syncytial viral pneumonia
C. Streptococcal pneumonia
D. Q fever pneumonia
E. Aspergilloma
Answer: d) Q fever pneumonia.
Q fever is due to Coxiella burnetii and is acquired via animal contact. It can occur in
outbreaks in farming communities and in abbatoirs. Treatment is with prolonged
courses of tetracyclines. Rarely infection can be persistent leading to chronic symptoms
including fatigue, malaise and sweats. Hepatitis, hepatosplenomegaly, maculopapular
rash and endocarditis are associated.

www
Dr. K
Re
A 5
had
felt
che
prot
The
Ans
The
Exa
>30
Emp
w.MRCPass.c
Khalid Yusuf
spiratory
0 year old
suffered a
better init
st radiogra
tein of 42 g
most likely
A. Collap
B. Empy
C. Serou
D. Fibro
E. Tuber
wer: b) Emp
e likely cau
mination o
0g would be
pyema (air f
com
f Elzohry ‐ So
y Q121
woman, is
chest infec
tially, but is
ph shows
g and pH of
y diagnosis i
pse of the le
yema
us pleural eff
tic lung disea
rculosis
pyema.
use is a p
f a pleural
consistent
fluid level)
ohag Teachin
admitted w
ction for wh
s now getti
a left sided
7.0.
is:
ft lung
fusion
ase
pneumonia
aspirate (m
with an exu
ng Hospital ‐
with malais
hich she wa
ing worse,
d pleural e
which has
microscopy
udate and a
‐ 2012
se and feve
as given a c
complainin
ffusion. An
s not reso
for organis
a pH of < 7.2
124
er. Four we
ourse of or
ng of interm
n aspirate s
olved, lead
sms, cultur
2 is suggest
Res
eks previou
ral amoxyci
mittent feve
shows fluid
ing to em
re). A prote
tive of infec
spiratory
usly she
llin. She
ers. Her
with a
mpyema.
ein level
ction.