Embed Size (px)
Citation preview

i Fakultetit të Mjekësisë Dentare
STOMATOLOGJIKE
Vellimi 14, Nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016
ISSN 2308-5290

Revista Stomatologjike Shqiptare2
Redaksia e Revistës Stomatologjike Shqiptare ju ofron mundësinë të reklamoni produktet tuaja dentare e farmaceutike në faqet e revistës. Gjithashtu ju mund të reklamoni apo të njoftoni për zhvillimin e kurseve, seminareve, konferencave të ndryshme, apo për aktivitete e shërbime të tjera të lidhura me stomatologjinë.
Reklamimi mund të kryhet në një faqe të plotë reviste, apo në trajtën e suplementit të revistës. Redaksia ofron gjithashtu mundësinë që të sponsorizoni abonimin 1-vjeçar në Revistë (për më shumë informacion shih seksionin Abonimi) për institucionin tuaj, në mënyrë që punonjësit tuaj të informohen mbi të rejat më të fundit në stomatologji, duke përmirësuar kështu edhe cilësinë e punës së tyre.
Përse të zgjidhni Revistën Stomatologjike Shqiptare për reklamimin e biznesit apo aktiviteteve tuaja?• Sepse Revista Stomatologjike Shqiptare është një burim prestigjioz informacioni,
e vetmja e këtij lloji në Shqipëri, e vlerësuar dhe e lexuar nga një numër i madh stomatologësh në mbarë vendin.
Reklamimi në Revistën Stomatologjike Shqiptare është mënyra më efi kase për të arritur tek klienti juaj.
Për më tepër informacion, ju lutem kontaktoni me Redaksinë e Revistës Stomatologjike Shqiptare në nr. e telefonit: +355 (0)4 2371589, ose në adresën e e-mail: [email protected]
Redaksia e Revistës Stomatologjike Shqiptare ju ofron mundësinë e abonimit 1-vjeçar.Abonimi mund të kryhet individual apo institucional, sipas tarifave të mëposhtme:
Tarifa
Abonim 1-vjeçar për individë 1000 lekë (përfshihet edhe tarifa e postimit)
Abonim 1-vjeçar për institucione 2000 lekë (përfshihet edhe tarifa e postimit)
Anëtarët e Shoqatës Stomatologjike Shqiptare që paguajnë rregu-llisht kuotizacionin e përcaktuar, mund të tërheqin revistat pa pagesë pranë Shoqatës.
Për më tepër informacion, ju lutem kontaktoni me Redaksinë e Revistës Stomatologjike Shqiptarenë nr. e telefonit: +355 (0)42371589,ose në adresën e e-mail: [email protected]
© Revista Stomatologjike Shqiptare
Design: Sokrat XHAVARA
Çmimi 1000 Lekë
Me Revistën Stomatologjike Shqiptare bashkëpunojnë:
Reklamimi
Abonimi
Shoqata Dentare ShqiptareShoqata Kirurgjikale Oromaxillo-Faciale
Shoqata e Ortodontëve ShqiptarëShoqata Shqiptare e Pedodontisë dhe Profi laksisë
Universiteti i Prishtinës Departamenti i StomatologjisëShoqëria Stomatologjike Apolonia

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 3
Revista Stomatologjike Shqiptare është revista zyrtare e Fakultetit të Mjekësisë Dentare, Universiteti i Mjekësisë, Tiranë, Shqipëri. Revista botohet në gjuhën shqipe dhe angleze, dy herë në vit.
Revista Stomatologjike Shqiptare ka për qëllim të botojë materiale me cilësi të lartë shkencore dhe klinike në të gjitha fushat e Stomatologjisë. Materialet e paraqitura për botim shqyrtohen nga redaksia e Revistës. Ajo synon gjithashtu të informojë mjekët stomatologë mbi aktivitete dhe të reja, si dhe të ofrojë një mundësi debati mbi aspekte të ndryshme të stomatologjisë.
The Albanian Stomatological Journal is the offi cial Journal of the Faculty of Dental Medicin at the Medical University of Tirana, Albania, published twice a year in Albanian language.
It is a peer-reviewed journal aiming to publish high quality material, both clinical and scientifi c, on all aspects of Dentistry. In addition it provides a mean of information for dentists about news and events and also a forum for exchange of opinions on all aspects of dentistry, including education issues.
Botimi i Revistës Stomatologjike Shqiptare mundësohet nga Shoqata Dentare Shqiptare
Albanian Stomatological JournalRevista Stomatologjike Shqiptare
Executive Editorial Board
Editor In-ChiefProf. Assoc. Edit Xhajanka
Managing EditorsProf. Xhina Mulo
Prof. Florian BEUERProf. Vincenzo CAMPANELLAProf. Ramazan ISUFIProf. Rozarka BUDINAProf. Assoc. Edit XHAJANKAProf. Assoc. Dorjan HYSIProf. Assoc. Agron METO D.M.Sc Fatmir LELAD.M.Sc Gerta KAÇANID.M. Sc. Kreshnik KERAJMsc Andis QENDROPh.D. Prunela POLIÇI
Lorena Qafmolla
D.M.Sc Gerta Kaçani
Manuscript editing
Scientifi c Editorial BoardProf. Peter POSPIECHProf. Giovanni MANES GRAVINAProf. Lindita XHEMNICAProf. Fejzi KERAJProf. Assoc. Besnik GAVAZIProf. Assoc. Etleva QELIProf. Assoc. Gloria STAKAD.M.Sc. Alketa QAFMOLLAD.M.Sc. Enida PETROD.M.Sc. Silvana BARAD.M.Sc Edlira DEDAPh.D. Ali GASHI
Ph.D. Philipp EBERLProf. Xhina MULOProf. Adem ALUSHIProf. Ruzhdie QAFMOLLAProf. Assoc. Merita BARDHOSHIProf. Assoc. Çeliana TOTI D.M.Sc . Koço GJILOD.M.Sc. Rozela XHEMNICAD.M.Sc Aldo VANGJELIMsc. Esat BARDHOSHIPh.D. Erda QORRIPh.D. Nedim KASAMI
Zyra e redaksisëEditorial Offi ceAdresa: Fakultetit të Mjekësisë Dentare, Universiteti i Mjekësisë, Rr. Dibrës, 371, Tiranë, Shqipëri.Address: Faculty of Dental Medicin at the Medical University of Tirana, Rr. Dibrës, 371, Tirana, Albania.e-mail: [email protected]

Revista Stomatologjike Shqiptare4
REVISTA STOMATOLOGJIKE SHQIPTAREVëllimi 14 Nr. 1 (54) Mars 2016
Vëllimi 14 Nr. 2 (55) Dhjetor 2016
Përmbajtja
Përmbajtja
Udhëzime për autorët 174
NDERI I STOMATOLOGJISE SHQIPTARE 6Trajtimi ortodontik i rrugës ajrore 8Dr. Andri Çabeli, Dr. Edlira Subashi, Dr. Rudin Kusi, Dr. Egi Mulo
Menaxhimi i Granulomes Piogjene me Diode Lazer 980 nm 22Prof. Assoc. Merita Bardhoshi1, Prof. Assoc. Edit Xhajanka1, Dr. Neada Hysenaj2, Prof. Assoc. Agron Meto3, Dr. Aida Meto3
Rikthimi i estetikës dentare nepermjet restaurimeve konservative 29D.M.Sc. Koço Gjilo, Dr. Dasaret Hajdini
Krahasimi i metodës së zakonshme të polimerizimit kundrejt metodës së injektimit me presion SR-Ivocap 41Prof. Assoc. Edit Xhajanka, D.M.Sc Koço Gjilo, Dr. Neada Hysenaj, Prof. Assoc. Merita Bardhoshi, D.M.Sc. Gerta Kaçani
Ndërlikimet endodontike në dhëmbët shtyllë vital 57Prof. Dr. Pavli Kongo, Anis Thodhorjani
Hypomineralizimi Molar-Inciziv 63Prof. Assoc. Etleva Droboniku (Qeli)1, Prof. Assoc. Dorjan Hysi1, Dr. Ina Droboniku2, Prof. Assoc. Çeliana Toti1, D.M.Sc. Enida Petro1
Metoda alternative nga titanium për reabilitimin implanto protetik : PEEK Prezantim Rasti 73Ph.D Erda Qorri1, Msc Fabio de Propris1, Msc Majlinda Kola1, Prof. Assoc Edit Xhajanka2, Prof. Assoc Mertia Bardhoshi2
Trajtimi pa ekstraksione në ortodonci me anë të briketave self-ligating. Raste Klinike 81Msc Manjola Gusho, D.M.Sc. Fatmir Lela
Avulsioni i dhëmbit incisiv central permanent dhe trajtimi i pasojave të tij. Prezantim rasti 87M.Sc. Ersela Alikaj1, 2, Prof. Dr. Xhina Mulo1, Dr. Alda Gjoni2
Odontoma e mandibules. Prezantim rasti 97Ph.D. Nedim Kasami, Dr. Vladimir Popvski
Menaxhimi i kafshimit të kryqëzuar anterior me aparate të lëvizshme. Prezantim rasti 107D.M.Sc. Rozela Xhemnica*; M.D-O.M.F.S. Milton Rroço; Prof. Dr. Lindita Xhemnica; Prof. Assoc. Çeliana Toti; Rudin Kusi
Shfrytëzimi i kurorës së integrar me kultin, si teknikë për suprastrukturën e implanteve të shkurtra Bicon. Prezantim Rasti 115Msc. Ledia Gaxho(1), Prof. Dr Ramazan Isufi (
Niveli i mërkurit në pështymë i çliruar nga mbushjet me amalgam 129D.M.Sc. Edlira Dedaj1, Prof. Rozarka Budina2, Dr. Henri Dedaj3
Çrregullimet muskulo-skeletale të dentistëve 143Rudina Berani, Prof. Rozarka Budina
Vendosje e implantit me udhëzues kirurgjik dhe ngarkimi i menjëhershëm i tij. Rast Klinik 155Dr. Fisnik Mekaj1, Dr. Eni Tutulaku2
Roli i etikës në Stomatologji 163Dr. Nikoll Deda1, Dr. Erisa Bllakaj2
NEKROLOGJI Prof. Dr. Dhori Pojani 170NEKROLOGJI Dr. Shk. Çerçiz Mingomataj 172

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 5
Table of Contents
Table of Contents
Volume 14 No. 1 (54) March 2016
Volume 14 No. 2 (55) December 2016
ALBANIAN STOMATOLOGICAL JOURNAL
Orthodontic treatment ortodontik of airway 14Dr. Andri Çabeli, Dr. Edlira Subashi, , Dr. Rudin Kusi, Dr. Egi Mulo
The management of pyogenic granuloma with the 980 nm diode laser 25Prof. Assoc. Merita Bardhoshi1, Prof. Assoc. Edit Xhajanka1, Dr. Neada Hysenaj2, Prof. Assoc. Agron Meto3, Dr. Aida Meto3
Dental Aesthetic rehabilitation via conservative restorations 35D.M.Sc. Koço Gjilo, Dr. Dasaret Hajdini
The comparison between the conventional plasmas polymerization and SR-Ivocap method 49Prof. Assoc. Edit Xhajanka, D.M.Sc Koço Gjilo, Dr. Neada Hysenaj, Prof. Assoc. Merita Bardhoshi, D.M.Sc. Gerta Kaçani
Endodontic complications of vital abutment teeth 60Prof. Dr. Pavli Kongo, Anis Thodhorjani
Molar Incisor Hypomineralization 68Prof. Assoc. Etleva Droboniku (Qeli)1, Prof. Assoc. Dorjan Hysi1, Dr. Ina Droboniku2, Prof. Assoc. Çeliana Toti1, D.M.Sc. Enida Petro1
Prosthetic implant rehabilitation with materials alternative to Titanium: PEEK. Case Report 77Ph.D Erda Qorri1, Msc Fabio de Propris1, Msc Majlinda Kola1, Prof. Assoc Edit Xhajanka2, Prof. Assoc Mertia Bardhoshi2
Non-extraction treatment in orthodontic using self-ligating braces. Case report 84Msc Manjola Gusho, D.M.Sc. Fatmir Lela
The sequelae of avulsed permanent central incisive and its treatment. Case report 92M.Sc. Ersela Alikaj1, 2, Prof. Dr. Xhina Mulo1, Dr. Alda Gjoni2
Odontoma of the Mandible. Case Report 102Ph.D. Nedim Kasami, Dr. Vladimir Popvski
Management of anterior dental crossbite with removable appliances. Case Report 111D.M.Sc. Rozela Xhemnica*; M.D-O.M.F.S. Milton Rroço; Prof. Dr. Lindita Xhemnica; Prof. Assoc. Çeliana Toti; Rudin Kusi
Use of Integrated Abutment Crown,a techinque for the load of Bicon short implants. Case Report 122Msc. Ledia Gaxho(1), Prof. Dr Ramazan Isufi (
The mercury levels released in saliva from amalgam fi llings 136D.M.Sc. Edlira Dedaj1, Prof. Rozarka Budina2, Dr. Henri Dedaj3
Musculo skeletal disorders in dentists 149Rudina Berani DMD, Prof. Rozarka Budina
Implant Placement with Surgical Guide and Immediate Placement of the Provisional Crown. A Case Report 159Dr. Fisnik Mekaj1, Dr. Eni Tutulaku2
The Role of Ethics in Dentistry 166Dr. Nikoll Deda1, Dr. Erisa Bllakaj2

Revista Stomatologjike Shqiptare6
NDERI I STOMATOLOGJISE SHQIPTARE
Stomatologjia, si çdo shkencë e mjekësisë ka ecurine e saj këto dhjetëvjeçarët e fundit.
Hapi cilësor i këtij zhvillimi është vëzhguar në lëmin e Kirurgjisë Oromaxilo Faciale, Ortodoncise, Protetikës Endodontisë etj. Nga një zhvillim i tillë kanë përfi tuar jo vetëm mësimdhënia por edhe popullata në tërësi. Kjo i dedikohet armatës së stomatologëve të cilët nga dita në ditë janë të azhornuar me të rejat më të fundit të kësaj fushe.
Duke e parë nga ky këndvështrim Urdhri i Stomato-
logut Shqiptar dhe Asambleja Kombëtare akordoi Ti-tullin “Nderi i Stomatologjisë Shqiptare“ disa prej tyre:
Prof. Dr. Ruzhdie Qafmolla.Me motivacionin: Për kontribut të shquar në
zhvillimet e Stomatologjisë Shqiptare si pedagoge, drejtuese shkencore, Kryetare e Shoqatës Dentare Shqiptare dhe Dekane, Themeluese e Fakultetit të Mjekësisë Dentare.
Prof. Dr. Ruzhdie Qafmolla
Prof. Dr. Rozarka Budina

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 7
Prof. Assoc. Nazmi Koçi.Për kontribut të shquar në zhvillimet e
Stomatologjisë Shqiptare si drejtues, pedagog dhe mjek i talentuar në specialitetin e Ortopedisë Stomatologjike.
Prof. Assoc. Gafurr Shtino.Për kontribut të shquar në zhvillimet e
Stomatologjisë Shqiptare, pedagog dhe specialist i shquar në fushën e Kirurgjisë OMF.
D.SH.M. Abdulla Bilali pas vdekjes.Për kontribut të shquar të Stomatologjisë Shqiptare
në fushën e Kirurgjisë OMF.
D.SH.M. Pjetër Pepa pas vdekjes.Për kontribut të shquar në fushën e shkencës dhe
të politikës.
Prof. Dr. Rozarka Budina.Për kontribut të shquar në zhvillimet e
Stomatologjisë Shqiptare si drejtuese, pedagoge, Kryetare e Shoqatës Dentare Shqiptare dhe mjeke e talentuar në specialitetin e Terapisë Stomatologjike.
Prof. Dr. Ramazan Isufi .Për kontribut të shquar në zhvillimet e
Stomatologjisë Shqiptare, pedagog dhe specialist i shquar në fushën e Kirurgjisë OMF.Prof. Dr. Ramazan Isufi
Prof. Assoc. Gafurr Shtino Prof. Assoc. Nazmi Koçi
Të afërm të D.SH.M Abdulla Bilali dhe D.SH.M Pjetër Pepa

Revista Stomatologjike Shqiptare8
AbstraktRruga ajrore normale është një nga faktorët e rëndësishëm për rritjen normale të strukturave kraniofaciale. Funksioni nazorespirator dhe lidhja e tij me rritjen kraniofaciale është me interes të madh jo vetëm për pediatrët, por edhe për ortodontët, otorinolaringologët, patologët e të folurit dhe anëtarë të tjerë të komunitetit të kujdesit shëndetësor. Rritja dhe funksioni i kaviteteve nazale, të nazofarinksit dhe të orofarinksit janë të lidhura ngushtë me rritjen normale të kafkës. Për shkak të marrëdhënieve të ngushta në mes të faringsit dhe strukturave dentofaciale, një ndërveprim reciprok pritet të ndodhë në mes të strukturave të faringut dhe modelit dentofacial dhe prandaj kjo justifi kon interesin ortodontik.
Diagnoza më e rëndësishme që mungon është rruga ajrore. Megjithëse, frymëmarrja është veprimi më i rëndësishëm i qenieve humane për të jetuar, ne harrojmë të kontrollojmë rrugën ajrore gjatë diagnozës së pacientëve ortodontikë.
Qëllimi i ketij artikulli është vënia në fokusin e ortodoncisë të menaxhimit edhe të rrugës ajrore duke patur ne konsideratë: konseguencat e vështirësisë së frymëmarrjes normale dhe trajtimin interdisiplinar e prevenimin.
FJALËT KYÇE:
rruga e ajrit,
malokluzioni,
trajtimi
Dr. Andri Çabeli1, Dr. Edlira Subashi2, Dr. Rudin Kusi2, Dr. Egi Mulo2
Trajtimi ortodontik i rrugës ajrore
1Universiteti Aldent, 2Klinikë dentare private
HyrjeFrymëmarrja me gojë ka qenë një temë e diskutueshme
në patogjenezën e disa malokluzioneve dentare. Një lidhje e tillë e dëmshme u evidentua 130 vjet më parë nga një artist i njohur amerikan, George Catlin, në librin e tij të titulluar “Keqrespirimi ose frymëmarrja e jetës”. Libri i Catlin më pas u rititullua “Mbyllni gojën dhe shpëtoni jetën tuaj “. Një kopje e këtij libri u soll në vëmendjen e komunitetit dentar nga Dr Edward H. Angle në 1925. Ai ribotoi librin e George Catlin, me titullin e tij origjinal. Në parathënie, Dr Angle referuar artistit deklaronte: “ Z. Catlin ështe plotësisht i saktë në besimin e tij, se disa forma të malokluzionit të dhëmbëve dhe shëmtimi i fytyrës janë për shkak të frymëmarrjes orale dhe, pa dyshim, ai është një nga të parët, në mos i pari, në këtë vend që ka drejtuar vëmendjen në këtë fakt”. Angle besonte që komplikimet e frymëmarrjes orale ishin ndër faktorët kryesorë që kontribuojnë në etiologjinë e malokluzioneve dentare. Ai besonte kaq shumë sa përfshiu një otolaringolog me kohë të plotë, Dr James Ross Reed, në stafi n e tij. Frymëmarrja me gojë është studjuar edhe nga shumë shkencëtarë të tjerë, si etiologji e mundshme për disa malokluzione dentare (1,2). Hulumtimi në këtë fushë është i shtrirë, por në një masë të madhe në kundërshtim. Kështu, marrëdhëniet shkak - pasojë midis frymëmarrjes së varfër dhe malokluzioneve duhet të shqyrtohet me kujdes rast pas rasti (3,4,5). Pavarësisht nga përfundimet e studiuesve të ndryshëm, një teori mbetet e zakonshme - që pengesat e rruges ajrore dhe malokluzioni janë të lidhura. Prandaj, profesionistët dentarë duhet të përfshijnë vëzhgimin dhe monitorimin e rrugës së sipërme ajrore si një pjesë integrale të ekzaminimit, duke fi lluar që në vitet e para pas lindjes.
Qëllimi përfundimtar duhet të jetë inkurajimi i zhvillimit kraniofacial, për të maksimalizuar potencialin e rrugës së sipërme ajrore gjatë gjithë jetës së individit (6, 7, 8).
QëllimiQëllimi i këtij artikulli është për të nxjerrë në pah aftësitë
dhe mjetet që ndihmojnë klinicistin në identifi kimin e pengesave të rrugës ajrore, për të përmirësuar diagnozën e pacientëve ortodontikë dhe trajtimin e malokuzioneve të lidhura me këtë problematikë.
Materiali & MetodaMetodologjia e përdorur në këtë artikull përbëhet
nga paraqitja e 2 rasteve klinike, të perzgjedhura, me problematikën e frymëmarrjes orale dhe anomalive dento-skeletale.
Për pacientët tanë shënimet e plota diagnostike konsistuan në:
Radiografi panoramike Fotografi modelesh dhe një ekzaminim i plotë
klinik objektiv dhe subjektiv,Analiza cefalometrike.
Ekzaminimi cefalometrik Diametri Faringeal Superior matet nga shtrirja
posteriore e palatumit të butë – me pikën më të afërt të murit faringeal. Nazofarinksi mesatar është 17,4 mm (15-20 mm) i gjërë.
Diametri Faringeal Superior është i zvogëluar në (fi g. 1):
Retruzionin maksilar Hipertrofi të adenoideve, etj.

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 9
Fig. 1: Diametri Faringeal Superior
Diametri Faringeal Inferior matet nga pika e ndërprerjes së bordit posterior të gjuhës dhe bordit inferior të mandibulës – me pikën më të afërt të murit posterior faringeal. Matja mesatare është 13,5 mm (11-14 mm) i gjërë (fi g. 2).
Gjërësia zvogëlohet në:Retruzioni i mandibulës Rotacioni posterior i mandibulës Mandibul e madhe, etj.
Fig. 2: Diametri Faringeal Inferior
Fig. 3: Analiza e pozicionit të gjuhës
Gjithashtu, në cefalometri shihet edhe postura e gjuhës. Në subjektet frymëmarrës oral, gjuha
pozicionohet poshtë, ndryshe nga pozicioni i gjuhës lart në palatum në subjektet me frymëmarrje nazale (fi g. 3).
Rasti klinik 1 është një pacient 10 vjeç, i cili u paraqit në klinikë me shqetësimin se dhëmbët e sipërm ishin të dalë përpara. Gjatë pyetjes, nëna referoj se djali gerhiste natën dhe ankohej edhe për dhimbje kraharori. Në ekzaminimin ekstraoral pacienti paraqiste inkompetencë labiale dhe qëndrim me gojë hapur.
Diagnoza e marrë mbas ekzaminimit klinik dhe radiologjik ishte:
Nofulla e ngushtë (fi g. 4) është si pasojë e faktit se frymëmarrësit orale mbajnë buzët e tyre të ndara dhe pozicioni i gjuhës është poshtë. Imbalanci në mes të presionit të gjuhës dhe muskujve të faqeve, rezulton në atë që muskujt kompresojnë procesin alveolar në regjionin e premolarëve. Njëkohësisht, nofulla e poshtme posturohet mbrapa. Këto veprime të njëkohshme janë quajtur teoria e kompresionit (9, 10, 11).
Tek pacienti u aplikua aparat funksional (twin-block), pa bërë ekstraksione.
Twin-block është një aparat shumë efi kas në korrigjimin e malokluzioneve të klasës së II-të, me retrusion mandibular. Studimet e mëparshme kanë treguar se TB është efektive në ripozicionimin përpara të mandibulës dhe në këtë mënyrë arrihet një profi l më harmonik i fytyrës (12). Ndryshimet e rrugës ajrore në pacientët me OSA janë matur pas trajtimit dhe kanë treguar një zgjerim të konsiderueshëm në volumin e faringut.
Fig. 4: Modelet dhe goja para trajtimit

Revista Stomatologjike Shqiptare10
Mbas një periudhe 6 mujore, me avancimin e mandibulës, pacientit ju hoq aparati i poshtëem, ndërkohë që aparatit të sipërm ju hoqën sipërfaqet distale dhe ju shtua një plan i inklinuar anterior për të ruajtur pozicionin përpara të mandibulës (fi g. 5).
Fig. 5: Aparati twin-block
Fig. 6: Pamjet para dhe mbas trajtimit ortodontik
Në fi gurën 6 shihen rezultatet pas trajtimit 14 mujor. Është arritur raporti i klasës së I-rë dhe harkada superiore është zgjeruar mjaftueshëm.
Pas trajtimit ortodontik të këtij djali 10 vjeçar mund të shohim se jo vetëm që është përmirësuar paraqitja e fytyrës së tij, por është përmirësuar në mënyrë dramatike rruga ajrore - të gjitha jo me kirurgji. Cefalometritë para dhe pas trajtimit (fi g. 7), tregojnë zgjerimin e rrugës ajrore dhe përmirësimin për të marrë frymë lirisht të këtij djali.
Para Pas

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 11
Fig. 7: Pamjet ekstraorale dhe cefalometrike para dhe mbas trajtimit ortodontik
Faza 1 e planit të trajtimit ishte aplikimi i trainer, mbas heqjes së adenoideve (fi g. 9).
Fig. 9: Aplikdimi i trainer
Aparatet e ndryshme të sistemit trajner veprojnë duke përmirësuar veprimtarinë muskulare të muskujve mastikatore dhe faciale, si dhe duke ri-edukuar gjuhën për t’u vendosur në një pozicion më fi ziologjik gjatë qetësisë. Duke ruajtur mandibulën në një pozicion përpara gjatë një periudhe prej përafërsisht 10 orë në ditë, ka një ndryshim të posturës mandibulare, e cila përmirëson aspektin sagital në pacientët me disto-okluzion. Përmes veprimit të tyre në muskujt e faqeve dhe buzëve, sistemi trajner çon ne ndryshime transversale të harqeve dentare. Së fundi, nëpërmjet veprimit të tyre në muskujt mbyllës të gojës dhe në posturën e gjuhës, këto aparate mund të përmirësojnë aspektin vertikal në pacientët si me kafshim të thellë ose të hapur. Këto efekte u panë edhe mbas fazës 1 tek pacienti ynë (fi g. 10).
Rasti klinik 2: Në vijim është një studim rasti i një pacienti 8 vjeçar, i cili u paraqit për një vlerësim ortodontik me një shqetësim kryesor “duam një buzëqeshje të bukur”. Gjatë intervistës fi llestare u zbulua se pacienti ishte një frymëmarrës kronik me gojë, dhe një gerhitës i rregullt. Prindërit gjithashtu raportuan një prirje për të qenë si i fj etur gjatë ditës, me pavëmendje në shkollë dhe jo i interesuar në sport. Në kohën e ekzaminimit, pacienti duket që merr frymë vetëm me gojë. Buzët e tij ishin inkompetente. U kryhen fotot përkatëse (fi gura 8) dhe studimi cefalometrik tregoi një rrugë ajrore të ngushtë, me hiperplazi adenoide që cënonte hapësirën ajrore të faringut. Diagnoza e marrë mbas ekzaminimit klinik dhe radiologjik ishte:
Fig. 8: Diagnoza dhe goja para trajtimit
Para Pas

Revista Stomatologjike Shqiptare12
Fig. 10: Pas fazës së parë
12 muaj mbas fazës 1, u aplikua aparati fi ks. Figura 11 tregon ndryshimet e fytyrës para dhe pas trajtimit, ndryshimet në hapesirën faringeale dhe rregullimin e pozicioneve të kaninëve ektopike. Mbas trajtimit, nëna raportoi një përmirësim dramatik në shëndetin e përgjithshëm të djalit, një reduktim në gjendjen e fj etur gjatë ditës, një përmirësim në performancën akademike dhe rritjen e aktivitetit sportive, - të gjitha shenjat e gjumit të mirë dhe të oksigjenimit.
Para Pas fazës së parë
Pas fazës së parëFaza e parë Faza e dytë Përfundimi
Fig. 11: Rezultatet pas trajtimit

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 13
1. Rubin MR. Mode of respiration and facial growth. Am J Or-thod. 1980;78:504-510.
2. Mocellin M, Fugmann EA, Gavazzoni FB. Estudo cefalomet-rico- radiografi co e otorrinolaringologico correlacionado o grau de obstrucao nasal e o padrao de crescimento facial em pacientes nao tratados ortodonticamente. Rev Bras Otorrinolaringol 2000;66:116-120.
3. Yamada T, Tanne K, Miyamoto K, Ymauchi K. Infl uences of na-sal respiratory obstruction on craniofacial growth in young Macaca fuscata monkeys. Am J Orthod.1997;111(1):38-43.
4. Watson RM, Warren DW, Fischer ND. Nasal resistance, skel-etal classifi cation and mouth breathing in orthodontic pa-tients. Am J Orthod. 1968;54(5):367-379.
5. Harari D, Redlich M, Miri S, et al. The eff ect of mouth breath-ing versus nasal breathing on dentofacial and craniofa-cial development in orthodontic patients. Laryngoscope 2010;120:2089-93.
6. Souki BQ, Pimenta GB, Souki MQ et al. Prevalence of maloc-clusion among mouth breathing children: do expectations meet reality? Int J Pediatr Otorhinolaryngol 2009;73:767-73.
7. Harvold EP, Chierici G, Vargervik K. Experiments on the development of dental malocclusions. Am J Orthod. 1972;61(1):38-44.
8. Gross A, Kellum GD, Michas C, Frantz D, Foster M, Walker M, Bishop FW. Openmouth posture and maxillary arch width in young children: a three-year evaluation. AmJ Orthod. 1994;106:635-640.
9. Linder-Arongon S, Backtrom A. A comparison between mouth and nose breathers with respect to occlusion and facial dimensions. Odont Revy. 1960;11:343-376.
10. Paul JL, Nanda RM. Eff ect of mouth breathing on dental oc-clusion. Angle Orthod. 1973;43:201-206.
11. Hilton LM. Clinical variations of mouthbreathing. Int J Oral Myol. 1978;4(1):5-7.
12. Lawton HM, Battagel JM, Kotecha B. A comparison of the Twin Block and Herbst mandibular advancement splints in the treatment of patients with obstructive sleep apnea: A prospective study. Eur J Orthod 2005;27(1):82-90.
REFERENCA
KonkluzioneDentistët janë në një pozicion unik për të parë fëmijët,
për të njohur shenjat dhe simptomat e frymëmarrjes me gojë, malokluzionin, anomalitë kraniofaciale dhe kushtet e lidhura me to si sindromi i apnesë obstruktive te gjumit. Diagnoza e malokluzioneve dentare dhe deformimeve skeletale të lidhura me frymëmarrjen me gojë, kërkon ekzaminime të shpeshta dhe të plota ortodontike. Trajtimi i hershëm për të reduktuar pengesat e rrugës
ajrore, obligimin e frymëmarrjes me gojë, deformimin kraniofacial dhe malokluzionin, është thelbësore për normalizimin e rritjes dhe zhvillimit. Trajtimi i hershëm maksimalizon suksesin e ortodoncisë dhe ortopedisë korrigjuese. Dentistët dhe otorinolaringologët ofrojnë trajtime unike që mund të zvogëlojnë pengesat e rrugës ajrore dhe deformimet kraniofaciale. Aparatet dentare ortodontike kanë treguar se përmirësojnë dimensionet sagitale të rrugëve ajrore të sipërme tek fëmijët.

Albanian Stomatological Journal14
AbstractNormal airway is an important factor for normal growth of craniofacial structures. Nazorespirator function and its connection with craniofacial growth is of great interest, not only for pediatric, but also for orthodontists, otolaryngologist, speech pathologists and other members of the healthcare community. The growth and function of the nasal cavities, nazopharynx, and oropharynx are closely related to normal growth of the skull. Due to the close relationship between pharynx and dentofacial structures, an expected mutual interaction between the structures of the pharynx and dentofacial model justifi es orthodontic interes.
Although, breathing is the most important action of human beings to live, we forget to put the air way in the diagnosis of orthodontic patients.
The purpose of this article is to bring into focus of orthodontics the management air way taking into account: the consequences of poor breathing, interdisciplinary treatment and prevention.
KEYWORDS :
airway,
malocclusion,
treatment
Dr. Andri Çabeli1, Dr. Edlira Subashi2, Dr. Rudin Kusi2, Dr. Egi Mulo2
Orthodontic treatment ortodontik of airway
1Aldent University, 2Private dental clinic
IntroductionMouth-breathing has been a controversial topic in
the pathogenesis of some dental malocclusions. An early account on the maladies associated with mouth-breathing was proposed approximately 130 years ago by a well-known American artist, George Catlin, in his book entitled “Malrespiration or the Breath of Life”. Catlin’s book was subsequently retitled “Shut Your Mouth and Save Your Life”. A copy of this book was brought to the attention of the dental community by Dr. Edward H. Angle in 1925. He reprinted George Catlin’s work in 1925, under its original title. In the foreword, Dr. Angle referred to the artist and stated: “In his belief that some forms of malocclusion of the teeth and facial deformity are due to mouth-breathing we only too well know Mr. Catlin to be entirely correct, and, doubtless, he is one of the fi rst, if not the fi rst, in this country to direct attention to this fact.” Dr. Angle’s belief that breathing complications were among the main contributing factors in the etiology of dental malocclusions probably developed from his medical training. He believed this to be of such importance that he included a full time otolaryngologist, Dr. James Ross Reed, on his teaching staff .
Mouth-breathing has been investigated by many scientists as a possible etiology for some dental malocclusions (1,2). The research in this area is expansive, but largely inconsistent. Thus, the cause and eff ect relationship of airway obstruction and malocclusion must be carefully examined on a case by case basis (3,4,5). Regardless of the various researcher’s conclusions, one theory remains common - that airway obstruction and malocclusion are related.
Therefore, dental professionals can include observation and monitoring of the upper airway as an
integral part of screening, then it would seem reasonable to begin within the fi rst several years following birth. The ultimate goal would be to encourage craniofacial development that would maximize the potential for upper-airway patency during sleep throughout the life of the individual (6, 7, 8).
AimThe aim of this article is to highlight the skills and tools
that assist the clinician in identifying airway obstruction, improving the diagnosis of orthodontics patients, and present treatment of associated malocclusions.
Material & MethodsThe methodology used in this article consists of 2
case reports with problems related with poor breathing and malocclusion.
For our patients complete diagnostic records consisted of:
Panoramic radiography
Pictures of models and a complete clinical examination,
Cephalometric analysis.
Cephalometric examinationSuperior pharyngeal diameter measured by the
extent of the posterior soft palate - the closest point to the pharyngeal wall is average 17.4 mm (15-20 mm) wide.
Superior pharyngeal diameter is reduced to (Photo 1):
Maxillary retrusion
Hypertrophy of adenoid, etc.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 15
Photo 1: Superior pharyngeal diameter
Inferior pharyngeal diameter measured from the point of termination of the posterior board of tongue and inferior board of mandible - the nearest point of pharyngeal posterior wall. Average measurement is 13.5 mm (11-14 mm) wide (Photo 2).
Width is reduced to: Retrusion of mandible Posterior rotation of the mandible Large mandibles, etc.
Photo 2: Inferior pharyngeal diameter
Photo 3: Analysis of tongue position
Also, in cephalometric analyses is seen the posture of tongue. In oral breathing subjects, tongue is positioned down, unlike the above position in palatum in nasal breathing subjects (Photo 3).
Case 1 is a 10 years old patient, who came to the clinic with concern that the upper teeth had come forward. During interrogation, the boy’s mother refers that he snores at night and complained of chest pain. In extraoral examination, the patient has labial incompetence and habitual open mouth. Diagnosis after clinical and radiological examination was:
Problems
Skeletal class II Mandibular retrusion OJ= 12 mm Narrow maxillary arch Noncoincidence of median lines
This narrow jaw (Photo 4) is a result of mouth breathers keeping their lips apart and their tongue position low. The imbalance between the tongue pressure, and the muscles in the cheek, result in cheek muscles compressing the alveolar process in the premolar region. Simultaneously, the lower jaw postures back. These simultaneous actions have been termed the compressor theory (9, 10, 11)..
At the patient was applied functional appliance (twin-block), without extractions.
The Twin Block (TB) appliance is a well-accepted approach in correcting Class II division 1 malocclusion with mandibular retrusion in recent years. Previous studies indicated that TB is eff ective in mandibular forward repositioning and thereby achieves a more harmonious facial profi le . The upper airway changes in adult patients with OSA were measured after mandibular repositioning treatment, and showed a signifi cant enlargement in pharyngeal volume (12).
Photo 4: Photographs of models and mouth before treatment
Albanian Stomatological Journal16
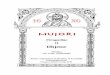
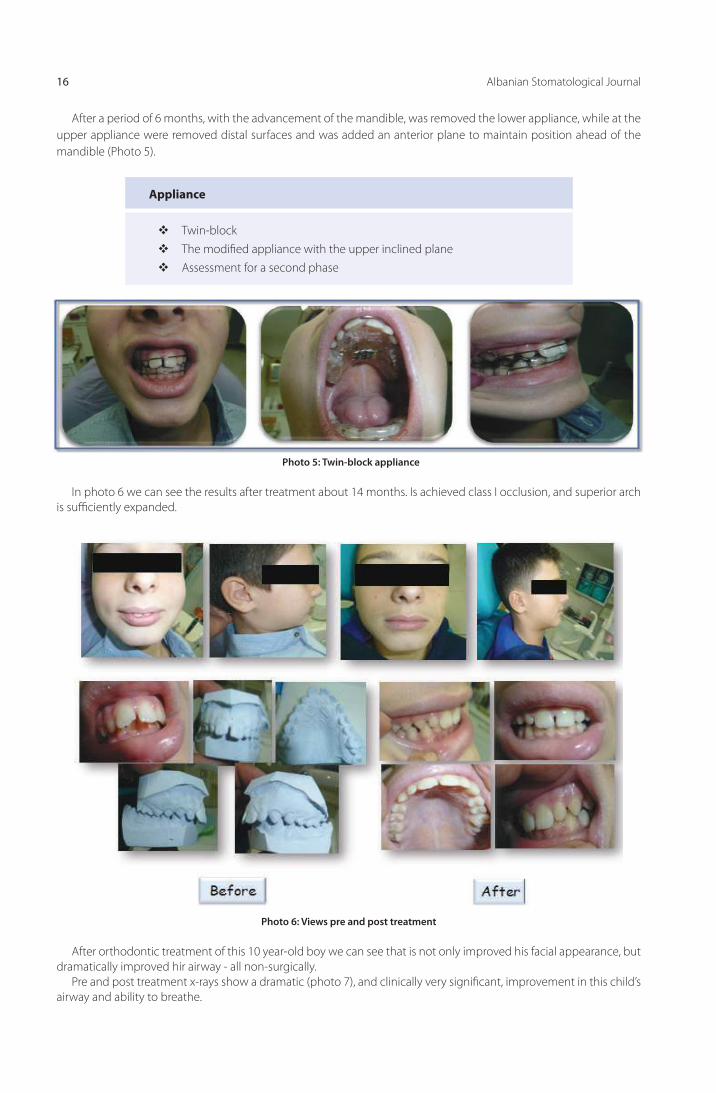
After a period of 6 months, with the advancement of the mandible, was removed the lower appliance, while at the upper appliance were removed distal surfaces and was added an anterior plane to maintain position ahead of the mandible (Photo 5).
Appliance
Twin-blockThe modifi ed appliance with the upper inclined plane Assessment for a second phase
Photo 5: Twin-block appliance
In photo 6 we can see the results after treatment about 14 months. Is achieved class I occlusion, and superior arch is suffi ciently expanded.
Photo 6: Views pre and post treatment
After orthodontic treatment of this 10 year-old boy we can see that is not only improved his facial appearance, but dramatically improved hir airway - all non-surgically.
Pre and post treatment x-rays show a dramatic (photo 7), and clinically very signifi cant, improvement in this child’s airway and ability to breathe.
Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 17
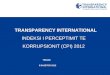
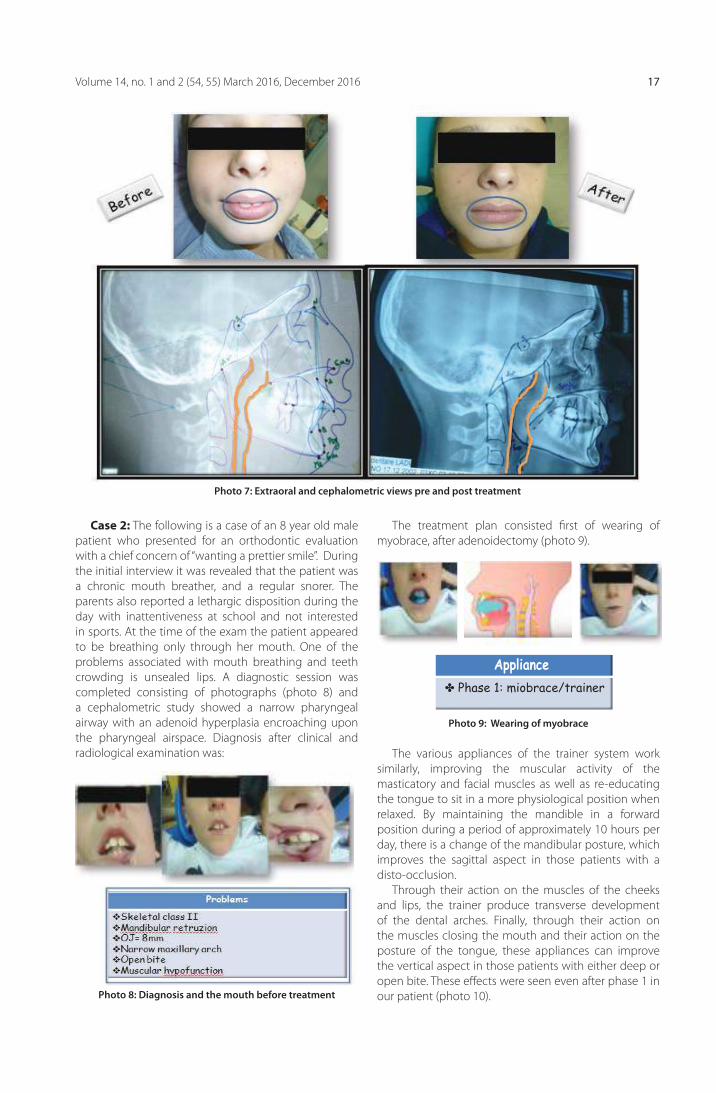
Case 2: The following is a case of an 8 year old male patient who presented for an orthodontic evaluation with a chief concern of “wanting a prettier smile”. During the initial interview it was revealed that the patient was a chronic mouth breather, and a regular snorer. The parents also reported a lethargic disposition during the day with inattentiveness at school and not interested in sports. At the time of the exam the patient appeared to be breathing only through her mouth. One of the problems associated with mouth breathing and teeth crowding is unsealed lips. A diagnostic session was completed consisting of photographs (photo 8) and a cephalometric study showed a narrow pharyngeal airway with an adenoid hyperplasia encroaching upon the pharyngeal airspace. Diagnosis after clinical and radiological examination was:
The treatment plan consisted fi rst of wearing of myobrace, after adenoidectomy (photo 9).
Photo 7: Extraoral and cephalometric views pre and post treatment
Photo 8: Diagnosis and the mouth before treatment
Photo 9: Wearing of myobrace
The various appliances of the trainer system work similarly, improving the muscular activity of the masticatory and facial muscles as well as re-educating the tongue to sit in a more physiological position when relaxed. By maintaining the mandible in a forward position during a period of approximately 10 hours per day, there is a change of the mandibular posture, which improves the sagittal aspect in those patients with a disto-occlusion.
Through their action on the muscles of the cheeks and lips, the trainer produce transverse development of the dental arches. Finally, through their action on the muscles closing the mouth and their action on the posture of the tongue, these appliances can improve the vertical aspect in those patients with either deep or open bite. These eff ects were seen even after phase 1 in our patient (photo 10).
✤ Phase 1: miobrace/trainer
Appliance

Albanian Stomatological Journal18
12 months of orthodontic phase 1, was followed by fullbraces appliance. Figure 11 shows the facial changes before and after treatment, the changes in the pharyngeal airway and the resolution of the ectopically positioned permanent maxillary canines. Post treatment, the mother reported a dramatic improvement in the patient’s overall health, level of alertness, a reduction in daytime sleepiness, an improvement in academic performance and increased athletic activity – all signs of better sleep and oxygenation.
Photo 10: After phase 1
Photo 11: Results after treatment
Before After phase 1
After phase 1Fase 1 Fase 2 Finish

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 19
1. Rubin MR. Mode of respiration and facial growth. Am J Or-thod. 1980;78:504-510.
2. Mocellin M, Fugmann EA, Gavazzoni FB. Estudo cefalomet-rico- radiografi co e otorrinolaringologico correlacionado o grau de obstrucao nasal e o padrao de crescimento facial em pacientes nao tratados ortodonticamente. Rev Bras Otorrinolaringol 2000;66:116-120.
3. Yamada T, Tanne K, Miyamoto K, Ymauchi K. Infl uences of na-sal respiratory obstruction on craniofacial growth in young Macaca fuscata monkeys. Am J Orthod.1997;111(1):38-43.
4. Watson RM, Warren DW, Fischer ND. Nasal resistance, skel-etal classifi cation and mouth breathing in orthodontic pa-tients. Am J Orthod. 1968;54(5):367-379.
5. Harari D, Redlich M, Miri S, et al. The eff ect of mouth breath-ing versus nasal breathing on dentofacial and craniofa-cial development in orthodontic patients. Laryngoscope 2010;120:2089-93.
6. Souki BQ, Pimenta GB, Souki MQ et al. Prevalence of maloc-clusion among mouth breathing children: do expectations meet reality? Int J Pediatr Otorhinolaryngol 2009;73:767-73.
7. Harvold EP, Chierici G, Vargervik K. Experiments on the development of dental malocclusions. Am J Orthod. 1972;61(1):38-44.
8. Gross A, Kellum GD, Michas C, Frantz D, Foster M, Walker M, Bishop FW. Openmouth posture and maxillary arch width in young children: a three-year evaluation. AmJ Orthod. 1994;106:635-640.
9. Linder-Arongon S, Backtrom A. A comparison between mouth and nose breathers with respect to occlusion and facial dimensions. Odont Revy. 1960;11:343-376.
10. Paul JL, Nanda RM. Eff ect of mouth breathing on dental oc-clusion. Angle Orthod. 1973;43:201-206.
11. Hilton LM. Clinical variations of mouthbreathing. Int J Oral Myol. 1978;4(1):5-7.
12. Lawton HM, Battagel JM, Kotecha B. A comparison of the Twin Block and Herbst mandibular advancement splints in the treatment of patients with obstructive sleep apnea: A prospective study. Eur J Orthod 2005;27(1):82-90.
REFERENCE
ConclusionsDentists are in a unique position to see the children,
to recognize the signs and symptoms of mouth breathing, malocclusions, craniofacial abnormalities and related conditions such as obstructive sleep apnea syndrome. Diagnosis of malocclusion and skeletal deformities associated with oral breathing, require frequent and complete orthodontic examinations. Early treatment to reduce the airway obstacles, obligation
of mouth breathing, craniofacial distortion and malocclusion is essential for normalization of growth and development. Early treatment maximizes the success of corrective orthodontics and orthopedics. Dentists and otorinolaringolog off er unique treatments that can reduce the airway obstacles and craniofacial distortions. Orthodontic dental appliances have shown to improve sagital dimensions of the upper airway in children.

Revista Stomatologjike Shqiptare20 Revista Stomatologjike Shqiptare20

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 21

Revista Stomatologjike Shqiptare22
AbstraktGranuloma piogjene eshte nje lezion muko-kutan beninj.
Ajo eshte nje pergjigje ndaj traumave te vazhdueshme dhe mund te jete e lidhur me ndryshimet hormonale.
Ne kavitetin oral paraqitet si nje nodul ose papul eritematoze, reziliente me nje siperfaqe te lemuar ose lobulare qe gjakoset lehtesisht.
Metodat e trajtimit jane te ndryshme si ato kirurgjikale (konvencionale) dhe trajtimi me lazer.
Trajtimi me lazer argon eshte perdorur gjate, por studimet tregojne se kane nje risk te larte per te formuar cikatrice.
Ne vitet e fundit trajtimi me lazer me vale te vazhdueshme te dioksidit te karbonit ka rezultuar ne nje opsion trajtimi efektiv.
Ne kete studim do paraqesim nje rast klinik te trajtimit te granulomes piogjene me diode lazer 980nm.
FJALËT KYÇE:
Granulome,
Lazer, lezion,
trajtim
kirurgjikal
Prof. Assoc. Merita Bardhoshi1, Prof. Assoc. Edit Xhajanka1, Dr. Neada Hysenaj2, Prof. Assoc. Agron Meto3, Dr. Aida Meto3
Menaxhimi i Granulomes Piogjene me Diode Lazer 980 nm
1Fakulteti i Mjekësisë Dentare, 2Klinika, Stomatologjike Universitare, 3Universiteti Aldent
HyrjeGranuloma piogjene eshte nje lezion muko-kutan
beninj. Ajo eshte nje pergjigje ndaj traumave te vazhdueshme dhe mund te jete e lidhur me ndryshimet hormonale. Ne kavitetin oral paraqitet si nje nodul ose papul eritematoze, reziliente me nje siperfaqe te lemuar ose lobulare qe gjakoset lehtesisht. Diametri i granulomes piogjene varion nga 2mm ne 2cm. Rralle lezionet mund te arrijne nje diameter prej 5 cm. Zakonisht lokalizohet ne gingive, por mund te gjendet dhe ne buze, gjuhe, mukozen orale dhe ne palatum. Ngjyra e granulomave piogjene varion nga e kuqe/roze ne vjollce. Lezionet e reja kane me shume gjasa te kene ngjyre te kuqe si rrjedhoje e nje numri me te larte te vazave te gjakut. Lezionet me te vjetra pergjithesisht jane ngjyre roze. Etiologjia e granulomave piogjene eshte e panjohur, megjithate traumat njihen si faktor pershpejtimi per avancimin e lezionit.
Metodat e trajtimit jane te ndryshme si ato kirurgjikale (konvencionale) dhe trajtimi me lazer. Trajtimi me lazer argon eshte perdorur gjate, por studimet tregojne se kane nje risk te larte per te formuar cikatrice. Ka disa studime te cilat raportojne perdorimin e lazerit me pulsime, megjithese perdorimi i tij u shfaq i suksesshem vetem ne eliminimin e granulomave shume te vogla. Ne vitet e fundit trajtimi me lazer me vale te vazhdueshme te dioksidit te karbonit ka rezultuar ne nje opsion trajtimi efektiv. Ne kete studim do paraqesim nje rast
klinik te trajtimit te granulomes piogjene me diode lazer 980nm.
Metodat, pacientetNe kete studim u trajtuan 2 paciente me granulome
piogjene. Ato u trajtuan me diode lazer 980 nm ne
Fig. 1 Granuloma Piogjene

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 23
Kliniken Stomatologjike Universitare, Tirane. U mor anamneza mjekesore dhe dentare e pacienteve, duke vijuar me pas me nje ekzaminim te detajuar ekstra dhe intra-oral.
Nepermjet testit plotesues te gjakut, formules se plote te gjakut dhe sedimentit te eritrociteve u be i mundur perjashtimi i semundjeve infektive. Pacientet nuk kishin ankesa sistemike. Te dhenat u mblodhen, nepermjet te cilave percaktuam dhe diagnozat klinike (fi g. 1). Perpara realizimit te procedures, pacientet fi rmosen formularin e konsensusit, pasi ato ishin informuar me detaje per menyren e trajtimit.
Diode lazer 980 nm qe u perdor kishte keto specifi ka: vale te vazhdueshme, fi ber optike 300 mikrometer dhe fuqi 3,5 w. Trajtimi u realizua me anestezi infi ltrative. Zona operative u ftoh nepermjet perdorimit te akullit per 2-5 minuta pas trajtimit. Te gjitha plaget u lane te hapur ne menyre qe te realizohej sherimi nepermjet granulacionit dhe epitelizimit sekondar, keshtu qe nuk u nevojiten sutura (fi g.2).
indeve te shoqeruar me plage te sheruara per nje kohe te gjate. Plaget u sheruan plotesisht pas 3-4 javesh pa cikatrice apo ndryshime pigmentare (fi g.3). Efekti estetik i terapise me lazer ishte evident. Rekurenca nuk u vune re ne pacientet te cilet u ndoqen deri ne 1 vit pas trajtimit.
Diskutime
Trajtimet konvencionale perfshijne trajtimet me lende kimike dhe ekscizione kirurgjikale. Megjithate keto trajtime nuk perjashtojne mundesine e komplikimeve si te cikatriceve apo ndryshimeve pigmentare. Keto komplikacione mund te sjellin probleme estetike te pacienteve. Trajtimet konvencionale shpesh shkaktojne dhimbje, hemoragji dhe probleme estetike. Trajtimi me lazer nuk kompromenton strukturat anatomike te buzes, kufi jte anatomike apo funksionalitetin e saj.
Disa pajisje te lazerit jane te suksesshme ne trajtimin e granulomave piogjene perfshire lazerat me pulsim 585 dhe 595 , lazeri 1064 nm dhe lazeri me dioksid karboni. Trajtimi me diode lazer 980 nm eshte nje alternative e suksesshme. Rrezja e lazer diode 980nm eshte e mire absorbuar nga hemoglobina. Ekscizioni u realizua teresisht, pa nevojen e suturimit si rrjedhoje e koagulimit te pershtatshem.
Konkluzioni
Nga rezultatet e arritura konkludojme qe aplikimi i diode lazer 980 nm ne trajtimin e granulomave piogjene eshte efektiv dhe i suksseshem.
Fig 3. Ndjekja,3jave pas trajtimit
Fig. 2 Menjehere pas trajtimit
Pas trajtimit u pershkruan analgjezik, por jo antibiotike. Vizitat post-operative u realizuan pas 10 diteve, 1 muaj, 6 muaj dhe 1 vit pas nderhyrjes. Lezionet u fotografuan dhe u dokumentuan ne te gjitha fazat e trajtimit dhe te sherimit.
RezultatetPas nderhyrjes nuk kishte hemoragji apo dhimbje.
Fuqia prej 3,5 w ne menyre te vazhdueshme dhe maja me kontakt te fokusuar sjellin nekroze superfi ciale te

Revista Stomatologjike Shqiptare24
1. Jose Y, Antonio-Jesus E, Leonardo B, Cosme G (2009) Treat-ment of oral mucocele–scalpel versus CO2 laser Med Oral Patol Cir Bucal. Sep 1; 14 (9): 469-474
2. Ata J, CarrilloC, BonetC, BalaguerJ, PenarrochaM, Penarro-cha M (2010) Oral mucocele: rewiew of the literature JClin-Exp Dent: 18-21
3. Baurmash HD (2003) Mucoceles and ranulas J Oral Maxil-lofacial Surgery; 61: 369-78
4. Baurmash H (2002) The etiology of superfi cial oral muco-celes J Oral Maxillofac Surg; 60: 237-8
5. Jinbu Y, Kusama M, Itoh H, Matsumoto K, Wang J, Noguchi T (2003) Mucocele of the glands of Blandin-Nuhn clinical and histopathologic analysis of 26 cases Oral Surg oral Med Oral PatholEndod; 95: 467-70
6. Bhaskar SN, Bolden TE, Weinmann JP (1956) Pathogenesis of mucoceles J Dent Res; 35: 863-74
7. Silva A Jr, Nikitakis NG, Balciunas BA, Meiller TF (2004) Su-perfi cial mucocele of the labial mucosa: a case report and review of the literature Gen Dent; 52: 424-7
8. Huang IY, Chen CM, Kao YH, Worthington P (2007) Treat-ment of mucocele of the lower lip with carbon dioxide laser J Oral MaxillofacSurg; 65: 855-8
REFERENCAT
9. Yamasoba T, Tayama N, Syoji M, Fukuta M (1990) Clinicosta-tistical study of lower lip mucoceles Head Neck; 12: 316-20
10. Romanos G, Nentwig G (1999) Diode laser 980 nm in Oral and Maxillofacial Surgical procedures Clinical observations Based on Clinical Applications Journal of Clinical Laser Medicine and Surgery Vol 17, Nr5: 193-197
11. Romanos G (2001) Der Laser in der ChirurgieEinsteiger–Handbuch: 52-53
12. Pick RM, Colvard MD (1962) Current status of Lasers in soft tissue dental surgery J Periodontol; 63: 589-602
13. Vitale M, Caprioglio C (2010) Lasers in dentistry Practical text book: 243-253
14. Gregnanin P, Cunha V, Hiramatsu L, Correa L (2010) Treat-ment of Mucocele of the lower lip with diode laser in pe-diatric patients: Presentation of 2 Clinical cases Pediatric Dentistry, Vol32, N.7: 539-541
15. Neckel C, Neustadt B (2012) Der Erbium: YAG und Dioden-laser in der aesthetisch–kosmetischen Zahnmedizin Jahr-buch Laser zahnmedizin: 85-89

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 25
AbstractPyogenic granuloma is a benign non/neo plastic mococutanous lesion. It is a reactional response to constant minor trauma and can be related to hormonal changes. In the mouth PG is manifested as a sessile or pedunculatet, resilient, erythematous, exophytic papule or nodule with a smooth or lobulated surface that bleed easly. Several methods can be applied to remove PG like surgery electrocauterisation and laser treatment. The argon laser has lon be used to trat PG but it is claimed to resul in an increased risk of scarring. In the past few years the continous – wave carbon dioxide laser has proved to be an eff ective treatment option. In this study we report an experience in the treatment of PG with diode laser 980 nm.
KEYWORDS:
Granuloma,
Lazer, Lesion,
Surgical
treatment
Prof. Assoc. Merita Bardhoshi1, Prof. Assoc. Edit Xhajanka1, Dr. Neada Hysenaj2, Prof. Assoc. Agron Meto3, Dr. Aida Meto3
The management of pyogenic granuloma with the 980 nm diode laser
1Faculty of Dental Medicine, 2University Dental Clinic, 3Aldent University
Introduction
Pyogenic granuloma is a benign non/neo plastic mococutanous lesion . It is a reactional response to constant minor trauma and can be related to hormonal changes. In the mouth PG is manifested as a sessile or pedunculatet, resilient, erythematous, exophytic papule or nodule with a smooth or lobulated surface that bleed easly. 1 2 3 the size of PG varies from 2 mm to 2 cm in diameter. Occasionally the lesions may reach a diameter of up 5 cm. PG prefentially aff ect the gingiva, but may also occur on te lips tounge oral mucosa and palate. The apparence of PG usually ranges in collour from red/pink to purple. Younger lesions are more likely to be red because of the high number of blood Vessels. Older lesions become pink. The exact cause of PG is unknow,Trauma is usually a precipitating factor.
Several methods can be applied to remove PG like surgery electrocauterisation and laser treatment. The argon laser has lon be used to trat PG but it is claimed to resul in an increased risk of scarring. There are several report about treatment of pulsed duy laser , although it was only successfully employed in removing very small granuloma .In the past few years the continous – wave carbon dioxide laser has proved to be an effective treatment option. In this study we report an experience in the treatment of PG with diode laser 980 nm.
Patients and Method
Two patients with PG were examinated in this study. They were treated with the 980 nm diode laser at the University of Tirana Dental School . An initial clinical examination consisting of the medical
Fig. 1 Pyogenic Granuloma

Albanian Stomatological Journal26
and dental history and a thorough extra and intra oral examination was performed . A complementary blood test , complete blood count and erythrocyte sedimentation rate test made it possible to exclude infectious diseases. The patients has no systemic complaints. The data collected was evaluated and a clinical diagnosis for the type of lesion was established fig 1 . Patients were given written and verbal information on the nature of laser treatment and dhe signed informed consent forms were obtained prior to the treatment . The 980 nm diode laser was applied using the following parameter - continous wave, 300 micrometer optical fiber and 3, 5 w power. The treatment was conducted under infiltration anesthesia . The treatment area was cooled by the application of ice for two to five minutes post operatively. All wounds were left open to heal by granulation and secondary epithelisation , therefore no sutures were required. Fig 2. After the treatment analgesic medication was prescribed to be taken as required ,but no antibiotics were prescribed . The follow-up visits were schedulated at ten days, one month, six months and one year after surgery. All of
and pigmentary changes. Fig 3 . The cosmetic effect of laser therapy was evident . No recurrence was observed in the patients who were followed up one year after the surgery.
DiscussionAesthetic treatment PG consists of the removal of the
lesion. Current treatment modalities include chemical cauterization and surgical excision. However these methods do not exclude the risk of complications such as scarring or pigmentary changes . These complications may lead to aesthetic problems for patients. Who accept the surgical removal of PG only with great diffi culty. The conventional lip shape procedure is often painful , results insignifi cant bleeding and poses cosmetic concerns. Laser treatment of the lip does not compromise the importance of the lip , its discrete anatomic borders such as the vermilion border or its functionality.
Various laser devices have been successfully used to treat PG including the 585 and 595 pulsed dye laser , the 1064 nm Nd. YAG and dioxide carbon laser. The pulsed dye laser is safe it can be used for lesions.
Treatment with 980 nm diode laser is a viable treatment option. The 980 nm diode laser beam is well absorbed by haemoglobine . The excision was well performed and suturing after surgery was not necessary because of good coagulation. The surgical period was signifi cantly reduced. From the goods results obtained it was concluded that the application of 980 nm diode laser in the treatment of PG appears to be of benefi cial eff ect.
Fig 3. Follow-up . 3 Weeks after the treatment
Fig 2 Immediately after the treatment
the lesions were photographically documented at all stages of treatment and healing.
ResultsPost operatively there was no bleeding or pain.
The power setting of 3, 5 w in continous mode and focused contact handpiece appeared to lead to sone superficial tissue necrosis associated with delayed wound healing. The wounds were completely healed after 3 to 4 weeks without scar formation

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 27
1. Jose Y, Antonio-Jesus E, Leonardo B, Cosme G (2009) Treat-ment of oral mucocele–scalpel versus CO2 laser Med Oral Patol Cir Bucal. Sep 1; 14 (9): 469-474
2. Ata J, CarrilloC, BonetC, BalaguerJ, PenarrochaM, Penarro-cha M (2010) Oral mucocele: rewiew of the literature JClin-Exp Dent: 18-21
3. Baurmash HD (2003) Mucoceles and ranulas J Oral Maxil-lofacial Surgery; 61: 369-78
4. Baurmash H (2002) The etiology of superfi cial oral muco-celes J Oral Maxillofac Surg; 60: 237-8
5. Jinbu Y, Kusama M, Itoh H, Matsumoto K, Wang J, Noguchi T (2003) Mucocele of the glands of Blandin-Nuhn clinical and histopathologic analysis of 26 cases Oral Surg oral Med Oral PatholEndod; 95: 467-70
6. Bhaskar SN, Bolden TE, Weinmann JP (1956) Pathogenesis of mucoceles J Dent Res; 35: 863-74
7. Silva A Jr, Nikitakis NG, Balciunas BA, Meiller TF (2004) Su-perfi cial mucocele of the labial mucosa: a case report and review of the literature Gen Dent; 52: 424-7
8. Huang IY, Chen CM, Kao YH, Worthington P (2007) Treat-ment of mucocele of the lower lip with carbon dioxide laser J Oral MaxillofacSurg; 65: 855-8
REFERENCE
9. Yamasoba T, Tayama N, Syoji M, Fukuta M (1990) Clinicosta-tistical study of lower lip mucoceles Head Neck; 12: 316-20
10. Romanos G, Nentwig G (1999) Diode laser 980 nm in Oral and Maxillofacial Surgical procedures Clinical observations Based on Clinical Applications Journal of Clinical Laser Medicine and Surgery Vol 17, Nr5: 193-197
11. Romanos G (2001) Der Laser in der ChirurgieEinsteiger–Handbuch: 52-53
12. Pick RM, Colvard MD (1962) Current status of Lasers in soft tissue dental surgery J Periodontol; 63: 589-602
13. Vitale M, Caprioglio C (2010) Lasers in dentistry Practical text book: 243-253
14. Gregnanin P, Cunha V, Hiramatsu L, Correa L (2010) Treat-ment of Mucocele of the lower lip with diode laser in pe-diatric patients: Presentation of 2 Clinical cases Pediatric Dentistry, Vol32, N.7: 539-541
15. Neckel C, Neustadt B (2012) Der Erbium: YAG und Dioden-laser in der aesthetisch–kosmetischen Zahnmedizin Jahr-buch Laser zahnmedizin: 85-89

Revista Stomatologjike Shqiptare28
Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 29
AbstraktEstetika në ditët e sotme po merr rëndësi gjithmonë e më shumë në vëmendjen e pacientit gjatë manipulimeve në dentistri. Për të arritur një rezultat sa më të mirë nga ana e mjekut kërkohet njohuri, praktike dhe zhdërvjelltësi në manipulimet praktike. Ekzistojne disa teknika dhe përdorime praktike të thjeshta e në te njëjtën kohë konservative, të cilat mund të na çojnë në një rezultat optimal siç janë:
Ndryshime të formës dhe gjatësisë; Simetrisë dhe dimensionit; Pozicionit dhe drejtimit; Sipërfaqeve të kurorës; Ngjyrës , etj.
Qëllimi:Të sjellim praktikën tonë për disa trajtime konservative të cilat ndryshojnë pamjen vizive dhe buzëqeshjen në përgjithësi, me qellim fokusimin drejt këtyre praktikave.
Materiale dhe Metoda:Janë marrë disa raste klinike nga puna jonë e përditshme disa vjecare, duke aplikuar protokollin terapeutik para dhe pas trajtimit.
D.M.Sc. Koço Gjilo, Dr. Dasaret Hajdini
Rikthimi i estetikës dentare nepermjet restaurimeve konservative
Fakulteti i Mjekësisë Dentare, Universiteti i Mjekësisë, Tiranë
HyrjeShkaku kryesor për paraqitjen e pacientit në klinikë,
gjithnjë e më shumë po bëhet estetika dentare. Reabilitimet e ndryshme për të realizuar estetikë dentare sa me te mire, kanë avancuar gjithnjë e më shumë. Keto reabilitime konsistojne qe nga ndërhyrjet e vogla në sistemin dhëmbor aktual, deri në ndërhyrje me komplekse me zëvendësimin komplet te dhëmbëve nëpërmjet mënyrave të avancuara si implantologjia, sistemi CAD/CAM etj. Rezultati i arritur duhet të realizohet me metoda sa më konservative e sa më pak traumatike. Kjo bën që ne të ruajmë elementët biologjikë dhe të ulim kostot e pacientit. Këto metoda fi llojnë me rregullimet e pjesës frontale nëpërmjet mbushjeve të thjeshta dhe deri në metodat kirurgjikale duke korrigjuar shumë elementë të ndryshëm të hapësirës së gojës.
Estetika dentare është një nga pjesët më të kërkuara nga pacientët dhe më të dëshiruara nga dentistët. Në këtë pjesë të dentistrisë arrihet rezultati fi nal estetik i mundshëm duke realizuar kërkesat estetike që sot kërkohen nga pacientët.Në pjesën e estetikës janë investuar pothuajse të gjitha disiplinat dentare, si konservative (fasetat dentare), paradontologjia, kirurgjia dhe sidomos protetika së bashku me laborantin dentar, të cilet kanë edhe rolin më të madh kontribues në rastet e mungesave të mëdha estetike. Gjithashtu edhe ortodoncia korrigjon probleme të mëdha estetike pa bërë sakrifi ca te materialet biologjike të hapësirës së gojës. Po keshtu edhe implantologjia i ka dhënë një shtysë akoma më të madhe rehabilitimit dentar, për vetë
rolin që ajo ka, pasi rrit shumë kompleksin e pacientit kur ai ka mungesa dhëmbësh.
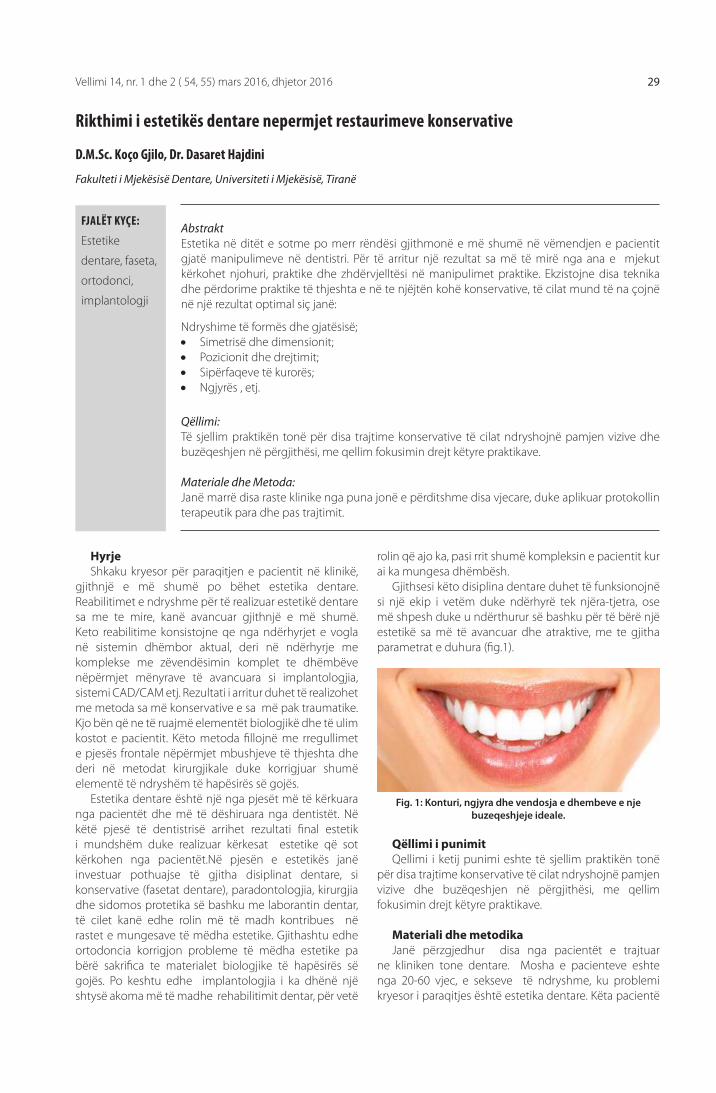
Gjithsesi këto disiplina dentare duhet të funksionojnë si një ekip i vetëm duke ndërhyrë tek njëra-tjetra, ose më shpesh duke u ndërthurur së bashku për të bërë një estetikë sa më të avancuar dhe atraktive, me te gjitha parametrat e duhura (fi g.1).
FJALËT KYÇE:
Estetike
dentare, faseta,
ortodonci,
implantologji
Qëllimi i punimitQellimi i ketij punimi eshte të sjellim praktikën tonë
për disa trajtime konservative të cilat ndryshojnë pamjen vizive dhe buzëqeshjen në përgjithësi, me qellim fokusimin drejt këtyre praktikave.
Materiali dhe metodikaJanë përzgjedhur disa nga pacientët e trajtuar
ne kliniken tone dentare. Mosha e pacienteve eshte nga 20-60 vjec, e sekseve të ndryshme, ku problemi kryesor i paraqitjes është estetika dentare. Këta pacientë
Fig. 1: Konturi, ngjyra dhe vendosja e dhembeve e nje buzeqeshjeje ideale.
Revista Stomatologjike Shqiptare30
janë diferencuar sipas problemeve estetike që kanë, duke i klasifi kuar në disa grupe të ndryshme sipas mospërputhjes së ligjeve të estetikës dentare.
Ato janë klasifi kuar në këto grupe:1. Rregullimi i gjatësisë së dhëmbëve frontalë2. Korrigjimi i formës me anë të mbushjeve3. Korrigjim i linjës gingivare nëpërmjet lazerit
dentar4. Protetikë fi kse nëpërmjet punimeve të
ndryshme estetike si fasetë, kurora, punime pjesore fi kse të mëdha
5. Zbardhimet dentare nëpërmjet mënyrës së realizimit nga mjeku e pacienti
6. Ortodoncia dentare7. Implantologjia dentare
Shpesh këto metoda janë realizuar nëpërmjet kombinimit të dy a më shumë disiplinave të ndryshme duke realizuar dhe estetikë sa më origjinale.
Rastet klinike dhe metodat e perdorura:1. Rregullimi i gjatësisë së dhëmbëve frontalëCdo ditë në klinikë paraqiten pacientë të cilët nuk janë
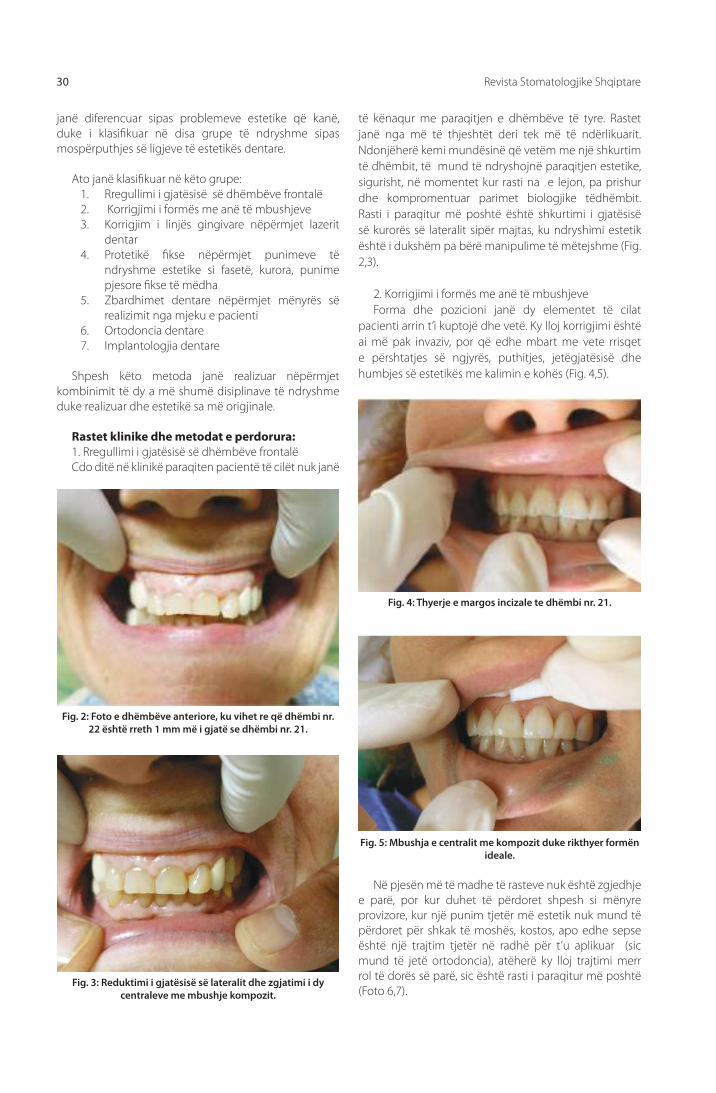
të kënaqur me paraqitjen e dhëmbëve të tyre. Rastet janë nga më të thjeshtët deri tek më të ndërlikuarit. Ndonjëherë kemi mundësinë që vetëm me një shkurtim të dhëmbit, të mund të ndryshojnë paraqitjen estetike, sigurisht, në momentet kur rasti na e lejon, pa prishur dhe kompromentuar parimet biologjike tëdhëmbit. Rasti i paraqitur më poshtë është shkurtimi i gjatësisë së kurorës së lateralit sipër majtas, ku ndryshimi estetik është i dukshëm pa bërë manipulime të mëtejshme (Fig. 2,3).
2. Korrigjimi i formës me anë të mbushjeveForma dhe pozicioni janë dy elementet të cilat
pacienti arrin t’i kuptojë dhe vetë. Ky lloj korrigjimi është ai më pak invaziv, por që edhe mbart me vete rrisqet e përshtatjes së ngjyrës, puthitjes, jetëgjatësisë dhe humbjes së estetikës me kalimin e kohës (Fig. 4,5).
Fig. 2: Foto e dhëmbëve anteriore, ku vihet re që dhëmbi nr. 22 është rreth 1 mm më i gjatë se dhëmbi nr. 21.
Fig. 3: Reduktimi i gjatësisë së lateralit dhe zgjatimi i dy centraleve me mbushje kompozit.
Fig. 4: Thyerje e margos incizale te dhëmbi nr. 21.
Fig. 5: Mbushja e centralit me kompozit duke rikthyer formën ideale.
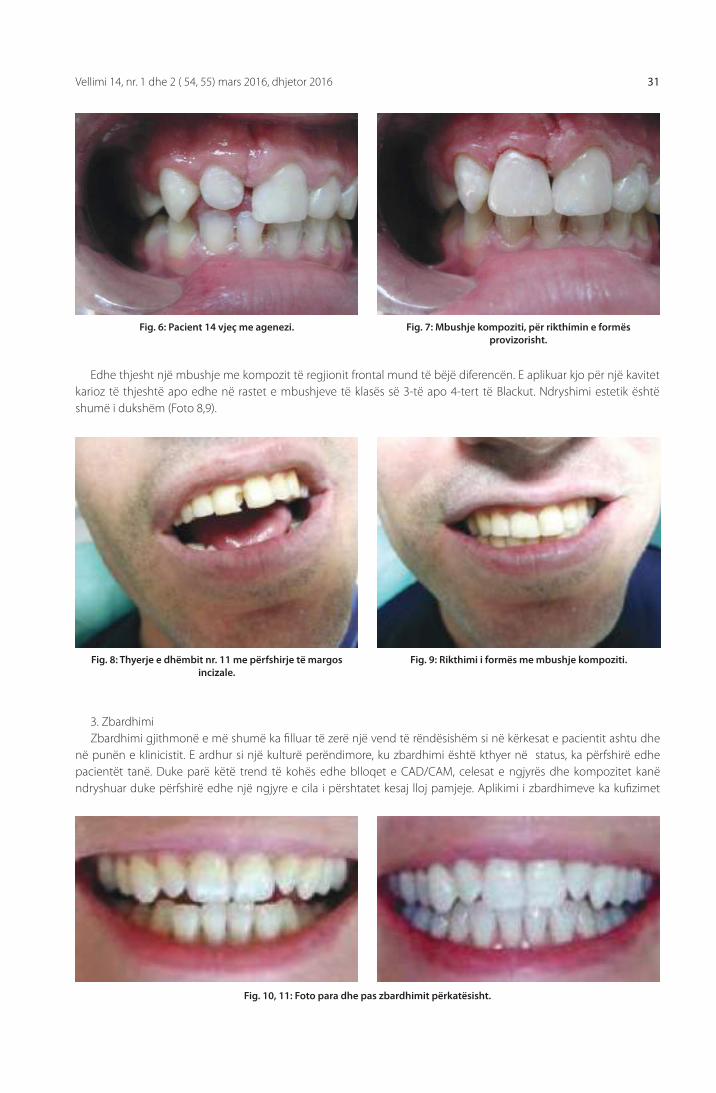
Në pjesën më të madhe të rasteve nuk është zgjedhje e parë, por kur duhet të përdoret shpesh si mënyre provizore, kur një punim tjetër më estetik nuk mund të përdoret për shkak të moshës, kostos, apo edhe sepse është një trajtim tjetër në radhë për t’u aplikuar (sic mund të jetë ortodoncia), atëherë ky lloj trajtimi merr rol të dorës së parë, sic është rasti i paraqitur më poshtë (Foto 6,7).
Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 31
Edhe thjesht një mbushje me kompozit të regjionit frontal mund të bëjë diferencën. E aplikuar kjo për një kavitet karioz të thjeshtë apo edhe në rastet e mbushjeve të klasës së 3-të apo 4-tert të Blackut. Ndryshimi estetik është shumë i dukshëm (Foto 8,9).
Fig. 8: Thyerje e dhëmbit nr. 11 me përfshirje të margos incizale.
Fig. 10, 11: Foto para dhe pas zbardhimit përkatësisht.
Fig. 9: Rikthimi i formës me mbushje kompoziti.
Fig. 6: Pacient 14 vjeç me agenezi. Fig. 7: Mbushje kompoziti, për rikthimin e formës provizorisht.
3. ZbardhimiZbardhimi gjithmonë e më shumë ka fi lluar të zerë një vend të rëndësishëm si në kërkesat e pacientit ashtu dhe
në punën e klinicistit. E ardhur si një kulturë perëndimore, ku zbardhimi është kthyer në status, ka përfshirë edhe pacientët tanë. Duke parë këtë trend të kohës edhe blloqet e CAD/CAM, celesat e ngjyrës dhe kompozitet kanë ndryshuar duke përfshirë edhe një ngjyre e cila i përshtatet kesaj lloj pamjeje. Aplikimi i zbardhimeve ka kufi zimet
Revista Stomatologjike Shqiptare32
e veta sidomos të moshës dhe dhëmbëve devitalë apo shumë të dëmtuar. Më poshtë është paraqitur rasti i një pacienti pas zbardhimit, ku pamja ka ndryshuar (Foto 10,11).
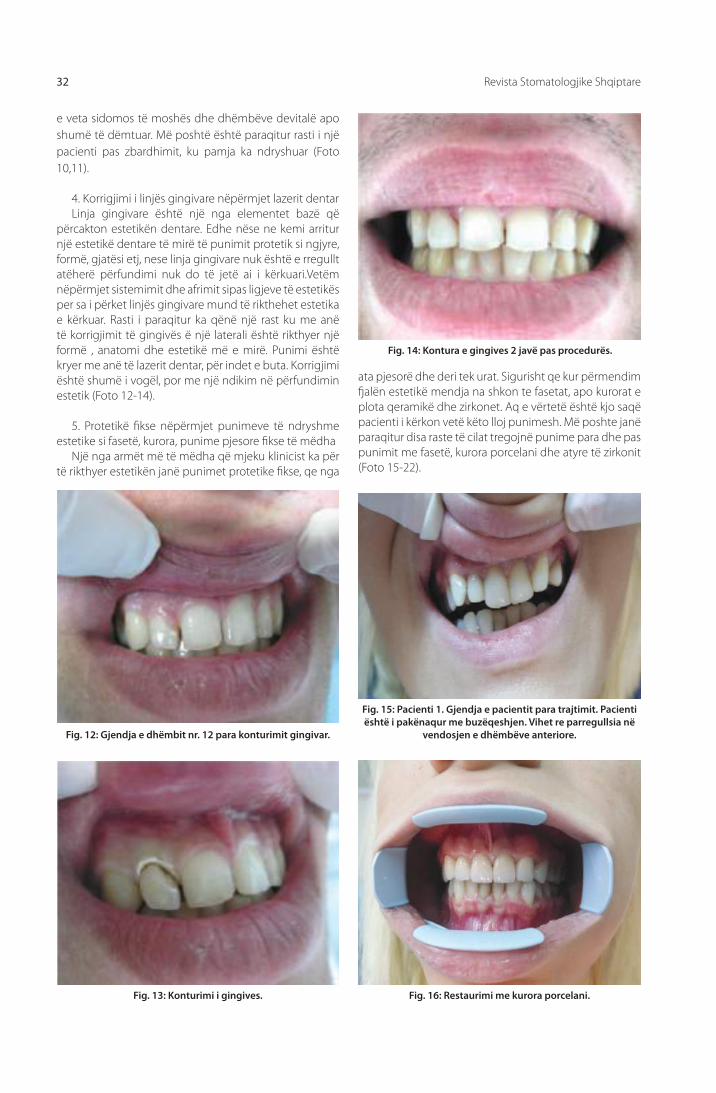
4. Korrigjimi i linjës gingivare nëpërmjet lazerit dentarLinja gingivare është një nga elementet bazë që
përcakton estetikën dentare. Edhe nëse ne kemi arritur një estetikë dentare të mirë të punimit protetik si ngjyre, formë, gjatësi etj, nese linja gingivare nuk është e rregullt atëherë përfundimi nuk do të jetë ai i kërkuari.Vetëm nëpërmjet sistemimit dhe afrimit sipas ligjeve të estetikës per sa i përket linjës gingivare mund të rikthehet estetika e kërkuar. Rasti i paraqitur ka qënë një rast ku me anë të korrigjimit të gingivës ë një laterali është rikthyer një formë , anatomi dhe estetikë më e mirë. Punimi është kryer me anë të lazerit dentar, për indet e buta. Korrigjimi është shumë i vogël, por me një ndikim në përfundimin estetik (Foto 12-14).
5. Protetikë fi kse nëpërmjet punimeve të ndryshme estetike si fasetë, kurora, punime pjesore fi kse të mëdha
Një nga armët më të mëdha që mjeku klinicist ka për të rikthyer estetikën janë punimet protetike fi kse, qe nga
Fig. 12: Gjendja e dhëmbit nr. 12 para konturimit gingivar.
ata pjesorë dhe deri tek urat. Sigurisht qe kur përmendim fj alën estetikë mendja na shkon te fasetat, apo kurorat e plota qeramikë dhe zirkonet. Aq e vërtetë është kjo saqë pacienti i kërkon vetë këto lloj punimesh. Më poshte janë paraqitur disa raste të cilat tregojnë punime para dhe pas punimit me fasetë, kurora porcelani dhe atyre të zirkonit (Foto 15-22).
Fig. 15: Pacienti 1. Gjendja e pacientit para trajtimit. Pacienti është i pakënaqur me buzëqeshjen. Vihet re parregullsia në
vendosjen e dhëmbëve anteriore.
Fig. 16: Restaurimi me kurora porcelani.
Fig. 14: Kontura e gingives 2 javë pas procedurës.
Fig. 13: Konturimi i gingives.

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 33
6. Punimet ortodontike dhe implantetTë arrihet një estetikë e kënaqshme shpesh herë nuk është kaq e thjeshtë. Punimi kërkon një bashkëpunim apo dhe
bashkërendim punimesh ndërmjet disa specialiteteve dentare ku më të rëndësishmet janë implantologjia, ortodoncia dhe paradontologjia me të cilët mjeku protezist duhet të jetë i familjarizuar apo të bashkëpunojë me mjekë të këtyre specialiteteve. Vetëm në këtë mënyrë mund të arrihet një përfundim sa më i mire ( Foto 23, 24).
KonkluzionEstetika për vetë kërkesat e pacientit do të mbetet prioriteti i padiskutueshëm i dentistrisë. Dentisti ka për detyrë
që nëpërmjet metodave sa më konservative të arrijë estetikën maksimale në mënyrë që pacientët të mbeten sa më të kënaqur. Zgjedhja e rrugës duhet bërë shpeshherë në bashkëpunim me specialiste të tjerë si ortodonti, implantologu, paradontologu, protezisti etj. Ky lloj ekipi i kualifi kuar realizon atë që quhet estetikë maksimale dhe ruan elementet biologjikë të hapësirës së gojës sic janë dhëmbët, paradonti, substanca kockore etj.
Fig. 17: Pacienti 2. Gjendja e pacientit para restaurimit me fasetat estetike. Pacienti është i pakënaqur me formën dhe
ngjyrën e dhëmbëve. Dhëmbët e preparuar per fasetat lumineers.
Fig. 18: Pacienti 2. Aplikimi i fasetave në gojë, në momentin e cementimit.
Fig. 19: Pacient me ulje të gjatësisë së kurorës si pasojë e abrazionit.
Fig. 21: Pacienti 3. Prova e metalit në gojë.
Fig. 20: Pacienti 3. Zgjatja e kulteve me anë të vidave të derdhura dhe vidave të qelqit.
Fig. 22: Pacienti 3. Aplikimi përfundimtar.
Revista Stomatologjike Shqiptare34
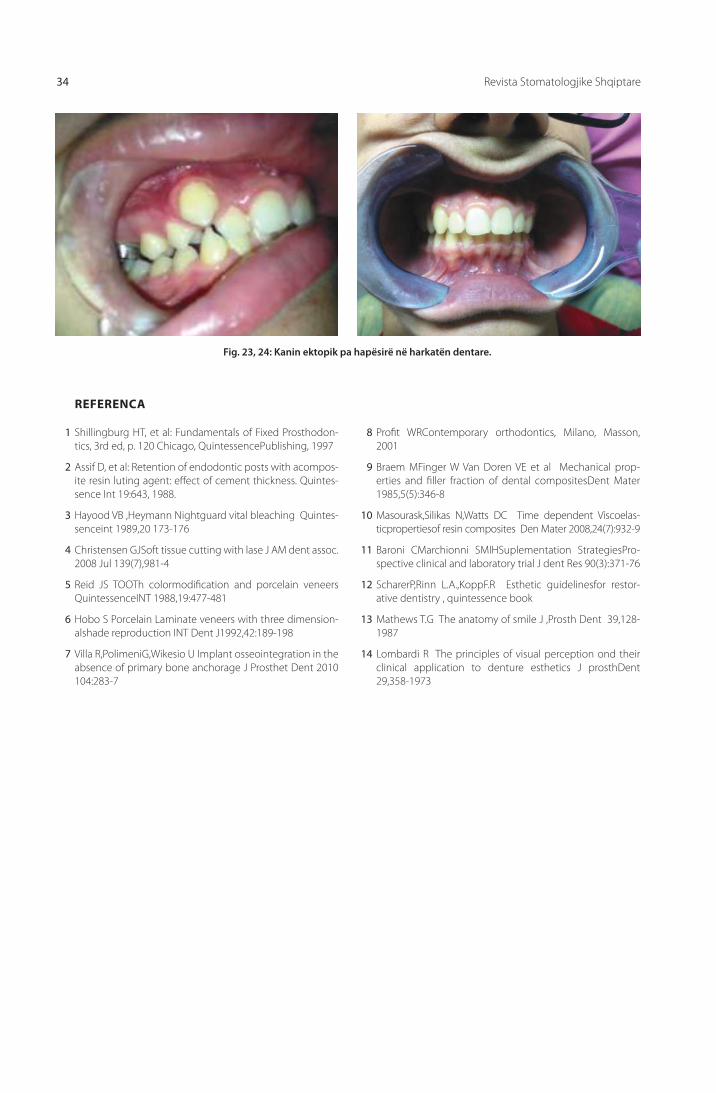
Fig. 23, 24: Kanin ektopik pa hapësirë në harkatën dentare.
1 Shillingburg HT, et al: Fundamentals of Fixed Prosthodon-tics, 3rd ed, p. 120 Chicago, QuintessencePublishing, 1997
2 Assif D, et al: Retention of endodontic posts with acompos-ite resin luting agent: eff ect of cement thickness. Quintes-sence Int 19:643, 1988.
3 Hayood VB ,Heymann Nightguard vital bleaching Quintes-senceint 1989,20 173-176
4 Christensen GJSoft tissue cutting with lase J AM dent assoc. 2008 Jul 139(7),981-4
5 Reid JS TOOTh colormodifi cation and porcelain veneers QuintessenceINT 1988,19:477-481
6 Hobo S Porcelain Laminate veneers with three dimension-alshade reproduction INT Dent J1992,42:189-198
7 Villa R,PolimeniG,Wikesio U Implant osseointegration in the absence of primary bone anchorage J Prosthet Dent 2010 104:283-7
8 Profi t WRContemporary orthodontics, Milano, Masson, 2001
9 Braem MFinger W Van Doren VE et al Mechanical prop-erties and fi ller fraction of dental compositesDent Mater 1985,5(5):346-8
10 Masourask,Silikas N,Watts DC Time dependent Viscoelas-ticpropertiesof resin composites Den Mater 2008,24(7):932-9
11 Baroni CMarchionni SMIHSuplementation StrategiesPro-spective clinical and laboratory trial J dent Res 90(3):371-76
12 ScharerP,Rinn L.A.,KoppF.R Esthetic guidelinesfor restor-ative dentistry , quintessence book
13 Mathews T.G The anatomy of smile J ,Prosth Dent 39,128-1987
14 Lombardi R The principles of visual perception ond their clinical application to denture esthetics J prosthDent 29,358-1973
REFERENCA
Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 35
Abstract Nowadays esthetics is becoming more important for the patients. To achieve a better result, the dentist should have theoretical knowledge, good practical skills and dexterity manipulation. There are some practical and simple techniques ,at the same time conservative which can lead us to a better result
Changes of: Form and length Symmetry and dimension Position and direction Coronal surfaces Color etc
Purpose:The purpose is to achieve better esthetic results using conservative techniques.
Materials and methods :We will show you some clinical cases from our daily practice of several years applying therapeutic protocol before and after the treatment.
D.M.Sc. Koço Gjilo, Dr. Dasaret Hajdini
Dental Aesthetic rehabilitation via conservative restorations
Faculty of Dental Medicine, University of Medicine, Tirana
EntryThe main reason for visiting the dentist nowadays
is becoming dental esthetics. The possible techniques used to achieve a better result are becoming more and more advanced. These techniques begin from the conservative treatments of the actual dental system to the more complex treatments like replacing all the teeth through advanced methods like dental implants, CAD/CAM system etc. The result should be achieved with conservative and less traumatic methods. Consequently we preserve the biological elements and decrease the costs of the patient. This methods begin with the restorations of the anterior side through simple fillings , to continue with chirurgical methods repairing different elements of the oral cavity. (1,2)
Dental esthetics is one of the most requested part by the patients and dentists. In this part of dentistry is achieved the fi nal possible esthetic result, fulfi lling the wishes of the patient. In esthetics are invested all of the dental disciplines like conservative dentistry( Veneers), periodontology, surgery and prosthodontics with the laboratory technician , which have the biggest role in case of major of esthetic defi ciencies
Orthodontics also repairs big esthetic problems without sacrifi cing the biological elements of the oral
cavity. Implantology as well has a big role in the dental rehabilitation .(3)
However these disciplines should work as a team to achieve the best possible esthetics.
KEYWORDS:
Dental
Aesthetic,
veneers,
orthodontics.
The purpose of the treatment
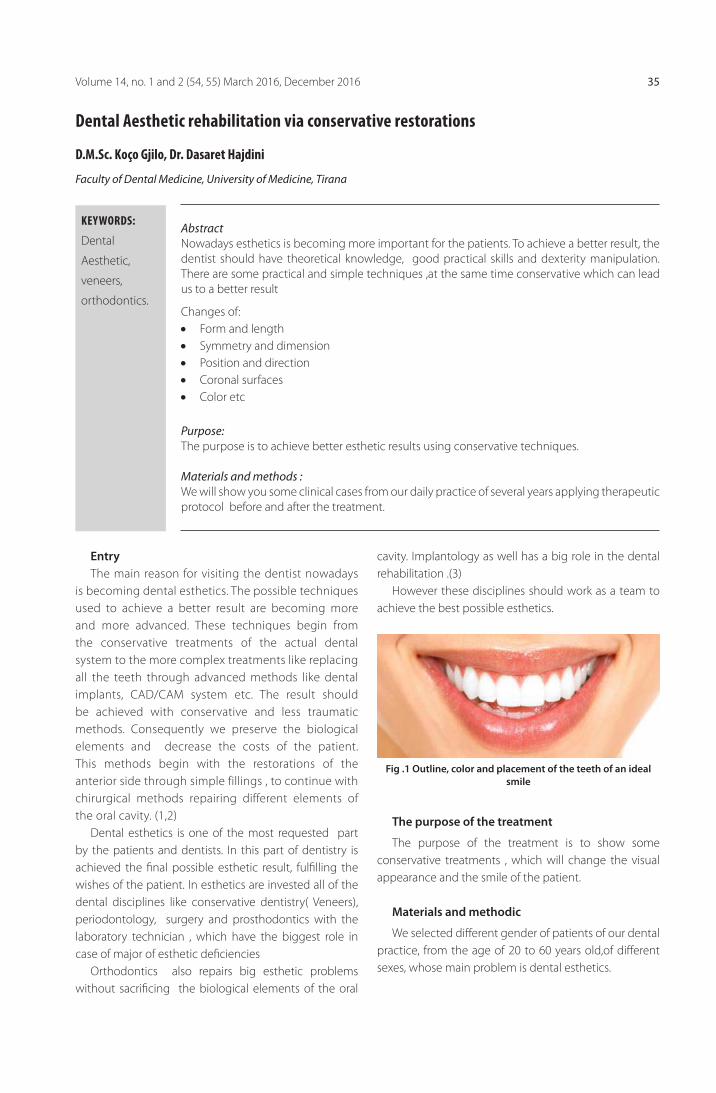
The purpose of the treatment is to show some conservative treatments , which will change the visual appearance and the smile of the patient.
Materials and methodic
We selected diff erent gender of patients of our dental practice, from the age of 20 to 60 years old,of diff erent sexes, whose main problem is dental esthetics.
Fig .1 Outline, color and placement of the teeth of an ideal smile

Albanian Stomatological Journal36
These patients are classifi ed in some groups based on their esthetic problems:
1. Adjust the length of the frontal teeth
2. Correction of the form by composite obturation
3. Correction of gingival line through dental laser
4. fi xed prosthodontic through diff erent aesthetic manipulation as Veneers, crowns, fi xed partial and dental reconstructing of full arcade
5. dental whitening ( home and in offi ce )
6. Dental Orthodontics
7. dental implantology
Clinical cases and the methods used:
1. Adjust the length of the frontal teethEevery day in clinic we face patients who are not
satisfi ed with the appearance of their teeth. Cases are from t simples to the most complex. Sometimes we have the possibility that with only an abbreviation of the tooth, the aesthetic appearance can change, of course, on some cases , without compromising the biological principles of the tooth( 4). The case presented below is a shortening of the upper left lateral crown, and the diff erence is obvious aesthetic without further manipulation (photo. 2,3).
2. Correction of form by composite obturation Form and position are two elements that the patients
comprehends by themselves. This type of correction is the least invasive, but also carries out the risks of adapting the color, adhesion, durability and aesthetics loss over time In most cases it is not the fi rst choice, but
Fig. 2 Left lateral is prox 1 mm longer than centrals
Fig. 3 Shortening of left lateral
Fig. 4 fracture of Incizal line of central 11
Fig. 5 Obturation of gingival line of central 11
most of the time is used as provisionally choice , when other work on aesthetic can not be used due to age, cost, or when another kind of treatment is to be done before as which can be Orthodontics treatment. (5,6)Then this type of treatment takes fi rst major role, as is the case shown below (photo 6,7)
Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 37
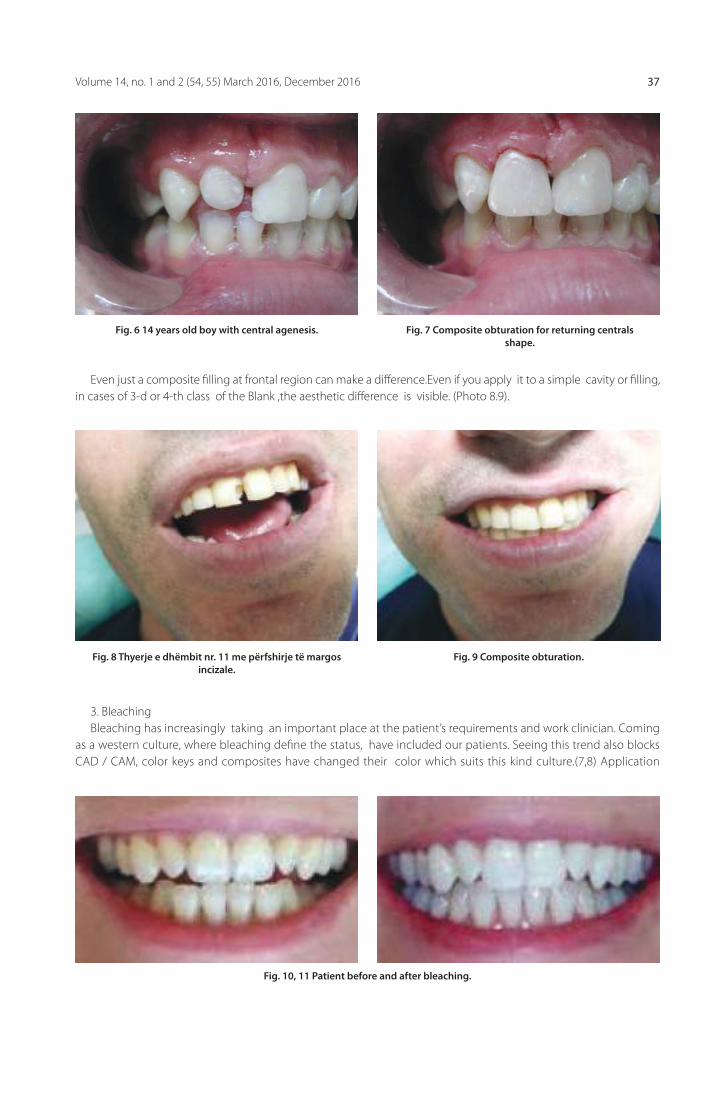
Fig. 8 Thyerje e dhëmbit nr. 11 me përfshirje të margos incizale.
Fig. 10, 11 Patient before and after bleaching.
Fig. 9 Composite obturation.
Fig. 6 14 years old boy with central agenesis. Fig. 7 Composite obturation for returning centrals shape.
Even just a composite fi lling at frontal region can make a diff erence.Even if you apply it to a simple cavity or fi lling, in cases of 3-d or 4-th class of the Blank ,the aesthetic diff erence is visible. (Photo 8.9).
3. BleachingBleaching has increasingly taking an important place at the patient’s requirements and work clinician. Coming
as a western culture, where bleaching defi ne the status, have included our patients. Seeing this trend also blocks CAD / CAM, color keys and composites have changed their color which suits this kind culture.(7,8) Application
Albanian Stomatological Journal38
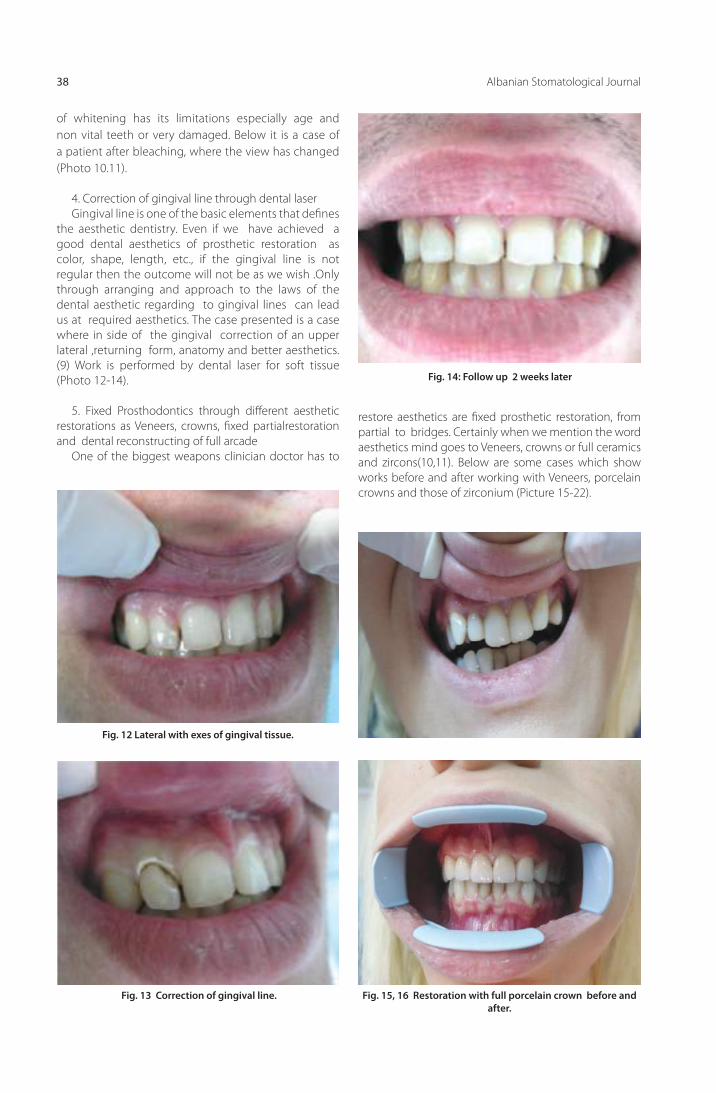
Fig. 12 Lateral with exes of gingival tissue.
Fig. 15, 16 Restoration with full porcelain crown before and after.
Fig. 14: Follow up 2 weeks later
Fig. 13 Correction of gingival line.
of whitening has its limitations especially age and non vital teeth or very damaged. Below it is a case of a patient after bleaching, where the view has changed (Photo 10.11).
4. Correction of gingival line through dental laserGingival line is one of the basic elements that defi nes
the aesthetic dentistry. Even if we have achieved a good dental aesthetics of prosthetic restoration as color, shape, length, etc., if the gingival line is not regular then the outcome will not be as we wish .Only through arranging and approach to the laws of the dental aesthetic regarding to gingival lines can lead us at required aesthetics. The case presented is a case where in side of the gingival correction of an upper lateral ,returning form, anatomy and better aesthetics.(9) Work is performed by dental laser for soft tissue (Photo 12-14).
5. Fixed Prosthodontics through diff erent aesthetic restorations as Veneers, crowns, fi xed partialrestoration and dental reconstructing of full arcade
One of the biggest weapons clinician doctor has to
restore aesthetics are fi xed prosthetic restoration, from partial to bridges. Certainly when we mention the word aesthetics mind goes to Veneers, crowns or full ceramics and zircons(10,11). Below are some cases which show works before and after working with Veneers, porcelain crowns and those of zirconium (Picture 15-22).

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 39
Fig. 17, 18 Patient with lumineers , before and after.
Fig. 19 Patient with an Abrasion
Fig. 21 Metal control in offi ce.
Fig. 20 After preparation
Fig. 22 After cementation.
6. Orthodontic treatments and implantsTo achieve a satisfactory aesthetics often is not so simple. It necessary that doctor will be open to collaborate with
other dental specialists especially implantologist, Orthodontist and periodontists and prosthodontist(12). Only in this way can we achieve a good result(Photo 23, 24).
ConclusionsAesthetics for patient self requirements will remain the undisputed priority of dentistry. The dentist has a duty
through as conservative methods to achieve maximum aesthetics so that patients remain more satisfi ed. The choice of the best way should be done often in collaboration with other specialists such as orthodontist, implantologist, periodontist, prosthodontist etc(13,14). This type of qualifi ed team realizes what is called maximum aesthetics and preserves the biological elements such as teeth, mouth, paradontium, etc.

Albanian Stomatological Journal40
Fig. 23, 24 Orthodontic treatment before and after of an ectopic canine
1 Shillingburg HT, et al: Fundamentals of Fixed Prosthodon-tics, 3rd ed, p. 120 Chicago, QuintessencePublishing, 1997
2 Assif D, et al: Retention of endodontic posts with acompos-ite resin luting agent: eff ect of cement thickness. Quintes-sence Int 19:643, 1988.
3 Hayood VB ,Heymann Nightguard vital bleaching Quintes-senceint 1989,20 173-176
4 Christensen GJSoft tissue cutting with lase J AM dent assoc. 2008 Jul 139(7),981-4
5 Reid JS TOOTh colormodifi cation and porcelain veneers QuintessenceINT 1988,19:477-481
6 Hobo S Porcelain Laminate veneers with three dimension-alshade reproduction INT Dent J1992,42:189-198
7 Villa R,PolimeniG,Wikesio U Implant osseointegration in the absence of primary bone anchorage J Prosthet Dent 2010 104:283-7
8 Profi t WRContemporary orthodontics, Milano, Masson, 2001
9 Braem MFinger W Van Doren VE et al Mechanical prop-erties and fi ller fraction of dental compositesDent Mater 1985,5(5):346-8
10 Masourask,Silikas N,Watts DC Time dependent Viscoelas-ticpropertiesof resin composites Den Mater 2008,24(7):932-9
11 Baroni CMarchionni SMIHSuplementation StrategiesPro-spective clinical and laboratory trial J dent Res 90(3):371-76
12 ScharerP,Rinn L.A.,KoppF.R Esthetic guidelinesfor restor-ative dentistry , quintessence book
13 Mathews T.G The anatomy of smile J ,Prosth Dent 39,128-1987
14 Lombardi R The principles of visual perception ond their clinical application to denture esthetics J prosthDent 29,358-1973
REFERENCE

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 41
AbstraktGjatë proçesit të polimerizimit poli-metil-metakrilati pëson një tkurrje kimike, e cila shkakton pasaktësi dimensionale në protezat e përfunduara. Nëpërmjet metodes se polimerizimit me presion tkurrja e rezinës kompensohet nga presimi i materialit te shtresave te siperme.
Qëllimi i studimit: Krahasimi i protezave tradicionale totale me protezat SR-Ivocap lidhur me qëndrueshmërine, funksionin, ruajtjen e okluzionit të balancuar, dekubituset, interferencat, stomatitet protetike, fortësine etj. Materiali dhe metoda: Gjatë një periudhë 5 vjeçare, u trajtuan me proteza totale të lëvizshme 245 paciente. Pacientët u ndanë në dy grupe: në grupin e parë u përfshinë 133 pacientë të trajtuar me proteza totale të realizuara me sistemin SR Ivocap; grupi i dytë me 112 pacientë, të trajtuar me proteza totale tradicionale. Në ekzaminimet e realizuara menjëherë pas aplikimit të protezave, si dhe pas 1, 2, 3 dhe 5 vitesh, u krahasuan dhe u vlerësuan parametrat: 1. Rritja e lartësisë së okluzionit (0,8-2,5mm) 2. Paratakimet , 3. Dekubituset 4. Qëndrueshmëria, 5. Stomatitet protetike dhe kandidoza etj.
Rezultatet: Nga kontrollet periodike, në protezat SR-Ivocap u vu re qëndrueshmëria shumë e mirë në 33,1% të pacientëve, rritja e lartësisë së okluzionit në 0% të rasteve, stomatiti protetik në 16.5%, interferencat në 9,7%, thyerjet e protezave në 0,8 %; krahasuar me protezat e zakonshme ku qëndrueshmëria ishte shumë e mirë në 19,7% të pacientëve; rritja e lartësisë së okluzionit në 52,6% , dekubituset në 41,9%, stomatiti protetik në 37,3%, interferencat në 81,25% , thyerjet e protezave në 19,9 % .
Konkluzionet: Nga analiza e rezultateve, konkludojmë që protezat me SR-Ivocap kanë epërsi në të gjitha parametrat, krahasuar me protezat tradicionale. Sistemi SR-Ivocap është metoda më e mirë për të arritur perfeksionin në protezat dentare.
Prof. Assoc. Edit Xhajanka, D.M.Sc Koço Gjilo, Dr. Neada Hysenaj, Prof. Assoc. Merita Bardhoshi, D.M.Sc. Gerta Kaçani
Krahasimi i metodës së zakonshme të polimerizimit kundrejt metodës së injektimit me presion SR-Ivocap
Fakulteti i Mjekësisë Dentare, Departamenti i Protetikës
FJALËT KYÇE:
polimerizimi,
injektim
me presion,
metoda
konvencionale,
dekubituse,
interferenca.
HyrjePoli-metil-metakrilati (PMMA) është materiali kryesor
i përdorur për bazën e protezave (1,2,3,11). Ky material ka veti fi zike optimale, estetike të lartë dhe toksicitet relativisht të ulët. Polimerizimi i rezinës mund të bëhet me metoda të ndryshme, ku më e perdorura është mënyra tradicionale e polimerizimit. (2,4). Por me këtë metodë eshtë e pashmangshme tkurrja e materialit, (Fig.1) e cila con në ndryshime dimensionale dhe pasaktësi të bazës së protezës dhe të okluzionit, të dokumentuara në shumë studime. (1,4,7) (Fig.2). Vetitë mekanike të materialit varen nga lloji i materialit dhe teknikat e përdorura. Per te shmangur pasaktesite dhe imprecizionet e metodës tradicionale të polimerizimit, u përpunua teknika e injektimit me presion. Në 1942, Pryor
(2) zhvilloi teknikën me injektim, me qëllim shmangien e efekteve negative të metodës tradicionale. Grunewald, në 1952, studoi teknikën e përdorur nga Pryor, duke konkluduar se kjo metodë nuk shfaqte avantazhe statistikisht të rëndësishme krahasuar me metodën tradicionale (2).
Gjatë polimerizimit proteza pëson një deformim
sferik, si pasojë e tkurrjes së materialit gjatë forcimit (1, 9,11,17) (Fig.2). Problemet e krijuara si pasojë e tkurrjes në metodën tradicionale të polimerizimit janë: paratakime
a b
Fig.1- Ngritja e lartësisë së okluzionit dhe paratakimet e krijuara pas polimerizimit me teknikën konvencionale;
a-proteza e modeluar me dyllë, b-ndryshimi i raporteve të okluzionit dhe i lartësisë së okluzionit pas polimerizimit

Revista Stomatologjike Shqiptare42
në okluzion, përputhje jo preçize e sipërfaqes mukozale të protezës me mukozën e fushës protetike , ngritje e lartësisë së okluzionit, (7, 8) strukturë johomogjene ose poroze e materialit, (14,18) ngacmim kimik i mukozës nga teprica të monomerit, (1) etj.
Qëllimi i studimit: Në studimin tonë kemi patur si qëllim konstruktimin e protezave sa më preçise lidhur me ruajtjen e okluzionit të balancuar bilateral pas polimerizimit, puthitjen maksimale me mukozën e fushës protetike, preçizionin në okluzion lidhur me paratakimet dhe ngritjen e lartësisë së okluzionit, dekubituset dhe lindjen e stomatiteve protetike dhe kandidozës, cilësitë fi ziko-kimike të rezinës etj. Gjithashtu, kemi patur qëllim krahasimin e këtyre parametrave në proteza të polimerizuara me metodën tradicionale dhe në proteza të polimerizuara me metodën e injektimit me presion të plastmasës, duke treguar metodën më efi kase.
Materiali dhe metoda: Në varësi të këtyre qëllimeve, u protezuan me proteza
totale dhe u studiuan për një periudhë 6-vjeçare 245 pacientë me grupmosha 35-50 vjeç, 50- 65 vjeç, mbi 65 vjeç, (mosha mesatare 57 vjeç). Pacientët i grupuam në dy grupe:
Në grupin e parë u përfshinë 133 pacientë të
Fig.2- a,b,c- Deformimi sferik i protezës nga polimerizimi konvencional (Sipas Korber)
Fig.3. Sistemi SR-Ivocap dhe polimerizimi me shtresa nen presion
protezuar me proteza totale të polimerizuara me metodën e injektimit me presion. Ne përzgjodhëm metodën SR-Ivocap për polimerizimin me presion të plastmasës.
Në grupin e dytë u përfshinë 112 pacientë të protezuar me proteza totale të polimerizuara me metodën e zakonshme të polimerizimit (konvencionale).
Në analizën e faktorëve anatomikë dhe gradës së atrofi së në të dy grupet e pacientëve, ndryshimet kanë qënë statistikisht jo të rëndësishme (analiza atatistikore nëpërmjet testit Hi- katror). Në të dy grupet e pacientëve, marrja e masave anatomike dhe funksionale, si dhe përcaktimi i Okluzionit qendror u kryen në të njëjtën mënyrë dhe me të njëjtat materiale. Gjatë rreshtimit u ndoqën parimet e okluzionit të balancuar bilateral, në artikulatorin Stratos 200.
Në 20 pacientë, 10 për çdo grup, përgatitëm edhe patenta allçie para polimerizimit, për të krahasuar ndryshimet e pozicionit të dhëmbëve dhe deformimin e protezës pas zëvendësimit të dyllit me rezinë.
Në metodën tradicionale të polimerizimit u përdor rezina Triplex Hot. Gjatë ciklit të polimerizimit janë respektuar etapat e njëpasnjëshme të këtij cikli. Për mufl imin e protezave, në të dy metodat e polimerizimit, është përdorur tipi 3 i allçisë.(14,15,19,20)
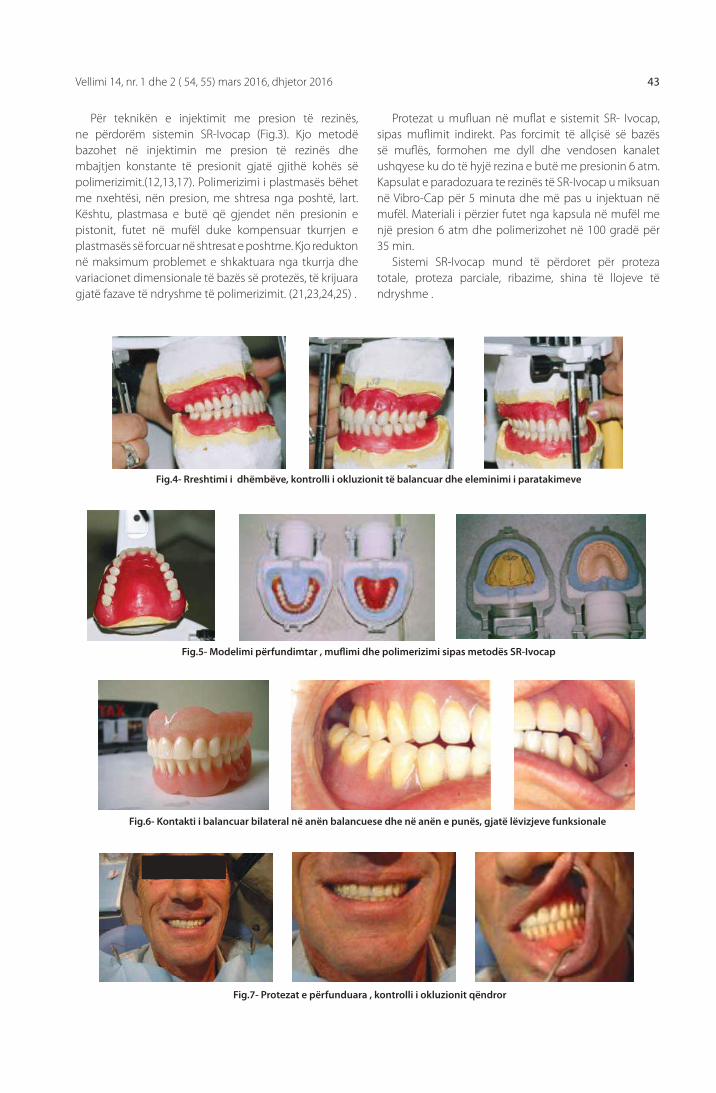
Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 43
Për teknikën e injektimit me presion të rezinës, ne përdorëm sistemin SR-Ivocap (Fig.3). Kjo metodë bazohet në injektimin me presion të rezinës dhe mbajtjen konstante të presionit gjatë gjithë kohës së polimerizimit.(12,13,17). Polimerizimi i plastmasës bëhet me nxehtësi, nën presion, me shtresa nga poshtë, lart. Kështu, plastmasa e butë që gjendet nën presionin e pistonit, futet në mufël duke kompensuar tkurrjen e plastmasës së forcuar në shtresat e poshtme. Kjo redukton në maksimum problemet e shkaktuara nga tkurrja dhe variacionet dimensionale të bazës së protezës, të krijuara gjatë fazave të ndryshme të polimerizimit. (21,23,24,25) .
Protezat u mufl uan në mufl at e sistemit SR- Ivocap, sipas mufl imit indirekt. Pas forcimit të allçisë së bazës së mufl ës, formohen me dyll dhe vendosen kanalet ushqyese ku do të hyjë rezina e butë me presionin 6 atm. Kapsulat e paradozuara te rezinës të SR-Ivocap u miksuan në Vibro-Cap për 5 minuta dhe më pas u injektuan në mufël. Materiali i përzier futet nga kapsula në mufël me një presion 6 atm dhe polimerizohet në 100 gradë për 35 min.
Sistemi SR-Ivocap mund të përdoret për proteza totale, proteza parciale, ribazime, shina të llojeve të ndryshme .
-
- -
- -
- - -
Fig.4- Rreshtimi i dhëmbëve, kontrolli i okluzionit të balancuar dhe eleminimi i paratakimeve
Fig.5- Modelimi përfundimtar , mufl imi dhe polimerizimi sipas metodës SR-Ivocap
Fig.6- Kontakti i balancuar bilateral në anën balancuese dhe në anën e punës, gjatë lëvizjeve funksionale
Fig.7- Protezat e përfunduara , kontrolli i okluzionit qëndror
-
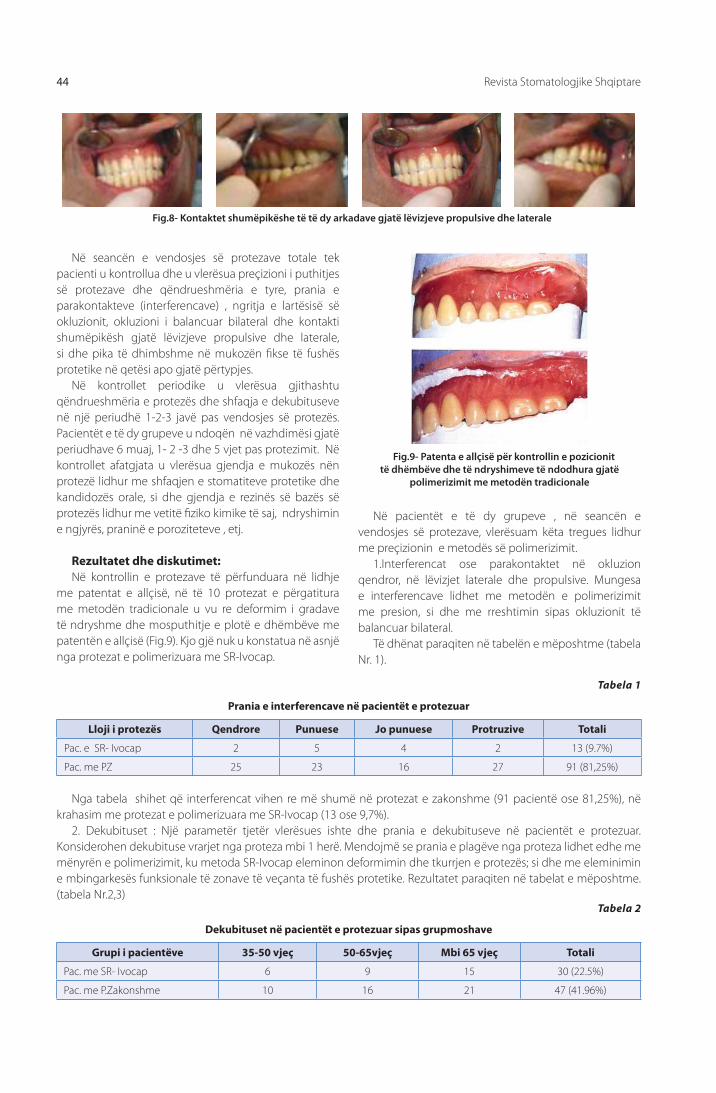
Revista Stomatologjike Shqiptare44
Në seancën e vendosjes së protezave totale tek pacienti u kontrollua dhe u vlerësua preçizioni i puthitjes së protezave dhe qëndrueshmëria e tyre, prania e parakontakteve (interferencave) , ngritja e lartësisë së okluzionit, okluzioni i balancuar bilateral dhe kontakti shumëpikësh gjatë lëvizjeve propulsive dhe laterale, si dhe pika të dhimbshme në mukozën fi kse të fushës protetike në qetësi apo gjatë përtypjes.
Në kontrollet periodike u vlerësua gjithashtu qëndrueshmëria e protezës dhe shfaqja e dekubituseve në një periudhë 1-2-3 javë pas vendosjes së protezës. Pacientët e të dy grupeve u ndoqën në vazhdimësi gjatë periudhave 6 muaj, 1- 2 -3 dhe 5 vjet pas protezimit. Në kontrollet afatgjata u vlerësua gjendja e mukozës nën protezë lidhur me shfaqjen e stomatiteve protetike dhe kandidozës orale, si dhe gjendja e rezinës së bazës së protezës lidhur me vetitë fi ziko kimike të saj, ndryshimin e ngjyrës, praninë e poroziteteve , etj.
Rezultatet dhe diskutimet:Në kontrollin e protezave të përfunduara në lidhje
me patentat e allçisë, në të 10 protezat e përgatitura me metodën tradicionale u vu re deformim i gradave të ndryshme dhe mosputhitje e plotë e dhëmbëve me patentën e allçisë (Fig.9). Kjo gjë nuk u konstatua në asnjë nga protezat e polimerizuara me SR-Ivocap.
Fig.8- Kontaktet shumëpikëshe të të dy arkadave gjatë lëvizjeve propulsive dhe laterale
Fig.9- Patenta e allçisë për kontrollin e pozicionit të dhëmbëve dhe të ndryshimeve të ndodhura gjatë
polimerizimit me metodën tradicionale
Në pacientët e të dy grupeve , në seancën e vendosjes së protezave, vlerësuam këta tregues lidhur me preçizionin e metodës së polimerizimit.
1.Interferencat ose parakontaktet në okluzion qendror, në lëvizjet laterale dhe propulsive. Mungesa e interferencave lidhet me metodën e polimerizimit me presion, si dhe me rreshtimin sipas okluzionit të balancuar bilateral.
Të dhënat paraqiten në tabelën e mëposhtme (tabela Nr. 1).
Tabela 1
Prania e interferencave në pacientët e protezuar
Lloji i protezës Qendrore Punuese Jo punuese Protruzive Totali
Pac. e SR- Ivocap 2 5 4 2 13 (9.7%)
Pac. me PZ 25 23 16 27 91 (81,25%)
Nga tabela shihet që interferencat vihen re më shumë në protezat e zakonshme (91 pacientë ose 81,25%), në krahasim me protezat e polimerizuara me SR-Ivocap (13 ose 9,7%).
2. Dekubituset : Një parametër tjetër vlerësues ishte dhe prania e dekubituseve në pacientët e protezuar. Konsiderohen dekubituse vrarjet nga proteza mbi 1 herë. Mendojmë se prania e plagëve nga proteza lidhet edhe me mënyrën e polimerizimit, ku metoda SR-Ivocap eleminon deformimin dhe tkurrjen e protezës; si dhe me eleminimin e mbingarkesës funksionale të zonave të veçanta të fushës protetike. Rezultatet paraqiten në tabelat e mëposhtme. (tabela Nr.2,3)
Tabela 2
Dekubituset në pacientët e protezuar sipas grupmoshave
Grupi i pacientëve 35-50 vjeç 50-65vjeç Mbi 65 vjeç Totali
Pac. me SR- Ivocap 6 9 15 30 (22.5%)
Pac. me P.Zakonshme 10 16 21 47 (41.96%)

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 45
Tabela 3
Dekubituset në pacientët e të dy grupeve
Grupi i pacientëve Pac me dekubituse % Totali (Nr)
Pacientë me Proteza SR-Ivocap 30 22.5 % 133
Pacientë me Proteza të Zakonshme 47 41.96 % 112
Totali i pacientëve 77 31.42 % 245
protezës janë shumë të pakta. Sipas autorëve tanë (Toti, Koçi) frakturat e protezave të zakonshme janë vërejtur në 20.2 % të rasteve. Në studimin tone patëm reultatet e mëposhtme: thyerje të protezave të zakonshme në 19 pacientë ose 19,9 %, përkundrejt 1 thyerje ose 0,8% në protezat SR-Ivocap.
4. Rritja e lartësisë së okluzionit pas polimerizimit. Në praktikën e përditshme hasen shpesh probleme që lidhen me ngritjen e lartësisë së kafshimit pas polimerizimit. Edhe autorë të tjerë shqiptarë kanë vënë re ngritje të kësaj lartësie në shifrat 0.8-2.5mm ( 5, 7, 14). Me metodën e polimerizimit me presion eleminohet plotësisht ky problem. Në tabelën Nr.4 paraqitet krahasimi i problemeve të lidhura me metodën e polimerizimit. Në studimin tonë, në pacientët me proteza të zakonshme ky problem u konstatua në 59 raste (52.6%), ndërsa në metodën SR-Ivocap në 0%, pra në asnjë pacient. Sipas autorëve Korber dhe Ludvig, (12,13) rritja e dimensionit vertikal në protezat tradicionale është rreth 10 herë më e madhe (165μm) se sa në protezat e sistemit SR-Ivocap (18,6 μm) (Fig. 10).
Në tabelën 4 jepen në mënyrë të përmbledhur problematikat e hasura në të dy grupet e pacientëve, të lidhura me metodën e polimerizimit. Nga tabela shihet se proteza me SR-Ivocap siguron një okluzion të saktë edhe pas polimerizimit, pa ngritje të lartësisë së kafshimit, paratakime, pa deformim të bazës së protezës, pa lëvizje të dhëmbëve në mufël etj.
Shihet se në protezat me SR-Ivocap numri i dekubituseve është shumë më i ulët , i hasëm dekubituset në 30 pacientë (22.5%), në krahasim me pacientët me Proteza të zakonshme, në 47 pacientë (41.96%). Mendojmë se kjo lidhet drejtpërdrejt me mënyrën e polimerizimit. Protezat SR-Ivocap sigurojnë një komfort maksimal për pacientin, pasi reduktojnë mundësinë e dekubituseve. Kjo është pasojë e eleminimit të tkurrjes dhe deformimit pas polimerizimit, si dhe të shpërndarjes uniforme të presionit përtypës në të gjithë sipërfaqen mbështetëse. Shpërndarja uniforme e forcave (1,13,28) shmang mbingarkesën dhe dekubituset në pika të veçanta të fushës protetike. Të dhënat janë paraqitur në grafi kun 1.
3. Fortësia e protezës. Protezat e polimerizuara me presion janë proteza me një fortësi shumë të lartë, ato nuk thyhen dhe as nuk dëmtohen gjatë funksionit, si edhe nga forca jo normale, rënia në tokë etj.(1,11,12,13.) Dhëmbët artifi cialë krijojnë lidhje kimike të fortë me rezinën, duke qenë materiale të të njëjtit sistem. (12). Në protezat SR--Ivocap materiali ka një strukturë homogjene dhe një fortësi të lartë. Frakturat i hasem më shumë në protezat e zakonshme: në 5 pac. të shkaktuara nga vetë pacienti dhe në 14 pac, të shkaktuara vetvetiu gjatë funksionit. Në pacientët me proteza SR-Ivocap thyerjet e
Fig. 10- Rritja e lartësisë së okluzionit ne teknikën e zakonshme dhe në metodën SR-Ivocap
Dekubituset ne pacientet e protezuar
05
10152025
35-50 vjeç 50-65 vjeç Mbi 65vjeç
Mosha
Numri
Pacientë me BPS
Pacientë me PZ
Grafiku 1
Dekubituset në pacientët e protezuar, sipas grupmoshave

Revista Stomatologjike Shqiptare46
Tabela Nr. 4
Krahasimi i Metodave të Polimerizimit
Problemi i lidhur me polimerizimin Proteza me SR-Ivocap Proteza me Metodën e Zakonshme
Rritja e DVOQ (0,8-2,5mm) 0 0% 59 pacientë 52.6%
Paratakime në Okl.Qendror 4 pacientë 3% 25 pacientë 22.3%
Dekub +infl amacione gingive 30 pacientë 22,5% 47 pacientë 41.96%
Mospërputhje me mukozën 4 pacientë 3% 16 pacientë 14.2%
Thyerje të Prot.pas disa vitesh 1 pacient 0.8% 19 pacientë 19.9%
Gjendja e mukozes pas 2-5 vitesh
0 5
10 15 20
Stomatit Protetik
Tipi 1
Stomatit Protetik
Tipi 2
Stomatit Protetik
Tipi 3
Mukoza
Numri
Pacientë me proteza të zakonshme Pacientë me proteza SR –Ivocap
Nga përpunimi statistikor (sipas testit Hi-Katror), i rezultateve të problematikave të të dy metodave të polimerizimit, rezultoi se ndryshimi midis dy rezultateve është statistikisht shumë i rëndësishëm.
5. Stomatitet protetike dhe Kandidoza kronike: Gjatë kontrolleve afatgjatë pas 2-3-5 vitesh nga protezimi, në pacientët e protezuar vlerësuam edhe gjendjen e mukozës së fushës protetike. Efektet e protezës mbi mukozë varen nga materiali me të cilin përgatitet proteza, nga ndjekja me saktësi e procedurave teknologjike të përgatitjes, si dhe nga reaktiviteti individual i organizmit,
veçoritë e indeve të gojës dhe higjena e pacientit.(9,23). Ato vërehen shpesh në persona që kanë kohë që mbajnë proteza të lëvizshme, pra lidhen drejtpërdrejt me protezën dhe presionin që ajo ushtron, me mënyrën e konstruktimit si dhe me strukturën mikroskopike të materialit të protezës. (9,28). Pr oteza SR-Ivocap redukton në maksimum lindjen e stomatiteve protetike dhe kandidozës orale, si rezultatet i strukturës homogjene dhe pa porozitete të materialit të polimerizuar nën presion. (Fig. 11) . Rezultatet e vrojtimit jepen në tabelën 5 dhe ne Grafi kun 2.
Tabela 5
Gjendja e mukozës tek të protezuarit e të dy grupeve 2-5 vjet pas protezimit
Lloji i Stomatitit protetik Pac. me proteza të zakonshme Pac. me proteza SR – Ivocap
Stomatit Protetik Tipi I 17 (15.1%) 10 (7.5%)
Stomatit protetik Tipi II 9 ( 8%) 7 (5.3%)
Stomatit protetik Tipi III 16 (14.2%) 5 (3.7%)
Totali 44 (37.3%) 22 (16.5%)
Grafiku 2

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 47
Në pacientët me proteza SR-Ivocap, stomatitet protetike janë ndeshur më rrallë; në 22 pacientë (16,5%), krahasuar me metodën e zakonshme në të cilën janë hasur në 44 pacientë (37,3%). Mendojmë se kjo lidhet drejt per drejt me strukturën shumë homogjene dhe pa porozitete të materialit SR- Ivocap pas polimerizimit. (Fig. 11)
3- Paradozimi i materialit dhe përzierja në kapsulë eleminon kontaktin me monomerin. Janë të përjashtuara gabimet e mundshme të dozimit dhe kontaminimi i materialit.
4- Struktura mikroskopike e materialit është homogjene, gjë që ul mundësinë e ngacmimit të mukozës dhe lindjes së stomatiteve protetike dhe kandidozës orale (Fig.12).
5- Polimerizimi me nxehtësi dhe nën presion siguron shkallë maksimale të polimerizimit, lidhje të fortë kimike me rezinën e dhëmbëve dhe qëndrueshmëri të ngjyrës së rezinës.
6- Fortësia e materialit është shumë e madhe, gjë që parandalon thyerjet e protezës.
7- Procedura e polimerizimit është më e shkurtër se polimerizimi tradicional (rreth 1.5 orë).
Anët negativeSi anë negative është vetëm problemi i lidhjes së
vështirë të materialit të pllakës së protezës të përgatitur me SR-Ivocap, me rezinat vetëpolimerizuese apo me rezinat e zakonshme termo-polimerizuese, në rastet e ribazimeve direkte, indirekte apo të shtesave të dhëmbëve të veçantë (në protezat subtotale). Kur nuk zbatohen me përpikmëri rregullat dhe etapat e polimerizimit nuk do të thotë që proteza të mos thyhet; pra mund të ndodhë thyerja e saj (1, 11).
Nga rezultatet e analizës tonë arritëm në konkluzionin se protezat e përgatitura me metodën e injektimit me presion kanë parametra funksionalë shumë më të lartë se protezat e polimerizuara me metodën tradicionale. Përparësitë e sistemit SR-Ivocap qëndrojnë në ruajtjen e volumit të plastmasës, kompensimin e tkurrjes së saj gjatë forcimit dhe në strukturën homogjene të materialit. Sistemi SR-Ivocap është një nga sistemet më efi kase për të arritur perfeksionin në protezat e lëvizshme..
Fig.11-Struktura mikroskopike e materialit në metodën konvencionale dhe në metodën SR-Ivocap
Konkluzione:Duke u bazuar në rezultatet e të dy grupeve dhe
në analizën e tyre, si dhe në rezultatet e literaturës, përcaktuam këto avantazhe të sistemit të polimerizimit me presion, SR-Ivocap:
Proteza e polimerizuar sipas këtij sistemi paraqet këto përparësi:1- Siguron përputhje preçize të sipërfaqes së
brendshme të protezës me mukozën e fushës protetike, pa krijuar pika presioni dhe dekubituse në mukozë.
2- Nuk ka ngritje të lartësisë së kafshimit si dhe paratakime, që çojnë në ngrënien e dhëmbëve pas polimerizimit të protezës dhe reokluzion të saj.
REFERENCA
1. Edit Xhajanka- “Proteza Biofunksionale dhe Sistemi BPS ne Shqiperi”, 2014, 193-202
2. Jafar Gharechahi, Nafi seh Asadzadeh, Flexural Strength of Acrylic Resin Denture Bases Processed by Two Diff erent Methods, J Dent (Tehran). 2014 Jul; 11(4): 398-405.
3. Abby A, Kumar R, Shibu J, Chakravarthy R. Comparison of the linear dimensional accuracy of denture bases cured the by conventional method and by the neë press technique. Indian J Dent Res. 2011;22:200-4.
4. Venus H, Boening K, Peroz I. The eff ect of processing meth-ods and acrylic resins on the accuracy of maxillary dentures and toothless denture bases: an in vitro study. Quintes-sence Int. 2011;42:669-77.
5. Keraj F. Rritja e lartesise se okluzionit qendror ne protezat totale me metoden e zakonshme te polimerizimit. Revista Stomatologjike Shqiptare, 2005, 28-32.
6. Consani RL, Domitti SS, Rizzatti Barbosa CM, Consani S. Effect of commercial acrylic resins on dimensional accuracy of the maxillary denture base. Braz Dent J. 2002;13:57-60.
7. Nogueira SS, Ogle RE, Davis EL. Comparison of accuracy between compression and injection molded complete dentures. J Prosthet Dent. 1999;82:291-303.
8. Takamata T, Setcos JC. Resin denture bases: review of ac-curacy and methods of polymerization. Int J Prosthodont. 1989;2:555-62.
Revista Stomatologjike Shqiptare48
9. Zarb GA, Bolender CL, Carlsson GE. Boucher’s prosthodon-tic treatment for edentulous patients. Mosby; 2005. pp. 337-42.
10. Jackson AD, Lang BR, Wang RF. The infl uence of teeth on denture base processing accuracy. Int J Prosthodont. 1993;6:333-40.
11. R. Qafmolla, Njohuri materiale stomatologjike, 2010, 45-48
12. Trage R. Experience gained with the SR-lvocap system. Quintessence Int. 1980;11:1-6.
13. Schmidt KH. The SR-lvocap system and the structure of denture bases. Quintessenz. 1975;26:59-62.
14. Jackson AD, Grisius RJ, Fenster RK, Lang BR. Dimensional accuracy of two denture base processing methods. Int J Prosthodont. 1989;2:421-8.
15. Baydas S, Bayindir F, Akyil MS. Eff ect of processing variables (diff erent compression packing processes and investment material types) and time on the dimensional accuracy of polymethyl methacrylate denture bases. Dent Mater J. 2003;22:206-13.
16. Yunus N, Rashid AA, Azmi LL, Abu-Hassan MI. Some fl exural properties of a nylon denture base polymer. J Oral Rehabil. 2005;32: 65-71.
17. Garfunkel E. Evaluation of dimensional changes in com-plete dentures processed by injection-pressing and the pack-and-press technique. J Prosthet Dent. 1983;50:757-61.
18. Lee CJ, Bok SB, Bae JY, Lee HH. Comparative adaptation ac-curacy of acrylic denture bases evaluated by two diff erent methods. Dent Mater J. 2010;29:411-7. Epub 2010 Jul 28.
19. Keenan PL, Radford DR, Clark RK. Dimensional change in complete dentures fabricated by injection molding and microwave processing. J Prosthet Dent. 2003 Jan;89(1):37-44.
20. Wolfaardt J, Cleaton-Jones P, Fatti P. The infl uence of pro-cessing variables on dimensional changes of heat-cured poly (methyl methacrylate) J Prosthet Dent. 1996;55:518-25.
21. Nogueira SS, Ogle RE, Davis EL. Comparison of accuracy between compression- and injection-molded complete dentures. J Prosthet Dent. 1999;82:291-300.
22. Venus H, Boening K, Peroz I. The eff ect of processing meth-ods and acrylic resins on the accuracy of maxillary dentures and toothless denture bases: an in vitro study. Quintes-sence Int. 2011;42:669-7.
23. Consani RL, Domitti SS, Rizzatti Barbosa CM, Consani S. Ef-fect of commercial acrylic resins on dimensional accuracy of the maxillary denture base. Braz Dent J. 2002;13:57-60.
24. Nogueira SS, Ogle RE, Davis EL. Comparison of accuracy be-tween compression and injection molded complete den-tures. J Prosthet Dent. 1999;82:291-303.
25. Miessi AC, Goiato MC, Santos DM, Dekon SF, Okida RC. In-fl uence of storage period and eff ect of diff erent brands of acrylic resin on the dimensional accuracy of the maxillary denture base. Braz Dent J. 2008;19:204-8.
26. Duymus ZY, Yanikoglu ND. The investigation of solubility values, water sorption and bond strength of auto-poly-merising and heat polymerizing acrylic resin materials. Eur J Prosthodont Restor Dent. 2006;14:116-20.
27. Parvizi A, Lindquist T, Schneider R, Williamson D, Boyer D, Dawson DV. Comparison of the dimensional accuracy of injection-molded denture base materials to that of conventional pressure-pack acrylic resin. J Prosthodont. 2004;13:83-9.
28. Kivovics P., Jahn M., Borbely J.,- Frequency and location of traumatic ulcerations following placement of complete dentures. Int J Prosthod. 7-8/2007.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 49
AbstractPoly-methyl methacrylate is susceptible to chemical shrinkage during polymerization. Considerable inaccuracy in the fi nished prosthesis is generally the result . SR-Ivocap system is a special procedure which fully compensates such shrinkage.
The aim of the study is to compare the Sr-Ivocap prostheses with conventional total prosthesis regarding the parameters of stability, function of the prosthesis, reaching the balanced occlusion, decubitis, interferences, prosthetic stomatitis, strength and mechanical stability of prosthesis, esthetics etc.
Material and method: For a 5-years period we prepared total prosthesis to 245 patients and we observed them. The patients are divided into two groups: the fi rst group included 133 patients with SR-Ivocap prosthesis; the second group, 112 patients with conventional polymerization total prosthesis. Based on the medical check of patients, immediately the prosthesis implementation and after a 1-2-3 and 5 year period, we compared the results of the prosthesis implementation process and prosthesis function in the 2 groups. The treatment results are evaluated based on some criteria. 1-Increase of vertical occlusion dimension (0,8-2,5mm); 2-Pressure points ( pre contacts - interferences ) 3-Decubitusis and gingiva infl ammations; 4-Low stability , no perfect fi t; 5-Prosthetic stomatitis and candidiasis etc.
Results: After the periodic controls the results show that in SR-Ivocap prosthesis the stability is very good in 33,1% of patients, against 19,7%; in conventional prosthesis; in SR-Ivocap dentures OVD increase in 0%, in traditional dentures 52,6%; In SR-Ivocap dentures decubitis were present in 22,5 %, in traditional dentures 41,9 %; prosthetic stomatitis were present in 16,5%, in SR-Ivocap dentures, against 37,3 % in traditional dentures; in SR-Ivocap dentures interferences were present in 9,7 %, while in traditional dentures interferences were 81,25 % ; denture fractures were 8,0 % in SR-Ivocap dentures and 19,9 % in traditional dentures.
Conclusions: From the results analyze we achieved the conclusion that SR-Ivocap prosthesis overlays in all the parameters, compared to conventional prosthesis.
The comparison between the conventional plasmas polymerization and SR-Ivocap method
KEYWORDS:
polymerization,
injection with
pressure,
conventional
method,
decubitis,
interference.
IntroductionThe majority of denture bases are fabricated using
poly methyl- methacrylate (PMMA). These materials have optimal physical properties and excellent esthetics with relatively low toxicity. (1,2,3,11). Compression molding with heat activation in a water bath for resin polymerization is the conventional method to process dentures.(2,4). However, shrinkage and dimensional change of denture bases during resin polymerization is unavoidable and has been well documented (1,4,7). (Fig.1, 2). Mechanical behavior of the denture base, including fl exural strength, depends on the type of the material and even on processing techniques. Therefore, acrylic resins and processing methods have been modifi ed to improve physical and chemical properties of denture bases. One example is the introduction of injection-molding technique. In 1942, Pryor (2) introduced the injection-molding technique to overcome the adverse eff ects of compression molding.
a b
Fig.1- Increasing vertical dimension and interferences created after polymerization in the traditional technique; a-dental
modeling wax, b-changes in occlusion after polymerization
Prof. Assoc. Edit Xhajanka, D.M.Sc Koço Gjilo, Dr. Neada Hysenaj, Prof. Assoc. Merita Bardhoshi, D.M.Sc. Gerta Kaçani
Faculty of Dental Medicine, Department of Prosthodontics

Albanian Stomatological Journal50
Fig.2- a ,b,c, Denture spherical deformation from traditional polymerization (According to Korber)
Fig.3. SR-Ivocap System
two groups: The fi rst group included 133 patients, treated with
complete removable dentures constructed with SR-Ivocap system; the second, with 112 patients, treated with complete removable dentures constructed with the traditional system.
Based on the analyze of anatomical factors and bone resorption grade, no statistical differences were noticed between the two groups. The statistical evaluation was made through a Hi-square test. The same technique and the same materials were used for anatomical and functional impressions, centric occlusion recordings for both groups of patients. The principles of bilateral balanced occlusion were followed during the teeth set-up, in Stratos 200 Articulator.
Plaster moldings were constructed for 20 patients, 10 for each group, to identify teeth position changes after polymerization. The Triplex Hot resin was used in the traditional way of polymerization. The cycle of polymerization was realized under the manufacturer’s instructions, and each step of the cycle was precisely followed. In the fl asking procedure, dental plaster type 3 was used (14,15,19). System SR-Ivocap was used as the technique of resin injection. This technique is based on resin injection with pressure (Fig.3).
According to Korber, prostheses undergo to a spherical deformation, as a result of resin shrinkage during the polymerization process (1,9,11,17) (Fig.2). The negative eff ects of traditional method are: interferences in occlusion, low fi t of inner denture surface with mucosal surface, the increase of vertical dimension, porosity of material,(14,18) chemical irritation of mucosa from free monomer,(1) etc.
The aim of the study: The construction of total prosthesis as effi ciently as
possible and the comparison with conventional total prosthesis regarding the parameters of stability and the function of the prosthesis, reaching the balanced occlusion, decubitis, interferences, prosthetic stomatitis, strength and mechanical stability of prosthesis, esthetics etc. Also, the comparison of these parameters for the traditional technique and resin injection technique, identifying the most effi cient method.
Materials and methods:245 patients were treated with total removable
dentures and were followed for a 5-year period. They were divided into three age-groups from 35-50 years old, 50-65 years old and over 65 years old (the average age was 57 years old). The patients were divided into
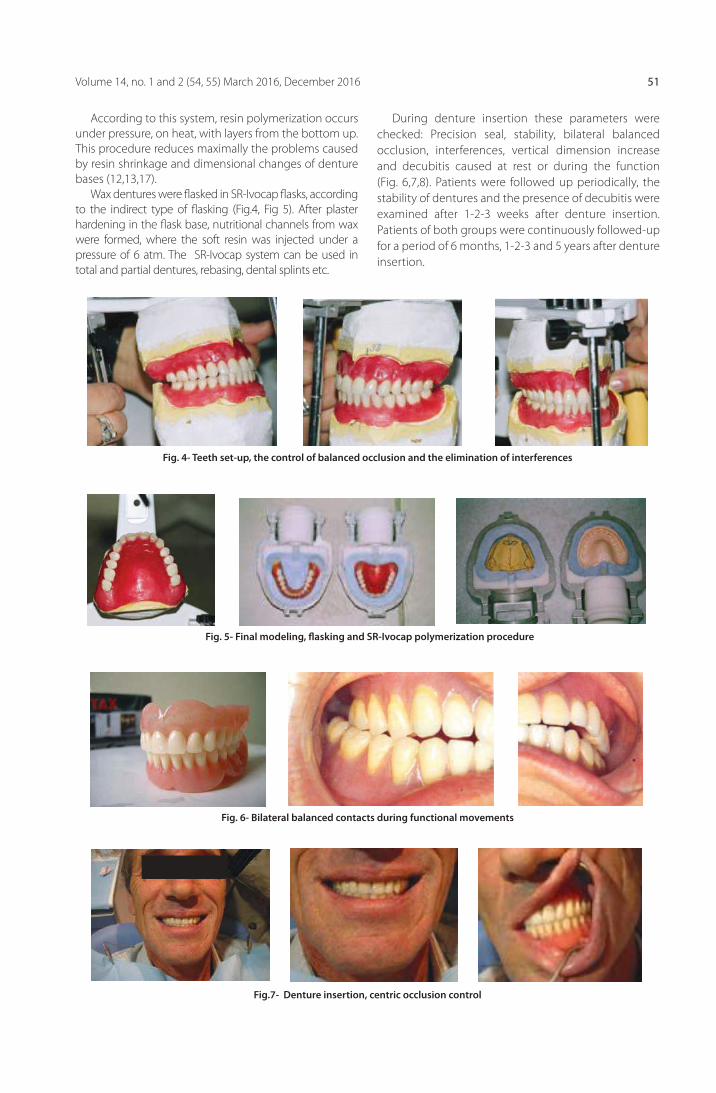
Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 51
According to this system, resin polymerization occurs under pressure, on heat, with layers from the bottom up. This procedure reduces maximally the problems caused by resin shrinkage and dimensional changes of denture bases (12,13,17).
Wax dentures were fl asked in SR-Ivocap fl asks, according to the indirect type of fl asking (Fig.4, Fig 5). After plaster hardening in the fl ask base, nutritional channels from wax were formed, where the soft resin was injected under a pressure of 6 atm. The SR-Ivocap system can be used in total and partial dentures, rebasing, dental splints etc.
-
- -
- - -
Fig. 4- Teeth set-up, the control of balanced occlusion and the elimination of interferences
Fig. 5- Final modeling, fl asking and SR-Ivocap polymerization procedure
Fig. 6- Bilateral balanced contacts during functional movements
Fig.7- Denture insertion, centric occlusion control
- - -
During denture insertion these parameters were checked: Precision seal, stability, bilateral balanced occlusion, interferences, vertical dimension increase and decubitis caused at rest or during the function (Fig. 6,7,8). Patients were followed up periodically, the stability of dentures and the presence of decubitis were examined after 1-2-3 weeks after denture insertion. Patients of both groups were continuously followed-up for a period of 6 months, 1-2-3 and 5 years after denture insertion.

Albanian Stomatological Journal52
A careful examination of mucosa for the presence of prosthetic stomatitis or oral candidiasis was realized. The physical and chemical properties of denture base resin, color change and porosity were also examined.
Results and discussions:Based on the examination of plaster molding, after
traditional denture polymerization, diff erent grades of deformations and no total adhesion of teeth in the plaster molding was noticed (Fig.9). These phenomena were not observed in the SR- Ivocap dentures.
In denture insertion phase these parameters were examined, assessing the accuracy of the way of polymerization:
1. Interferences in centric occlusion, in lateral and propulsive movements.
The lack of interferences is related to the way of polymerization with pressure and the way of teeth alignment, according to bilateral balanced occlusion. The data are in the table 1.
Fig. 8- Multi-points contacts of the two jaws during propulsive and lateral movements
Fig. 9- The examination of plaster molding after traditional denture polymerization
Tab. 1
The presence of interferences
Interferences Centric Interferences
Working Interferences
Non-working Interferences
ProtrusiveInterferences Total
SR- Ivocap Prosthesis 2 5 4 2 13 (9.7%)
Traditional Prosthesis 25 23 16 27 91 (81,25%)
Based on the table, the interferences are more often in traditional dentures (91 patients or 81,25%), compared to
SR-Ivocap dentures (13 patients or 9,7%).
2. Decubitis: Another assessor parameter is the presence of decubitis to denture wearing patients. We think that the presence
of decubitis is closely related to the way of polymerization, where the SR-Ivocap method eliminates deformation and denture shrinkage (1,3,4,28). It also eliminates the overloading of certain areas of prosthetic fi eld. The results are in the table 2 and table 3:
Tab. 2
Decubitis in prosthesis-patients according to their age
The group of patients 35-50 years old 50-65 years old Over 65 years old Total
SR- Ivocap Prosthesis 6 9 15 30 (22.5%)
Traditional Prosthesis 10 16 21 47 (41.96%)
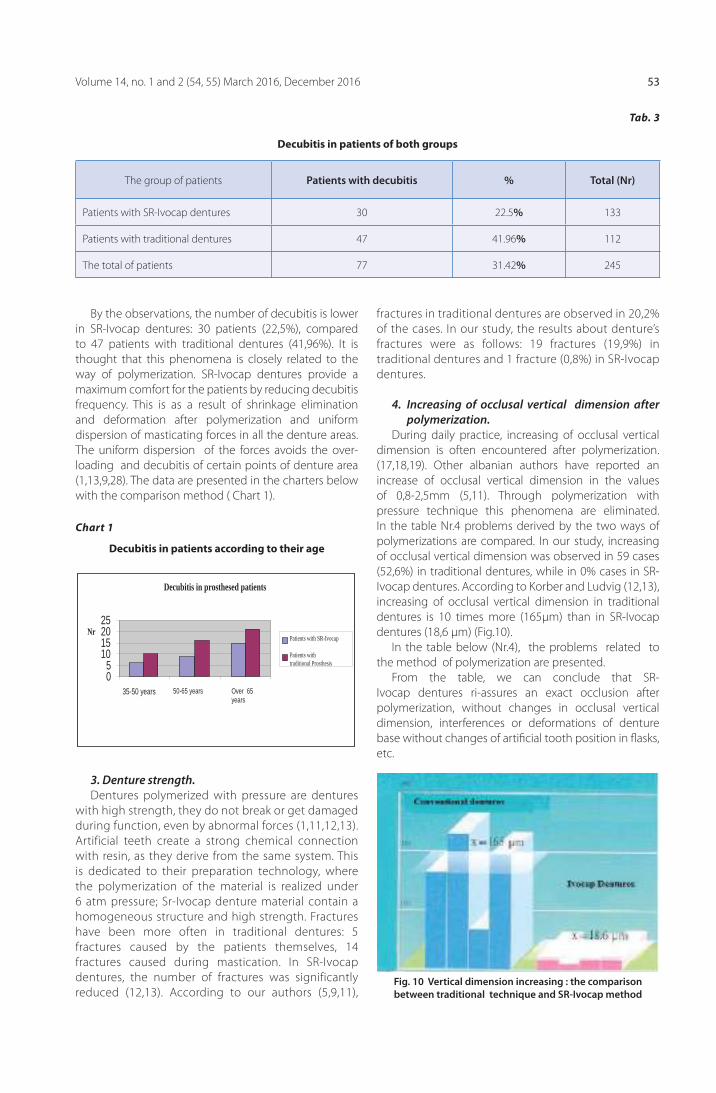
Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 53
Decubitis in prosthesed patients
05
10152025
35-50 years 50-65 years Over 65years
NrPatients with SR-Ivocap
Patients with traditional Prosthesis
Tab. 3
Decubitis in patients of both groups
The group of patients Patients with decubitis % Total (Nr)
Patients with SR-Ivocap dentures 30 22.5% 133
Patients with traditional dentures 47 41.96% 112
The total of patients 77 31.42% 245
By the observations, the number of decubitis is lower in SR-Ivocap dentures: 30 patients (22,5%), compared to 47 patients with traditional dentures (41,96%). It is thought that this phenomena is closely related to the way of polymerization. SR-Ivocap dentures provide a maximum comfort for the patients by reducing decubitis frequency. This is as a result of shrinkage elimination and deformation after polymerization and uniform dispersion of masticating forces in all the denture areas. The uniform dispersion of the forces avoids the over-loading and decubitis of certain points of denture area (1,13,9,28). The data are presented in the charters below with the comparison method ( Chart 1).
Fig. 10 Vertical dimension increasing : the comparison between traditional technique and SR-Ivocap method
Chart 1
Decubitis in patients according to their age
3. Denture strength.Dentures polymerized with pressure are dentures
with high strength, they do not break or get damaged during function, even by abnormal forces (1,11,12,13). Artificial teeth create a strong chemical connection with resin, as they derive from the same system. This is dedicated to their preparation technology, where the polymerization of the material is realized under 6 atm pressure; Sr-Ivocap denture material contain a homogeneous structure and high strength. Fractures have been more often in traditional dentures: 5 fractures caused by the patients themselves, 14 fractures caused during mastication. In SR-Ivocap dentures, the number of fractures was significantly reduced (12,13). According to our authors (5,9,11),
fractures in traditional dentures are observed in 20,2% of the cases. In our study, the results about denture’s fractures were as follows: 19 fractures (19,9%) in traditional dentures and 1 fracture (0,8%) in SR-Ivocap dentures.
4. Increasing of occlusal vertical dimension after polymerization.
During daily practice, increasing of occlusal vertical dimension is often encountered after polymerization.(17,18,19). Other albanian authors have reported an increase of occlusal vertical dimension in the values of 0,8-2,5mm (5,11). Through polymerization with pressure technique this phenomena are eliminated. In the table Nr.4 problems derived by the two ways of polymerizations are compared. In our study, increasing of occlusal vertical dimension was observed in 59 cases (52,6%) in traditional dentures, while in 0% cases in SR-Ivocap dentures. According to Korber and Ludvig (12,13), increasing of occlusal vertical dimension in traditional dentures is 10 times more (165μm) than in SR-Ivocap dentures (18,6 μm) (Fig.10).
In the table below (Nr.4), the problems related to the method of polymerization are presented.
From the table, we can conclude that SR-Ivocap dentures ri-assures an exact occlusion after polymerization, without changes in occlusal vertical dimension, interferences or deformations of denture base without changes of artifi cial tooth position in fl asks, etc.

Albanian Stomatological Journal54
Mucosa situation after 2-5 years
0 5
10 15 20
ProstheticStomatitis
Type 1
Prosthetic Stomatitis
Type 2
ProstheticStomatitis
Type 3
Mucosa
Nr.
Patients with traditional dentures Patients with SR –Ivocapdentures
Tab. Nr.4
The comparison of methods of polymerization
Problems realated to polymerization Dentures with SR-Ivocap Traditional prosthesis
Increasing of vertical dimension (0,8-2,5mm) 0 patients 0% 59 patients 52.6%
Interferences in C.Occlusion 4 patients 3% 25 patients 22.3%
Decubitis+ gingiva infl ammation 30 patients 22,5% 47 patients 41.96%
No adaptibility with oral mucosa 4 patients 3% 16 patients 14.2%
Denture fracture after some years 1 patients 0.8% 19 patients 19.9%
From the statistical evaluation (according to Hi-Square test), the diff erence between the two diff erent methods of polymerization was statistically important.
5. Prosthetic stomatitis and chronic candidiasis: for a period of 2-3and 5 years after denture insertion, oral mucosa was carefully examined. Denture’s eff ects on oral mucosa depends on the type of material used,(24,25) the careful accuracy of technological procedures for denture preparation, (1,9,11) the individual reaction of the organism, (25,26) patient’s hygiene and oral tissue
features (9,23). Prosthetic stomatitis are classifi ed in three groups (according to Newton) : Pin- Point Hyperemia, Diff use Erythema, Nodular Type.
They are often present in denture wearing patients for a long time (9,17,19), so they are directly related to the denture and its pressure, the way of denture construction and microscopic structure of denture material (12,13). SR- Ivocap dentures reduces maximally prosthetic stomatitis and oral candidiasis, as a result of its polymerized material under pressure, which has homogeneous structure and no porosity.The results are presented in Tab. 5 and chart 2.
Chharrt 22
Tab. 5
The situation of mucosa in prosthesis-patients of the two groups 2-5 years after denture insertion
Types of Prosthetic Stomatitis Patients with traditional dentures Patients with SR – Ivocap dentures
Prosthetic Stomatitis Type I 17 (15.1%) 10 (7.5%)
Prosthetic Stomatitis Type II 9 ( 8%) 7 (5.3%)
Prosthetic Stomatitis Type III 16 (14.2%) 5 (3.7%)
Total 44 (37.3%) 22 (16.5%)

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 55
It is obvious the reduction of prosthetic stomatitis in SR- Ivocap dentures in 22 patients (16,5%), compared to the values in traditional dentures 44 patients (37,3%). It is thought this result because of the homogeneous structure, without porosity of SR-Ivocap material after polymerization. ( Fig 11)
or interferences, which cause teeth consumption after denture polymerizing and its re-occlusion
3. The predosing of material in capsules avoid the contact of monomer, which is irritating. The material contamination and possible mistakes in dosing polymer and monomer are avoided.
4. The microscopic structure of the material is homogeneous, without pores, by reducing so mucosa irritation and prosthetic stomatitis (associated or not with oral candidiasis).
5. The polymerization under 6 atm pressure and with heat assures strong chemical connection between denture base material and artifi cial teeth and stability of resin color.
6. Dentures have high strength, avoiding so denture’s fracture under diff erent functional and non-functional forces.
7. Polymerization procedure is shorter than traditional polymerization.
Negative sidesIn direct and indirect rebasing procedures or artifi cial
teeth adding in subtotal dentures there are diffi culties in chemical relation between the denture base material and auto-polymerizing resin or thermo-polymerizing resin. It is important to follow precisely the steps of polymerization, in order to avoid denture fractures. (1, 11).
From the analysis of the results we conclude that SR-Ivocap prosthesis overlays in all the parameters, compared to conventional prosthesis. The advantages of this system are mainly in maintaining the same resin volume, shrinkage compensation during polymerization and the homogeneous structure of the material. The SR-IVOCAP system is the best way to achieve perfection in dental prosthesis.
Fig.11 Microscopic structure of the material in the conventional method and in SR-Ivocap method
Conclusions.
The advantages of SR-Ivocap injection system based on the results of our study, but also based on the literature are:
1. A precise adaption of inner denture surface with oral mucosa, by creating the adequate retention and avoiding decubitis
2. There is no increase of occlusal vertical dimension
REFERENCES
1. Edit Xhajanka- “Proteza Biofunksionale dhe Sistemi BPS ne Shqiperi”, 2014, 193-202
2. Jafar Gharechahi, Nafi seh Asadzadeh, Flexural Strength of Acrylic Resin Denture Bases Processed by Two Diff erent Methods, J Dent (Tehran). 2014 Jul; 11(4): 398-405.
3. Abby A, Kumar R, Shibu J, Chakravarthy R. Comparison of the linear dimensional accuracy of denture bases cured the by conventional method and by the neë press technique. Indian J Dent Res. 2011;22:200-4.
4. Venus H, Boening K, Peroz I. The eff ect of processing meth-ods and acrylic resins on the accuracy of maxillary dentures and toothless denture bases: an in vitro study. Quintes-sence Int. 2011;42:669-77.
5. Keraj F. Rritja e lartesise se okluzionit qendror ne protezat totale me metoden e zakonshme te polimerizimit. Revista Stomatologjike Shqiptare, 2005, 28-32.
6. Consani RL, Domitti SS, Rizzatti Barbosa CM, Consani S. Effect of commercial acrylic resins on dimensional accuracy of the maxillary denture base. Braz Dent J. 2002;13:57-60.
7. Nogueira SS, Ogle RE, Davis EL. Comparison of accuracy between compression and injection molded complete dentures. J Prosthet Dent. 1999;82:291-303.
8. Takamata T, Setcos JC. Resin denture bases: review of ac-curacy and methods of polymerization. Int J Prosthodont. 1989;2:555-62.
9. Zarb GA, Bolender CL, Carlsson GE. Boucher’s prosthodon-tic treatment for edentulous patients. Mosby; 2005. pp. 337-42.
10. Jackson AD, Lang BR, Wang RF. The infl uence of teeth on denture base processing accuracy. Int J Prosthodont. 1993;6:333-40.

Albanian Stomatological Journal56
11. R. Qafmolla, Njohuri materiale stomatologjike, 2010, 45-48
12. Trage R. Experience gained with the SR-lvocap system. Quintessence Int. 1980;11:1-6.
13. Schmidt KH. The SR-lvocap system and the structure of denture bases. Quintessenz. 1975;26:59-62.
14. Jackson AD, Grisius RJ, Fenster RK, Lang BR. Dimensional accuracy of two denture base processing methods. Int J Prosthodont. 1989;2:421-8.
15. Baydas S, Bayindir F, Akyil MS. Eff ect of processing variables (diff erent compression packing processes and investment material types) and time on the dimensional accuracy of polymethyl methacrylate denture bases. Dent Mater J. 2003;22:206-13.
16. Yunus N, Rashid AA, Azmi LL, Abu-Hassan MI. Some fl exural properties of a nylon denture base polymer. J Oral Rehabil. 2005;32: 65-71.
17. Garfunkel E. Evaluation of dimensional changes in com-plete dentures processed by injection-pressing and the pack-and-press technique. J Prosthet Dent. 1983;50:757-61.
18. Lee CJ, Bok SB, Bae JY, Lee HH. Comparative adaptation ac-curacy of acrylic denture bases evaluated by two diff erent methods. Dent Mater J. 2010;29:411-7. Epub 2010 Jul 28.
19. Keenan PL, Radford DR, Clark RK. Dimensional change in complete dentures fabricated by injection molding and mi-crowave processing. J Prosthet Dent. 2003 Jan;89(1):37-44.
20. Wolfaardt J, Cleaton-Jones P, Fatti P. The infl uence of pro-cessing variables on dimensional changes of heat-cured poly (methyl methacrylate) J Prosthet Dent. 1996;55:518-25.
21. Nogueira SS, Ogle RE, Davis EL. Comparison of accuracy between compression- and injection-molded complete dentures. J Prosthet Dent. 1999;82:291-300.
22. Venus H, Boening K, Peroz I. The eff ect of processing meth-ods and acrylic resins on the accuracy of maxillary dentures and toothless denture bases: an in vitro study. Quintes-sence Int. 2011;42:669-7.
23. Consani RL, Domitti SS, Rizzatti Barbosa CM, Consani S. Ef-fect of commercial acrylic resins on dimensional accuracy of the maxillary denture base. Braz Dent J. 2002;13:57-60.
24. Nogueira SS, Ogle RE, Davis EL. Comparison of accuracy be-tween compression and injection molded complete den-tures. J Prosthet Dent. 1999;82:291-303.
25. Miessi AC, Goiato MC, Santos DM, Dekon SF, Okida RC. In-fl uence of storage period and eff ect of diff erent brands of acrylic resin on the dimensional accuracy of the maxillary denture base. Braz Dent J. 2008;19:204-8.
26. Duymus ZY, Yanikoglu ND. The investigation of solubility values, water sorption and bond strength of auto-poly-merising and heat polymerizing acrylic resin materials. Eur J Prosthodont Restor Dent. 2006;14:116-20.
27. Parvizi A, Lindquist T, Schneider R, Williamson D, Boyer D, Dawson DV. Comparison of the dimensional accuracy of injection-molded denture base materials to that of conventional pressure-pack acrylic resin. J Prosthodont. 2004;13:83-9.
28. Kivovics P., Jahn M., Borbely J.,- Frequency and location of traumatic ulcerations following placement of complete dentures. Int J Prosthod. 7-8/2007.

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 57
AbstraktMundësitë për zëvendësimin e mungesës së dhëmbëve këto vitet e fundit janë rritur shumë sidomos me rritjen e cilësisë së implanteve. Por, metdoda klasike me punim protetik fi ks mbetet mënyra kryesore në praktikën e përditshme. Nga ana tjetër proçedurat restorative ortopedike shoqërohen me heqje masive të dentinës së dhëmbëve intakt dhe për rrjedhojë ndikimi mbi pulpën e dhëmbit është i pashmangshëm.
Qëllimi i punimitVlerësimi I ndikimit të proçedurave restorative mbi dhëmbët vital bazuar në të d hënat radiologjike.Materiali dhe metodaPunimi u bazua në përzgjedhjen e rasteve me punime ortopedike ne 215 panoramike te paraqitur gjatë vitit 2014-2015 në klinikën e Albanian University.
RezultatetNë 215 panoramike u gjetën 233 dhëmbë shtyllë frontal dhe 310 molarë intakte. Pa ndryshime periapikale për dhëmbët frontalë 187 (80.2%) dhe 277 (89.3%) molarë.
DiskutimPërqindja më e lartë e ndërlikimeve vërehet te frontalët për shkak të trashësisë më të vogël të shtresës së dentinës në raport me molarët.
PërfundimePër parandalimin e ndërlikimeve të vonshme duhen vlerësuar me kujdes si trashësia e indeve të forta, mosha e pacientit dhepozicioni I dhëmbeve shtyllë në harkatë.
Prof. Dr. Pavli Kongo, Anis Thodhorjani
Ndërlikimet endodontike në dhëmbët shtyllë vital
Albanian University, Tirane
FJALËT KYÇE:
Proteza fi kse,
endodonti,
periapeks,
dekortikim
Mungesa e dhembeve ne harqet dentare esht nje problem funksional dhe estetik. Principi I zevendesimit te tyre eshte kthimi funksionit dhe estetikes me nje kosto minimale biologjike.
Megjithate arritjet ne parandalimin apo uljen e numrit te dhembe te hequr ende perqindja e pacienteve me mungesa te dhembeve eshte ne shifra te larta.
Metodat e zevendesimit kane evoluar megjithate metoda me e shpeshte qe ndeshim ne praktiken e perditshme eshte ajo klasike me ura fi kse metal-qeramike. Implantet jane akoma te parritshem per shumicen e pacienteve tone.
Por duhet theksuar se shume autore mendojne se “procedurat restorative protetik perfaqesojne nje risk te perhershem dhe me efekte negative mbi pulpen”, pasi ato shoqerohen me heqjen e nje sasie te konsiduerushem denine, sasi e cila varet nga shume faktore (mosha, lloji I defektit, okluzioni si dhe pozicioni I dhembeve shtyle ne harqet dentare). Per rrjedhoje irritimi I pulpes eshte I paevitueshem, mund te jete I shpejte, pacienti reagon me dhimbje e cila fl et per nje pulpe qe vuan. Por ngacmiety mund te jene te lehta e te durueshme nga ana e pacienteve e nderkoh jane ato qe nxisin fi llimisht nje nekrobioze e me pas nekrozen totale te pulpes e cila perfundon ne process krinik periapikal pas 2-3 vjetesh.
Materiali- MetodikaNisur nga konstatimet tona klinike e radiologjike
ne nderrmorem kete studim retrospektiv te 215
panoramikeve te pacienteve te paraqitur ne kliniken tone gjate periudhes 2015-2016. U perqendruam ne vleresimin e gjendjes se periapexit te dhembeve shtylle vital.
RezulatetPer te vleresuar me sakte ndikimin e procedurave
restorative protetike ne ndame 2 grupe. Fillimisht u analizua raporti idhembe shtylle me
trajtim endodontic me dhembet shtylle vital.
Tab. Nr.1
Nr. Total Te mjekuar Vital
Frontal 513 280-54.7% 233-45.3%
Molaret 550 240-43.6% 310-56.4%
Sic shihet nga tabela afersisht gjysma e dhembe shtylle I nenshtrohet mjekimit endodontic paraprak e kushtezuar per mendimin tone nga lloji I materialit qe ne perdorim Remanium CSR I cili nuk jep derdhje precise dhe kerkon dekortikim te thelle te kulteve. Atuore te huaj shifra te ulta per trajtim paraprak te dhembeve shtylle (7% Aber), Christensen 6% duke perdorur aliazhe fi snik te cilat nuk kerkojne dekortikim te thelle.

Revista Stomatologjike Shqiptare58
Tab.nr.2
Nr. Total Te mjekuar Vital
Frontal 233 187-80.2% 46-19.8%
Molaret 310 280-90.3% 30-9.7%

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 59
Nga te dhenat e tabeles e rezulton se diferenca eshte e ndjeshme, perqindja me e larte e nderlikimeve ne dhembet shtylle frontal lidhet me trashesine me te vogel te dentines ne dhembet frontal ne raport me molaret.
Diskutimi. Dekortikimi mbete nje process irrtimi I shpejt ose I
ngadalshem per pulpen e dhembit. Ecuria varet nga shume faktore por nder me kryesoret mbetet:
- Heqje mbi 0.3mm e dentines,
- Rritja e nrumit te kanalezave te ekspozuar
- Zgjerimi I lumenit te kanalezave dentianre ne drejtim te pulpes
(1), (2),(4)
1. Aber. S “Early endodontics complications- following fi xed prosthodontics restoration”international journal of den-tistry June 2010
2. Cohen S. “Pathways of the pulp” 2007
3. Goodcare Ch. “Clinical complication in fi xed prosthodon-tics” The journal of fi xed Prosthetic dentistry 2010
REFERENCA
4. Cromin R. “An update on fi xed prosthodontics” JADA, prill 1997
5. Seltzer-Bender “Principles and practice of endodontics” 2002
6. Walls. A “Crowns and extra coronal restorations- Endodon-tic considerations” B. Dental journey 2002
Shumica e autoreve I referohen nderlikimeve te hershme pas cimentimit. Nderkoh qe ka te tjere qe paraqesin qe nderlikimet deri ne 33%, 15 vjet pas cimentimit te ures fi kse. Ndersa sipas Seltzer ne dhembet vital ke rritje te numrit te nderlikimeve ne dhembet vital kemi rritje te numrit te nderlikimeve ne rreth 1%.
Perfundimet. Respektimi me rigorozitet I parimeve te preparimit,
perdoirmi I koronave provizore, jane garanci per vazhdimesi dhe jetegjatesine e ures fi kse metal porcelan.

Albanian Stomatological Journal60
AbstractOptions for replacing missing teeth in recent years have increased a lot especially with the increase of the quality of implants. But classic fi xed prosthetic is used mostly in daily practice.Preparation of vital tooth for fi xed restorations increases the risk of pulpal damage.
AimThe aim of this paper is to assess the impact of restorative procedures on vital teeth by means of radiological data.
Material and methods The material consistedin 215 panoramic x-rays with fi xed prostheticprosthesispresented during the 2014-2015 at the dental clinic Albanian University.
Results In 215 panoramic were found 233frontal teeth and 310 molarsvital. Without periapical changes incisors 187 (80.2%) and 277 (89.3%) molars.
Discussion The highest percentage of complications noted at the frontal region due to the smaller thickness of the layer of dentin compared with molars.
Conclusions To prevent late complications clinicians should carefully assess thickness of hard tissue, the patient’s age and tooth position in the arch.
Prof. Dr. Pavli Kongo, Anis Thodhorjani
Endodontic complications of vital abutment teeth
Albanian University, Tirane
KEYWORDS:
Fixed Partial
Dentures,
Endodontic
treatment,
periapical,
tooth
preparation
The lack of teeth in dental arches is a functional and aesthetic problem. The principle of replacing them is the return function and esthetics with a biological minimum cost.
However, advances in preventing or reducing the number of teeth, yet lifted the proportion of patients with lack of teeth it is in substantial numbers.
Replacement methods have evolved, however, methods of frequent encountered in everyday practice is classical fi xed metal-ceramic bridges. Implants are still unprocurable for the majority of our patients.
But it should be noted that many authors think that “restorative prosthetic procedures represent a permanent risk and negative eff ects on the pulp”, as they are associated with the removal of a considerable quantity of dentina, amount of which depends on many factors (age, type of defect, occlusion and the position of teeth in the dental arch). Consequently the pulp irritation is inevitable, can be fast, the patient responds to pain which is about a pulp suff ering. But we might have a light irritation at the beginning secondly a nekrobioze then the total necrosis of the pulp which ends in chronic periapical process after 2-3 years.
Material-methodGiven our clinical and radiological fi ndings we took
this retrospective study of 215 patients panoramic
featured in our clinic during the period 2015-2016. We focused on evaluation the situation of periapex of vital abutment tooth.
ResultTo evaluate accurately the impact of restorative
prosthetic procedures we shared two groups.Initially we analyzed the proportion of teeths with
endodontic treatment and vital teeth.
Tab. Nr.1
Total Nr. Endodontic Vital
Incisors 513 280-54.7% 233-45.3%
Molars 550 240-43.6% 310-56.4%
The table shows that approximately half the tooth bar is subjected to the preliminary endodontic treatment conditional our opinion on the type of material we use Remanium CSR which does not require precise pouring and deep preparation. Foreign authors have encountered low percentage of tooth of endodontic treatment (7% Aber), Christensen 6% because they use noble alloys.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 61
Tab.nr.2
Total Nr. Endodontic Vital
Incisors 233 187-80.2% 46-19.8%
Molars 310 280-90.3% 30-9.7%

Albanian Stomatological Journal62
The data of the table show that the diff erence is signifi cant, the highest percentage of complications in the incisor teeth is related to the thickness of dentin in the frontal teeth in relation to the molars.
DiscussionIrritation remains a low or fast process for the pulp
tooth. Performance depends on many factors but remains
among the most important:- Removal of the 0.3mm dentin,- Increase of the number of canals exposed- Expansion of the lumen of dentinar canals towards
pulp
1. Aber. S “Early endodontics complications- following fi xed prosthodontics restoration”international journal of den-tistry June 2010
2. Cohen S. “Pathways of the pulp” 2007
3. Goodcare Ch. “Clinical complication in fi xed prosthodon-tics” The journal of fi xed Prosthetic dentistry 2010
REFERENCES
4. Cromin R. “An update on fi xed prosthodontics” JADA, prill 1997
5. Seltzer-Bender “Principles and practice of endodontics” 2002
6. Walls. A “Crowns and extra coronal restorations- Endodon-tic considerations” B. Dental journey 2002
• (1), (2), (4)Most authors refer to early complications after
cementation. While others had implications that represent up to 33%, 15 years after the cementation of fi xed bridge. While according Seltzer in vital teeth have increased the number of complications in vital teeth have increased the number of complications in about 1%.
ConclusionsAdhering strictly to the principles of preparation, the
use of provisional crowns are guarantee of continuity and life of fi xed porcelain metal bridge.

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 63
AbstraktTermi Hypomineralizimi molar inciziv (MHI) është përdorur për herë të parë nga Weerheijm (2001) si “hypomineralizim me origjinë sistemike që prek 1-4molarët e parë permanent (PFMs) dhe që shoqërohet me prekjen edhe të incizivëve “.Në mars 2003 u realizua takimi i Athinës në të cilin u vendos emërtimi,defi nicioni dhe kriteret diagnostike të MHI.Kriteret për dignozën e MHI u dhanë nga Weerheijm (2003). Ato përfshijnë opacitetet asimetrike,shkatërrimin posteruptiv të smaltit,restaurimet atipike.Prevalenca e MHI në Europë varion nga 4% - 25%,në Tiranë në 1575 femijë të moshës 8-10 vjeç(2015)14%.Në studime të ndryshme si faktorë etiologjike autorët përmendin : infeksionet respiratore,komplikacionet perinatale , dioksinat,lindjet premature ose me peshë të vogël,çrregullime të metabolizmit të Ca dhe F,sëmundjet e fëmijërisë (otitis,tonsilitis,fruthi,rubeola etj),antibiotiket,ndotjen e mjedisit.Trajtimi i këtyre defekteve varet nga forma në të cilën ato shfaqen.
Qëllimi i këtij artikulli është të trajtojë faktorët etiologjike,shfaqjen klinike të defekteve morfologjike të MHI,diagnozën dhe trajtimin e këtyre lezioneve
Prof. Assoc. Etleva Droboniku (Qeli)1, Prof. Assoc. Dorjan Hysi1, Dr. Ina Droboniku2, Prof. Assoc. Çeliana Toti1,D.M.Sc. Enida Petro1
Hypomineralizimi Molar-Inciziv
1Fakulteti i Mjekësisë Dentare, Universiteti i Mjekësisë Tiranë; 2Klinika Dentare “Droboniku” Tiranë
FJALËT KYÇE:
hypomineralizi
m,molar,inciziv,
smalt,opacitet
HyrjeTermi hypomineralizim molar –inciziv (MHI) është
prezantuar për herë të parë në vitin 2001 nga Weer-heijm(1).Në kongresin e 6 të Akademisë Europiane të Dentistrisë Pediatrike(EADP) në Dublin (15-17 qershor 2002) iu kushtua një vëmendeje e madhe defekteve të mineralizimit të smaltit.Një nga konkluzionet e kongresit ishte se kishte te dhëna të pakta në lidhje me prevalencen e MHI në Europë ndërkohe që den-tistët sugjeronin se prevalenca e MHI ishte në rritje.Për të trajtuar këtë problem në dentistrinë pediatrike në mars 2003 u realizua takimi i Athinës në të cilin u vendos emërtimi,definicioni dhe kriteret diagnostike të MHI.
Sipas Weerheijm hypomineralizimi molar inciziv (MIH) është shfaqje klinike e defekteve morfologjike të smaltit që përfshijnë faqen okluzale të një ose më shumë molarëve permanente ose 1/3 incizale të incizivëve si rezultat i “hypomineralizimit me origjinë sistemike”(Athinë 2003) (2)
Ky defi nicion u zgjodh për të theksuar faktin që molarët janë gjithmonë të përfshirë në këtë anomali dhe ka një lidhje me opacitetet e kufi zuara në inciziv.
Në vitin 2009 nëInterim Seminar dhe Workshop për MHI në Helsinki u miratua me konsensus një dokument për prevalencën,diagnozën ,etiologjinë dhe trajtimin e femijëve dhe adoleshentëve me MHI(Lygidakiset al)(3).Ky dokument shërben si guidë për studimet dhe klinicistët në lidhje me MHI.
Prevalenca e MHI në Europë 4-25 % (4,5,6,7).Në Tirane në studimin e kryer në vitin 2015 në 1575 fëmije të grupmoshës 8-10 vjeç prevalenca ishte 14 % (8)
Me shpesh preken molarët e parë permanentë (2).Këto defekte mund të lokalizohen edhe te molarët e dytë të qumështit,kuspidet e kaninëve permanentë dhe molarët e dytë permanentë.(2)
Qëllimi i këtij artikulli panoramik është të përshkruaj diagnozën,karakteristikat klinike , prevalencën,faktorët etiologjik dhe menaxhimin klinik të MHI.
Hypomineralizimi i smaltit:Smalti është indi më i fortë i organizmit.Ka origjinë
ektodermale.Ai përbëhet nga 96% kripëra minerale dhe 4 % lëndë organike dhe ujë.Përbërsi kryesor i lëndës inorganike është kalçium hidroksiapatiti Ca10(PO4)6(OH)2.
Në sasi më të vogla ka karbonat kalçiumi,fosfat kalçiumi,karbonat magneziumi etj.Lënda organike e smaltit përbëhet kryesisht nga proteinat e smaltit: amelogenin,enamelin, ameloblastin,tuftelin.
Formimi i smaltit ndodh në dy stade.Në stadin e parë,stadin e sekretimit ameloblastet sekretojnë lëndën organike(proteinat) të smaltit. Matriksi i smaltit konsiston në proteinat e smaltit,karbohidrate dhe një sasi shumëtë vogël kristalesh kalçium hidroksiapatit.Në stadin e dytë ndodh mineralizimi i smaltit ,largohen proteinat dhe uji dhe precipitojnë me shumicë kriperat minerale.Ky proces quhet maturim. .Gjate maturimit ameloblastet nga qeliza prodhuese kthehen në qeliza transportuese duke larguar proteinat dhe ndihmuar transportin aktiv të kalçiumit dhe fosfatit në matriks.Pra ameloblastet jane qelizat specifi ke për maturimin e smaltit.Maturimi i smaltit konsiston në :
1. precipitimin e kristaleve të apatitit dhe kripërave minerale
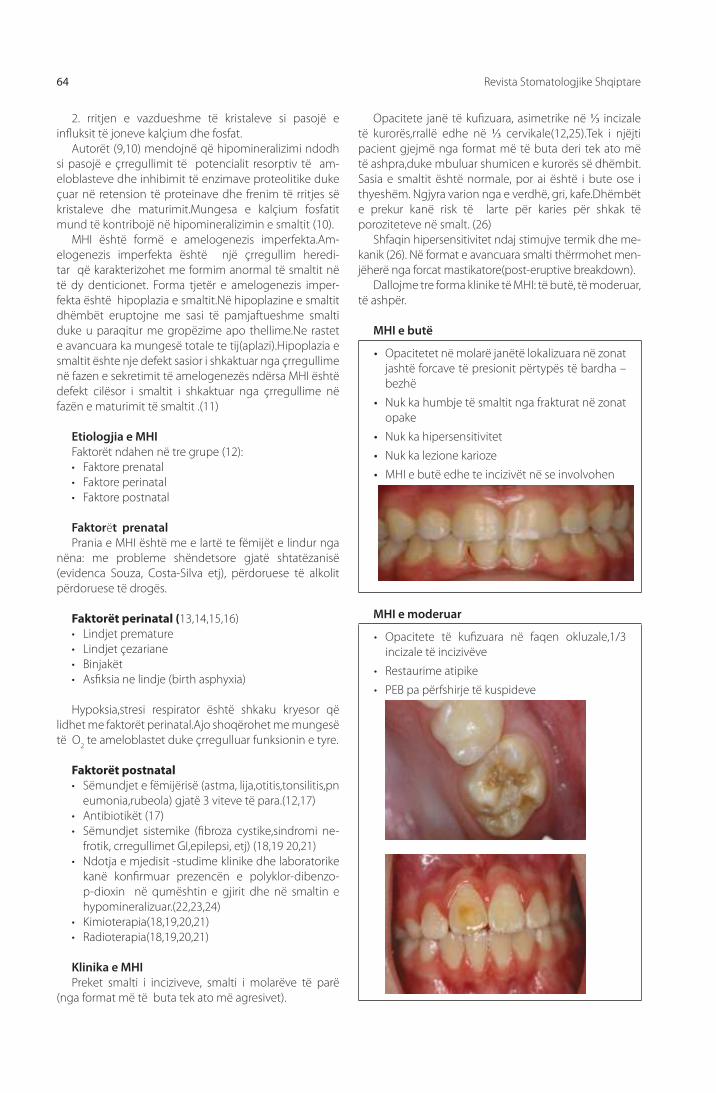
Revista Stomatologjike Shqiptare64
2. rritjen e vazdueshme të kristaleve si pasojë e infl uksit të joneve kalçium dhe fosfat.
Autorët (9,10) mendojnë që hipomineralizimi ndodh si pasojë e çrregullimit të potencialit resorptiv të am-eloblasteve dhe inhibimit të enzimave proteolitike duke çuar në retension të proteinave dhe frenim të rritjes së kristaleve dhe maturimit.Mungesa e kalçium fosfatit mund të kontribojë në hipomineralizimin e smaltit (10).
MHI është formë e amelogenezis imperfekta.Am-elogenezis imperfekta është një çrregullim heredi-tar që karakterizohet me formim anormal të smaltit në të dy denticionet. Forma tjetër e amelogenezis imper-fekta është hipoplazia e smaltit.Në hipoplazine e smaltit dhëmbët eruptojne me sasi të pamjaftueshme smalti duke u paraqitur me gropëzime apo thellime.Ne rastet e avancuara ka mungesë totale te tij(aplazi).Hipoplazia e smaltit ështe nje defekt sasior i shkaktuar nga çrregullime në fazen e sekretimit të amelogenezës ndërsa MHI është defekt cilësor i smaltit i shkaktuar nga çrregullime në fazën e maturimit të smaltit .(11)
Etiologjia e MHI Faktorët ndahen në tre grupe (12):• Faktore prenatal • Faktore perinatal• Faktore postnatal
Faktorët prenatal Prania e MHI është me e lartë te fëmijët e lindur nga
nëna: me probleme shëndetsore gjatë shtatëzanisë (evidenca Souza, Costa-Silva etj), përdoruese të alkolit përdoruese të drogës.
Faktorët perinatal (13,14,15,16)• Lindjet premature• Lindjet çezariane • Binjakët• Asfi ksia ne lindje (birth asphyxia)
Hypoksia,stresi respirator është shkaku kryesor që lidhet me faktorët perinatal.Ajo shoqërohet me mungesë të O2 te ameloblastet duke çrregulluar funksionin e tyre.
Faktorët postnatal• Sëmundjet e fëmijërisë (astma, lija,otitis,tonsilitis,pn
eumonia,rubeola) gjatë 3 viteve të para.(12,17)• Antibiotikët (17)• Sëmundjet sistemike (fi broza cystike,sindromi ne-
frotik, crregullimet GI,epilepsi, etj) (18,19 20,21)• Ndotja e mjedisit -studime klinike dhe laboratorike
kanë konfi rmuar prezencën e polyklor-dibenzo-p-dioxin në qumështin e gjirit dhe në smaltin e hypomineralizuar.(22,23,24)
• Kimioterapia(18,19,20,21)• Radioterapia(18,19,20,21)
Klinika e MHIPreket smalti i inciziveve, smalti i molarëve të parë
(nga format më të buta tek ato më agresivet).
Opacitete janë të kufi zuara, asimetrike në ⅓ incizale të kurorës,rrallë edhe në ⅓ cervikale(12,25).Tek i njëjti pacient gjejmë nga format më të buta deri tek ato më të ashpra,duke mbuluar shumicen e kurorës së dhëmbit.Sasia e smaltit është normale, por ai është i bute ose i thyeshëm. Ngjyra varion nga e verdhë, gri, kafe.Dhëmbët e prekur kanë risk të larte për karies për shkak të poroziteteve në smalt. (26)
Shfaqin hipersensitivitet ndaj stimujve termik dhe me-kanik (26). Në format e avancuara smalti thërrmohet men-jëherë nga forcat mastikatore(post-eruptive breakdown).
Dallojme tre forma klinike të MHI: të butë, të moderuar, të ashpër.
MHI e butë
• Opacitetet në molarë janëtë lokalizuara në zonat jashtë forcave të presionit përtypës të bardha –bezhë
• Nuk ka humbje të smaltit nga frakturat në zonat opake
• Nuk ka hipersensitivitet
• Nuk ka lezione karioze
• MHI e butë edhe te incizivët në se involvohen
MHI e moderuar
• Opacitete të kufi zuara në faqen okluzale,1/3 incizale të incizivëve
• Restaurime atipike
• PEB pa përfshirje të kuspideve

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 65
MHI e ashper
• Shkatërrim post eruptiv
• Karies në zonat edefektit
• Hipersensitivitet dentinar
• Destruksion i kurorës –involvim i pulpës
• Restaurime atipike defektoze
• Probleme estetike
Diagnoza e MHIMosha 8 vjeç është mosha me adekuate për të ekzaminuar në lidhje me MHI (kanë eruptuar 4 molarët permanent
dhe 8 incizivët) (2).Ekzaminimi kryhet në dhëmb të lagur nga pështyma.Përdoren kriteret diagnostike të Weerheijm K L (2)• Prania ose mungesa e opaciteteve te kufi zuara• Shkatërrimi post-eruptiv i smaltit(PEB)• Restaurimet atipike• Ekstraksion i molarëve për shkak të MHI
Table 1:
Kriteret diagnostike të MIH (Weerheijm et al 2001a)
Kritert Defi nicion
Opacitet Një defekt që përfshin një alterim të transluçencës së smaltit në shkallë të ndryshme. Smalti difektoz është normal në trashësi me sipërfaqe tëbutë dhe mund të jetë i bardhë,i verdhë,kaf.Lezioni ka kufi j të kufi zuar dhe të dallueshëm nga smalti normal.
PEB Një defekt që shkaktohet nga trauma dhe atricioni.
Restaurim atipik Forma dhe madhesia e restaurimit nuk korrespondon me karakteristikat tipike të restaurimeve.Në shume raste restaurimet janë ekstensive dhe shtrihen deri në sipërfaqet bukale dhe palatinale.Nëkufi jtë e restaurimeve mund të vihen re opacitete..
Extraksion për shkak të MIH
Mungesa e një molari duhet të lidhet me dhëmbët e tjerë tëdenticionit.Mungesa e molarit të parë permanent në një denticion të shëndoshë shton dyshimin qëmund të ketë qenë një molar me MHI
Menaxhimi klinik i MHIFëmijët me MHI i nënshtrohen më shume trajtimeve
dentare se femijët e tjerë (27).Këta femijë janë më anksioz gjatë trajtimeve(27).
Menaxhimi klinik i MHI është i vështirë për shkak të (11) :
1. sensitivitetit dhe ecurisë së shpejtë të kariesit në molarët dhe incizivët e prekur
2. bashkëpunimit të vështirë me fëmijët3. vështirësi në kryerjen e anestezisë4. përsëritjes së frakturave të mureve në kufi j të
restaurimit.
Trajtimi varet nga forma e MHI.
Ne format e buta rekomandohet remineralizim dhe desensitivizim(27):
• larja e dhëmbëve me furça të buta dhe pasta që përmbajnë fl uoride
• aplikimi i produkteve me CPP-ACP( casein phospho-peptide-amorphous calcium phospate).
CPP-ACP vepron me fl uoridet duke prodhuar fosfatin e kalçiumit amorf i cili fi ksohet në sipërfaqen e dhëmbit duke siguruar jone të tretshme kalciumi,fl uoride, fosfate të cilat nxisin remineralizimin (28).
• fl uoride topikale (varnishe,xhele 0,4%SnF ).
Fluoridet topikale e remineralizojnë dhëmbin, reduk-tojnë sensitivitetin dhe rritin rezistencën ndaj demineral-izimit për shkak të fl uorapatitit që formohet (29).
• silante
Mund të përdoren silante rezinoz ose silante glass ionomer.Silantet glass iononmer rekomandohen në fi surat e molarëve me MHI pjesërisht të eruptuar ku kontrolli i lagështisëështë i vështirë.Silantet glass ionomer sigurojnë mbrojtje nga kariesi dhe reduktojnë permeabilitetin e sipërfaqes.Retensioni është difektoz me kalimin e kohës dhe është e nevojshme të zëvëndësohen më vonë kur dhëmbi erupton plotësisht me silante rezinoz (30).
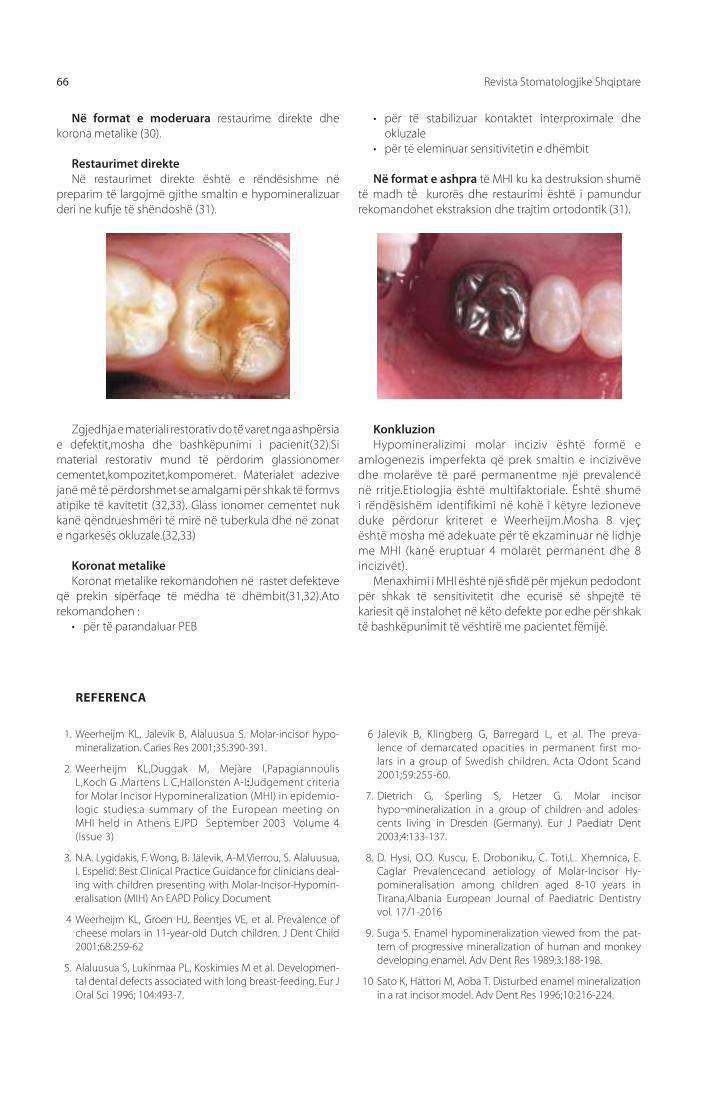
Revista Stomatologjike Shqiptare66
1. Weerheijm KL, Jalevik B, Alaluusua S. Molar-incisor hypo-mineralization. Caries Res 2001;35:390-391.
2. Weerheijm KL,Duggak M, Mejàre I,Papagiannoulis L,Koch G .Martens L C,Hallonsten A-l:Judgement criteria for Molar Incisor Hypomineralization (MHI) in epidemio-logic studies:a summary of the European meeting on MHI held in Athens EJPD September 2003 Volume 4 (Issue 3)
3. N.A. Lygidakis, F. Wong, B. Jälevik, A-M.Vierrou, S. Alaluusua, I. Espelid: Best Clinical Practice Guidance for clinicians deal-ing with children presenting with Molar-Incisor-Hypomin-eralisation (MIH) An EAPD Policy Document
4 Weerheijm KL, Groen HJ, Beentjes VE, et al. Prevalence of cheese molars in 11-year-old Dutch children. J Dent Child 2001;68:259-62
5. Alaluusua S, Lukinmaa PL, Koskimies M et al. Developmen-tal dental defects associated with long breast-feeding. Eur J Oral Sci 1996; 104:493-7.
6 Jalevik B, Klingberg G, Barregard L, et al. The preva-lence of demarcated opacities in permanent first mo-lars in a group of Swedish children. Acta Odont Scand 2001;59:255-60.
7. Dietrich G, Sperling S, Hetzer G. Molar incisor hypo¬mineralization in a group of children and adoles-cents living in Dresden (Germany). Eur J Paediatr Dent 2003;4:133-137.
8. D. Hysi, O.O. Kuscu, E. Droboniku, C. Toti,L. Xhemnica, E. Caglar Prevalencecand aetiology of Molar-Incisor Hy-pomineralisation among children aged 8-10 years in Tirana,Albania European Journal of Paediatric Dentistry vol. 17/1-2016
9. Suga S. Enamel hypomineralization viewed from the pat-tern of progressive mineralization of human and monkey developing enamel. Adv Dent Res 1989;3:188-198.
10 Sato K, Hattori M, Aoba T. Disturbed enamel min eralization in a rat incisor model. Adv Dent Res 1996;10:216-224.
REFERENCA
Në format e moderuara restaurime direkte dhe korona metalike (30).
Restaurimet direkteNë restaurimet direkte është e rëndësishme në
preparim të largojmë gjithe smaltin e hypomineralizuar deri ne kufi je të shëndoshë (31).
• për të stabilizuar kontaktet interproximale dhe okluzale
• për të eleminuar sensitivitetin e dhëmbit
Në format e ashpra të MHI ku ka destruksion shumë të madh të kurorës dhe restaurimi është i pamundur rekomandohet ekstraksion dhe trajtim ortodontik (31).
Zgjedhja e materiali restorativ do të varet nga ashpërsia e defektit,mosha dhe bashkëpunimi i pacienit(32).Si material restorativ mund të përdorim glassionomer cementet,kompozitet,kompomeret. Materialet adezive janë më të përdorshmet se amalgami për shkak të formvs atipike të kavitetit (32,33). Glass ionomer cementet nuk kanë qëndrueshmëri të mirë në tuberkula dhe në zonat e ngarkesës okluzale.(32,33)
Koronat metalikeKoronat metalike rekomandohen në rastet defekteve
që prekin sipërfaqe të mëdha të dhëmbit(31,32).Ato rekomandohen :
• për të parandaluar PEB
KonkluzionHypomineralizimi molar inciziv është formë e
amlogenezis imperfekta që prek smaltin e incizivëve dhe molarëve të parë permanentme një prevalencë në rritje.Etiologjia është multifaktoriale. Është shumë i rëndësishëm identifikimi në kohë i këtyre lezioneve duke përdorur kriteret e Weerheijm.Mosha 8 vjeç është mosha më adekuate për të ekzaminuar në lidhje me MHI (kanë eruptuar 4 molarët permanent dhe 8 incizivët).
Menaxhimi i MHI është një sfi dë për mjekun pedodont për shkak të sensitivitetit dhe ecurisë së shpejtë të kariesit që instalohet në këto defekte por edhe për shkak të bashkëpunimit të vështirë me pacientet fëmijë.

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 67
11 Van Amerongen WE, Kreulen CM. Cheese molars: A pilot study of the etiology of hypo calcifi cations in fi rst perma-nent molars. J Dent Child 1995;62:266-269.
12. Vanessa William, BDSc, DClinDent , Louise B Messer, BDSc, LDS, MDSc, PhD Michael F Burrow, BDSc, MDS, PhD, MEd Molar Incisor Hypomineralization: Review and Recommen-dations for Clinical Management Pediatric Dentistry – 28:3 2006: 224-232
13. Jalevik B, Noren JG. Enamel hypomineralization of perma-nent fi rst molars: A morphological study and survey of pos-sible aetiological factors. Int J Paediatr Dent 2000;10:278-289.
14. Seow WK. Enamel hypoplasia in the primary dentition: a review. J Dent Child 1991;58:441-452.
15. Seow WK. A study of the development of the permanent dentition in very low birthweight children. Pediatr Dent 1996;18:379-384.
16. Seow WK. Eff ects of preterm birth on oral growth and de-velopment. Aust Dent J 1997;42:85-91.
17. Nguyen C. Problems of prematurity and its eff ect on growth and development. Synopses 1997;16:1, 6-11.
18. Martinez A, Cubillos P, Jimenez M, Brethauer U, Catalan P, Gonzalez U. Prevalence of developmental enamel defects in mentally retarded children. J Dent Child 2002;69:151-155.
19. Jalevik B, Noren JG, Barregard L. Etiologic factors infl enc-ing the prevalence of demarcated opacities in permanent fi rst molars in a group of Swedish children. Eur J Oral Sci 2001;109:230-234.
20. Hall R. The prevalence of developmental defects of tooth enamel (DDE) in a paediatric hospital department of den-tistry population (part I). Adv Dent Res 1989;3:114-119.
21. Seow WK. Enamel hypoplasia in the primary dentition: a review. J Dent Child 1991;58:441-452.
22. Kirkham J, Robinson C, Straff ord SM, Shore RC, Bonass WA, Brookes SJ, Wright JT. The chemical composition of tooth enamel in junctional epidermolysis bullosa. Arch Oral Biol 2000;45:377-386.
23. Alaluusua S, Lukinmaa PL, Vartiainen T, Partanen M, Torp-pa J, Tuomisto J. Polychlorinated dibenzo-p-dioxins and dibenzofurans via mother’s milk may cause developmen-tal defects in the child’s teeth. Environ Toxicol Pharmacol 1996;1:193-197.
24. Alaluusua S, Lukinmaa PL, Koskimies M, Pirinen S, Holtta P, Kallio M, Holttinen T, Salmenpera L. Developmental dental defects associated with long breast-feeding. Eur J Oral Sci 1996;104:493-497.
25. Jan J, Vrbic V. Polychlorinated biphenyls cause develop-mental enamel defects in children. Caries Res 2000;34:469-473.
26. Baroni C, Marchionni S.MIH supplementation strategies: prospective clinical and laboratory trial.J Dent Res. 2011 Mar;90(3):371-6.
27. Leppaniemi A, Lukinmaa PL, Alaluusua S. Nonfl uoride hy-pomineralizations in the permanent fi rst molars and their impact on the treatment need. Caries Res 2001;35:36-40.
28. Jalevik B, Klingberg GA. Dental treatment, dental fear and behaviour management problems in children with severe enamel hypomineralization of their permanent fi rst molars. Int J Paediatr Dent 2002;12:24-32.
29. Reynolds EC. New modalities for a new generation: Casein phosphopeptide-amorphous calcium phosphate, a new remineralization technology. Synopses 2005;30:1-6.
30. Messer LB. Getting the fl uoride balance right: Children in long-term fl uoridated communities. Synopses 2005;30:7-10.
31. Manton DJ, Messer LB. Pit and fi ssure sealants: Another major cornerstone in preventive dentistry. Aust Dent J 1995;40:22-29.
32. Fayle SA. Molar incisor hypomineralisation: Restorative management. Eur J Paediatr Dent. 2003 Sep;4(3):121–126
33. Mahoney EK. The treatment of localized hypoplastic and hypomineralized defects in fi rst permanent molars. N Z Dent J 2001;97:101-105.
34. Croll TP. Restorative options for malformed permanent mo-lars in children. Compend Contin Educ Dent 2000;21:676-678, 680, 682.

Albanian Stomatological Journal68
IntroductionThe term Molar Incisor Hypomineralization (MIH) was
introduced in 2001 by Weerheijm(1). At the 6th Congress of the European Academy of
Paediatric Dentistry (EAPD) great attention was focussed on the mineralisation defects of enamel.One of the conclusions of the Congress was that there were
limited prevalence data of Molar Incisor Hypominer-alisation (MIH) meantime suggestions were made by cli-nicians that the prevalence of MIH is increasing.In march 2003 a meeting was held in Athens to treet this issues.In this meeting were established the nomeclature, defi ni-tion, judgement criteria for Molar Incisor Hypomineral-ization.
According to Weerheijm Molar Incisor Hypominer-alization (MIH) is clinical appearence of morphological enamel defects aff ecting occlusal part of one or more of four fi rst permanent molars or ⅓ incisal part of incisors as result of “ hypomineralisation of systemic origin”(Athine 2003) (2)
This defi nition was chosen to emphasize the fact that molars are always aff ecting and there is acorrelacion with demarcated opacities in incisors.
An Interim Seminar and Workshop on MIH was organised in Helsinki in 2009.The outcome of this event is the present consensus paper on the prevalence, diagnosis, aetiology and treatment for children and adolescents presenting with MIH.(Lygidakiset al)(3).This paper serves as a guidance for clinicians and researchers dealing with MHI.
The prevalence of MHI in Europe (using the criteria
of Weerheijm) ranges from 4% to 25 % (4,5,6,7).The prevalence of MHI among 1575 children aged 8-10 years in Tirana was found to be 14%. (8)
First permanent molars are more aff ected. (2).Although the defects described as MIH can sometimes also be noticed on second primary molars,second permanent molars and tips of the permanent canines the most frequent occurrence in children is that of fi rst permanent molar. (2)
The purpose of this review is to describe the diagnosis, clinical features, prevalence, etiological factors of MIH and to describe treatment options in management of such clinical disorders.
Enamel HypomineralisationMature enamel is the hardest mineralized tissue of
the human body.Enamel is of ectodermal origin.It is composed by 96% mineral material and 4 % organic material and water. The main component of inorganic material is calcium hydroxyapatite crystals.Other minerals such as carbonate,magnesium,potassium,sodium and fl uoride are also present in small amounts.The main component of organic materials are enamel proteins : amelogenine ,enameline, ameloblastine, tufteline.
Enamel formation occurs in two stges.In the fi rst stage called secretory stage ameloblasts produce enamel matrix which is composed of proteins,carbohydrates and only a small amount of calcium hydroxyapatite crystals. The second stage is called maturation stage.During this stage enamel matrix completes its mineralization process.During the maturation of enamel matrix ameloblasts
AbstraktThe term Molar Incisor Hypomineralization (MIH) was introduced in 2001 by Weerheijm(1). According to Weerheijm Molar Incisor Hypomineralization (MIH) is clinical appearence of morphological enamel defects aff ecting occlusal part of one or more of four fi rst permanent molars or ⅓ incisal part of incisors as result of “ hypomineralisation of systemic origin”(Athine 2003) .In March 2003 in Athens meeting were established the nomeclature, defi nition, judgement criteria for Molar Incisor Hypomineralization.Diagnostic criteria for MHI developed byWeerheijm K L include:demarcated opacities, posteruptive enamel breakdown(PEB),atypical restoration,extracted molar due to MIHThe prevalence of MHI in Europe (using the criteria of Weerheijm) ranges from 4% to 25 % (4,5,6,7).The prevalence of MHI among 1575 children aged 8-10 years in Tirana was found to be 14%.In diff erent studies authors describe as putative etiological factors: diseases of the fi rst 3 years (asthma, otitis media, tonsillitis, chicken pox, pneumonia, rubella etc)antibiotic therapy ,systemic illnes,environmental conditionsTreatment of these lessions depends by their clinical forms.
The aim of this review is to describe the diagnosis, clinical features, prevalence, etiological factors of MIH and to describe treatment options in management of such clinical disorders.
Prof. Assoc. Etleva Droboniku (Qeli)1, Prof. Assoc. Dorjan Hysi1, Dr. Ina Droboniku2, Prof. Assoc. Çeliana Toti1,D.M.Sc. Enida Petro1
Molar Incisor Hypomineralization
1Faculty of Dental Medicine,University of Medicine Tiranë, 2 Dental Clinic “Droboniku”Tiranë
KEYWORDS:
Hypominer-
alization, molar,
incisor, enamel,
opacity
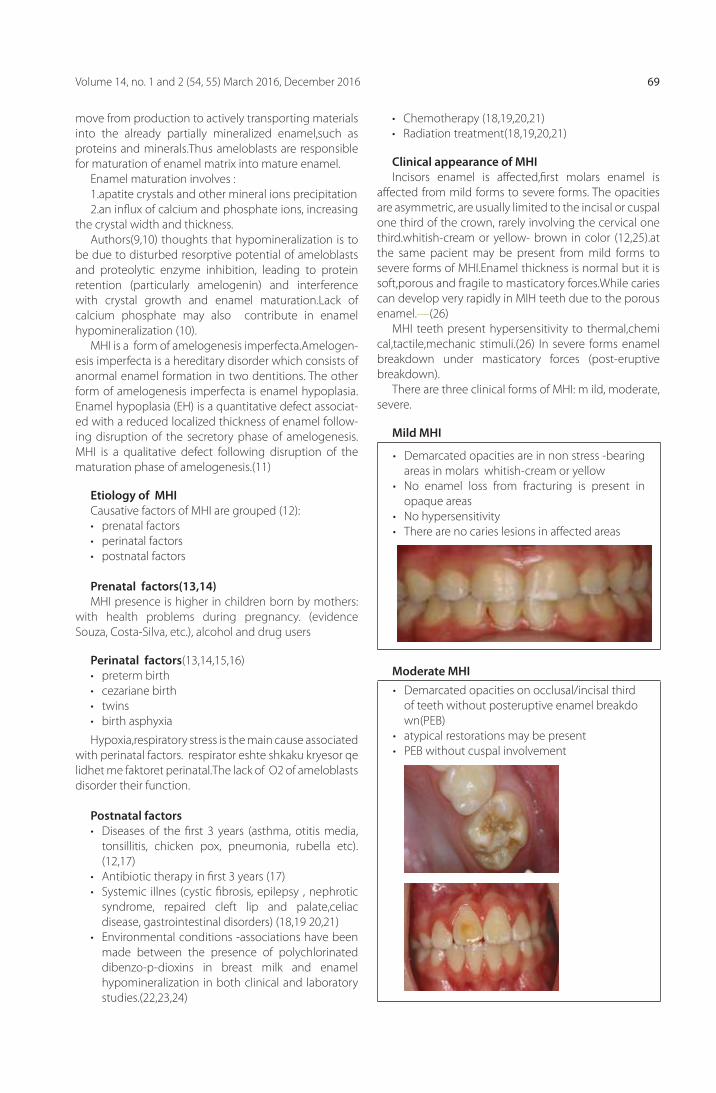
Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 69
move from production to actively transporting materials into the already partially mineralized enamel,such as proteins and minerals.Thus ameloblasts are responsible for maturation of enamel matrix into mature enamel.
Enamel maturation involves :1.apatite crystals and other mineral ions precipitation2.an infl ux of calcium and phosphate ions, increasing
the crystal width and thickness.Authors(9,10) thoughts that hypomineralization is to
be due to disturbed resorptive potential of ameloblasts and proteolytic enzyme inhibition, leading to protein retention (particularly amelogenin) and interference with crystal growth and enamel maturation.Lack of calcium phosphate may also contribute in enamel hypomineralization (10).
MHI is a form of amelogenesis imperfecta.Amelogen-esis imperfecta is a hereditary disorder which consists of anormal enamel formation in two dentitions. The other form of amelogenesis imperfecta is enamel hypoplasia.Enamel hypoplasia (EH) is a quantitative defect associat-ed with a reduced localized thickness of enamel follow-ing disruption of the secretory phase of amelogenesis. MHI is a qualitative defect following disruption of the maturation phase of amelogenesis.(11)
Etiology of MHI Causative factors of MHI are grouped (12):• prenatal factors • perinatal factors • postnatal factors
Prenatal factors(13,14)MHI presence is higher in children born by mothers:
with health problems during pregnancy. (evidence Souza, Costa-Silva, etc.), alcohol and drug users
Perinatal factors(13,14,15,16)• preterm birth• cezariane birth• twins• birth asphyxia
Hypoxia,respiratory stress is the main cause associated with perinatal factors. respirator eshte shkaku kryesor qe lidhet me faktoret perinatal.The lack of O2 of ameloblasts disorder their function.
Postnatal factors• Diseases of the fi rst 3 years (asthma, otitis media,
tonsillitis, chicken pox, pneumonia, rubella etc).(12,17)
• Antibiotic therapy in fi rst 3 years (17)• Systemic illnes (cystic fi brosis, epilepsy , nephrotic
syndrome, repaired cleft lip and palate,celiac disease, gastrointestinal disorders) (18,19 20,21)
• Environmental conditions -associations have been made between the presence of polychlorinated dibenzo-p-dioxins in breast milk and enamel hypomineralization in both clinical and laboratory studies.(22,23,24)
• Chemotherapy (18,19,20,21)• Radiation treatment(18,19,20,21)
Clinical appearance of MHIIncisors enamel is aff ected,fi rst molars enamel is
aff ected from mild forms to severe forms. The opacities are asymmetric, are usually limited to the incisal or cuspal one third of the crown, rarely involving the cervical one third.whitish-cream or yellow- brown in color (12,25).at the same pacient may be present from mild forms to severe forms of MHI.Enamel thickness is normal but it is soft,porous and fragile to masticatory forces.While caries can develop very rapidly in MIH teeth due to the porous enamel.—(26)
MHI teeth present hypersensitivity to thermal,chemical,tactile,mechanic stimuli.(26) In severe forms enamel breakdown under masticatory forces (post-eruptive breakdown).
There are three clinical forms of MHI: m ild, moderate, severe.
Mild MHI
• Demarcated opacities are in non stress -bearing areas in molars whitish-cream or yellow
• No enamel loss from fracturing is present in opaque areas
• No hypersensitivity• There are no caries lesions in aff ected areas
Moderate MHI• Demarcated opacities on occlusal/incisal third
of teeth without posteruptive enamel breakdown(PEB)
• atypical restorations may be present• PEB without cuspal involvement

Albanian Stomatological Journal70
Severe MHI
posteruptive enamel breakdown is present
• There are caries lesions in aff ected areas
• Hipersensitivity• Crown desctruction –
pulpal involvement• atypical restorations are
present • aesthetics problems
Diagnosis of MHIAn examination for MIH should be performed on wet teeth after cleaning. Eight years of age was considered as the
best time for any examination for MHI. At this age,in most children, all 4 permanent molars will be erupted, as will be the majority of the incisors(2).
Weerheijm K L (2) develop diagnostic criteria for MHI:• demarcated opacities• posteruptive enamel breakdown(PEB)• atypical restoration• extracted molar due to MIH
Table 1:
Defi nitions of the criteria used for diagnosing MIH (Weerheijm et al 2001a)
Criteria Defi nitions
Opacity A defect involving an alteration in the translucency of the enamel, variable in degree. The defective enamel is of normal thickness with a smooth surface and can be white, yellow or brown in color. The border of the lesions is demarcated.
PEB A defect that indicated defi ciency of the surface after eruption of the tooth. This may be caused by such factors as trauma and attrition.
Atypical restoration
Size and shape of restoration do not conform to typical restorative characteristics. In most cases, restorations will be extended to the buccal or the palatinal smooth surface. At the border of the restoration, opacity may be noticed.
Extraction due to MIH
Absence of a molar should be related to the other teeth of the dentition. Absence of a fi rst permanent molar in a sound dentition is suspected to have been an MIH molar.
Clinical management of MHIMIH children receive much more dental treatment
than unaff ected children (27).These children have dental anxiety (27).
Clinical management of MHI is diffi cultdue to (11) :1. the sensitivity and rapid caries progression in af-
fected teeth 2. the limited cooperation of children3. the diffi culties in obtaining anesthesia4. the repeated marginal breakdown of restorations
The treatment is depending by the clinical form of MHI.
Treatment of mild form of MHI Remineralization and desensitization(11,27):
• brush aff ected teeth gently with a desensitizing toothpaste containing fl uoride on a soft toothbrush
• casein phosphopeptide-amorphous calcium phos-phate (CPP-ACP) oral care products.The CPP-ACP can interact with fl uoride ions, producing an amor-phous calcium phosphate stabilized by CPP at the tooth surface and providing soluble calcium, fl uo-ride, and phosphate ions to promote remineraliza-tion with fl uorapatite that is more acid resistant.
• topical fl uoride (varnishes,gel 0,4%SnF ).Topical fl uoride, delivered as concentrated varnishes or gels, can remineralize enamel, reduce sensitivity, and enhance resistance to demineralization by providing a reservoir of fl uoride ions for redeposition as fl uorapatite during remineralization.
• silant.For partially erupted PFMs where moisture
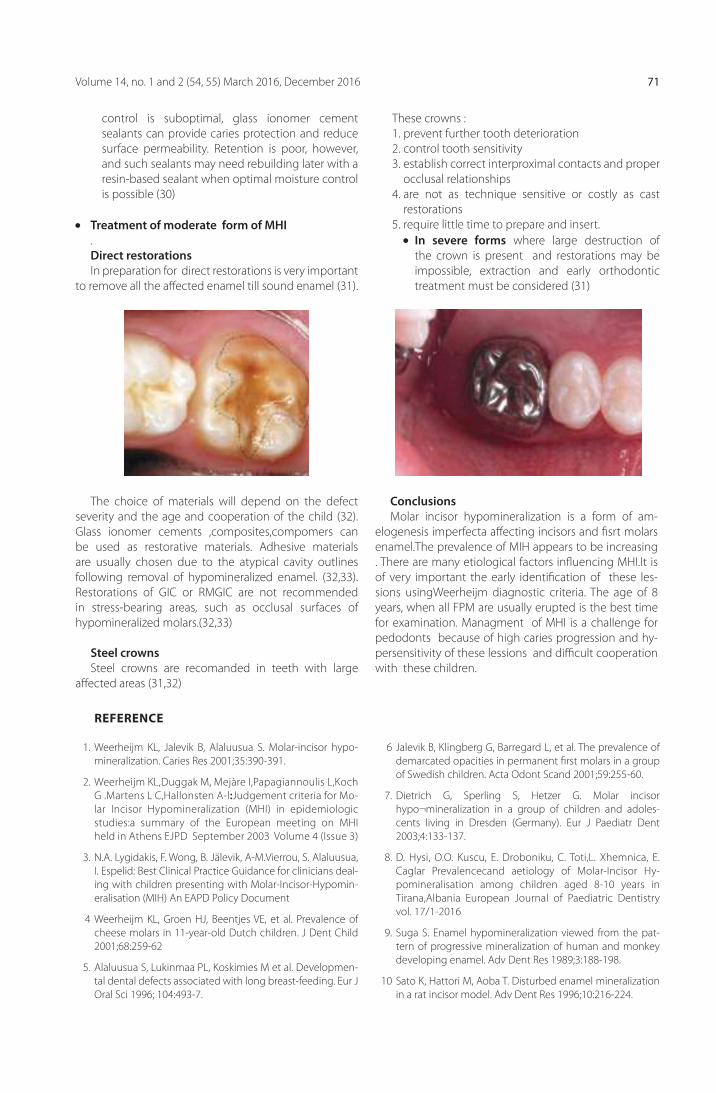
Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 71
control is suboptimal, glass ionomer cement sealants can provide caries protection and reduce surface permeability. Retention is poor, however, and such sealants may need rebuilding later with a resin-based sealant when optimal moisture control is possible (30)
Treatment of moderate form of MHI.Direct restorations In preparation for direct restorations is very important
to remove all the aff ected enamel till sound enamel (31).
These crowns :1. prevent further tooth deterioration2. control tooth sensitivity3. establish correct interproximal contacts and proper
occlusal relationships4. are not as technique sensitive or costly as cast
restorations5. require little time to prepare and insert. In severe forms where large destruction of
the crown is present and restorations may be impossible, extraction and early orthodontic treatment must be considered (31)
The choice of materials will depend on the defect severity and the age and cooperation of the child (32).Glass ionomer cements ,composites,compomers can be used as restorative materials. Adhesive materials are usually chosen due to the atypical cavity outlines following removal of hypomineralized enamel. (32,33).Restorations of GIC or RMGIC are not recommended in stress-bearing areas, such as occlusal surfaces of hypomineralized molars.(32,33)
Steel crownsSteel crowns are recomanded in teeth with large
aff ected areas (31,32)
ConclusionsMolar incisor hypomineralization is a form of am-
elogenesis imperfecta aff ecting incisors and fi srt molars enamel.The prevalence of MIH appears to be increasing . There are many etiological factors infl uencing MHI.It is of very important the early identifi cation of these les-sions usingWeerheijm diagnostic criteria. The age of 8 years, when all FPM are usually erupted is the best time for examination. Managment of MHI is a challenge for pedodonts because of high caries progression and hy-persensitivity of these lessions and diffi cult cooperation with these children.
1. Weerheijm KL, Jalevik B, Alaluusua S. Molar-incisor hypo-mineralization. Caries Res 2001;35:390-391.
2. Weerheijm KL,Duggak M, Mejàre I,Papagiannoulis L,Koch G .Martens L C,Hallonsten A-l:Judgement criteria for Mo-lar Incisor Hypomineralization (MHI) in epidemiologic studies:a summary of the European meeting on MHI held in Athens EJPD September 2003 Volume 4 (Issue 3)
3. N.A. Lygidakis, F. Wong, B. Jälevik, A-M.Vierrou, S. Alaluusua, I. Espelid: Best Clinical Practice Guidance for clinicians deal-ing with children presenting with Molar-Incisor-Hypomin-eralisation (MIH) An EAPD Policy Document
4 Weerheijm KL, Groen HJ, Beentjes VE, et al. Prevalence of cheese molars in 11-year-old Dutch children. J Dent Child 2001;68:259-62
5. Alaluusua S, Lukinmaa PL, Koskimies M et al. Developmen-tal dental defects associated with long breast-feeding. Eur J Oral Sci 1996; 104:493-7.
6 Jalevik B, Klingberg G, Barregard L, et al. The prevalence of demarcated opacities in permanent fi rst molars in a group of Swedish children. Acta Odont Scand 2001;59:255-60.
7. Dietrich G, Sperling S, Hetzer G. Molar incisor hypo¬mineralization in a group of children and adoles-cents living in Dresden (Germany). Eur J Paediatr Dent 2003;4:133-137.
8. D. Hysi, O.O. Kuscu, E. Droboniku, C. Toti,L. Xhemnica, E. Caglar Prevalencecand aetiology of Molar-Incisor Hy-pomineralisation among children aged 8-10 years in Tirana,Albania European Journal of Paediatric Dentistry vol. 17/1-2016
9. Suga S. Enamel hypomineralization viewed from the pat-tern of progressive mineralization of human and monkey developing enamel. Adv Dent Res 1989;3:188-198.
10 Sato K, Hattori M, Aoba T. Disturbed enamel min eralization in a rat incisor model. Adv Dent Res 1996;10:216-224.
REFERENCE

Albanian Stomatological Journal72
11 Van Amerongen WE, Kreulen CM. Cheese molars: A pilot study of the etiology of hypo calcifi cations in fi rst perma-nent molars. J Dent Child 1995;62:266-269.
12. Vanessa William, BDSc, DClinDent , Louise B Messer, BDSc, LDS, MDSc, PhD Michael F Burrow, BDSc, MDS, PhD, MEd Molar Incisor Hypomineralization: Review and Recommen-dations for Clinical Management Pediatric Dentistry – 28:3 2006: 224-232
13. Jalevik B, Noren JG. Enamel hypomineralization of perma-nent fi rst molars: A morphological study and survey of pos-sible aetiological factors. Int J Paediatr Dent 2000;10:278-289.
14. Seow WK. Enamel hypoplasia in the primary dentition: a review. J Dent Child 1991;58:441-452.
15. Seow WK. A study of the development of the permanent dentition in very low birthweight children. Pediatr Dent 1996;18:379-384.
16. Seow WK. Eff ects of preterm birth on oral growth and de-velopment. Aust Dent J 1997;42:85-91.
17. Nguyen C. Problems of prematurity and its eff ect on growth and development. Synopses 1997;16:1, 6-11.
18. Martinez A, Cubillos P, Jimenez M, Brethauer U, Catalan P, Gonzalez U. Prevalence of developmental enamel defects in mentally retarded children. J Dent Child 2002;69:151-155.
19. Jalevik B, Noren JG, Barregard L. Etiologic factors infl enc-ing the prevalence of demarcated opacities in permanent fi rst molars in a group of Swedish children. Eur J Oral Sci 2001;109:230-234.
20. Hall R. The prevalence of developmental defects of tooth enamel (DDE) in a paediatric hospital department of den-tistry population (part I). Adv Dent Res 1989;3:114-119.
21. Seow WK. Enamel hypoplasia in the primary dentition: a review. J Dent Child 1991;58:441-452.
22. Kirkham J, Robinson C, Straff ord SM, Shore RC, Bonass WA, Brookes SJ, Wright JT. The chemical composition of tooth enamel in junctional epidermolysis bullosa. Arch Oral Biol 2000;45:377-386.
23. Alaluusua S, Lukinmaa PL, Vartiainen T, Partanen M, Torp-pa J, Tuomisto J. Polychlorinated dibenzo-p-dioxins and dibenzofurans via mother’s milk may cause developmen-tal defects in the child’s teeth. Environ Toxicol Pharmacol 1996;1:193-197.
24. Alaluusua S, Lukinmaa PL, Koskimies M, Pirinen S, Holtta P, Kallio M, Holttinen T, Salmenpera L. Developmental dental defects associated with long breast-feeding. Eur J Oral Sci 1996;104:493-497.
25. Jan J, Vrbic V. Polychlorinated biphenyls cause develop-mental enamel defects in children. Caries Res 2000;34:469-473.
26. Baroni C, Marchionni S.MIH supplementation strategies: prospective clinical and laboratory trial.J Dent Res. 2011 Mar;90(3):371-6.
27. Leppaniemi A, Lukinmaa PL, Alaluusua S. Nonfl uoride hy-pomineralizations in the permanent fi rst molars and their impact on the treatment need. Caries Res 2001;35:36-40.
28. Jalevik B, Klingberg GA. Dental treatment, dental fear and behaviour management problems in children with severe enamel hypomineralization of their permanent fi rst molars. Int J Paediatr Dent 2002;12:24-32.
29. Reynolds EC. New modalities for a new generation: Casein phosphopeptide-amorphous calcium phosphate, a new remineralization technology. Synopses 2005;30:1-6.
30. Messer LB. Getting the fl uoride balance right: Children in long-term fl uoridated communities. Synopses 2005;30:7-10.
31. Manton DJ, Messer LB. Pit and fi ssure sealants: Another major cornerstone in preventive dentistry. Aust Dent J 1995;40:22-29.
32. Fayle SA. Molar incisor hypomineralisation: Restorative management. Eur J Paediatr Dent. 2003 Sep;4(3):121–126
33. Mahoney EK. The treatment of localized hypoplastic and hypomineralized defects in fi rst permanent molars. N Z Dent J 2001;97:101-105.
34. Croll TP. Restorative options for malformed permanent mo-lars in children. Compend Contin Educ Dent 2000;21:676-678, 680, 682.

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 73
PërmbledhjeTitanium ka qënë materiali i preferuar për prodhimin e implanteve.Megjithatë në vitet e fundit është folur për shume disavantazhe të implantit,shumë kërkime janë bërë për një material i cili është akoma dhe më i biokompatibel. PEEK është semikristalin termoplastikë me mekanikë shumë të mirë dhe veti kimike të rezistencës që janë mbajtur në temperatura të larta.Struktura kimike e këtyre ketoneve poliaromatikë, jep një stabilitet në temperatura të larta (mbi 300 ° C), rezistencë ndaj agjentëve kimikë dhe dëmeve nga rrezatimet,kompatibilitet të lartë me shumë agjentë rinforcues si fi brat e xhamit dhe të karbonit, jep rezistencë më të madhe në krahasim me shumë materiale. Në fund të viteve 90 këto materiale ishin konsideruar si lider për zëvëndesimin e metalit kryesishtë në ortopedi.Ky rast klinik përshkruan vendosjen e një implanti për të zevendesuar dhëmbin 26 me nje atrofi posteriore maksilare si rezultat i pneumatizimit të sinusit maksilar që ka ulur ndjeshëm sasinë dhe lartësinë e kockës së mbetur.
Ph.D Erda Qorri1, Msc Fabio de Propris1, Msc Majlinda Kola1, Prof. Assoc Edit Xhajanka2, Prof. Assoc Mertia Bardhoshi2
Metoda alternative nga titanium për reabilitimin implanto protetik: PEEK Prezantim Rasti
1 Albanian University, 2 Fakulteti i Mjekësisë Dentare, Universiteti i Mjekësisë, Tiranë
FJALËT KYÇE:
polimerë
termoplastik,
biomaterial,
kompatibilitet
të lartë,
zëvendësim
metalikë ,
kocka atrofi ke.
Te dhena te pergjithshmeMateriali i përzgjedhur për fabrikimin e implanteve ka
qënë titaniumi dhe lidhjet e tij.Shpesh është përzgjedhur si metal nga forca e tij ,pesha e tij e ulët,rezistenca ndaj korrozionit si dhe inercitë e tij biologjike.Megjithatë në këto vitet e fundit si pasojë e disa disavantazheve të titaniumit jane bërë kërkime për një material i cili është akoma dhe më i përshtatshëm.Në fakt kur shtresa okside e një implanti prej titaniumi lëvizet,titaniumi mund të behet korroziv sic janë dhe metalet e tjera.Nga një anë ky korrozion çon në një dobësim të strukturës metalike si dhe në lirimin e elementeve korrozive i cili mund të prodhojë osteolizë.
Kjo gjë mund të çojë në dështimin e implantit.Për më tepër në ditët e sotme ka shumë kundërshtime mbi alergjinë ose mbi hipersensibilitetin që ky material mund të japi.
Në 2006 në një klinikë tëMuller dhe Valentine – Thon autorët kanë testuar 56 pacientë që kanë pasur probleme shëndetësore pas një ndërhyrje klasike kirurgjikale implantare e bazuar në titanium.Mbi të gjithë këta pacientë është bërë testi MELISA,21 kanë rezultuar pozitiv,për 16 testi nuk ka pasur valencë dhe për 19 testi ka rezultuar negativ. Pas heqjes së implantit të gjithë pacientët kanë pasur përmirësimë.Autorët kanë konkluduar duke thënë se titaniumi mund të çojë në një hipersensibilitet dhe që nuk duhet më të konsiderohen universalisht si “biologjikisht inert”.
Për më shumë një problem tjetër është paraqitur nga përputhshmëria ë këtij materiali me disa nga teknologjitë moderne të screening si rezonanca magnetike(MRI).
Për të kapërcyer këtë problem kërkimet në vitet e fundit janë konkretizuar mbi projektimin e zëvëndësimit
të titaniumit.Një ndër materialet më premtuese është polyetheretherketone (PEEK)1.
PEEK është pjesë e familjes së polimerit termoplastik me temperaturë të lartë,strukturat kimike të këtij ketoni poliaromatik i japin një stabilitet dhe një temperaturë mbi 300 ° C,rezistencë ndaj agjentëve kimik dhe dëmeve nga rretimet,kompatibilitet të lartë më shumë agjentë rinforcues si fi brat e xhamit dhe të karbonit, jep rezistencë më të madhe në krahasim me shumë materiale.Në fund të viteve ‘90 këto materiale ishin konsideruar si lider për zëvëndesimin e metalit kryesishte në ortopedi.
Në 1992 PEEK është përdorur në aplikimet dentare,në fi llim në formë pilastrash estetike e më pas si implante.Që në atë kohë janë vënë re shumë variacione në përbërjen e tij per te permiresuar karakteristikat e punes tek implantet. Përmbajtja e tij bën izoelasticitetin e implantit,që do të thotë se densiteti dhe elasticiteti (moduli i Young) është identike me kockën.Eshtë vërtetuar se një diferencë e madhe midis elasticitetit të materialit të implantit dhe të kockes con në gjenerim më të madh të stresit si pasojë e diff erencës së deformimit nën ngarkesë.
Përbërësit e PEEK sigurojnë një deformim identik me kockën kështu që ka një shperndarje më homogjene nga streset përgjate ndërfaqes implant-kocke2.
Prioritetet sipërfaqesore të një materiali mund të modifi kohen nga një numer i madh teknikash.Një nga keto teknika është . e cila është përshkruar si një produkt shumë inovativ.Plasma është një gaz i jonizuar i cili mund të fabrikohet në një sistem me reaksione të mbyllura me përmbajtjen e një përzjerjeje gazi me presion të ulet menjeherë pas një eksitimi me valë elektromagnetike.
Për këtë motiv falë përdorimit të llampës OPLASMA mund të modifi kojmë siperfaqen PEEK të

Revista Stomatologjike Shqiptare74
implantit në mënyrë që të rritet aderimi qelizor dhe i biokampatibilitetit.
Ndërkaq me trajtimin e plazmës vërehet një reduktim në energjinë siperfaqësore duke rezultuar me rritje të lagshmerisë nga ana e likideve3.
Rast klinikPacienti (mashkull 33 vjec) është paraqitur me
probleme funksionale lidhur me humbjen e 26 si pasojë e kariesit profund. (foto 1). Gjatë anamnezës pacienti jo duhanpires paraqet kushte të mira shëndetësore pa patologji te pergjithshme.
së mbetur, është menduar për inserimin e një implanti në PEEK , Perso B.
Perso B mund të inserohet në një lartesi të mbetur të kockës nga 3-10mm pa qënë e nevojshme të realizojme teknika rigjenerative dhe të rritet kreshta inferiore me 2mm.
Protokolli i inserimit parashikon një sekuence me freza dhe disqe me burim aktiv duke u nisur nga freza më e vogel 0,4 mm me spesor të frezës 5mm dhe diameter të diskut 22 mm, ndërsa gjatësia e frezës kalon ne menyre pogresive me diametër gjithmon e me të madhe deri sa të arrihet në dimensionin mesio-distal aq sa edentulia na lejon,duke bere kujdes të mos demtojme rrënjën e dhëmbëve fqinje.Këshillohet të lihet te paktën një milimeter kocke nga rrënja e dhëmbëve fqinje.
Pasi kemi realizuar kalimin e fundit me frezë dhe disk mund të rregullojmë ne mënyrë intraoperatore humbjen B duke e bërë me dimensionin e dëshiruar.
Përpara se të fusim implantin manualisht procedohet me preparimin e sipërfaqes nëpërmjet përdorimit të llampës Osmoplasma. (foto 2)
Falë përdorimit të llampës mund të modifi kojmë sipërfaqen e implantit PEEK në menyrë që të rritet adezioni qelizor dhe biokompatibiliteti . (foto 3)
Në projektimin e akomodimit implantar,duhet të kihet parasysh ku do të arrije freza ku të jetë pozicioni,dimensioni dhe angulimi i abatmentit të ardhshem implantoprotetik, është e nevojshme të kërkohet një aksialitet i favorshëm nga pikpamja protezike.
Duhet që freza të arrijë deri në qëndër të kreshtës.Humbja B ka një gjatësi pre 19 mm,lartësi 12mm dhe
spesor 0.9mm
Gjatë egzaminimit klinik paraqiten në kushte të mira të higjenës orale dhe një atrofi posteriore maksilare në zonen 26 si pasojë të pneumatizimit të sinusitmaksilar. Ne këtë situate sasia e kockës së mbetur sipas klasifi kimit SA3 sipas klasifi kimit të Misch (1987) për të evituar ndërhyrje invazive e cila con në rritjen e sasise së kockes
Foto nr.1. Pamje radiologjike e zones se edentulise
Foto.Nr 2. Llampa OSMOPLASMA per trajtimin e siperfaqes implantare
Foto.Nr 3. Pamje ne mikroskp e siperfaqes se implantit te trajtuar me OSMOPLASMA
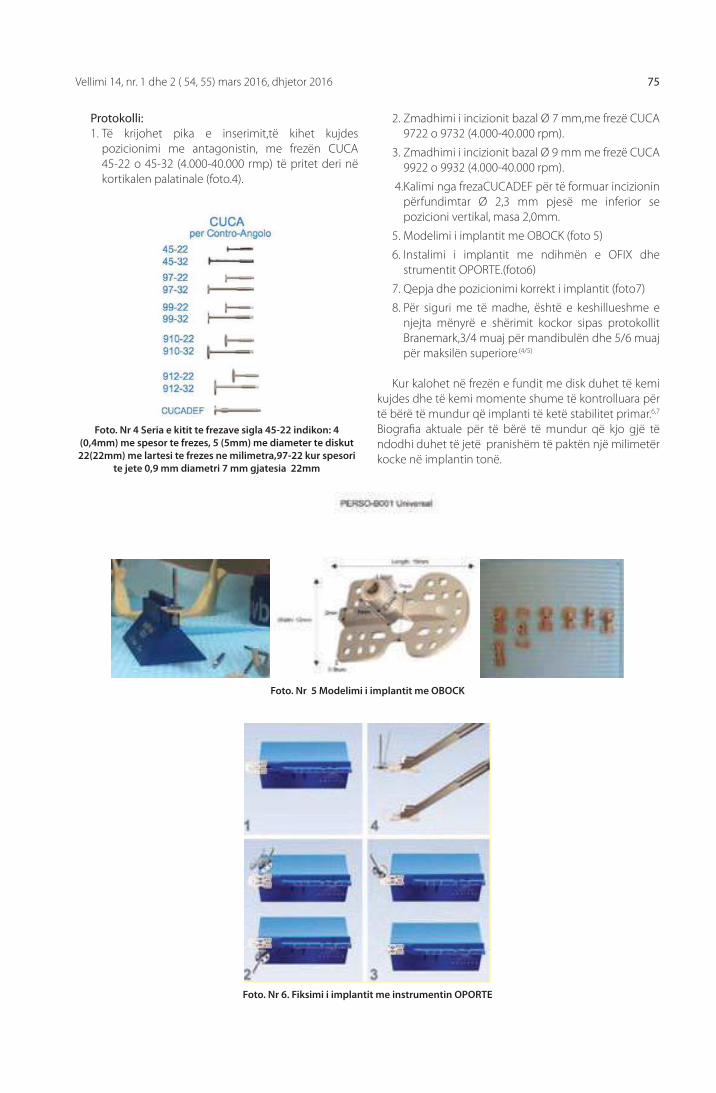
Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 75
Protokolli:1. Të krijohet pika e inserimit,të kihet kujdes
pozicionimi me antagonistin, me frezën CUCA 45-22 o 45-32 (4.000-40.000 rmp) të pritet deri në kortikalen palatinale (foto.4).
Foto. Nr 4 Seria e kitit te frezave sigla 45-22 indikon: 4 (0,4mm) me spesor te frezes, 5 (5mm) me diameter te diskut 22(22mm) me lartesi te frezes ne milimetra,97-22 kur spesori
te jete 0,9 mm diametri 7 mm gjatesia 22mm
Foto. Nr 5 Modelimi i implantit me OBOCK
2. Zmadhimi i incizionit bazal Ø 7 mm,me frezë CUCA 9722 o 9732 (4.000-40.000 rpm).
3. Zmadhimi i incizionit bazal Ø 9 mm me frezë CUCA 9922 o 9932 (4.000-40.000 rpm).
4. Kalimi nga frezaCUCADEF për të formuar incizionin përfundimtar Ø 2,3 mm pjesë me inferior se pozicioni vertikal, masa 2,0mm.
5. Modelimi i implantit me OBOCK (foto 5)
6. Instalimi i implantit me ndihmën e OFIX dhe strumentit OPORTE.(foto6)
7. Qepja dhe pozicionimi korrekt i implantit (foto7)
8. Për siguri me të madhe, është e keshillueshme e njejta mënyrë e shërimit kockor sipas protokollit Branemark,3/4 muaj për mandibulën dhe 5/6 muaj për maksilën superiore.(4/5)
Kur kalohet në frezën e fundit me disk duhet të kemi kujdes dhe të kemi momente shume të kontrolluara për të bërë të mundur që implanti të ketë stabilitet primar.6,7 Biografi a aktuale për të bërë të mundur që kjo gjë të ndodhi duhet të jetë pranishëm të paktën një milimetër kocke në implantin tonë.
Foto. Nr 6. Fiksimi i implantit me instrumentin OPORTE

Revista Stomatologjike Shqiptare76
REFERENCA :
1. Maria, K., et al., Polyetheretherketone (PEEK) Dental Im-plants: A Case for Immediate Loading. International Jour-nal of Oral Implantology and Clinical Research, 05-08/2011
2. Kurtz S, Devine J. PEEK biomaterials in trauma, orthopedic, and spinal implants: A review.Biomaterials2007;28:4845-69.
4. Briem, D., Response of primary fi broblasts and osteoblasts to plasma treated polyetheretherketone (PEEK)surfaces, J. Mat. Science: Mat. In Med 16: 671-677, 2005
5. JulP.I. Brånemark, R. Adell, T. Albrektsson, U. Lekholm, S. Lun-dkvist, B. Rockler,Osseointegrated titaniumfi xtures in the treatment of edentulousness, Biomaterials, Volume 4, Issue 1, January 1983, Pages 25–28R.
6. Adell, U. Lekholm, B. Rockler, P-I. Brånemark, J. Lindhe, B. Er-iksson, L. Sbordone, Marginal tissue reactions at osseointe-grated titanium fi xtures: (I). A 3-year longitudinal prospec-tive study.International Journal of Oral and Maxillofacial Surgery, Volume 15, Issue 1, February 1986, Pages 39–52
7. Ki-Sun Lee, Joo-Hee Shin, Jong-Eun Kim, Jee-Hwan Kim, Won-Chang Lee, Sang-Wan Shinand Jeong-Yol Lee. (2017) Biomechanical Evaluation of a Tooth Restored with High Performance Polymer PEKK Post-Core System: A 3D Finite Element Analysis. BioMed Research Internation-al 2017, 1-9. Online publication date: 1-Jan-2017.
Foto. Nr 7 Inserimi i implaniti Peek

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 77
Abstract: For several decades, titanium and its alloys has been the preferred and elective material for the manufacturing of the implants. However in recent years, because of some potential disadvantages of titanium, many researches has been done for fi nding a material which is even more powerful.PEEK is a semicrystalline thermoplastic with excellent mechanical and chemical resistance properties that are retained to high temperatures.The chemical structure of these polyromantic ketones confers a stability at elevated temperatures(above 300 °C),resistance to chemical and radiation damage, high compatibility with many reinforcing agents such as glass fi bers and carbon, and higher resistance compared to many other metals. Already in the late 90s, this material was considered as the leading replacement metal, especially in orthopedics. This case report describes the placement of an implant in the position of the tooth number 26 in the maxillary area which is atrophic as a result of the pneumatic left maxillary sinus, that has signifi cantly reduced the amount and the height of the residual bone.
Prosthetic implant rehabilitation with materials alternative to Titanium: PEEK. Case Report
KEYWORDS:
thermoplastic
polymers,
biomaterial,
high
compatibility,
replacement
metal, atrophic
bone.
GeneralityTitanium and its alloys has been the preferred
and elective material for the manufacturing of the implants.it was often choose due to his resistance, weight, corrosion resistance and biological inertia. However, in recent years, because of some potential disadvantages of titanium, many researches has been done for fi nding a material which is even more powerful. In fact, when the oxide surface of the implant is moved, titanium could be corrosive as other metals. This corrosion damage the metallic structure and can eliberate corrosive elements that could be produce the osteolizis. This mean the failure of the implant.Morever nowadays there are many objections on the allergy or hypersensitivity this material can give. In 2006 authors Muler Valentine Thon has testing 56 pacients who have had health problems after a classical titanium implant surgery.Allthepatients were subjected to the MELISA test. 21 tested patience was fi nd positive, for the 16 test has no valence and 19 test was negative. After implant remove the general status of the patients was improved. Authors concluded that titanium shouldn’t be considered “biological inert”.Another problem is presented by the compatibility of this material with some modern screening technologies such as MRI.To overcome this problem researches in
recent years have been materialized on the design of titanium replacement. One of the most promising materials is polyetheretherketone (PEEK)1.
PEEK is part of the thermoplastic polymer family with high temperature, chemical structures of this ketone polyaromatic give stability and a temperature above 300 ° C, resistance to chemical agents and radiations damage, high compatibility with many agents like glass and carbon, It gives greater resistance than many materials. In the late ‘90s these materials were considered as leading to the replacement of metal mostly in orthopedics.
In 1992 PEEK was used in dentistry, fi rst in aesthetic then as implants. Since that time, many variations are observed in its composition to improve better characteristics for the implants. Its content makes implant isofl exibile, which means that the density and elasticity (Young module) is identical to bone. It is proved that a great diff erence between the elasticity of the material of the implant and bone leads to greater stress. The PEEK components provide an identical deformation with bone, so that will give a homogeneous distribution of stresses along the implant-bone interface2. Surface property of a material can be modifi ed by a large number of techniques. One of this technices is plasma treatment, which is an innovative technical.
Ph.D Erda Qorri1, Msc Fabio de Propris1, Msc Majlinda Kola1, Prof. Assoc Edit Xhajanka2, Prof. Assoc Mertia Bardhoshi2
1 Albanian University, 2 Faculty of Dental Medicine, University of Medicine, Tirana
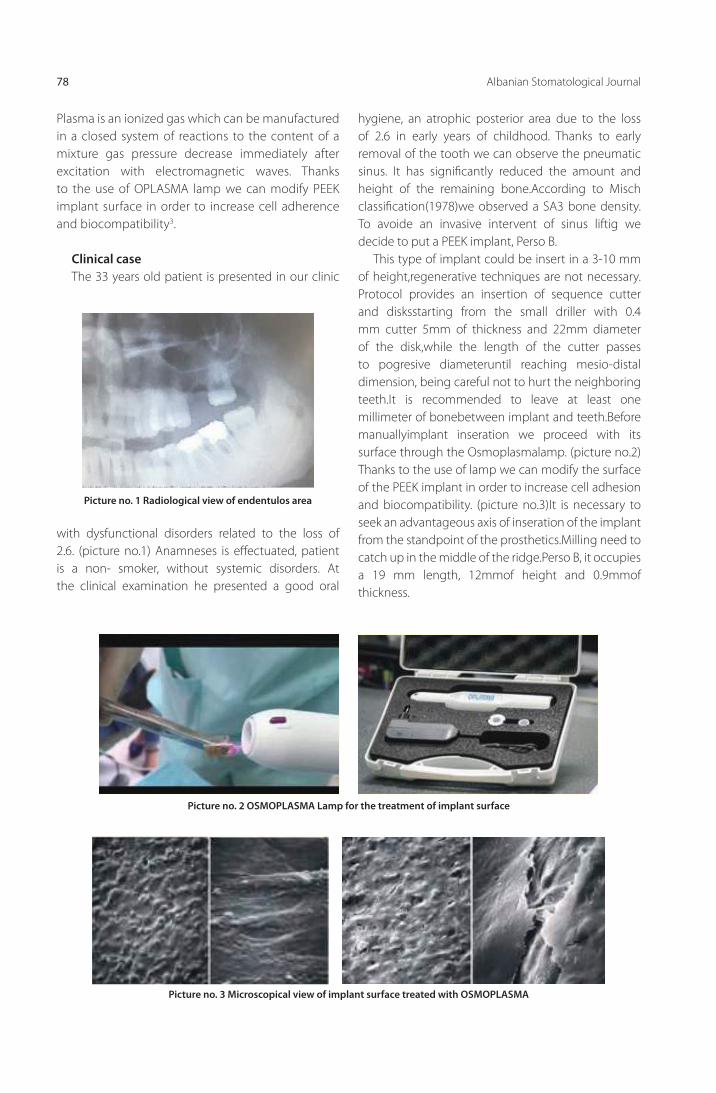
Albanian Stomatological Journal78
Plasma is an ionized gas which can be manufactured in a closed system of reactions to the content of a mixture gas pressure decrease immediately after excitation with electromagnetic waves. Thanks to the use of OPLASMA lamp we can modify PEEK implant surface in order to increase cell adherence and biocompatibility3.
Clinical caseThe 33 years old patient is presented in our clinic
hygiene, an atrophic posterior area due to the loss of 2.6 in early years of childhood. Thanks to early removal of the tooth we can observe the pneumatic sinus. It has signifi cantly reduced the amount and height of the remaining bone.According to Misch classifi cation(1978)we observed a SA3 bone density. To avoide an invasive intervent of sinus liftig we decide to put a PEEK implant, Perso B.
This type of implant could be insert in a 3-10 mm of height,regenerative techniques are not necessary.Protocol provides an insertion of sequence cutter and disksstarting from the small driller with 0.4 mm cutter 5mm of thickness and 22mm diameter of the disk,while the length of the cutter passes to pogresive diameteruntil reaching mesio-distal dimension, being careful not to hurt the neighboring teeth.It is recommended to leave at least one millimeter of bonebetween implant and teeth.Before manuallyimplant inseration we proceed with its surface through the Osmoplasmalamp. (picture no.2)Thanks to the use of lamp we can modify the surface of the PEEK implant in order to increase cell adhesion and biocompatibility. (picture no.3)It is necessary to seek an advantageous axis of inseration of the implant from the standpoint of the prosthetics.Milling need to catch up in the middle of the ridge.Perso B, it occupies a 19 mm length, 12mmof height and 0.9mmof thickness.
with dysfunctional disorders related to the loss of 2.6. (picture no.1) Anamneses is eff ectuated, patient is a non- smoker, without systemic disorders. At the clinical examination he presented a good oral
Picture no. 1 Radiological view of endentulos area
Picture no. 2 OSMOPLASMA Lamp for the treatment of implant surface
Picture no. 3 Microscopical view of implant surface treated with OSMOPLASMA

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 79
Protocol:
1. To create the insertion point, careful with the antagonistic tooth,CUCA 45-22 o 45-32 (4000-40000 RMP) could be extended until the palatal
Picture no. 4 Milling and disks for bone preparation
Picture no. 5 Implant modelation with OBOCK
bone size. (picture no.4)
2. Increasing the basic incisionØ 7 mm, CUCA 9722 o 9732 (4.000-40.000 rpm).
3. Increasing the basic incisionØ 9 mm, CUCA 9922 o 9932 (4.000-40.000 rpm).
4. Passing from CUCADEF to create the fi nal bone incision,Ø 2,3, with inferior size of vertical position size 2,0mm.
5. Shaping implant on OBOCK. (picture no.5)
6. Inseration of implant, helped by OFFIX instrument OPORTE. (picture no.6)
7. Sewing and correct positioning of the implant. (picture no.7)
8. It is recommended the same way bone healing, by Branemark protocol, 3-4 months for the mandibua and 4-5 months for the maxilla.4,5
When changing in recent disc must be careful, we have to make very careful and controlled movement to ensure the stability of implant.6,7
Picture no. 6. Fixing the implant with OPORTE instrument

Albanian Stomatological Journal80
REFERENCA :
1. Maria, K., et al., Polyetheretherketone (PEEK) Dental Im-plants: A Case for Immediate Loading. International Jour-nal of Oral Implantology and Clinical Research, 05-08/2011
2. Kurtz S, Devine J. PEEK biomaterials in trauma, orthopedic, and spinal implants: A review.Biomaterials2007;28:4845-69.
4. Briem, D., Response of primary fi broblasts and osteoblasts to plasma treated polyetheretherketone (PEEK)surfaces, J. Mat. Science: Mat. In Med 16: 671-677, 2005
5. JulP.I. Brånemark, R. Adell, T. Albrektsson, U. Lekholm, S. Lun-dkvist, B. Rockler,Osseointegrated titaniumfi xtures in the treatment of edentulousness, Biomaterials, Volume 4, Issue 1, January 1983, Pages 25–28R.
6. Adell, U. Lekholm, B. Rockler, P-I. Brånemark, J. Lindhe, B. Er-iksson, L. Sbordone, Marginal tissue reactions at osseointe-grated titanium fi xtures: (I). A 3-year longitudinal prospec-tive study.International Journal of Oral and Maxillofacial Surgery, Volume 15, Issue 1, February 1986, Pages 39–52
7. Ki-Sun Lee, Joo-Hee Shin, Jong-Eun Kim, Jee-Hwan Kim, Won-Chang Lee, Sang-Wan Shinand Jeong-Yol Lee. (2017) Biomechanical Evaluation of a Tooth Restored with High Performance Polymer PEKK Post-Core System: A 3D Finite Element Analysis. BioMed Research Internation-al 2017, 1-9. Online publication date: 1-Jan-2017.
Picture no 7. Insertion of PEEK implant

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 81
PërmbledhjePacientët që do të prezantohen në këtë artikull paraqesin grumbullime dentare të mëdha si në harkun dentar maksilar, ashtu dhe në atë mandibular. Pacientët u trajtuan me briketa self-ligating, Sistemin Damon, pa ekstraksione dhe pa reduktim të smaltit interdentar (stripping). Nga studimi i cefalometrisë dhe modeleve të allçisë pas mbarimit të trajtimit u vu re një proklinim i dhëmbëve frontalë në maksilar dhe mandibulë. Pavarësisht shqetësimit të proklinimit të dhëmbëve frontalë, hapësira e nevojshme për të rreshtuar dhëmbët u krijua nga mekanizma të tjerë, në veçanti nga ekspansioni. Indet e buta, si p.sh buzët, kanë ndjekur lëvizjen e dhëmbëve duke sjellë ndryshime të dukshme dhe të dëshirueshme në profi let e pacientëve.
Msc Manjola Gusho, D.M.Sc. Fatmir Lela
Trajtimi pa ekstraksione në ortodonci me anë të briketave self-ligating. Raste Klinike
Fakulteti i Mjekësisë Dentare, Universiteti i Mjekësisë, Tiranë.
FJALËT KYÇE:
grumbullime
dentare, trajtim
pa ekstraksione,
briketa
self-ligating,
buzëqeshje të
bukura.
Hyrje:Në ortodonci, plani i trajtimit është ndoshta faza
më e rëndësishme e trajtimit, sepse nga ai varet rezultati fi nal për sa i përket anës funksionale dhe estetike të pacientit. Grumbullimet dentare janë ato që hasen më shpesh tek pacientët, të cilët kërkojnë një trajtim ortodontik. Mënyrat për t’u trajtuar këto grumbullime varen nga disa faktorë, por ajo që në fakt duhet të udhëheqë trajtimin tonë është pamja estetike e jashtme e pacientit. Ekzistojnë situata kur kemi grumbullime dentare të mëdha si në maksilar ashtu dhe në mandibulë, por profi li i pacientit nuk të lejon
të bësh ekstraksione, sepse në fi nal mund të rezultojnë harqe dentare të rreshtuara mirë, por të ngushtë dhe jo estetikë si dhe korridore bukale të theksuara në buzëqeshje.
Lind pyetja, A mund të trajtohen me sukses këta pacientë pa ekstraksione? Trajtimi ortodontik duhet të bazohet në estetikën fi nale të pacientit si dhe në stabilitetin e tij në kohë.
Briketat self-ligating kanë zënë një vend të rëndësishëm sot në ortodonci. Ato shkurtojnë kohën e trajtimit, pacienti paraqitet rrallë në vizita dhe këto vizita janë më të shkurtra.

Revista Stomatologjike Shqiptare82
Për shkak të mungesës së fërkimit hark slot, forcat që i transmetohen dhëmbit janë të vogla, komode për pacientin. Ato bëjnë zgjerim në sens transversal të harqeve dentare, duke ulur ndjeshëm nevojën për ekstraksione.
Qëllimi:
Të vlerësojë zhvillimin tridimensional të harqeve dentare maksilar dhe mandibulë si dhe infl uencën e tyre në profi lin e pacientëve, të cilët paraqesin grumbullime dentare të mëdha. Trajtimi është bërë me briketa self-ligating, Damon Q, pa ekstraksione ose reduktim të smaltit interdentar.
Materiale dhe metoda:
Janë mbledhur për studim 12 pacientë, ndërmjet 11- 19 vjec, të cilët paraqesin grumbulime të mëdha dentare (maksilar 5-7 mm dhe madibulë 4-5 mm). Të gjithë pacientët janë trajtuar me briketa self-ligating Damon Q, pa ekstraksione (përveç molarëve të tretë).
Të gjithë pacientëve iu bënë matje në modelin e allcisë në sens transversal me anën e një vizore të milimetruar,
të vendosur paralel me planin okluzal. Në zonën kanine u mat nga maja e një kuspidi tek tjetri, në zonën premolare në nivelin e kuspidëve vestibularë të premolarëve të pare dhe të dytë, ndërsa në zonën molare, nga maja e kuspidit mezio-vestibular të molarëve të pare dhe të dytë.
U bë krahasimi i vlerave cefalometrike dhe profi leve të pacientëve para dhe pas trajtimit ortodontik.
RezultateNga studimi i matjeve u arrit në këto konkluzione:
- Distanca interkanine pësoi ndyshime të vogla, rreth 2-3 mm.
- Ndryshimet më të madha u vunë re në zonën e premolarëve dhe pak në atë të molarëve të parë.
- Vlerat e matjeve të cefalometrisë para dhe pas trajtimit pësuan rritje. U vu re një zmadhim i aksit të incisivëve superiorë dhe inferior në lidhje me planin maksilar dhe respektiv mandibular. Kjo nuk përben asnjë problem pasi profi li i pacientëve është përmirësuar ndjeshëm nga këto zhvendosje të dhëmbëve frontalë.

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 83
1. Damon Dh. The Damon low-friction bracket: a biologically compatible straight-wire system. J. ClinOrth 1998;32:670-680.
2. Harradine, N. W. (2001). Self-ligating brackets and treatment effi ciency.ClinOrthod Res, Vol.4, No. 4, pp. 220-227, ISSN 1168-3811.
3. Rinchuse DJ, Miles PG. Self-ligating brackets: present and future. Am J OrthodDentofacialOrthop. 2007Aug; 132(2):216-22.
4. Harradine N W T 2008. The history and development of self-ligating brackets. Seminars in orthodontics 14: 5-18.
5. Ibel G. et al: Non-Extraction Therapy of Crowding with the Damon System – case Reports and Cephalometric Evalua-tion InfOrthodKieferorthop 2009, 41:207-218
Konkluzione:Rreshtim i grumbullimeve dentare me anë të
briketave self-ligating, Sistemi Damon, zgjeron harkun dentar në gjerësi dhe në gjatësi. Forma e harkut dentar ka një infl uencë direkte tek buzëqeshja e pacientit .Zgjerimi në gjerësi zvogëlon korridoret bukale laterale
duke rezultuar në buzëqeshje të bukura.Harku ideal duhet të jetë i gjerë, të ketë formën U dhe k orridoret e errëta duhen të ruhen pak, sepse kjo e bën buzëqeshjen më tërheqëse.
Trajtimi pa ekstraksione me Sistemin Damon ka një ndikim pozitiv mbi profi lin e pacientëve.
REFERENCA
6. Turpin DL. In-vivo studies off er best measure of self-ligation. Am J OrthodDentofacialOrthop. 2009 Aug; 136(2):141-2.
7. Turpin DL. In-vivo studies off er best measure of self-ligation.Am J OrthodDentofacialOrthop. 2009 Aug; 136(2):141-2.
8. Pandis N, Polychronopoulou A, Makou M, Eliades T. Man-dibular dental arch changes associated with treatment of crowding using self-ligating and conventional brackets. Eur J Orthod. In press.
9. Maijer, R. & Smith, D. C. (1990). Time saving with self-ligating brackets.Journal of Clinical Orthodontics, Vol. 24, No. 1, pp. 29-31, ISSN 0238-7895.
35 mm
34 mm
45 mm
35 mm0 mm ndryshim
42 mm8 mm ndryshim
50 mm5 mm ndryshim
29 mm
32 mm
45 mm
29 mm0 mm ndryshim
36 mm8 mm ndryshim
53 mm8 mm ndryshim
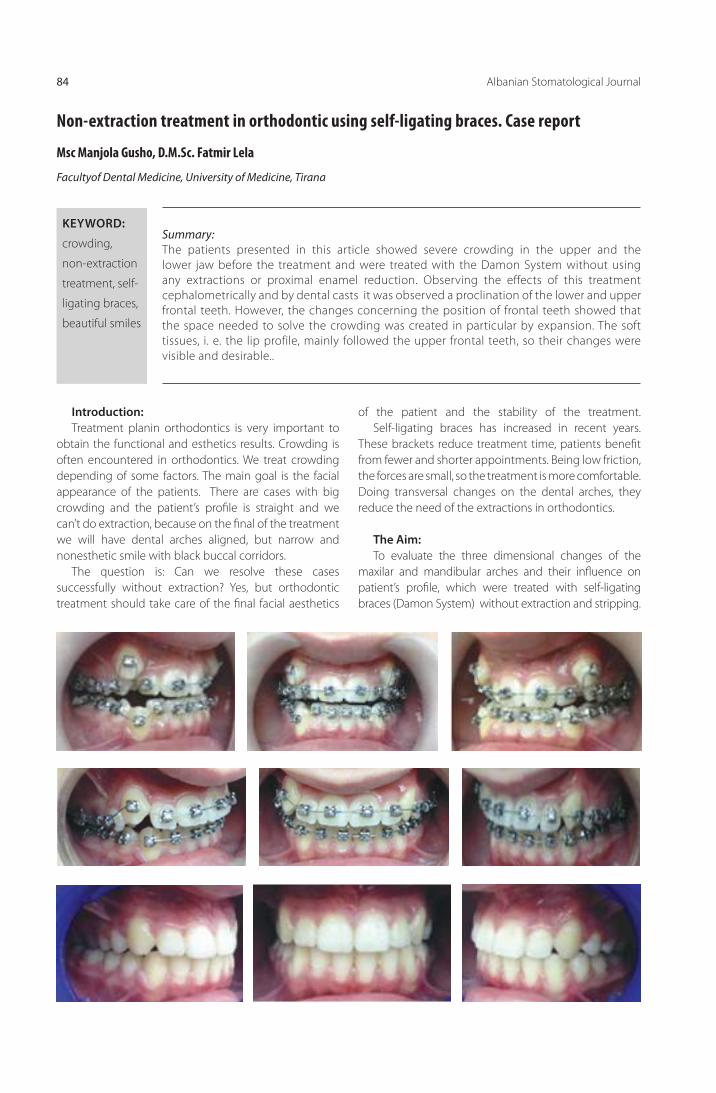
Albanian Stomatological Journal84
Summary:The patients presented in this article showed severe crowding in the upper and the lower jaw before the treatment and were treated with the Damon System without using any extractions or proximal enamel reduction. Observing the effects of this treatment cephalometrically and by dental casts it was observed a proclination of the lower and upper frontal teeth. However, the changes concerning the position of frontal teeth showed that the space needed to solve the crowding was created in particular by expansion. The soft tissues, i. e. the lip profile, mainly followed the upper frontal teeth, so their changes were visible and desirable..
Msc Manjola Gusho, D.M.Sc. Fatmir Lela
Non-extraction treatment in orthodontic using self-ligating braces. Case report
Facultyof Dental Medicine, University of Medicine, Tirana
KEYWORD:
crowding,
non-extraction
treatment, self-
ligating braces,
beautiful smiles
Introduction:Treatment planin orthodontics is very important to
obtain the functional and esthetics results. Crowding is often encountered in orthodontics. We treat crowding depending of some factors. The main goal is the facial appearance of the patients. There are cases with big crowding and the patient’s profi le is straight and we can’t do extraction, because on the fi nal of the treatment we will have dental arches aligned, but narrow and nonesthetic smile with black buccal corridors.
The question is: Can we resolve these cases successfully without extraction? Yes, but orthodontic treatment should take care of the fi nal facial aesthetics
of the patient and the stability of the treatment. Self-ligating braces has increased in recent years.
These brackets reduce treatment time, patients benefi t from fewer and shorter appointments. Being low friction, the forces are small, so the treatment is more comfortable. Doing transversal changes on the dental arches, they reduce the need of the extractions in orthodontics.
The Aim:To evaluate the three dimensional changes of the
maxilar and mandibular arches and their infl uence on patient’s profi le, which were treated with self-ligating braces (Damon System) without extraction and stripping.
Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 85
Materials and Methods In this article are selected to investigate 12 patients,
between 11 and 19 years old. All of them present severe crowding in the upper and the lower arch ( 5-7 mm on maxillar and 4-5 mm on mandibular arch). All the patients are treated with self-ligating braces Damon Q, without extraction (except the third molars) and stripping. To compare the transversal changes, it was used a fl exible scale, parallel to the occlusal plane.
On canine, we measured the distance between the cusp tips of the canines, on the premolars the distance between the buccal cusp tips of the fi rst and second premolars and the distance between mesiobuccal cusp tips of the fi rst and second molars.
We compared the cephalometric tracingand the profi le changes of the patients before and after treatment.
Results:According to the results of this research:
- Intercanine distance tends to increase with 2-3 mm
- The biggest changes were observed in the premolar area and the molars changed a little.
- Cephalometric measurements before and after treatment showed that the axes of the incisors were increased, but this is not a problem, because the patient profi le was improved a lot at the end of the treatment.
The narrow dental arches are unattractive, because the frontal teeth look prominent and the buccal corridor aren’t at all aesthetic, because this makes the smile more attractive.

Albanian Stomatological Journal86
1. Damon Dh. The Damon low-friction bracket: a biologically compatible straight-wire system. J. ClinOrth 1998;32:670-680.
2. Harradine, N. W. (2001). Self-ligating brackets and treatment effi ciency.ClinOrthod Res, Vol.4, No. 4, pp. 220-227, ISSN 1168-3811.
3. Rinchuse DJ, Miles PG. Self-ligating brackets: present and future. Am J OrthodDentofacialOrthop. 2007Aug; 132(2):216-22.
4. Harradine N W T 2008. The history and development of self-ligating brackets. Seminars in orthodontics 14: 5-18.
5. Ibel G. et al: Non-Extraction Therapy of Crowding with the Damon System – case Reports and Cephalometric Evalua-tion InfOrthodKieferorthop 2009, 41:207-218
Conclusions:Correcting of the crowding with self-ligating braces,
Damon System increase arch perimeter in both, arch length and arch width. The arch form has a big infl uence on the patient’s smile. The ideal arch is broad and has
U shape. Broadening the arches decrease the lateral buccal, but these corridors should not be eliminated at all, because this make the smile more attractive.
The non-extraction treatment with Damon System has a positive impact on the patient’s profi le too.
REFERENCE
6. Turpin DL. In-vivo studies off er best measure of self-ligation. Am J OrthodDentofacialOrthop. 2009 Aug; 136(2):141-2.
7. Turpin DL. In-vivo studies off er best measure of self-ligation.Am J OrthodDentofacialOrthop. 2009 Aug; 136(2):141-2.
8. Pandis N, Polychronopoulou A, Makou M, Eliades T. Man-dibular dental arch changes associated with treatment of crowding using self-ligating and conventional brackets. Eur J Orthod. In press.
9. Maijer, R. & Smith, D. C. (1990). Time saving with self-ligating brackets.Journal of Clinical Orthodontics, Vol. 24, No. 1, pp. 29-31, ISSN 0238-7895.
35 mm
34 mm
45 mm
35 mm0 mm of diff erence
42 mm8 mm of diff erence
50 mm5 mm of diff erence
29 mm
32 mm
45 mm
29 mm0 mm of diff erence
36 mm8 mm of diff erence
53 mm8 mm of diff erence

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 87
AbstraktLëndimet traumatike janë ndër episodet më të disfavorshme në jetën e një fëmije. Ato shoqërohen me dhimbje, dëmtim të estetikës, dëmtim të funksionit. Humbja e hershme e dhëmbëve të përhershëm frontalë, në fëmijët në rritje në mënyrë të vecantë paraqet një situatë të rendë përsa i përket të gjithë këtyre komponentëve së bashku, meqenëse dhëmbët frontalë janë të rëndësishëm edhe estetikisht, edhe funksionalisht. Fëmija që ka pësuar këtë lëndim traumatik, ka kaluar një moment të dhimbshëm, pasiqë trauma që të shkaktojë avulsion të dhembit ka qenë e konsiderueshme, gjithashtu preket në mënyrë të ndjeshme estetika, fonetika dhe padyshim aspekti psiko-emocional i fëmijës. Kur një dhëmb i përhershëm ka humbur, dhëmbët ngjitur kanë tendencë të migrojnë në hapësirën e krijuar duke sjellë ngushtim të hapësirës. Rifi timi i hapësirës me aparate të lëvizshëm gjithmonë varet nga bashkëpunimi i fëmijëve në mbajtjen e aparatit edhe respektimin e vizitave periodike të aktivizimit nga mjeku gjatë gjithë kohës së trajtimit .Në këtë punim është paraqitur rasti klinik,i një fëmije që ka humbur incizivin central të djathte (11) dhe është paraqitur pas një periudhe më të gjate se një vjeçare për të korrigjuar pasojat estetike dhe funksionale të humbjes së këtij dhembi. Iu aplikua me sukses aparat i levizshëm ortodontik, u krijua hapësira e duhur, dhe në fund të trajtimit ortodontik u vendos aparat fi ks ruajtës i hapësirës dhe zëvendësimi i përkohshëm i dhëmbit.
M.Sc. Ersela Alikaj1, 2, Prof. Dr. Xhina Mulo1, Dr. Alda Gjoni2
Avulsioni i dhëmbit incisiv central permanent dhe trajtimi i pasojave të tij. Prezantim rasti
1 Universiteti i Mjekësisë, Fakulteti i Mjekësisë Dentare;2 Klinika Dentare “MATIS”
FJALËT KYÇE:
grumbullime
dentare, trajtim
pa ekstraksione,
briketa
self-ligating,
buzëqeshje të
bukura.
Hyrje:Traumat dentare në dhëmbët anteriorë në fëmijët e
moshës parashkollore janë nje ngjarje e rëndë, por që shpesh injorohet. Fëmijët, me dëmtime në dhëmbët anteriorë dhe prindërit e tyre paraqesin një sfi dë për dentistin. Humbja apo dëmtimi i dhëmbëve anteriorë tek fëmijët nuk paraqesin thjesht një problem dentar, ato kanë një ndikim të madh psikologjik si tek prindërit edhe fëmija, vecanërisht, nëse lëndimi shkakton humbje të rëndësishme të strukturës së dhëmbit. 14,15 .Traumat e dhëmbëve janë shkaktari i tretë më i rëndësishëm i humbjes së dhëmbëve. Me mënyrat e sotme të mësimdhënies, fëmijët janë më të ekspozuar ndaj situatave ku trauma është pasojë e tyre 2 . Gjatë moshës shkollore, fëmijët luajnë në mënyrë aktive në natyrë. Edhe pse këto aktivitete janë tregues të rritjes dhe zhvillimit të fëmijës, aktivitete të pakujdesshme si humbja e ekuilibrit dhe lëvizjet e pakordinuara rrisin mundësinë e lëndimeve.
Avulsioni është zhvendosja traumatike e dhëmbit nga alveola e tij. Ndodh më shpesh gjatë aksidenteve duke përfaqësuar 0.5% deri në 3% të lëndimeve traumatike të dhëmbëve të përhershëm. Më së shumti ndodhin në fëmijët në mes të shtatë dhe nëntë vjeç 2, 11, 10. Menaxhimi adekuat brenda 30 minutave të para nga momenti i aksidentit është shumë i rëndësishëm për prognozën e dhëmbit. Ndihma imediate mjekësore është raportuar të jetë efektive në ruajtjen e ligamentit periodontal (PDL), qelizat e të cilit janë në një gjendje të qëndrueshme edhe
pas shkëputjes 3,5,11. Qumështi mbetet një nga solucionet më të përdorura dhe të rekomanduara të ruajtjes 4, 7, 9. Vetite e tij kryesore janë disponueshmërinë e lartë, një pH fi ziologjik dhe osmolaritet biokompatibël me qelizat PDL. Në varësi të dëmtimit të PDL, dhëmbët e avulsuar dhe të rënë në kontakt me ambientin e jashtëm me shpesh zhvillojnë infl amacion përreth ligamentit duke u komplikuar me rezorbim të rëndë apo përfunduar deri në ankilozë 5,9,10. Ankiloza ndikon në zhvillimin e kockave alveolare në pacientët e rinj.
Qëllimi i parë i trajtimit të avulsionit është të mbahet dhëmbi vital ose të paktën funksional që të shmanget rezorbimi dhe ankiloza duke rezultuar në rritjen normale të kreshtës alveolare. Nëse kjo nuk mund të arrihet, është me rëndësi të madhe nderhyrja dhe trajtimi nga mjeku ortodont për të parandaluar ndryshimet në kockën alveolare dhe ngushtimet e harqeve dentare apo anomalive funksionale, për shkak të humbjes së dhëmbëve. Struktura alveolare e kockave është e nevojshme për vendosjen e një implant pas përfundimit të zhvillimit deri në moshën 20 vjeç apo edhe më vonë.
Qëllimi :. Qëllimi i punimit është :
Të tregojë pasojat e mosndërhyrjes në kohë pas humbjes traumatike të dhëmbit permanent.
Të tregojë rezultatet që arrihen me perdorimin e një aparati të thjesht ortodontik.

Revista Stomatologjike Shqiptare88
Të tregojë rëndësinë e trajtimit në kohë dhe rëndësinë e informimit të prindërve dhe pacientëve lidhur me avulsionin.
Materiali dhe Metoda : Është bërë paraqitja e një rasti klinik, një fëmijë që
ka pësuar avulsion të dhëmbit permanent central të djathtë. Është paraqitur gjendja me foto dhe radiografi a në momentin e paraqitjes në klinikë. Është trajtuar me aparat të lëvizshëm për rregullimin e malokluzionit dhe rekuperimin e vendit, ndjekja për rreth një vit dhe janë paraqitur të dy menyra të ruajtjes së hapësrës dhe gjendja në fund të trajtimit.
Prezantimi i rastit :Pacientia E. B., 9 vjeҫ, u paraqitet në klinikën tonë
rreth më shumë se një vit pasi kishte humbur dhembin 11 pas një aksidenti. Trauma ishte si rrjedhojë e rrëzimit në kopshtin e shtëpisë së saj. Sipas referimit të prindërve, pati lacerim të buzës së poshtme dhe hemorragji . Është shkuar tek kirurgu oral për ndërhyrjen e parë në indet e buta pas dy orësh, ndërsa dhëmbin nuk e kanë ruajtur, megjithëse e kishin disponuar. Është informuar nga kirurgu për reinplantimin nëqoftëse do ta kishin ruajtur
dhëmbin dhe ndjekjen nga një mjek ortodont sa më shpejt. Pacientia e shendetshtme pa histori mjekësore të semundjeve. Më pas nuk kanë bërë asnjë ndërhyrje dhe janë paraqitur në klinikën tonë vetëm pas një viti. Gjendja e pacientes paraqitet ne fotot 1 dhe 2 në momentin e parë. E. referon se edhe pas një viti ajo ndihet fajtore që nuk u tregua më e kujdesshme edhe e tregon historinë e lëndimit shumë e prekur.
Në fotot duket zvogëlimi i hapësirës që i përkiste dhëmbit 11, spostim i dhëmbëve fqinjë, spostim djathtas i linjës mediane në nofullën e sipërme dhe një dëmtim i rëndësishëm i estetikës së vajzës si edhe i fonetikës së saj. Pacientia paraqet edhe një sërë problemesh të tjera dentare: procese karioze, ekstraktuar 16 si pasojë e komplikacioneve të kariesit.
Pasi u studiua modeli edhe nga te dhënat radiografi ke ku duket zvogëlimi i hapësirës dhe problemet e tjera dentare, iu shpjeguan prindërve të pacientes mënyrat e trajtimit, kostot, rëndësia e trajtimit, u këshillua sanimi i kavitetit oral dhe rëndësia e trajtimit.
Duke rënë dakord me prindërit, u vendos për një aparat të thjeshtë të lëvizshëm ortodontik, për të siguruar hapësirën e nevojshme për dhëmbin central, si dhe për të rregulluar problemet e okluzionit (Foto 3, 4)
Foto 2
Foto 1

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 89
Vlen të theksohet se mundësitë ekonomike ishin të kufi zuara, dhe prindërit ishin relativisht bashkëpunues lidhur me kohën e kërkuar për trajtim.
Në foton 5 duket ecuria gjatë trajtimit :
Pas krijimit të hapësirës së nevojshme, detyra e radhës është të ruhet hapësira dhe të bëhet zëvendësimi i përkohshëm i dhëmbit.
Fillimisht u provua me hark retainer dhe ndërtim direkt me kompozit i dhëmbit, por rezultoi e pasuksesshme si zgjidhje, pasi nuk pati qëndruëshmërinë e duhur (foto 8, 9).
Foto 3Foto 7
Foto 8
Foto 9
Foto 4
Foto 5
Foto 6
Pas rreth një viti hapësira e nevojshme u realizua. Gjendja pas heqjes së aparatit është treguar në fotot 6, 7
Pas kësaj u vendos të realizohej një ruajtës fi ks i hapësirës i fi ksuar me banda tek molarët dhe zevendësimi i dhëmbit u bë më dhëmb rezine. (foto 10, 11, 12, 13).
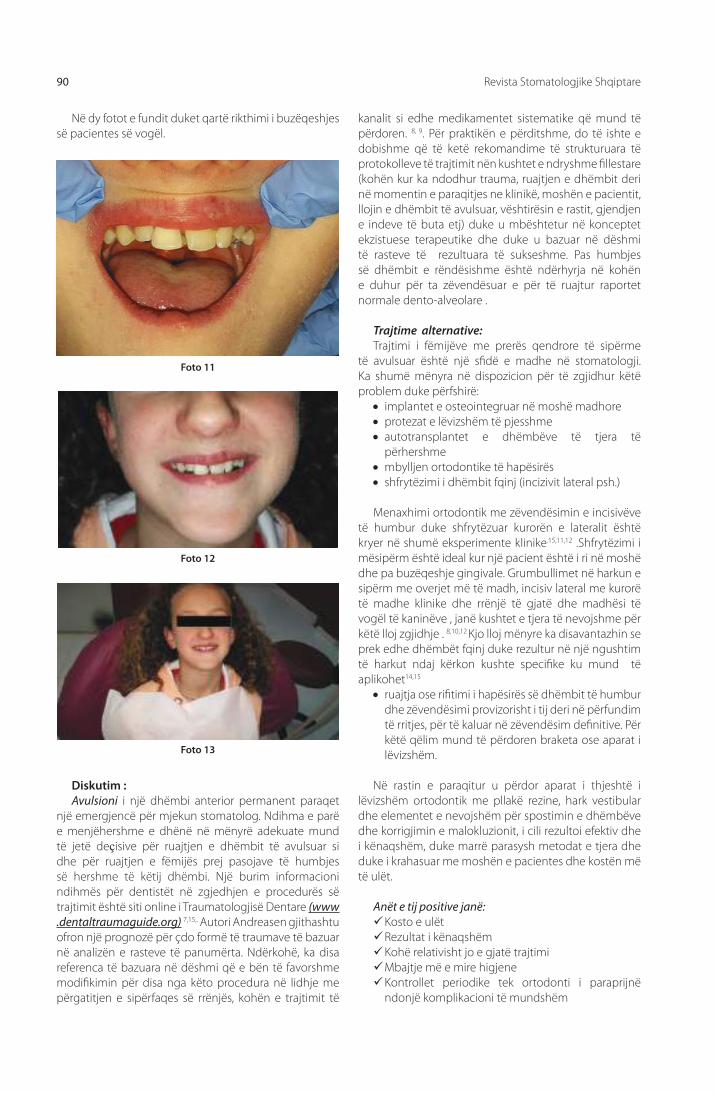
Revista Stomatologjike Shqiptare90
Në dy fotot e fundit duket qartë rikthimi i buzëqeshjes së pacientes së vogël.
kanalit si edhe medikamentet sistematike që mund të përdoren. 8, 9. Për praktikën e përditshme, do të ishte e dobishme që të ketë rekomandime të strukturuara të protokolleve të trajtimit nën kushtet e ndryshme fi llestare (kohën kur ka ndodhur trauma, ruajtjen e dhëmbit deri në momentin e paraqitjes ne klinikë, moshën e pacientit, llojin e dhëmbit të avulsuar, vështirësin e rastit, gjendjen e indeve të buta etj) duke u mbështetur në konceptet ekzistuese terapeutike dhe duke u bazuar në dëshmi të rasteve të rezultuara të sukseshme. Pas humbjes së dhëmbit e rëndësishme është ndërhyrja në kohën e duhur për ta zëvendësuar e për të ruajtur raportet normale dento-alveolare .
Trajtime alternative:Trajtimi i fëmijëve me prerës qendrore të sipërme
të avulsuar është një sfi dë e madhe në stomatologji. Ka shumë mënyra në dispozicion për të zgjidhur këtë problem duke përfshirë:
implantet e osteointegruar në moshë madhore protezat e lëvizshëm të pjesshme autotransplantet e dhëmbëve të tjera të
përhershme mbylljen ortodontike të hapësirës shfrytëzimi i dhëmbit fqinj (incizivit lateral psh.)
Menaxhimi ortodontik me zëvendësimin e incisivëve të humbur duke shfrytëzuar kurorën e lateralit është kryer në shumë eksperimente klinike.15,11,12 .Shfrytëzimi i mësipërm është ideal kur një pacient është i ri në moshë dhe pa buzëqeshje gingivale. Grumbullimet në harkun e sipërm me overjet më të madh, incisiv lateral me kurorë të madhe klinike dhe rrënjë të gjatë dhe madhësi të vogël të kaninëve , janë kushtet e tjera të nevojshme për këtë lloj zgjidhje . 8,10,12 Kjo lloj mënyre ka disavantazhin se prek edhe dhëmbët fqinj duke rezultur në një ngushtim të harkut ndaj kërkon kushte specifi ke ku mund të aplikohet14,15
ruajtja ose rifi timi i hapësirës së dhëmbit të humbur dhe zëvendësimi provizorisht i tij deri në përfundim të rritjes, për të kaluar në zëvendësim defi nitive. Për këtë qëlim mund të përdoren braketa ose aparat i lëvizshëm.
Në rastin e paraqitur u përdor aparat i thjeshtë i lëvizshëm ortodontik me pllakë rezine, hark vestibular dhe elementet e nevojshëm për spostimin e dhëmbëve dhe korrigjimin e malokluzionit, i cili rezultoi efektiv dhe i kënaqshëm, duke marrë parasysh metodat e tjera dhe duke i krahasuar me moshën e pacientes dhe kostën më të ulët.
Anët e tij positive janë: Kosto e ulëtRezultat i kënaqshëmKohë relativisht jo e gjatë trajtimiMbajtje më e mire higjeneKontrollet periodike tek ortodonti i paraprijnë
ndonjë komplikacioni të mundshëm
Foto 11
Foto 12
Foto 13
Diskutim :Avulsioni i një dhëmbi anterior permanent paraqet
një emergjencë për mjekun stomatolog. Ndihma e parë e menjëhershme e dhënë në mënyrë adekuate mund të jetë deҫisive për ruajtjen e dhëmbit të avulsuar si dhe për ruajtjen e fëmijës prej pasojave të humbjes së hershme të këtij dhëmbi. Një burim informacioni ndihmës për dentistët në zgjedhjen e procedurës së trajtimit është siti online i Traumatologjisë Dentare (www .dentaltraumaguide.org) 7,15,. Autori Andreasen gjithashtu ofron një prognozë për çdo formë të traumave të bazuar në analizën e rasteve të panumërta. Ndërkohë, ka disa referenca të bazuara në dëshmi që e bën të favorshme modifi kimin për disa nga këto procedura në lidhje me përgatitjen e sipërfaqes së rrënjës, kohën e trajtimit të
Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 91
1. Cortes M.I.S., Marcenes W., Sheiham A. Impact of traumatic injuries to the permanent teeth on the oral health-related quality of life of 12–14-year-old children. Commun. Dent. Oral Epidemiol. 2002;30:193–198.
2. Antunes L.A.A., Leão A.T., Maia L.C. The impact of dental trauma on quality of life of children and adolescents: A criti-cal review and measurement instruments. Ciênc. Saúde. Coletiva. 2012;17:3417–3424.
3. Bendo C.B., Paiva S.M., Varni J.Ë., Vale M.P. Oral health-related quality of life and traumatic dental injuries in Brazilian ado-lescents. Commun. Dent. Oral Epidemiol. 2014;42:216–223.
4. Glendor U. Aetiology and risk factors related to traumatic dental injuries—A revieë of the literature. Dent. Traumatol. 2009;25:19–31.
5. Livny A., Sgan-Cohen H.D., Junadi S., Marcenes W. Trau-matic dental injuries and related factors among sixth grade schoolchildren in four Palestinian toëns. Dent. Traumatol. 2010;26:422–426.
6. Traebert J., Marcon K.B., Lacerda J.T. Prevalence of traumatic dental injuries and associated factors in schoolchildren of Palhoça, Santa Catarina State. Ciênc. Saúde. Coletiva. 2010;15:1849–1855.
7. Lee JY, Divaris K. Hidden consequences of dental trauma: the social and psychological eff ects. Pediatr Dent. 2009;31:96–101.
8. Andreasen JO, Andreasen FM, Andersson L. Textbook and color atlas of traumatic injuries to the teeth. 4. Oxford: John wiley Professional; 2007.
9. Locker D. Prevalence of traumatic dental injury in grade 8 children in six Ontario communities. Can J Public Health. 2005;96:73
10. Fleming P. S., Seehra J., Dibiase A. T. Combined orthodon-tic-restorative management of maxillary central incisors lost following traumatic injury: a case report. Orthodon-tics. 2011;12(3):242–251.
11. Kokich V. G., Nappen D. L., Shapiro P. A. Gingival contour and clinical crown length: their eff ect on the esthetic ap-pearance of maxillary anterior teeth. American Journal of Orthodontics. 1984;86(2):89–94. doi: 10.1016/0002-9416(84)90300-2.
12. Kokich V. G., Kokich V. O. Interrelationship of orthodontics with periodontics and restorative dentistry. In: Nanda R., editor. Biomechanics and Esthetic Strategies in Clinical Or-thodontics. St. Louis, Mo, USA: Elsevier; 2005.
13. Kovich V. Esthetics and anterior tooth position: an orth-odontic perspective. Part I: croën length. Journal of Esthetic and Restorative Dentistry. 1993;5(1):19–23. doi: 10.1111/j.1708-8240.1993.tb00739.x.
14. Kokich V. G., Spear F. M. Guidelines for managing the orthodontic-restorative patient. Seminars in Orthodon-tics. 1997;3(1):3–20. doi: 10.1016/S1073-8746(97)80036-9.
15. Kokich V. G. Esthetics and vertical tooth position: orthodon-tic possibilities. Compendium of Continuing Education in Dentistry. 1997;18(12):1225–1231.
REFERENCA:
Anët negative : Domosdoshmëria e bashkëpunimit të pacientit. Rezultati dhe kohëzgjatja do të varen shumë nga
mbajtja korrekte prej pacientit si dhe paraqitja në intervalet e duhura të kohës tek mjeku për të kryer aktivizimet e nevojshme.
Aparati është pak masiv dhe mund të paraqesi vërshtirësi në të folur dhe mbajtur gjatë kohës së trajtimit.
Përfundime: Humbja traumatike e një dhëmbi frontal permanent,
bën pjesë në aksidentet dentare më “fatkeqe” për një fëmjë dhe prindërit e tij.
Ndërhyrja e urgjencës konsiston në mjekimin e
plagëve eventuale dhe mundësisht reimplantimin sa më shpejt të dhëmbit të avulsuar.
Në rastet kur reimplantimi i dhëmbit të avulsuar nuk mund të realizohet, atëherë është e domosdoshme vendosja e ruajtësit të hapësirës, në mënyrë që të parandalohen spostimet e dhëmbëve fqinjë, spostime të cilat me kalimin e kohës do të rezultojnë në malokluzion, estetikë të varfër si dhe probleme funksionale.
Në rastin kur kjo ka ndodhur, del detyrë për mjekun ortodont të korrigjojë malokluzionin, të rifi tohet hapësira e dhëmbit të humbur, si dhe të ruhet kjo hapësirë dhe të bëhet zëvendësimi i përkohshëm i dhëmbit të munguar, deri kur të përfundojë rritja e pacientit e të bëhet zëvendësimi defi nitiv i tij me metodat e njohura kirurgjikale edhe ortopedike.

Albanian Stomatological Journal92
Introduction :Traumatic injuries to the anterior teeth among the
young children are tragic but often an ignored problem. Children with injuries of their anterior teeth, and their concerned parents present a challenge for the dentist that is often unparalleled. There is perhaps no single dental disturbance that has a greater psychological impact on both the parents and the child than the fracture or loss of a child’s anterior tooth, especially if the injury involves an extensive loss of the tooth structure. Traumatic injuries, being on the rise, are the third largest cause for the mortality of teeth. With the so-called advanced civilized modes of teaching, children are more exposed to situations where trauma becomes a mandatory consequence of involvement.During the school age, children actively indulge in outdoor play. Though these activities are markers of growth and development of the child, careless activities, loss of balance and impaired movements increase the possibility of injuries.
Avulsion is a traumatic displacement of the tooth from its socket. It is an accident, representing 0.5% to 3% of traumatic injuries in permanent dentition, mostly aff ecting children between seven and nine years of age. An adequate management within the fi rst half hour is most important for the prognosis of the tooth. Diff erent medical storage media have been reported to be eff ective in maintaining the periodontal ligament (PDL)
cells in a viable state after avulsion, but milk remains one of the most commonly used and recommended storage media. Its main advantages are high availability, a physiologically compatible pH and osmolality with the PDL cells. Depending on the injury to the PDL these replanted teeth often develop surrounding infl ammation followed by severe resorption ending up in ankylosis. Ankylosis aff ects alveolar bone development in younger patients.
The fi rst goal of avulsion treatment is to keep the tooth vital or at least functional in place avoiding resorption and ankylosis resulting in normal growth of the alveolar ridge. If this cannot be achieved it is of great importance to prevent the alveolar bone from collapsing due to tooth loss. Alveolar bone structure is necessary for the the placement of an implant after completion of alveolar bone development up to the age of 20 or even later.
Aims:The purpose of the articleis :To demonstrate the consequences of non-
interference in time after traumatic permanent tooth loss .
To show the results achieved with the use of a removable orthodontic appliance .
To demonstrate the importance of the
Abstract:Traumatic injuries are among the most unfavorable episodes in the life of a child. They are associated with pain, aesthetical and functional issues. The early loss of permanent frontal teeth in growing children in particular, is a serious situation in terms of all these components together, because the anterior teeth are important both aesthetically and functionally. A child who has suff ered this traumatic injury, has had a painful moment, because the trauma has been considerable to cause the avulsion of the tooth, and also the aesthetics, phonetics and obviously psycho-emotional aspect of the child are signifi cantly aff ected.Early loss of permanent anterior teeth in growing children has a psychological impact on the child.. When a permanent tooth is lost, the teeth adjacent to the created space tend to migrate into the space resulting in the space loss. Management of regaining space with the removable appliance always depends on child cooperation for using the appliance as well as for the recall visits at the doctor.In this article it is presented a clinical case, a child who has lost the rightcentral incisive(11) and has come to the dental studio after a period longer than a year to correct aesthetic and functional consequences of the loss of the tooth. A removable orthodontic appliance was successfully applied,the necessary space was created, and at the end of orthodontic treatment a space maintainer and a temporary tooth replacement has been done.
M.Sc. Ersela Alikaj1, 2, Prof. Dr. Xhina Mulo1, Dr. Alda Gjoni2
The sequelae of avulsed permanent central incisive and its treatment.Case report
1 University of Medicine,Faculty of Dental Medicine2 Dental Clinic “MATIS”
KEYWORDS:
Dental trauma,
Avulsion, Space
maintainer

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 93
emergency treatment and the importance of informing parents and patients regarding avulsionin .
Material and Method:A clinical case is presented, a child who has suff ered
the loss of the right centralpermanent tooth. The situation is presented with photos and X-rays at the timethe patient is presented for the fi rst time at the clinic. A removable appliance is applied to regain the missing space and to correct the eventual malocclusion, for a year. At the end,two ways of maintaining the spaceare presented.
Case presentationPatient E. B., 9 years old , was presented at our clinic
about more than a year after she lost the tooth 11 following an accident . Trauma was due to the fall in the garden of her house.Referring to the parents, she had laceration of lower lip and bleeding. The patient went to the oral surgeon for the fi rst intervention in the soft tissues two hours after the accident, but they did not preserve the avulsed tooth. The surgeon informed the
parents for the reimplantation procedure and for the necessity of an orthodontist as soon as possible. The patient was with no history of medical diseases. No intervention was made and the patient with her parents are presented at our clinic only after a year. The condition of the patient presented in photo 1 and 2 in the fi rst appointment.
In the photos is shown the reduced space that belonged to the tooth 11, displacement of teeth, shift to the right of the median line of the upper jaw and a signifi cant impairment of the aesthetics and phonetics of the little girl . Patient also introduces other dental problems: carious cavities, extracted tooth 16 as a result of complications of cariesin the past.
Once the model and also the radiographic examination that shows the reducedspace and other dental problems were studied,the situation was explained to the parents of the patient:the treatment alternatives, costs, the importance of treatment, the need of sanitation of the oral cavity.
We decided to apply a simple removable appliance, in order to recreate the needed space for the central tooth, and to treat the malocclusion (Photo 3, 4)
Photo 2
Photo 1

Albanian Stomatological Journal94
It is worth to mention that economic opportunities were limited, and parents were relatively cooperative regarding the time required for treatment.
Photo 5 shows the patient during the treatment:
After creating the necessary space, the next task is to preserve the space and tomade a temporary tooth replacement.
First was tried with retainer arc and direct composite reconstruction, but it resulted unsuccessful as a solution, because there was no proper sustainability (photo8,9).
Photo 3Photo 7
Photo 8
Photo 9
Photo 4
Photo 5
Photo 6
After about a year the needed space was created. The situation after the orthodontic treatment is shown in photo 6, 7
After that,it was decided to use a space maintainer,fi xed with bands on molars and a resin tooth for re - placement of the avulsed tooth. (Photo 10 , 11 , 12 , 13 ) .
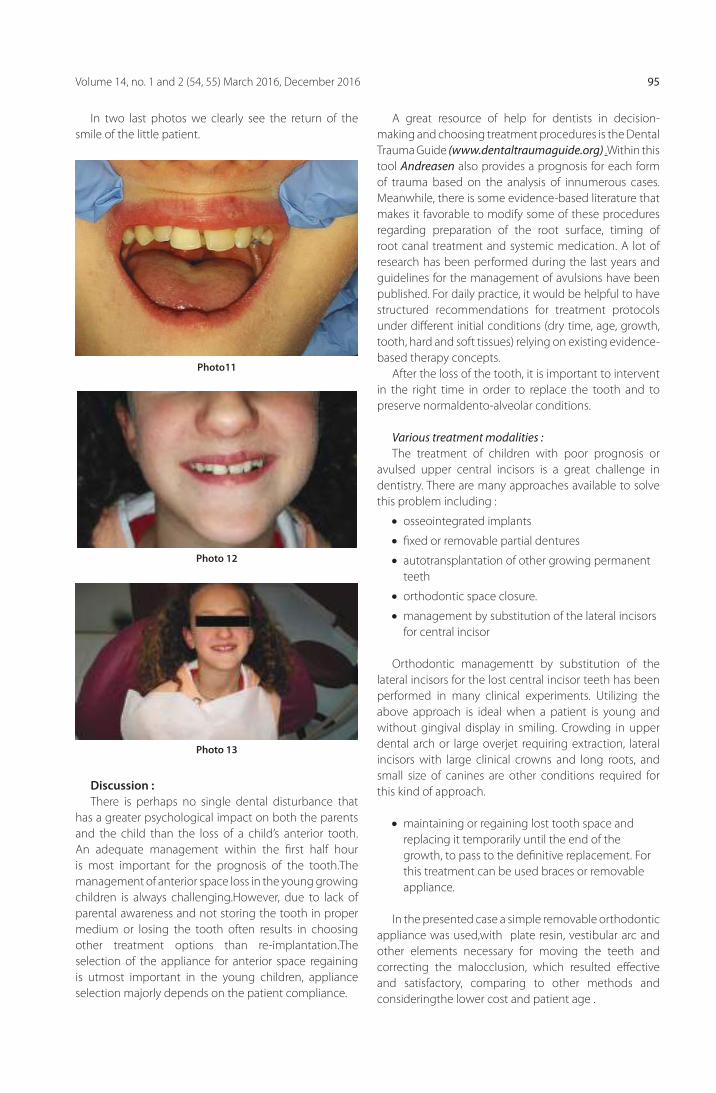
Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 95
In two last photos we clearly see the return of the smile of the little patient.
A great resource of help for dentists in decision-making and choosing treatment procedures is the Dental Trauma Guide (www.dentaltraumaguide.org) .Within this tool Andreasen also provides a prognosis for each form of trauma based on the analysis of innumerous cases. Meanwhile, there is some evidence-based literature that makes it favorable to modify some of these procedures regarding preparation of the root surface, timing of root canal treatment and systemic medication. A lot of research has been performed during the last years and guidelines for the management of avulsions have been published. For daily practice, it would be helpful to have structured recommendations for treatment protocols under diff erent initial conditions (dry time, age, growth, tooth, hard and soft tissues) relying on existing evidence-based therapy concepts.
After the loss of the tooth, it is important to intervent in the right time in order to replace the tooth and to preserve normaldento-alveolar conditions.
Various treatment modalities :The treatment of children with poor prognosis or
avulsed upper central incisors is a great challenge in dentistry. There are many approaches available to solve this problem including :
osseointegrated implants
fi xed or removable partial dentures
autotransplantation of other growing permanent teeth
orthodontic space closure.
management by substitution of the lateral incisors for central incisor
Orthodontic managementt by substitution of the lateral incisors for the lost central incisor teeth has been performed in many clinical experiments. Utilizing the above approach is ideal when a patient is young and without gingival display in smiling. Crowding in upper dental arch or large overjet requiring extraction, lateral incisors with large clinical crowns and long roots, and small size of canines are other conditions required for this kind of approach.
maintaining or regaining lost tooth space and replacing it temporarily until the end of the growth, to pass to the defi nitive replacement. For this treatment can be used braces or removable appliance.
In the presented case a simple removable orthodontic appliance was used,with plate resin, vestibular arc and other elements necessary for moving the teeth and correcting the malocclusion, which resulted eff ective and satisfactory, comparing to other methods and consideringthe lower cost and patient age .
Photo11
Photo 12
Photo 13
Discussion :The re is perhaps no single dental disturbance that
has a greater psychological impact on both the parents and the child than the loss of a child’s anterior tooth.An adequate management within the fi rst half hour is most important for the prognosis of the tooth.The management of anterior space loss in the young growing children is always challenging.However, due to lack of parental awareness and not storing the tooth in proper medium or losing the tooth often results in choosing other treatment options than re-implantation.The selection of the appliance for anterior space regaining is utmost important in the young children, appliance selection majorly depends on the patient compliance.

Albanian Stomatological Journal96
Positive sides are:Low CostSatisfactory resultRelatively no long time treatmentPossibility to maintain good hygienePeriodic checks to orthodontist prevent any
possible complication
Negative sides:
The necessity of cooperation of the patient.
Outcome and duration will depend heavily on the correct maintenance and appearance of the patient at appropriate intervals of time to the doctor to perform the necessary activations.
The appliance is relatively massive and may present diffi culties in speakingand holding properly during the treatment.
Conclusions:The traumatic loss of a permanent frontal tooth , can
be one of the most unfortunate dental accidents for a child and his parents.
The emergency intervention consists of the medication of eventual injuries of soft tissues, and if possible reimplantation as soon as possible of the avulsed tooth.
In case that this reimplantationof the avulsed tooth cannot be done, it is necessary applying the space maintainer, in order to prevent the dislocation of adjacent teeth, which can lead to malocclusion, poor esthetics and functional issues.In case that this is already happened, the orthodontist should correct the malocclusion, regain the missing space, maintain the space and temporary replace dhe missing tooth, till the growth is terminated, and after that, the necessary interventions can be performed to permanently replace the tooth.
1. Cortes M.I.S., Marcenes W., Sheiham A. Impact of traumatic injuries to the permanent teeth on the oral health-related quality of life of 12–14-year-old children. Commun. Dent. Oral Epidemiol. 2002;30:193–198.
2. Antunes L.A.A., Leão A.T., Maia L.C. The impact of dental trauma on quality of life of children and adolescents: A criti-cal review and measurement instruments. Ciênc. Saúde. Coletiva. 2012;17:3417–3424.
3. Bendo C.B., Paiva S.M., Varni J.Ë., Vale M.P. Oral health-related quality of life and traumatic dental injuries in Brazilian ado-lescents. Commun. Dent. Oral Epidemiol. 2014;42:216–223.
4. Glendor U. Aetiology and risk factors related to traumatic dental injuries—A revieë of the literature. Dent. Traumatol. 2009;25:19–31.
5. Livny A., Sgan-Cohen H.D., Junadi S., Marcenes W. Trau-matic dental injuries and related factors among sixth grade schoolchildren in four Palestinian toëns. Dent. Traumatol. 2010;26:422–426.
6. Traebert J., Marcon K.B., Lacerda J.T. Prevalence of traumatic dental injuries and associated factors in schoolchildren of Palhoça, Santa Catarina State. Ciênc. Saúde. Coletiva. 2010;15:1849–1855.
7. Lee JY, Divaris K. Hidden consequences of dental trauma: the social and psychological eff ects. Pediatr Dent. 2009;31:96–101.
8. Andreasen JO, Andreasen FM, Andersson L. Textbook and color atlas of traumatic injuries to the teeth. 4. Oxford: John wiley Professional; 2007.
9. Locker D. Prevalence of traumatic dental injury in grade 8 children in six Ontario communities. Can J Public Health. 2005;96:73
10. Fleming P. S., Seehra J., Dibiase A. T. Combined orthodon-tic-restorative management of maxillary central incisors lost following traumatic injury: a case report. Orthodon-tics. 2011;12(3):242–251.
11. Kokich V. G., Nappen D. L., Shapiro P. A. Gingival contour and clinical crown length: their eff ect on the esthetic ap-pearance of maxillary anterior teeth. American Journal of Orthodontics. 1984;86(2):89–94. doi: 10.1016/0002-9416(84)90300-2.
12. Kokich V. G., Kokich V. O. Interrelationship of orthodontics with periodontics and restorative dentistry. In: Nanda R., editor. Biomechanics and Esthetic Strategies in Clinical Or-thodontics. St. Louis, Mo, USA: Elsevier; 2005.
13. Kovich V. Esthetics and anterior tooth position: an orth-odontic perspective. Part I: croën length. Journal of Esthetic and Restorative Dentistry. 1993;5(1):19–23. doi: 10.1111/j.1708-8240.1993.tb00739.x.
14. Kokich V. G., Spear F. M. Guidelines for managing the orthodontic-restorative patient. Seminars in Orthodon-tics. 1997;3(1):3–20. doi: 10.1016/S1073-8746(97)80036-9.
15. Kokich V. G. Esthetics and vertical tooth position: orthodon-tic possibilities. Compendium of Continuing Education in Dentistry. 1997;18(12):1225–1231.
REFERENCES :

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 97
AbstraktNje lesion I perbere nga indi osteoid eshte hequr gjate nje intervenimi kirurgjikal nje ditor pa ndonje augmentacion me materiale zevendesuese kockore. Nuk patem komplikime post operative. Radiografi te percjellese te bera pas 3 muajsh respektivisht dy viteve, treguan se plaga eshte sheruar plotesisht.
Perfundim: 1. Odontomat jane lezione benigne te cilat mund te trajtohen me procedura nje ditore kirurgjikale pa nevoje absolute per augmentacion me materiale ksenogjene ose alogjene kockore.
Hyrje: Odontomat përbëjnë një defekt zhvillimi të indeve të forta të dhëmbëve dhe janë klasifi kuar si tumore beninje odontogene. Ata janë të përbërë nga të gjitha strukturat e dhëmbëve dhe indet si: zmalti, dentini,cementi dhe pulpa. Ne saje te karakteristikave histomorfologjike ,dallohen dy lloje të odontomave : komplekse dhe compound ( te perbera ).Odontomat përfaqësojnë nga 4.7% deri në 76% të tumoreve odontogjene. Etiologjia e tyre nuk eshte e sqaruar akoma. Lendimet, infeksionet dhe faktorët gjenetik janë emeruar shpesh ndër shkaqet. Odontomat zakonist janë zbuluar rastësisht në imazhet radiografi ke te marra në lidhje erupcionet e munguara ose erupcionet ektopike te dhembeve.
Qëllimi i studimit: Të paraqesim rastin studimor te një odontomi complex në anën e majtë te mandibulles te një vajzë 11-vjeçare.
Materialet, metodat dhe rezultatet: Analizat perfshine dokumentacionin mjekësor te pacientes, materijalet diagnostike, radiografi te orthopantomografi ke dhe përshkrimi i protokollit operativ. Rasti studimor ka qenë I komparuar me literature recente te derisotme.
Ph.D. Nedim Kasami, Dr. Vladimir Popvski
Odontoma e mandibules. Prezantim rasti
Klinika Universitare per kirurgji maksilofaciale. Qendra Klinike “Nënë Tereza”, Shkup, Republika e Maqedonisë.
FJALËT KYÇE:
kompleks
odontoma,
egzaminime
radiografi ke,
tumore
odontogjene.
Hyrje Odontomat janë një defekt të zhvillimit të indeve të
forta të dhëmbëve. Ato janë klasifi kuar nga Organizata Botërore e Shëndetësisë, si beninje, lezione odontogjene te ngjajshme me tumoret (hamartoma). Ato janë të vendosura në regjionin maksilofacial, në eshtrat dhe indet e buta percjellese [1] dhe janë të përbëra nga të gjitha strukturat e dhëmbëve dhe indet, dmth smalta, dentina, cementi dhe pulpa [2]. Odontomat mund të dallohen në bazë të paraqitjeve të tyre anatomike: compound odontoma (strukturave të vogla te ngjajshme me dhembin), complex odontoma (një konglomerat nga dentina, smalta dhe cementumi) dhe cistike [3].
Diagnoza mund të verifi kohet me egzaminim radiografi k. Odontomat më tej nën-klasifikohen në bazë të madhesise dhe karakteristikave të tyre radiografike ne compound dhe complex odontoma.
Etiologjia e formacioneve odontomatike nuk është e kuptuar ende plotësisht. Ata zhvillohen nga komponentët epiteliale dhe mezenhimale të aparatit dentar, duke prodhuar smalt dhe dentin. Ata mund të paraqiten në çdo moshë, por janë më të shpeshta në dy dekadat e para të jetës, me një moshë mesatare prej 14-18 vjeç. Faktorë të tjerë të mundshem përfshijnë çështje
gjenetike si hiperaktivitet odontoblastik dhe ndryshimet në komponentët gjenetike përgjegjëse për kontrollin e zhvillimit dentar, si qe jane sindromi Gardner ose sindromi Hermann.
Odontomat janë në përgjithësi të vogla, megjithatë, rastesisht mund të rriten dhe të behen te mëdhaja, duke rezultuar në ekspansionin e kockave (4).
Histologjikisht, odontomat compound kanë strukture te ngjajshme me dhëmbin te cilat janë te radhitura ne menyre uniforme, ngjajshem me dhembin normal. Strukturat në odontomat komplekse janë të përziera dhe të paorganizuara (5).
Diagnoza diferenciale perfshin: Ameloblastoma, myxoma, ameloblastic fi bro-odontoma, cementoblasto-ma, fi broma ameloblastike dhe tumori epithelial odonto-gjen kalcifi kues të cilat janë me shpesh te vendosura në regjionin posterior te mandibulles (6).
Recidive nuk jane te pershkruara, në qoftë se ajo përsëritet, duhet të menjanohen lezionet e tjera odontogjene si qe jane cista odontogjene kalcifi kuese dhe fi bro odontoma ameloblastike (7-8).
Qasje konzervative qe nenkupton enukleacion kirurgjikal ose kiretazhe eshte zgjedhja adekuate. Giansanti et al. pasi qe percjelli nje numer te
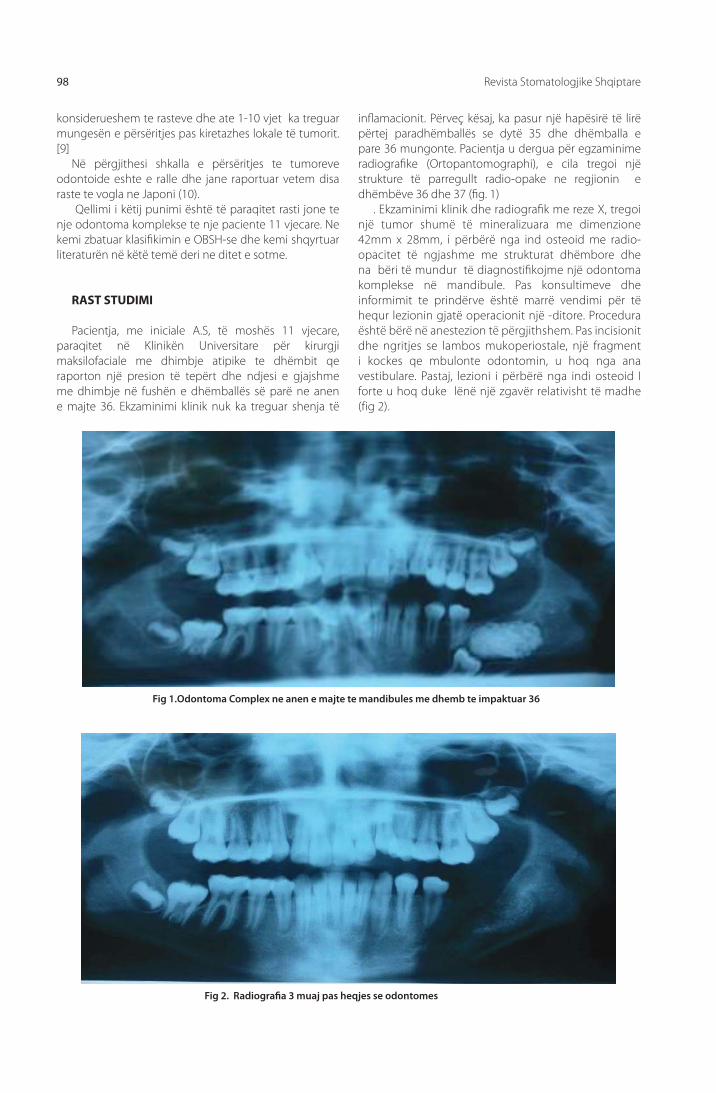
Revista Stomatologjike Shqiptare98
konsiderueshem te rasteve dhe ate 1-10 vjet ka treguar mungesën e përsëritjes pas kiretazhes lokale të tumorit. [9]
Në përgjithesi shkalla e përsëritjes te tumoreve odontoide eshte e ralle dhe jane raportuar vetem disa raste te vogla ne Japoni (10).
Qellimi i këtij punimi është të paraqitet rasti jone te nje odontoma komplekse te nje paciente 11 vjecare. Ne kemi zbatuar klasifi kimin e OBSH-se dhe kemi shqyrtuar literaturën në këtë temë deri ne ditet e sotme.
RAST STUDIMI
Pacientja, me iniciale A.S, të moshës 11 vjecare, paraqitet në Klinikën Universitare për kirurgji maksilofaciale me dhimbje atipike te dhëmbit qe raporton një presion të tepërt dhe ndjesi e gjajshme me dhimbje në fushën e dhëmballës së parë ne anen e majte 36. Ekzaminimi klinik nuk ka treguar shenja të
infl amacionit. Përveç kësaj, ka pasur një hapësirë të lirë përtej paradhëmballës se dytë 35 dhe dhëmballa e pare 36 mungonte. Pacientja u dergua për egzaminime radiografi ke (Ortopantomographi), e cila tregoi një strukture të parregullt radio-opake ne regjionin e dhëmbëve 36 dhe 37 (fi g. 1)
. Ekzaminimi klinik dhe radiografi k me reze X, tregoi një tumor shumë të mineralizuara me dimenzione 42mm x 28mm, i përbërë nga ind osteoid me radio-opacitet të ngjashme me strukturat dhëmbore dhe na bëri të mundur të diagnostifi kojme një odontoma komplekse në mandibule. Pas konsultimeve dhe informimit te prindërve është marrë vendimi për të hequr lezionin gjatë operacionit një -ditore. Procedura është bërë në anestezion të përgjithshem. Pas incisionit dhe ngritjes se lambos mukoperiostale, një fragment i kockes qe mbulonte odontomin, u hoq nga ana vestibulare. Pastaj, lezioni i përbërë nga indi osteoid I forte u hoq duke lënë një zgavër relativisht të madhe (fig 2).
Fig 1.Odontoma Complex ne anen e majte te mandibules me dhemb te impaktuar 36
Fig 2. Radiografi a 3 muaj pas heqjes se odontomes

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 99
Nuk gjetem kapsule te defi nuar te qarte por pak a shume lezioni ishte mire I ndare nga kocka e shendoshe perreth.
Molari i pare i impaktuar ( i vendosur gati pranë tehut te poshtem të mandibules) gjithashtu u hoq me osteotomi. Hemostaze e përpiktë është kryer dhe plaga u mbyll me qepje pa e plotësuar zgavrën me ndonje graft zëvendësues kockor. Materiali është dërguar për ekzaminim histopatologjik e cila konfi rmoi diagnozën e një odontoma komplekse. Pas 10 ditëve plaga u shërua si duhet dhe u hoqën suturat. Orthopantomographite percjellese te marë tre muaj më vonë (fi g. 2) konfi rmoi se procesi i shërimit te plages ishte korekt. Radiografi ja e mare pas dy vitesh më vonë tregoi shërim të plotë dhe mineralizim te hapësirës së zonës se operuar si dhe folikulla e dhëmballës se tretë ishte e dukshme (fi g 3).
DISKUTIMI
Në rastin tonë, shqyrtimi histopatologjike tregoi një tumor odontogjen dhe, e kombinuar me fotot klinike, intraoperative dhe radiografi te, ka konfi rmuar diagnozën e odontoma komplekse.
Për shkak të mungesës së simptomave të qarta te dhimbjes (jo në rastin tonë), lezionet te tipit odontomatik zakonisht zbulohen rastësisht - në imazhet radiografi ke të marra për shkak të erupcionit të ndërprerë ose anomali dentare të lidhura me maloklusion [11].
Në imazhet radiografi ke, lezionet duken si fokuse radio-opake te rrethuar me një aureolë radiolucente ose si një numër i vatrave të tilla qe përfaqësojnë odontoide (në odontomat përbëra-compound odontoma). Prania e tyre mund të tregohet nga zgjerimi kockave, dhimbje të lehtë ekspandimi ,erupcion i vonuar apo mungese shpërthimi te dhëmbëve të përhershëm ose perzistenca e dhëmbëve qumeshtore [12].
Fig. 3. Dy vjet me pas . Vereni mineralizimin e zones se operuar dhe dukshmerine e folikules se dhembit 38
Fig.4. Pamje inraorale qe tregon erupcion te nje mase te ngjashme me dhembin nga mukoza e anes se djathte te faqes
Odontomat e përbërë janë më të zakonshme në nofullat e përparme, ndërsa odontomat komplekse paraqiten më shpesh në pjeset e pasme te nofullave..
Rrallë mund tëjene te vendosura në indet e buta si mukoza bukale qe raportohet nga Venigalla et al. (13).
Në rastin tonë nuk gjetem dhëmbë te qumeshtit te perzistuar. Kishte mungese te dhëmbëve të përhershëm në mandibule dhe një hapësirë të lirë pa dhëmbë ne anen posteriore të paradhëmballës se dytë ne anën e majtë.
Odontomat kompound zakonisht përbëhen nga disa odontoide dhe madhësia e tyre ndryshon [14]. Një numër te ngjashëm te odontoideve (37 mostra) është identifi kuar nga Kubasiewicz-Ros et al (15) dhe nga Niharika në vende te ndryshme ( sektori i përparme i maksilles) (16).
Në rastin e përshkruar nga Jankowska et al, një odontoma kompleks e hequr te një i ri ishte i përbërë nga 19 odontoide (17).
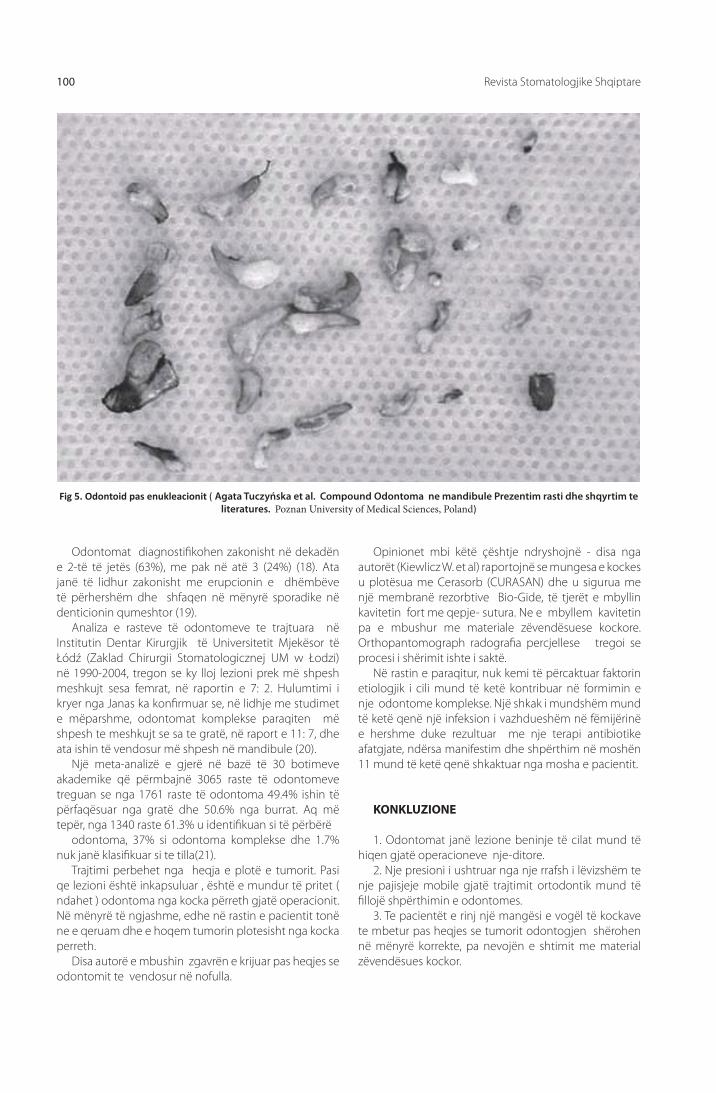
Revista Stomatologjike Shqiptare100
Odontomat diagnostifi kohen zakonisht në dekadën e 2-të të jetës (63%), me pak në atë 3 (24%) (18). Ata janë të lidhur zakonisht me erupcionin e dhëmbëve të përhershëm dhe shfaqen në mënyrë sporadike në denticionin qumeshtor (19).
Analiza e rasteve të odontomeve te trajtuara në Institutin Dentar Kirurgjik të Universitetit Mjekësor të Łódź (Zaklad Chirurgii Stomatologicznej UM w Łodzi) në 1990-2004, tregon se ky lloj lezioni prek më shpesh meshkujt sesa femrat, në raportin e 7: 2. Hulumtimi i kryer nga Janas ka konfi rmuar se, në lidhje me studimet e mëparshme, odontomat komplekse paraqiten më shpesh te meshkujt se sa te gratë, në raport e 11: 7, dhe ata ishin të vendosur më shpesh në mandibule (20).
Një meta-analizë e gjerë në bazë të 30 botimeve akademike që përmbajnë 3065 raste të odontomeve treguan se nga 1761 raste të odontoma 49.4% ishin të përfaqësuar nga gratë dhe 50.6% nga burrat. Aq më tepër, nga 1340 raste 61.3% u identifi kuan si të përbërë
odontoma, 37% si odontoma komplekse dhe 1.7% nuk janë klasifi kuar si te tilla(21).
Trajtimi perbehet nga heqja e plotë e tumorit. Pasi qe lezioni është inkapsuluar , është e mundur të pritet ( ndahet ) odontoma nga kocka përreth gjatë operacionit. Në mënyrë të ngjashme, edhe në rastin e pacientit tonë ne e qeruam dhe e hoqem tumorin plotesisht nga kocka perreth.
Disa autorë e mbushin zgavrën e krijuar pas heqjes se odontomit te vendosur në nofulla.
Opinionet mbi këtë çështje ndryshojnë - disa nga autorët (Kiewlicz W. et al) raportojnë se mungesa e kockes u plotësua me Cerasorb (CURASAN) dhe u sigurua me një membranë rezorbtive Bio-Gide, të tjerët e mbyllin kavitetin fort me qepje- sutura. Ne e mbyllem kavitetin pa e mbushur me materiale zëvendësuese kockore. Orthopantomograph radografi a percjellese tregoi se procesi i shërimit ishte i saktë.
Në rastin e paraqitur, nuk kemi të përcaktuar faktorin etiologjik i cili mund të ketë kontribuar në formimin e nje odontome komplekse. Një shkak i mundshëm mund të ketë qenë një infeksion i vazhdueshëm në fëmijërinë e hershme duke rezultuar me nje terapi antibiotike afatgjate, ndërsa manifestim dhe shpërthim në moshën 11 mund të ketë qenë shkaktuar nga mosha e pacientit.
KONKLUZIONE
1. Odontomat janë lezione beninje të cilat mund të hiqen gjatë operacioneve nje-ditore.
2. Nje presioni i ushtruar nga nje rrafsh i lëvizshëm te nje pajisjeje mobile gjatë trajtimit ortodontik mund të fi llojë shpërthimin e odontomes.
3. Te pacientët e rinj një mangësi e vogël të kockave te mbetur pas heqjes se tumorit odontogjen shërohen në mënyrë korrekte, pa nevojën e shtimit me material zëvendësues kockor.
Fig 5. Odontoid pas enukleacionit ( Agata Tuczyńska et al. Compound Odontoma ne mandibule Prezentim rasti dhe shqyrtim te literatures. Poznan University of Medical Sciences, Poland)

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 101
1. Barnes L, Everson JW, Reichart P, Sidransky D. Pathol-ogy and Genetics of Head and Neck Tumours. IARC Press. 2005;285:310-311.
2. Tyagi P., Singla S. Complex composite odontome. J Clin Pe-diatr Dent. 2010;3(2):117-120.
3. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxil-lofacial Pathology. 3rd ed. Philadelphia: W.B Saunders Co.; 2009.
4. Oz YG, Tosun G, Kiziloğlu D, Durmuş E, Şener Y. An unusual association of odontomas with primary teeth. Eur J Dent. 2007;1:45–49. [PMC free article] [PubMed]
5. Srivastava A, Annaji AG, Nyamati BS, Singh G, Shivakumar GC, Sahana S. Complex odontoma in both the jaws: a rare case report. J Orofac Res. 2012;2:56–60.
6. Guerrisi M, Piloni MJ, Keszler A. Odontogenic tumors in children and adolescents. A 15-year retrospective study in Argentina. Med Oral Patol Oral Cir Bucal. 2007;12:E180–5. [PubMed]
7. Reichart PA, Philipsen HP. Odontogenic tumors and allied lesions. London: Quintessence; 2004. Compound odon-toma; pp. 149–153
8. Chen Y, Li TJ, Gao Y. Ameloblastic fi broma and related le-sions: a clinicopathologic study with reference to their na-ture and inter-relationship. J Oral Pathol Med. 2005;34:588–595. [PubMed]
9. Giansanti JS, Someren A, Waldron CA. Odontogenic adeno-matoid tumor (adenoameloblastoma). Survey of 3 cases. Oral Surg Oral Med Oral Pathol. 1970;30:69–88. [PubMed]
10. Reichart PA, Philipsen HP. Odontogenic Tumors and Allied Le-sions. London: Quintessence Publishing; 2004. pp. 105–15.
11. Kiewlicz W, Gawrońska Skorkowska J, Szycik V, Dijakiewic-zM. Leczenie implantoprotetyczne po usunięciu zębiaka złożonego żuchwy – opis przypadku. 2005. Prot Stom. LV(5):357-361.
12. Khan N, Shrivastava N, Shrivastava TV, Samadi FM. An-unusual case of compound odontome associated with maxillary impacted central incisor. Natl J Maxillofac Surg. 2014;5(2):192-194.
13. Venigalla A, Guttikonda LK, Nelakurthi H, Babburi S, Pinisetti S, Kotti AB, Kalapala L. Ectopic CompoundOdontoma in the Buccal Mucosa: Report of a Rare Case.
Case Reports in Dentistry. 2015;2015:1-4.
14. Lee ChH, Park GJ. Complex and compound odontomas are clinico-pathological entities. Basic and Applied Pathology. 2008;1:30-33.
15. Kubasiewicz-Ross P, Mochniej H, Mierzwa D, Hadzik J. Zębiak zestawny kości żuchwy zawierający 37 odon-toidów. Opis przypadku. Magazyn Stomatologiczny. 2015;4:40-42.
16. Niharika P, Reddy BVT, Kiran MJ, Boyapati R, Keerti PS. Super Odontoma – A Destructive Swarm Entity. JCDR. 2015;9(3):1
17. Janowska K, Bogacz M, Dziadek H, Obersztyn I. Zębiakzłożony przyczyną zatrzymania zębów stałych – opis przypadku. TPS. 2015;5:42-44.
18. Khan M, ud Din Q, Ishfaq M. Odontomes − a descriptive case series on 38 patients. JKCD. 2011;1(2):91-94.
19. Mathew AK, Shenai P, Chatra L, Veena KM, Rao PK, Prabhu R. Compound odontoma in deciduous dentition. Ann Med Health Sci Res. 2013;3(2):285-287.
20. Janas A. Zębiaki złożone zlokalizowane w miejscu nie wyrzniętych zębów. Implantoprotetyka. 2008;IX (3):28-30.
21. Hidalgo-Sánchez O, Leco-Berrocal MI, Martínez-GonzálezJM. Meta-analysis of theepidemiology and clini-calmanifestations of odontomas. Med Oral Patol Oral CirBu-cal. 2008;13:730-734.
REFERENCA

Albanian Stomatological Journal102
Abstract:
Introduction: Odontomas constitute a developmental defect of hard dental tissues and are classifed as benign odontogenic tumours. They are composed of all dental structures and tissues: enamel, dentin, cementum and pulp. As regards histomorphological features, two types of odontomas have been diferentiated: complex and compound.Odontomas represent from 4.7% to 76% of odontogenic tumours. Their aetiology has not been fully understood. Injury, infection and genetic factors are often named among the causes. Odontomas are usually detected by chance in radiographic images taken in relation to disrupted eruption or mislocation of teeth.
Aim of study: To present the case study of an erupting compound odontoma on the left side of the mandible in an 11-year-old girl.
Material, methods and results: The analysis covered medical documentation of the patient, diagnostic casts, orthopantomographs and description of operative protocol. The case study has been complemented with the review of up-to-date literature.A lesion composed of osteoid tissue was removed during one-day surgery without subsequent augmentation with bone substitute material. There were no post-surgery complications. A follow-up orthopantomograph taken 3 months and 2 years later showed that the wound had been healing correctly.
Conclusions: 1. Odontomas are benign lesions which can be removed during one-day surgery without the absolute need of augmentation with xenogenic or allogenic material.
Ph.D. Nedim Kasami, Dr. Vladimir Popvski
Odontoma of the Mandible. Case Report
University Clinic for Maxillofacial SurgeryClinical Center “Mother Teresa” Skopje Republic of Macedonia
KEYWORDS:
complex
odontoma,
clinical
manifestations,
radiographic
examination
INTRODUCTIONOdontomas are a developmental defect of hard
dental tissues. They have been classifi ed by the World Health Organisation as benign, tumour-like odontogenic lesions (hamartoma). They are located in themaxillofacial area, in bones and adjacent sof tissues [1] and are composed of all of the dental structures and tissues, i.e. enamel, dentin, cementum and pulp [2]. Odontomas can be diff erentiated according to their anatomical presentations: Compound odontoma-clusters of several denticles and complex odontoma-well defi ned tumefaction mass. The diagnosis can be performed by radiographic examination. Odontomas are further sub-classifi ed based upon their gross and radiographic features into compound (small tooth-like structures), complex (a conglomeration of dentin, enamel and cementum) and cystic.(3).
The aetiology of odontoma formation has not been fully understood. They develop from epithelial and mesenchymal components of the dental apparatus, producing enamel and dentin. They can occur at any age, but are most common in the first two decades of life, with an average age of 14–18 years.
Other probable factors include genetic issues such as odontoblastic hyperactivity and alterations in the genetic components responsible for controlling dental development, Gardner syndrome or Hermann syndrome.
Odontomas are generally small; however, they may occasionally grow large, resulting in bone expansion (4).
Histologically, compound odontoma have the tooth-like structures which are arranged in a uniform manner similar to the normal tooth. The structures in complex odontomas are mixed and disorganized (5).
Diff erential diagnosis considers: Ameloblastoma, myxoma, ameloblastic fi bro odontoma, cementoblas-toma, ameloblastic fi broma, and calcifying epithelial od-ontogenous tumor which were more frequently located in the posterior region of the mandible (6).
Recurrence is not described; if it recurs, one must rule out other odontogenic lesions such as calcifying odontogenic cyst and ameloblastic fi bro-odontoma (7-8)
Conservative approach by means of surgical enucleation or curettage is the treatment of choice.
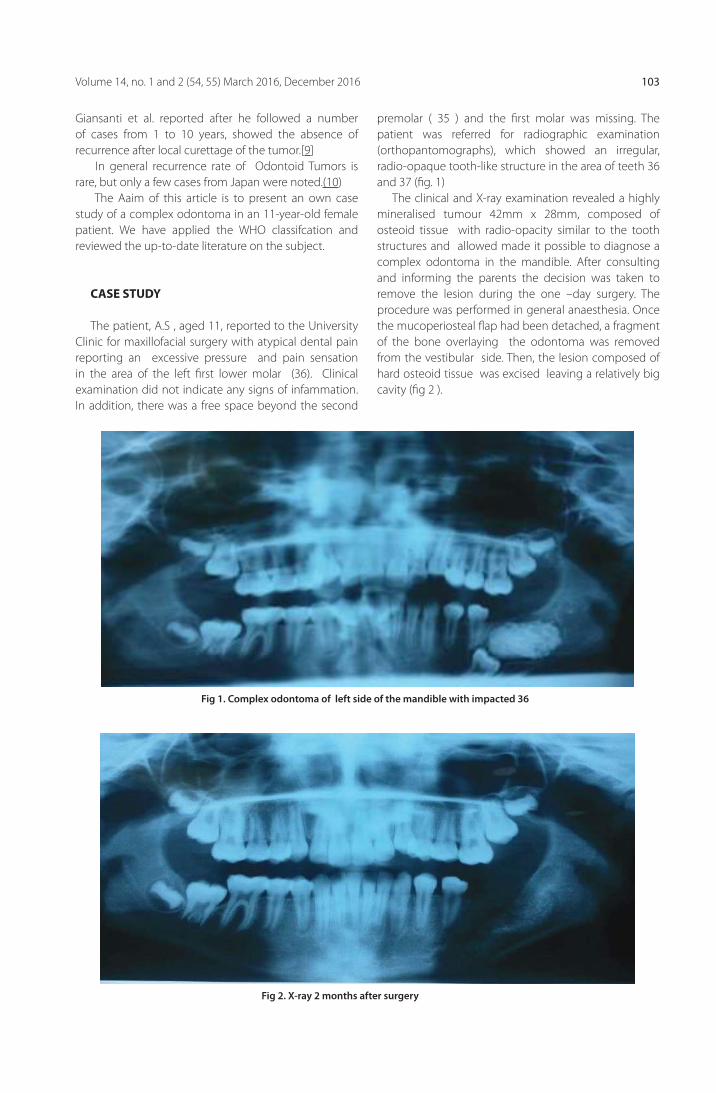
Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 103
Giansanti et al. reported after he followed a number of cases from 1 to 10 years, showed the absence of recurrence after local curettage of the tumor.[9]
In general recurrence rate of Odontoid Tumors is rare, but only a few cases from Japan were noted.(10)
The Aaim of this article is to present an own case study of a complex odontoma in an 11-year-old female patient. We have applied the WHO classifcation and reviewed the up-to-date literature on the subject.
CASE STUDY
The patient, A.S , aged 11, reported to the University Clinic for maxillofacial surgery with atypical dental pain reporting an excessive pressure and pain sensation in the area of the left fi rst lower molar (36). Clinical examination did not indicate any signs of infammation. In addition, there was a free space beyond the second
premolar ( 35 ) and the fi rst molar was missing. The patient was referred for radiographic examination (orthopantomographs), which showed an irregular, radio-opaque tooth-like structure in the area of teeth 36 and 37 (fi g. 1)
The clinical and X-ray examination revealed a highly mineralised tumour 42mm x 28mm, composed of osteoid tissue with radio-opacity similar to the tooth structures and allowed made it possible to diagnose a complex odontoma in the mandible. After consulting and informing the parents the decision was taken to remove the lesion during the one –day surgery. The procedure was performed in general anaesthesia. Once the mucoperiosteal fl ap had been detached, a fragment of the bone overlaying the odontoma was removed from the vestibular side. Then, the lesion composed of hard osteoid tissue was excised leaving a relatively big cavity (fi g 2 ).
Fig 1. Complex odontoma of left side of the mandible with impacted 36
Fig 2. X-ray 2 months after surgery

Albanian Stomatological Journal104
We did not found well defi ned capsule, but nevertheless the lesion was well circumscribed from the surrounding healthy bone.
The impacted fi rst molar ( placed almost near the inferior margin of the mandible ) was also operatively extracted. Meticulous haemostasis was performed and the wound was closed with sutures without fi lling the cavity with any bone substitute. The material was sent for histopathological examination which confi rmed the diagnosis of a complex odontoma . After 10 days the wound was declared to heal correctly and the sutures were removed. Follow- up orthopantomographs taken three months later (fi g. 2) confi rmed that the wound healing process was correct. Two years late orthopantomograph showed complete healing and mineralization of the space of the operated area as well the follicle of the third molar was visible (fi g 3).
DISCUSSION
In our case, the histopathological examination indicated an odontogenic tumour and, combined with the clinical and intraoperative picture, confi rmed the diagnosis of a complex odontoma. Due to the lack of distinct pain symptoms ( not in our case ), odontoma-type lesions are usually discovered by chance – in radiographic images taken because of disrupted eruption or dental anomalies in malocclusion [11].
In radiographic images, lesions are visible as a well-defi ned radio-opaque focus surrounded with a radiolucent halo or as a number of such foci representing odontoids ( in compound odontoma ). Their presence may be indicated by bone expansion, slight expanding pain, delayed or arrested eruption of permanent teeth or persistent deciduous teeth [12].
Fig. 3. Two years after. Notice the mineralization and the follicle of 38
Fig 4. Intraoral view showing eruption of tooth-like mass from right buccal mucosa.
Compound odontomas are more common in the anterior jaws, while complex odontomas occur more often in the posterior jaws.
Rarely they can be placed in the soft tissues as buccal mucosa reported by Venigalla et al.(13).
In our case we did not identify persistent deciduous teeth. There was missing permanent teeth in the mandible and a free toothless space posterior to the second premolar of the left side.
Compound odontomas are usually composed of several odontoids and their size oscillates [14]. A similar number of odontoids (37 specimens) was identifi ed by Kubasiewicz-Ros et al (15) and by Niharika at a diff erent location (the anterior section of the maxilla) (16).

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 105
In the case described by Jankowska et al, a complex odontoma removed in a teenager was composed of 19 odontoids (17).
Odontomas are diagnosed usually in the 2nd decade of life (63%), lessoften in the 3rd one (24%) (18). They are usually associated with permanent dentition and appear sporadically in deciduous dentition (19). The analysis of odontoma cases treated in the Dental Surgery Institute of the Medical University of Łódź (Zakład Chirurgii Stomatologicznej UM w Łodzi) in 1990-2004 indicates that this type of lesion aff ects more often men than women, at the ratio of 7:2. The research conducted by Janas confi rmed that, in relation to the earlier studies, complex odontomas occur more often in men than women, at the ration of 11:7, yet they were more often located in the mandible (20).
An extensive meta-analysis based on 30 academic publications containing 3065 cases of odontoma demonstrated that out of 1761 cases of odontoma 49.4% were represented by women and 50.6% by men. Moreover, out of 1340 cases 61.3% were identifi ed as compound odontoma, 37% as complex odontoma and 1.7% were not classiffi ed as either (21).
The treatment consists in complete excision of the tumour. As the lesion is encapsulated, it is possible to dissect the odontoma from the surrounding bone during the surgery. Similarly, also in the case of our patient, the odontoma located in the mandible was fully removed.
Some authors fi ll the cavity created after the removal
of the odontoma. Opinions on that matter vary – some of the authors ( Kiewlicz W. et al ) report that bone defi ciency was complemented with Cerasorb (Curasan) and secured with a resorbable Bio-Gide membrane, others close the cavity tightly with sutures. We closed the cavity without fi lling it with bone substitute material. The follow-up orthopantomograph showed that the healing process was correct.
In the presented case, we did not determine the aetiological factor, which might have contributed to the complex odontoma. A possible cause might have been a persistent infection in early childhood and athe resulting lated long-term antibiotics therapy, whereas its
manifestation and eruption at the age of 11 might have been triggered by the age of the patient.
CONCLUSIONS
1. Odontomas are benign lesions which may be excised during a one-day surgery.
2. The pressure exerted by the plate of a removable ap-pliance during the orthodontic treatment may initiate the eruption of the odontoma.
3. In young patients a slight bone defi ciency left after the excision of an odontogenic tumour heals correctly without the need of augmentation with bone substitute material (an this is up to theindividual decision of athe surgeon).
Fig 5. Odontoids after enucleation ( Agata Tuczyńska et al. Compound Odontoma in the mandible Case study and literature review Poznan University of Medical Sciences, Poland)
Albanian Stomatological Journal106
1. Barnes L, Everson JW, Reichart P, Sidransky D. Pathol-ogy and Genetics of Head and Neck Tumours. IARC Press. 2005;285:310-311.
2. Tyagi P., Singla S. Complex composite odontome. J Clin Pe-diatr Dent. 2010;3(2):117-120.
3. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxil-lofacial Pathology. 3rd ed. Philadelphia: W.B Saunders Co.; 2009.
4. Oz YG, Tosun G, Kiziloğlu D, Durmuş E, Şener Y. An unusual association of odontomas with primary teeth. Eur J Dent. 2007;1:45–49. [PMC free article] [PubMed]
5. Srivastava A, Annaji AG, Nyamati BS, Singh G, Shivakumar GC, Sahana S. Complex odontoma in both the jaws: a rare case report. J Orofac Res. 2012;2:56–60.
6. Guerrisi M, Piloni MJ, Keszler A. Odontogenic tumors in children and adolescents. A 15-year retrospective study in Argentina. Med Oral Patol Oral Cir Bucal. 2007;12:E180–5. [PubMed]
7. Reichart PA, Philipsen HP. Odontogenic tumors and allied lesions. London: Quintessence; 2004. Compound odon-toma; pp. 149–153
8. Chen Y, Li TJ, Gao Y. Ameloblastic fi broma and related le-sions: a clinicopathologic study with reference to their na-ture and inter-relationship. J Oral Pathol Med. 2005;34:588–595. [PubMed]
9. Giansanti JS, Someren A, Waldron CA. Odontogenic adeno-matoid tumor (adenoameloblastoma). Survey of 3 cases. Oral Surg Oral Med Oral Pathol. 1970;30:69–88. [PubMed]
10. Reichart PA, Philipsen HP. Odontogenic Tumors and Allied Le-sions. London: Quintessence Publishing; 2004. pp. 105–15.
11. Kiewlicz W, Gawrońska Skorkowska J, Szycik V, Dijakiewic-zM. Leczenie implantoprotetyczne po usunięciu zębiaka złożonego żuchwy – opis przypadku. 2005. Prot Stom. LV(5):357-361.
12. Khan N, Shrivastava N, Shrivastava TV, Samadi FM. An-unusual case of compound odontome associated with maxillary impacted central incisor. Natl J Maxillofac Surg. 2014;5(2):192-194.
13. Venigalla A, Guttikonda LK, Nelakurthi H, Babburi S, Pinisetti S, Kotti AB, Kalapala L. Ectopic CompoundOdontoma in the Buccal Mucosa: Report of a Rare Case.
Case Reports in Dentistry. 2015;2015:1-4.
14. Lee ChH, Park GJ. Complex and compound odontomas are clinico-pathological entities. Basic and Applied Pathology. 2008;1:30-33.
15. Kubasiewicz-Ross P, Mochniej H, Mierzwa D, Hadzik J. Zębiak zestawny kości żuchwy zawierający 37 odon-toidów. Opis przypadku. Magazyn Stomatologiczny. 2015;4:40-42.
16. Niharika P, Reddy BVT, Kiran MJ, Boyapati R, Keerti PS. Super Odontoma – A Destructive Swarm Entity. JCDR. 2015;9(3):1
17. Janowska K, Bogacz M, Dziadek H, Obersztyn I. Zębiakzłożony przyczyną zatrzymania zębów stałych – opis przypadku. TPS. 2015;5:42-44.
18. Khan M, ud Din Q, Ishfaq M. Odontomes − a descriptive case series on 38 patients. JKCD. 2011;1(2):91-94.
19. Mathew AK, Shenai P, Chatra L, Veena KM, Rao PK, Prabhu R. Compound odontoma in deciduous dentition. Ann Med Health Sci Res. 2013;3(2):285-287.
20. Janas A. Zębiaki złożone zlokalizowane w miejscu nie wyrzniętych zębów. Implantoprotetyka. 2008;IX (3):28-30.
21. Hidalgo-Sánchez O, Leco-Berrocal MI, Martínez-GonzálezJM. Meta-analysis of theepidemiology and clini-calmanifestations of odontomas. Med Oral Patol Oral CirBu-cal. 2008;13:730-734.
REFERENCES

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 107
AbstraktKy studim përshkruan rastin e trajtimit të një vajze 8-vjeçare me kafshim kryqëzuar anterior, duke përdorur një seri të apartesh të lëvizshme për të sjell dhëmbët në okluzion normal. Për të korrigjuar kafshimin e kryqëzuar anterior dhe për të rrjeshtuar ashtu siç duhet incizivët u përdor një aparat i lëvizshëm me pllakë me bazë rezinën që përfshin brenda saj vidat që bëjnë të mundur zgjerimin. Dalja e vone e incisivit lateral të majtë maksilar u trajtua me një pllakë rezine të dytë e cila përfshinte një sustë labiolinguale. Pas një periudhe 8 mujore, kafshimi i kryqëzuar anterior që përfshinte shumë incisivë u korrigjua.
D.M.Sc. Rozela Xhemnica1; M.D-O.M.F.S. Milton Rroço2; Prof. Dr. Lindita Xhemnica1; Prof. Assoc. Çeliana Toti1; Rudin Kusi3.
Menaxhimi i kafshimit të kryqëzuar anterior me aparate të lëvizshme. Prezantim rasti
1Fakulteti i Mjekësise Dentare, 2Spitali Rajonal Durrës, 3Universiteti Zoja e Këshillit të Mirë
FJALËT KYÇE:
raportimi i
rastit, kafshim
i kryqëzuar,
aparat i
lëvizshëm
Hyrje. Kafshim i kryqëzuar anterior është një term i përdorur
për të përshkruar anomalinë okluzale e cila përfshin pozicionimin palatinal të dhëmbëve anterior maksilar krahasuar me dhëmbët anterior mandibular. Kafshimi i kryqëzuar anterior mund të jetë me origjinë dentare ose skeletare. Ai me origjinë dentare vjen si pasojë e inklinimit aksial jo normal të dhëmbëve anteriore maksilare, ndërsa kafshimi i kryqëzuar me origjinë skeletale shpesh shoqërohet me probleme skeletare si; prognati mandibulare dhe me defi çit të zhvillimit të pjesës së poshtme të fytyrës. Diagnoza diferenciale midis kafshimit të kryqëzuar anterior dentar dhe atij skeletar është esenciale në vendosjen e trajtimit klinik.(7) Kjo arrihet duke u perpjekur për të vendosur mandibulen në pozicionin qëndor dhe duke përcaktuar raportin midis molarëve dhe incisivëve të dy nofullave. Nëse molarët janë në raport sipas Klasës së I dhe incisivët në kafshim majë më majë mund të ndërmeret një korrigjim dentar.
Kafshimi i kryqëzuar anterior ka një incidence të raportuar prej 4-5% dhe zakonisht është si rezultat i nje keqpozicionimi i incisivëve maksilar që rezulton me një rrugë linguale eruptimi. (8) Faktorë të tjerë etiologjik përfshijnë: trauma të incisivëve primarë maksilar, gjë e cila çon në zhvendosjen e folikulit të dhëmbit permanent; prania e një dhëmbi të tepërt në regjionin e incisivëve; zakoni i kafshimit të buzës së sipërme; një dhëmb ose rrënje qumështi që akoma nuk eshte ndërruar, mund të jetë nekrotike ose pa pulpe; dalja e vonuar e dhëmbëve të qumështit dhe odontomat.
Qëllimi kryesor për të trajtuar kafshim e kryqëzuar anterior është për të nxjerr dhëmbin/dhëmbët maksilar të prekur, labialisht në një kafshim normalisht të qëndrueshëm që të parandalojë rikthimin në pozicionin fi llestar. Trajtimi mund të përfshijë lëvizjen në drejtim lingual të dhëmbëve mandibularë, lëvizjen në drejtim labial të dhëmbëve maksilar ose të dyja së bashku të kombinuara. (1) Teknika të ndryshme janë përdorur për të arritur këtë qëllim si p.sh.: shtyrja me gjuhë, plane të inklinuara prej kompoziti, aparate rezine të lëvizshme me susta linguale ose aparate fi kse. Në mënyrë që të
shpenzojmë sa me pak dhe të mos shkaktojmë dëmë që lidhen me indet e buta, për pacientët e vegjël, aparatet e lëvizshme janë të thjeshtë për tu vendosur dhe hequr, të rehatshëm dhe të tolerueshëm. Ky artikull dokumenton rastin e një pacienteje, kafshimi i kryqëzuar anterior i të cilës u korrigjua në mënyrë te suksesshme duke përdorur dy aparatë rezine të lëvishme të njëpasnjëshme.
Prezantimi i rastit dhe ndërhyrja klinike:Një vajzë 8-vjeçare u papraqit ne klinikën tonë
dentare. Ajo ankohej për një pamje jo estetike të incisivit central maksilar, i cili ishte pozicionuar prapa dhëmbëve anterior të poshtëm. Historia e saj mjekësore dhe dentare nuk ishte kontribuse dhe pacientia gjithashtu nuk kishte nje histori familjare të Klasës së III te malokluzionit. Incisivët e përhershëm maksilar si majtas dhe djathtas ishin të dyja në kafshim të kryqëzuar (fi gura 1) dhe
Figura 1: Foto intraorale para trajtimit
incizivët lateral maksilar nuk kishin eruptuar plotësisht akoma. Pacientja ishte në fi llimet e një denticioni të përzier dhe kishte molarët në raport të Klasës së I në të dy anët me një overjet 2 mm dhe një overbite 100%. Vija mediane dentare maksilare dhe ajo faciale përputheshin me njëra tjetrën, ndërsa vija mediane mandibulare derivonte përafërsisht 2 mm në të majtë. Hapësira të vogla ndërmjet dhëmbëve ishin të pranishme në harkun maksilar dhe gjithashtu kishte edhe distancë mesio-distale për të arritur lëvizjen me drejtim labial të incizivit central maksilar. Paranomeksi nuk jepte asnjë evidencë

Revista Stomatologjike Shqiptare108
për patologji dentare (fi gura2a) dhe pamja me radiografi cefalometrike laterale nuk paraqiste asnjë evidencë për një problem thelbësor midis harqeve mandibulare dhe maksilare (fi gura 2b).
Objektivat e trajtimit të pacientit ishin për të korrigjuar kafshimin e kryqëzuar anterior, për të vendosur një overbite dhe overjet normal, për të rreshtuar dhëmbët anterior në inklinim ideal dhe për të përmirësuar estetiken faciale dhe dentare të pacientit. Fëmija u këshillua dhe motivua për të mbajtur një higjenë orale të mirë. Për të rrjeshtuar dhëmbët maksilar dhe për të korrigjuar kafshimin, u përdor aparat rezine i lëvizshëm me sipërfaqe përtypëse posteriore për të hapur kafshimin. (fi gura 3a dhe b). Vida e cila inkorporohet në bazën e aparatit aktivizohet 0.25 mm çdo 4 ditë për 16 jave. Pas dy muajsh, incizivët maksilar dhe mandibularë paraqiteshin në një raport majë më majë gjithashtu dhe kafshimi i kryqëzuar u korrigjua me dy muaj të tjerë shtesë (fi gura 4). Sipërfaqet posteriore të ngritjes së kafshimit u hoqën dhe vazhdoi aktivizimi i vidës për çdo 7 ditë për 2 muaj të tjerë me qëllim që të arrihet një overjet normal. Gjatë seancave të trajtimit ( rreth 6 muaj) incizivët lateral maksilar të përhershëm eruptuan, nga të cilët i majti u pozicionua në kafshim të kryqëzuar
Figura 2a: paranomeksi para trajtimit
Figura 2b: Radiografi cephalometrike para trajtimit
Figura 3: a-aparati i levizshem rezine
Figura 5: Foto intraorale pas 6 muajsh
Figura 3: b- Pamje klinike e aparatit
Figura 4: Foto intra orale pas muajit te dytë

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 109
(fi gura5). Detyrimisht një pllakë e re rezine u përgatit me një sustë labio-linguale e cila u aktivizua çdo një muaj për dy muajt në vazhdim deri sa ky kafshim u rregullua. Ne fund të 8 muajve trajtimi aktiv, kafshimi i kryqëzuar i incizivëve maksilar u rregullua në mënyrë të suksesshme dhe asnjë problem klinik dhe radiografi k nuk u vu re për rreth 6 muajt në vazhdimi (fi gura6 a-c).
Figura 6: a. Foto intraorale pas trajtimit
Figura 6b. Paranomeksi pas trajtimit
Figura 6c. Radiografi cefalometrike pas trajtimit
Diskutime:Një nga qëllimet kryesore të dentistrisë pediatrike
është për të mirëmbajtur dhe për të përmirësuar integritetin e harqeve dentare për të lejuar eruptimin
e dhëmbëve permanent dhe për të parandaluar zhvillimin e mëtejshëm të komplikacioneve të maloklusionit. Kafshimi i kryqëzuar anteriror futet tek rastet e rralla e cila është një shqetësim i madh estetik dhe funksional për fëmijët e prindërit që rrallë korrigjohet vetëvetiu.(1) Sidoqoftë, pacientet që paraqiten me Klasën e III të kafshimit nga forma e moderuar deri tek ajo më e rënda e kafshimit të kryqëzuar dhe atij të thellë kanë nevojë për një ndërhyrje të hershme. Mosha ideale për të trajtuar kafshimin e kryqëzuar anterior është mes 8-11 vjeç, periudhë kur rrënja nuk është mbyllur akoma dhe dhëmbët janë në fazë aktive të eruptimit.(3) Kafshimi i kryqëzuar anterior shfaqet zakonisht tek dhëmbët e përparëm pa asnjë mospërputhje skeletale, e cila vjen si pasojë e zhvendosjes funksionale përpara të mandibulës gjatë mbylljes. Kur mandibula orientohet në një raport centrik normal, mund të arrihet një overjet normal ose kafshim majë më majë i incisivëve. Nëse korrigjimi shtyhet për një fazë tjetër të maturimit, mund të çojë në probleme skeletale të malokluzionit dhe kërkon trajtime më komplekse. Teknika të ndryshme janë përdorur për të korrigjuar kafshimin e kryqëzuar anterior duke përfshirë: shtyrjen me gjuhë; plane të inklinuara me kompozit, aparate të lëvizshme rezine me susta linguale dhe aparate fikse.(2) Në varësi të moshës së fëmijës, vendosja e trajtimit duhet të marrë në konsideratë numrin e dhëmbëve që kërkojnë repozicionim, këndin e kafshimit dhe numrin total të dhëmbëve të përfshira dhe motivimin e fëmijës dhe prindërve në lidhje me trajtimin. (5).
Forma më e zakontë e trajtimit të kafshimit të kryqëzuar anterior është shtyrja me gjuhe, në të cilën pacienti udhëzohet si të kafshojë në orët e lira. Forca e ushtruar në drejtimin lingual detyron dhëmbët maksilare të përfshira për të lëvizur përpara, duke patur si bosht orientimi dhëmbët maksilar dhe duke i detyruar që të marrin të njëjtat forca linguale. Sidoqoftë kjo teknikë nuk është e mjaftueshme aq më shumë kur përfshihet më shumë se një dhëmb.(6)
Plani i inklinuar i kafshimit prej kompoziti është një mënyrë tjetër efektive trajtimi që është e thjeshtë dhe jo-invazive, e cila në disa raste zgjidhet si metoda e parë e trajtimit. Sidoqoftë, plani prej kompoziti nuk mund të përdoret në rastet kur kafshimi i kryqëzuar përfshin 1/3 e gjatësisë së kurorës.(4) Për më tepër, cementi i përdorur për këtë tip aparati mund të shkaktoj gingivit.(5) Në rastin konkret, përdorimi i planit të inklinuar prej kompoziti është i papërshtatshëm përderisa ky kafshim përfshinte 1/3 e gjatësisë së kurorës.
Aparati i lëvizshëm ortodontik paraqitet si një zgjidhje tjetër, e thjeshtë dhe estetikisht e pranueshme per trajtimin e kashimit të kryqëzuar (8) e cila ka tre avantazhe madhore : 1- aparati përgatitet në laborator dhe jo direkt në gojën e pacientit, duke reduktuar kohën e qëndrimit të pacientit në poltron. 2- Mund të hiqen në evente të rëndësishme sociale 3- Ato janë lehtësisht të pastrueshëm, duke siguruar një higjenë orale të mirë.

Revista Stomatologjike Shqiptare110
Lëvizshmëria e deshiruar e dhëmbëve kontrollohet nga sustat dhe gjithashtu baza mbetet rigide pavarsisht se ndahet në dy pjesë të aparatit prej rezine, kështu ai mbahet lëhtësisht dhe tendenca për ta hequr reduktohet. Për këto arsye rasti i paraqitur është trajtuar duke përdorur aparate të lëvizshme prej rezine. Aparati i parë përfshinte një vidë aktivizimi i të cilës bënte zgjerimin e aparatit dhe zhvendosjen e dhëmbëve anterior përpara, ndërsa në aparatin e dytë përdorëm susta labio-linguale për të zhvendosur vetëm incizivin lateral maksilar.
1. Park JH, Kim TË. Anterior crossbite correction with a series of clear removable appliances: A case report. Esthet Restor Dent 2009; 21:149-59.
2. Vadiakas G, Viazis AD. Anterior crossbite correction in the early deciduous dentition. Am J Orthod Dentofacial Orthop 1992; 102: 160-2.
3. Kiyak Ha. Patients’ and parents’ expectations from early treatment.Am J Orthod Dentofacial Orthop 2006; 129:S50-4.
4. Sari S, Gokalp H, Aras S. Correction of anterior dental cross-bite ëith composite as an inclined plane. Int J Peadiatr Dent 2001; 11:201-8.
REFERENCAT:
5. Croll TP, Riesenberger RE. Anterior crossbite correction in the primary dentition using fi xed inclined planes. II. Further examples and discussion. Quintessence Int 1996; 45-51.
6. Graber TM. Orthodontics Principles and Practice. 3-rd ed. Philedelphia. W.B. Saunders Company; 1972.p.673-5.
7. Croll TP. Correction of anterior tooth crossbite with bonded resin-composite slopes. Quintessence Int 1996;27:7-10
8. Field HW. Treatment of nonskeletal problems in preado-lescent children. In: Profi t WR, editor. Contemporary Ortho-dontics. 4-th ed. St Louis, Missouri: Elsevier; 2007.p.433-94.
Konkluzione. Pacientja nuk raportoi asnjë shqetësim gjatë seancave
të trajtimit. Trajtimi rezultoi i suksesshëm në korrigjimin e malokluzionit dhe buzëqeshjes estetike. Bazuar në rezultatet e paraqitura, aparati i lëvizshëm me një sustë mund të konsiderohet si zgjedhja e parë e trajtimit të korrigjimit të kafshimit të kryqëzuar anterior dentar për më shumë se një inciziv, ndërsa aparti i lëvizshem me një sustë mund të konsiderohet si zgjedhja e pare e korrigjimit të këtij kafshimi për vetëm një dhëmb inciziv.
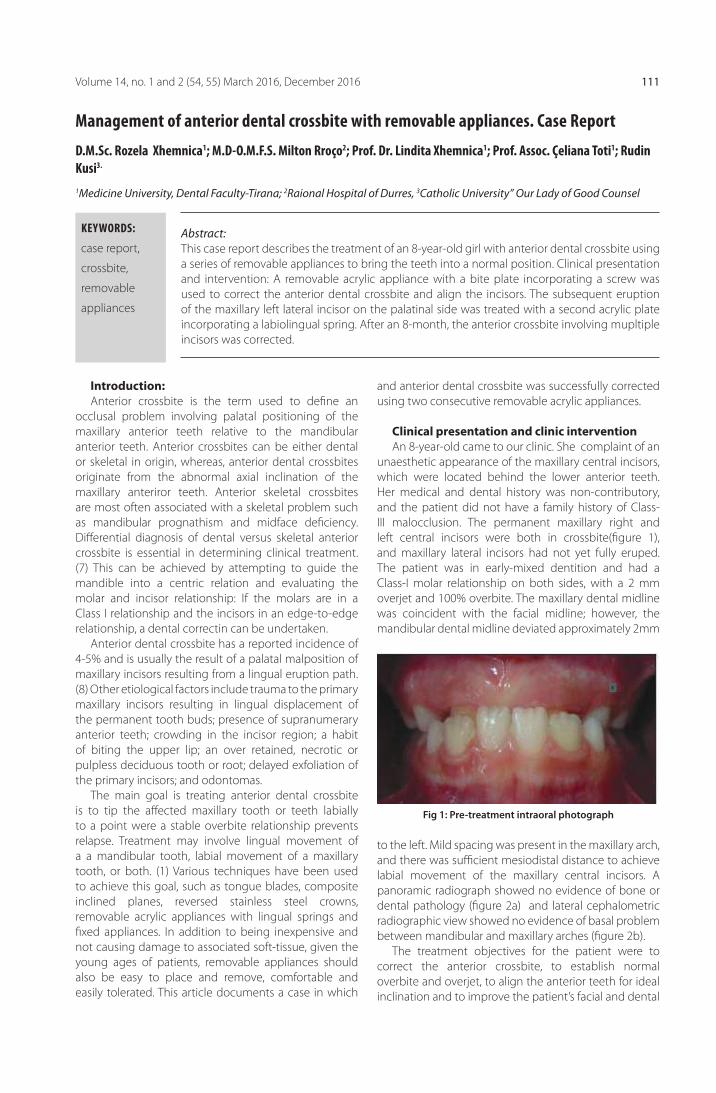
Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 111
Abstract: This case report describes the treatment of an 8-year-old girl with anterior dental crossbite using a series of removable appliances to bring the teeth into a normal position. Clinical presentation and intervention: A removable acrylic appliance with a bite plate incorporating a screw was used to correct the anterior dental crossbite and align the incisors. The subsequent eruption of the maxillary left lateral incisor on the palatinal side was treated with a second acrylic plate incorporating a labiolingual spring. After an 8-month, the anterior crossbite involving mupltiple incisors was corrected.
Management of anterior dental crossbite with removable appliances. Case Report
KEYWORDS:
case report,
crossbite,
removable
appliances
Introduction: Anterior crossbite is the term used to defi ne an
occlusal problem involving palatal positioning of the maxillary anterior teeth relative to the mandibular anterior teeth. Anterior crossbites can be either dental or skeletal in origin, whereas, anterior dental crossbites originate from the abnormal axial inclination of the maxillary anteriror teeth. Anterior skeletal crossbites are most often associated with a skeletal problem such as mandibular prognathism and midface defi ciency. Diff erential diagnosis of dental versus skeletal anterior crossbite is essential in determining clinical treatment.(7) This can be achieved by attempting to guide the mandible into a centric relation and evaluating the molar and incisor relationship: If the molars are in a Class I relationship and the incisors in an edge-to-edge relationship, a dental correctin can be undertaken.
Anterior dental crossbite has a reported incidence of 4-5% and is usually the result of a palatal malposition of maxillary incisors resulting from a lingual eruption path.(8) Other etiological factors include trauma to the primary maxillary incisors resulting in lingual displacement of the permanent tooth buds; presence of supranumerary anterior teeth; crowding in the incisor region; a habit of biting the upper lip; an over retained, necrotic or pulpless deciduous tooth or root; delayed exfoliation of the primary incisors; and odontomas.
The main goal is treating anterior dental crossbite is to tip the aff ected maxillary tooth or teeth labially to a point were a stable overbite relationship prevents relapse. Treatment may involve lingual movement of a a mandibular tooth, labial movement of a maxillary tooth, or both. (1) Various techniques have been used to achieve this goal, such as tongue blades, composite inclined planes, reversed stainless steel crowns, removable acrylic appliances with lingual springs and fi xed appliances. In addition to being inexpensive and not causing damage to associated soft-tissue, given the young ages of patients, removable appliances should also be easy to place and remove, comfortable and easily tolerated. This article documents a case in which
and anterior dental crossbite was successfully corrected using two consecutive removable acrylic appliances.
Clinical presentation and clinic interventionAn 8-year-old came to our clinic. She complaint of an
unaesthetic appearance of the maxillary central incisors, which were located behind the lower anterior teeth. Her medical and dental history was non-contributory, and the patient did not have a family history of Class-III malocclusion. The permanent maxillary right and left central incisors were both in crossbite(fi gure 1), and maxillary lateral incisors had not yet fully eruped. The patient was in early-mixed dentition and had a Class-I molar relationship on both sides, with a 2 mm overjet and 100% overbite. The maxillary dental midline was coincident with the facial midline; however, the mandibular dental midline deviated approximately 2mm
Fig 1: Pre-treatment intraoral photograph
to the left. Mild spacing was present in the maxillary arch, and there was suffi cient mesiodistal distance to achieve labial movement of the maxillary central incisors. A panoramic radiograph showed no evidence of bone or dental pathology (fi gure 2a) and lateral cephalometric radiographic view showed no evidence of basal problem between mandibular and maxillary arches (fi gure 2b).
The treatment objectives for the patient were to correct the anterior crossbite, to establish normal overbite and overjet, to align the anterior teeth for ideal inclination and to improve the patient’s facial and dental
D.M.Sc. Rozela Xhemnica1; M.D-O.M.F.S. Milton Rroço2; Prof. Dr. Lindita Xhemnica1; Prof. Assoc. Çeliana Toti1; Rudin Kusi3.
1Medicine University, Dental Faculty-Tirana; 2Raional Hospital of Durres, 3Catholic University” Our Lady of Good Counsel
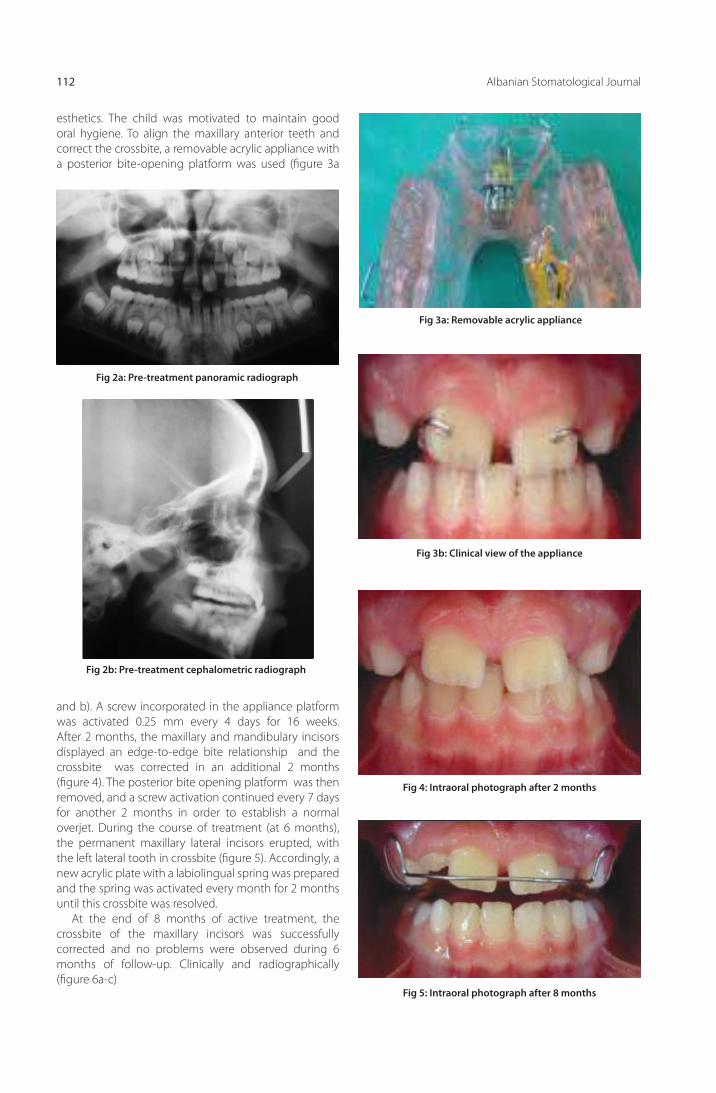
Albanian Stomatological Journal112
Fig 2a: Pre-treatment panoramic radiograph
Fig 2b: Pre-treatment cephalometric radiograph
Fig 3a: Removable acrylic appliance
Fig 5: Intraoral photograph after 8 months
Fig 3b: Clinical view of the appliance
Fig 4: Intraoral photograph after 2 months
esthetics. The child was motivated to maintain good oral hygiene. To align the maxillary anterior teeth and correct the crossbite, a removable acrylic appliance with a posterior bite-opening platform was used (fi gure 3a
and b). A screw incorporated in the appliance platform was activated 0.25 mm every 4 days for 16 weeks. After 2 months, the maxillary and mandibulary incisors displayed an edge-to-edge bite relationship and the crossbite was corrected in an additional 2 months (fi gure 4). The posterior bite opening platform was then removed, and a screw activation continued every 7 days for another 2 months in order to establish a normal overjet. During the course of treatment (at 6 months), the permanent maxillary lateral incisors erupted, with the left lateral tooth in crossbite (fi gure 5). Accordingly, a new acrylic plate with a labiolingual spring was prepared and the spring was activated every month for 2 months until this crossbite was resolved.
At the end of 8 months of active treatment, the crossbite of the maxillary incisors was successfully corrected and no problems were observed during 6 months of follow-up. Clinically and radiographically (fi gure 6a-c)

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 113
Fig 6a: intraoral photograph after the treatment
Fig 6b: Post-tratment panoramic radiograph
Fig 6c. Post treatment cephalometric
DiscussionOne of the main goals of pediatric dentistry is
to maintain or improve arch integrity to allow for the eruption of permanent teeth and prevent the development of a more complicated malocclusion. Anterior dental crossbite is a rare condition that is of major esthetic and functional concern to children and parents and that seldom corrects itself (1). However, developing Class III patients with moderate to severe anterior crossbite and deep bite may need early intervention. The ideal age to treat anterior crossbite
is between 8 years and 11 years, the period when the root is being formed and the tooth is in the active stage of eruption.(3) Anterior dental crossbite is a habitual established crossbite of anterior teeth, without any skeletal discrepancy, resulting from functional forward shift of the mandible on closure. When the mandible is guided into a normal centric relation, a normal overjet or an edge-to-edge position fo incisors can be obtained. If correction is delayed to a later stage of maturity, it may lead to a skeletal malocclusion and require more complex treatment.
Diff erent techniques have been used to correct anterior dental crossbite, including tongue blades, composite inclined planes, reversed stainless steel crowns, removable acrylic appliances with lingual springs and fi xed appliances.(2,In addition to the age of the child, treatment decisions should also take into account the number of teeth requiring repositioning, the degree of overbite, the total number of teeth involved and the motivation of the child and the parents for treatment.(5)
The most basic form of treatment for anterior crossbite is tongue blade, which the patient is instructed to bite on during leisure hours. The biting force is applied to the lingual aspect of the involved maxillary tooth to move the tooth forward, with the incisal edges of the mandibular teeth acting as a fulcrum to absorb the reciprocal lingual forces. However, this technique is rarely suffi cient when more than one tooth is involved.(6)
Crossbite may also be corrected using a reversed, pre-fabricated stainless steel crown. The chief disadvantage with this treatment is the diffi culty adapting a preformed crown to fi t the tooth in crossbite. Furthermore, because of its unaesthetic appearance, this form of treatment is often rejected by children and their relatives.
A composite inclined bite-plane is another effective treatment method that is simple and non-invasive, making it the first choice of treatment in some cases. However, a composite plane cannot be used in cases where the anterior crossbite exceeds 1/3 the crown length.(4) Moreover, the cement used with this type of appliance may cause gingivitis.(5) In the present case, the use of a composite inclined plane was inappropriate, as the anterior crossbite exceeded 1/3 of crown length.
Removable orthodontic appliances represent another safe, easy and esthetically acceptable alternative for the treatment of anterior crossbite (8) that has three major advantages: (1) the appliances are fabricated in the laboratory rather than directly in the patient’s mouth, thereby reducing chair time; (2) They can be removed on socially sensitive occasions (where visible wires on the facial part of the teeth would be undesirable); and (3) They are easily cleaned,

Albanian Stomatological Journal114
1. Park JH, Kim TË. Anterior crossbite correction with a series of clear removable appliances: A case report. Esthet Restor Dent 2009; 21:149-59.
2. Vadiakas G, Viazis AD. Anterior crossbite correction in the early deciduous dentition. Am J Orthod Dentofacial Orthop 1992; 102: 160-2.
3. Kiyak Ha. Patients’ and parents’ expectations from early treatment.Am J Orthod Dentofacial Orthop 2006; 129:S50-4.
4. Sari S, Gokalp H, Aras S. Correction of anterior dental cross-bite ëith composite as an inclined plane. Int J Peadiatr Dent 2001; 11:201-8.
REFERENCAT:
5. Croll TP, Riesenberger RE. Anterior crossbite correction in the primary dentition using fi xed inclined planes. II. Further examples and discussion. Quintessence Int 1996; 45-51.
6. Graber TM. Orthodontics Principles and Practice. 3-rd ed. Philedelphia. W.B. Saunders Company; 1972.p.673-5.
7. Croll TP. Correction of anterior tooth crossbite with bonded resin-composite slopes. Quintessence Int 1996;27:7-10
8. Field HW. Treatment of nonskeletal problems in preado-lescent children. In: Profi t WR, editor. Contemporary Ortho-dontics. 4-th ed. St Louis, Missouri: Elsevier; 2007.p.433-94.
providing good oral hygiene. The amount of desired movement of the teeth can be controlled by the screw and also the base plate remains rigid despite being cut into two parts of acrylic appliances, thereby, it’s management is easy and less tendency to dislodge. For these reasons, the case reported here was treated using removable acrylic appliances. The first appliance was fitted with a screw to achieve labial movement of multiple teeth, whereas the second appliance used a labiolingual spring to tip a single maxillary lateral
incisor. Conclusion. The patient did not report any discomfort during the course of treatment. Treatment resulted in successful correction of the malocclusion and esthetic smile.
Based on the results presented here, a removable appliance with a screw may be considered the fi rst choice of treatment to correct anterior dental crossbite of more than one incisor, whereas a removable appliance with a labiolingual springs may be considered the fi rst choice of treatment for correction of crossbite of one incisor tooth.

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 115
AbstraktiQёllimi i kёtij artikulli ёshtё prezantimi i aplikimit të teknikës kurora e integruar me kultin të suprastruktures në pacientë, e cila duhet marrë në konsideratë si një alternativë e mirë për ngarkimin e implanteve teke me mbyllje konike. Kjo teknikë është një teknikë alternative për zëvendësimin e një dhëmbi tek, me një kurorë mbi implant, ku kulti dhe kurora janë një trup i vetëm. Mekanizmi me mbyllje konike ose sic quhet ndryshe me ftohje është ai që siguron lidhjen e implantit me kompleksin kult-kurorë.
Msc. Ledia Gaxho(1), Prof. Dr Ramazan Isufi (1)
Shfrytëzimi i kurorës së integrar me kultin, si teknikë për suprastrukturën e implanteve të shkurtra Bicon. Prezantim Rasti
Fakulteti i Mjekësisë Dentare, Universiteti i Mjekësisë, Tiranë
FJALËT KYÇE:
Kurora e
integruar me
kultin (KIK),
implantet
e shkurtra
,mbyllja konike,
Bicon
HyrjeTeknikat e zakonshme, pёr tё arritur integritetin
struktural tё komplekseve kurorё-kult dhe implant-kult nё restaurimet implantare teke, pёrfshijnё vida dhe cementim(1-16).
Studimet me follow up afatgjatё kanё raportuar disa komplikacione ku pёrfshihen humbja e vidёs, fraktura e saj dhe dёshtime tё komponentёve tё tjerё.(1-7)Nё rastet e restaurimeve teke qё zёvendёsojnё molarёt mandibular, humbja e vidёs duket tё jetё njё problem i madh (1,6,8,9). Nga ana tjetёr, njё nga komplikacionet si mukoziti peri-implantar dhe peri-implantiti raportohen tё ndodhin nё literaturё si pasojё e mbetjeve tё cementit pas vendosjes sё kurorёs. Mbetjet e cementit nё sulkusin gingivar, qё mund tё duken dhe nё radiografi , mund tё cojnё nё humbjen e kockёs pёrreth implantit (13,14,34). Kjo teknikё alternative i ofron klinicistёve disa avantazhe.
Nё kёtё sistem implantar pa vidё qё ne kemi pёrdorur, implanti dhe kulti lidhen nga njё mbyllje konike prej 3̊. Forcat e mёdha tё fёrkimit qё krijohen nga mbyllja konike prishin shtresёn e oksidit tё titaniumit dhe metalet ndёrfuten me njёri-tjetrin me ftohje (17).Pjesa koronare qё mbёshtjell kultin prej aliazhi titanium ёshtё kompozit-rezinoz me pjesёza mikrombushёse (highly fi lled composit) dhe light-cured (Shofu). Korona e Integruar me Kultin ёshtё njё restaurim implantar ku implanti, kulti dhe materiali i kurorёs janё njё trup (21).
Prezantimi i rastitKy raportim klinik pёrshkruan rastin e njё pacienteje
femёr 41-vjec me mungesё tё tre dhёmbёve (36, 44, 45), tё zёvendёsuar me implante tё shkurtra teke me mbyllje konike. Secili prej tyre u ngarkua me KIK. Pacientja ishte duhanpirёse (4 cigare/ditё), e kategorizuar si ASA II (bazuar nё sistemin e klasifi kimit tё statusit fi zik nga Shoqata Amerikane e Anestezistëve). Nё planin tonё tё trajtimit, implantet u aplikuan me teknikёn kirurgjikale me dy faza. Ky rast raporton vendosjen e tre implanteve
Fig.1 Largësia mes kulmin e implantit dhe nervore inferiore alveolare
tё shkurtra Bicon, njё prej tё cilёve (44) shumё afёr nervit alveolar inferior dhe foraminёs mentale.
Raportim rastiNjё paciente femёr 41–vjece referoi pёr halitozё me
shkak praninё e urave metal-porcelan nё tё dyja anёt e nofullёs sё poshtme (35 X 37 38 dhe 43 X X 46 47) dhe gjakosje spontane tё gingivave. Pёrpara vendosjes sё implantit, u hoqёn urat dhe u lanё indet e buta tё shёroheshin. Gjatё planit tё trajtimit vendosёm tё aplikonim njё implant 5.0 x 6.0 mm Integra CP-3.0 mm well tek 36, implant 4.5 x 6.0 mm Integra-CP-3.0 mm well tek 44, implant 5.0 x 5.0 mm Integra-CP-3.0 mm well tek 45. Pas 2 javёsh u hap lembo dhe tre implantet e shkurtra Bicon u vendosёn me procedurёn kirurgjikale me dy faza. Njё distancё prej 3.08 mm e ndante apeksin e implantit tё 45-ёs nga kanali mandibular. (Figura 1, 2)
Shpimi u bё nёn irrigimin e jashtёm me shpejtёsi 1000 rrot/min dhe 2-3 mm mё thellё se gjatёsia e zgjedhur e implantit. Njё kult me 2 mm post u vendos nё shpimin

Revista Stomatologjike Shqiptare116
Fig.5 Aplikimi i implantit në sitin e tij
Fig.2 Lejohet distancën mes kulmin e implantit dhe nervore alveolare inferiore.
pilot dhe u konfi rmua pёrshtatja me njё shabllon vacum-press. Xhepat (siti) u zgjeruan nëpërmjet frezave të osseotomisë pa irrigim dhe me shpёjtёsi maksimale prej 50 rrot/min. Kocka e grumbulluar gjatё zgjerimit u pёrdor mё vonё si graft autolog. Pas vendosjes sё implantit, siti kirurgjikal u suturua dhe pacienti u kёshillua pёr kujdesin post-operator. Pas 2 javёsh suturat u hoqёn dhe shёrimi i indeve tё buta nuk pati problem. Pas 3,5 muajsh ndjekjeje, gjёndja e indeve tё buta u vlerёsua.
Anestezia lokale u administrua pёrreth zonёs sё implanteve dhe ato u ekspozuan. Njё kunj udhëzues 3.0 mm u vendos nё pusin e cdo implanti pёr të kontrolluar osseointegrimin dhe angulimin e tij. Implantet ishin plotësisht të osseointegruar dhe kocka e tepёrt u hoq me anë të zgjeruesve të sulkusit (sulcus reamer) qё i korrespondon tapave shёruese tё zgjedhura (4.0 x 5.0 mm 0˚ - 3.0 mm pёr 44 dhe 45; 6.5 x 5.0 mm 0˚ - 3.0 mm pёr 36).
2 javё mё pas tapat shёruese u hoqёn, u mor masa nёpёrmjet kunjave 3.0 mm prej titanium dhe si material mase u pёrdor polieter medium (3M Espe). Pas forcimit tё materialit tё masёs dhe heqjes së lugës së masës, kunjat ngelen tё inseruara nё implant. Kunjat e masёs u inseruan nё njё analog dhe u dёrguan nё laborator sё bashku me ngjyrёn (Vita shades) dhe kafshimin.
Pasi tekniku i laboratorit zgjodhi kultin e duhur, pёrgatiti restaurimet e KIK. Nё seancёn e aplikimit tё KIK, implantet u pastruan dhe u thanё me njё tampon pambuku dhe KIK u vendosёn sipas aksit gjatёsor tё kunjave udhëzuese pёr tё realizuar mekanizmin e mbylljes konike. Lidhja implant-kult siguron njё pozicionim universal prej 360̊. Njё udhёzues rezine lehteson orientimin dhe vendosjen e KIK, duke siguruar pikat e kontaktit me dhёmbёt qё e kufi zojnё dhe ata antagonist. Kontaktet interproksimale dhe okluzioni u kontrolluan me njё letёr artikulacioni 40 μ (Coltène /WhaledentGmbH+Co. KG). Pasi ishin vendosur, u pa e nevojshme tё rregullohej okluzioni dhe dy KIK u hoqёn pёr tu modifi kuar nё laborator. Njё skemё e gabuar okluzale rrit magnitudёn e ngarkesave dhe intensifi kon stresin mekanik. Ky faktor rrit shpeshtёsinё e komplikacioneve tё restaurimeve implantare dhe/ose tё mbёshtetjes kockore (18). Radiografi tё periapikale dhe foto u regjistruan.
Fig.3 Panorameks para aplikimittëimplanteve
Fig.4 Përcaktimi i madhësisë së implantit
Aplikimi i molarit të parë mandibular majtas (36) Faza e pare kirurgjikale:
Gjatё ndjekjes nё vazhdimёsi:Kurora e Integruar me Kultin i siguroi pacientit: 1. Estetikёn, funksionin dhe rehatinё. 2. Njё adaptim shumё i mirё (shkёlqyer) marginal
nёpёrmjet teknikёs pa cementim. 3.Qёndrueshmёri tё ngjyrёs.
U mbajt nёn observim grumbullimi i pllakёs bakteriale pёrreth materialit tё koronёs dhe u pa akumulim supragingival i saj rreth KIK. Kjo ishte dicka qё pritej pasi ёshtё treguar vazhdimisht qё materialet me bazё rezinoze akumulojnё pllakё nё njё masё mё tё madhe se struktura e dhёmbit natyral apo restaurimet qeramike (19,20,22).

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 117
Fig.9 Kunja guiduese që tregon drejtimin e implantit të integruar
Fig.10 Kulti shërues i bardhë i vendosur në pusin e implantit
Fig.11 Doreza vidhosëse për kontrollin e osseointegrimit
Fig.12 KIK në model
Fig.6 Prerja e tapes së shërimit
Fig.7 Radiografi pas aplikimit te implantit
Fig.8 Heqja e tapësshëruese
Faza e dytëkirurgjikale:
Fig.13 Foto e Kurorës sё Integruar me Kultin (KIK)

Revista Stomatologjike Shqiptare118
Fig.15 Radiografi pas vendosjessëkurorës
Fig.16 Panorameks para aplikimit të implanteve
Fig.17 Foto para aplikimit të implanteve
Fig.18 Lembomuko periostale
Fig.19 Implantet pas prerjes së tapave shëruese
Fig.20 Radiografi pas aplikimit
Fig.21 Zbulimiiimplanteve
Aplikimi i dy premolarëve mandibular djathtas (44, 45)Faza e pare kirurgjikale:
Faza e dytë kirurgjikale:
Fig.14 Goditja për realizimin e mbyllje skonike

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 119
Fig.23 Kunjatguidueseqëtregojnëdrejtimin e implantevetëintegruara. Fig.27 KIK në model
Fig.24 Kultetshëruesetëbardhatëvendosuranëpusin e implanteve Fig.28 Goditjapërrealizimin e mbylljeskonike.
Fig.25 Indet e buta pas heqjessëtapavetëshërimit Fig.29 Pamjevestibulare pas vendosjessë KIK
Fig.22 Heqja e tapaveshërueseFig. 26 Foto e KuroravetëIntegruara me Kultin (KIK)

Revista Stomatologjike Shqiptare120
Fig.31 Fotoklinike e KIK 44, 45
Fig.34 Radiografi periapikale pas 2 vjetësh e 36
Fig.32 Fotoklinike e KIK
Fig. 30 Radiografi periapikale e implanteve dhe ngarkesave të tyre (44, 45)
Fig.33 Radiografi periapikale pas 2 vjetësh e 44 dhe 45
Kontrolli pas 2 vjetësh i implanteve klinikisht dhe me grafi :
DiskutimiMaterialet mё tё zakonshme pёr restaurimin e
dhёmbёve por edhe tё implanteve janё kurorat metal-porcelan dhe ato qeramike. Restaurimi qё u pёrdor nё kёtё rast ndryshon nga kurorat metal-porcelan nё atё qё metali i kultit dhe materiali i kurorёs (kompozit rezinoz) bashkohen nga nje lidhje kimike dhe mekanike nё kushte laboratorike, pёr kёtё arsye ska nevojё pёr cementim. Dy teknikat mё tё zakonshme pёr tё fi ksuar kultin nё restaurimet implantare teke janё pёrdorimi i vidёs dhe ndërlidhjet konike (Konike Morse dhe mbylljet konike) (24).
Nё rastin tonё kultet u lidhёn me implantet nёpёrmjet mbylljes konike pa vidё. KIK-u ёshtё njё teknikё pёr korona teke tё mbёshtetura mbi implante, ku kulti dhe kurora janё njё trup. Kjo teknikё ёshtё prezantuar pёr herё tё parё nё 2007 nga Urdaneta dhe Marincola (23).
Avantazhet qё ofron kjo teknikё jane: njё adaptim marginal shumё i mirё (perfekt), nje lidhje hermetike implant-kult ndaj fl orёs bakteriale, nje material kurore me fortёsi dhe shkallё abrasive tё njёjtё me smaltin e dhёmbit natyral, njё teknikё laboratorike e thjeshtё dhe njё numёr i reduktuar i komponentёve protetik. Nё saje tё natyrёs light-cured tё kёtij materiali, mund tё bёhen modifi kime edhe nё poltronin dentar (23). Nga ana tjetёr, disavantazhet e kёsaj teknike vijnё nga materiali rezinoz i pёrdorur pёr kurorёn qё akumulon pllakё bakteriale nё njё shkallё mё tё lartё dhe priren tё ndryshojnё ngjyrё mё shpejt se dhёmbi natyral apo restaurimet terёsisht qeramike (23). Nga ana tjetёr kompozitet rezinoze kanё treguar qё shkaktojnё mё pak abrazion tё smaltit tё antagonistёve nё krahasim me porcelanin (25-27). Njё nga disavantazhet mё tё mёdhaja tё restaurimeve metal-porcelan dhe tёrёsisht qeramike ёshtё abarazioni qё shkaktojnё nё denticionin natyral. Ky fakt mbeshtetet nga studimet e vazhdueshme in vivo dhe in vitro (28-33). Megjithatё, studime tё tjera nevojiten pёr vlerёsuar performancёn afatgjatё tё Kurorave tё Integruara me Kultin (KIK).
KonkluzionKurora e Integruar me Kultin, teknika pa vidё dhe pa
cementim, i siguruan pacientit estetikёn, funksionin dhe rehatinё gjatё periudhёs sё post-ngarkesёs. Implanti i vendosur afёr me nervin alveolar inferior nuk pati komplikacione.
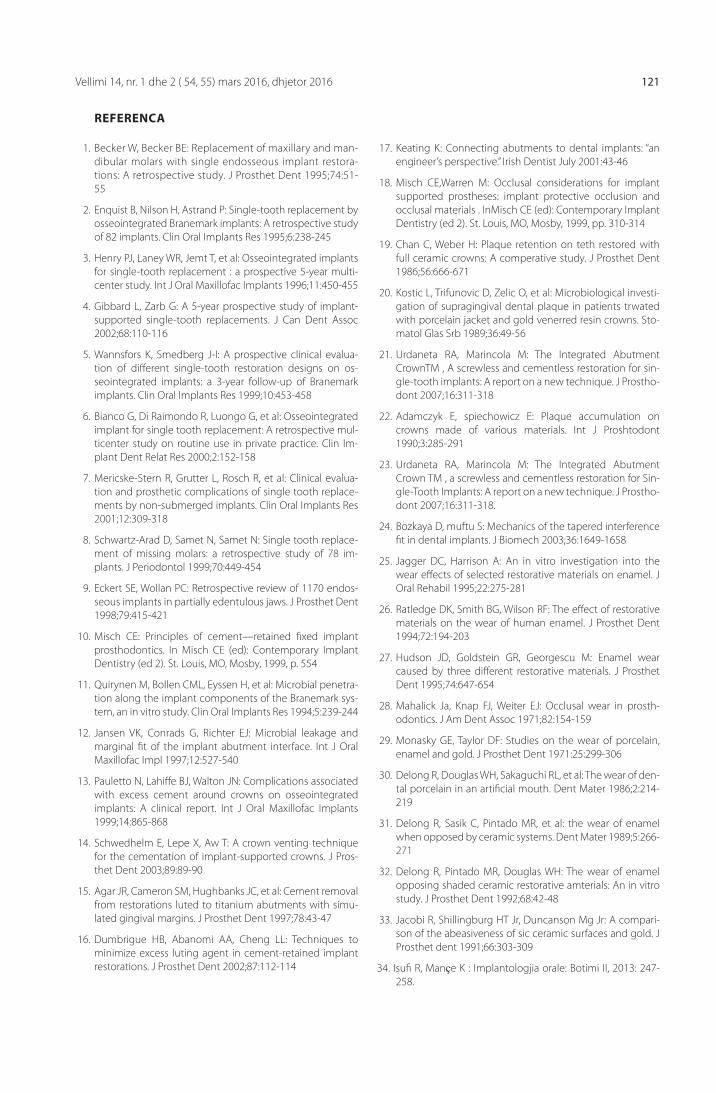
Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 121
1. Becker W, Becker BE: Replacement of maxillary and man-dibular molars with single endosseous implant restora-tions: A retrospective study. J Prosthet Dent 1995;74:51-55
2. Enquist B, Nilson H, Astrand P: Single-tooth replacement by osseointegrated Branemark implants: A retrospective study of 82 implants. Clin Oral Implants Res 1995;6:238-245
3. Henry PJ, Laney WR, Jemt T, et al: Osseointegrated implants for single-tooth replacement : a prospective 5-year multi-center study. Int J Oral Maxillofac Implants 1996;11:450-455
4. Gibbard L, Zarb G: A 5-year prospective study of implant-supported single-tooth replacements. J Can Dent Assoc 2002;68:110-116
5. Wannsfors K, Smedberg J-I: A prospective clinical evalua-tion of diff erent single-tooth restoration designs on os-seointegrated implants: a 3-year follow-up of Branemark implants. Clin Oral Implants Res 1999;10:453-458
6. Bianco G, Di Raimondo R, Luongo G, et al: Osseointegrated implant for single tooth replacement: A retrospective mul-ticenter study on routine use in private practice. Clin Im-plant Dent Relat Res 2000;2:152-158
7. Mericske-Stern R, Grutter L, Rosch R, et al: Clinical evalua-tion and prosthetic complications of single tooth replace-ments by non-submerged implants. Clin Oral Implants Res 2001;12:309-318
8. Schwartz-Arad D, Samet N, Samet N: Single tooth replace-ment of missing molars: a retrospective study of 78 im-plants. J Periodontol 1999;70:449-454
9. Eckert SE, Wollan PC: Retrospective review of 1170 endos-seous implants in partially edentulous jaws. J Prosthet Dent 1998;79:415-421
10. Misch CE: Principles of cement—retained fi xed implant prosthodontics. In Misch CE (ed): Contemporary Implant Dentistry (ed 2). St. Louis, MO, Mosby, 1999, p. 554
11. Quirynen M, Bollen CML, Eyssen H, et al: Microbial penetra-tion along the implant components of the Branemark sys-tem, an in vitro study. Clin Oral Implants Res 1994;5:239-244
12. Jansen VK, Conrads G, Richter EJ: Microbial leakage and marginal fi t of the implant abutment interface. Int J Oral Maxillofac Impl 1997;12:527-540
13. Pauletto N, Lahiff e BJ, Walton JN: Complications associated with excess cement around crowns on osseointegrated implants: A clinical report. Int J Oral Maxillofac Implants 1999;14:865-868
14. Schwedhelm E, Lepe X, Aw T: A crown venting technique for the cementation of implant-supported crowns. J Pros-thet Dent 2003;89:89-90
15. Agar JR, Cameron SM, Hughbanks JC, et al: Cement removal from restorations luted to titanium abutments with simu-lated gingival margins. J Prosthet Dent 1997;78:43-47
16. Dumbrigue HB, Abanomi AA, Cheng LL: Techniques to minimize excess luting agent in cement-retained implant restorations. J Prosthet Dent 2002;87:112-114
17. Keating K: Connecting abutments to dental implants: “an engineer’s perspective.” Irish Dentist July 2001:43-46
18. Misch CE,Warren M: Occlusal considerations for implant supported prostheses: implant protective occlusion and occlusal materials . InMisch CE (ed): Contemporary Implant Dentistry (ed 2). St. Louis, MO, Mosby, 1999, pp. 310-314
19. Chan C, Weber H: Plaque retention on teth restored with full ceramic crowns: A comperative study. J Prosthet Dent 1986;56:666-671
20. Kostic L, Trifunovic D, Zelic O, et al: Microbiological investi-gation of supragingival dental plaque in patients trwated with porcelain jacket and gold venerred resin crowns. Sto-matol Glas Srb 1989;36:49-56
21. Urdaneta RA, Marincola M: The Integrated Abutment CrownTM , A screwless and cementless restoration for sin-gle-tooth implants: A report on a new technique. J Prostho-dont 2007;16:311-318
22. Adamczyk E, spiechowicz E: Plaque accumulation on crowns made of various materials. Int J Proshtodont 1990;3:285-291
23. Urdaneta RA, Marincola M: The Integrated Abutment Crown TM , a screwless and cementless restoration for Sin-gle-Tooth Implants: A report on a new technique. J Prostho-dont 2007;16:311-318.
24. Bozkaya D, muftu S: Mechanics of the tapered interference fi t in dental implants. J Biomech 2003;36:1649-1658
25. Jagger DC, Harrison A: An in vitro investigation into the wear eff ects of selected restorative materials on enamel. J Oral Rehabil 1995;22:275-281
26. Ratledge DK, Smith BG, Wilson RF: The eff ect of restorative materials on the wear of human enamel. J Prosthet Dent 1994;72:194-203
27. Hudson JD, Goldstein GR, Georgescu M: Enamel wear caused by three diff erent restorative materials. J Prosthet Dent 1995;74:647-654
28. Mahalick Ja, Knap FJ, Weiter EJ: Occlusal wear in prosth-odontics. J Am Dent Assoc 1971;82:154-159
29. Monasky GE, Taylor DF: Studies on the wear of porcelain, enamel and gold. J Prosthet Dent 1971:25:299-306
30. Delong R, Douglas WH, Sakaguchi RL, et al: The wear of den-tal porcelain in an artifi cial mouth. Dent Mater 1986;2:214-219
31. Delong R, Sasik C, Pintado MR, et al: the wear of enamel when opposed by ceramic systems. Dent Mater 1989;5:266-271
32. Delong R, Pintado MR, Douglas WH: The wear of enamel opposing shaded ceramic restorative amterials: An in vitro study. J Prosthet Dent 1992;68:42-48
33. Jacobi R, Shillingburg HT Jr, Duncanson Mg Jr: A compari-son of the abeasiveness of sic ceramic surfaces and gold. J Prosthet dent 1991;66:303-309
34. Isufi R, Manҫe K : Implantologjia orale: Botimi II, 2013: 247-258.
REFERENCA

Albanian Stomatological Journal122
AbstractThe purpouse of this study is to present the aplication of Integrated Abutment Crown technique in patients, as an alternative technique to restore single locking-taper implants. This is an alternative technique to replace one missing tooth, in which the abutment and the crown are a single body. The connection beetwen the implant and abutment-crown complex is realised by locking-taper mechanism or in the other words, cold-welding mechanism.
Msc. Ledia Gaxho(1), Prof. Dr Ramazan Isufi (1)
Use of Integrated Abutment Crown,a techinque for the load of Bicon short implants. Case Report
Faculty of Dental Medicine, University of Medicine, Tirana
KEYWORDS:
Integrated
Abutmetn
Crown (IAC),
short implants,
locking-taper,
Bicon
IntroductionCommon techniques to achieve structural integrity of
the crown-abutment and implant-abutment complexes in single-tooth implant restorations include screws and cement (1-16). Long term follow up studies have reported several complications including screw loosening, fracture and other component failures (1-7). In cases of single tooth restorations replacing mandibular molars, screw loosening appears tobe a greater problem (1,6,8,9). On the other hand, one of the complications as peri-implant mucositis and peri-implantitis are reported in the literature to happen as an incomplete cement removal, after placing a crown. Incomplete cement removal from the gingival sulcus can lead to loss of peri-implant bone that may be visualized radiographically(13,14).This alternative technique off ers to the clinicians some advantages.
In this screwless implant system that we were using, the implant and the abutment is connected by means of 3.0˚ locking taper. The high friction force created by the locking taper breaks down the titanium oxide layer and the metals are fused together in a cold weld (17). The coronal part bonded over the titanium alloy abutment is a light cured, highly fi lled composite resin material ( Shofu). The integrated abutment crown is an implant restoration where the implant, abutment and the crown material are one unit(21).
Clinical presentationThis clinical report describes a case of 41-years old
female with three missing teeth ( 36, 44, 45 ) restored with/by single-tooth locking-taper short
implants. Each one of them was loaded with an Integrated Abutment Crown. The patient was a smoker (4 cigarettes/day), cathegorised as ASA II ( based on American Society of Anesthesiologyst physical status classifi cation system) In our plan of treatment the implants were placed with a two stage technique. This case reports the placement of three short Bicon implants, one of them (44) closely to the inferior alveolar nerve and mental foramina.
Fig. 1 Distance between the apex of implant and inferior alveolar nerve.
Case reportA 41 year-old female patient was referred complaining
halitosis coming from porcelain fused to metal bridges on both sides of the mandible (35 X 37 38 and 43 X X 46 47), with spontaneous bleeding. Before implant placement, the bridges were taken off and the gum was allowed to heal. During the plan of treatment we decided to place a 5.0 x 6.0 mm Integra-CP-3.0 mm well at 36, 4.5 x 6.0 mm Integra-CP-3.0 mm well at 44, 5.0 x 5.0 mm Integra-CP-3.0 mm well at 45. After 2 weeks the fl ap was elevated and three Bicon Implants were placed in two-stage procedure. A 3.08 mm separated the apex of the lower right premolar implant (45) osteotomy and the mandibular canal. (Figure 1, 2)
The drilling with external irrigation was performed 2.0 mm-3.0mm deeper than chosen implants at a maximum 1000 rpm. An abutment with 2.0 mm post was placed into pilot hole and confi rm appropriateness with a vacu-press template. The sockets were widen with wider reamer burs without irrigation, at a maximum of 50 rpm. The harvested bone was used later as an autolog graft.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 123
Fig.5 Implant insertion into the osteotomy
Fig. 2 Allowed distance between the apex of implant and alveolar inferior nerve.
After placing the implants the surgical site was sutured, and this patient was given surgical instruction. After two weeks sutures were removed and the soft tissue healing was uneventful. At the 3.5-month follow up, soft tissue condition was evaluated.
Local anesthetic was administered around the implant area and the implants were exposed. A 3 mm guide pin was seated into the well of each implant to check the osseointegration and angulation. They were fully osseointegrated and excess bone was removed with sulcus reamer corresponding to the chosen healing abutments (4.0 x 5.0 mm 0˚ - 3.0 mm for 44 and 45; 6.5 x 5.0 mm 0˚ - 3.0 mm for 36).
Two weeks after, healing abutments were removed, impression was made with 3 mm titanium impression posts and polyether medium bodied (3M Espe) material. After removing the impression, the impression posts remain attached to the implant. The impression posts were inserted to an analog and send to the laboratory together with the appropriate shade and the bite. (Vita shades) .
The laboratory technician after choosing the proper abutment, provided the IAC restorations. At the insertion appointment the implants were fl ush and dry well with a cotton tip and the IAC were seated and tapped on in long axis of abutment post to engage locking taper. Implant to abutment connection provides for 360° of universal abutment positioning. A resin seating jig facilitates the orientation and seating of the IAC, providing contact points with adjacent teeth and opposing structures. The interproximal contacts and the occlusion were checked with a 40μ articulating paper (Coltène /Whaledent GmbH+Co. KG). It was necessary to adjust the occlusion, removing the two IAC for laboratory modifi cations after they were been seated. A poor occlusal scheme both increases the magnitude of loads and intensifi es mechanical stress. This factors increase the frequency of complications of implant restorations and/or bone support(18). Periapical radiographs and photos were recorded.
During follow up:The Integrated Abutment Crowns provided the
patients:
Fig. 3 Pre-operative panoramic radiograph
Fig.4 Implant size selection
Application of mandibular left fi rst molar (36) First surgical stage:
1. The esthetic, function and comfort during the post-loading follow up period.
2. Excellent marginal adaption with the cementless interface.
3. Color stability (colors remained stable during the period of observation).
Plaque accumulation was observed around the crown material. The supragingival plaque accumulation was observed around IAC . This was expected because it has been consistenly shown that resin-based materials accumulate plaque at a higher rate than tooth structure and all-ceramic restorations(19,20,22).

Albanian Stomatological Journal124
Fig. 9 Guide pin showing the trajectory of the integrated implant
Fig. 10 White healing abutment seated in the well of the implant
Fig. 11 Threaded knob to control the osseointegratio
Fig. 12 IAC on stone model
Fig. 6 The cut of healing plug
Fig. 7 Post-implant insertion radiograph
Fig. 8 Healing plug being removed
Second surgical stage:
Fig. 13 Photo of Integrated Abutment Crown (IAC)

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 125
Fig. 15 Post- crown insertion radiograph
Fig. 16 Panoramic radiograph before implant placement
Fig. 17 Picture before implant placement
Fig. 18 Mucoperiostal lembo
Fig. 19 Implants after the cut of healing plugs
Fig. 20 Post-implant insertion radiograph
Fig. 21 Uncovering procedure
Application of two mandibular right premolars (44, 45)First surgical stage:
Second surgical stage:
Fig. 14 Straight handle used to engage the locking taper

Albanian Stomatological Journal126
Fig. 23 Guide pins showing the trajectory of the integrated implant Fig. 27 IACs on stone model
Fig. 24 White healing abutments seated in the well of the implants Fig. 28 Straight handle used to engage the locking taper
Fig. 25 Smooth tissue after removing healing cups Fig. 29 Facial view after insretion o the IACs
Fig.22 Healing plugs being removedFig. 26 Photo of Integrated Abutment Crowns (IACs)

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 127
DiscussionThe most common material used for the restoration
of both, teeth and implants, are ceramo-metal or all-ceramic crowns.
The implant restoration used in this case diff ers from cemented metal-ceramic crowns in that the metal abutments and the crown material were chemo-mechanically bonded in the laboratory, therefor there was no need for cement. Two common techniques to secure the abutment to the implant in single-tooth implant restorations are the use of a screw and the use of a tapered interference fi t (Morse tapers and locking tapers)(24).
The abutments were connected to the implants with a screwless locking-taper. The Integrated Abutment Crown (IAC) is a technique used for single-tooth implant-supported crown, where the abutment and the crown are one unit. This technique was fi rst introduced by Urdaneta and Marincola in 2007 (23).
The integrated abutment crowns off er excellent marginal adaption with a cementless interface, a bacterially sealed implant-abutment connection, a crown material with a similar wear rate and hardness values of human enamel, a simple laboratory technique and a reduced number of prosthetic components. Due to the light-cured nature of the crown material, chairside modifi cations can be accomplished(23).
Resin materials, when polished, achieve higher roughness values compared with all ceramic materials, accumulate plaque at a higher rate and are more likely to stain than tooth structure and all ceramic restorations(23).
Composite resins have also been shown to cause less wear on opposing enamel than porcelain(25-27). One of the major disadvantages of metal-ceramic and all ceramic restorations is their abrasiveness to opposing natural dentition. Both in nivo and in vitro studies have consistently demonstrated that porcelain causes excessive enamel wear(28-33).
However, other studies are necessary to evaluate the performance of Integrated Abutment Crowns (IAC) with a longer follow up.
ConclusionsThe Integrated Abutment Crown, the screwless and
cementless technique provided the patients the esthetic, function and comfort during the post-loading follow up period. The implant placed nearly to the inferior alveolar nerve was uneventful.
Fig. 31 Clinical photo of IACs 44, 45
Fig. 34 Periapical radiograph after 2 years of 36
Fig. 32 Clinical photo of IACs 36
Fig. 30 Periapical radiograph of the implants and their loadings (44, 45)
Fig. 33 Periapical radiograph after 2 years of 44 and 45
Clinical and radiographic control of implants after 2 years:
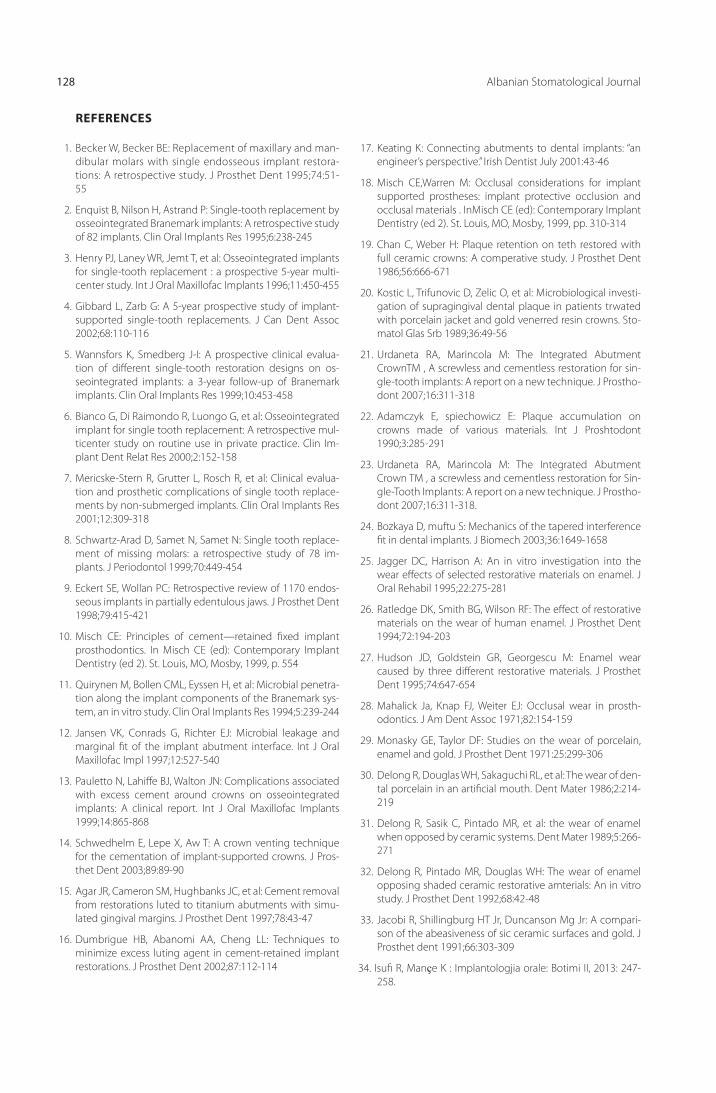
Albanian Stomatological Journal128
REFERENCES
1. Becker W, Becker BE: Replacement of maxillary and man-dibular molars with single endosseous implant restora-tions: A retrospective study. J Prosthet Dent 1995;74:51-55
2. Enquist B, Nilson H, Astrand P: Single-tooth replacement by osseointegrated Branemark implants: A retrospective study of 82 implants. Clin Oral Implants Res 1995;6:238-245
3. Henry PJ, Laney WR, Jemt T, et al: Osseointegrated implants for single-tooth replacement : a prospective 5-year multi-center study. Int J Oral Maxillofac Implants 1996;11:450-455
4. Gibbard L, Zarb G: A 5-year prospective study of implant-supported single-tooth replacements. J Can Dent Assoc 2002;68:110-116
5. Wannsfors K, Smedberg J-I: A prospective clinical evalua-tion of diff erent single-tooth restoration designs on os-seointegrated implants: a 3-year follow-up of Branemark implants. Clin Oral Implants Res 1999;10:453-458
6. Bianco G, Di Raimondo R, Luongo G, et al: Osseointegrated implant for single tooth replacement: A retrospective mul-ticenter study on routine use in private practice. Clin Im-plant Dent Relat Res 2000;2:152-158
7. Mericske-Stern R, Grutter L, Rosch R, et al: Clinical evalua-tion and prosthetic complications of single tooth replace-ments by non-submerged implants. Clin Oral Implants Res 2001;12:309-318
8. Schwartz-Arad D, Samet N, Samet N: Single tooth replace-ment of missing molars: a retrospective study of 78 im-plants. J Periodontol 1999;70:449-454
9. Eckert SE, Wollan PC: Retrospective review of 1170 endos-seous implants in partially edentulous jaws. J Prosthet Dent 1998;79:415-421
10. Misch CE: Principles of cement—retained fi xed implant prosthodontics. In Misch CE (ed): Contemporary Implant Dentistry (ed 2). St. Louis, MO, Mosby, 1999, p. 554
11. Quirynen M, Bollen CML, Eyssen H, et al: Microbial penetra-tion along the implant components of the Branemark sys-tem, an in vitro study. Clin Oral Implants Res 1994;5:239-244
12. Jansen VK, Conrads G, Richter EJ: Microbial leakage and marginal fi t of the implant abutment interface. Int J Oral Maxillofac Impl 1997;12:527-540
13. Pauletto N, Lahiff e BJ, Walton JN: Complications associated with excess cement around crowns on osseointegrated implants: A clinical report. Int J Oral Maxillofac Implants 1999;14:865-868
14. Schwedhelm E, Lepe X, Aw T: A crown venting technique for the cementation of implant-supported crowns. J Pros-thet Dent 2003;89:89-90
15. Agar JR, Cameron SM, Hughbanks JC, et al: Cement removal from restorations luted to titanium abutments with simu-lated gingival margins. J Prosthet Dent 1997;78:43-47
16. Dumbrigue HB, Abanomi AA, Cheng LL: Techniques to minimize excess luting agent in cement-retained implant restorations. J Prosthet Dent 2002;87:112-114
17. Keating K: Connecting abutments to dental implants: “an engineer’s perspective.” Irish Dentist July 2001:43-46
18. Misch CE,Warren M: Occlusal considerations for implant supported prostheses: implant protective occlusion and occlusal materials . InMisch CE (ed): Contemporary Implant Dentistry (ed 2). St. Louis, MO, Mosby, 1999, pp. 310-314
19. Chan C, Weber H: Plaque retention on teth restored with full ceramic crowns: A comperative study. J Prosthet Dent 1986;56:666-671
20. Kostic L, Trifunovic D, Zelic O, et al: Microbiological investi-gation of supragingival dental plaque in patients trwated with porcelain jacket and gold venerred resin crowns. Sto-matol Glas Srb 1989;36:49-56
21. Urdaneta RA, Marincola M: The Integrated Abutment CrownTM , A screwless and cementless restoration for sin-gle-tooth implants: A report on a new technique. J Prostho-dont 2007;16:311-318
22. Adamczyk E, spiechowicz E: Plaque accumulation on crowns made of various materials. Int J Proshtodont 1990;3:285-291
23. Urdaneta RA, Marincola M: The Integrated Abutment Crown TM , a screwless and cementless restoration for Sin-gle-Tooth Implants: A report on a new technique. J Prostho-dont 2007;16:311-318.
24. Bozkaya D, muftu S: Mechanics of the tapered interference fi t in dental implants. J Biomech 2003;36:1649-1658
25. Jagger DC, Harrison A: An in vitro investigation into the wear eff ects of selected restorative materials on enamel. J Oral Rehabil 1995;22:275-281
26. Ratledge DK, Smith BG, Wilson RF: The eff ect of restorative materials on the wear of human enamel. J Prosthet Dent 1994;72:194-203
27. Hudson JD, Goldstein GR, Georgescu M: Enamel wear caused by three diff erent restorative materials. J Prosthet Dent 1995;74:647-654
28. Mahalick Ja, Knap FJ, Weiter EJ: Occlusal wear in prosth-odontics. J Am Dent Assoc 1971;82:154-159
29. Monasky GE, Taylor DF: Studies on the wear of porcelain, enamel and gold. J Prosthet Dent 1971:25:299-306
30. Delong R, Douglas WH, Sakaguchi RL, et al: The wear of den-tal porcelain in an artifi cial mouth. Dent Mater 1986;2:214-219
31. Delong R, Sasik C, Pintado MR, et al: the wear of enamel when opposed by ceramic systems. Dent Mater 1989;5:266-271
32. Delong R, Pintado MR, Douglas WH: The wear of enamel opposing shaded ceramic restorative amterials: An in vitro study. J Prosthet Dent 1992;68:42-48
33. Jacobi R, Shillingburg HT Jr, Duncanson Mg Jr: A compari-son of the abeasiveness of sic ceramic surfaces and gold. J Prosthet dent 1991;66:303-309
34. Isufi R, Manҫe K : Implantologjia orale: Botimi II, 2013: 247-258.

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 129
Abstrakt
Hyrje Amalgami është një material që përdoret për mbushjen e dhëmbëve për një kohë të gjatë. Emri i tij i referohet një procesi kimiko-fi zik, me anë të të cilit realizohet një përzierje metalesh në gjendje të ndryshme fi zike dhe produkti më pas kalon në fazë kristaline. Një dozë amalgam përmban: 440 mg mërkur dhe 400 mg lidhje Ag, Sn, Cu, Zn. Një mbushje me amalgam lëshon çdo ditë 0.5-1.0 μg mërkur, sasi kjo që mund të shtohet nga korrozioni, abrazioni, shkarkime elektrike që prodhohen nga metale të ndryshme në mjedisin me pështymë të kavitetit oral. Dhe kripërat e ushqimeve, përtypja e çimçakëzit, lëngjet e gazuara, acidet ushqimore shpejtojnë shpërbërjen e amalgamit.
Qëllimi Të evidentohet çlirimi i mërkurit në pështymë nga mbushjet me amalgam dhe të matet niveli i tij me anë të testeve.
Materiali dhe metodaNë këtë studim janë përfshirë 70 subjekte me mbushje amalgami në gojë dhe 30 subjekte që nuk kanë asnjë mbushje amalgami (mund të kenë prani të mbushjeve me kompozit). Te këto subjekte u realizuan teste për matjen e nivelit të mërkurit të cliruar në pështymë para dhe pas mastikimit.
Rezultate dhe diskutime Në subjektet me mbushje amalgami në gojë u vu re që çlirohej mërkur si para dhe pas mastikimit. Sikurse referon dhe referenca, sasia e mërkurit të çliruar pas mastikimit rritet. Ne subjektet pa mbushje amalgami u vu re që nuk kishte ndryshim të ngjyrës së testeve të kryera.
KonkluzioneNga mbushjet me amalgam çlirohet mërkur si para dhe pas mastikimit. Sasia e mërkurit që çlirohet në pështymë pas mastikimit rritet krahasuar me atë para mastikimit. Te subjektet pa mbushje amalgami nuk çlirohet mërkur në pështymë.
FJALËT KYÇE:
Amalgam,
teste, çlirim
Hyrje Amalgami është një material që përdoret për
mbushjen e dhëmbëve për një kohë të gjatë. Emri i tij i referohet një procesi kimiko-fi zik, me anë të të cilit bëhet një përzierje metalesh në gjendje të ndryshme fi zike dhe produkti më pas kalon në fazë kristaline (1, 2).
Një dozë amalgam përmban 440 mg mërkur dhe 400 mg nga lidhja e metaleve të tjera (1). Në shumë studime të kryera në disa vende të botës është arritur në konkluzionin se në pacientë që kanë mbushje amalgami në gojë, çlirohet vazhdimisht zhivë në pështymë (4, 5, 6, 7,
12, 13, 14, 15, 16, 17, 18, 19). Një dozë amalgami çliron cdo ditë 0.5 – 1 mg mërkur si rezultat i abrazionit, korrozionit (3, 8, 9, 10,
11, 12, 13), reaksioneve elektrolitike, që ndodhin në mjedisin e gojës.
Mërkuri është metal mjaft toksik, sidomos për sistemin nervor (ku dhe grumbullohet) dhe për veshkat. Fenomeni i çlirimit të mërkurit nga mbushjet me amalgam është një fenomen kimiko-fi zik. Kur krijohet materiali, përzjehet mërkur me lidhjen Sn-Cu (kallaj- bakër) dhe ky element është pak më tepër në sasi krahasuar me pluhurin. Arsyeja është të realizohet lagia e të gjitha pjesëzave solide. Në harkun kohor të disa minutave fi llojnë të formohen kristalet e lidhjes së re që përmbajnë mërkur. Kristalet e sapoformuara paraqesin një strukturë molekulare jo tërësisht perfekte dhe thithin një sasi të lartë metali likid.
D.M.Sc. Edlira Dedaj1, Prof. Rozarka Budina2, Dr. Henri Dedaj3
Niveli i mërkurit në pështymë i çliruar nga mbushjet me amalgam
1Universiteti Aldent, 2Fakulteti i Mjekësisë Dentare, 3Klinikë private,

Revista Stomatologjike Shqiptare130
Struktura kristaline duke kaluar muajt dhe vitet paraqet një fenomen evoluimi dhe maturimi. Kjo bën që të duhet më pak mërkur se sa është lidhur. Një pjesë e tij del nga lidhja kristaline dhe i shtohet pjesës së palidhur, që është e pranishme në origjinë të materialit. Është pikërisht kjo sasi në gjendje të lëvizë lirshëm në metal dhe në temperaturën 37°C avullon në formën e avujve në kavitetin e gojës.
Dokumenti i parë zyrtar nga OBSH (Organizata Botërore e Shëndetësisë) mbi mërkurin inorganik në 1991 u ndihmua nga puna e Svare, që tregoi sesi avujt e mërkurit janë gjithmonë të pranishme në kavitetin oral të subjekteve me mbushje amalgami dhe në rastet kur nuk ka stimulim të sipërfaqeve të mbushura (5).
Qëllimi
Të evidentohet çlirimi i mërkurit në pështymë nga mbushjet me amalgam dhe të matet niveli i tij me anë të testeve.
Materiali dhe metoda
Studimi përfshin realizimin e testeve për të matur nivelin e mërkurit të çliruar para dhe pas mastikimit në pështymën e 70 subjekteve me mbushje amalgami në gojë (me numër të ndryshëm sipërfaqesh të mbushura). Është marrë dhe një grup kontrolli me 30 subjekte pa mbushje amalgami (mbushjet e amalgamit nuk kanë qenë asnjëherë të pranishme). Përzgjedhja e subjekteve në të dy grupet është bërë në mënyre rastësore. Mosha e subjekteve varion nga 17 vjeç në 69 vjeç me një moshë mesatare, të grupuar në grupmoshën 31-35. Studimi është shtrirë gjatë një periudhe kohore prej 4 vjetësh (2010- 2014).
Secilit subjekt i është marrë konsensusi për përfshirjen e tij në studim. Në të gjithë subjektet është marrë anamneza nëpërmjet një kartele tip, ku janë dokumentuar me hollësi gjeneralitetet e pacientit, anamneza vitae, anamneza familjare. Tek anamneza i është kushtuar vëmendje dietës ushqimore (duke dokumentuar shpeshtinë e përdorimit të produkteve të detit), profesionit (për të përjashtuar mundësinë
Protokolli për kryerjen e testeve
Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 131
Grafiku 1
Subjektet që iu janë nënshtruar testeve
Tabela 1
Rezultatet e matjeve të nivelit të mërkurit në pështymën e disa subjekteve me mbushje amalgami
Subjekti Mosha Gjinia Niveli i mërkurit para mastikimit
Niveli i mërkurit pas mastikimit
1. 36 F 0,05 0,1
2. 35 F 0,05 0,4
3. 26 F 0,1 0,4
4. 56 M 0,1 0,4
5. 38 M 0,2 0,8
6. 25 M 0,1 0,4
7. 29 F 0,1 0,4
8. 24 F 0,1 0,8
9. 17 F 0,05 0,1
10. 36 F 0,025 0,05
11. 27 F 0,2 0,8
12. 52 F 0,05 0,1
13. 41 F 0,025 0,05
14. 49 F 0,025 0,05
15. 21 F 0,05 0,1
Rezultatee punës në mjedise me mërkur), prejardhjes së individëve (duke gjykuar për zona të banuara, të cilat kanë qenë pranë zonave industriale që përdorin mërkur). Duke qenë se disa medikamente mund të ndikonin në saktësinë e testeve të kryera, subjektet iu nënshtruan një pyetësori.
Testi i zgjedhur për matjen e nivelit të mërkurit në pështymë të çliruar, është HMT Mercury Test. Pështyma që do t’i nënshtrohet testimit, në fillim përpunohet. Për këtë merret 10 ml pështymë, 8 ml të së cilës përzjehen me 2 ml acid acetik 10%. Përzierja zjehet dhe filtrohet. Duhet që pH i përzierjes së marrë të jetë 3-5. Për këtë mund të shtohet hidroksid matriumi. 6 ml e kësaj përzierjeje testohet me testet e gatshme dhe bëhet vlerësimi i ngjyrës së përzierjes sipas shkallës së ngjyrave të paraqitur në kutinë e testeve. E njëjta procedurë ndiqet dhe për matjen e nivelit të mërkurit në pështymë pas mastikimit 10 minuta të cimcakëzit.
70%
30%
Subjekte qe kane kryer testetsubjekte me mbushje amalgami subjekte pa mbushje amalgami
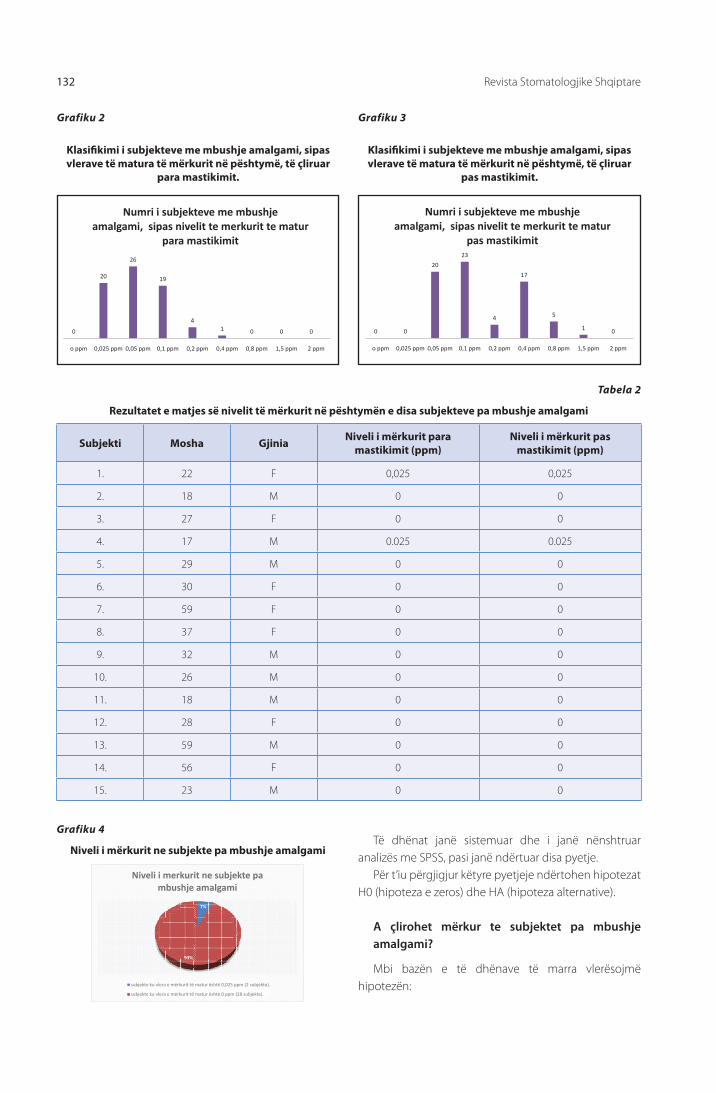
Revista Stomatologjike Shqiptare132
0
20
26
19
41 0 0 0
o ppm 0,025 ppm 0,05 ppm 0,1 ppm 0,2 ppm 0,4 ppm 0,8 ppm 1,5 ppm 2 ppm
Numri i subjekteve me mbushje amalgami, sipas nivelit te merkurit te matur
para mastikimit
Grafiku 2
Klasifi kimi i subjekteve me mbushje amalgami, sipas vlerave të matura të mërkurit në pështymë, të çliruar
para mastikimit.
Grafiku 3
Klasifi kimi i subjekteve me mbushje amalgami, sipas vlerave të matura të mërkurit në pështymë, të çliruar
pas mastikimit.
0 0
20
23
4
17
5
1 0
o ppm 0,025 ppm 0,05 ppm 0,1 ppm 0,2 ppm 0,4 ppm 0,8 ppm 1,5 ppm 2 ppm
Numri i subjekteve me mbushje amalgami, sipas nivelit te merkurit te matur
pas mastikimit
Tabela 2
Rezultatet e matjes së nivelit të mërkurit në pështymën e disa subjekteve pa mbushje amalgami
Subjekti Mosha Gjinia Niveli i mërkurit para mastikimit (ppm)
Niveli i mërkurit pas mastikimit (ppm)
1. 22 F 0,025 0,025
2. 18 M 0 0
3. 27 F 0 0
4. 17 M 0.025 0.025
5. 29 M 0 0
6. 30 F 0 0
7. 59 F 0 0
8. 37 F 0 0
9. 32 M 0 0
10. 26 M 0 0
11. 18 M 0 0
12. 28 F 0 0
13. 59 M 0 0
14. 56 F 0 0
15. 23 M 0 0
Grafiku 4
Niveli i mërkurit ne subjekte pa mbushje amalgami
7%
93%
Niveli i merkurit ne subjekte pa mbushje amalgami
subjekte ku vlera e mërkurit të matur është 0,025 ppm (2 subjekte).
subjekte ku vlera e mërkurit të matur është 0 ppm (28 subjekte).
Të dhënat janë sistemuar dhe i janë nënshtruar analizës me SPSS, pasi janë ndërtuar disa pyetje.
Për t’iu përgjigjur këtyre pyetjeje ndërtohen hipotezat H0 (hipoteza e zeros) dhe HA (hipoteza alternative).
A çlirohet mërkur te subjektet pa mbushje amalgami?
Mbi bazën e të dhënave të marra vlerësojmë hipotezën:

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 133
H0: ”Në pacientët pa mbushje amalgami nuk ka çlirim të mërkurit, si para ashtu edhe pas mastikimit.”
HA: “Në pacientët pa mbushje amalgami ka çlirim të mërkurit, si para ashtu edhe pas mastikimit.”
Vërtetimi i hipotezës zero na jep një vlerësim pozitiv
edhe mbi cilësinë e matjes me anë të testerit. Sipas hipotezës, niveli i pritshëm i rezultatit të matur për nivelin të çliruar të mërkurit në subjektet pa mbushje amalgami, duhet të jetë 0 ppm si para mastikimit ashtu edhe pas mastikimit.
Duke përdorur metoda joparametrike të SPSS për të verifi kuar me anë të testit One-Sample Binomial Test, verifi kojmë se probabiliteti i marrjes së një vlere zero (<=0) në matjen e nivelit të mërkurit të cliruar si para ashtu edhe pas mastikimit në subjektet pa mbushje amalgami është 0.98.
Vërejmë se hipoteza e zeros provohet me nivel besueshmërie mbi 95%, pra te subjektet pa mbushje amalgami nuk çlirohet mërkur para/ pas mastikimit.
A ndryshon niveli i çlirimit të mërkurit mes subjekteve me dhe pa mbushje?
Për “Niveli i mërkurit para mastikimit”:H0: “Shpërndarja e vlerave të nivelit të mërkurit
Tabela 3
Përmbledhje e testimit te hipotezave
Hipoteza 0 Testi Sig. Vendimi
1Kategoritë e përcaktuara nga Niveli i mërkurit para mastikimit me vlerë <=0.0 dhe vlerë >0.00 vërehen me probabilitete respektivisht 0.98 dhe 0.02.
One-Sample Binomial Test
.120Pranohet hipoteza
zero.
2Kategoritë e përcaktuara nga Niveli i mërkurit pas mastikimit me vlerë <=0.0 dhe vlerë >0.00 vërehen me probabilitete respektivisht 0.98 dhe 0.02.
One-Sample Binomial Test
.120Pranohet hipoteza
zero.
Niveli α=.05.
para mastikimit nuk ndryshon ndërmjet subjekteve pa mbushje dhe me mbushje”.
HA: “Shpërndarja e vlerave të nivelit të mërkurit para mastikimit ndryshon ndërmjet subjekteve pa mbushje dhe me mbushje”.
Për “Niveli i Hg pas mastikimit”:H0: “Shpërndarja e vlerave të nivelit të mërkurit
pas mastikimit nuk ndryshon ndërmjet subjekteve pa mbushje dhe me mbushje”.
HA: “Shpërndarja e vlerave të nivelit të mërkurit pas mastikimit ndryshon ndërmjet subjekteve pa mbushje dhe me mbushje”.
Për analizë përdorim testin joparametrik të shembujve të pavarur, si më poshtë:
Tabela 4
Përmbledhje e testimit te hipotezave
Hipoteza 0 Testi Sig. Vendimi
1Shpërndarja e Niveli i mërkurit para mastikimit ështëe njëjtë ndërmjet kategorive të krijuara nga SipërfaqeZeroJoZero.
Independent-Samples Mann-Whitney U Test
.000Hidhet poshtë
hipoteza 0.
2Shpërndarja e Niveli i mërkurit pas mastikimit është e njëjtë ndërmjet kategorive të krijuara nga SipërfaqeZeroJoZero.
Independent-Samples Mann-Whitney U Test
.000Hidhet poshtë
hipoteza 0.
Niveli α=.05.
Nga rezultatet shohim se konfi rmohet ndryshimi ndërmjet shpërdarjes së vlerave të matjeve te subjektet pa mbushje dhe atyre me mbushje amalgami, pasi me besueshmëri mbi 95% hidhet poshtë hipoteza zero, që pretendon shpërndarje të njëjtë të vlerave në dy
kategoritë. Pra matjet evidentojnë ndryshimin e nivelit të çlirimit të mërkurit ndërmjet subjekteve pa mbushje dhe atyre me mbushje amalgam si para dhe pas mastikimit, me një besueshmëri 95%.

Revista Stomatologjike Shqiptare134
Raste klinike
DiskutimeNë subjektet me mbushje amalgami çlirohet
vazhdimisht mërkur në hapësirën e gojës. Kjo sasi rritet në rastin e mastikimit të çimçakëzit. Stimulimi i pacientit, nëpërmjet mastikimit, rrit sasinë e mërkurit të çliruar dhe kjo rritje shtohet sipas numrit të sipërfaqeve të mbushura. Sasitë e mërkurit të çliruar në kavitetin e gojës nga mbushjet me amalgam nuk janë të mëdha ose toksike, por problemi është se ato janë të vazhdueshme
Figurat 1- Rezultatet e testit për matjen e nivelit të mërkurit të çliruar para dhe pas mastikimit (subjekti K. Z, mosha 17 vjeç, pa mbushje amalgam ne gojë) –Vlerat e matura të mërkurit të çliruar janë 0.025 ppm para mastikimit dhe 0.025 ppm pas
mastikimit të çamçakëzit
Figura 2- Rezultatet e testit për matjen e nivelit të mërkurit të çliruar para dhe pas mastikimit (subjekti M. P, mosha 38
vjeç, me 10 sipërfaqe amalgami në gojë) –Vlerat e matura te mërkurit të çliruar janë 0,2 ppm para mastikimit dhe 0.8 ppm
pas mastikimit të çimçakëzit
dhe mërkuri ka tendencë të grumbullohet duke qenë se është metal i rëndë. Grumbullimi i vazhdueshëm i këtij elementi, e ekspozon individin ndaj risqeve që sjell mërkuri në organizëm. Në këtë studim u pa se në subjektet pa mbushje amalgami nuk çlirohet mërkur, ndërsa në subjektet me mbushje amalgami çlirohet mërkur në pështymë si para dhe pas mastikimit të çimçakëzit . Të njëjtat të dhëna referon dhe referenca (3,
4, 5, 6, 7, 14, 15, 79, 20, 21, 22, 23, 24). Clirimi i mërkurit në pështymë është një dukuri e pakundërshtueshme, që ndodh në cdo subjekt me mbushje amalgami, dhe, vlerat matura në këtë studim, për nivelin e mërkurit në pështymë janë të krahasueshme me vlera në studimet e kryera nga Gradl dhe Gebhardt(25), Engin-Deniz me bp(26), Mayer me bp(27), Gerhard me bp (28), Ott me bp (29). Ndërkohë autorë si Schiwara me bp(30), kanë sjellë rezultate me vlera më të larta të çlirimit të mërkurit.
Konkluzione1. Nga mbushjet me amalgam çlirohet mërkur si para
dhe pas mastikimit. Vlerat e matura të mërkurit në pështymë në subjektet me mbushje amalgami variojnë nga 0,025 ppm- 1,5 ppm.
2. Tek subjektet pa mbushje amalgami nuk çlirohet mërkur në pështymë.Vlerat e matura të mërkurit në peshtymë në subjektet pa mbushje amalgami janë 0 ppm, me përjashtim të dy rasteve (6% e subjekteve), ku vlerat e matura janë 0,025 ppm.
1. Garg N, Garg A, Textbook of Preclinical Conservative Den-tistry, 2011: 163-200
2. Budina R, Gavazi B, Droboniku E, Dentistria Restorative, 2010, 91-100
REFERENCA
3. Gay DD, Cox RD, Reinhard JW. Chewing releases mercury from fi lling (letter). Lancet 1979; 1:985-986.
4. Mackert JR Jr. Factors aff ecting estimation of dental amal-gam mercury exposure from measurements of mer-

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 135
cury vapor levels in intraoral and expired air. J Dent Res 1987;66:1775-1780.
5. Svare CW, Peterson Lc, Reinhardt JW. The eff ect of dental amalgams on mercury levels in expired air. J Dent Res 1981; 60: 1668-1671.
6. Vimy MJ, Lorscheider FL. Intraoral air mercury released from dental amalgam. J Dent Res 1985;64: 1069-1071.
7. Vimy MJ, Lorscheider FL. Serial measurements of intraoral air mercury: Estimation of daily dose from dental amalgam. J Dent Res 1985; 64: 1072-1075
8. Ronchi F, Nobili P. Biocompatibilità dei materiali odon-toiatrici. In: Progressi in odontoiatria. Cap 8. Torino: Utet 2005:277-312.
9. Sutow E, Maillet W, Taylor J, Hall G. In vivo galvanic currents of intermittently contacting dental amalgam and other metallic restorations 2004; 20(9):823-831.
10. Bergman M. Corrosion in the oral cavity. Potential local and systemic eff ects. Int Dent J 1986 Mar; 36(1):41-4.
11. Inovay J, Bànòczy J. The role of electrical potential diff erenc-es in the etiology of chronic diseases of the oral mucosa. Dent Res 1961;40(5):884-890.
12. Brune, D.: Corrosion of amalgams. J Dent Res 1981; 89, 506-514.
13. Moberg, L.-E.: Corrosion of dental amalgam and mercury vapor emission in vitro. Scand J Dent Res 1988; 96, 473-477.
14. Takahashi, Y., Hasegawa, J. und Kameyama, Y.: Dissolution of metallic mercury in artifi cial saliva and eleven other solu-tions. Dent Mater 1989; 5, 256-259.
15. Marek, M.: The release of mercury from dental amalgam: The mechanism and in vitro testing. J Dent Res 1990; 69, 1167-1174.
16. Olsson, S., Berglund, A. and Bergman, M.: Release of ele-ments due to electrochemical corrosion of dental amal-gam. J Dent Res 1994; 73, 33-43.
17. Westerhoff , B., Darwish, M. und Holze, R.: A comparitive electrochemical in vitro evaluation of the corrosion behav-iour of dental amalgams. J Oral Rehab 1995; 22, 121-127.
18. Holland, R. I.: Corrosion testing by potentiodynamic polar-ization in various electrolytes. Dent Mater 1992; 8, 241-245.
19. Brune, D. und Evje, D. M.: Man´s mercury loading from a dental amalgam. Sci Tot Environ 1985; 44, 51-63.
20. Holland, R. I.: Corrosion testing by potentiodynamic polar-ization in various electrolytes. Dent Mater 1992; 8, 241-245.
21. Berglund, A.: An in vitro and in vivo Study of the release of mercury vapor from diff erent types of amalgam alloys. J Dent Res 1993; 72, 939-946.
22. Halbach, S.: Fakten und Zahlen: Quecksilber aus Amalgam-füllungen. Pharm Z 1995; 140, 9-13.
23. Guo, T., Baasner, J., Gradl, M. und Kistner, A.: Determination of mercury in saliva with a fl ow-injection system. Anal Chim Acta 1996; 320, 171-176.
24. Brune, D.: Metal release from dental biomaterials. Biomate-rials 1986; 7, 163-175.
25. Gradl, M. und Gebhardt, A.: Ermittlung der Quecksilberb-elastung aus Amalgamfüllungen. Labormedizin 1992; 16, 384-386.
26. Engin-Deniz, B., Nell, A., Perger, M. und Sperr, W.: Die Queck-silberkonzentration im Speichel zehnjähriger Kinder in Kor-relation zur Anzahl und Größe ihrer Amalgamfüllungen. Z Stomatol 1992; 89, 471-479.
27. Mayer, R., Dobler, J., Gehlen, S. und Gradl, M.: Zur Ermittlung der Quecksilberfreisetzung aus Amalgamfüllungen mit Hil-fe des sogenannten Kaugummitests. Die Quintessenz 1994; 45, 1143-1152.
28. Gerhard, I., Waldbrenner, P., Thuro, H. und Runnebaum, B.: Diagnostik von Schwermetallbelastungen mit dem pero-ralen DMPS-Test und dem Kaugummitest. Klin Lab 1992; 38, 404-411.
29. Ott, K. H. R., Loh, F., Kröncke, A., Schaller, K.-H., Valentin, H. und Weltle, D.: Zur Quecksilberbelastung durch Amalgam-füllungen. Dtsch Zahnärztl Z 1984; 39, 199-205.
30. Schiwara, H.-W., Daunderer, M., Kirchherr, H., Heß, C., Hard-ers, B., Hoppe, H.-W., Molsen, C., Engler, J., Scholze, M., Bu-chterkirche, B. und Buchterkirche, C.: Bestimmung von Kupfer, Quecksilber, Methylquecksilber, Zinn, Methylzinn und Silber in Körpermaterial von Amalgamtragern 1992; 38: 391- 403.

Albanian Stomatological Journal136
Abstract
Introduction The amalgam is a material used for teeth fi lling for a long time. Its name refers to a chemical-physical process, through which is made a mix of metals in diff erent physical conditions and then the product passes into the crystalline phase. An amalgam dosis contains: 440 mg mercury and 400 mg welding of Ag, Sn, Cu, Zn. An amalgam fi lling releases every day 0.5-1.0 μg mercury and the amount can be increased by corrosion, abrasion, electric discharges produced by diff erent metals in the saliva environment of the oral cavity. Also food salt, chewing gum, carbonated juices and food acids accelerate dissolution of amalgam.
AimEmphasizing the release of mercury form amalgam fi llings in the saliva and measuring its levels by testing.
Materials and methodologyIn this research have been involved 70 subjects with amalgam fi llings in their mouths and 30 subjects that do not have any amalgam fi lling (may have presence of composite fi llings). These subjects have been tested for the measurement of the mercury levels released in the saliva before and after mastication.
Results and DiscussionsIn the subjects with amalgam fi lling in their mouth has been noted the release of mercury before and after the mastication. And as literature refers, the amount of mercury released after mastication increases. In the subjects without amalgam fi llings has been noted that there was no colour change of the tests performed.
ConclusionsFrom the amalgam fi llings mercury is released before and after mastication. The amount of mercury released in the saliva after mastication increases compared to that released before mastication. There is no amalgam release in the saliva of the subjects that dont have any amalgam fi lling.
The mercury levels released in saliva from amalgam fi llings
KEYWORDS:
Amalgam,
testing, release
IntroductionThe amalgam is a material used for teeth fi lling for a
long time. Its name refers to a chemical-physical process, through which is made a mix of metals in diff erent physical conditions and then the product passes into the crystalline phase. (1, 2).
An amalgam dosis contains: 440 mg mercury and 400 mg welding of other metals. (1). In many researches conducted in diff erent countries of the world, has been deducted that in the mouth of the patients that have amalgam fi llings, mercury is continuously released in the saliva.(4, 5, 6, 7, 12, 13, 14, 15, 16, 17, 18, 19). A dose of amalgam releases from 0.5 – 1 mg of mercury daily as a result of abrasion,
corrosion (3, 8, 9, 10, 11, 12, 13) and electrolitic reactions that happen in the mouth environment.
Mercury is a pretty toxic metal, especially for the nervous system (where it is collected) and for the kidneys as well. The release of mercury from the amalgam fi lling is a chemical-physical phenomenon. The material is created from the mixture of mercury with the welding of Sn-Cu (tin and copper) and this element is in a relatively bigger amount than the dust. This is done in order to wet all the solid pieces. In the length of a few minutes the crystals starts the creation of the new welding that contain mercury. The newly created crystals represent a non totally perfect molecular structure and absorb a
D.M.Sc. Edlira Dedaj1, Prof. Rozarka Budina2, Dr. Henri Dedaj3
1Aldent University, 2Dental Medicine Faculty, 3Private Clinic

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 137
greater amount of liquid metal. The crystalline structure shows a phenomenon of evolution and maturation with the passing of months and years. This gives the impression that there is less mercury than its real presence. A part of it comes out from the crystalline structure and is added to the uwelded part that is present in the origin of the material. And precisely this amount is able to move freely in the metal and in a temperature of 37°C, it evaporates in the form of steams in the mouth cavity.
The fi rst offi cial document of WHO (World Health Organization) about inorganic mercury in 1991, has been helped by the work of Svare, who demonstrated that mercury steams are always present in the oral cavity of the subjects who have amalgam fi llings, including the cases when there is no stimulation of the fi lled surfaces (5).
Objective
Emphasizing the release of mercury form amalgam fi llings in the saliva and measuring its levels by testing.
Materials and methodologyThe study involves the performance measurements
tests for the levels of mercury before and after mastication released in the saliva of 70 subjects with amalgam fi lling in their mouth (with diff erent numbers of fi lled surfaces). There has also been tested a testing group of 30 subjects without amalgam fi lling (amalgam fi llings have never been present).
The selection of the subjects of both groups has been random. The age of the subjects varies from 17 to 69 years, with an average age of approximately 31-35. The research is conducted during a period of 4 years (2010- 2014).
Each subject has been asked for the consensus of the inclusion in the research. The anamnesis of each subject has been collected through a fi le where all the generalities of the patient have been drafted in a detailed manner, anamnesis vitae, familiar anamnesis. A special attention in the anamnesis has been paid to the nutrition diet ( drafting the frequency of the consumption of seafood), to the profession (in order to exclude the possibility of a job in mercury environments), the origin
The protocol for conducting tests

Albanian Stomatological Journal138
Resultsof the individuals (considering the inhabitet areas near the industrial ones that use mercury). Considering that some medicaments could infl uence in the preciseness of the tests performed, the subjects have undergone a questionnaire.
The test chosen for the measurement of the mercury level released in the saliva, is the Mercury Test. The saliva to be examined, will fi rst be processed. This will be done taking 10 ml of saliva, 8 mg of which will be mixed with 2 ml acetic acid 10%. The mixture will then be boiled and fi ltered. The pH of the mixture must be 3-5. To achieve this, natrium hydroxide can be added. 6 ml of the mixture is tested with the sample tests and the examination of the color of the mixture is done in accordance with the color scale featured in the test boxes. The same procedure is followed for the measurement of the mercury levels released in the saliva 10 minutes after mastication.
Chart 1
Subjects that have taken the test
Table 1
The results of the measurement of the mercury levels released in the saliva of some patients with amalgam fi llings.
Subject Age Gender The level of mercury before mastication
The level of mercury after mastication
1. 36 F 0,05 0,1
2. 35 F 0,05 0,4
3. 26 F 0,1 0,4
4. 56 M 0,1 0,4
5. 38 M 0,2 0,8
6. 25 M 0,1 0,4
7. 29 F 0,1 0,4
8. 24 F 0,1 0,8
9. 17 F 0,05 0,1
10. 36 F 0,025 0,05
11. 27 F 0,2 0,8
12. 52 F 0,05 0,1
13. 41 F 0,025 0,05
14. 49 F 0,025 0,05
15. 21 F 0,05 0,1
Subjects that have taken the test
70%
30%
subjects with amalgam fillings subjects without amalgam fillings

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 139
Chart 2
The classifi cation of the subjects with amalgam fi lling according to the mercury levels measured in the saliva,
released before mastication.
Chart 3
The classifi cation of the subjects with amalgam fi lling according to the mercury levels measured in the saliva,
released after mastication.
Table 2
The results of the measurement of mercury levels in the saliva of some subjects without amalgam fi llings
Subject Age Gender Mercury level before mastication (ppm)
Mercury level after mastication (ppm)
1. 22 F 0,025 0,025
2. 18 M 0 0
3. 27 F 0 0
4. 17 M 0.025 0.025
5. 29 M 0 0
6. 30 F 0 0
7. 59 F 0 0
8. 37 F 0 0
9. 32 M 0 0
10. 26 M 0 0
11. 18 M 0 0
12. 28 F 0 0
13. 59 M 0 0
14. 56 F 0 0
15. 23 M 0 0
Chart 4
Mercury levels in subjects without amalgam fi llings
0
20
26
19
41 0 0 0
o ppm 0,025 ppm 0,05 ppm 0,1 ppm 0,2 ppm 0,4 ppm 0,8 ppm 1,5 ppm 2 ppm
The number of subjects with amalgam filling, according to the mercury level
measured before mastication.
0 0
20
23
4
17
5
1 0
o ppm 0,025 ppm 0,05 ppm 0,1 ppm 0,2 ppm 0,4 ppm 0,8 ppm 1,5 ppm 2 ppm
The number of subjects with amalgam filling according to the mercury levels measured
after mastication.
7%
93%
Mercury levels in subjects without amalgam fillings
subjects where the measured value of released mercury is 0,025 ppm (2 subjects).
subjects where the measured value of released mercury is 0 ppm (28 subjects).
The above data have been arranged and undergone the SPSS examintaion, after some questions have been raised.
In order to answer these questions H0 hypothesis are created (the zero hypothesis) and HA (alternative hypothesis).
Is mercury released in subjects without amalgam fi lling?On the basis of the data collected, we can evaluate
the hypothesis:H0: ”There is no mercury release in patients without

Albanian Stomatological Journal140
amalgam filling, both before and after mastication..”HA: “ In patients with amalgam fi llings mercury is
released both before and after mastication.”The confirmation of the zero hypothesis provides
us a positive evaluation for the quality of the
measurement by testing. According to the hypothesis, the expected level of the measured result for the mercury released in the subjects without amalgam filling, is estimated to be 0 ppm both before and after mastication.
released before mastication doesn’t diff er from subjects with or without fi lling”.
HA: “The distribution of the rates of the mercury levels released before mastication diff ers from subjects with or without fi lling”.
For “Hg level after mastication”:H0: “ The distribution of the rates of the mercury levels
released after mastication doesn’t diff er from subjects with or without fi lling”.
HA: “The distribution of the rates of the mercury levels released after mastication diff ers from subjects with or without fi lling”.
The nonparametric test of independent examples is used for the examination, as follows:
From the results is noted the confi rmation of the diff erend between the distribution of the values of measurement in the subjects without fi lling and those with amalgam fi lling, beacuse the zero hypothesis which claims equal distribution of the values in both categories
is rejected with a rate of reliability of 95%. Therefore the measurements highlight the diff erence of the level of mercury release between subjects without and those with amalgam fi lling, both before and after mastication, with a reliability rate of 95%.
Using some nonparametric methods of SPSS to examine by testing with the One-Sample Binomial Test, is verifi ed that the probability of taking a value zero (<=0) when measuring the level of mercury released both before and after mastication in the subjects without amalgam fi lling is 0.98.
It is noted that the zero hypothesis is proved with a level of reliability above 95%, as a result, there is no mercury release in the subjects without amalgam fi lling both before and after mastication.
Does the mercury level released diff er from subject with and without fi lling?
For “Mercury level before mastication”:H0: “ The distribution of the rates of the mercury levels
Tabla 3
Hypothesis testing summary
Hypothesis 0 Test Sig. Verdict
1Categories determined by: Mercury level before mastication with the values <=0.0 and values >0.00 are observed with the respective probabilities of 0.98 and 0.02.
O n e - S a m p l e Binomial Test
.120Zero Hypothesis accepted
2Categories determined by: Mercury level after mastication with the values <=0.0 and values >0.00 are observed with the respective probabilities of 0.98 and 0.02.
O n e - S a m p l e Binomial Test
.120Zero Hypothesis accepted
Level α=.05.
Tabla 4
Hypothesis testing summary
Hypothesis 0 Testi Sig. Vendimi
1The distribution of The mercury levels before mastication is the same between the categories created from ZeroNonZeroSurfaces.
I n d e p e n d e n t - S a m p l e s Mann-Whitney U Test
.000Hypothesis 0 rejected
2The distribution of The mercury levels before mastication is the same between the categories created from ZeroNonZeroSurfaces.
I n d e p e n d e n t - S a m p l e s Mann-Whitney U Test
.000Hypothesis 0 rejected
Level α=.05.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 141
Clinic Cases
DiscussionIn the subjects with amalgam fi lling, mercury is
continuously released in the mouth area. This amount increases when masticating chewing gum. The stimulation of the patient through mastication increases the amount of mercury released and this increase goes further depending on the number of the fi lled surfaces.The amount of mercury released in the mouth cavity
Images 1- The results of the tests for the measurement of mercury levels released before and after mastication (subject K. Z, age 17 years, without amalgam fi lling in his mouth) – The measured values of the released mercury are 0.025 ppm before
mastication and 0.025 ppm after the mastication of the chewing gum.
Image 2- The results of the tests for the measurement of mercury levels released before and after mastication (subject M. P, age 38 vjeç, with 10 surfaces of amalgam in the mouth) –The measured values of the released mercury are 0,2 ppm
before mastication and 0.8 ppm after the mastication of chewing gum.
from amalgam fi llings is not huge nor toxic, but the problem consists in their frequency nad the tendency to be accumulated being a heavy metal. The continuous accumulation of this element exposes the individual to the risks that mercury brings to the organism. In this study has been noticed that in subjects without amalgam fi lling mercury is not released, whether in subjects with amalgam fi lling, mercury is released in saliva both before and after mastication of chewing gum.
The same data are also referred from literature (3, 4, 5,
6, 7, 14, 15, 79, 20, 21, 22, 23, 24). The release of mercury in saliva is an incontrovertible phenomenon that occurs in every subject with amalgam fi lling and the measured values of mercury during this study are comparable to those of Gradl dhe Gebhardt(25), Engin-Deniz with bp(26), Mayer with bp(27), Gerhard with bp (28), Ott with bp (29). Meanwhile authors like Schiwara with bp(30), have brought results with higher levels of mercury release.
Conclusions1. Mercury is released from the amalgam fi llings both
before and after mastication. The measured values of mercury in saliva in the subjects with amalgam fi lling vary from 0,025 ppm- 1,5 ppm.
2. In subjects without amalgam fi lling mercury is not released in the saliva. The measured values of mercury in saliva in the subjects without amalgam fi llings are 0 ppm, excluding the two cases rasteve (6% of the subjects), where the measured values are 0,025 ppm.
REFERENCES
1. Garg N, Garg A, Textbook of Preclinical Conservative Den-tistry, 2011: 163-200
2. Budina R, Gavazi B, Droboniku E, Dentistria Restorative, 2010, 91-100
3. Gay DD, Cox RD, Reinhard JW. Chewing releases mercury from fi lling (letter). Lancet 1979; 1:985-986.
4. Mackert JR Jr. Factors aff ecting estimation of dental amal-gam mercury exposure from measurements of mer-

Albanian Stomatological Journal142
cury vapor levels in intraoral and expired air. J Dent Res 1987;66:1775-1780.
5. Svare CW, Peterson Lc, Reinhardt JW. The eff ect of dental amalgams on mercury levels in expired air. J Dent Res 1981; 60: 1668-1671.
6. Vimy MJ, Lorscheider FL. Intraoral air mercury released from dental amalgam. J Dent Res 1985;64: 1069-1071.
7. Vimy MJ, Lorscheider FL. Serial measurements of intraoral air mercury: Estimation of daily dose from dental amalgam. J Dent Res 1985; 64: 1072-1075
8. Ronchi F, Nobili P. Biocompatibilità dei materiali odon-toiatrici. In: Progressi in odontoiatria. Cap 8. Torino: Utet 2005:277-312.
9. Sutow E, Maillet W, Taylor J, Hall G. In vivo galvanic currents of intermittently contacting dental amalgam and other metallic restorations 2004; 20(9):823-831.
10. Bergman M. Corrosion in the oral cavity. Potential local and systemic eff ects. Int Dent J 1986 Mar; 36(1):41-4.
11. Inovay J, Bànòczy J. The role of electrical potential diff erenc-es in the etiology of chronic diseases of the oral mucosa. Dent Res 1961;40(5):884-890.
12. Brune, D.: Corrosion of amalgams. J Dent Res 1981; 89, 506-514.
13. Moberg, L.-E.: Corrosion of dental amalgam and mercury vapor emission in vitro. Scand J Dent Res 1988; 96, 473-477.
14. Takahashi, Y., Hasegawa, J. und Kameyama, Y.: Dissolution of metallic mercury in artifi cial saliva and eleven other solu-tions. Dent Mater 1989; 5, 256-259.
15. Marek, M.: The release of mercury from dental amalgam: The mechanism and in vitro testing. J Dent Res 1990; 69, 1167-1174.
16. Olsson, S., Berglund, A. and Bergman, M.: Release of ele-ments due to electrochemical corrosion of dental amal-gam. J Dent Res 1994; 73, 33-43.
17. Westerhoff , B., Darwish, M. und Holze, R.: A comparitive electrochemical in vitro evaluation of the corrosion behav-iour of dental amalgams. J Oral Rehab 1995; 22, 121-127.
18. Holland, R. I.: Corrosion testing by potentiodynamic polar-ization in various electrolytes. Dent Mater 1992; 8, 241-245.
19. Brune, D. und Evje, D. M.: Man´s mercury loading from a dental amalgam. Sci Tot Environ 1985; 44, 51-63.
20. Holland, R. I.: Corrosion testing by potentiodynamic polar-ization in various electrolytes. Dent Mater 1992; 8, 241-245.
21. Berglund, A.: An in vitro and in vivo Study of the release of mercury vapor from diff erent types of amalgam alloys. J Dent Res 1993; 72, 939-946.
22. Halbach, S.: Fakten und Zahlen: Quecksilber aus Amalgam-füllungen. Pharm Z 1995; 140, 9-13.
23. Guo, T., Baasner, J., Gradl, M. und Kistner, A.: Determination of mercury in saliva with a fl ow-injection system. Anal Chim Acta 1996; 320, 171-176.
24. Brune, D.: Metal release from dental biomaterials. Biomate-rials 1986; 7, 163-175.
25. Gradl, M. und Gebhardt, A.: Ermittlung der Quecksilberb-elastung aus Amalgamfüllungen. Labormedizin 1992; 16, 384-386.
26. Engin-Deniz, B., Nell, A., Perger, M. und Sperr, W.: Die Queck-silberkonzentration im Speichel zehnjähriger Kinder in Kor-relation zur Anzahl und Größe ihrer Amalgamfüllungen. Z Stomatol 1992; 89, 471-479.
27. Mayer, R., Dobler, J., Gehlen, S. und Gradl, M.: Zur Ermittlung der Quecksilberfreisetzung aus Amalgamfüllungen mit Hil-fe des sogenannten Kaugummitests. Die Quintessenz 1994; 45, 1143-1152.
28. Gerhard, I., Waldbrenner, P., Thuro, H. und Runnebaum, B.: Diagnostik von Schwermetallbelastungen mit dem pero-ralen DMPS-Test und dem Kaugummitest. Klin Lab 1992; 38, 404-411.
29. Ott, K. H. R., Loh, F., Kröncke, A., Schaller, K.-H., Valentin, H. und Weltle, D.: Zur Quecksilberbelastung durch Amalgam-füllungen. Dtsch Zahnärztl Z 1984; 39, 199-205.
30. Schiwara, H.-W., Daunderer, M., Kirchherr, H., Heß, C., Hard-ers, B., Hoppe, H.-W., Molsen, C., Engler, J., Scholze, M., Bu-chterkirche, B. und Buchterkirche, C.: Bestimmung von Kupfer, Quecksilber, Methylquecksilber, Zinn, Methylzinn und Silber in Körpermaterial von Amalgamtragern 1992; 38: 391- 403.

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 143
Përmbledhje Ushtrimi i profesionit të stomatologut përfshin një sërë elementesh stresues per sistemin muskulo-skeletal që vijnë si pasojë e pozicioneve të veçanta të punës për një kohë të gjatë,lëvizjeve të vazhduara përsëritëse në një pozicion, sforcimin e dorës dhe të krahut,pajisjeve vibruese që përdoren në praktikën e përditshme të punës.
Qëllimi: të informojmë komunitetin e dentistëve mbi sëmundjet profesionale dhe mënyrën e parandalimit,diagnostikimit dhe trajtimit të tyre.
Materiali dhe metoda: u përzgjodh referenca që trajton sëmundjet kryesore muskulo-skeletale të dentistëve. Përmes të dhënave të literaturës u njohëm me prevalencën e këtyre çrregullimeve, klinikën,shkaqet e tyre si edhe protokollet e parandalimit,diagnostikimit dhe menaxhimin.
Konkluzione dhe rekomandime: studimet tregojnë që një rol të rëndësishëm në parandalimin e çrregullimeve muskuloskeletale të dentistëve luajnë promovimi i pozicioneve të shëndetshme të punës dhe alterimi i punës herë ulur e herë në këmbë.Gjithashtu duhet të shmangen seancat e zgjatura me një pacient.
FJALËT KYÇE:
çrregullime
muskulo
skeletale,
dentist,
pozicion pune
Rudina Berani DMD, Prof. Rozarka Budina
Çrregullimet muskulo-skeletale të dentistëve
Fakulteti i Mjekësisë Dentare, Universiteti i Mjekësisë, Tiranë
Hyrje Çrregullimet muskulo-skeletale janë një grup
gjendjesh patologjike ku përfshihen nervat, tendinet,muskujt dhe strukturat mbajtëse si disqet intervertebrale. Ushtrimi i profesionit të stomatologut përfshin një sërë elementesh stresues që vijnë si pasojë e pozicioneve të veçanta të punës për një kohë të gjatë,lëvizjeve të vazhduara përsëritëse në një pozicion, sforcimin e dorës dhe të krahut,pajisjeve vibruese që përdoren në praktikën e përditshme të punës.Një nga pozicionet e parehatshme të regjionit qafë-kokë është ai kur përpiqemi të përmirësojmë shikueshmërinë dhe fushpamjen.Ky pozicion shkakton diskomfort cervikal i cili mund të përkeqsohet nga rritja e tensionit në muskujt cervikal, dhe ndërkohë që ka një dhimbje të tillë dentisti duhet të punojë dhe ti përgjigjet pacientëve.
Prevalenca e simptomaveSimptomat më të përhapura te dentistët përfshijnë
dhimbje ose diskomfort të qafës,shpatullës, bërrylit, kyçit të dorës ose të dorës, dhimbje të kurrizit dhe dhimbje të këmbës.
Në një studim të bërë te dentistët në Nebraska, 29% prej tyre vuanin simptoma të dhimbjes, simptoma neuropatike 25%, mpirje 15%, çpuese 17%, këto kryesisht në regjionin e qafës dhe të ekstremiteteve të sipërme. Regjioni kryesor që kishte simptoma si pasojë e punës ishte dora (56% të rasteve), që ndiqej nga qafa (46% të rasteve), gishti i madh (me 30% të rasteve), dhe gishti tregues (me 26% të rasteve). Dentistët në përgjithësi ankohen më së shumti për probleme të qafës, shpatullës, dhe pjesës së poshtme të kurrizit,
që janë aq shqetësuese saqë ndërhyjnë në aktivitetet ditore të tyre. (1,2,3)
Të dhënat e mbledhura nga dentistë polakë dhe norvegjezë tregojnë se dhimbja e qafës dhe ajo lumbo-sakrale janë më të përhapura. Dentistët e gjinisë femërore ankojnë më shumë për simptoma muskulo-skeletale krahasuar me kolegët e tyre të gjinisë mashkullore.
Studimet në USA tregojnë për një prevalencë të dhimbjeve të shpinës te dentistët në raport një në dy, ndërkohë që në popullatën e përgjithshme ky raport është një në shtatë. Në Danimarkë, midis 432 dentistave 60% kishin dhimbje kurrizi dhe qafe edhe kur aplikonin teknikën e punës ulur.Në një studim në Japoni që klasifi kon mostrën e marë në studim sipas inklinimit te trupit, posturat e trupit tek dentistët u grupuan në tre kategori. Postura më e zakonshme ishte ajo e pozicionit të përkulur para-djathtas.Ky studim konkludoi se postura trupore e dentistëve në punën e tyre të përditshme është shkaku kryesor dhe i vazhduar i shqetësimeve shëndetsore që lidhen me punën tek dentistët. Në një studim në Gjermani, u vu re se parametrat psiko-fi ziologjike lidheshin me dizajnin e paisjeve dhe shfrytëzimin e hapsirave në vendin e punës. Procedurat me lëvizje përsëritëse(si psh pastrimi i gurzave) dhe pozicioni i papërshtatshëm në përpjekje për të patur akses në kavitetin oral, u identifi kuan si faktorë kontribues në shqetësimet muskulo-skeletale. Në një tjetër studim nga ergonomistë,po ashtu gjermanë,u analizuan faktorët që infl uencojnë dhe përcaktojnë pozicionin e trupit gjatë punës.Të dhënat e EMG (elektromiogramës)gjatë disa aktiviteteve që kryhen në procedura rutinë në stomatologji, treguan

Revista Stomatologjike Shqiptare144
se muskujt që ndodheshin nën një sforcim të vazhduar ishin kryesisht ata spinal cervikal dhe ata lumbar. Sidomos muskujt cervikal ishin tejet të stresuar dhe të sforcuar. Faktorët e riskut në praktikën stomatologjike për ekstremitetet e sipërme përfshijnë pozicione të detyruara të gishtit dhe të kyçit të dorës, shtrëngime të përsëritura me rrotacion të kyçit të dorës,pajisjet vibruese, dizejnimin e papërshtatshëm të pajisjeve të punës për praktikat e përditshme. Kohëzgjatja dhe intensiteti i ekspozimit ndaj këtyre faktorëve (ditë pune në javë, vitet e punës),janë aspekte të rëndësishme që gjithashtu numërohen si elemente që ndikojnë në akumulim të stresit ergonomik. Tek elementët e stresit ergonomik në shpinë gjithashtu përfshihet edhe postura statike me inklinim të shtyllës kurrizore, qëndrimin në këtë pozicion përgjatë 2/3 e një trajtimi dentar që zgjat mesatarisht një orë. Shtylla kurrizore e përballon më mirë peshën e trupit qoftë në ekstension qoftë në rrotacion, kur pjesa lumbare e saj qëndron drejt dhe jo e fl ektuar. Dhimbjet në pjesën e sipërme të shpinës ulen ndjeshëm kur kalojmë ulur 60-79% të kohës së punës. Gjatë punës është mirë të mos harrojmë se postura shpesh kompromentohet, kur dentisti përkulet ose rrotullohet për të patur një fushpamje më të mirë. (4,10)
Klasifi kimi i çrregullimeve muskulo-skeletale Problemet e qafës dhe shpatullave:çrregullimet me
dhimbje miofaciale,spondiloza cervikale, sindroma e shpërhapjes torakale, tendiniti rrotator i artikulacioneve.
Çregullime të dorës dhe kyçit të dorës:sindroma DeQuervain, tendosinoviti i gishtit tregues, sindroma e tunelit Karpal,sindroma Guyon,sindroma e tunelit kubital,sindroma e dridhjeve dorë-krah, fenomeni Raynaud.
Çregullime të shtyllës kurrizore:hernia e disqeve intervertebrale,dhimbje të mesit,probleme me nervin shiatik.
Shenjat dhe simptomat kryesore janë ngadalsim i lëvizjeve,deformime,ulje të fuqisë, humbje të funksioneve muskulare,dhimbje, mpirje,ndjesi shpuese,djegie, krampe,ngurtësim.
Faktorët e çrregullimeve muskulo-skeletale që lidhen me profesionin Veprimet rutinë si lëvizjet energjike të dorës,lëvizjet
e përsëritura (pastrimi i gurëzave, përgatitja e kanalit të rrënjës,llustrimi), postura fi kse ose të pazakonta,pajisje dhe instrumenta vibruese, lëvizje të vështira të vazhduara, puna me instrumenta të vegjël për periudha të gjata kohore, ushtrimi i forcës për mbajtjen e instrumentave janë faktorët kryesorë të sëmundjeve muskuloskeletale profesionale tek dentistët.
Një faktor risku nuk është gjithmonë shkaku i çregullimeve.Niveli i riskut varet nga kohëzgjatja në të cilën ekspozohet mjeku kundrejt ketyre kushteve,sa shpesh ekspozohet,niveli i ekspozimit.Zakonisht kom-binimi i disa prej faktorëve të riskut kontribuon në sin-ergji dhe shkakton çrregullime muskulo-skeletale.Është e rëndësishme të mos fokusohemi vetëm në vendin e punës. Faktorë risku mund të paraqiten dhe në aktiv-itete të tjera jo profesionale.Jo çdo njeri i ekspozuar ndaj një ose disa faktorëve risku do të pësojë një çrregullim muskulo skeletal.Njerëzit reagojnë në mënyra të ndry-shme ndaj këtyre faktorëve. Po ashtu është vënë re edhe roli i faktorëve predispozues siç janë mosha,artritet, së-mundjet e veshkave,çrregullimet hormonale,diabeti dhe hipotiroidizmi.(5,6)
Sëmundjet e qafës dhe shpinësFaktorë risku që lidhen me ushtrimin e profesionit të
dentistit janë përkulja e vazhduar, e zgjatur e qafës dhe e shpatullave,mungesa e mbështetjes së gjymtyrëve të sipërme dhe pamundsia për të ndërprerë punën.Personeli dentar zakonisht punon në pozicione të vështira për disa arsye:për të patur fushëpamje më të mirë

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 145
në brëndësi të kavitetit oral,për të realizuar një pozicion më konfort për pacientin,për të kordinuar pozicionet me asistentët si edhe për të marrë dhe lëshuar instrumentat dhe pajisjet gjatë punës.(11)
Çrregullimet me dhimbje miofacialeAnkesat:dhimbje dhe ngurtësim të muskujve të qafës,
të shpatullave dhe të krahut,pika të dhimbshme në prekje ose gjatë masazhimit,reduktim të lëvizjeve.
Shkaqet kryesore: tejzgjatjet dhe tendosjet e muskujve të qafës ose shpatullave.
Spondiloza CervikaleAnkesat:dhimbje të vazhdueshme dhe ngurtësim
i qafës dhe shpatullave,dhimbje koke,dhimbje e krahut ose dorës,mpirje, ndjesi shpimi, ngathtësi në lëvizje.
Shkaqet kryesore: degjenerim i diskut spinal nga mosha që çon në komprimim të nervit dhe në dëmtim të palcës së kurrizit, artrite.
Sindroma e shpërhapjes torakaleAnkesat: dhimbje në shpatulla, krahë dhe duar
(të treja),mpirje dhe ngrirje të gishtave,dobësi të muskujve,krahë dhe duar të ftohta.
Shkaqet kryesore:komprimimi i nervave dhe enëve të gjakut,trauma.
Tendinitet rrotatore të artikulacioneve Ankesat:dhimbje dhe mpirje në lëvizjet para dhe
prapa të shpatullave,dobësi muskulare.Shkaqet kryesore: edema dhe dëmtime të indeve në
aparatin e artikulacionit, posturë jo normale e shpatullave .(7)
Çrregullimet e dorës dhe të kyçitFaktorë risku që lidhen me dentistrinë janë lëvizjet
përsëritëse të dorës dhe kyçit të dorës,pozicionet anormale të kyçit,stresi mekanik i nervave digitale
sidomos gjatë mbajtjes së instrumentave të mprehtë,punë të sforcuara,përdorimi për një kohë të gjatë i instrumentave vibruese,pushim i pamjaftueshëm gjatë punës. Stresi në kyç dhe në dorë mund të jetë direkt i lidhur me dizajnin e pajisjeve që mjeku mban në dorë. Veglat e punës me vibrim njihen si dëmtuese të nervit median të kyçit të dorës. Mbajtja e instrumentit me forcë është një nga gabimet më të shpeshta që bëjnë mjekët.
Tendosinoviti DeQuervainAnkesat:dhimbje në gishtin e madh dhe në zonën
e kyçit gjatë pastrimit të gurëzave, gjatë manipulimeve rotative në ekstraksione,enjtje në zonën e gishtit të madh, reduktim të lëvizjeve të gishtit të madh të shoqëruara me dhimbje.
Shkaqet kryesore: enjtja e indeve sinoviale, trashja e tendineve, trauma ose rrotullime që përsëriten gjatë lëvizjeve të dorës/kyçit .
Tendosinoviti i gishtit tregues Ankesat:dhimbje gjatë lëvizjeve që shkaktojnë tension
për tendinet,nxehtësi,enjtje, rigiditet dhe tensionim i tendineve që ndihet me prekje.
Shkaqet: lëvizje të forta shtrënguese të vazhdueshme.
Sindroma e Tunelit KarpalAnkesat:mpirje të dorës ose gishtit,dhimbje, rrën-
qethje, djegie, ngathtësi,dobësi e deri në atrofi të muskujve përkatës. Simptomat shpesh përkeqsohen me shtimin e aktivitetit.Dhimbjet dhe mpirjet zgjojnë dentistin natën dhe kalojnë vetëm pas disa lëvizjeve ose masazhit (konsiderohet sipmtoma kyç për diag-nozën).
Shkaqet kryesore: shtypja e nervit median në kyç gjatë traumave, lëvizjeve të forta, lëvizjeve përsëritëse që devijojnë nga pozicionet normale.

Revista Stomatologjike Shqiptare146
Sindroma GuyonAnkesat:dhimbje, dobësi, mpirje, dridhje, djegie
në gishtin e vogël dhe pjesërisht e gishtit të unazës. Simptomat përkeqësohen gjatë natës ose herët në mëngjes.
Shkaqet kryesore:shtypja e nervit ulnar në kanalin Guyon në pëllëmbën e dorës, lëvizje të përsëritura të forta të kyçit; presion i shtuar dhe i vazhduar në pëllëmbën e dorës.
Sindroma e Tunelit KubitalAnkesat:dhimbje,mpirje,dridhje dhe pandjeshmëri në
prekje në gishtin e vogël dhe atë të unazës anash dhe në kurrizin e dorës,humbje kontrolli në lëvizjet fi ne,reduktim i forcës shtrënguese.
Shkaqet kryesore:komprimimi i nervit ulnar në bërryl gjatë traumave ose punës me orë të zgjatura, komprimim gjatë fl eksionit të bërrylit .
Sindroma e dridhjes së dorës-krahut Ankesat: pandjeshmëri dhe zbardhje të përsëritura
të gishtave dhe dorës,reduktim i shkathtësisë, i forcës shtrënguese dhe ndjeshmërisë, rritje e ndjeshmërisë ndaj të ftohtit.

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 147
Shkaqet kryesore: vibracionet dëmtojnë nervat, duke çuar në reduktim të qarkullimit të gjakut dhe paksim të oksigjenit në indet përreth.
Fenomeni Raynaud Ankesat:spazma të përsëritura të enëve të gjakut të
majave të gishtave duke shkaktuar zbardhje, mpirje dhe dhimbje, rritje e ndjeshmërisë ndaj temperaturave të ulta.
Shkaqet kryesore: sindroma e tunelit karpal, sëmundje të indit lidhor, vibracionet e përsëritura ose përdorimi i instrumentave dhe pajisjeve vibruese.(8,9)
Çrregullimet e shpinësFaktore risku që lidhen me stomatologjinë janë
kryesisht pozicione pune të vështira.
Hernia e diskut të kolonës vertebraleAnkesat: mpirje e kurrizit dhe këmbës,dhimbje,
dobësi.Simptomat përkeqësohen gjatë kollitjes,teshtitjes,uljes,ngarjes së makinës,përkuljes përpara.
Shkaqet kryesore: ënjtje ose fragmentim i diskut intervertebral në kanalin spinal duke kompresuar dhe irrituar nervat spinale, lëvizje të vështira pa çlodhjen e duhur.
Dhimbja e fundshpinësAnkesat: dhimbje,ngrirje në pjesën e poshtme të
kurrizit dhe indeve përreth.Diskomforti i pjesës së poshtme të shpinës, që lidhet më së shumti me posturën
e keqe të mjekut. Një faktor shtesë, që kontribuon në dhimbjen e pjesës së poshtme të shpinës është edhe masa e madhe trupore, pra mbipesha. Është shumë e rëndësishme që mjeku të ketë tonifi kim të mirë abdominal pasi kjo ndihmon në mbështetje trupore më komode dhe më të shëndetshme për pjesën e poshtme të shpinës.
Shkaqet kryesore: pozicione të vështira dhe lëvizje të sforcuara, dridhjet në përgjithësi, pamundësia ose kufi zimi në kryerjen e disa lëvizjeve të trupit.Kompromisi për të mbajtur pozicion të tërhequr të shpinës bëhet me qëllim për të përmirësuar fushëpamjen ose sepse distanca nga pacienti është e madhe. Qëndrimi ulur e rrit presionin intradiskal lumbar, ndërsa qëndrimi në këmbë e redukton shumë këtë presion. Për këtë arsye, qëndrimi në këmbë mund të shërbejë si një pushim i shkurtër, dhe ndihmon për të parandaluar apo për të lehtësuar dhimbjen e fundit të shpinës.
Nervi ShiatikAnkesat:dhimbje që fi llojnë në mes dhe përhapen
përgjatë kofshës së këmbës,dobësi, mpirje dhe dridhje e këmbës.
Shkaqet: nje prolaps i diskut intervertebal shtyp nervin shiatik, i cili përkeqësohet gjatë qëndrimeve të zgjatura ulur ose pozicioneve të vështira .(7)
Trajtimi dhe menaxhimi i çrregullimeve muskulo-skeletale (ÇMS)Origjina e ÇMS është komplekse dhe me shumë

Revista Stomatologjike Shqiptare148
1. Murphy DC, (1998).Ergonomics and the Dental Care Work-er. American Public Health Association, United Book Press, Washington, DC;.129-143,143-191
2. Williamson D, (2002).Musculoskeletal disorders: their symp-toms and possible causes. Smartpractice;PPT.
3. Xhemnica L,(2006) .Çrregullimet muskulo-skeletale të den-tistëve në realcion me pozicionet e punës ,Revista Stoma-tologjike ,Vol .4 Nr.4,295-299.
4. Rucker, et al., (2002). Ergonomic risk factors associated with clinical dentistry. Journal of the California Dental Associa-tion, Feb.;30(2):139-148.
5. Burke FJ, Main JR, Freeman R,(1997). The practice of dentist-ry: an assessment of reasons for premature retirement. Br Dent J.;182:250-254.
6. Shugars, et al., (1987).Musculoskeletal pain among general dentists, General Dentistry,; 535:272-276.
REFERENCA
7. Marshall, et al., (1997).Musculoskeletal symptoms in New South Wales dentists, Australian Dental Journal; 42:(4):240-6.
8. Anton, et al., (2002).Prevalence of Musculoskeletal Symp-toms and Carpal Tunnel Syndrome Among Dental Hygien-ists, American Journal of Industrial Medicine; 42:248-257.
9. Hamann, et al., (2001).Prevalence of carpal tunnel syndrome and median mononeuropathy among dentists, Journal of the American Dental Association Feb; 132(2): 163-70.
10. Alexopoulos EC, Stathi IC, Charizani F,(2004) Prevalence of musculoskeletal disorders in dentists, BMC Musculoskeletal Disorders 5:16DOI: 10.1186/1471-2474-5-16.
11. Rawi NH , Khatib HE, Rajoub L,(2016) Work-related Muscu-loskeletal Pain among Diff erent Dental Specialists in United Arab Emirates. The Journal of Contemporary Dental Prac-tice, August ;17(8):639-644.
simptoma. Është e rëndësishme që diagnoza të përcaktohet nga një mjek specialist i sëmundjeve profesionale. Vet-diagnostikimi nuk rekomandohet. Testet diagnostikuese përfshijnë ekzaminime fi zike provokuese dhe elektromiografi . Trajtimi mund të fi llojë që nga medikamentet e thjeshta të tipit analgjezik deri në ndërhyrje kirurgjikale si edhe adaptime ergonomike në punë dhe shtëpi .
Konkluzione dhe rekomandime Studimet tregojnë që një rol të rëndësishëm në
parandalimin e çrregullimeve muskuloskeletale të den-tistëve luan promovimi i pozicioneve të shëndetshme të punës,alterimi i punës herë ulur e herë në këmbë.Gjatë punës duhet të aplikohen disa pauza të vogla dhe të shmangen seancat e zgjatura me një pacient.Kryesore për ruajtjen e një pozicioni të shëndetshëm gjatë punës janë mbështetja e përshtatshme lumbare
në karriken e dentistit, pozicionimi i duhur i pacientit, dhe pozicionimi i duhur i asistentit dentar. Vendosja e veglave rekomandohet në një rreze 40 cm nga person-eli.Postura e gabuar gjatë punës si psh ulja,rrotullimi, animi i qafës për një kohë të gjatë dhe afrimi i shpatul-lës janë gabimet më të shpeshta që bën një dentist në përpjekje për të patur një fushpamje më të qartë në kavitetin oral. Rekomandohen lupat dentare të cilat sig-urojnë një fushë operative të zmadhuar dhe ndihmo-jnë për përmirësimin e fushpamjes gjatë punës. Gjatë protokolleve të trajtimit të pacientëve për preparimin e kurorave dhe të urave të cilat kërkojnë aplikimin e një force të zgjatur mbi ekstremitetet e sipërme, duhet të planifi kohen pushime të shkurtra herë pas here. Kjo përfshin shtriqjen ose shplodhjen e pjesëve të stresu-ara dhe të kontraktuara të trupit për një periudhë të shkurtër prej 8-10 sekondash.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 149
Summary The profession of dentist comprises a number of stressful elements due to specifi c job posture exposure for a long period of time, constant repeatedly motions in the same position, tense hand and arm muscles during procedures, vibrating equipments used in everyday working practice.Aim of the study: to inform the community of dentists on professional-related disorders and the ways of preventing, diagnosing and treating them.Material and method: literature addressing the major musculoskeletal disorders in dentists was selected. The prevalence of these disorders was observed through data literature fi ndings, clinical specifi cations, etiology, prevention protocols, diagnosis and management.Conclusions: studies show that the crucial role in musculoskeletal disorders prevention in dentists, is the promotion of healthy working postures, alteration of work posture during procedures, and avoiding of prolonged sessions in a single patient.
KEYWORDS:
musculo
skeletal
disorders,
dentist,
working
posture.
Rudina Berani DMD, Prof. Rozarka Budina
Musculo skeletal disorders in dentists
Faculty of Dental Medicine, University of Medicine, Tirana
Introduction Musculo-sceletal disorders are a group of pathological
conditions involving nerves, tendons, muscles and intervertebral discs as retaining structures. The profession of dentist includes a number of stressful elements due to specifi c job posture for a long period of time, continously repetitive movements in the same position, hand and arm exhaustion, vibrating equipments used in everyday dental practice, etc. One of the most uncomfortable posture of head-neck region, results to be the one while we try to improve the visibility during the clinical interventions.This causes cervical discomfort that can worsens by growth of pressure in cervical muscles, and the dentist should continue working with the patients while is in such pain.
Prevalence of the symptomsThe most prevalent symptoms in dentists include
neck, shoulder, elbow, wrist and hand, back and leg pain and discmofort.A survey on Nebraska dentists found that 29% of them suffer symptoms of pain, 25% neuropathic, 15% numbness, 17% pinching, these symptoms were found mainly in the region of the neck and upper extremities. The main region suffering of these symptoms as a result of the work procedures, equipments or posture, was the hand (56% of cases), followed by the neck (46% of cases), thumb (30% of cases), and the index finger (26% of cases). Dentists’ most common complain andhealth issues, result to be about neck, shoulder, and
lower part of the spine.These problems are much disturbing and interfere with their everyday life and activities. (1,2,3)
Data collected from the polish and norwegian dentist suggests that neck and lumbo-sacral pain seams to be in the most large extent of all symptoms.Compared to their male colleagues,female dentistsare statistically observed to complain more about musculo-sceletal symptoms.
Studies in the USA indicate a prevalence of back pain in dentists one in two, while in common population this ratio is one in seven. In Denmark, 60% out of 432 dentists in total, experienced neck and back pain even while applying sitting work techniques.
A study categorising body inclination in Japan,dentists body postures were grouped into three most common types. The most common posture was the bending forward and right position. This study concludes that body posture of dentists in their daily work, is the basis and continuing cause of health concerns related to profession.
A study in Germany found that psycho-physiological parameters were related to equipment design and use of space in the workplace. Repeated actions during procedures (ex. scaling and root planing) and inappropriate positions while trying to have access to the oral cavity, were identifi ed as contributing factors to musculoskeletal concerns. There are also other studies by german ergonomist, which analyze factors that infl uence and determine the body posture.
EMG (electromyogram) data during routine

Albanian Stomatological Journal150
procedures in dentistry, mainly showed that the cervical and lumbar spinal muscles were inconstantly stressed. Neck muscles were also much stressed. Upper extremities risk factors in dental practice include, thumb and wrist forced positions, rotative tightening repeated actions of carpal and wrist region, vibrating equipments, poor design of working equipments in daily practice. Duration (working days per week, years of work) and the intensity of exposure to these factors are the most important aspects of these ergonomic stress elements.Spine ergonomic stress elements include a static posture combined with a spine inclination, standing in this same position during 2/3 of dental treatment time which is about an hour. If lumbal segment of the body stands straight and not fl exed in extension or rotation, than the spine can cope better the body weight.Upper spine pain decline sharply when 60-79% of the working time is sitting. When dentists bend or rotate to have a better intervention view, posture is often compromised.(4,10)
Classifi cation of MSD’s Neck and shoulder disorders: Myofascial Pain
Disorder, Cervical Spondylolysis, Thoracic Outlet Syndrome, Rotator Cuff Tendinitis / Tears.
Hand and Wrist Disorders: DeQuervain’s Disease, Trigger Finger, Carpal Tunnel Syndrome, Guyon’s Syndrome, Cubital Tunnel Syndrome, Hand-Arm Vibration Syndrome, Raynaud’s Phenomenon.
The spinal disorders: Spinal Discs Hernia, Lumbar Pain, Sciatica Nerve Disorders.
Common signs and symptoms are slow limited motions, deformations, fatigue, loss of muscle
function, pain, numbness, tingling, burning, cramps, rigidity.
MSD’s factors related to the profession Routine actions as wrist powerful strong motions,
repetitive motions (scaling and root planing, root canal preparation, polishing etc), fi xed or unusual posture,vibrating equipment and instruments, frequent and diffi cult movements, working with small instruments for long periods, the force applied to hold instruments.
A risk factor is not always the cause of disorders. The level of risk depends on the length of time the person is exposed to these conditions, how often is exposed, exposure level. Usually is the combination of several risk factors (compared to a single factor) which causes or contributes to a MSD.It is recommended that the focus should not only be in the workplace. Risk factors may also appear in other non professional activities.Not every person exposed to one or more risk factors suffers a MSD. People react differently to these factors.It is now noticed the role of predisposing factors such as age, arthritis, kidney disease, hormonal disorders, diabetes and hypothyroidism.(5,6)
Neck and back disordersRisk factors related to dentistry profession are the static
fl exion protracted neck and shoulder, the lack of support of the upper limbs, impossibility to stop working.Dental staff positions are usually diffi cult working positions for better observe intraoral cavity,to achieve a comfort position for the patient,to coordinate with assistants

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 151
positions and to take and drop instruments and devices while working.(11)
Myofascial Pain Disorder
Complaints: pain and muscle rigidity in the neck, shoulder and arm, painful contact areas during massage, slow decreasing motions.
Causes: excessive stretch of the neck or shoulder muscles.
Cervical SpondylosisComplaints: persistent pain and rigidity of the neck
and shoulders, headaches, arm or hand pain, numbness, tingling, slow decreasing motions.
Causes: spinal disc degeneration because of age, leading to nerve compression and spinal cord damage, arthritis.
Thoracic Outlet SyndromeComplaints: pain in the shoulder, arm and hand (the
three of them), fi ngers numbness and rigidity, muscle weakness, cold arm and hands.
Causes: compression of nerves and blood vessels, trauma.
Rotator Cuff Tendinitis / TearsComplaints: pain and numbness in the back and forth
movements of the shoulders, muscular weakness.Causes: edema and bone articulation tissue
damage,abnormal shoulder posture.(7)
Hand and Wrist DisordersRisk factors related to dentistry are hand and wrist
repetitive motions,abnormal wrist positions, mechanical stress of digital nervesespecially while holding sharp instruments, diffi cultinterventions, long periods usage of vibrating instrument, insuffi cient breaks during working hours.
Hand and wrist stress can be directly related to the design of the equipment which the doctor holds during procedures. Vibrating equipments are recognized as main cause of wrist nerve damaging. Intensive strongly holding of the equpment is also one of the most common mistakes that doctors make.
DeQuervain’s DiseaseComplaints: thumb and wrist pain while scaling
and root planing, pain in rotative motions during teeth extractions, thumb swelling, thumb motion reduction associated with pain.
Causes: swelling of synovial tissue, tendons thickness, trauma or repeated rotative actions during hand/wrist motions.
Trigger FingerComplaints: pain during motionswhich cause tension
on tendons, heat, swelling, rigidity of the tendons.Causes: continous strong clutch motions.
Carpal Tunnel SyndromeComplaints: hand or fi nger numbness, pain, burning,
motion deceleration, weakness and evenatrophy of relevant muscle. Symptoms often worsen with the increasing of the activity.The pain and numbness that wakes up the patient during the night, and which are reliefed soon after some massage, are considered as key symptoms for diagnosis.

Albanian Stomatological Journal152
Causes:wrist median nerve pressure during trauma, sharp strong motions, repetitive movements divertingfrom wrists neutral positions.
Guyon’s SyndromeComplaints:pain, weakness, numbness, tremors,
burning of small and partly ring fi nger. Symptoms aggravates during the night or early in the morning.
Causes: The ulnar nerve compression at Guyon canal in the palm, strong repetitive motion of the wrist,increased pressure in the palm.
Cubital Tunnel SyndromeComplaints: pain, numbness, tremor and insensitivity
of the little and ring fi nger, on the back dorsal side of the hand, a loss of control in fi ne motions, reduction of the strenous force.
Causes: compression of the ulnar nerve at the elbow level during trauma or long working hours, during elbow fl exion.
Hand-Arm Vibration Syndrome
Complaints: insensitivity and repeated paling ofhand

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 153
and fi ngers, motion deceleration, decreased sensitivity but increased sensitivity to cold.
Causes: The vibrations can damage nerves, resulting in blood fl ow reduction and oxygen depletions in the surrounding tissues.
Raynaud’s Phenomenon
Complaints: repeated spasms of blood vessels causing pale fi ngertips, numbness and pain, increased susceptibility to cold.
Causes: Carpal tunnel syndrome, connective tissue diseases, repeated vibration orcontinous usage of vibrating equipments.(8,9)
Spine disorders
Main risk factor related to dentistry is diffi cult working posture.
Herniated Spinal Disc
Complaints: Spine and leg numbness, gout, pain, weakness. Worsens during coughing, sneezing, sitting, driving, bending forward.
Causes: swelling or fragmentation of intervertebral disc in the spinal canal by pressing and irritating spinal nerves, severe movement without adequate relaxation.
Lower Back PainComplaints: pain, freezing at the bottom of the spine
and surrounding tissues. Discomfort of the lower part of the back, related mostly with bad posture of the physician. An additional factor contributing to the pain of the lower back part is the body weight, it means, overweight. It is very important that the doctor have good abdominal tonifi cation in order to support the bottom of the back.
Causes: diffi cult positions and strenuous movements, tremors throughout the body, inability to perform several body movements. The compromise to keep reversed backward back, is made in order to improve visibility or because of the unconfortable distance with the patient. Sitting increases the lumbar intradiscal pressure, while standing reduces this pressure a lot. For this reason, standing can serve as a brief pause, and helps to prevent or ease the lower back pain.
SciaticaComplaints: pain radiating from the lumbar part of
the body along the thigh and leg, weakness, numbness and trembling foot.
Causes: an intervertebal prolapsed disc presses the sciatic nerve, which deteriorates during extended stays seated or diffi cult positions.(7)

Albanian Stomatological Journal154
MSD’s Treatment and ManagementMSD etiology is much complexed and with a lot
of symptoms. Thus make sure that the diagnosis is determined by a specialist. Self-diagnosis is not recommended. Diagnostic tests and examinations include physical and provocative examinations, and also an electromyography. Diagnosing and interventing right on time, is the key to successful treatment. Treatment can range from analgesics to surgical intervention, and also evaluating and adopting safe work and home ergonomics.
Conclusions and recommendations Studies show that an important role in prevention
of musculo-sceletal disorders is promoting healthy working positions, alterations of sitting and standing work style.Application of short pauses during working
hours.Prolonged sessions on one patient should be preferably avoid.Basis of maintaining a safe working position are a good lumbar support on the dentist’ chair, a proper patient positioning, and a proper positioning of dental assistant.Setting equipments within a radius of 40 cm from the assisting staff .Wrong posture while working, such as seating, rotation, tilting of the neck for a long time and a tense defl ecting shoulder are most frequent mistakes while trying to have a clearer oral cavity view.Dental magnifying glasses help to improve the sight during work procedures because they increased operational fi eld of view.During treatment for crowns and bridges preparation which require a stretched fi xed position of the upper limbs, therefore it should always be planned a short break from time to time.This involves stretching or relaxing of the stressed parts of the body for a short period of 8-10 seconds.
1. Murphy DC, (1998).Ergonomics and the Dental Care Work-er. American Public Health Association, United Book Press, Washington, DC;.129-143,143-191
2. Williamson D, (2002).Musculoskeletal disorders: their symp-toms and possible causes. Smartpractice;PPT.
3. Xhemnica L,(2006) .Çrregullimet muskulo-skeletale të den-tistëve në realcion me pozicionet e punës ,Revista Stoma-tologjike ,Vol .4 Nr.4,295-299.
4. Rucker, et al., (2002). Ergonomic risk factors associated with clinical dentistry. Journal of the California Dental Associa-tion, Feb.;30(2):139-148.
5. Burke FJ, Main JR, Freeman R,(1997). The practice of dentist-ry: an assessment of reasons for premature retirement. Br Dent J.;182:250-254.
6. Shugars, et al., (1987).Musculoskeletal pain among general dentists, General Dentistry,; 535:272-276.
REFERENCES
7. Marshall, et al., (1997).Musculoskeletal symptoms in New South Wales dentists, Australian Dental Journal; 42:(4):240-6.
8. Anton, et al., (2002).Prevalence of Musculoskeletal Symp-toms and Carpal Tunnel Syndrome Among Dental Hygien-ists, American Journal of Industrial Medicine; 42:248-257.
9. Hamann, et al., (2001).Prevalence of carpal tunnel syndrome and median mononeuropathy among dentists, Journal of the American Dental Association Feb; 132(2): 163-70.
10. Alexopoulos EC, Stathi IC, Charizani F,(2004) Prevalence of musculoskeletal disorders in dentists, BMC Musculoskeletal Disorders 5:16DOI: 10.1186/1471-2474-5-16.
11. Rawi NH , Khatib HE, Rajoub L,(2016) Work-related Muscu-loskeletal Pain among Diff erent Dental Specialists in United Arab Emirates. The Journal of Contemporary Dental Prac-tice, August ;17(8):639-644.

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 155
PermbledhjeImplantet dentare janë një alternativë gjerësisht e përdorur nëpër botë për zevendësimin e dhëmbëve që mungojnë. Osteointegrimi i sukseshëm implanteve ka çuar në përdorimin e tyre masiv.Vitet e fundit edhe në Shqipëri ka fi lluar të jetë ndër alternativat e preferuara. Planifi kimi i sukseshëm dhe ekzekutimi i kujdesshëm i proçedures kirurgjikale është shumë i rëndesishëm për të pasur një shkallë të lartë suksesi duke mos rrezikuar strukturat anatomike. E gjithë kjo mund të arrihet me anë të tomografi së së kompjuterizuar, planifi kimit të implanteve me software 3D, teknikës së prodhimit të udhëzuesit kirurgjikal, dhe kirurgjisë së asistuar me kompjuter.Ky artikull paraqet një rast klinik me një implant të vendosur me udhëzues kirurgjik dhe ngarkimin e tij të menjëhershëm.
FJALËT KYÇE:
CAD/CAM,
tomografi e
kompjuterizuar,
implant,
udhëzues
kirurgjik.
Dr. Fisnik Mekaj1, Dr. Eni Tutulaku1
Vendosje e implantit me udhëzues kirurgjik dhe ngarkimi i menjëhershëm i tij. Rast Klinik
1 Klinikë private
Implantet dentare janë një alternativë gjerësisht e përdorur nëpër botë për zevendësimin e dhëmbëve që mungojnë. Osteointegrimi isukseshëm implanteve ka çuar në përdorimin e tyre masiv.Vitet e fundit edhe në Shqipëri ka fi lluar të jetë ndër alternativat e preferuara. Komplikimet që u ndodhin zakonisht implanteve janë të shkaktuara nga keqdiagnostifi kimi, planifi kimi jo i mirë, metoda e gabuar kirurgjikale apo nga vendosja e gabuar e tyre. Shpesh këto probleme mund të anashkalohen me përdorimin e udhëzuesit kirurgjikal (surgical guide). Edhe pse ende implantet mund të vendosen në mënyre konvencionale, rezultatet klinike mund të jenë të paparashikueshme si pasojë e:vendosjes, drejtimit apo devijimit. Gjithashtu mund të jetë pak e veshtirë për të arritur rezultate protetike të kënaqshme.
Planifi kimi isukseshëm dhe ekzekutimi i kujdesshëmi proçedurës kirurgjikale është shumë i rëndësishëm për të pasur një shkallë të lartë suksesi duke mos rrezikuar strukturat anatomike.
E gjithë kjo mund të arrihet me anë të tomografi së së kompjuterizuar, planifi kimit të implanteve me software 3D, teknikës së prodhimit të udhëzuesit kirurgjikal, dhe kirurgjisë së asistuar me kompjuter.
Suksesi i implaneve dentare është drejtperdrejt i lidhur me vleresimin e pacientit dhe planifi kimin e mirë të ndërhyrjes.
Në fi llimet e implantologjisë , implantet vendoseshin aty ku gjendej sasia më e madhe e kockës pa u kujdesur shumë se ku do të vendosej apo si do të arrihej rindërtimi protetik. Edhe ndryshimet më të vogla të vendosjes së implantit karshi vendosjes ideale do të vështirësonin prodhimin e strukturës protetike. Vendosja e kujdesshme e implantit kërkohet në mënyrë që të arrihen rezultate shumë të mira estetike dhe funksionale.Meqënëse kaviteti oral ka sipërfaqe të kufi zuar, një shkallë e lartë
preçizioni është shumë e rëndësishme për rindërtimin protetik.
Udhëzuesi kirurgjik mundëson një nderhyrje kirurgjikale të parashikueshme, të sigurtë dhe minimalisht invazive. Synimi kryesor i udhëzuesit është të drejtojëfrezat kirurgjikale dhe të sigurojë vendosje të saktë të implantit sipas planifi kimit të bërë paraprakisht. Në mënyrë që transferimi i planit të trajtimit të jetë i saktë, udhëzuesi kirurgjik i prodhuar me sistemin CAD CAM ose Cerecështë një metodë shumë e mire dhe e shpejtë.
Për të pasur implante të sukseshëm duhen mbajtur parasysh 3 gjëra:
1. Implanti duhet vendosur në mënyrë që të jetë i rrethuar me kockë ose graft kockor.
2. E rëndësishme është të mos dëmtohen struktura anatomike të rendësishme si nervi alveolar inferior, membrana e Shneiderit tek sinuset maksilare apo rrënjët e dhëmbëve pranë.
3. Pozicioni i implantit duhet të jetë i përshtatshëm për strukturën e përhershme protetike.
Udhëzuesit kirurgjikëndahen në 3 tipe1. Udhëzues kirurgjikëtë mbështetur në kockë,2. Udhëzues kirurgjikë të mbështetur në mukozë,3. Udhëzues kirurgjikëtë mbështetur te dhëmbet
pranë implantit
Proçedurat e prodhimit të udhëzuesit kirurgjikal:1. Marrja e masës në mënyre dixhitale apo në
mënyrë konvencionale2. Radiografi 3D (CBCT)3. Planifi kimi virtual i implantit dhe i strukturës pro-
tetike që do të vendoset mbi të4. Planifi kimi i udhëzuesit kirurgjik5. Prerja me CAD CAM e udhëzuesit

Revista Stomatologjike Shqiptare156
Rast KlinikPacientja paraqitet me mungesë të 46 prej disa
vitesh. Hapi i parëështë vizita e pacientit dhe vlerësimi i hapsirave. Më pas merret masa në mënyre dixhitale me Omnicamnga Sirona ose merret masakonvencionale me silikon.Pacientja dërgohet për CBCT dhe me pas fillon planifi kmi virtuali implantit.
Sapo hapet software 3D bëhet vleresimi i strukturave të rëndësishme anatomike siçështe në rastin konkret nervi alveolar inferior.Ne Fig.2 nervi alveolar inferior është lehtësisht i dallueshëm me vijën e pandërprerë ngjyrë rozë. Fig.3 paraqet raportin e implantit virtual me kortikalen mandibulare dhe me nervin alveolar inferior si dhe pozicionimi i kurorës në raport me kreshten mandibulare dhe raportin e kurores me gingiven.Pasi është planifi kuar pozicioni i përshtatshëm i implantit dhe kurorës që do të vendoset mbi të ky plan ruhet dhe eksportohet si .ssi fi le në InLab CAD ose në Cerec nga ku do të fi lloje të projektohet udhëzuesi kirurgjik (Fig.4)
Shumë e rëndësishme gjatë projektimit të udhëzuesit është trashësia e sistemit të frezave. (Fig.5 dhe Fig. 6). Pasi bëhet projekti në kompjuter informacioni kalon nga InLab CAD në InLab CAM ku bëhet bluarja e tij nga pllakat transparente te PMMA të prodhuara nga Sirona (Fig.7).
Fig. 1
Fig. 5
Fig. 2
Fig. 6
Fig. 3
Fig. 7
Fig. 8Fig. 4
Pasi është prodhuar udhëzuesi kirurgjik përpara ndërhyrjes kirurgjikale bëhet një provë e stabilitetit për të evituar të papritura gjatë ndërhyrjes. Më pas vendoset në tretesirëklorexidine 0.2% ose në tretësirë betadine për të ulur sa më shumë ngarkesen bakteriale gjatëndërhyrjes.
Për ndërhyrjen përveç instrumentave të zakonshëm kirurgjik na duhet gjithashtu kiti kirurgjik i implanteve (Surgical Guide Set) dhe kiti i çelsave udhëzues (Guide Drill Key , Sleeves Fig.9).
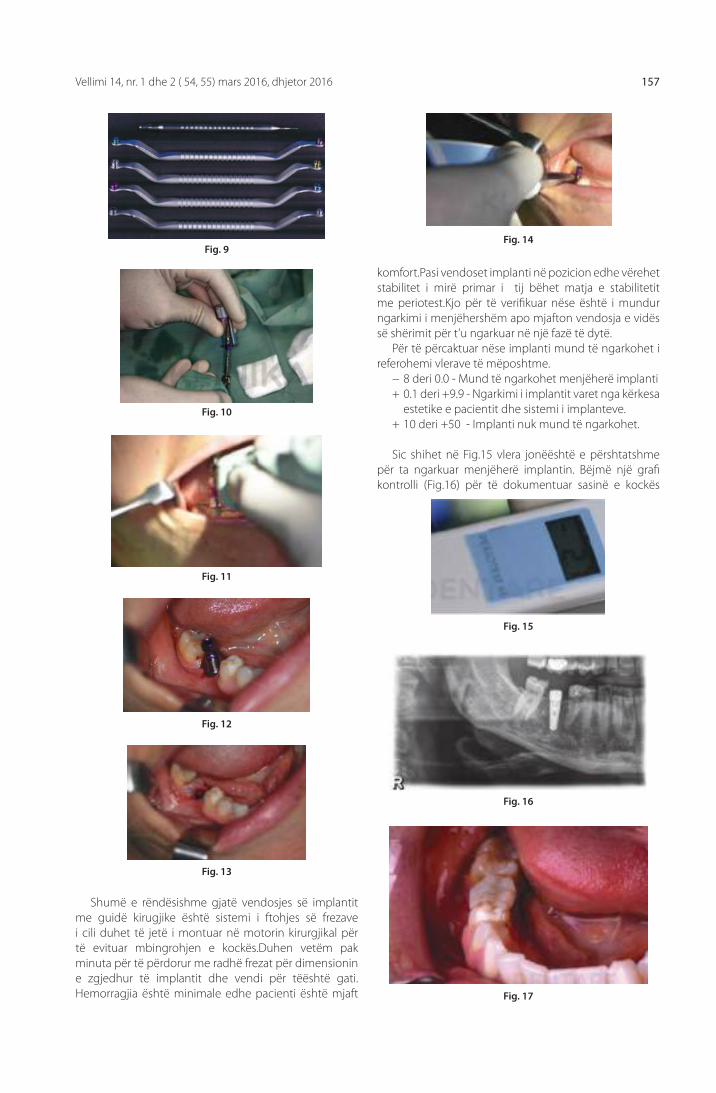
Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 157
Shumë e rëndësishme gjatë vendosjes së implantit me guidë kirugjike është sistemi i ftohjes së frezave i cili duhet të jetë i montuar në motorin kirurgjikal për të evituar mbingrohjen e kockës.Duhen vetëm pak minuta për të përdorur me radhë frezat për dimensionin e zgjedhur të implantit dhe vendi për tëështë gati.Hemorragjia është minimale edhe pacienti është mjaft
Fig. 10
Fig. 11
Fig. 12
Fig. 13
Fig. 14
Fig. 15
Fig. 16
Fig. 17
Fig. 9
komfort.Pasi vendoset implanti në pozicion edhe vërehet stabilitet i mirë primar i tij bëhet matja e stabilitetit me periotest.Kjo për të verifi kuar nëse është i mundur ngarkimi i menjëhershëm apo mjafton vendosja e vidës së shërimit për t’u ngarkuar në një fazë të dytë.
Për të përcaktuar nëse implanti mund të ngarkohet i referohemi vlerave të mëposhtme.
− 8 deri 0.0 - Mund të ngarkohet menjëherë implanti+ 0.1 deri +9.9 - Ngarkimi i implantit varet nga kërkesa
estetike e pacientit dhe sistemi i implanteve.+ 10 deri +50 - Implanti nuk mund të ngarkohet.
Sic shihet në Fig.15 vlera jonëështë e përshtatshme për ta ngarkuar menjëherë implantin. Bëjmë një grafi kontrolli (Fig.16) për të dokumentuar sasinë e kockës

Revista Stomatologjike Shqiptare158
REFERENCA
Fig. 18
rreth implantit dhe për të kontrolluar raportet e implantit me strukturat afër tij. Pasi gjithshka duket mirë vazhduam me marrjen e masës në mënyrëklasike me transfer. Në modelin e allçisë punojmë me abutmentin dhe me kurorën provizore mbi implant. Materiali i zgjedhur për kurorën në rastin tonëështë emax nga Ivoclar Vivadent.Kurora e prodhuar ngjitet me cement provizor dhe kujdesemi shumë që mos të kemi mbetje të cementit perreth koletit.Gjithashtu kurora duhet të jetë në infra okluzion për të evituar mbingarkesë të implantitgjatë osteointegrimit.
DiskutimiImplantologjia e udhëzuar me kompjuter premton
rezultate shumë të mira sidomos kur kërkesa për shpejtësi dhe estetike është e madhe. Përdorimi i software-ve kompjuterik mundëson saktësi më të madhe dhe rezultate më të parashikueshme. Vendosja virtuale e implantit bëhet në kompjuter dhe më pas plani transferohet tek pacienti me anë të udhezuesit kirurgjik i cili drejton frezimin gjatë ndërhyrjes. Aftësia për të paracaktuar pozicionin e implantit përpara kirurgjisë na jep avantazhin e saktësisë më të mirë për të prodhuar një strukturë protetike provizore dhe vendosjen e saj në të njëjtën ditë me kirurgjinë.Gjithsesi mbetet një zgjedhje e kirurgut dhe pacientit për protezizimin e
implantit brënda ditës sepse duhet një higjenë shumë e kujdesshme nga ana e pacientit, dietë ushqimore e butë dhe e lëngshme për të paktën një muaj. Pas 6 muaj gjëndja e implantit të vendosur paraqitet si nëFig.18.
1. Block M, Finger I, Castellon P, et al: Single tooth immedi-ateprovisional restoration of dental implants: Technique and early results. J Oral Maxillofac Surg 62:1131, 2004
2. Mitrani R, Phillips K: Pickup impression technique for fabricat-ing the surgical template for implant placement and provi-sional restoration. Pract Proc Aesthet Dent 16:389, 2004
3. Tsoukaki M, Kalpidis CD, Sakellari D, Tsalikis L, Mikrogiorgis G, et al. (2013) Clinical, radiographic, microbiological, and immunological outcomes of fl apped vs. fl apless dental implants: a prospective randomized controlled clinical tri-al. Clin Oral Implants Res 24: 969–976.
4. Sunitha RV, Sapthagiri E (2013) Flapless implant surgery: a 2-year follow-up study of 40 implants. Oral Surg Oral Med Oral Pathol Oral Radiol 116: e237–e243.
5. Chrcanovic BR, Albrektsson T, Wennerberg A (2014) Rea-sons for failures of oral implants. J Oral Rehabil 41: 443–476.
6. Cannizzaro G, Leone M, Consolo U, Ferri V, Esposito M (2008) Immediate functional loading of implants placed with flapless surgery versus conventional implants in partially edentulous patients: a 3-year randomized con-trolled clinical trial. Int J Oral Maxillofac Implants 23: 867–875
7. Lindeboom JA, van Wijk AJ (2010) A comparison of two implant techniques on patient-based outcome measures: a report of fl apless vs. conventional fl apped implant place-ment. Clin Oral Implants Res 21: 366–370.

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 159
AbstractDental implants have become a widely used alternative for lost tooth replacement. The successful osteointegration of implants has led to their massive use. In the last years even in Albania they have become a preferred alternative. The careful planning and the meticulous surgery is very important to have success with implants without risking to damage any anatomical structurer.All of this can be achieved with computerized tomography, 3D planning of the implants, CAD CAM production of the surgical guide and computer assisted surgery. This article evaluates a clinical case placed with a surgical guide and its immediate provisionalzation.
KEYWORDS:
Computer-
aided design/
computer-
assisted
manufacture,
computed
tomography,
implant,
surgical guide
Dr. Fisnik Mekaj1, Dr. Eni Tutulaku1
Implant Placement with Surgical Guide and Immediate Placement of the Provisional Crown. A Case Report
1 Private practice
Dental implants are a widely used alternative for the replacement of missing teeth. Their successful osteointegration has led to their massive use in today’s dentistry. Lately they are a preferred alternative even in Albania.
The complication that happen to implants usually happen because of the miss diagnose, bad planning, the wrong surgical method or their misplacement.These problems can be avoided by using a surgical guide. Even though implants can be placed well enough with the conventional method, the clinical result with the surgical guide are more predictable: placement, direction and deviation. With the conventional method also the prosthetic results later on can be more diffi cult.
The planning and the careful execution of the surgical procedure is very important to have a big success range without risking to damage any anatomical structure.
All of this can be achieved with the computerized tomography, planning the implants with 3D software, a surgical guide or computer assisted surgery.
The success of dental implants is directly linked with the evaluation of the patient and a good surgery planning.
At the beginning of implantology, the implants were placed where the bone seemed more suitable without caring how to place the prosthetics afterwards. Even the slightly change from the ideal position of the implant can make more diffi cult the production of the prosthetic rehabilitation. The careful placement of the implant is necessary to achieve the best esthetic and functional results.
Since the oral cavity is a limited area, a high degree of precision is very important for prosthetic reconstruction.
The surgical guide enables a predictable surgery, safe and minimally invasive. The main aim of the surgical guide is providing the accurate route for the drills and to assure the exact placement of the implant as the 3D planning.
In order to transfer the accuratetreatment plan, the surgical guide produced by CAD CAM or CERECsystem is a very good and quick method.
To have success with implants there are three things that should be kept in mind:
1. The implant should be surrounded by bone or bone graft.
2. It is important not to damage any important anatomical structures such as the inferior alveolar nerve, the Shneidermembrane of the maxillary sinuses or the roots of nearby teeth.
3. The implant’s position must be suitable for the permanent prosthetic structure.
The surgical guides are divided into three types:1. Bone supported surgical guide2. Mucosa supported surgical guide3. Teeth supported surgical guide
Production procedures for a guided surgery:1. Taking the measure in a digital or a conventional
manner2. 3D radiography (CBCT)3. The virtual planning of the implant and the
prosthetic structure 4. Planning of the surgical guide5. Cutting the guide with CAD CAM

Albanian Stomatological Journal160
Clinical caseThe patient presented in the clinic with tooth 46 missing
for years. The fi rst step is thepatientsvisit and spaceevaluation. Afterward the impression is taken digitally with Omnicam by Sirona or a conventional impression can be taken with silicon. The patient is sent to do the CBCT exam and afterwards starts the virtual PLANNING of the implant.
As soon as the 3D software starts is important the evaluation of anatomical structures such as the inferior alveolar nerve in this case. In Fig.2 the inferior alveolar nerve is easily recognizable with the uninterrupted pink line. Fig.3 presents therelationship of the virtual implant with the cortical bone of the mandible and inferior alveolar nerve. Also it shows the positionof the crown in relation to the mandibular crest and gum.
Once a fi tting position of the implant and crown is plannedthe data is saved and exported as a.ssi fi le in inlabCAD orCEREC where we begin to design of the guide (Fig.4)
Very important when designing the surgical guide is the thickness of the drilling system. (Fig.5 and Fig. 6). Once the project in the computer is ready we transfer the information from inlab CAD in inlabCAM wherebegins the grinding of transparent plates of PMMA produced by Sirona (Figure 7).
Fig. 1
Fig. 5
Fig. 2
Fig. 6
Fig. 3
Fig. 7
Fig. 8Fig. 4
Once produced the surgical guide is better that before surgery to test its stability in order to avoid surprises during the surgery. Afterwards the PMMA guide is placed in 0.2% chlorhexidine solution or betadine solution to minimizing bacterial load during the surgery.
For the surgery other than the usual surgical instruments we also need implants Surgical Guide Set and Guide Drill Key, Sleeves Fig.9.
During placement of the implant with a surgical

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 161
guide, the cooling system of the drilling systemis very important to be cor rect. It must be mounted on the surgical motor to avoid overheating of the bone. It only takes a few minutes to use the drills for the chooses dimension of the implant and the place for it is ready. Bleeding is minimal and the patient is very comfortable. Once the implant is placed in the planned position and
Fig. 10
Fig. 11
Fig. 12
Fig. 13
Fig. 14
Fig. 15
Fig. 16
Fig. 17
Fig. 9
we have a good primary stability we measure it with periotest. This is needed to verify if it is possible the immediate loading of the implant or we should just place the healing screw to load it at a later stage.
To determine whether the implant can be loaded we refer to the following values.
− 8 to 0.0 - Theimplantcan be loaded immediately+ 0.1 to +9.9 – Loading the implant or not depends
on the patient’s aesthetic requirements and implant system.
+ 10 to +50 - The implant cannot be loaded.
As seen in Fig.15 our value is suitable for immediately loading of the implant. We made an radiography (Fig.16) to document the amount of bone around the implant

Albanian Stomatological Journal162
REFERENCES
1. Block M, Finger I, Castellon P, et al: Single tooth immedi-ateprovisional restoration of dental implants: Technique and early results. J Oral Maxillofac Surg 62:1131, 2004
2. Mitrani R, Phillips K: Pickup impression technique for fabricat-ing the surgical template for implant placement and provi-sional restoration. Pract Proc Aesthet Dent 16:389, 2004
3. Tsoukaki M, Kalpidis CD, Sakellari D, Tsalikis L, Mikrogiorgis G, et al. (2013) Clinical, radiographic, microbiological, and immunological outcomes of fl apped vs. fl apless dental implants: a prospective randomized controlled clinical tri-al. Clin Oral Implants Res 24: 969–976.
4. Sunitha RV, Sapthagiri E (2013) Flapless implant surgery: a 2-year follow-up study of 40 implants. Oral Surg Oral Med Oral Pathol Oral Radiol 116: e237–e243.
5. Chrcanovic BR, Albrektsson T, Wennerberg A (2014) Rea-sons for failures of oral implants. J Oral Rehabil 41: 443–476.
6. Cannizzaro G, Leone M, Consolo U, Ferri V, Esposito M (2008) Immediate functional loading of implants placed with flapless surgery versus conventional implants in partially edentulous patients: a 3-year randomized con-trolled clinical trial. Int J Oral Maxillofac Implants 23: 867–875
7. Lindeboom JA, van Wijk AJ (2010) A comparison of two implant techniques on patient-based outcome measures: a report of fl apless vs. conventional fl apped implant place-ment. Clin Oral Implants Res 21: 366–370.
Fig. 18
and check implant’s relationwith theanatomical struc-tures nearby. After everything was good we proceeded with the conventional impression of the implant with transfer system. In the workmodel we prepared the abutment and the provisional crown of the implant. The material chosen for the crown in our case is Emax by IvoclarVivadent. The crown is cemented with tempo-rary cement and we took good care not to have residual cement around the neck of the implant. Also the crown should not be in full occlusion to avoid overloading dur-ing osteointegration of the implant.
DiscussionComputerguided implantology promises very good
results, especially when the demand for speed and aes-thetic is getting bigger every day. Using a computer software enables us to have greater precision and more predictable results. The virtual placement of the implant is done on the computer and then the plan is transferred to the patient through the surgical guide, which direct-sthe drills during the surgery. Theability to predetermine the position of the implant before surgery gives us the advantage of better accuracy to produce a temporary prosthetic structure and its placement on the same day as the surgery. Still it remains a choice of the surgeon and patient to make the crown for the implant within the
same day because patient should be very careful with hygiene also soft and liquid diet is advised for at least a month. After six months the situation of the implant is as shown in Fig.18.

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 163
AbstraktEtika në stomatologji ndryshon nga Etika në përgjithësi, madje Kodet ndryshojnë nga njëri vend në tjetrin si dhe brenda të njëjtit shtet. Etika është e lidhur ngushtë me ligjin, rregullat dhesistemet e jashme. Për zgjidhjen e këtyre probleme është përpiluar Kodi i Etikës në Stomatologji. Ky është një document themelor i cili rregullon dhe përcakton kushtet e ushtrimit të profesionit të stomatologut në Republikën e Shqipërisë.
FJALËT KYÇE:
Kod , etike,
stomatologji
Dr. Nikoll Deda1, Dr. Erisa Bllakaj2
Roli i etikës në Stomatologji
1President i Urdhrit të Stomatologut, 2Këshilltare e për marrëdhëniet me jashtë e Presidentit të USSH
Bashkëjetesa me Kodin e Etikës shumë herë është e vështirë dhe përbën një sfi dë të përditshme. Etika nuk bazohet tek preferencat apo ndjenjat personale, ajo është një system social i përpiluar për të vendosur korniza brenda një profesioni. Megjithatë, janë elementet si etika dhe morali që na mundësojnë një praktikë të shëndoshë për të rritur standardet e mirëqënies kolektive.
Etika në stomatologji ndryshon nga Etika në përgjithësi, madje Kodet ndryshojnë nga njëri vend në tjetrin si dhe brenda të njëjtit shtet (SHBA, Britania e Madhe, etj). Sidoqoftë, ruajnë disa tipare të përbashkëta, si për shembull: përkushtimi i mjekut stomatolog ndaj pacientit, vendosja e tij mbi interesat personale.
Etika është e lidhur ngushtë me ligjin, rregullat dhe sistemet e jashme, ndërkohë që morali është i lidhur me personalitetin, veprimin dhe mos veprimin, te mi-ren dhe te keqen. Një individ mund të ndjekë verbër-isht rregullat e përcaktuara nga etika dhe të mos jetë aspak i moralshëm, ndërkohë që, mund të jëtë shumë i moralshëm gjë që e çon në shkeljen e rregullave të Kodit.
Stomatologjia është një profesion i njohur, në të njëjtën kohë është dhe një biznes që gjeneron të ar-dhura (mjeku stomatolog vë në dispozicion njohuritë dhe aftësitë e tij për të nxjerrë të ardhura). Ka një ten-sion të dukshëm midis këtyre dy aspekteve dhe hasen vështirësi për ruajtjen e ekuilibrave midis tyre.
Disa mjekë stomatologë tundohen të minimalizo-jnë përkushtimin ndaj profesionalizmit që të rrisin të ardhurat e tyre si për shembull: me anë të reklamimit agresiv ose duke u fokusuar më tepër në proceduat
kozmetike. Nëse këto procedura ekzagjerohen mund të sjellin uljen e respektit të publikut ndaj profesionit të stomatologut. Si pasojë mjeku stomatolog do të shihet si një biznesmen i cili vendos interestat e veta mbi ato të komunitetit. Për shkak të aspektit komercial të stomatologjisë, statusi i mjekut stomatolog është duke u degraduar në disa vende të botës. Problemi gjeneron pakenaqësi dhe humbje të kredibilitetit.
Një rasti i rëndë është kur pacienti mundohet të kontestojë informacionin e dhënë nga mjeku kurues me informacionin e marrë nga një burim në internet. Disa nga procedurat e kryera zakonisht nga mjeku stomatolog, sot kryhen nga higjenisti, terapisti, asis-tenti dentar apo dhe laboranti dentar dhe sallonet e kozmetikës.
Një sjellje e tillë është në konfl ikt me parimet e Kodit të Etikës. Për zgjidhjen e këtyre probleme është përpiluar Kodi i Etikës në Stomatologji. Ky është një dokument themelor i cili rregullon dhe përcakton kushtet e ushtrimit të profesionit të stomatologut në Republikën e Shqipërisë.
Principet e Etikës
- Autonomia. Mjeku ka për detyrë të respektojë të drejtat e pacientit për konfi dencialitet dhe për lirinë e zgjedhjes.
- Mos bërja keq. Mjeku ka për detyrë të mbrojë pacientin pa e dëmtuar. Kjo mundësohet duke njohur limitet dhe aftësitë profesionale, konsul-timi me kolegë të tjerë, edukimi në vazhdim dhe angazhim i personelit të kualifi kuar.
- Ndershmëria. Mjeku stomatolog ka për detyrë

Revista Stomatologjike Shqiptare164
të trajtojë pacentin në mënyrë të drejtë. Selek-sionimi i pacientëve nuk mund të inkurajohet, përkundrazi bie ndesh me udhëzimet e kodit. Trajtimet e urgjencave, “kritika” të justifi kuara ndaj një akti operator të kryer në mënyrë jo kor-rekte, dëshmia e ekspertëve në raste të rënda neglizhimi apo abuzimi janë aspekte të tjera që nderojnë profesionin dhe rrisin besueshmërinë e pacientëve. Shpërblimi dhe sekserizmi duhen reklamuar duke qenë se dëmtojnë imazhin e një sjellie të mirë.
- Vërtetësia. Mjeku stomatolog ka për detyrë të komunikojë sinqerisht me pacientin duke i vënë në dispozicion të gjithë informacionin e nevo-jshëm që ka të bëj me integritetin e tij. Në asnjë moment nuk duhet të abuzojë me besimin e de-dikuar nga pacienti për tu paraqitur si dikush me vlera dhe tituj të tjerë përveç atyre që zotëron. Duhet të zbatojë në përputhje me parimet dhe protokollet e përcaktuara në ligj dhe çdo akt operator të jetë i regjistruar në një regjistër të posacëm / kartela. Të mos abuzojë dhe manipu-lojë tarifat e shërbimit, datat e trajtimeve dhe të mos kryejë ndërhyrje të panevojshme me qëllim përfi timi. Paisjet dhe metodat terapeutike të jenë bashkohore në përputhje me standarded e për-cakuara në protokolle.
- Bëj mirë. Mjeku stomatolog ka për detyrë të pro-movojë mirëqënien e pacientit. Të bashkëpunojë me USSH – në për të rapotruar rastet e abuzime-ve dhe neglizhencave.
Kodi i Etikës është një premtim, ai ka rol në:
1. Promovimin e marrëdhënies midis mjekut sto-matolog dhe pacientit;
2. Promovimin e sjelljes profesinoale midis mjekut stomatolog dhe ekipit mjekësor;
3. Përcakton cilat janë devijimet nga disiplina;
4. Mbron reputacionin e mjekut dhe praktikës së tij;
5. Garanton sekretin profesional;
Gjithçka e parashikuar në Kod është detyrë për tu zbatuar nga të gjithë anëtarët e USSH, për rrjed-hojë, të gjithë anëtarët e USSH kanë të drejta të barabarta. Mjeku stomatolog ka detyrë të mbrojë të drejtat thelbësore dhe prestigjit të profesionit
të tij. Mjeku stomatolog që ushtron një nga dis-iplinat/specialitet profesionale nuk duhet në asnjë moment të dëmtojë cilësinë e punës së një mjeku tjetër.
Mjeku stomatolog duhet të ekzekutojë profesionin e tij për trajtimin e pacientëve sipas normave etiko-profesionale të përcaktuara dhe të njohura nga USSH. Këto norma janë të përfshira në udhëzuesit e praktika-ve mjekësore ose traktate të njohura nga organizata, shoqëri e borde të profiliozuara shkencore.
Në marrëdhëniet ndërkolegjiale, mjeku duhet t’i trajtojë kolegët si vëllezërit e tij, ashtu si do të dëshi-ronte të trajtohej ai nga ata. Përbën shkelje disiplinore fajësimi, përgojimi ose çdo akt tjetër negativ kundrjet një kolegu në prani të pacientit, personelit ndihmës ose një pale të tretë.
Në rastin e divergjencave midis kolegëve, mjekët stomatologë duhet të përpiqen të arrijnë në mirëkup-tim, në të kundërt duhet të drejtohen pranë kryesisë së USSH për zgjidhjen e konfl ikitit sipas ligjit në fuqi. Mjeku stomatolog nuk ka të drejtë të shprehet për tra-jtimin e kryer nga një koleg tjetër, por vetëm në rastin kur shëndeti i pacientit është i rrezikuar. Nëqoftëse më shumë mjekë konsultojnë një pacient, nuk duhet të kundërshtohen në prani të pacientit apo familjarëve të tij.
Mjeku stomatolog gjatë rapotimit profesional me kolegët e specialiteteve të tjera, duhet të respektojë pavarësinë e tyre profesionale duke mos ndërhyrë në ekspertizën e tyre. Garantimi direkt apo indirekt i një akti mjekësor është i ndaluar. Çdo konsultim i kryer jashtë ambienteve zyrtare dhe të miratuara është i ndaluar.
Konkluzione
Detyra juaj si mjek stomatolog është të jeni profesionist. Nëqoftëse do ta konsideroni veten si profesionist, nëqoftëse doni të njiheni si profesionist dhe nëqoftëse do të jeni profesionist, atëherë ju duhet të silleni si i tillë. Në të kundërt rrezikoni të merrni një titull pa pasur parasysh të gjitha përgjegjësitë dhe angazhimet që sjell ai.
Si mjek stomatolog duhet të respektoni pacientin për veçoritë e tyre në nevoja dhe vlera. Vendosja e nevojave të pacientit në vend të parë, e bën mjekun stomatolog të vetdijshëm për përgjegjësitë që do

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 165
1. Dokumenti themeltar – Statuti, Kodi – Urdhri i Stomato-logut të Shqipërisë, 2016
2. Dokumenti themeltar – Statuti, Kodi – Urdhri i Mjekut të Shqipërisë,
3. Etics Handbook for Dentists – American College of Dentists, 2012
REFERENCA
4. Principles of Ethics and Code of Professional Conduct – ADA, 2016
5. Codul de Deontologie Medicala – CMDR, 2017
6. Codice di Deontologia Medica – FNOMCeO, 2014
ta shoqërojnë gjatë gjithë jetës së tij si profesionist i shëndetësisë.
Ai duhet të ketë integritet, të jetë i drejtë ndaj pacientave dhe ndaj kolegëve. Ai duhet të kërkojë perfeksionimin personal dhe si rezultat përmirësimin e standardeve brenda komunitetit të mjekëve stomatolog. Një mjek stomatolog është i përfshirë brenda rregullave dhe kodeve dhe si rrjedhojë është i detyruar t’i zbatoj ato pa dallim.
Përpjekja për tu përmirësuar si profesionist jep një kontribut të rëndësishëm në stomatologji, shoqëri dhe mbi të gjitha është në dobi të pacientëve të cilëve u shërben.
Etika është thelbësore për të qenë një mjek stomatolog. Një prirje ndaj etikës dhe sjellies së moralshme përcakton qëndrimin tuaj në shoqëri si një profesionist. Pa u bazuar në Kodin e Etikës, thjeshtë nuk mund të jeni një profesionist i vërtet.

Albanian Stomatological Journal166
AbstractCo existence with the Code of Ethic si soft en diffi cultand poses a daily challenge. Ethic sis not basedon personal preferences or feelings, it is a social system designed to set frameworks with in a profession. Ethics in dentistry diff ers from general Ethics, and Codes vary from one country to another and with in the same country. Ethics is close ly related to the law, rule sand external systems. In order to solve these problems, it is drawn up the Code of Ethics in Dentistry. Thisis a fundamental document which regulate sand defi nes the conditions of practicing dentist profession in the Republic of Albania.
KEYWORDS:
Code, ethics,
dentistry
Dr. Nikoll Deda1, Dr. Erisa Bllakaj2
The Role of Ethics in Dentistry
1President of the Albanian Order of Dentists, 2Consultant for Foreign Aff airs of the President of the Albanian OD
Coexistence with the Code of Ethics is often difficult and poses a daily challenge. Ethics is not based on personal preferences or feelings, it is a social system designed to set frameworks within a profession. However, there are elements such as ethics and morality that allows us a sound practice in order to increase the standards of collective welfare.
Ethics in dentistry differs from general Ethics, and Codes vary from one country to another and within the same country (in the USA, Great Britain, etc.). Nevertheless, they maintain some common features, such as, for example: the commitment of the dentist to patient, putting him above personal interests.
Ethics is closely related to the law, rules and ex-ternal systems, while moral is associated with per-sonality, acting and not-acting, good and evil. An individual can blindly follow rules set by ethics and not be moral at all; meanwhile, he can be a very moral man, which leads to violation of provisions of the Code.
Dentistry is a well-known profession, at the same time, it is a business that generates revenues (a dentist makes available his knowledge and skills in order to obtain revenues). There is an obvious ten-sion between these two aspects and difficulties are encountered in maintaining the balance between them.
Some dentists are tempted to minimize com-mitment to professionalism in order to increase
their revenues, such as for example: by aggressive advertising or focusing more on cosmetic proce-dures. If these procedures are exaggerated, they may trigger the reduction of public respect for the profession of dentist. Consequently, the den-tist will be seen as a businessman who puts his interests above those of the community. Due to the commercial aspect of dentistry, the statute of the dentist is being degraded in some countries of the world. The problem generates resentment and loss of credibility.
A severe case is when the patient tries to challenge the information provided by the curing doctor with the information obtained from an internet source. Some of the usual procedures performed by the den-tist nowadays are performed by the hygienist, thera-pist, or dental assistant and dental technician.
Such behavior is in confl ict with the principles of the Code of Ethics. In order to solve these problems, it is drawn up the Code of Ethics in Dentistry. This is a fundamental document which regulates and defi nes the conditions of practicing dentist profession in the Republic of Albania.
Principles of Ethics
- Autonomy. The doctor has a duty to respect the patient’s rights to confi dentiality and freedom of choice.
- No wrongdoing. The doctor has a duty to pro-tect the patient without injuring him. This is

Volume 14, no. 1 and 2 (54, 55) March 2016, December 2016 167
made possible by recognizing professional limits and skills, consulting with colleagues, continuing education and commitment of qualifi ed person-nel.
- Honesty. The Dentist has a duty to treat the patient fairly. Selection of patients cannot be encouraged; on the contrary, it does not com-ply with the guidelines of the code. Treatment of emergencies, justifi ed “criticism” against an operational act performed incorrectly, expert testimony in cases of serious negligence or abuses are other aspects that honor the profes-sion and increase the reliability of the patients. Compensation and improper mediation should be advertised as damage to the image of good conduct.
- Truthfulness. The Dentist has a duty to com-municate honestly with the patient by making available all the necessary information related to his integrity. At no time he should abuse with the committed trust of the patient so as to ap-pear as someone with values and titles other than those that he is awarded. He should apply in accordance with the principles and protocols stipulated in the law and every operational act should be registered in a special register/fi le. He should neither abuse, nor manipulate ser-vice fees, dates of treatment and he should not carry out unnecessary interventions for profi t purposes. Equipment and therapeutic methods should be modern and in accordance with the standards determined in protocols.
- Do well. The dentist has a duty to promote the welfare of the patient. To cooperate with the Al-banian Order of Dentists in order to report cases of abuse and neglect.
The Code of Ethics is a promise, it plays a role in:
1. Promotion of the relationship between the den-tist and the patient;
2. Promotion of professional behavior between the dentist and the medical team;
3. Determines the deviations from discipline;
4. Defends the reputation of the doctor and his practice;
5. Guarantees professional secrecy;
Everything provided in the Code is a duty to be applied by all members of the Albanian Order of Dentists, therefore, all the members of the AOD have equal rights. A dentist has a duty to protect the funda-mental rights and prestige of his profession. A dentist who practices one of the disciplines/professional spe-cialties at no moment should harm the quality of the work of another doctor.
A dentist must execute his profession in order to treat patients according to the ethical-professional norms defi ned and recognized by the AOD. These norms are included in the guidelines of medical prac-tices or treaties recognized by scientifi c profi le organi-zations, associations and boards.
Intercollegiate relations, the doctor should treat colleagues like his brothers, the way he would like to be treated by them. Blaming, slandering or any other negative act against a colleague in the presence of the patient, support staff or a third party constitutes disciplinary breach.
In case of divergences between colleagues, den-tists should try to reach an understanding; on the contrary they should address the management board of the OD in order to resolve the confl ict under ap-plicable law. The Dentist has no right to express about the treatment performed by a colleague, except the case when the patient’s health is endangered. If sev-eral doctors consult a patient, they should not be objected in the presence of the patient or his family members.
A dentist, during the professional reporting with colleagues of other specialties should respect their professional independence without interfering in their expertise. Direct or indirect provision of a medi-cal act is prohibited. Any consultation carried out and approved outside offi cial and approved premises is prohibited.
Conclusions
Your duty as a dentist is to be professional. If you consider yourself as a professional, if you want to be recognized as a professional and if you are professional, then you must behave as such. Otherwise you risk to getting a title without considering all the responsibilities and the commitments it entails.

Albanian Stomatological Journal168
1. Dokumenti themeltar – Statuti, Kodi – Urdhri i Stomato-logut të Shqipërisë, 2016
2. Dokumenti themeltar – Statuti, Kodi – Urdhri i Mjekut të Shqipërisë,
3. Etics Handbook for Dentists – American College of Dentists, 2012
REFERENCES
4. Principles of Ethics and Code of Professional Conduct – ADA, 2016
5. Codul de Deontologie Medicala – CMDR, 2017
6. Codice di Deontologia Medica – FNOMCeO, 2014
As a dentist you must respect the patient for their features in needs and values. Placing the needs of the patient in the fi rst place makes the dentist aware of the responsibilities that will accompany him all his life as a health professional.
He must have integrity, be fair to the patients and to colleagues. He must seek personal perfection and, as a result, improvement of standards within the community of dentist. A dentist is involved within the
rules and codes and is therefore obliged to implement them indiscriminately.
The eff ort to improve as a professional gives an important contribution to dentistry, society and above all it is for the benefi t of patients it serves.
Ethics is essential to being a dentist. A trend towards ethics and moral behavior determines your position in society as a professional. If you do not rely on the Code of Ethics, you simply cannot be a true professional.

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 169

Revista Stomatologjike Shqiptare170
Prof Dr Dhori Pojani lindi ne Korce ne 10 mars 1931, kreu ne qytetin e lindjes shkollen 7 vjecare e me pas Shkollen e Mesme Mjekesore ne Tirane. Ne vitet 1951 – 1957 diplomohet shkelqyeshem ne Fakultetin e Mjekesise se Sofj es (Bullgari), si Mjek Stomatolog dhe specializohet prane Prof Davidov, kirurg maksilofacial, prane po ketij Fakulteti ne Kirurgji Stomatologjike.
PROF. DR. DHORI POJANI
Shqiperine qe nxjerr per te paren here kuadrot e saj te larte, harton programet dhe shkruan disa nga tekstet e para mesimore te studenteve stomatologe.
Ne vitet 1968 – 1969, specializohet ne Kilniken Universitare te Kirurgjise Maksilofaciale, Bukuresht, Rumani, nen kujdesin e Prof Dr Valerian Popesku; per Defektet e Lindura te Buzes dhe Qiellzes dhe
NEKROLOGJI
Pas studimeve punon ne vende dhe pozicione te ndryshme derisa ne 1959 hapet per te paren here Fakulteti i Mjekesise ne Universitetin e Tiranes. Prof Dr Dhori eshte themelues dhe organizator i Deges se Stomatologjise ne Fakultetin e Mjekesise. Punon si pedagog dhe drejtues i kesaj Dege. Ne
Ankilozat e ATM, me program nga OBSH (OMS).Vitet ne vijim jane per te dashurin Doktor
Dhori dhe Profesorin e palodhur, vite te realizimit te nje aktiviteti te gjere klinik kirurgjikal, themelimit te Sherbimit Spitalor te Kirurgjise Orale e Maksilofaciale Shqipetare, te pandare

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 171
nga angazh“imi i panderprere dhe i perkushtuar arsimor dhe shkencor. Ne 29. 10. 1976 Presidiumi i Kuvendit Popullor i jep Urdherin “NAIM FRASHERI” te klasit te dyte (dekret Nr 5481).
Mbron Doktoraturen me 04. 07. 1987 dhe i akordohet (vendim Nr.157 i KLA) Grada Shkencore “DOKTOR I SHKENCAVE”. Me tej, ne 09. 07. 1988, si rezultat i punes se tij ne aresim dhe zhvillimin e Shkencave Mjekesore, fi ton Titullin Shkencor “PROFESOR” (vendim Nr.178 i KLA).
Doli ne pension ne 1993, por vazhdoi te punoje, te shkruaje, te ndjeke dhe promovoje gjenerata me te reja mjekesh e studentesh; te jete prane me te rinjve ne specialitetin e KOMF, apo te udheheqe punimet e disertacionet e tyre doktorale deri ne ditet e fundit te jetes.
Zgjidhet Anetar Nderi i Shoqates Stomatologjike Shqipetare, ne tetor 2007 dhe po ne ate vit zgjidhet Anetar Nderi i Shoqates te Kirurgeve Orale dhe Maksilofaciale te Kosoves.
Breza te shumte te mjekeve e njohin Profesor Dhorin per devocionin ne punen aresimore shkencore me studentet stomatologe, kualifi kimin pasuniversitar ne kurset e plota te Kirurgjise Orale dhe Maksilofaciale dhe krijimin e degeve te ketij sherbimi ne rrethe te tjera te vendit.
Ne aktivitetin e tij klinik eshte iniciues i aplikimit te metodave bashkekohore per gjithe periudhen ne te cilen ai punoi. Ne aktivitetin e tij shkencor numerohen me shume se 60 punime shkencore (artikuj, referate, tekste mesimore e specializuese kirurgjikale).
Me ikjen e tij familja humbi njeriun me te dashur te saj: komuniteti intelektualin e afte e te pakursyer, krijues dhe gjithmone prane njerezve; ata qe e deshen nje shok dhe mik te paharruar.
Ne diten e ndarjes se Prof Dhorit nga jeta, Rektori i Universiteti Mjekesor, Prof Dr Arben Gjata shkroi: Po ikin nje nga nje baballaret e Mjekesise Shqiptare, ashtu të heshtur e madheshtore, sic kane punuar e jane perpjekur ne të gjalle, pasi lisat madheshtore nuk kane nevoje per makjazh qe të duken. RIP Prof Dhori Pojani.
Revista Stomatologjike Shqiptare172
Çerçiz Mingomataj lindi ne Vlore me
07.05.1937. Shkollen 7 vjeçare, shkollen e mesme
dhe Politeknikun Mjekesor e kreu ne Tirane me
rezultate maksimale. Pasi punoi per 3 vjet si
mjek, vazhdoi studimet e larta ne Gjermani dhe
ne Tirane. Ne vitin 1985, mbrojti disertacionin per
Kandidat i Shkencave Mjekesore dhe ne vitin 1995
fi toi titullin Doktor i Shkencave Mjekesore.
Ka punuar si mjek Stomatolog ne Tirane dhe
ne Skrapar, si Drejtor i Sherbimit Stomatologjik
ne Ministrine e Shendetesise. Ka qene iniciator
i themelimit te revistes “Buletini Stomatologjik”
dhe Kryeredaktor i saj. Ka qene per shume kohe
pedagog i jashtem i Fakultetit te Mjekesise
Dega Stomatologji si edhe anetar i kolegjiumit
DR. SHK. ÇERÇIZ MINGOMATAJ
te “Revista Stomatologjike Shqiptare” . Ka qene
autor dhe bashkeautor i shume teksteve, artikujve
e referimeve shkencore. Qe prej vitit 2005, ka
qene shef i Departamentit te Stomatologjise ne
Albanian University dhe, ne vitin 2008 Dekan
i Fakultetit te Shkencave Mjekesore ne Albanian
University.
Çerçizi ka patur nje aktivitet te spikatur ne jeten
politike e shoqerore te vendit. Ai ka kryer per nje
kohe te gjate detyren e Sekretarit te Pergjithshem
te Partise Republikane.
Ai u nda nga ne me 28.05.2016, per te mos u
harruar kurre, duke lene ne hidherim te thelle
gruan, femijet, niperit, shoket, miqte dhe studentet
e tij.
NEKROLOGJI
Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 173
Duke u nisur nga ajo çka ti jetove edhe une dua te shkruaj shkurt, jo per “vdekjen” por per jeten tende…
I dashur Çerçiz,
Dua te shkruaj gjate per ty, por e kam te veshtire, aq me te veshtire e kam te pranoj ikjen tende. Largimi nga jeta i prinderve, sidomos i nenes, te afermve, te njohurve dhe i kujtdo qe ke takuar ne kete jete, te le nje boshllek ne zemer, boshllek qe nuk harrohet per nje kohe te gjate, por humbja e shokut, e mikut eshte diçka e veçante.
Sa shume gjera qe kemi perjetuar se bashku! Nder mend me vijne shume kujtime e mbresa, por qe te shkruaj per ty e kam shume te veshtire, kjo jo se nuk kam ç’te shkruaj, por jane aq te shumta mbresat e kujtimet, sa me mundon pyetja nese mund ti shkruaj te gjitha, çfare duhet te shkruaj dhe çfare duhet te mbaj ne arkiven e shpirtit tim…
Une dua te te kujtoj perhere ashtu siç ishe, energjik, plot jete dhe buzegaz. Ti ishe dhe mbete i veçante ne shoqerine tone. Ti e deshe jeten, familjen, shoqerine, punen, veten tende, çdo gje te bukur qe te jepte force dhe te ngjallte shprese ne kete bote te eger. Perballe te gjitha sfidave te jetes ti nuk u dorezove kurre, madje edhe atehere kur shendeti u perkeqesua se tepermi.
As ne endrrat dhe as ne mendimet e trishta, nuk shoh dhe nuk mendoj kurre ikjen e miqve te mi. Fjala e fundit qe perhere shkembej me ta eshte “Mirupafshim” dhe kurre nuk kam thene “Lamtumire”. Keshtu edhe per ty i dashur Çerçiz po them: Takohemi tek “Tajvani”! Do te ulemi me grate tona dhe do te pijme nga nje gote vere apo kafen tone te zakonshme.
Prof. Dr. Foto Toti
Mjeshter i Madh
Revista Stomatologjike Shqiptare174
UDHEZUES PËR AUTORËT
Revista Stomatologjike Shqiptare ofron mundë-sinë e botimit të artikujve të lidhur me fushën e stomatologjisë. Te gjithe artikujt do te dorezohen prane adreses se email: [email protected]. Revista pranon tipet e mëposhtme të artikujve:
Artikuj origjinalë: Studime shkencore që raportojnë rezultate të kërkimeve laboratorike, klinike dhe analitike epidemiologjike, bazuar në hipotezën fi llestare të studimit..
Artikuj panoramikë: Vlerësime kritike të literaturës bashkëkohore mbi një çështje me rëndësi aktuale klinike, ku mund të përfshihen edhe të dhëna ose shembuj nga eksperienca klinike dhe shkencore e vetë autorëve.
Përshkrime rasti: Përshkrime të rasteve të rralla apo të patakuara më parë që prekin strukturat e regjionit orofacial, të shoqërimeve të papritura të dy a më shumë sëmundjeve apo përgjigjeve të papritura ndaj trajtimit.
Letër drejtuar redaksisë: Letra mund të përmbajë komente e kritika konstruktive mbi artikuj të botuar më parë në Revistën Stomatologjike Shqiptare. Në raste të tilla autorit të artikullit të mëparshëm do t’i jepet mundësia t’i përgjigjet letrës në të njëjtin numër reviste. Letrat gjithashtu mund të përmbajnë opinione mbi aspekte të tjera të profesionit të stomatologjisë, si arsimi, ngritja profesionale, konceptet e reja mbi sëmundjet dhe trajtimin e tyre, mbi çështje të etikës në ushtrimin e profesionit, etj. Letrat drejtuar redaksisë nuk mund të kenë më shumë se pesë autorë.
Njoftime mbi të reja, takime dhe aktivitete: Do të pranohen për publikim vetëm nëse do të konsiderohen me interes nga redaksia.
Për t’u pranuar për shqyrtim nga redaksia, artikujt duhet të përmbushin një sërë kushtesh, prandaj autorët janë të lutur të ndjekin me përpimëri udhëzimet si vijojnë.
Të përgjithshmeDorëshkrimet duhet të paraqiten të shtypur në
versionin Microsoft Word, faqe A4, me 32 rreshta. Shkronjat duhet të jenë të stilit Times New Roman, me madhësi 12 ppt. Dorëshkrimet duhet të dorëzohen në 2 kopje të shtypura, ku secila të përmbajë tekstin dhe ilustrimet, si dhe në CD. Në CD duhet shënuar me shkrim të lexueshëm sistemi operues dhe software i përpunimit të tekstit (psh Word 2000, ose Word XP), si dhe emri i autorit kryesor.
Artikujt origjinalë dhe panoramikë nuk duhet të kalojnë 15 faqe (përfshirë edhe referencat), ndërsa dorëshkrimet e tjera nuk duhet të kalojnë 8 faqe.
Dorëshkrimet duhet të shoqërohen nga një letër shpjeguese drejtuar K/redaktorit, e fi rmosur nga të gjithë autorët e punimit, ku të paraqitet a)kërkesa për
botim, dhe të jepen b)informacione të nevojshme për redaksinë, si tipi i artikullit që paraqet dorëshkrimi, rëndësia dhe të rejat që sjell ai. Letra shoqëruese duhet të përmbajë edhe c)informacion për dorëzimin ose publikimin e mëparshëm tjetërkund të të gjithë ose një pjese të dorëshkrimit (shih seksionin Copyright), d)një fj ali ose paragraf deklarimi për marrëdhëniet fi nanciare ose të tjera që mund të çojnë në konfl ikt interesash, e)një fj ali ose paragraf deklarimi që dorëshkrimi është lexuar dhe miratuar nga të gjithë autorët (shih seksionin Autorësia), si dhe f)data e dorëzimit të dorëshkrimit në redaksi. Jeni të lutur të paraqiteni në redaksi për të tërhequr formularët-tip.
Drejtshkrimi i gjuhës shqipe është i detyrueshëm. Nuk pranohet zëvendësimi i shkronjës ë dhe ç me shkronjat e dhe c përkatësisht.
Dorëzimi në redaksi mund të bëhet me postë, me fax, ose dorazi në zyrën e redaksisë. Kopjet që paraqiten për botim nuk kthehen.
AutorësiaSi autorë të punimeve duhet të listohen vetëm ata
individë që kanë kontribuar në mënyrë thelbësore në realizimin e punimit dhe që janë të gatshëm të marrin përsipër përgjegjësinë publike mbi përmbajtjen e punimit. Të gjithë autorët duhet të fi rmosin një deklaratë si provë e miratimit të autorësisë së punimit.
TekstiTeksti duhet të përmbajë në fletë të veçanta seksionet
e mëposhtme:
Faqja e titullit Faqja e titullit përmban: 1) Titullin e artikullit-i shkurtër
(në shqip dhe anglisht), por informues (titulli nuk duhet të ketë më shumë se 100 karaktere, përfshirë edhe hapësirat, nëntitulli jo më shumë se 50 karaktere); 2) Emrat dhe mbiemrat e të gjithë autorëve, paraprirë nga titujt shkencorë dhe akademikë përkatës; 3) Institucioni i punës për secilin autor (ju lutem përdorni përkrah emrit të autorit numrat sipas sekuencës 1, 2, etj. për të bërë lidhjen me institucionin përkatës); 4) Emri dhe adresa e autorit përgjegjës për komunikimin e mëtejshëm me redaksinë, adresa e e-mailit dhe numri i tel dhe fax-it (ju lutem shënoni nëse pranoni që adresa e e-mailit dhe numri juaj i tel. dhe fax-it të publikohen në revistë).
Faqja me përmbledhjen e artikullit:Përmbledhja e artikullit duhet të përmbajë jo më
shumë se 120 fj alë. Në të duhet të prezantohen titulli i artikullit (pa autorët), qëllimi kryesor i punimit, materiali dhe metodat e përdorura si dhe rezultatet dhe arritjet në mënyrë të shkurtuar. Përmbledhja duhet të paraqitet në dy versione, në shqip dhe në anglisht. Nuk duhet të

Vellimi 14, nr. 1 dhe 2 ( 54, 55) mars 2016, dhjetor 2016 175
përdoren më shumë se 5 fj alë të shkurtuara, për të cilat duhet dhënë shpjegimi përkatës.
Përmbledhja duhet të pasohet nga 3-6 fj alë kyç (shqip dhe anglisht), të cilat ndihmojnë në indeksimin e artikullit. Fjalët kyç duhet të përzgjidhen në konformitet me nomenklaturën ndërkombëtare të sëmundjeve (Shih Indeksin Mjekësor-Index Medicus).
Trupi i tekstit Duhet të fi llojë me faqe të re dhe me titullin e punimit
(pa emrat e autorëve). Në trupin e tekstit çdo referencë, fi gurë dhe tabelë numërohet me numër rendor sipas rendit që citohet. Nuk përdoren shkurtime të tjera përveç atyre që janë përdorur në abstrakt dhe njësive matëse. Teksti duhet të organizohet në mënyrën e mëposhtme:
Artikujt origjinalëHyrja duhet të paraqesë shkurtimisht bazën
racionale dhe shkencore mbi të cilën mbështetet studimi. Nuk këshillojmë përmbledhje të gjata të literaturës. Hyrja duhet të mbyllet me përcaktimin e qartë të qëllimeve të studimit.
Materialet and Metodat duhet të paraqiten në mënyrë të detajuar. Duhet të përcaktohet lloji dhe mënyra e përzgjedhjes së popullatës në studim, parametrat e vëzhguar, medikamentet e përdorur etj., si dhe koha e fi llimit dhe mbarimit të studimit. Në këtë seksion duhet të paraqitet shkurtimisht edhe lloji i metodës statistikore të përdorur për përpunimin e të dhënave. Studimet që referojnë të dhëna mbi eksperimente në qenie njerëzore, do të pranohen për botim vetëm nëse eksperimentet janë kryer në përputhje me World Medical Association Declaration of Helsinki (versioni i vitit 2002, shih http://www.wma.net/e/policy/b3.htm), dhe nëse është e nevojshme me aprovimin e Bordit Shqiptar të Etikës.
Rezultatet e vëzhgimeve të studimit duhet të paraqiten qartë dhe pa u interpretuar.
Diskutimi zakonisht fi llon me një përmbledhje të shkurtër të rezultateve kryesore (pa përsëritur seksionin e rezultateve), duke i interpretuar dhe krahasuar me rezultatet e studimeve të ngjashme. Teksti duhet të përfundojë me një konkluzion të shkurtër dhe me një koment mbi rëndësinë klinike të rezultateve të studimit.
Artikulli panoramik
Hyrja (si më sipër)
Materialet dhe metodat: në këtë seksion duhet të përshkruhen metodat e përzgjedhjes dhe shqyrtimit të literaturës (p.sh. indekset bibliografi ke dhe database të përdorur, kriteri kohor dhe gjuhësor i përzgjedhjes së punimeve, e informacione të tjera me rëndësi).
Teksti dhe konkluzionet: teksti duhet të përfaqësojë një analizë kritike të literaturës mbi çështjen e zgjedhur. Konkluzionet e nxjerra duhet të bazohen në argumente.
Të shpjegohen cilat janë çështjet që ende nuk janë zgjidhur dhe që kërkojnë studime të mëtejshme. Mund të përdoren edhe tabela për përmbledhjen e literaturës së shqyrtuar (tabelat duhet të dorëzohen në një faqe të veçantë), ashtu si dhe analiza të posaçme statistikore.
Përshkrime rasti
Hyrja: duhet të përshkruajë të dhënat e literaturës mbi rastin që do të trajtohet.
Përshkrimi i rastit dhe Rezultatet: në këtë seksion duhet të bëhet përshkrimi i rastit, me të dhëna të detajuara. Mund të përdoren edhe tabela për paraqitjen e të dhënave në mënyrë kronologjike (tabelat duhet të dorëzohen në një faqe të veçantë), si dhe fotografi dhe radiografi me cilësi të lartë, të përzgjedhura me kujdes (veç tekstit).
Diskutimi: në këtë seksion duhet të interpretohen të dhënat e përshkruara më sipër, në bazë të eksperiencës së vetë autorit dhe të literaturës në këtë fushë.
IlustrimetTë gjitha tabelat, fi gurat dhe fotografi të duhet të
paraqiten në fi le/folder të veçantë nga teksti. Fotot duhet të dorëzohen në format TIF ose JPG. Subjektet njerëzore nuk duhet të jenë të identifi kueshëm në fotografi , me përjashtim të rasteve kur ata japin miratimin e tyre me shkrim, i cili duhet të dorëzohet në redaksi së bashku me fotografi të. Fotografi të me ngjyra kanë mundësi të kufi zuara paraqitjeje sipas mundësive teknike dhe kostos së botimit. Redaksia këshillon përdorimin e fi gurave sa më të thjeshta e të qarta për lexuesin.
Të gjitha ilustrimet duhet të shoqërohen nga një numër arab që korespondon me pjesën e tekstit ku citohet (p.sh. Tab. 1), dhe nga legjenda përkatëse.
Të gjitha ilustrimet e marra në libra, revista apo botime të tjera, janë të pranueshme vetëm në qoftë se shoqërohen me lejen me shkrim të autorit dhe botuesit përkatës.
ReferencatReferencat dorëzohen në një faqe të veçantë.
Referencat duhet të citohen në artikull, dhe të identifi kohen nëpërmjet një numri korespondues sipas rendit që citohen. Artikujt e cituar nga revistat duhet të kenë vetëm një numër identifi kimi, pamvarësisht sa herë citohen; citimet nga tekstet e librave mund të kenë më shumë se një numër identifi kimi, nëse faqet e cituara ndryshojnë. Titujt e revistave duhet të përdoren të shkurtuar sipas rregullave të përcaktuara. Nëse keni dyshime mbi shkurtimin e saktë që duhet të përdorni, mund t’i referoheni listës në ftp://nlmpubs.nlm.nih.gov/online/journals/ljiweb.pdf ose Index Medicus.
Referencat nga artikujt e revistave duhet të kenë këtë renditje: mbiemrat dhe inicialet e emrave të të gjithë autorëve, viti i botimit (në kllapa), titulli i artikullit, titulli

Revista Stomatologjike Shqiptare176
i revistës (me shkrim të pjerrët), numri i vëllimit, faqja e parë dhe e fundit e artikullit të cituar. Shembull: 1. Baum BJ, Voutetakis A, Wang J (2004). Salivary glands:
novel target sites for gene therapeutics. Trends Mol Med. 10: 585-590. Nëse artikulli ka shtatë apo më tepër autorë, mund të
listoni tre të parët dhe të shtoni et al. Referencat nga tekstet e librave duhet të kenë këtë
renditje: mbiemrat dhe inicialet e emrave të autorëve, viti i botimit(në kllapa), titulli i kapitullit, titulli i librit (me shkrim të pjerrët), edicioni, vëllimi, vendi i publikimit, shtëpia botuese, numrat e faqeve të cituara.
Shembull: 2. Scully C (2004). The oral cavity and lips. In: Burns
DA, Breathmach SM, Cox N, Griffi ths C, eds. Rooks Textbook of Dermatology. 7th Edition. Blackwell Science: Oxford, pp.66.1.-66.121.
Falenderimet dhe hollësitë e mbështetjes në formën e granteve, pajisjeve, ose barnave shtypen në përfundim të tekstit, menjëherë pas referencave. Në rast se përmenden persona, redaksia kërkon që krahas punimit, të paraqitet edhe një letër miratimi e fi rmosur nga personi i përmendur.
CopyrightLetra shoqëruese e fi rmosur nga të gjithë autorët
duhet të deklarojë që ata e kanë parë dhe miratuar shkrimin dhe se punimi nuk është publikuar dhe nuk do të publikohet tjetërkund brenda vendit (ju lutem tërhiqni formularin tip pranë redaksisë).
Punimet e dorëzuara në redaksi i nënshtrohen shqyrtimit nga një grup prej minimumi dy redaktorësh shkencorë. Të gjitha sugjerimet e nevojshme i bëhen të njohura autorit para botimit me anë të e-mail/fax. (disa herë në trajtë reçense). Autorët duhet të bëjnë korrigjimet e ndryshme dhe duhet të ridorëzojnë punimin në redaksi brenda 30 ditësh nga marrja e sugjerimeve.
Pas miratimit të artikullit për botim, redaksia i dërgon autorit përgjegjës për korrespondencën një njoftim me e-mail/fax.
Çdo artikull duhet të vijë në dy gjuhë, në gjuhën shqipe dhe në gjuhën angleze sipas rregullave të sipërpërmendura.
Shkrimet që nuk do t’u përmbahen udhëzimeve do t’u rikthehen autorëve për rishikim pa u marrë në shqyrtim.