Embed Size (px)
Citation preview
Ruolo dell’immunoterapia
associata a radioterapia locale per spiegare l’abscopal effect:
un raro caso clinico
Do#.ssa'Annalisa'Nardone'Rimini,&07)10&novembre&2015&
Melanoma'cutaneo''• Incidenza)di)3+5/100000/anno)nei)paesi)mediterranei)(ESMO)2015)))))• “Recalcitrant)disease”))))• MalaAa)complessa)che)richiede)spesso))più'modalità'terapeu8che'')• Malgrado)l’evoluzione)in)ogni)ambito)terapeuHco)la)prognosi)nelle)forme)
avanzate)rimane))scarsa))• Dal)50%)al)75%)dei)melanomi)metastaHci)coinvolge)l’encefalo)• )Il)melanoma)è)la)terza)causa)più)frequente)di)metastasi)cerebrali)FR:))+)sesso)maschile)
))+)melanoma)mucosale)o)della)regione)testa)collo)))+)soSoHpo)nodulare)))+)presenza)di)ulcerazione)e)mitosi)
))))))))+)esordio)con)stadio)IV)
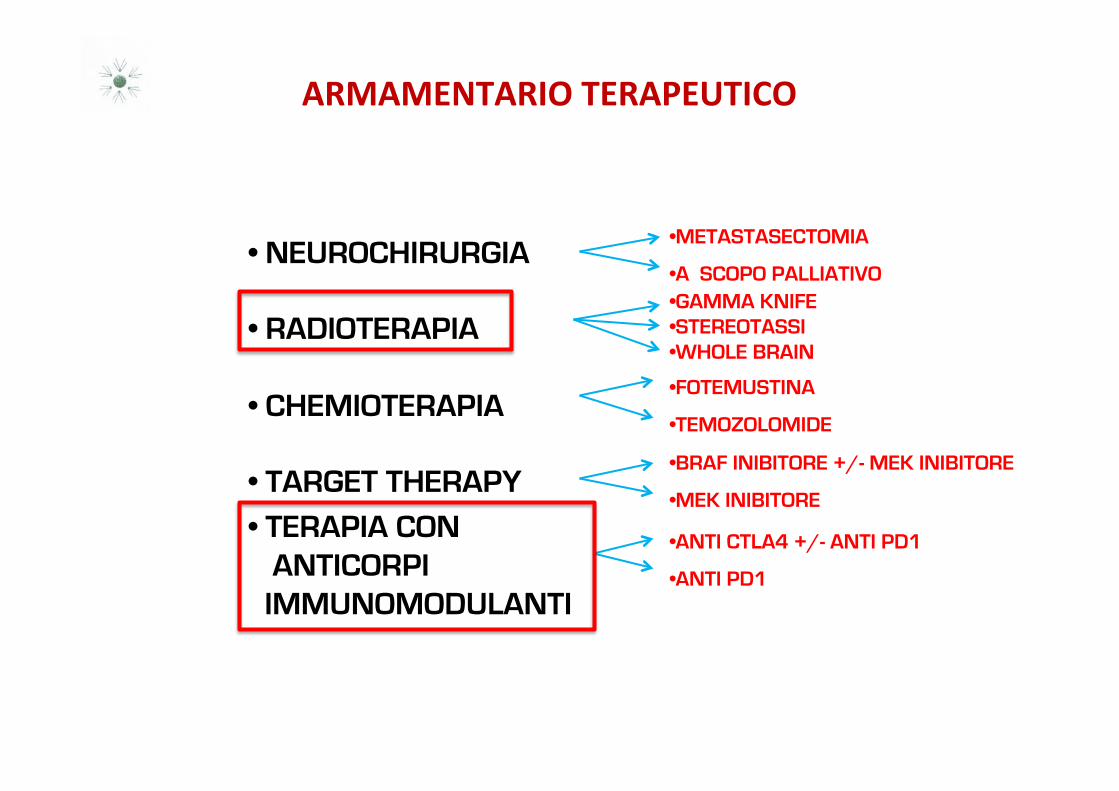
ARMAMENTARIO'TERAPEUTICO''
• NEUROCHIRURGIA
• RADIOTERAPIA
• CHEMIOTERAPIA
• TARGET THERAPY
• TERAPIA CON ANTICORPI IMMUNOMODULANTI
• METASTASECTOMIA
• A SCOPO PALLIATIVO • GAMMA KNIFE • STEREOTASSI • WHOLE BRAIN
• FOTEMUSTINA
• TEMOZOLOMIDE
• BRAF INIBITORE +/- MEK INIBITORE
• MEK INIBITORE
• ANTI CTLA4 +/- ANTI PD1
• ANTI PD1
''
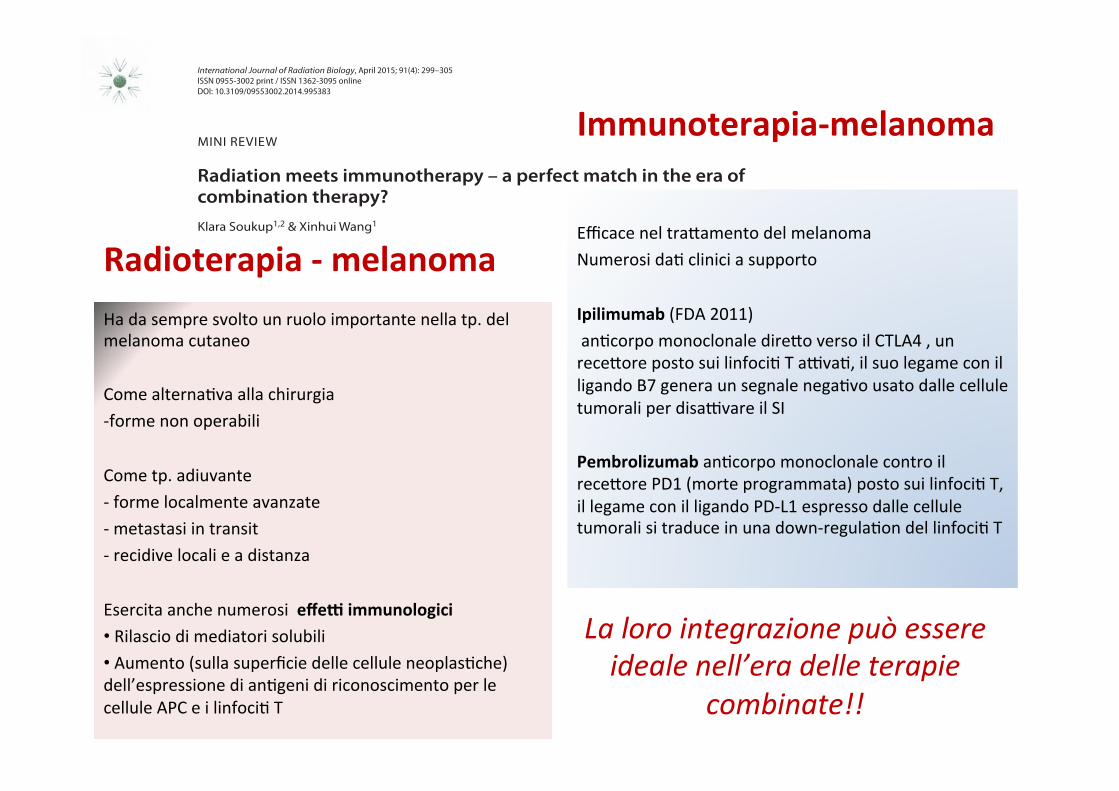
Radioterapia'B'melanoma'
Ha)da)sempre)svolto)un)ruolo)importante)nella)tp.)del)melanoma)cutaneo)))Come)alternaHva)alla)chirurgia))+forme)non)operabili)))Come)tp.)adiuvante))+)forme)localmente)avanzate)+)metastasi)in)transit)+)recidive)locali)e)a)distanza)))Esercita)anche)numerosi))effeD'immunologici')• )Rilascio)di)mediatori)solubili))• )Aumento)(sulla)superficie)delle)cellule)neoplasHche))dell’espressione)di)anHgeni)di)riconoscimento)per)le)cellule)APC)e)i)linfociH)T)
)Efficace)nel)traSamento)del)melanoma)Numerosi)daH)clinici)a)supporto))Ipilimumab)(FDA)2011)))anHcorpo)monoclonale)direSo)verso)il)CTLA4),)un)receSore)posto)sui)linfociH)T)aAvaH,)il)suo)legame)con)il)ligando)B7)genera)un)segnale)negaHvo)usato)dalle)cellule)tumorali)per)disaAvare)il)SI))Pembrolizumab)anHcorpo)monoclonale)contro)il))receSore)PD1)(morte)programmata))posto)sui)linfociH)T,)il)legame)con)il)ligando)PD+L1)espresso)dalle)cellule)tumorali)si)traduce)in)una)down+regulaHon)del)linfociH)T)
La&loro&integrazione&può&essere&ideale&nell’era&delle&terapie&
combinate!!&
299
International Journal of Radiation Biology, April 2015; 91(4): 299–305ISSN 0955-3002 print / ISSN 1362-3095 onlineDOI: 10.3109/09553002.2014.995383
Correspondence: Dr Xinhui Wang, MD, PhD, Department of Surgical Oncology, Massachusetts General Hospital, Harvard Medical School, 55 Fruit Street, Boston, MA 02114, USA. Tel: 1 617 726 7881. E-mail: [email protected]
(Received 3 July 2014; revised 29 September 2014; accepted 18 November 2014)
© 2015 Informa UK Ltd. This is an open-access article distributed under the terms of the “http://creativecommons.org/licenses/by-nc-nd/3.0/” CC-BY-NC-ND 3.0 License which permits users to download and share the article for non-commercial purposes, so long as the article is reproduced in the whole without changes, and provided the original source is credited.
Radiation meets immunotherapy – a perfect match in the era of combination therapy?Klara Soukup1,2 & Xinhui Wang1
1Division of Surgical Oncology, Department of Surgery, Massachusetts General Hospital – Harvard Medical School, Boston, MA, USA, and 2Department of Tumor Immunology, CCRI, St Anna Kinderkrebsforschung, Vienna, Austria
Introduction
For several decades, the concept of cancer immunotherapy (CIT) has been struggling to establish itself as the fourth pillar of acknowledged cancer treatment strategies alongside surgery, radiation and chemotherapy. With its nomination as Science ‘Breakthrough of the Year 2013’ (Couzin-Frankel 2013) and
preclinical studies gradually translating into clinical data, the field of CIT has finally reached a state of acceptance among the established oncological domains. Currently, different immuno-therapeutic approaches are standing their ground as powerful treatment strategies for a wide range of malignant diseases. A very prominent and recent example of an outstanding CIT success involves immune checkpoint blockade therapy by monoclonal antibodies (mAb) targeting inhibitory molecules on either immune effector T-cells or tumor cells. Interfering with co-inhibitors has been shown to unleash a powerful anti-tumor T-cell response (Pardoll 2012). Promising early-stage clinical trials have shown safety and impressive activity of mAb block-ing activity of programmed cell death 1 (PD1), expressed on T-cells (Topalian et al. 2012), or one of its ligands, programmed death-ligand 1 (PD-L1) (Brahmer et al. 2012). Recently, the FDA approved lambrolizumab, a PD1-targeting mAb for treatment of advanced or unresected melanomas that no longer respond to other drugs (Hamid et al. 2013). Furthermore ipilimumab, a mAb against cytotoxic T-lymphocyte-associated antigen 4 (CTLA4) on T-cells, was approved for the treatment of meta-static melanoma (Lipson and Drake 2011). In 2013, a combina-tion of anti-CTLA4 and anti-PD1 mAb treatment was reported to act synergistically in increasing survival and tumor regression in advanced melanoma patients (Wolchok et al. 2013). This novel immunomodulatory approach exhibits great potential especially for the treatment of severe malignancies resistant to conventional therapies.
However, major obstacles to broad clinical applicability of CIT become more evident. Whereas significant improve-ments of overall and progression-free survival can be achieved in individual cancer patients, most CIT strategies fail to establish long-lasting tumor rejection in large patient groups – with many patients responding poorly to treatment (Brahmer and Pardoll 2013, Fishman 2014, Raval et al. 2014). The precise processes behind this high variability of thera-peutic efficacy remain to be clarified, but most likely involve high heterogeneity of different tumor types as well as poor
MINI REVIEW
AbstractPurpose: This review focuses on recent advances in the field of combining radiation with immunotherapy for the treatment of malignant diseases, since various combinatorial cancer therapy approaches have lately proven highly successful.Results: With initial case reports and anecdotes progressively converting into solid clinical data, interest in cancer immunotherapy (CIT) has risen steeply. Especially immune checkpoint blockade therapies have recently celebrated tremendous successes in the treatment of severe malignancies resistant to conventional treatment strategies. Nevertheless, the high variability of patient responses to CIT remains a major hurdle, clearly indicating an urgent need for improvement. It has been suggested that successful cancer therapy most probably involves combinatorial treatment approaches. Radiotherapy (RT) has been proposed as a powerful partner for CIT due to its broad spectrum of immune modulatory characteristics. Several preclinical studies, supported by an increasing number of clinical observations, have demonstrated synergistic interactions between RT and CIT resulting in significantly improved therapy outcomes.Conclusions: Numerous reports have shown that radiation is capable of tipping the scales from tumor immune evasion to elimination in different tumor types. The next puzzle to be solved is the question of logistics – including types, schedule and dosage of combinatorial RT and CIT strategies.
Keywords: Radiation, radiotherapy, immunotherapy, cancer, combination therapy
TRAB_A_995383.indd 299 4/23/2015 4:26:01 PM
Down
load
ed b
y [9
3.63
.158
.204
] at 0
1:25
23
Octo
ber 2
015
ImmunoterapiaBmelanoma'
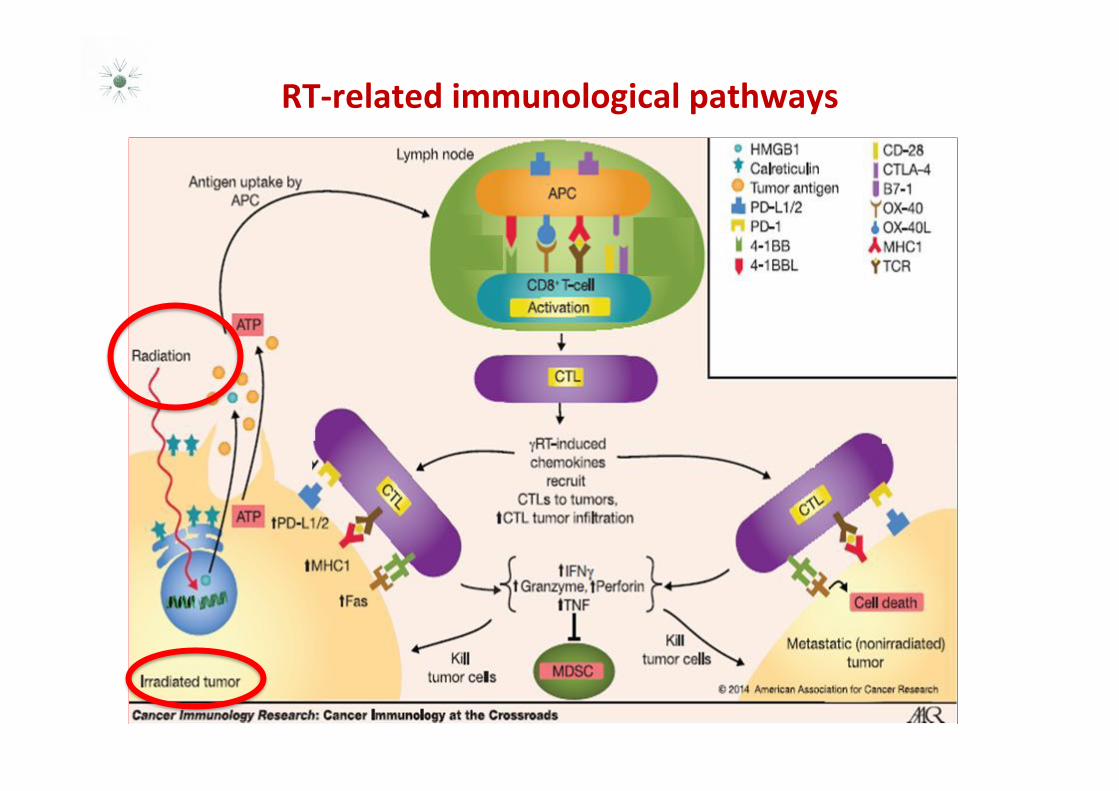
RTBrelated'immunological'pathways'
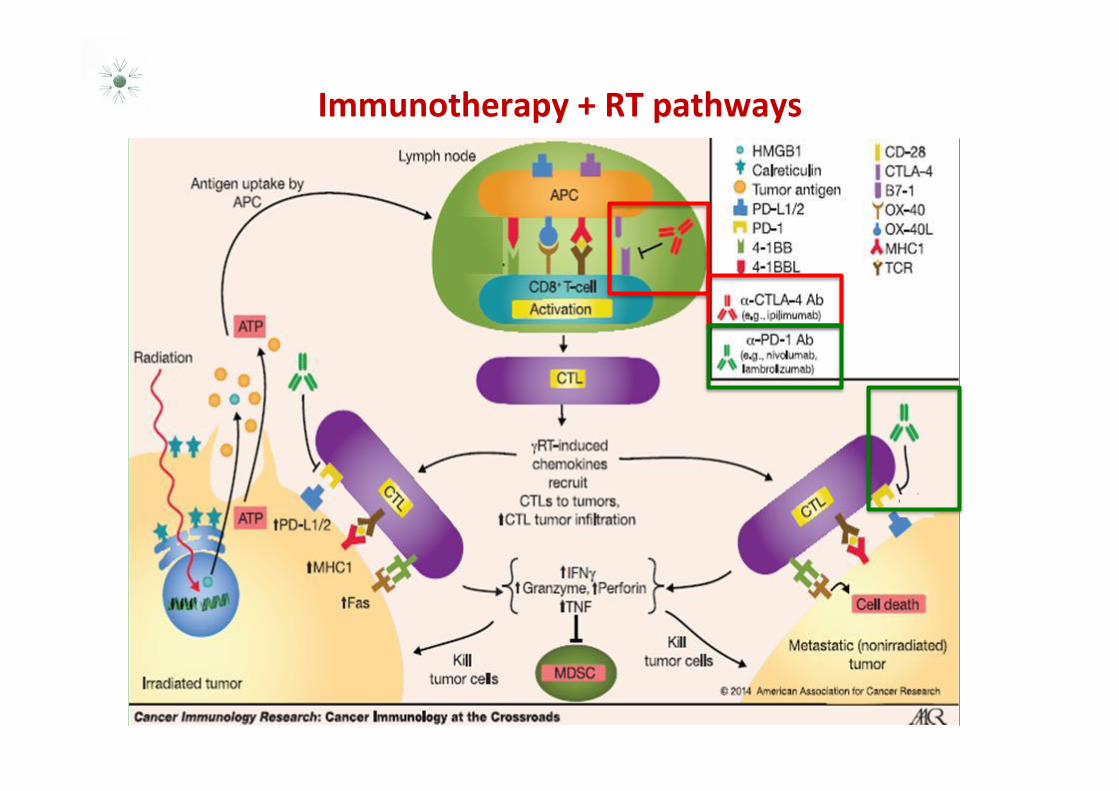
Immunotherapy'+'RT'pathways'
CASO'CLINICO'
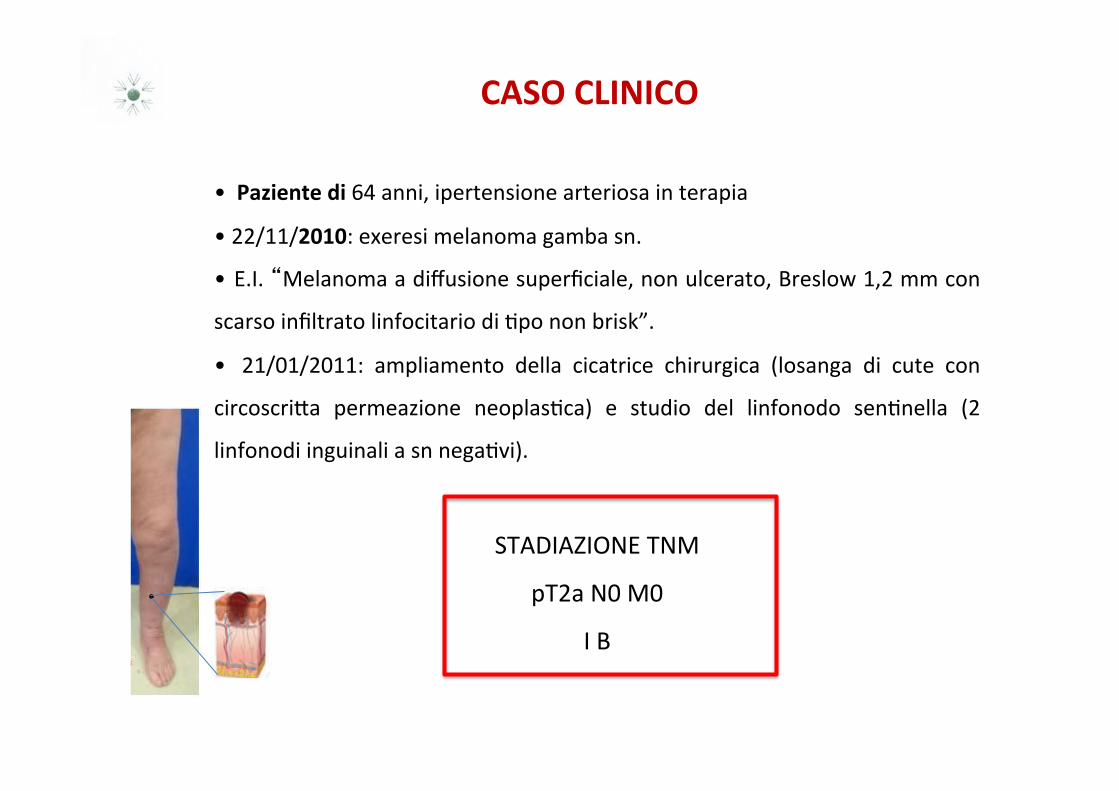
• ''Paziente'di'64)anni,)ipertensione)arteriosa)in)terapia))
• )22/11/2010:)exeresi)melanoma)gamba)sn.))
• )E.I.)�Melanoma)a)diffusione)superficiale,)non)ulcerato,)Breslow)1,2)mm)con)
scarso)infiltrato)linfocitario)di)Hpo)non)brisk”.)
• ) 21/01/2011:) ampliamento) della) cicatrice) chirurgica) (losanga) di) cute) con)
circoscriSa) permeazione) neoplasHca)) e) studio) del) linfonodo) senHnella) (2)
linfonodi)inguinali)a)sn)negaHvi).)
STADIAZIONE)TNM))
pT2a)N0)M0)
I)B)
NCCN Guidelines IndexMelanoma Table of Contents
Discussion
Version 1.2016, 10/23/15 © National Comprehensive Cancer Network, Inc. 2015, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®.
NCCN Guidelines Version 1.2016 StagingMelanoma
ST-1
Used with the permission of the American Joint Committee on Cancer (AJCC), Chicago, Illinois. The original and primary source for this information is the AJCC Cancer Staging Manual, Seventh Edition (2010) published by Springer Science+Business Media, LLC (SBM). (For complete information and data supporting the staging tables, visit www.springer.com.) Any citation or quotation of this material must be credited to the AJCC as its primary source. The inclusion of this information herein does not authorize any reuse or further distribution without the expressed, written permission of Springer SBM, on behalf of the AJCC.
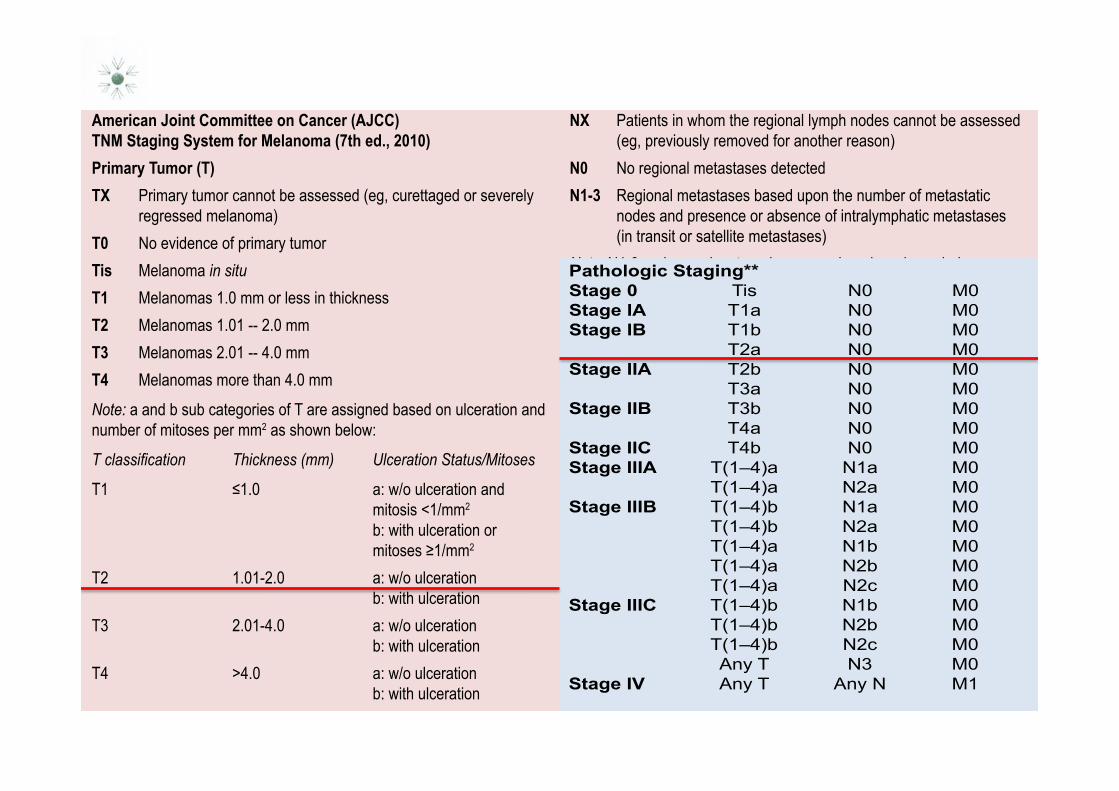
Table 1American Joint Committee on Cancer (AJCC) TNM Staging System for Melanoma (7th ed., 2010)Primary Tumor (T)TX Primary tumor cannot be assessed (eg, curettaged or severely
regressed melanoma)T0 No evidence of primary tumorTis Melanoma in situT1 Melanomas 1.0 mm or less in thickness T2 Melanomas 1.01 -- 2.0 mmT3 Melanomas 2.01 -- 4.0 mm T4 Melanomas more than 4.0 mm Note: a and b sub categories of T are assigned based on ulceration and number of mitoses per mm2 as shown below:
7�FODVVL¿FDWLRQ� 7KLFNQHVV��PP�� 8OFHUDWLRQ�6WDWXV�0LWRVHV
7�� � � ����� � � �D��Z�R�XOFHUDWLRQ�DQG� mitosis <1/mm2 b: with ulceration or PLWRVHV����PP2
T2 1.01-2.0 a: w/o ulceration b: with ulceration
T3 2.01-4.0 a: w/o ulceration b: with ulceration
T4 >4.0 a: w/o ulceration b: with ulceration
Regional Lymph Nodes (N)NX Patients in whom the regional lymph nodes cannot be assessed
(eg, previously removed for another reason)N0 No regional metastases detectedN1-3 Regional metastases based upon the number of metastatic
nodes and presence or absence of intralymphatic metastases (in transit or satellite metastases)
Note: N1-3 and a-c sub categories are assigned as shown below:1�&ODVVL¿FDWLRQ� 1R��RI�0HWDVWDWLF�1RGHV� 1RGDO�0HWDVWDWLF�0DVVN1 1 node a: micrometastasis*
b: macrometastasis**N2 2-3 nodes a: micrometastasis*
b: macrometastasis** c: in transit met(s)/satellite(s) ZLWKRXW metastatic nodes
N3 4 or more metastatic nodes, or matted nodes, or in transit met(s)/satellite(s) ZLWK meta- static node(s)
*Micrometastases are diagnosed after sentinel lymph node biopsy and completion lymphadenectomy (if performed). 0DFURPHWDVWDVHV�DUH�GH¿QHG�DV�FOLQLFDOO\�GHWHFWDEOH�QRGDO�PHWDVWDVHV�FRQ¿UPHG�E\�WKHUDSHXWLF�O\PSKDGHQHFWRP\�RU�ZKHQ�QRGDO�PHWDVWDVLV�exhibits gross extracapsular extension.
Continue
Printed by Leonarda Rella on 10/29/2015 7:59:13 AM. For personal use only. Not approved for distribution. Copyright © 2015 National Comprehensive Cancer Network, Inc., All Rights Reserved.
NCCN Guidelines IndexMelanoma Table of Contents
Discussion
Version 1.2016, 10/23/15 © National Comprehensive Cancer Network, Inc. 2015, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®.
NCCN Guidelines Version 1.2016 StagingMelanoma
ST-2
Distant Metastasis (M)M0 No detectable evidence of distant metastasesM1a Metastases to skin, subcutaneous, or distant lymph nodes M1b Metastases to lungM1c Metastases to all other visceral sites or distant metastases to
any site combined with an elevated serum LDH
Note: Serum LDH is incorporated into the M category as shown below:0�&ODVVL¿FDWLRQ� 6LWH� 6HUXP�/'+M1a Distant skin, subcutaneous, Normal or nodal mets
M1b Lung metastases Normal
M1c All other visceral Normal metastases Any distant metastasis Elevated
Anatomic Stage/Prognostic GroupsClinical Staging*Stage 0 Tis N0 M0Stage IA T1a N0 M0Stage IB T1b N0 M0 T2a N0 M0Stage IIA T2b N0 M0 T3a N0 M0Stage IIB T3b N0 M0 T4a N0 M0Stage IIC T4b N0 M0Stage III $Q\7�� �1��� 0�Stage IV Any T Any N M1*Clinical staging includes microstaging of the primary melanoma and clinical/radiologic evaluation for metastases. By convention, it should be used after complete excision of the primary melanoma with clinical assessment for regional and distant metastases.
Pathologic Staging**Stage 0 Tis N0 M0Stage IA T1a N0 M0Stage IB T1b N0 M0 T2a N0 M0Stage IIA T2b N0 M0 T3a N0 M0Stage IIB T3b N0 M0 T4a N0 M0Stage IIC T4b N0 M0Stage IIIA T(1–4)a N1a M0 T(1–4)a N2a M0Stage IIIB T(1–4)b N1a M0 T(1–4)b N2a M0 T(1–4)a N1b M0 T(1–4)a N2b M0 T(1–4)a N2c M0Stage IIIC T(1–4)b N1b M0 T(1–4)b N2b M0 T(1–4)b N2c M0 Any T N3 M0Stage IV Any T Any N M1
**Pathologic staging includes microstaging of the primary melanoma and pathologic information about the regional lymph nodes after partial or complete lymphadenectomy. Pathologic Stage 0 or Stage IA patients are the exception; they do not require pathologic evaluation of their lymph nodes.
Used with the permission of the American Joint Committee on Cancer (AJCC), Chicago, Illinois. The original and primary source for this information is the AJCC Cancer Staging Manual, Seventh Edition (2010) published by Springer Science+Business Media, LLC (SBM). (For complete information and data supporting the staging tables, visit www.springer.com.) Any citation or quotation of this material must be credited to the AJCC as its primary source. The inclusion of this information herein does not authorize any reuse or further distribution without the expressed, written permission of Springer SBM, on behalf of the AJCC.
Printed by Leonarda Rella on 10/29/2015 7:50:07 AM. For personal use only. Not approved for distribution. Copyright © 2015 National Comprehensive Cancer Network, Inc., All Rights Reserved.

METASTASI'IN'TRANSIT'E'AI'LINFONODI'REGIONALI'...dopo'12'mesi'
• 'Novembre)2011:)comparsa)di)metastasi)in)transit)traSate)con)))) ) ) ) ) )
) )eleSrochemioterapia ) ) ) ) ) ) ))
• )Marzo)2012)e)OSobre)2012:)Due)ulteriori)traSamenH)di)) ) ) ) ) ) )
) )eleSrochemioterapia)su)gamba)sn)
• )Febbraio)2013:)adenopaHa)inguinale)sn))intervento)di)linfadenectomia)inguino))))) ) )
) )crurale)))))oSuratoria)(3/27))
• )Novembre)2013):)ulteriore)eleSrochemioterapia)su)gamba)sn.)
Analisi'mutazionale'su'metastasi'so#ocute'gamba'sn:''
'BRAF'e'NRAS'wild'type'
) )BRAF'inibitoriBMEK'inibitori''
MELANOMA'METASTATICO'
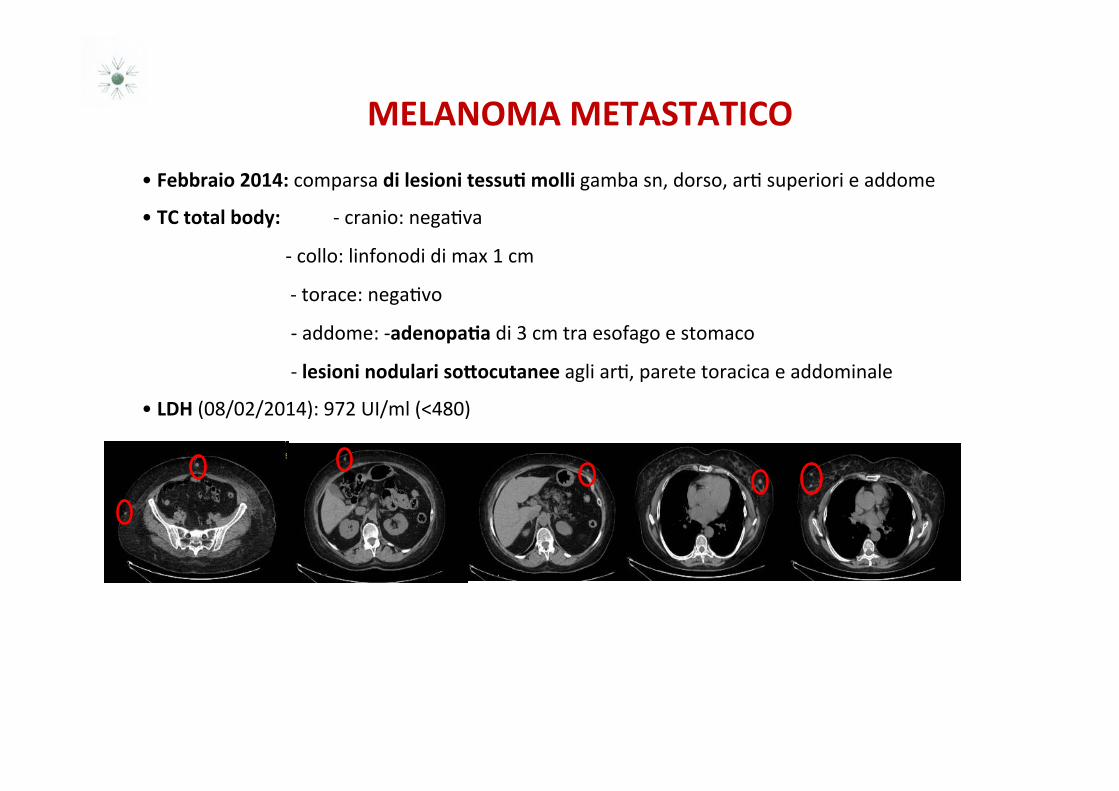
• 'Febbraio'2014:'comparsa)di'lesioni'tessu8'molli'gamba)sn,)dorso,)arH)superiori)e)addome)
• )TC'total'body:' )+)cranio:)negaHva)
) )))))))))))+)collo:)linfonodi)di)max)1)cm)
) ))))))))))))+)torace:)negaHvo)
)))))))))))))))))))))))))))))))+)addome:)+adenopa8a)di)3)cm)tra)esofago)e)stomaco)
)))))))))))))))))))))))))))))))+)lesioni'nodulari'so#ocutanee'agli)arH,)parete)toracica)e)addominale)
• )LDH'(08/02/2014):)972)UI/ml)(<480))
TERAPIA'DI'I'LINEA'
')
• )12/02/2014:'1°ciclo'di'IPILIMUMAB'3'mg/Kg'(D.T.'240'mg)''
• ''16/04/2014:'4°'e'ul8mo'ciclo'di'IPILIMUMAB:'durante'il'tra#amento'
comparsa'di'prurito'agli'ar8,'già'al'2'ciclo,'associato'ad'eosinofilia,'
modicamente'controllato'con'terapia'an8staminica.''
Durante'il'tra#amento'incremento'progressivo'di'LDH'(1388'UI/ml'ad'
Aprile''2014)''
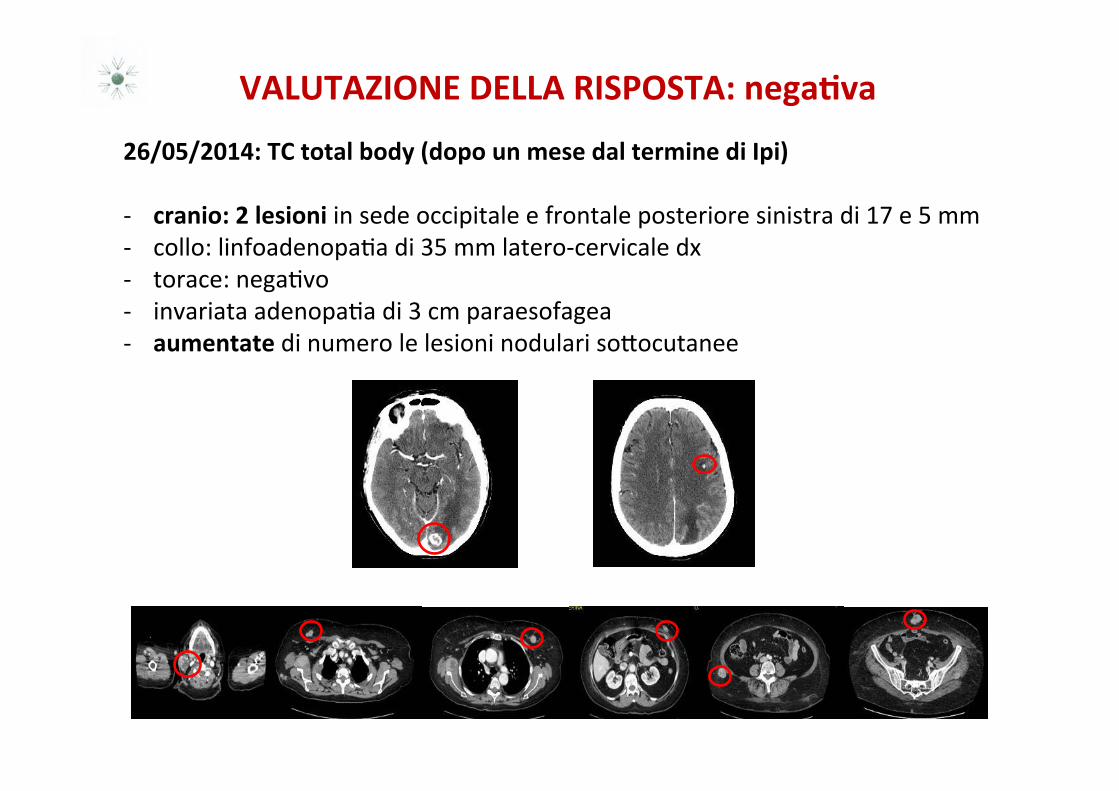
VALUTAZIONE'DELLA'RISPOSTA:'nega8va''
26/05/2014:'TC'total'body'(dopo'un'mese'dal'termine'di'Ipi)''+ cranio:'2'lesioni)in)sede)occipitale)e)frontale)posteriore)sinistra)di)17)e)5)mm)+ collo:)linfoadenopaHa)di)35)mm)latero+cervicale)dx)+ torace:)negaHvo)+ invariata)adenopaHa)di)3)cm)paraesofagea)+ aumentate)di)numero)le)lesioni)nodulari)soSocutanee)
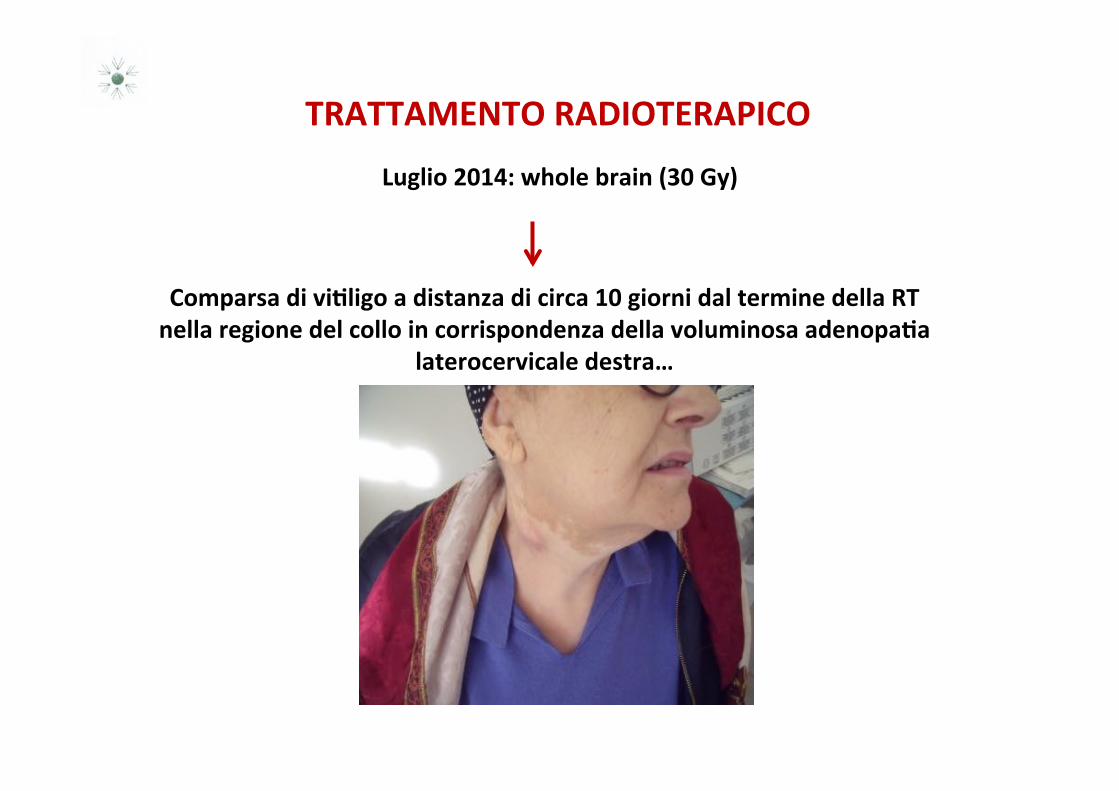
TRATTAMENTO'RADIOTERAPICO'
Luglio'2014:'whole'brain'(30'Gy)') Comparsa'di'vi8ligo'a'distanza'di'circa'10'giorni'dal'termine'della'RT'
nella'regione'del'collo'in'corrispondenza'della'voluminosa'adenopa8a'laterocervicale'destra…'
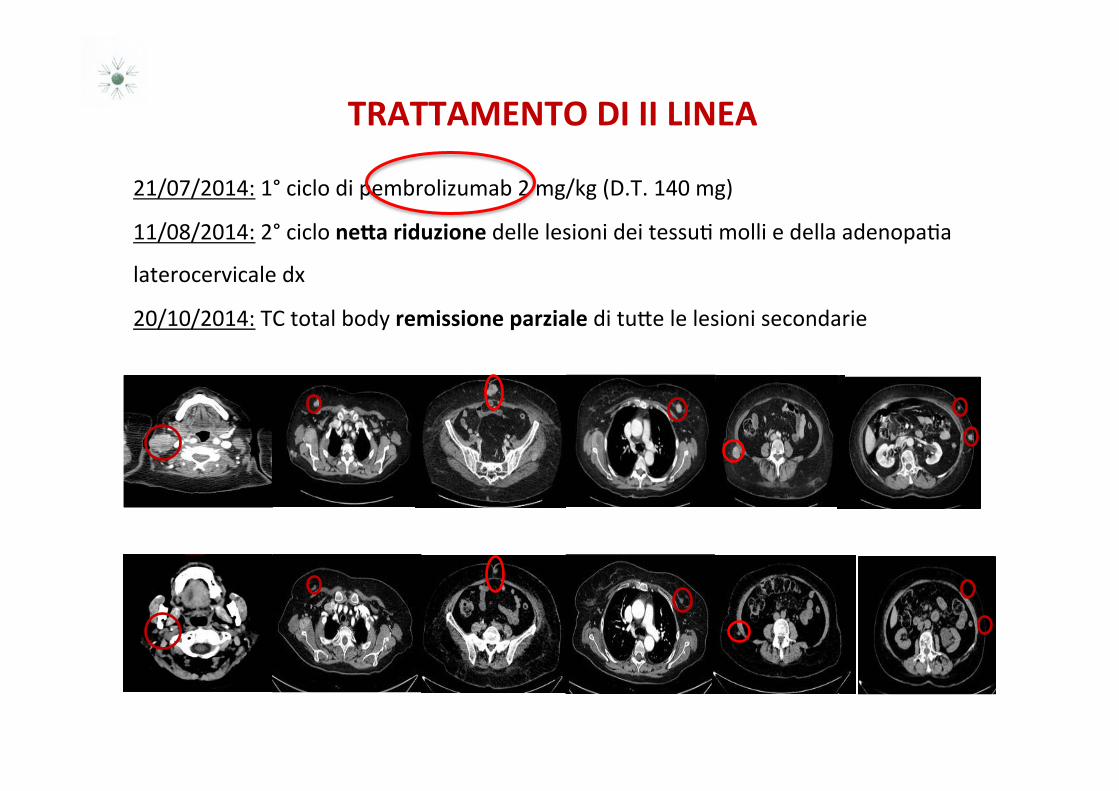
21/07/2014:)1°)ciclo)di)pembrolizumab)2)mg/kg)(D.T.)140)mg))
11/08/2014:)2°)ciclo)ne#a'riduzione'delle)lesioni)dei)tessuH)molli)e)della)adenopaHa)))
laterocervicale)dx))
20/10/2014:)TC)total)body)remissione'parziale'di'tuSe)le)lesioni)secondarie)
TRATTAMENTO'DI'II'LINEA'
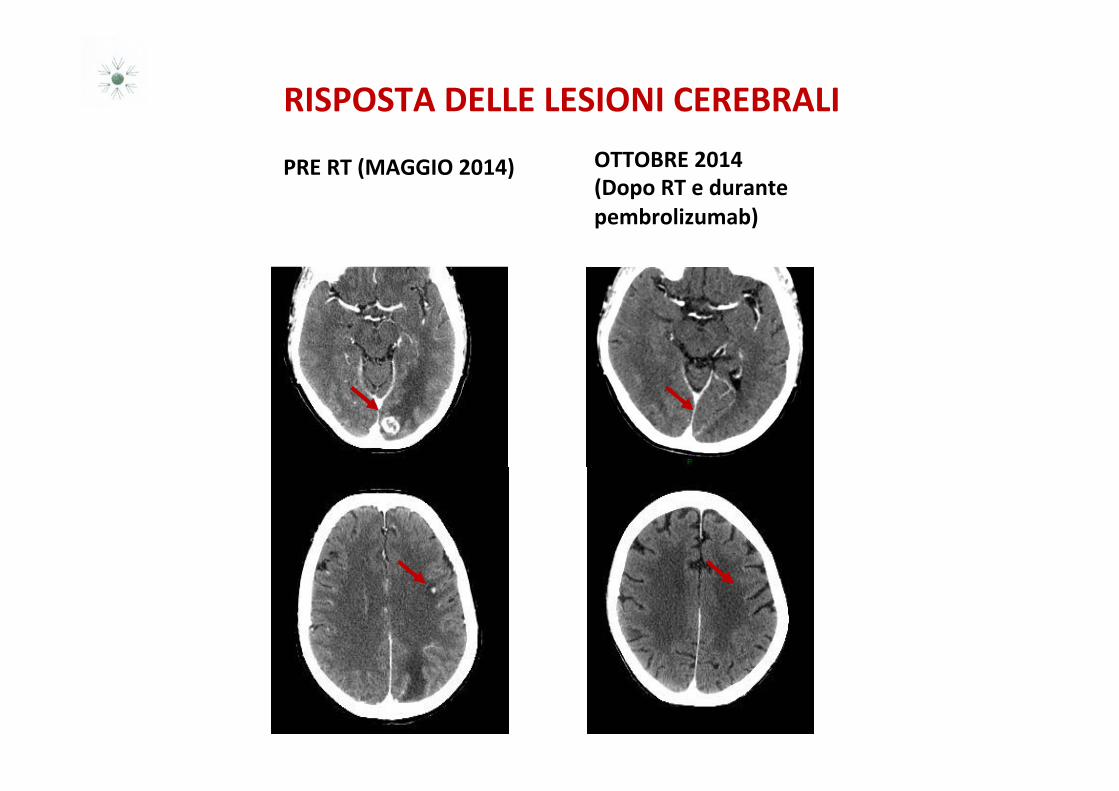
RISPOSTA'DELLE'LESIONI'CEREBRALI'
PRE'RT'(MAGGIO'2014)' OTTOBRE'2014''(Dopo'RT'e'durante''pembrolizumab)'
'
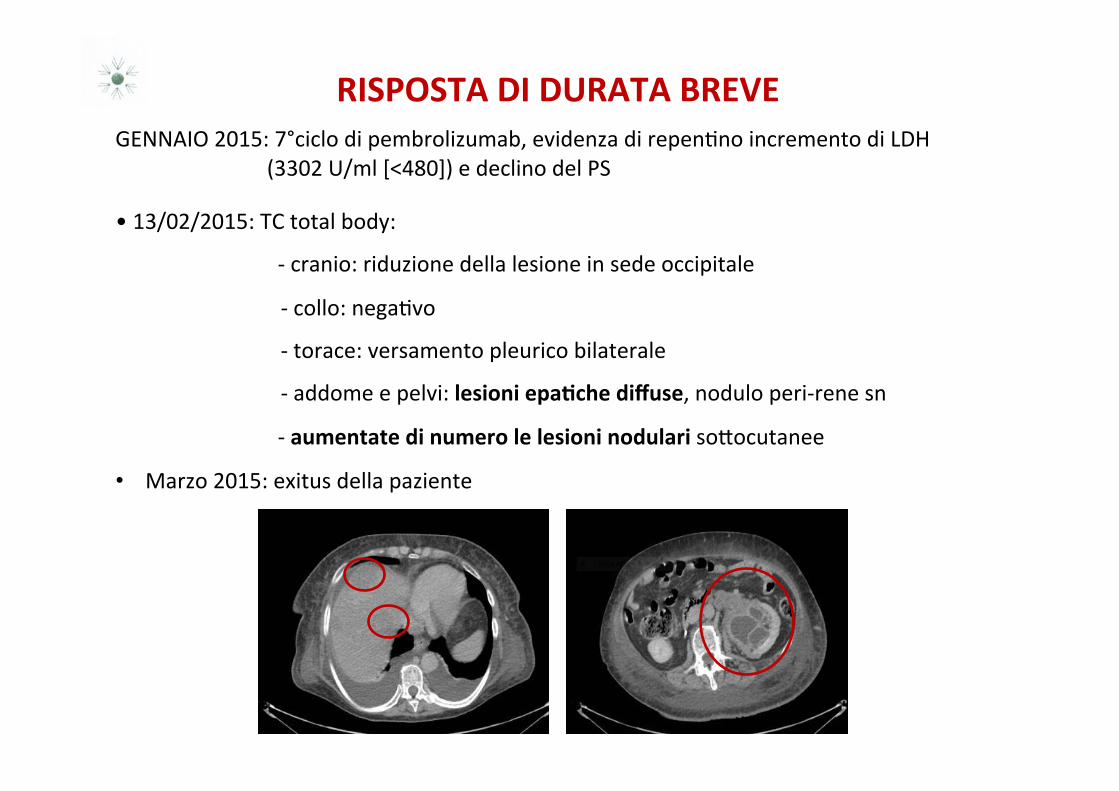
GENNAIO)2015:)7°ciclo)di)pembrolizumab,)evidenza)di)repenHno)incremento)di)LDH))))))))))))))))))))))))))))))(3302)U/ml)[<480]))e)declino)del)PS))
• )13/02/2015:)TC)total)body:))
))))))))))))))))))))))))))))))+)cranio:)riduzione)della)lesione)in)sede)occipitale)
) ) )))))+)collo:)negaHvo)
) ) )))))+)torace:)versamento)pleurico)bilaterale)
) ) )))))+)addome)e)pelvi:)lesioni'epa8che'diffuse,)nodulo)peri+rene)sn))
))))))))))))))))))))))))))))))+)aumentate'di'numero'le'lesioni'nodulari'soSocutanee)
• Marzo)2015:)exitus)della)paziente)
RISPOSTA'DI'DURATA'BREVE'
COSA'HA'INDOTTO'LA'RISPOSTA'
REMISSIONE'PARZIALE'LEGATA'AD'ABSCOPAL'EFFECT?''
'''''''''''RAPIDA'RISPOSTA'AD'ANTIBPD1?''''''''''
SOMMA'DI'ABSCOPAL'EFFECT'ED'ANTIBPD1?'
COS’È'L’ABSCOPAL'EFFECT'?)
• DescriSo)da)Mole)nel)1953)è)un)fenomeno'raro'che'consiste'nella'regressione'di'un'tumore'in'una'sede'lontana'dal'sito'irradiato.'
)• Le)interazioni)tra)RT)e)sistema)immunitario)del)paziente)sono)
alla)base)dell’effeSo)abscopal)))• Il)ripetersi'di'casi'di'abscopal'ha)portato)i)ricercatori)ad)
individuare)numerosi)meccanismi,)già)descriA,)con)cui)la)RT)suscita)una)risposta)

Brief Report
The Abscopal Effect Associated With a SystemicAnti-melanoma Immune ResponseEmily F. Stamell, MD,* Jedd D. Wolchok, MD, PhD,y,z,x,k Sacha Gnjatic, PhD,z,x
Nancy Y. Lee, MD,{ and Isaac Brownell, MD, PhD**,yy
*Division of Dermatology, Department of Medicine, Albert Einstein College of Medicine, Bronx, New York; yMelanoma andSarcoma Service, Department of Medicine, zLudwig Institute for Cancer Research, and xLudwig Center for CancerImmunotherapy, Memorial Sloan-Kettering Cancer Center, New York, New York; kWeill-Cornell Medical College, New York,New York; {Department of Radiation Oncology and **Dermatology Service, Department of Medicine, Memorial Sloan-Kettering Cancer Center, New York, New York; and the yyDermatology Branch, National Cancer Institute, Bethesda,Maryland
Received Mar 2, 2012. Accepted for publication Mar 8, 2012
Summary
We report a case of metastaticmelanoma treated with pallia-tive radiotherapy to theprimary tumor. The patientalso experienced regression ofnonirradiated lesions, demon-strating the abscopal effect.Importantly, serology showedanti-MAGEA3 antibodies,documenting an associationbetween the abscopal effectand a systemic antitumorimmune response. Whereasthe literature suggests immuneactivation after tumor irradia-tion, this case documents anantitumor response seen indirect association with absco-pal clearance. Implications forradiation in melanoma immu-notherapy are discussed.
The clearance of nonirradiated tumors after localized radiation therapy is known as the abscopaleffect. Activation of an antitumor immune response has been proposed as a mechanism for theabscopal effect. Here we report a patient with metastatic melanoma who received palliative radi-ation to his primary tumor with subsequent clearance of all his nonirradiated in-transit metas-tases. Anti-MAGEA3 antibodies were found upon serological testing, demonstrating anassociation between the abscopal effect and a systemic antitumor immune response. A brainrecurrence was then treated with a combination of stereotactic radiosurgery and immunotherapywith ipilimumab. The patient experienced a complete remission that included resolution of nodalmetastases, with a concomitant increase in MAGEA3 titers and a new response to the cancerantigen PASD1. This case supports the immune hypothesis for the abscopal effect, and illus-trates the potential of combining radiotherapy and immunotherapy in the treatment of mela-noma. ! 2013 Elsevier Inc.
Reprint requests to: Isaac Brownell, MD, PhD, Dermatology Branch,National Cancer Institute, 10 Center Drive, Bethesda, Maryland 20892.Tel: 301-496-6770; Fax: 301-496-5370; E-mail: [email protected]
Conflict of interest: JDW has been a consultant to and received grantsfrom Bristol-Myers Squibb.AcknowledgmentsdWe thank Erika Ritter for technical support andDaphne Demas for medical photography.
Int J Radiation Oncol Biol Phys, Vol. 85, No. 2, pp. 293e295, 20130360-3016/$ - see front matter ! 2013 Elsevier Inc. All rights reserved.doi:10.1016/j.ijrobp.2012.03.017
Radiation OncologyInternational Journal of
biology physics
www.redjournal.org
Spontaneous regression of metastatic melanoma e Clinical evidence ofthe abscopal effect
R.J. Bramhall a,*, K. Mahady b, A.H.S. Peach a
aLeeds General Infirmary, Great George Street, Leeds LS13EX, UKbDepartment of Radiology, Leeds General Infirmary, UK
Accepted 26 September 2013Available online 7 October 2013
Abstract
Introduction: Metastatic melanoma is poorly understood. Regression of primary lesions has been associated with poor prognosis, but spon-taneous regression of all metastatic disease is clearly beneficial. A patient’s own immune responses occasionally appear to stimulate spon-taneous regression of metastatic disease in melanoma.Patients and methods: We present six interesting cases of complete or nearly complete spontaneous regression of metastatic melanoma,suggest possible causes and review the literature.Results and conclusions: These cases show clear radiological, pathological or clinical evidence of spontaneous regression of metastaticmelanoma. This remains a poorly understood phenomena warranting further investigation and may prove useful in the development of im-mune mediated solutions.! 2013 Elsevier Ltd. All rights reserved.
Keywords: Spontaneous regression metastatic melanoma abscopal effect
Introduction/aims
Spontaneous regression of any tumour has been definedas: 1) a clinical and histological diagnosis of malignancy;2) lack of therapeutic manipulation sufficient to accountfor regression; 3) clinical evidence of regression; 4) a sig-nificant period of follow-up; 5) if possible, histological ex-amination of tissue sites where regression has occurred.1 Itis not synonymous with cure and need not necessarilyresult in complete tumour disappearance. Spontaneousregression can be described as either partial or complete,but there are no definitive criteria. Various clinical featureshave been described including loss of pigmentation withinthe lesion or an area of surrounding hypopigmentation‘halo-phenomenon’, reduction in size, telangiectasia andevidence of scarring. Pathological features suggestive ofcomplete regression include an inflammatory cell infiltrate(particularly T-cell lymphocytes and plasma cells), exten-sive deposition of dermal melanophages and papillarydermal fibrosis, without any evidence of melanocytic
proliferation.2 In partial or early regression, some of thesemay be present with areas of ongoing melanocytic prolifer-ation, with or without the presence of tumour infiltratinglymphocytes. Other lesions such as lichenoid keratosisand regressed or halo naevae can mimic regressed mela-noma, but tend to show a greater degree of melanosisand a less symmetric lichenoid infiltrate.2
Partial regression of primary melanoma is well recog-nised, occurs in 10e35% of cases3 and forms part of theminimum histopathology data set for reporting melanoma.Thin melanomas may show focal regression in 7e61% ofall lesions.4 Some papers have found partial regression tobe an adverse prognostic factor,3,5,6 but most of the evi-dence suggests that it has little effect on the risk of meta-static disease.7,8 This is particularly relevant whenconsidering criteria for sentinel node biopsy in thin mela-nomas as it is possible that regression could result in adecreased measurement of Breslow Thickness and there-fore an inappropriately favourable prognosis. The degreeof regression evident histologically, within the primarylesion, appears to be more relevant though with lesionsshowing regression of more than 50e80% appearing todemonstrate an increased propensity to metastasise.9
* Corresponding author.E-mail address: [email protected] (R.J. Bramhall).
0748-7983/$ - see front matter ! 2013 Elsevier Ltd. All rights reserved.http://dx.doi.org/10.1016/j.ejso.2013.09.026
Available online at www.sciencedirect.com
ScienceDirect
EJSO 40 (2014) 34e41 www.ejso.com
doi:10.1016/j.ijrobp.2003.09.012
BIOLOGY CONTRIBUTION
IONIZING RADIATION INHIBITION OF DISTANT UNTREATED TUMORS(ABSCOPAL EFFECT) IS IMMUNE MEDIATED
SANDRA DEMARIA, M.D.,* BRUCE NG, M.S.,† MARY LOUISE DEVITT, A.A.S.,‡ JAMES S. BABB, PH.D.,§NORIKO KAWASHIMA, M.S.,* LEONARD LIEBES, PH.D.,† AND SILVIA C. FORMENTI, M.D.‡
Departments of *Pathology, †Medicine, ‡Radiation Oncology, and §Radiology, New York University School of Medicine,New York, New York
Purpose: Ionizing radiation can reduce tumor growth outside the field of radiation, known as the abscopal effect.Although it has been reported in multiple malignancies, the abscopal effect remains a rare and poorly understoodevent. Ionizing radiation generates inflammatory signals and, in principle, could provide both tumor-specificantigens from dying cells and maturation stimuli that are necessary for dendritic cells’ activation of tumor-specific T cells. We therefore tested the hypothesis that the abscopal effect elicited by radiation is immunemediated. This was directly tested by enhancing the number of available dendritic cells using the growth factorFlt3-Ligand (Flt3-L).Methods and Materials: Mice bearing a syngeneic mammary carcinoma, 67NR, in both flanks were treated withFlt3-L daily for 10 days after local radiation therapy (RT) to only 1 of the 2 tumors at a single dose of 2 or 6 Gy.The second nonirradiated tumor was used as indicator of the abscopal effect. Data were analyzed using repeatedmeasures regression.Results: RT alone led to growth delay exclusively of the irradiated 67NR tumor, as expected. Surprisingly,growth of the nonirradiated tumor was also impaired by the combination of RT and Flt3-L. As control, Flt3-Lhad no effect without RT. Importantly, the abscopal effect was shown to be tumor specific, because growth of anonirradiated A20 lymphoma in the same mice containing a treated 67NR tumor was not affected. Moreover, nogrowth delay of nonirradiated 67NR tumors was observed when T cell deficient (nude) mice were treated withRT plus Flt3-L.Conclusions: These results demonstrate that the abscopal effect is in part immune mediated and that T cells arerequired to mediate distant tumor inhibition induced by radiation. © 2004 Elsevier Inc.
Ionizing radiation, Antitumor immunity, Flt3-Ligand, Dendritic cells, Breast cancer.
INTRODUCTION
Despite improvements in detection and treatment, breastcancer remains a deadly disease for many women. Thetendency of breast cancer cells to spread systemically earlyon in its course requires an effective systemic treatment.The main limitation of currently available treatments is thefailure to eradicate systemic disease, even when the tumor isclinically at an early stage. New treatment strategies areconstantly explored to successfully address this problem. Inthis respect, antitumor immunity may have a unique role,complementary to the use of other currently available mo-dalities of treatment. Cytolytic T cells (CTL) can eliminate
tumor cells with exquisite specificity and efficacy indepen-dently from both their proliferative status and intrinsic che-mosensitivity (reviewed in Ref. 1). Recent advances inunderstanding how the immune system functions allow forthe rational design of new strategies to induce effectiveantitumor immunity by targeting antigens to dendritic cells(DC) (2).Poor immunogenicity of cancer cells often prevents the
development of an effective antitumor immune response.Most cancer cells do not express costimulatory moleculesand, therefore, cannot trigger the activation of naive T cells(3, 4). Tumor-specific antigens need to be “transferred”
Reprint requests to: Sandra Demaria, M.D., Department ofPathology, MSB-563, New York University School of Medicine,550 First Avenue, New York, NY 10016. Tel: (212) 263-7308;Fax: (212) 263-8211; E-mail: [email protected] in part at the 44th Annual Meeting of the American
Society for Therapeutic Radiology and Oncology, New Orleans,LA, October 6–10, 2002.The authors thank Elaine Thomas for Flt3-Ligand. S.D. was
supported by Grant K08 CA89336 from NIH/NCI and by a grantfrom the Speaker’s Fund for Biomedical Research: Toward the
Science of Patient Care, awarded by the city of New York. S.C.F.was supported by Grants DAMD17-01-1-0345 from the Depart-ment of Defense, TURSG CCE 103174 from the American CancerSociety, and by a grant from the Breast Cancer Research Founda-tion.Acknowledgments—The authors thank Dr. R. Schneider for hiscritical input.Received Jan 6, 2003, and in revised form Jul 24, 2003. Ac-
cepted for publication Sep 3, 2003.
Int. J. Radiation Oncology Biol. Phys., Vol. 58, No. 3, pp. 862–870, 2004Copyright © 2004 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/04/$–see front matter
862
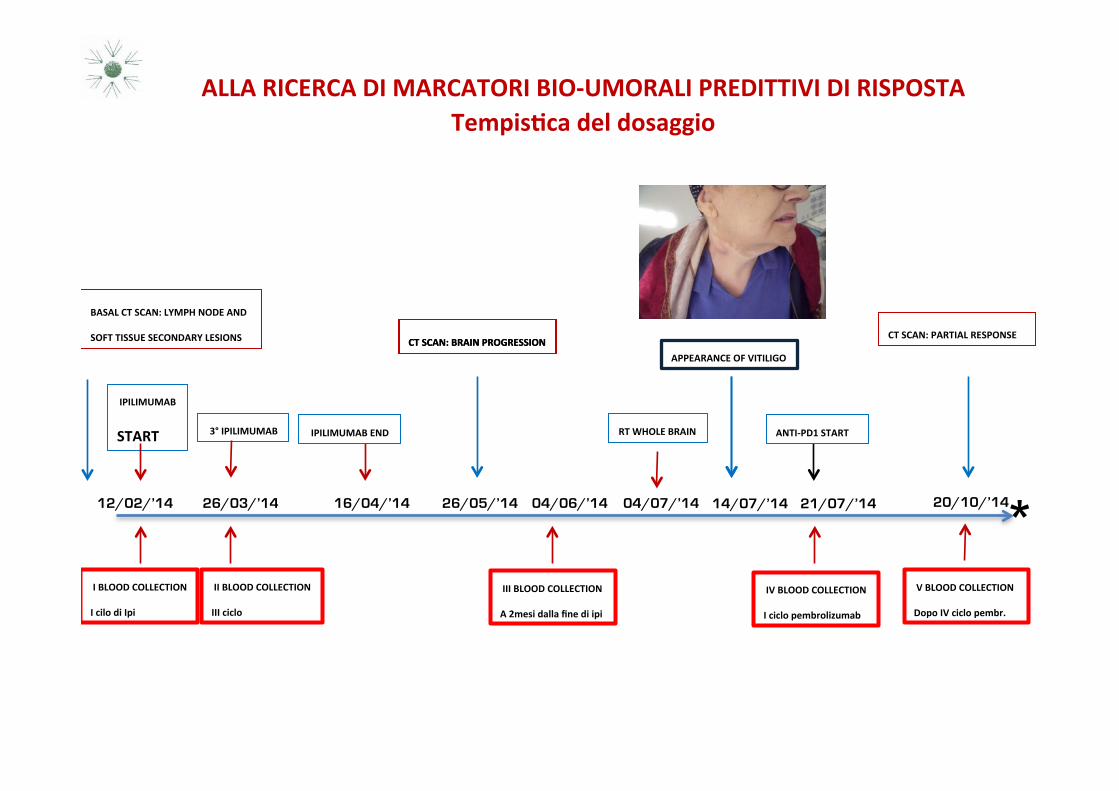
'IPILIMUMAB'
START'
'I'BLOOD'COLLECTION'
I'cilo'di'Ipi'''
12/02/’14) 26/03/’14) 16/04/’14) 26/05/’14)
CT'SCAN:'BRAIN'PROGRESSION'
RT'WHOLE'BRAIN''
04/07/’14) 14/07/’14)04/06/’14)
APPEARANCE'OF'VITILIGO'
21/07/’14) 20/10/’14)*'II'BLOOD'COLLECTION'
III'ciclo'''
'IPILIMUMAB'END'
BASAL'CT'SCAN:'LYMPH'NODE'AND'
SOFT'TISSUE'SECONDARY'LESIONS''
'III'BLOOD'COLLECTION'
A'2mesi'dalla'fine'di'ipi'''
'IV'BLOOD'COLLECTION'
I'ciclo'pembrolizumab'''
ANTIBPD1'START'
CT'SCAN:'BRAIN'PROGRESSION'CT'SCAN:'PARTIAL'RESPONSE'
'V'BLOOD'COLLECTION'
Dopo'IV'ciclo'pembr.'''
'3°'IPILIMUMAB''
ALLA'RICERCA'DI'MARCATORI'BIOBUMORALI'PREDITTIVI'DI'RISPOSTA''Tempis8ca'del'dosaggio''
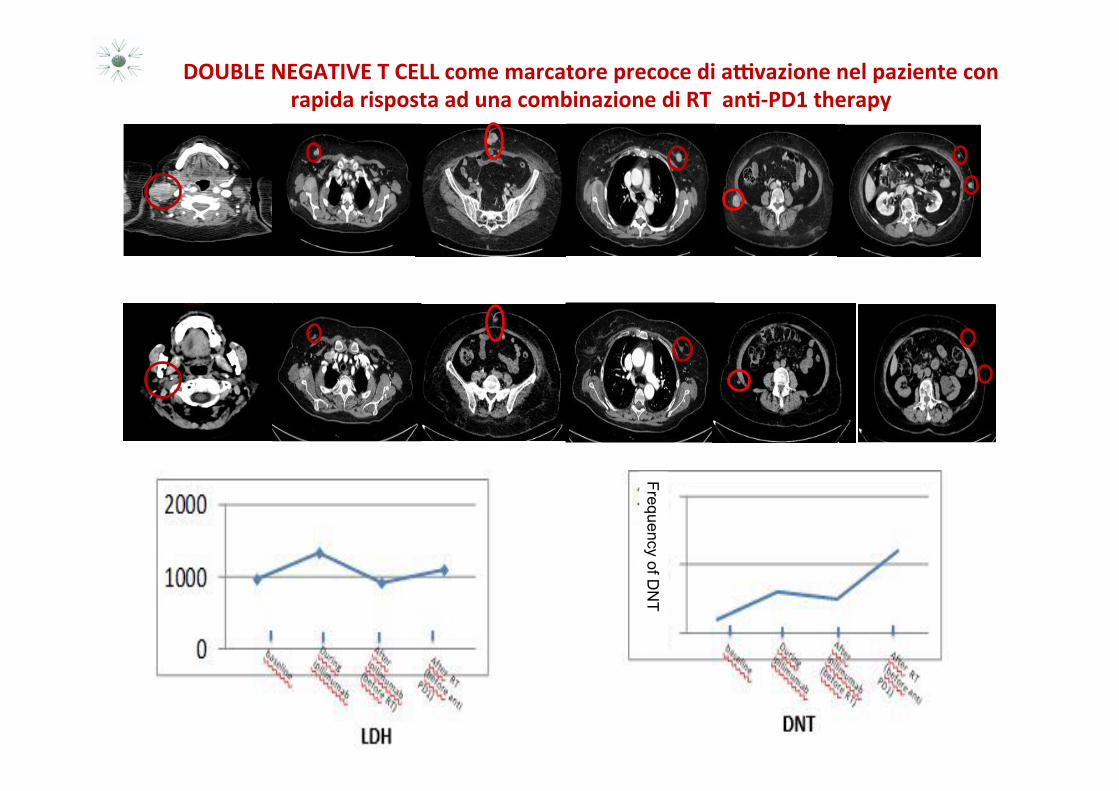
DOUBLE'NEGATIVE'T'CELL'come'marcatore'precoce'di'aDvazione'nel'paziente'con'rapida'risposta'ad'una'combinazione'di'RT''an8BPD1'therapy'
Frequency of DN
T
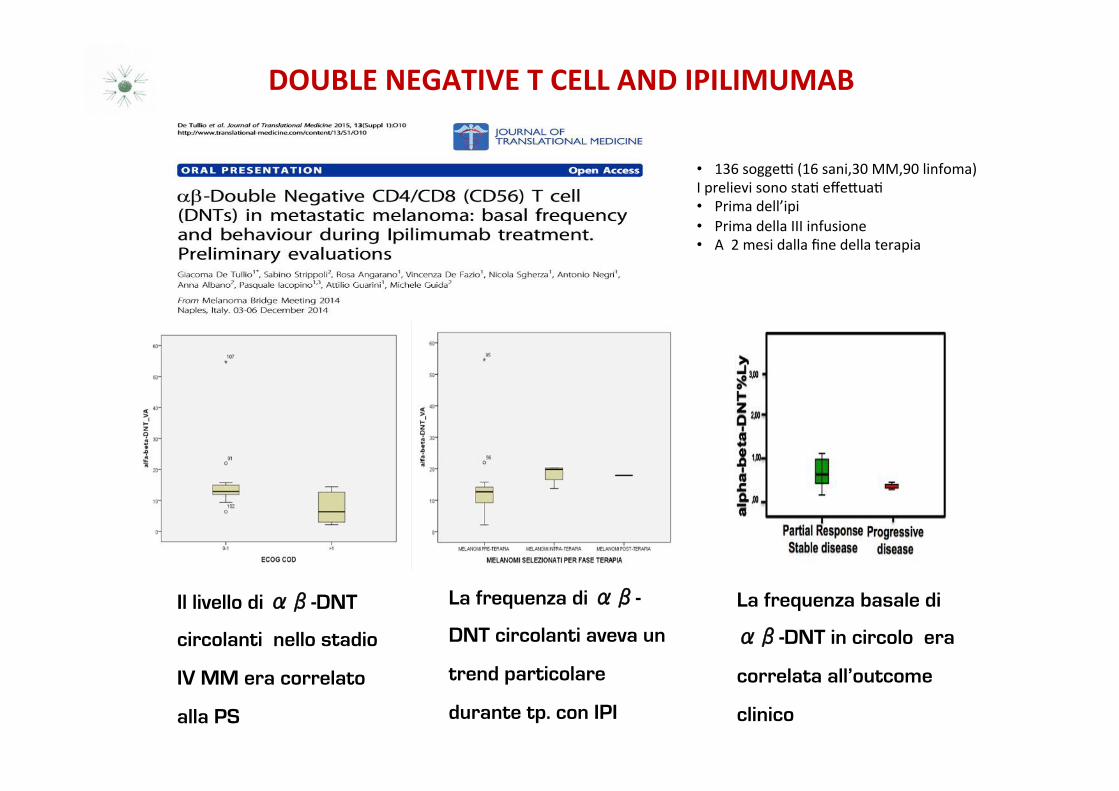
DOUBLE'NEGATIVE'T'CELL'AND'IPILIMUMAB''
!
Il livello di ��-DNT
circolanti nello stadio
IV MM era correlato
alla PS
!
La frequenza di ��-
DNT circolanti aveva un
trend particolare
durante tp. con IPI
La frequenza basale di
��-DNT in circolo era
correlata all’outcome
clinico
• 136)soggeA)(16)sani,30)MM,90)linfoma))I)prelievi)sono)staH)effeSuaH)• Prima)dell’ipi)• Prima)della)III)infusione)• A))2)mesi)dalla)fine)della)terapia)
COSA'INSEGNA'IL'CASO'CLINICO)
• IN) PAZIENTI) CON) METASTASI) CEREBRALI,) L�IMPIEGO) DELLA) RADIOTERAPIA)
NELL�INTERVALLO)TRA)DUE)TRATTAMENTI)IMMUNOTERAPICI) )PU0�)POTENZIARE)
L�ATTIVITA)ANTI+TUMORALE)DI)ENTRAMBI)
'
'
• IL) TIMING) OTTIMALE,) LA) SCHEDULA) DI) OGNI) TRATTAMENTO) E) LA) TECNICA)
MIGLIORE) )PER)OTTENERE) IL)MASSIMO)BENEFICIO)CLINICO)ED) IMMUNOLOGICO)
DEVONO)ANCORA)ESSERE)CHIARITI)DAI)NUMEROSI)TRIALS)CLINICI)IN)CORSO))
COSA'INSEGNA'IL'CASO'CLINICO)
L’IMPIEGO'DI'ALCUNE'STRATEGIE'COMBINATE'È'INFICIATO'da'
aumento'della'tossicità''
risposte'di'breve'durata'
''
I' MECCANISMI' BIOLOGICI' ALLA' BASE' DI' TALE' DIFFERENTE' RISPOSTA' DEVONO'
ESSERE'ULTERIORMENTE'CHIARITI'''
' ' ' ' ' ' ' 'QUINDI'''
' E’' NECESSARIO' RIVALUTARE' I' PARAMETRI' CLINICI,' LABORATORISTICI' E'
IMMUNOLOGICI' 'PER'COMPRENDERE'I'MECCANISMI'CHE'MEDIANO'IL'SINERGISMO'
TRA' IMMUNO' E' RADIOTERAPIA' E' SELEZIONARE* I* PAZIENTI* CANDIDABILI* A* TALE*
SEQUENZA'E'RILEVARE'IN'TEMPO'UNA'BUONA'RISPOSTA'AL'TRATTAMENTO''
Dove*andiamo?*
Grazie))





























