Embed Size (px)
Citation preview
CA R D I O L O G Y A N D CA R D I A C
SU R G E RY RE V I E W S –
Seeking your views
October 2001
Department of Health, Social Services and Public SafetyAn Roinn Sláinte, Seirbhísí Sóisialta agus Sábháilteachta Poiblí
1
Consultation Paper
CARDIOLOGY AND CARDIAC SURGERY REVIEWS -
SEEKING YOUR VIEWS
This consultation pack has been prepared to provide the public, relevant
interest groups and health service staff with information on the outcome of
the cardiology and cardiac surgery reviews and to invite comments on the
reviews and their recommendations.
This consultation process, which will run until 4th January 2002, is being
undertaken to assist the Minister in reaching final decisions on the
implementation of the reports’ recommendations.
2
CARDIOLOGY AND CARDIAC SURGERY
Background
Heart disease remains a major cause of illness and death here. Whilst the numbers of
deaths from this disease continue to fall, rates of coronary artery disease remain higher
than in most European countries.
The best way to deal with the incidence of heart disease in the long term is to assist
people to take life decisions that will reduce their risk of developing the disease. This
preventative approach complements the cardiology and cardiac surgery services,
provided to deliver the necessary range of diagnostic, therapeutic and treatments to
manage and deal with heart disease when it arises.
Our service aim is to provide efficient and effective clinical services, which dovetail
to meet the full range of patients’ needs at the onset of the disease and as it progresses.
It is important that services work as part of a seamless system, a ‘managed clinical
network’ of care, to ensure that patients receive the best possible care in a timely and
sensitive way to minimise the impact of the disease on their lives.
Reviews of Cardiology Services and Cardiac Surgery
Recognising that cardiology and cardiac surgery are rapidly changing clinical fields,
the Department commissioned reviews of both clinical areas, and is now consulting on
the outcome of the reviews.
Cardiology Review
The cardiology review was a professional review, led by Dr Campbell, the Chief
Medical Officer, and completed in 1999. The goal of that professional Review was to
help shape the strategic direction of future services here, including: standards of care
with regard to treatment; location of facilities; and maximization of professional
skills.
3
The cardiac surgery review, also chaired by Dr Campbell, was commissioned in
response to the recent decreasing throughput of patients in cardiac surgery. That
review was completed in September 2001.
The Cardiology Report was written by professionals and primarily aimed at clinicians
working in the field of Cardiology. It was circulated to clinicians at the time, and has
already informed developments in the areas of cardiology intervention.
Recent policy developments have focused on building acute services underpinned by
effective clinical networks. This is now considered crucial to the provision of
modern, clinically and cost effective cardiology services that are accessible to those
who require them. There have also been major developments in the field of
interventional cardiology since the review was first commissioned in 1998.
These factors coupled with other recent initiatives, including the Acute Hospitals
Review, the Ambulance Review and the Review of Cardiac Surgery, have underlined
the transitional nature of the 1999 professional review and highlighted the need for a
further review of adult cardiology services in the next 2-3 years.
The Review of Cardiology Services Report was initially circulated to Boards and
Trusts in 1999. Reflecting the views expressed by the Boards and others, the review
was subsequently linked with a parallel review of Cardiac Surgery, which was
commissioned in 2000.
Cardiac Surgery Review
The Minister commissioned the Cardiac Surgery Review, in response to concerns at
the decreasing numbers of patients undergoing surgery at the regional cardiac surgery
unit in the Royal Victoria Hospital. This reduction could be explained in part by the
increased demand on intensive care facilities in the post-operative period. A
consequence of this has been that fewer people have been able to access surgery and
waiting times have increased significantly.
4
The Review report identifies the significant factors contributing to the decreased
throughput in cardiac surgery. It recommends a number of measures that should be
taken to improve services and to alleviate some of the current pressures. It also looks
forward and anticipates the future demand for cardiac surgery over the forthcoming
years.
This consultation paper brings together the products of the two reviews. The key
principles, outlined in the Cardiac Surgery Review Report, apply to both service areas.
They are that future services must:
• Be patient focused
• Ensure quality outcomes;
• Facilitate timely access
• Ensure equity of access
• Make appropriate use of resources
Subsequent Developments in Cardiology
Since the Report was completed in 1999, there have been significant developments in
both interventional cardiology and provision of service. These include:
• the capacity for coronary angiography has been increased by the establishment
of an Angiography Suite at Altnagelvin Hospital(due to open Autumn 2001);
• the opening of a 3rd Cardiac Catheterisation laboratory at the RVH;
• a regional audit of the provision of Thrombolytic drugs is under way and is due
to report early in 2002;
• an number of initiatives have been taken by Boards, GPs and the NI Chest,
Heart and Stroke Association to increase the availability of defibrillators in the
community;
5
• progress has been made in the utilization of existing cardiac catheterisation labs
to make full use of the existing capacity;
• a number of initiatives have been introduced by General Practitioners to
support people with cardiac disease and promote good health. These include
chronic disease management clinics, smoking cessation clinics, and local
rehabilitation programmes.
Consultation Pack
The Department is now consulting on the findings of the reviews and the
recommendations. To facilitate this process, this paper and the attached documents
have been issued widely as a consultation pack. The pack includes:
Appendix 1 An updated summary of the Cardiology review and revised and
updated recommendations.
Appendix 2 Executive summary of the Cardiac Surgery Review and its
recommendations.
Appendix 3 Joint action Plan, drawing on the key recommendations of the
two reviews.
Appendix 4 An ‘equality issues’ paper
Appendix 5 Glossary
The full documents, outlining the terms of reference of the reviews, their method and
details of the background to their recommendations are available on the Department’s
website: www.dhsspsni.gov.uk.
Consultation process
The Department would welcome comments on the outcome of the two reviews and
the recommendations of the joint Action Plan for their implementation. Recognising
that some of the recommendations have significant resource implications, it should be
6
noted that the speed and approach to implementation will be influenced both by the
outcome of the consultation process and the availability of resources in 2002-03 and
beyond. With this in mind, it would be helpful for comments to cover the relative
priority of recommendations, where appropriate.
Commenting on the Way Forward
In line with its commitment to assess the equality implications of proposals for service
changes, the Department would particularly welcome any comments on the potential
impact of the proposals and Action Plan on those groups of potential service users
identified in equality legislation.
In particular, you may wish to consider the following questions:
• Do you think that the two Reviews have covered the necessary ground?
• What do you feel are the priority areas for action?
• Are there additional actions/recommendations that need to be included
to improve services?
• Are there other actions to improve access to services that should be
taken?
• Is there anything else that can or should be done to promote equality of
access regardless of age, gender or geographic location?
• If the recommendations are implemented what is their potential impact
on other services within the hospital and community sectors?
Any comments should be sent to Tom Reid, Room 111, Dundonald House, Upper
Newtownards Road, Belfast BT4 3SF or e-mailed to him at
[email protected]. Comments should be received by 4th January 2002.
7
If you have any queries about the consultation process or require any further
information, please write to Tom Reid at the above address or ring him tel. 028
90524947.

8

9
Appendix 1
REVIEW OF CARDIOLOGY SERVICES
EXECUTIVE SUMMARY
&
RECOMMENDATIONS
10
REVIEW OF CARDIOLOGY SERVICES
EXECUTIVE SUMMARY
(i) Cardiovascular disease, primarily coronary heart disease, has been a major
cause of death here for many decades and remains the major cause of death
today. Significant efforts to prevent disease and to treat established disease
have, however, resulted in a decrease in the death rates from coronary heart
disease over the past two decades.
(ii) Cardiology is that branch of medicine which deals with the diagnosis and
treatment of heart disease. Many recent developments within cardiology have
improved the treatment of patients with heart disease. In particular, recent
advances in stenting have improved the outlook for patients with blocked
coronary arteries. Public expectations of successful treatments are now higher
than ever.
(iii) Advances in treatments are taking place in tandem with demographic changes.
The number of older people here has been increasing and will continue to do
so. As age is the major risk factor for heart disease, an ageing population will
undoubtedly result in increasing pressures on cardiology services.
(iv) This report sets out recommendations for the strategic direction of future
cardiology services here, including standards of care with regard to treatment,
location of facilities and maximisation of professional skills. It recommends
that a network of cardiology services should be developed and that research
into cardiovascular disease should be strengthened by co-ordinating actions and
developing a database of all research work.
11
CURRENT PROVISION OF SERVICE
Pre Hospital Intervention
(v) Prompt and effective treatment of patients suffering a heart attack can help save
lives and improve long-term outcome. We have a responsive mobile coronary
care service that covers most locations. It provides first line emergency
medical service to patients with acute chest pain. This includes pain relief,
resuscitation and the administration of thrombolytic (clot-busting) drugs.
There has been no regional evaluation of mobile coronary care services.
Non-invasive investigations / Outpatient care
(vi) Non-invasive investigations form a key element in the accurate diagnosis and
management of all forms of cardiac disease and are therefore of critical
importance.
(vii) No patient should have to wait longer than 8 weeks for a cardiology outpatient
appointment. All hospitals providing acute services here conduct a range of
non-invasive cardiology investigations. Demand for cardiology investigations
has increased in recent years and is expected to continue to increase.
(viii) All cardiology units here should provide the range of investigations necessary
to confirm the diagnosis and inform treatment options. Investigations requiring
advanced technology or specialised expertise should be concentrated on sites
where a sufficient number of investigations are conducted and the clinical
expertise is available to support the service.
(ix) Open access to investigations for general practitioners exists in most hospitals.
General practitioners should have managed direct access to a range of
cardiology investigations. Protocols for managed direct access should be
agreed between locally based general practitioners and cardiologists.
12
Interventional Cardiology
(x) Interventional (or invasive) cardiology consists of angiography, the dye test
that is used to view the coronary arteries and percutaneous intervention (PCI),
the treatment of blocked coronary arteries. Treatment may consist of balloon
angioplasty or angioplasty plus the insertion of a stent, designed to keep the
coronary artery open.
(xi) Despite increased activities, waiting times for many procedures continue to
grow, with clear evidence of geographical variation in access to invasive
procedures. Referring doctors should be given details of waiting times by
individual cardiologists and patients should be given the opportunity to join the
shortest waiting list. Following diagnostic angiography, no patient should wait
more than three months for a PCI.
Cardiac rehabilitation
(xii) All patients who suffer a heart attack should be offered cardiac rehabilitation.
Cardiac rehabilitation services are aimed at all patients with established heart
disease, to facilitate physical, psychological and emotional recovery and enable
patients to achieve and maintain better health.
(xiii) Rehabilitation programmes should adopt a multi-disciplinary approach and
opportunities should be maximised for the voluntary and statutory sector to
work collaboratively to deliver rehabilitation programmes.

13
THE FUTURE OF CARDIOLOGY SERVICES
(xiv) A managed clinical network should be developed for cardiology services The
network should emphasise partnership, effective use of resources and
maximising the quality of service to patients. The use of information
technology should be maximised within a network, particularly where it
improves patient access to a rapid diagnosis (for example when cardiologists
assess ECGs transmitted electronically and provide advice to primary care
professions).
14
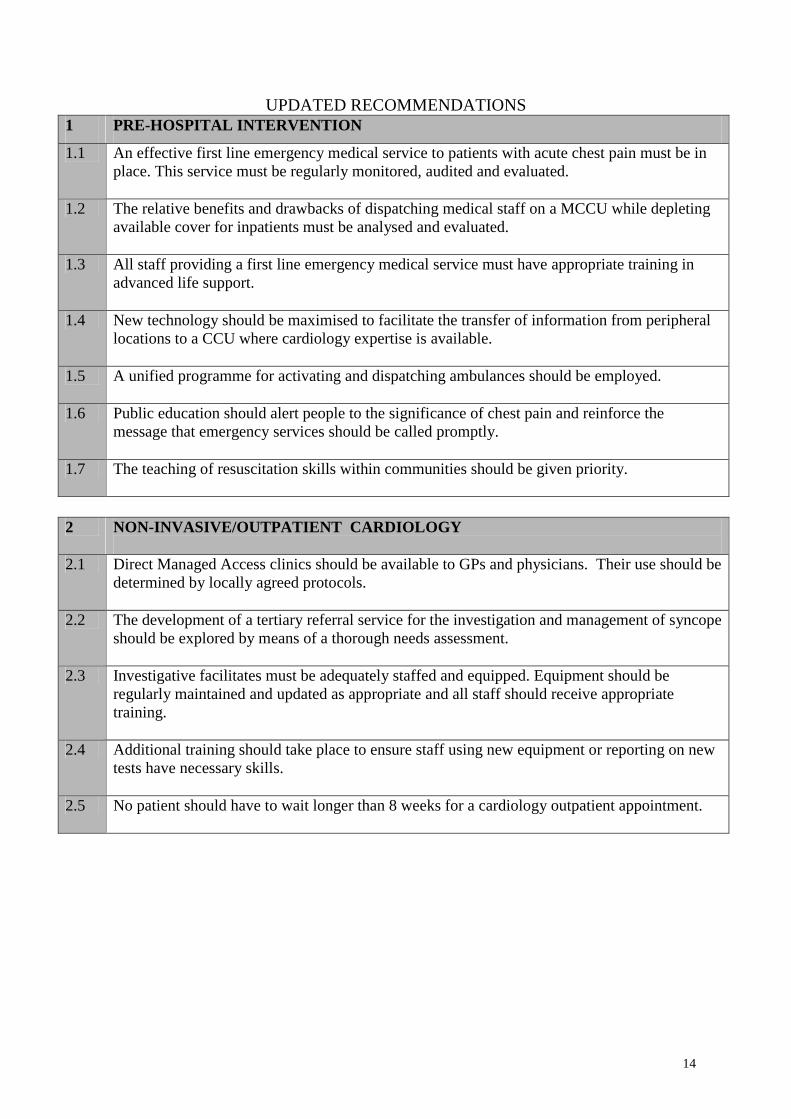
UPDATED RECOMMENDATIONS 1 PRE-HOSPITAL INTERVENTION
1.1 An effective first line emergency medical service to patients with acute chest pain must be in place. This service must be regularly monitored, audited and evaluated.
1.2 The relative benefits and drawbacks of dispatching medical staff on a MCCU while depleting available cover for inpatients must be analysed and evaluated.
1.3 All staff providing a first line emergency medical service must have appropriate training in advanced life support.
1.4 New technology should be maximised to facilitate the transfer of information from peripheral locations to a CCU where cardiology expertise is available.
1.5 A unified programme for activating and dispatching ambulances should be employed.
1.6 Public education should alert people to the significance of chest pain and reinforce the message that emergency services should be called promptly.
1.7 The teaching of resuscitation skills within communities should be given priority.
2 NON-INVASIVE/OUTPATIENT CARDIOLOGY
2.1 Direct Managed Access clinics should be available to GPs and physicians. Their use should be
determined by locally agreed protocols.
2.2 The development of a tertiary referral service for the investigation and management of syncope should be explored by means of a thorough needs assessment.
2.3 Investigative facilitates must be adequately staffed and equipped. Equipment should be regularly maintained and updated as appropriate and all staff should receive appropriate training.
2.4 Additional training should take place to ensure staff using new equipment or reporting on new tests have necessary skills.
2.5 No patient should have to wait longer than 8 weeks for a cardiology outpatient appointment.
15
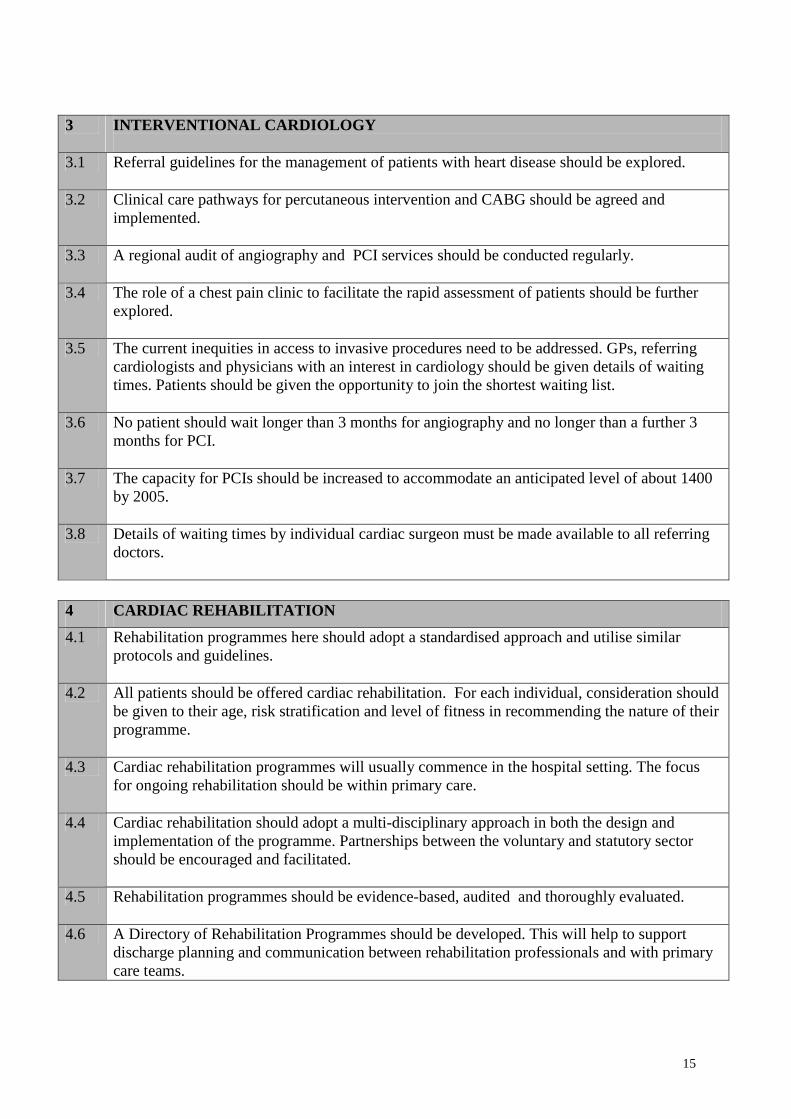
3 INTERVENTIONAL CARDIOLOGY
3.1 Referral guidelines for the management of patients with heart disease should be explored.
3.2 Clinical care pathways for percutaneous intervention and CABG should be agreed and
implemented.
3.3 A regional audit of angiography and PCI services should be conducted regularly.
3.4 The role of a chest pain clinic to facilitate the rapid assessment of patients should be further explored.
3.5 The current inequities in access to invasive procedures need to be addressed. GPs, referring cardiologists and physicians with an interest in cardiology should be given details of waiting times. Patients should be given the opportunity to join the shortest waiting list.
3.6 No patient should wait longer than 3 months for angiography and no longer than a further 3 months for PCI.
3.7 The capacity for PCIs should be increased to accommodate an anticipated level of about 1400 by 2005.
3.8 Details of waiting times by individual cardiac surgeon must be made available to all referring doctors.
4 CARDIAC REHABILITATION
4.1 Rehabilitation programmes here should adopt a standardised approach and utilise similar protocols and guidelines.
4.2 All patients should be offered cardiac rehabilitation. For each individual, consideration should be given to their age, risk stratification and level of fitness in recommending the nature of their programme.
4.3 Cardiac rehabilitation programmes will usually commence in the hospital setting. The focus for ongoing rehabilitation should be within primary care.
4.4 Cardiac rehabilitation should adopt a multi-disciplinary approach in both the design and implementation of the programme. Partnerships between the voluntary and statutory sector should be encouraged and facilitated.
4.5 Rehabilitation programmes should be evidence-based, audited and thoroughly evaluated.
4.6 A Directory of Rehabilitation Programmes should be developed. This will help to support discharge planning and communication between rehabilitation professionals and with primary care teams.
16
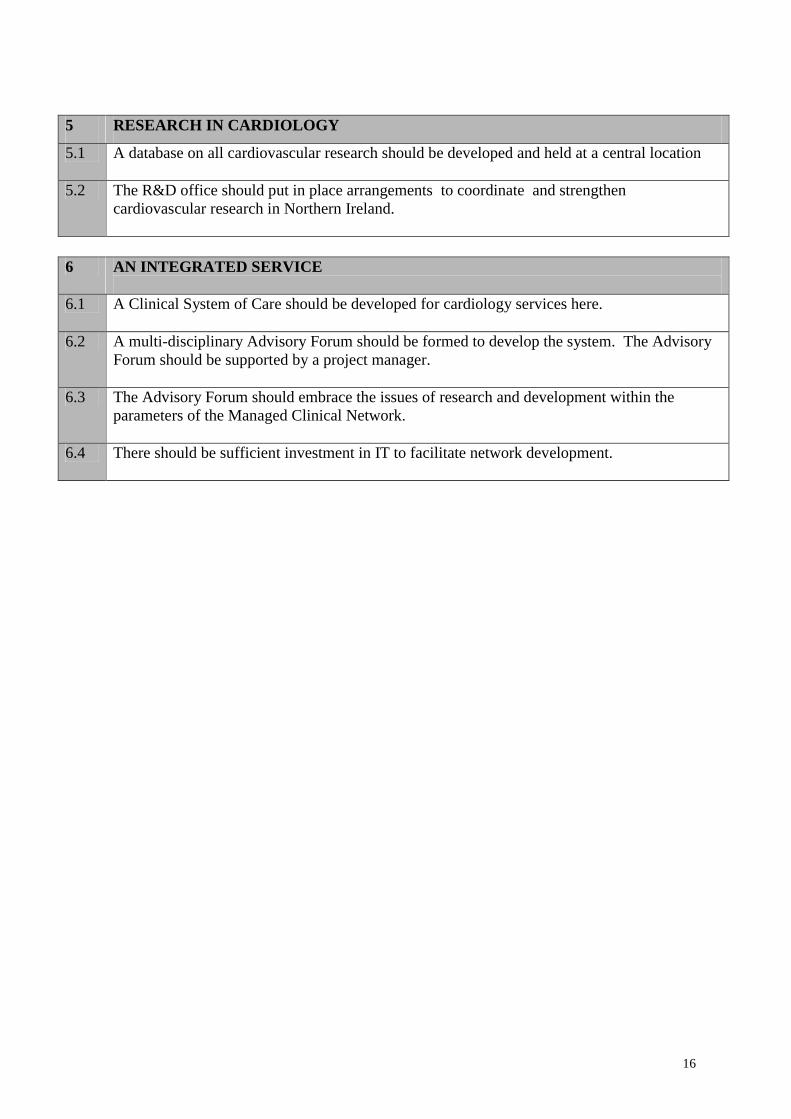
5 RESEARCH IN CARDIOLOGY
5.1 A database on all cardiovascular research should be developed and held at a central location
5.2 The R&D office should put in place arrangements to coordinate and strengthen cardiovascular research in Northern Ireland.
6 AN INTEGRATED SERVICE
6.1 A Clinical System of Care should be developed for cardiology services here.
6.2 A multi-disciplinary Advisory Forum should be formed to develop the system. The Advisory
Forum should be supported by a project manager.
6.3 The Advisory Forum should embrace the issues of research and development within the parameters of the Managed Clinical Network.
6.4 There should be sufficient investment in IT to facilitate network development.

17
Appendix 2
CARDIAC SURGERY REVIEW
EXECUTIVE SUMMARY
&
RECOMMENDATIONS
18
REVIEW OF CARDIAC SURGERY
EXECUTIVE SUMMARY
(i) Heart disease remains a major cause of death and illness here, where rates are
higher than almost all other places in Europe. For a proportion of patients with
heart disease surgery provides a means to relieve symptoms and improve
quality of life.
(ii) Developments in the field of cardiology and cardiac surgery now mean that
much more can be done to treat people with heart disease. In turn, public
expectations of successful treatments are now higher than before.
(iii) Cardiac surgery services at the Royal Victoria Hospital (the Royal) have, for
the past few years, been under considerable pressure. Much of this pressure is
due to an increased demand on intensive care facilities in the post-operative
period. This has in turn resulted in fewer people being able to access surgery
and consequently the waiting time for surgery has been increasing.
(iv) This report identifies the significant factors contributing to the decreased
throughput in cardiac surgery. It recommends a number of measures that
should be taken to improve services and to alleviate some of the current
pressures. It also anticipates the future demand for cardiac surgery over the
forthcoming years.
(v) Cardiac surgery is provided by a dedicated and committed team of highly
skilled professionals at the Royal Victoria Hospital. Without exception
patients spoke highly of the care they received and commended staff for their
hard work and dedication to the service. Building on the strengths of the
19
current service is a key principle in striving for excellence within cardiac
surgery.
IMPROVING CURRENT SERVICES
(vi) Cardiac surgery should be a patient-centred service. Measures to ensure that
patients are well informed partners in the decision-making process are
recommended. For example, patients referred for or awaiting surgery should
be kept fully informed of waiting time and expected date for surgery. Clearly
designated responsibility for the management of the waiting list, admission
procedures and follow up is recommended.
(vii) A patient’s pathway to cardiac surgery is relatively complex, typically
involving a number of hospital visits and several investigations before they are
placed on the waiting list for surgery. The referral mechanism needs to be
simplified with direct referral from cardiologist to cardiac surgeon replacing
current procedures. It is important that all patients are prioritised on agreed
clinical criteria and undergo surgery within the waiting time appropriate to
their clinical need.
(viii) No patient should wait longer than 8 weeks for a cardiac surgery outpatient
appointment and by 2003 they should have had surgery within 12 months of
attending outpatients. Regularly updated and accurate waiting times for each
cardiac surgeon should be made available to referring cardiologists.
(ix) Following surgery, patients are transferred to the cardiac surgery intensive care
unit (CSICU). A number of steps, some of which have already been initiated,
are recommended that would improve both the efficiency and effectiveness of
patient care in CSICU. These include the application of agreed clinical
protocols for patient management the introduction of fast tracking for suitable
patients and improving medical cover especially anaesthetic cover to the unit.
20
(x) Staffing levels, particularly nurse staffing, are the major underlying problem in
the cardiac surgery unit and are directly responsible for the unit’s difficulty in
functioning at optimal capacity. Recruiting and retaining nurses presents a
major challenge. Stressful work load, long working hours, poor morale and
inadequate levels of remuneration all contribute to recruitment and retention
problems. This report recommends immediate action to enhance nurse staffing
levels, review remuneration, and strengthen medical support to the cardiac
surgery unit.
(xi) A multidisciplinary team (MDT) approach is critical in cardiac surgery. The
MDT should meet regularly to provide the opportunity for staff to share
information, discuss relevant issues and review practices and procedures.
(xii) Other factors will also play a role in strengthening the service. Integrating
cardiac and thoracic surgery would provide opportunities to improve patient
management and this should be actively pursued. Overcoming some of the
physical obstacles such as having intensive care and high dependency care
facilities adjacent to one another would make services more manageable.
FUTURE SERVICES
(xiii) Our cardiac surgery rates and in particular our rates of coronary artery
bypassing (CABG) were close to the European average of 429 per million in
1999. Intervention rates, however, vary from country to country. This poses
the question as to the appropriate level of surgery. In England the National
Service Framework for Coronary Heart Disease (NSF) have proposed an
increase in CABG to 750 per million. We will need to keep under constant
review the surgical provision indicated for our population.
21
(xv) The rapid developments within cardiology will undoubtedly influence the
demand for cardiac surgery. The percutaneous intervention (PCI) rate will
continue to increase over the next few years with little change anticipated in the
need for CABG surgery.
(xvi) As a priority the number of CABG procedures must be increased to the current
target of 800 and waiting times for surgery must be decreased. While the
Royal are increasing the number of CABG procedures there will remain a need
to send patients elsewhere for surgery in the short to medium term if the
waiting list is to be brought under control.
(xvii) This report does not address the provision of paediatric cardiac surgery in
detail. Decisions regarding this will be deferred until the National Review of
Paediatric and Congenital Cardiac Services has been completed. Any changes
in the provision of PCS will have an impact on adult services, which will then
need to be reassessed in light of developments. This will include the need to
explore opportunities for North South collaboration in the delivery of care.
(xviii) Data collection, rigorous local audit and participation in national audit is
essential in ensuring a high quality service. The results of audit should be
made widely available.
(xix) A high quality of cardiac surgery is provided at the Royal. Recommendations
contained in this report aim to strengthen the quality of current services and to
ensure that, as a highly respected regional service, cardiac surgery will
continue to meet the needs of the community.
22
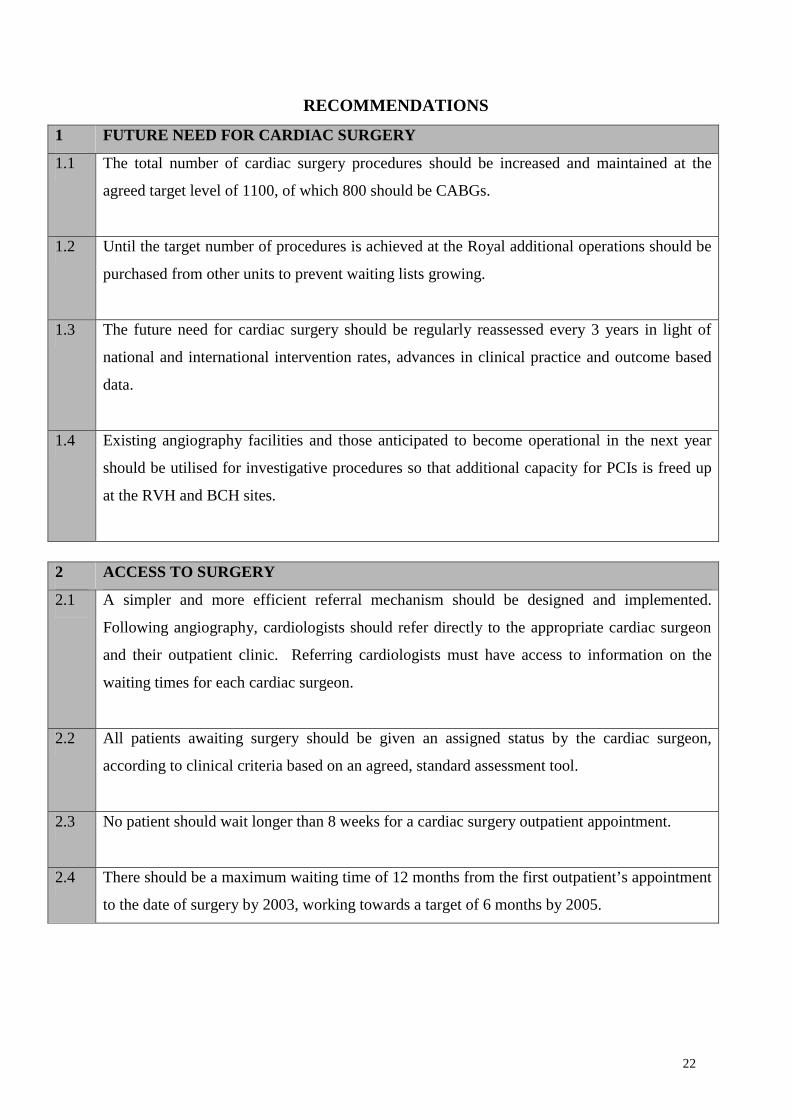
RECOMMENDATIONS 1 FUTURE NEED FOR CARDIAC SURGERY
1.1 The total number of cardiac surgery procedures should be increased and maintained at the
agreed target level of 1100, of which 800 should be CABGs.
1.2 Until the target number of procedures is achieved at the Royal additional operations should be
purchased from other units to prevent waiting lists growing.
1.3 The future need for cardiac surgery should be regularly reassessed every 3 years in light of
national and international intervention rates, advances in clinical practice and outcome based
data.
1.4 Existing angiography facilities and those anticipated to become operational in the next year
should be utilised for investigative procedures so that additional capacity for PCIs is freed up
at the RVH and BCH sites.
2 ACCESS TO SURGERY
2.1 A simpler and more efficient referral mechanism should be designed and implemented.
Following angiography, cardiologists should refer directly to the appropriate cardiac surgeon
and their outpatient clinic. Referring cardiologists must have access to information on the
waiting times for each cardiac surgeon.
2.2 All patients awaiting surgery should be given an assigned status by the cardiac surgeon,
according to clinical criteria based on an agreed, standard assessment tool.
2.3 No patient should wait longer than 8 weeks for a cardiac surgery outpatient appointment.
2.4 There should be a maximum waiting time of 12 months from the first outpatient’s appointment
to the date of surgery by 2003, working towards a target of 6 months by 2005.
23
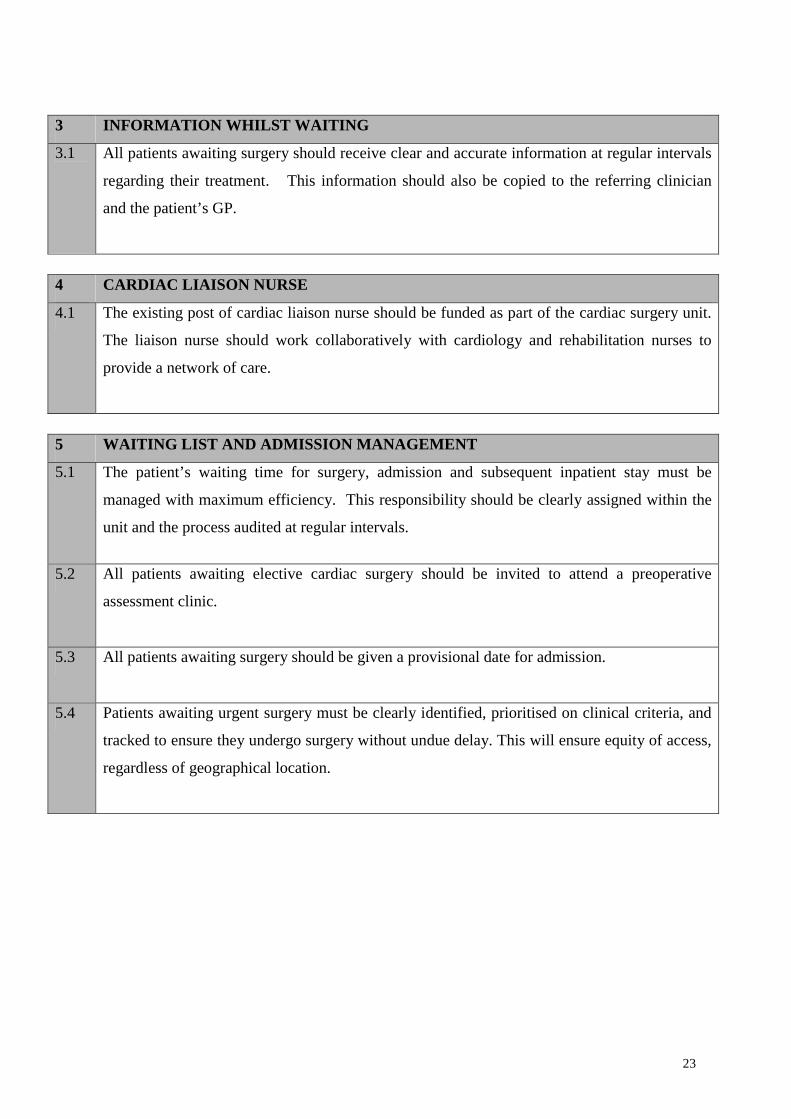
3 INFORMATION WHILST WAITING
3.1 All patients awaiting surgery should receive clear and accurate information at regular intervals
regarding their treatment. This information should also be copied to the referring clinician
and the patient’s GP.
4 CARDIAC LIAISON NURSE
4.1 The existing post of cardiac liaison nurse should be funded as part of the cardiac surgery unit.
The liaison nurse should work collaboratively with cardiology and rehabilitation nurses to
provide a network of care.
5 WAITING LIST AND ADMISSION MANAGEMENT
5.1 The patient’s waiting time for surgery, admission and subsequent inpatient stay must be
managed with maximum efficiency. This responsibility should be clearly assigned within the
unit and the process audited at regular intervals.
5.2 All patients awaiting elective cardiac surgery should be invited to attend a preoperative
assessment clinic.
5.3 All patients awaiting surgery should be given a provisional date for admission.
5.4 Patients awaiting urgent surgery must be clearly identified, prioritised on clinical criteria, and
tracked to ensure they undergo surgery without undue delay. This will ensure equity of access,
regardless of geographical location.
24
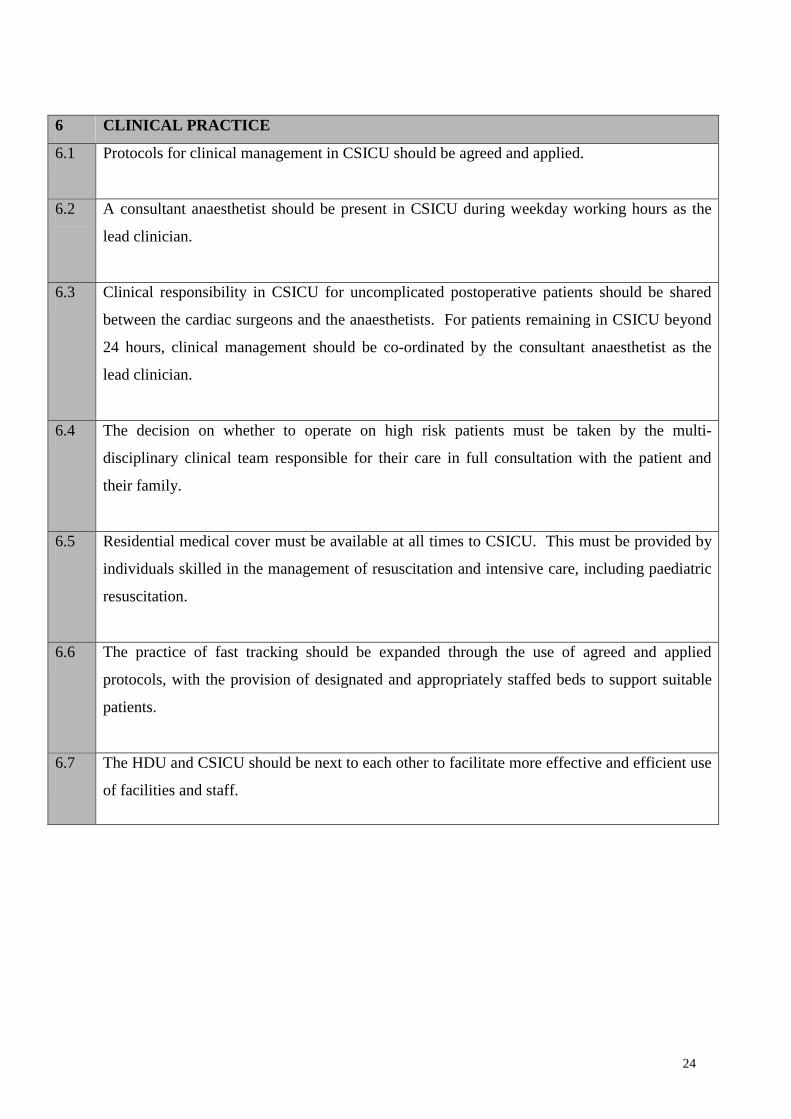
6 CLINICAL PRACTICE
6.1 Protocols for clinical management in CSICU should be agreed and applied.
6.2 A consultant anaesthetist should be present in CSICU during weekday working hours as the
lead clinician.
6.3 Clinical responsibility in CSICU for uncomplicated postoperative patients should be shared
between the cardiac surgeons and the anaesthetists. For patients remaining in CSICU beyond
24 hours, clinical management should be co-ordinated by the consultant anaesthetist as the
lead clinician.
6.4 The decision on whether to operate on high risk patients must be taken by the multi-
disciplinary clinical team responsible for their care in full consultation with the patient and
their family.
6.5 Residential medical cover must be available at all times to CSICU. This must be provided by
individuals skilled in the management of resuscitation and intensive care, including paediatric
resuscitation.
6.6 The practice of fast tracking should be expanded through the use of agreed and applied
protocols, with the provision of designated and appropriately staffed beds to support suitable
patients.
6.7 The HDU and CSICU should be next to each other to facilitate more effective and efficient use
of facilities and staff.
25
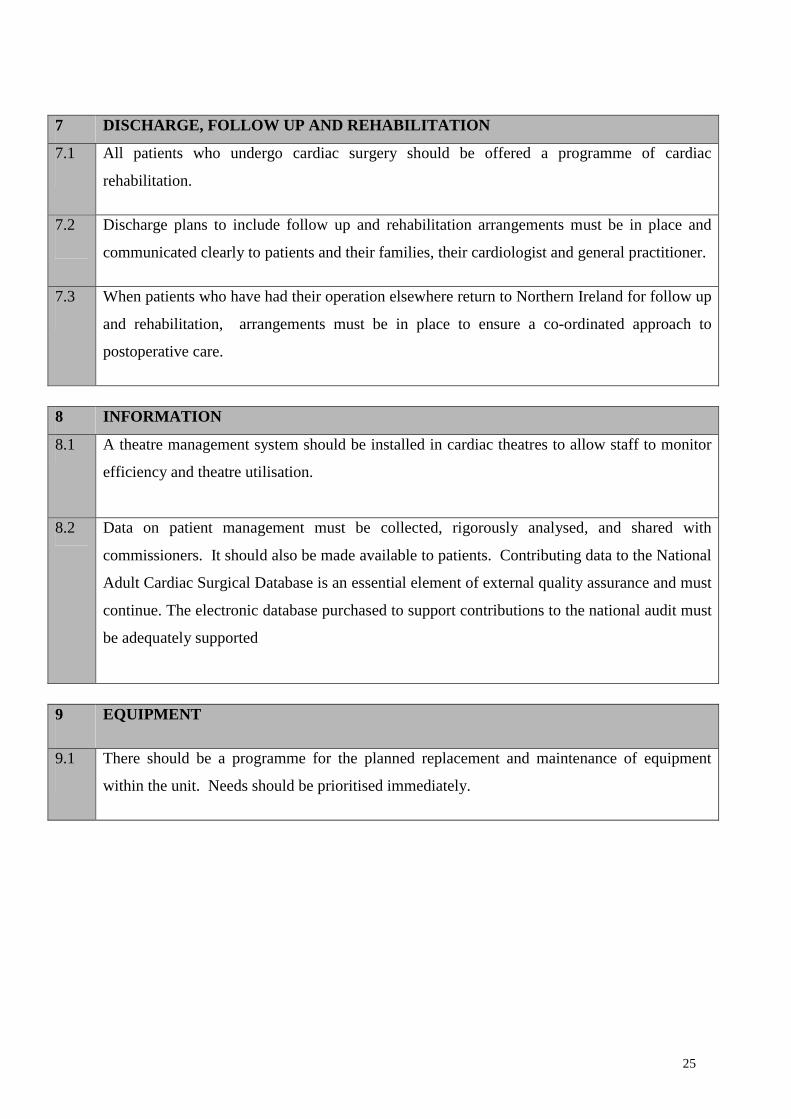
7 DISCHARGE, FOLLOW UP AND REHABILITATION
7.1 All patients who undergo cardiac surgery should be offered a programme of cardiac
rehabilitation.
7.2 Discharge plans to include follow up and rehabilitation arrangements must be in place and
communicated clearly to patients and their families, their cardiologist and general practitioner.
7.3 When patients who have had their operation elsewhere return to Northern Ireland for follow up
and rehabilitation, arrangements must be in place to ensure a co-ordinated approach to
postoperative care.
8 INFORMATION
8.1 A theatre management system should be installed in cardiac theatres to allow staff to monitor
efficiency and theatre utilisation.
8.2 Data on patient management must be collected, rigorously analysed, and shared with
commissioners. It should also be made available to patients. Contributing data to the National
Adult Cardiac Surgical Database is an essential element of external quality assurance and must
continue. The electronic database purchased to support contributions to the national audit must
be adequately supported
9 EQUIPMENT
9.1 There should be a programme for the planned replacement and maintenance of equipment
within the unit. Needs should be prioritised immediately.
26
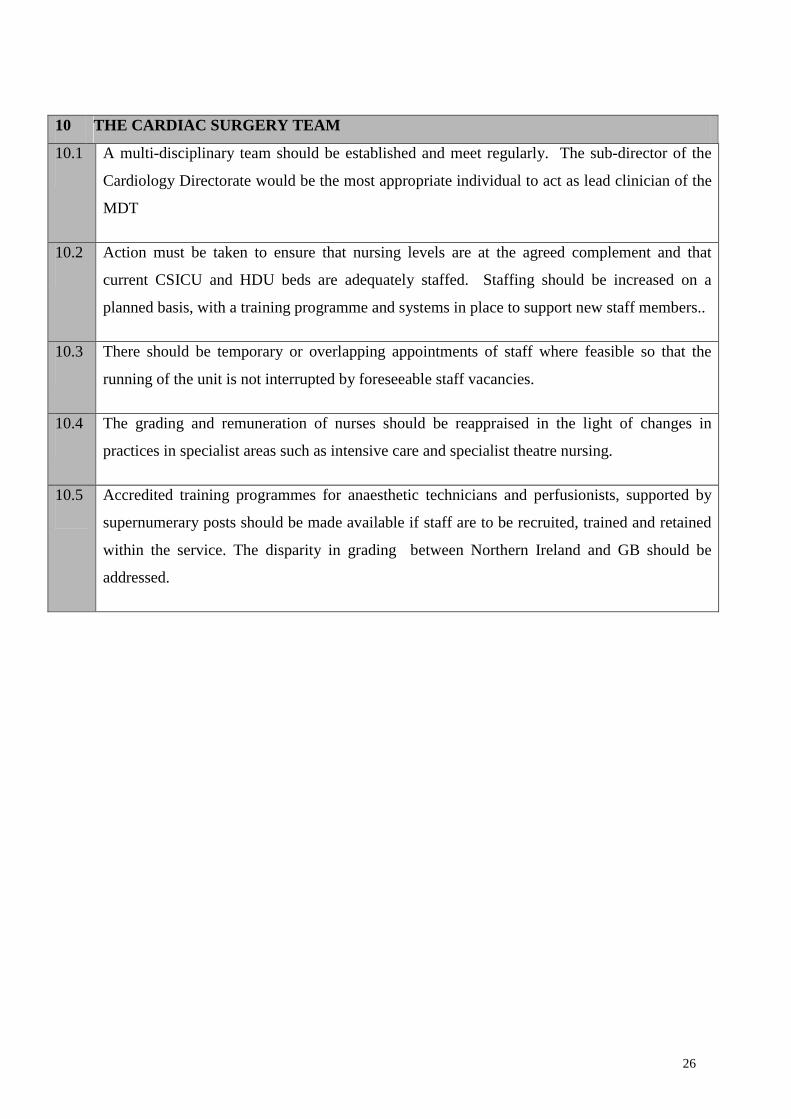
10 THE CARDIAC SURGERY TEAM
10.1 A multi-disciplinary team should be established and meet regularly. The sub-director of the
Cardiology Directorate would be the most appropriate individual to act as lead clinician of the
MDT
10.2 Action must be taken to ensure that nursing levels are at the agreed complement and that
current CSICU and HDU beds are adequately staffed. Staffing should be increased on a
planned basis, with a training programme and systems in place to support new staff members..
10.3 There should be temporary or overlapping appointments of staff where feasible so that the
running of the unit is not interrupted by foreseeable staff vacancies.
10.4 The grading and remuneration of nurses should be reappraised in the light of changes in
practices in specialist areas such as intensive care and specialist theatre nursing.
10.5 Accredited training programmes for anaesthetic technicians and perfusionists, supported by
supernumerary posts should be made available if staff are to be recruited, trained and retained
within the service. The disparity in grading between Northern Ireland and GB should be
addressed.
27
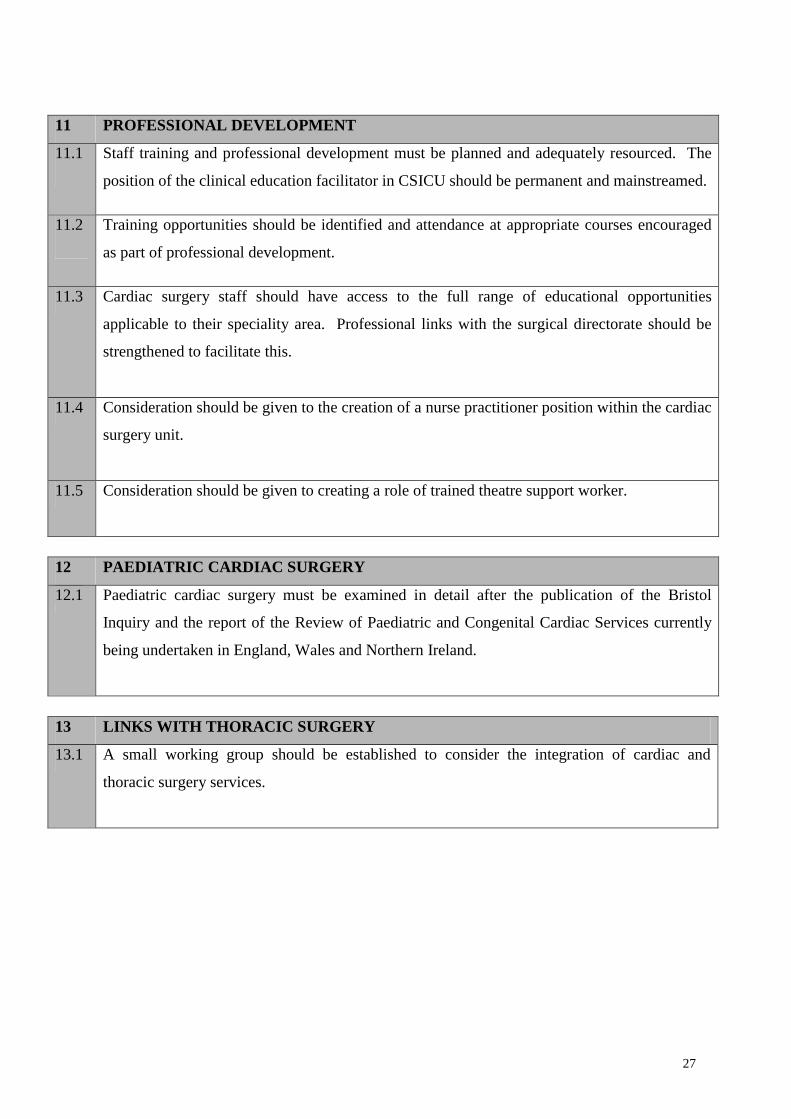
11 PROFESSIONAL DEVELOPMENT
11.1 Staff training and professional development must be planned and adequately resourced. The
position of the clinical education facilitator in CSICU should be permanent and mainstreamed.
11.2 Training opportunities should be identified and attendance at appropriate courses encouraged
as part of professional development.
11.3 Cardiac surgery staff should have access to the full range of educational opportunities
applicable to their speciality area. Professional links with the surgical directorate should be
strengthened to facilitate this.
11.4 Consideration should be given to the creation of a nurse practitioner position within the cardiac
surgery unit.
11.5 Consideration should be given to creating a role of trained theatre support worker.
12 PAEDIATRIC CARDIAC SURGERY
12.1 Paediatric cardiac surgery must be examined in detail after the publication of the Bristol
Inquiry and the report of the Review of Paediatric and Congenital Cardiac Services currently
being undertaken in England, Wales and Northern Ireland.
13 LINKS WITH THORACIC SURGERY
13.1 A small working group should be established to consider the integration of cardiac and
thoracic surgery services.

28
29
Appendix 3
CARDIOLOGY
&
CARDIAC SURGERY
JOINT ACTION PLAN
30
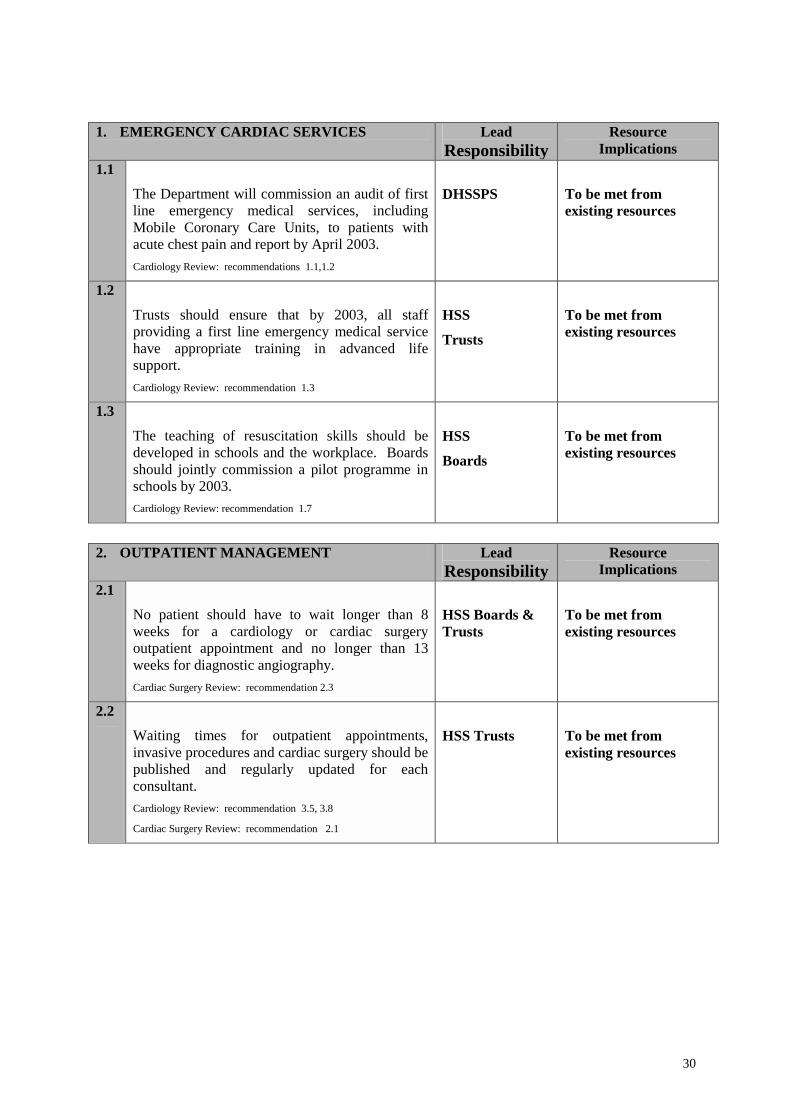
1. EMERGENCY CARDIAC SERVICES Lead Responsibility
Resource Implications
1.1
The Department will commission an audit of first line emergency medical services, including Mobile Coronary Care Units, to patients with acute chest pain and report by April 2003. Cardiology Review: recommendations 1.1,1.2
DHSSPS
To be met from existing resources
1.2
Trusts should ensure that by 2003, all staff providing a first line emergency medical service have appropriate training in advanced life support. Cardiology Review: recommendation 1.3
HSS
Trusts
To be met from existing resources
1.3
The teaching of resuscitation skills should be developed in schools and the workplace. Boards should jointly commission a pilot programme in schools by 2003. Cardiology Review: recommendation 1.7
HSS
Boards
To be met from existing resources
2. OUTPATIENT MANAGEMENT Lead
Responsibility Resource
Implications 2.1
No patient should have to wait longer than 8 weeks for a cardiology or cardiac surgery outpatient appointment and no longer than 13 weeks for diagnostic angiography. Cardiac Surgery Review: recommendation 2.3
HSS Boards & Trusts
To be met from existing resources
2.2
Waiting times for outpatient appointments, invasive procedures and cardiac surgery should be published and regularly updated for each consultant. Cardiology Review: recommendation 3.5, 3.8
Cardiac Surgery Review: recommendation 2.1
HSS Trusts
To be met from existing resources
31
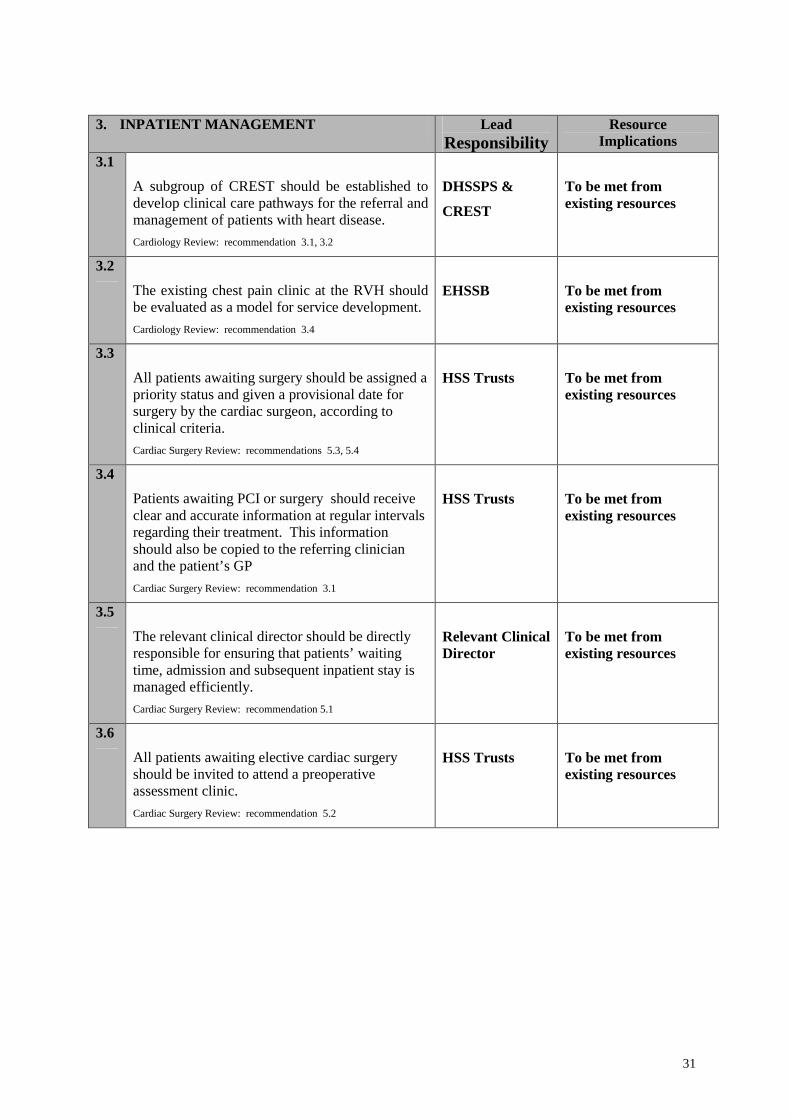
3. INPATIENT MANAGEMENT Lead
Responsibility Resource
Implications 3.1
A subgroup of CREST should be established to develop clinical care pathways for the referral and management of patients with heart disease. Cardiology Review: recommendation 3.1, 3.2
DHSSPS &
CREST
To be met from existing resources
3.2
The existing chest pain clinic at the RVH should be evaluated as a model for service development. Cardiology Review: recommendation 3.4
EHSSB
To be met from existing resources
3.3
All patients awaiting surgery should be assigned a priority status and given a provisional date for surgery by the cardiac surgeon, according to clinical criteria. Cardiac Surgery Review: recommendations 5.3, 5.4
HSS Trusts
To be met from existing resources
3.4
Patients awaiting PCI or surgery should receive clear and accurate information at regular intervals regarding their treatment. This information should also be copied to the referring clinician and the patient’s GP Cardiac Surgery Review: recommendation 3.1
HSS Trusts
To be met from existing resources
3.5
The relevant clinical director should be directly responsible for ensuring that patients’ waiting time, admission and subsequent inpatient stay is managed efficiently. Cardiac Surgery Review: recommendation 5.1
Relevant Clinical Director
To be met from existing resources
3.6
All patients awaiting elective cardiac surgery should be invited to attend a preoperative assessment clinic. Cardiac Surgery Review: recommendation 5.2
HSS Trusts
To be met from existing resources
32
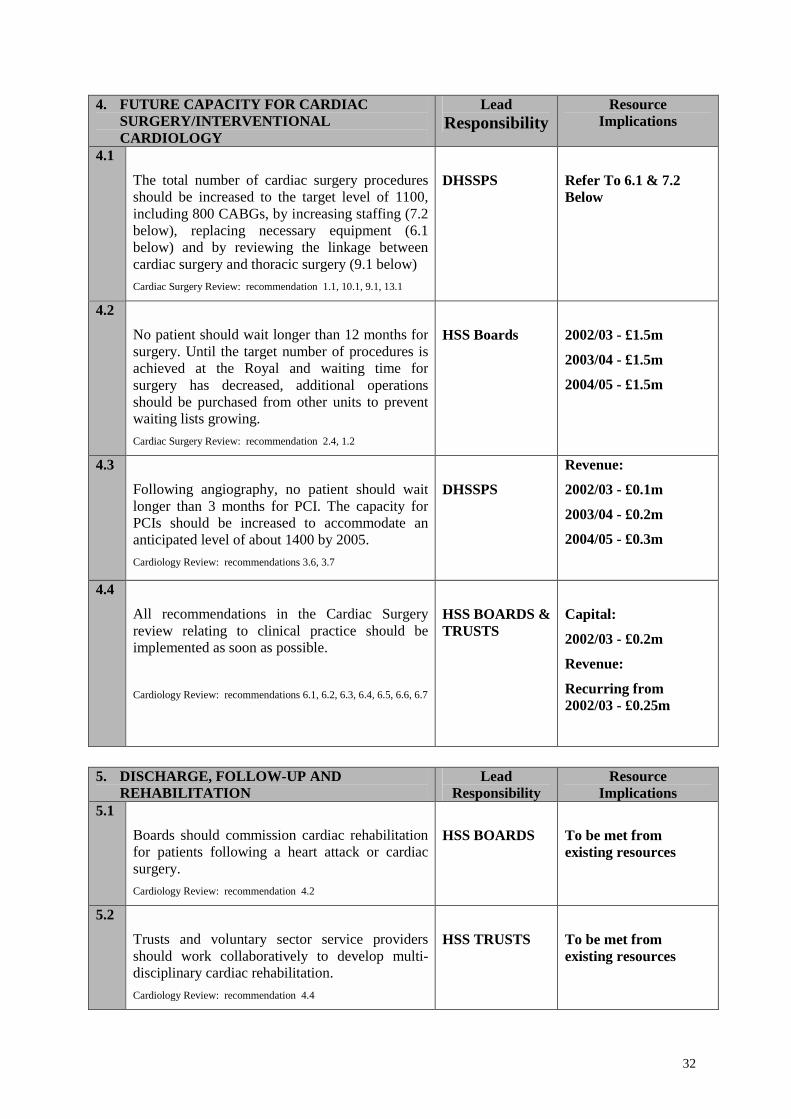
4. FUTURE CAPACITY FOR CARDIAC SURGERY/INTERVENTIONAL CARDIOLOGY
Lead Responsibility
Resource Implications
4.1
The total number of cardiac surgery procedures should be increased to the target level of 1100, including 800 CABGs, by increasing staffing (7.2 below), replacing necessary equipment (6.1 below) and by reviewing the linkage between cardiac surgery and thoracic surgery (9.1 below) Cardiac Surgery Review: recommendation 1.1, 10.1, 9.1, 13.1
DHSSPS
Refer To 6.1 & 7.2 Below
4.2
No patient should wait longer than 12 months for surgery. Until the target number of procedures is achieved at the Royal and waiting time for surgery has decreased, additional operations should be purchased from other units to prevent waiting lists growing. Cardiac Surgery Review: recommendation 2.4, 1.2
HSS Boards
2002/03 - £1.5m
2003/04 - £1.5m
2004/05 - £1.5m
4.3
Following angiography, no patient should wait longer than 3 months for PCI. The capacity for PCIs should be increased to accommodate an anticipated level of about 1400 by 2005. Cardiology Review: recommendations 3.6, 3.7
DHSSPS
Revenue:
2002/03 - £0.1m
2003/04 - £0.2m
2004/05 - £0.3m
4.4
All recommendations in the Cardiac Surgery review relating to clinical practice should be implemented as soon as possible.
Cardiology Review: recommendations 6.1, 6.2, 6.3, 6.4, 6.5, 6.6, 6.7
HSS BOARDS & TRUSTS
Capital:
2002/03 - £0.2m
Revenue:
Recurring from 2002/03 - £0.25m
5. DISCHARGE, FOLLOW-UP AND
REHABILITATION Lead
Responsibility Resource
Implications 5.1
Boards should commission cardiac rehabilitation for patients following a heart attack or cardiac surgery. Cardiology Review: recommendation 4.2
HSS BOARDS
To be met from existing resources
5.2
Trusts and voluntary sector service providers should work collaboratively to develop multi-disciplinary cardiac rehabilitation. Cardiology Review: recommendation 4.4
HSS TRUSTS
To be met from existing resources
33
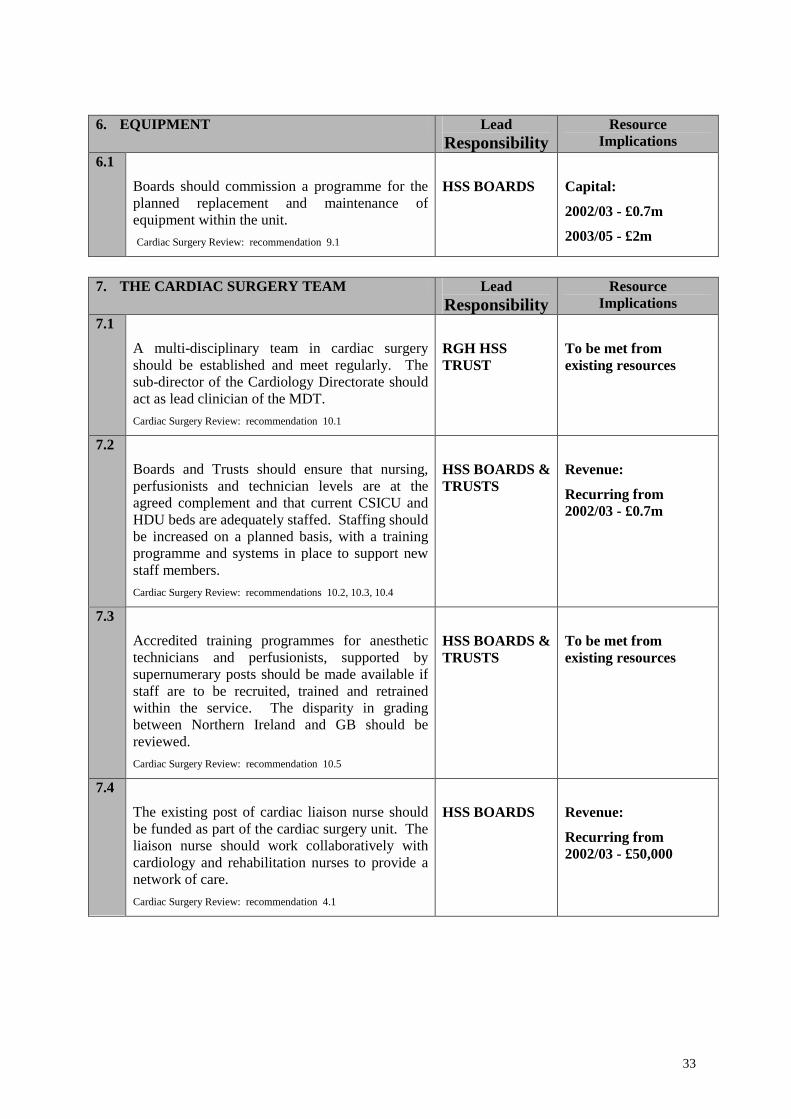
6. EQUIPMENT Lead
Responsibility Resource
Implications 6.1
Boards should commission a programme for the planned replacement and maintenance of equipment within the unit. Cardiac Surgery Review: recommendation 9.1
HSS BOARDS
Capital:
2002/03 - £0.7m
2003/05 - £2m
7. THE CARDIAC SURGERY TEAM Lead
Responsibility Resource
Implications 7.1
A multi-disciplinary team in cardiac surgery should be established and meet regularly. The sub-director of the Cardiology Directorate should act as lead clinician of the MDT. Cardiac Surgery Review: recommendation 10.1
RGH HSS TRUST
To be met from existing resources
7.2
Boards and Trusts should ensure that nursing, perfusionists and technician levels are at the agreed complement and that current CSICU and HDU beds are adequately staffed. Staffing should be increased on a planned basis, with a training programme and systems in place to support new staff members. Cardiac Surgery Review: recommendations 10.2, 10.3, 10.4
HSS BOARDS & TRUSTS
Revenue:
Recurring from 2002/03 - £0.7m
7.3
Accredited training programmes for anesthetic technicians and perfusionists, supported by supernumerary posts should be made available if staff are to be recruited, trained and retrained within the service. The disparity in grading between Northern Ireland and GB should be reviewed. Cardiac Surgery Review: recommendation 10.5
HSS BOARDS & TRUSTS
To be met from existing resources
7.4
The existing post of cardiac liaison nurse should be funded as part of the cardiac surgery unit. The liaison nurse should work collaboratively with cardiology and rehabilitation nurses to provide a network of care. Cardiac Surgery Review: recommendation 4.1
HSS BOARDS
Revenue:
Recurring from 2002/03 - £50,000
34
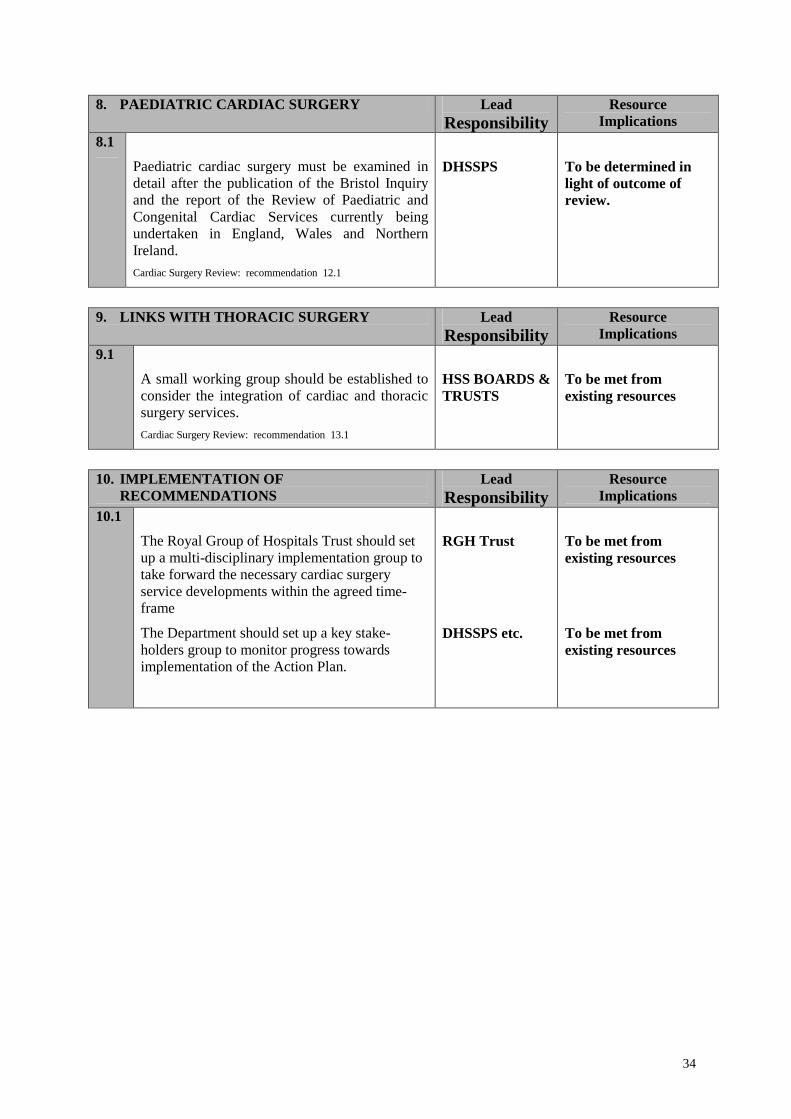
8. PAEDIATRIC CARDIAC SURGERY Lead Responsibility
Resource Implications
8.1
Paediatric cardiac surgery must be examined in detail after the publication of the Bristol Inquiry and the report of the Review of Paediatric and Congenital Cardiac Services currently being undertaken in England, Wales and Northern Ireland. Cardiac Surgery Review: recommendation 12.1
DHSSPS
To be determined in light of outcome of review.
9. LINKS WITH THORACIC SURGERY Lead
Responsibility Resource
Implications 9.1
A small working group should be established to consider the integration of cardiac and thoracic surgery services. Cardiac Surgery Review: recommendation 13.1
HSS BOARDS & TRUSTS
To be met from existing resources
10. IMPLEMENTATION OF
RECOMMENDATIONS Lead
Responsibility Resource
Implications 10.1
The Royal Group of Hospitals Trust should set up a multi-disciplinary implementation group to take forward the necessary cardiac surgery service developments within the agreed time-frame
The Department should set up a key stake-holders group to monitor progress towards implementation of the Action Plan.
RGH Trust
DHSSPS etc.
To be met from existing resources
To be met from existing resources

35
Appendix 4
CARDIOLOGY
&
CARDIAC SURGERY
EQUALITY ISSUES
36
Equality Obligations
The Northern Ireland Act, 1998, has placed new statutory equality obligations on each
of the bodies within the HSSPS family. From 1 January 2000, the Department and all
of its associated bodies must, in carrying out their functions, have due regard to the
need to promote equality of opportunity:
• between persons of different religious belief, political opinion, racial group, age,
marital status or sexual orientation;
• between men and women generally;
• between persons with a disability and persons without; and
• between persons with dependants and persons without.
Without prejudice to these obligations, a public authority is also required, in carrying
out its functions, to have regard to the desirability of promoting good relations
between persons of different religious belief, political opinion or racial group.
While the Department will undertake a full equality impact assessment on the
recommendations contained within this report, with regard to equity of access to
cardiac surgery services there are a number of issues which it may be useful to
highlight at this stage.
Age
The risk of heart disease increases with advancing age. Older people are more likely
to suffer from more severe cardiac disease which has the potential for substantial
improvement using modern day cardiac surgery interventions.
While chronological age is not a barrier to treatment, there is a perception, often
highlighted in the media and medical literature, that ageism exists in relation to access
to cardiac interventions. The age range of those who undergo cardiac surgery here
37
demonstrates that the majority are aged over 50 years, with a small number aged over
80 years.
Gender
Nationally and internationally, cardiac heart disease is much more common in men
than in women. At any age the absolute risk of a coronary event in women is about a
fifth of that for men.
Relatively few studies in this area have concentrated specifically on women.
However, national and international patterns suggest that women are proportionately
under represented among patients undergoing cardiac surgery.
Deprivation
Although deprivation does not fall within the range of issues which the Department
must consider under its equality impact assessment, there is a clear relationship
between coronary heart disease and social deprivation which must be taken into
account by those who plan and deliver the service.
Internationally, there is a substantial body of research evidence which clearly
demonstrates the relationship between socio-economic deprivation and high levels of
coronary heart disease. While the overall death rates from coronary heart disease have
been falling for the last two decades, the death rate for men aged under 65 in the most
deprived communities continues to rise. Much of this variation in mortality rates by
deprivation can be explained by differences in risk factor prevalence rather than
access to cardiology services and cardiac surgery.
As highlighted in 'Investing for Health', the Department and the Executive is
committed to addressing inequalities in health. In this regard and with reference to its
statutory equality obligations, the Department would welcome views on the potential
equality implications of the recommendations outlined in this report.

38

39
Appendix 5
CARDIOLOGY
&
CARDIAC SURGERY
GLOSSARY
40
Acute myocardial infarction
Heart attack. Refers to the death of heart muscle (myocardium) which follows sudden reduction in or cessation of the flow of blood down the coronary arteries, e.g. narrowing due to atheroma of the vessels, leading to thrombosis in the coronary arteries. Advanced life support Attempt to restore spontaneous circulation following cardiac arrest using basic life support, defibrillation, advanced airway management and drugs. Angina, angina pectoris
Literally pain in the chest. Usually gripping or crushing in nature in the chest and/or left arm and jaw felt when there is insufficient blood supply to the heart muscle.
Stable angina is the term used for angina (pectoris) which is relatively predictable and the intensity and frequency of which remains similar over long periods.
Unstable angina is angina (pectoris) which is severe and unpredictable and which threatens to progress to an acute myocardial infarction.
Angiogram
A procedure in which a fine catheter is inserted via a blood vessel to inject x-ray opaque dye into the coronary arteries to obtain an x-ray image of the anatomy of the coronary arteries. Angioplasty
A procedure in which a small balloon on the end of a catheter is inserted into an artery (in CHD the coronary arteries) and inflated to widen a narrowed artery.
41
Arrhythmia
An abnormal rhythm of the heart. Artery
A blood vessel that carries blood away from the heart. Atheroma
Deposits of fatty material and cholesterol inside the walls of arteries. Atherosclerosis
Narrowing and thickening of arteries due to the development of fibrous tissue in the wall and sometimes calcium deposits. Usually associated with atheroma. CABG
Coronary artery bypass grafting. An open-heart operation in which blockages to the coronary arteries are bypassed by grafting on a length of artery or vein to bring a fresh blood supply to the heart muscle. Cardiac arrest
Complete cessation of the heart beat. Cardio-pulmonary resuscitation (CPR) The techniques of treating arrest of the heart by artificial respiration and cardiac compression.
42
Cardiothoracic
Of the heart and chest contents e.g. oesophagus and lungs. Catheter, cardiac
A long, narrow tube which, when passed through the veins or arteries into the heart cavities is used for measuring pressures or injecting x-ray opaque dye for outlining the heart and blood vessels. Catheterisation laboratory
The x-ray laboratory in which an angiogram is performed. Coronary angiogram
An angiogram of the coronary arteries. Coronary arteries
The arteries that supply the heart muscle with blood. Coronary heart disease
Narrowing or blockage of the coronary arteries by atheroma, leading to angina, coronary thrombosis or heart attack, heart failure, and/or sudden death. Defibrillator
An instrument for delivering an electric shock in an attempt to terminate ventricular fibrillation.
43
Electrocardiogram (ECG) A recording of the heart’s electrical activity obtained from electrodes positioned on the chest wall and limbs. An exercise (stress) ECG is taken before and during exercise (usually using a treadmill or stationary bicycle) to obtain objective and quantitative recording of myocardial ischaemia on exertion. Echocardiogram
An image and measurement of the heart obtained using ultrasound. Embolism
The migration through the bloodstream of a blood clot from one part of the body to another where it causes an occlusion. Infarction
Death of tissue following interruption of the blood supply. Ischaemia
Blood supply inadequate for tissue needs especially during exercise. Perfusionist
Specially trained staff who manage the heart-lung bypass equipment used during open heart surgery. Primary care
The conventional first point of contact between a patient and the National Health Service.
44
Primary prevention
The prevention of the development of a condition e.g. CHD, by avoidance of factors known to contribute to its development e.g. smoking, lack of exercise. See also secondary prevention. Protocols
A plan detailing the steps that will be taken in the treatment of a patient or in a research study. Percutaneous intervention A composite term that includes PTCA and stenting Percutaneous transluminal coronary angioplasty (PTCA) Angioplasty of the coronary arteries i.e. the introduction of a balloon on a catheter through the skin (percutaneous), into a blood vessel (transluminal) and into the coronary arteries to widen them. Revascularisation
A procedure to improve the blood supply. In the case of CHD these include CABG and PTCA. Secondary prevention
In the case of CHD, interventions such as lifestyle changes or drugs aimed at slowing or reversing the progression of disease.
45
Stent
An artificial structure inserted into a coronary artery following PTCA to support the vessel wall and reduce the risk of re-occlusion. Tertiary centre
A major medical centre providing open-heart surgery and PTCA, which receives referrals from both primary and secondary care. Thrombolysis
The lysis (dissolving) of blood clots by the use of thrombolytic drugs. Thrombolytic therapy
A class of drugs used to achieve thrombolysis. Thrombosis
The process of clot formation (thrombus – clot). Unstable angina pectoris
Angina which threatens progression to heart attack. Ventricles
The two main pumping chambers of the heart.