Embed Size (px)
Citation preview

Short Stature
Jackson Smith M.D.
Division of Endocrinology
University of Kentucky
Objectives
Review growth charts
Discuss initial evaluation
• Mid-parental height
• Bone age
• Laboratory studies
Identify patients eligible for GH therapy
Who are Candidates for GH
GH deficient
Turner syndrome
SGA
• No catch-up growth by age 2
Idiopathic short stature
• < 2.25 SD below mean for age
Chronic renal failure
• Pre-transplant
Prader-Willi syndrome
Noonan syndrome
Short stature homeobox (SHOX) gene mutation
Growth Charts
www.cdc.gov/growthcharts
Clinical growth charts
3rd to 97th %http://www.cdc.gov/growthcharts/clinical_charts.h
tm#Set2
2.25th to 97th %http://www.humatrope.com/Documents/pdf/growth_chart_b
oth.pdf
OK135S067
http://www.humatrope.com/Documents/pdf/growth_chart_both.pdf

Definitions
Short stature:
• Height more than 2 SD below the population mean (or less than the 3rd %).
Growth failure:
Short Stature: Initial Evaluation
History• Birth length and weight• Parent (family) heights and growth history• Chronic illnesses and/or medications• Nutrition• Thorough review of systems
Examination Calculate target height Consider obtaining a “bone age”
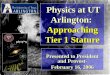
Height Distribution of Patients
- 4 - 2 0 2 4
0.0
0.2
0.4
0.6
0.8
1.0
Height SDS
Average adult height
General Population
M: 5' 9”F: 5' 4”
Average adult height (US general population*)
*From Kuczmarski RJ et al. 2000 NCHS
Target Height(Mid-parental Height)
Target height for males (inches) =
father’s height + (mother’s height + 5 inches) 2
Target height for females (inches) = mother’s height + (father’s height - 5 inches) 2
Height may vary by +/- 4 inches (2 SD) from target height

“Bone Age”
AP view of left hand Result: age in years (and months) Congruent with age
• Genetic short stature• Primary growth abnormality
“Delayed” = < 2SD for age• Nonspecific:
– Many secondary causes (hypothyroid, GH deficiency)– Seen with some primary growth abnormalities
• Constitutional delay in growth
Predicted Height
Baley-Pinneau
• Most commonly used method.
• May be requested with bone age report:– Patients height needed to calculate.
– If available from radiologist!
• Assumes a normal growth velocity.
Greatest source of inaccuracy: inaccurate bone age interpretation.
Short Stature: Differential Diagnosis
Conditions evident by age 3. Genetic short stature Constitutional delay of growth Primary growth abnormalities
• Small for gestational age (SGA)• Abnormalities in bone formation:
– Is the child dysmorphic?– Does the child have:
• Turner syndrome• Prader-Willi syndrome• Noonan syndrome
Secondary Growth Disorders Chronic disease (chronic renal insufficiency)
Malnutrition Endocrine
• Hypothyroidism• Growth hormone deficiency
– Isolated– Hypopituitarism
• Cushing syndrome• Calcium and mineralization disorders
– Rickets– Calcium, phosphorus abnormalities
MM
M
--- M 6.5”M 5”11”
5’2”

Genetic Short Stature Other names: familial or intrinsic short stature
Height compatible with mid-parental height.
Child is:
• Otherwise healthy
• Proportional and non-dysmorphic
Bone age = chronological age.
Follow-up: height maintains same %
Constitutional Delay in Growth
Diagnosis of exclusion.
History and physical exam normal.
Family history: delayed growth and/or puberty (not always present).
Bone age delayed.
Predicted height consistent with parental heights.
Growth rate normal.
Normal laboratory evaluation: if needed?

Laboratory Evaluation
Chronic disease and calcium disorders:• CBC, sedimentation rate, electolytes,
CO2, creatinine, calcium, UA Hypothyroidism:
• TSH (primary) and Free T4 (central) Growth hormone deficiency:
• IGF-I
Laboratory Evaluation
If associated with delayed puberty
• FSH
Others based on history and physical
• Celiac disease testing– Tissue transglutaminase antibody
• Karyotype
Constitutional Delay in Growth
Normal growth velocity
Typically have a delay in onset of puberty.
• Abnormal delay:– Girls: no breast development by 13 years.
– Boys: no testicular enlargment by 14 years.
Height may drop further below the 3rd % when peers enter puberty.
Requires follow-up of linear growth and pubertal development in ~6 months (longer in most cases).
SGA
90% will achieve “catch-up” growth by age 2 (height > 2.3%).
10% will remain < 2SD below average.
Adult height• SGA patients: height < 3% at age 2
– 95% will be short adultsPediatric Research 1995;38:733-9
July 2001 FDA approves use of GH for “SGA children who do not achieve catch-up growth by 2 years of age”.
Turner Syndrome
Incidence: 1:2500 newborn girls
Short stature evident by 3 years old (older if mosiac karyotype)
Karyotype:
• Classic: 45,X
• Many other mosiac forms
Dysmorphic features may be few or absent in mosiac varieties
Turner Syndrome: Classic Features
Short stature 100%
Gonadal failure 94%
Abnormal upper-to
-lower segment ratio 90%
Otitis media 75%
Characteristic facies
with micrognathia 60%
Cubitus valgus 45%
Low posterior hairline 40%
High arched palate 35%
Short metacarpals 35%
Genu valgum 30%
Multiple nevi 25%
Webbed neck 23%
Strabismus 17%
Scoliosis 12%
Nail dysplasia 12%

SHOX Mutation
Short stature homeobox (SHOX) gene mutation
Laboratory Evaluation
Chronic disease and calcium disorders:• CBC, sedimentation rate, electolytes,
CO2, creatinine, calcium, UA Hypothyroidism:
• TSH (primary) and Free T4 (central) Growth hormone deficiency:
• IGF-I
Laboratory Evaluation
If associated with delayed puberty
• FSH
Others based on history and physical
• Celiac disease testing– Tissue transglutaminase antibody
• Karyotype
Height -2.25 SDS (1.2 percentile)
No distinguishing phenotypic features
Likely heterogeneous etiology, such as:
• Familial/genetic factors
• Abnormalities of GH/IGF axis
• Abnormalities of growth plate
IGF-I may be normal or low
Height velocity may be normal or low
Idiopathic Short Stature (ISS)
http://www.humatrope.com/Documents/pdf/growth_chart_both.pdf
GH Treatment of ISS
ISS is a diagnosis of exclusion• May include patients with:
– Genetic short stature– Constitutional delay in growth
Criteria for possible treatment with GH• Predicted adult height (based on BA)
– Less than 5 feet 3 inches: males– Less than 4 feet 11 inches: females
GH therapy is not approved to treat less severe short stature!

GH Treatment
Risks• Slipped capital femoral epiphysis
• Pseudotumor cerebri
• Pancreatitis
• Increased long term mortality?
– Increased death due to bone tumors or cerebral hemorrhage
– Duration or follow-up from start of GH to time of census or death ~ 17 years
– Greater risk seen in those on higher dosages
– J Clin Endocrinol Metab 97: 416–425, 2012
GH Treatment
Cost
• About $50 per mg– 4 year old (15 kg) = $12,000/year
– 16 year old (60 kg) = $48,000/year
• Estimated cost in ISS: $50,000 per inch!
(based on 2006 calculation)
FDA Approved Indications for GH Therapy
GH deficient
Turner syndrome
Prader-Willi syndrome
SGA or IUGR
• Lack of “catch up” growth by age 2
Idiopathic short stature
• < 2.25 SDS or
• < (1.2 percentile) or
• Predicted height– < 5’3” boys
– < 4’11” girls
Chronic renal failure
• Pre-transplant